

Vitamins in the Prevention and Support Therapy of Neurodegenerative Diseases

 ,
,  , , , , , and
, , , , , and 
Abstract
1. Introduction
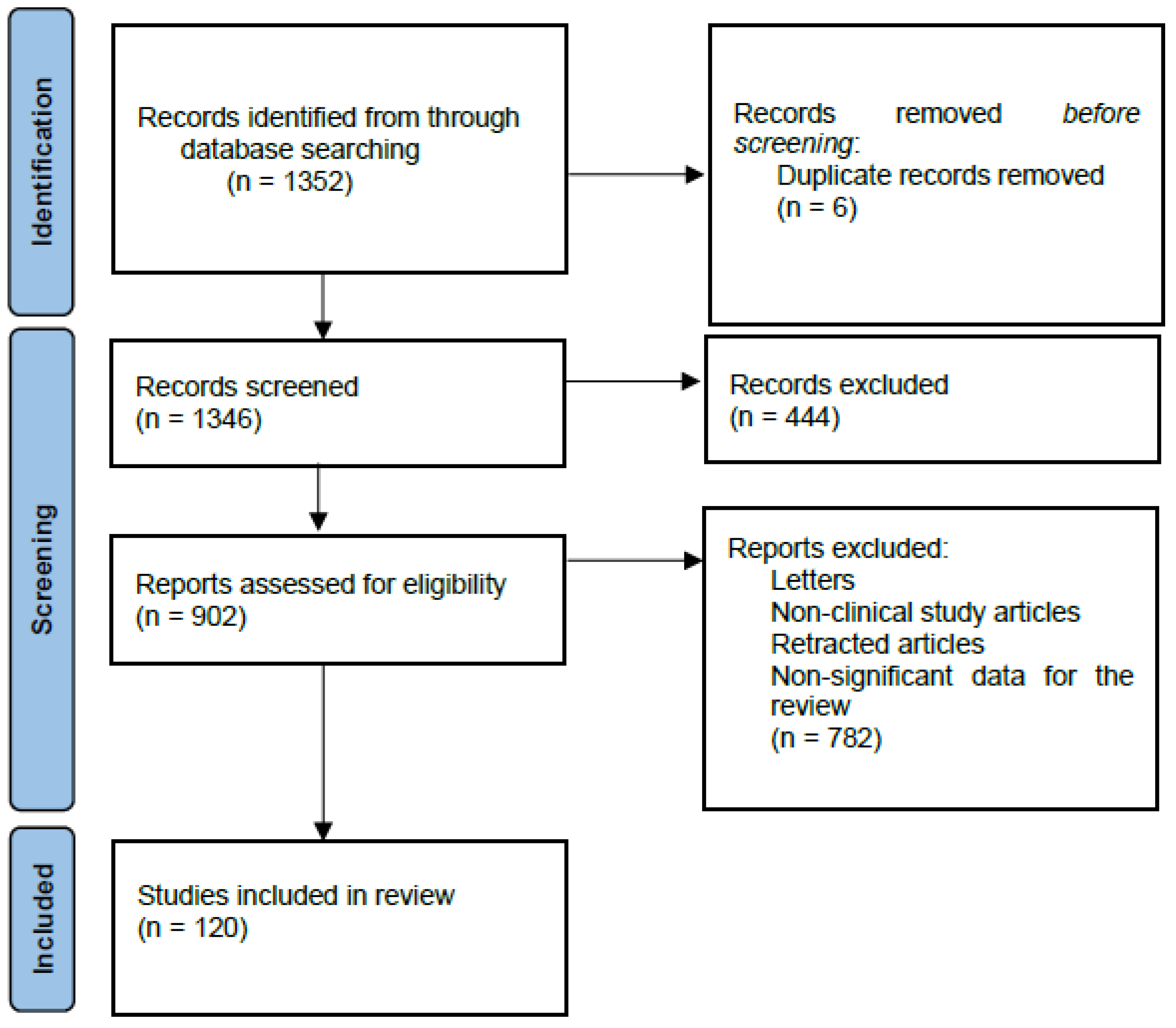
2. Methods
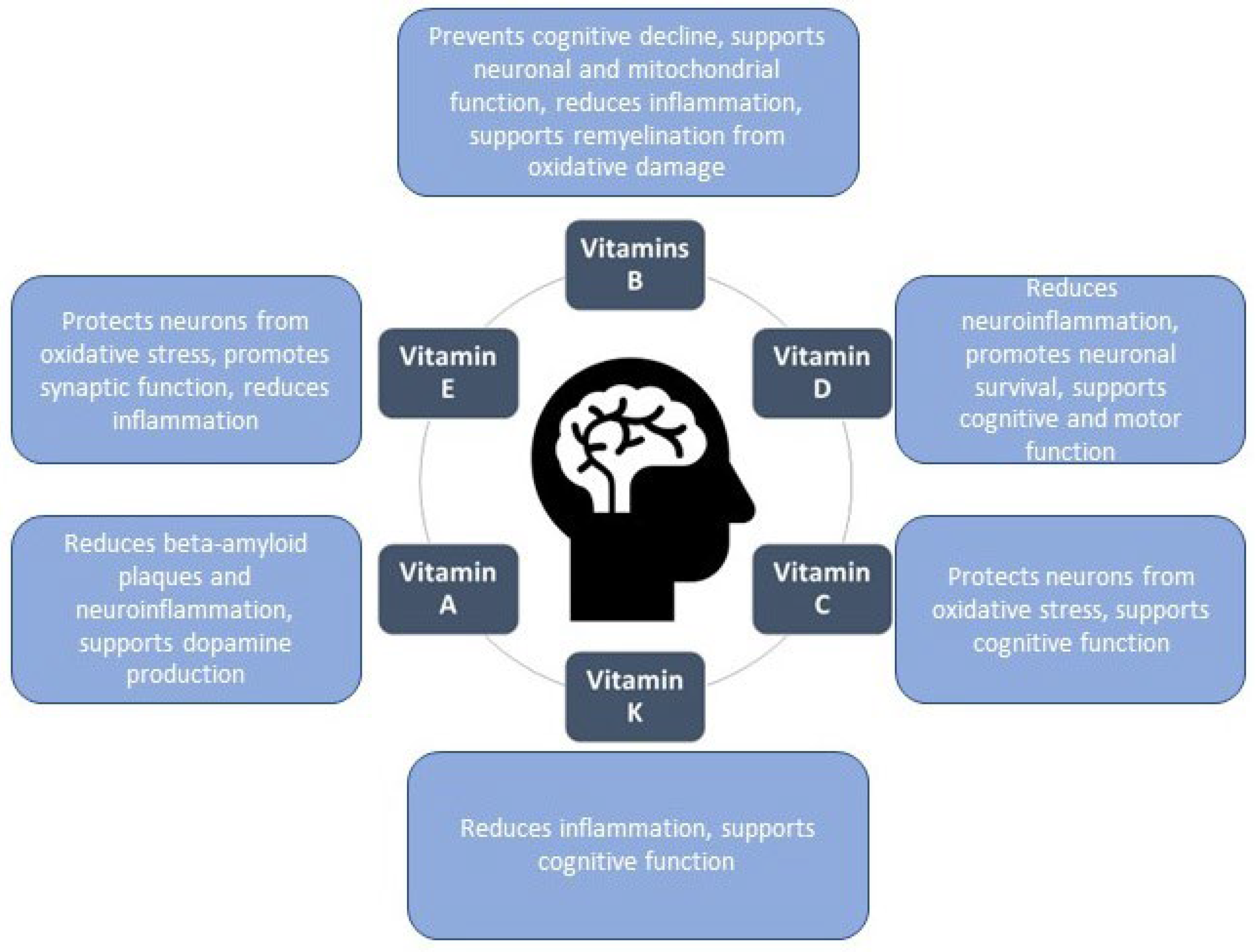
3. Vitamins in Neurodegenerative Diseases
3.1. Water-Soluble Vitamins
3.1.1. Vitamins B
3.1.2. Vitamin C
3.2. Fat-Soluble Vitamins
3.2.1. Vitamin D
3.2.2. Vitamin E
3.2.3. Vitamin A
3.2.4. Vitamin K
4. The Authorized Health Claims Related to the Vitamins Relevant toNeurodegenerative Diseases
5. Conclusion

{kind=link}
{kind=link}
| Vitamin | Main Function in the Brain | Neuroprotective Effect | Nutritional Source | References |
|---|---|---|---|---|
| B1 | Energy metabolism, neuronal function | Prevents cognitive decline, supports neuronal function | Whole grains, pork, sunflower seeds, pistachio nuts, soybeans, brown rice, legumes (lentils, beans) | [10,11,12,13,19,100,101] |
| B2 | Energy metabolism, antioxidant defense, neurotransmitter regulation, and myelin health | Supports cognitive functions and visual perception, protects neurons from oxidative stress | Milk, liver, pork, beef, eggs, green leafy vegetables, almonds | [16,17,19,100,102] |
| B3 | Energy metabolism, antioxidant defense, neurotransmitter regulation, anti-inflammatory | Supports mitochondrial function, reduces inflammation, protects neurons from oxidative damage, improves cognitive function | Poultry, fish (tuna, salmon), peanuts, macadamia nuts, pork, beef, mushrooms, whole grains | [19,21,22,23,24,25,100,102] |
| B6 | Neurotransmitter synthesis (serotonin, dopamine, GABA), homocysteine metabolism | Reduces cognitive decline, supports mood and motor control, lowers homocysteine | Bananas, potatoes, poultry, fish, chickpeas | [10,19,26,28] |
| B7 | Myelin synthesis, mitochondrial energy metabolism, gene expression | Supports remyelination, reduces inflammation, promotes neuron survival and energy metabolism | Egg yolks, nuts, seeds, salmon, dairy products, sweet potatoes | [19,31,32,33] |
| B9 | DNA synthesis, repair, homocysteine regulation, neurotransmitter synthesis | Lowers homocysteine, prevents cognitive decline, supports neurodevelopment | Leafy greens (spinach, kale), citrus fruits, beans, peas | [19,35,36,37,38,39,41,42,45,100] |
| B12 | DNA synthesis, myelin formation, homocysteine regulation, neurotransmitter regulation | Protects myelin, reduces oxidative stress, supports motor and cognitive function | Meat, fish, eggs, dairy products | [10,19,37,39,41,42,43,44,45,46,103] |
| D | Calcium homeostasis, neuroinflammation, neurotransmitter regulation | Reduces neuroinflammation, promotes neuronal survival, supports cognitive and motor function | Fatty fish (salmon, mackerel, sardines), egg yolks, butter | [58,59,60,61,62,63,64,102] |
| E | Antioxidant, neurotrophic factor support | Protects neurons from oxidative stress, promotes synaptic function, reduces inflammation | Nuts (almonds, sunflower seeds), spinach, avocado, vegetable oils (sunflower, safflower, wheat germ) | [67,69,71,72,73,78,104] |
| A | Synaptic plasticity, gene regulation, immune modulation | Reduces beta-amyloid plaques, supports dopamine production, reduces neuroinflammation | Plant sources (as beta-carotene): carrots, sweet potatoes, spinach, kale, mangoes, and apricots; liver, meat, fish, eggs, milk | [71,73,78,79,80] |
| C | Antioxidant, neurotransmitter synthesis, neuroprotection | Protects neurons from oxidative stress, supports cognitive function | Citrus fruits (oranges, lemons, grapefruits), strawberries, kiwi, bell peppers, broccoli, tomatoes | [49,50,51,52,54,56,57] |
| K | Sphingolipid metabolism, anti-inflammatory | Reduces inflammation, supports cognitive function | Green leafy vegetables (kale, spinach, broccoli), soybeans | [85,86,87,88,89,90,91,92,93,95,105] |
| Vitamin | Key Findings | Reference |
|---|---|---|
| Vitamin A | Improves cognitive deficits in Alzheimer’s Disease patients | [106] |
| Beneficial effect on reference memory | [107] | |
| Vitamin D | Enhances cognitive performance and reduces Aβ-related biomarkers in Alzheimer’s Disease patients | [108] |
| Prevents cognitive decline and improves spatial learning and memory in aging rats | [109] | |
| Vitamin E | Lowers risk of Parkinson’s Disease | [73] |
| Prevents the loss of dopaminergic neurons | [110] | |
| Beneficial effect on AD-related neuropathologic changes | [111] | |
| Vitamin E + carotenoids + omega-3 fatty acids | Results in positive outcomes, reducing the severity of the disease in Alzheimer’s Disease patients | [71] |
| Vitamin B3 + B6 + B12 + Folate | Improves cognitive performance, decreases homocysteine levels, inhibits the expression of inflammatory factors | [37] |
| Vitamin B9 + B12 | Improves cognitive function in patients with atrophy ratios higher than the median | [112] |
| Folic acid + vitamin B6 + vitamin B12 | Slows the atrophy of specific brain regions that are a key component of the Alzheimer’s Disease process and that are associated with cognitive decline | [113] |
| Vitamin C | Decreases the accumulation of amyloid plaques; improves the degenerative alterations in the brain of Alzheimer’s Disease mice, leading to improvement in blood–brain barrier disruption and changes in mitochondrial function | [56] |
| Vitamin C + E | Reduces the vulnerability of CSF and plasma lipoproteins to oxidation | [114] |
| Significant effect on the course of Alzheimer’s Disease over 1 year of supplementation | [115] | |
| K | Reduces neuronal deterioration and cognitive loss | [116] |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xu Lou, I.; Ali, K.; Chen, Q. Effect of nutrition in Alzheimer’s disease: A systematic review. Front. Neurosci. 2023, 17, 1147177. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://neurodegenerationresearch.eu/ (accessed on 27 November 2024).
- Garre-Olmo, J. Epidemiología de la Enfermedad de Alzheimer y Otras Demencias. Rev. Neurol. 2018, 66, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Lamptey, R.N.L.; Chaulagain, B.; Trivedi, R.; Gothwal, A.; Layek, B.; Singh, J. A Review of the Common Neurodegenerative Disorders: Current Therapeutic Approaches and the Potential Role of Nanotherapeutics. Int. J. Mol. Sci. 2022, 23, 1851. [Google Scholar] [CrossRef] [PubMed]
- Tsagalioti, E.; Trifonos, C.; Morari, A.; Vadikolias, K.; Giaginis, C. Clinical Value of Nutritional Status in Neurodegenerative Diseases: What Is Its Impact and How It Affects Disease Progression and Management? Nutr. Neurosci. 2018, 21, 162–175. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, V.E.; Herrera, P.F.; Laura, R. Effect of Nutrition on Neurodegenerative Diseases. A Systematic Review. Nutr. Neurosci. 2021, 24, 810–834. [Google Scholar] [CrossRef]
- Bakulski, K.M.; Seo, Y.A.; Hickman, R.C.; Brandt, D.; Vadari, H.S.; Hu, H.; Park, S.K. Heavy Metals Exposure and Alzheimer’s Disease and Related Dementias. J. Alzheimers Dis. 2020, 76, 1215–1242. [Google Scholar] [CrossRef]
- Kumar, R.R.; Singh, L.; Thakur, A.; Singh, S.; Kumar, B. Role of Vitamins in Neurodegenerative Diseases: A Review. CNS Neurol. Disord. Drug Targets 2022, 21, 766–773. [Google Scholar] [CrossRef]
- Helberger, N.; Forms Matter: Informing Consumers Effectively. BEUC 2013. Available online: http://www.beuc.eu/publications/x2013_089_upa_form_matters_september_2013.pdf (accessed on 27 November 2024).
- Calderon-Ospina, C.A.; Nava-Mesa, M.O. B vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci. Ther. 2020, 26, 5–13. [Google Scholar] [CrossRef]
- Gibson, G.E.; Hirsch, J.A.; Fonzetti, P.; Jordan, B.D.; Cirio, R.T.; Elder, J. Vitamin B1 (thiamine) and dementia. Ann. N. Y. Acad. Sci. 2016, 1367, 21–30. [Google Scholar] [CrossRef]
- Jia, W.; Wang, H.; Li, C.; Shi, J.; Yong, F.; Jia, H. Association between dietary vitamin B1 intake and cognitive function among older adults: A cross-sectional study. J. Transl. Med. 2024, 22, 165. [Google Scholar] [CrossRef]
- Costantini, A.; Pala, M.I.; Compagnoni, L.; Colangeli, M. High-dose thiamine as initial treatment for Parkinson’s disease. BMJ Case Rep. 2013, 2013, bcr2013009289. [Google Scholar] [CrossRef] [PubMed]
- Goncharova, P.S.; Davydova, T.K.; Popova, T.E.; Novitsky, M.A.; Petrova, M.M.; Gavrilyuk, O.A.; Al-Zamil, M.; Zhukova, N.G.; Nasyrova, R.F.; Shnayder, N.A. Nutrient Effects on Motor Neurons and the Risk of Amyotrophic Lateral Sclerosis. Nutrients 2021, 13, 3804. [Google Scholar] [CrossRef] [PubMed]
- Bettendorff, L. Thiamin. In Present Knowledge in Nutrition, 10th ed.; Erdman, J.W., Macdonald, I.A., Zeisel, S.H., Eds.; Wiley-Blackwell: Washington, DC, USA, 2012; pp. 261–279. [Google Scholar]
- Suwannasom, N.; Kao, I.; Pruß, A.; Georgieva, R.; Bäumler, H. Riboflavin: The health benefits of a forgotten natural vitamin. Int. J. Mol. Sci. 2020, 21, 950. [Google Scholar] [CrossRef] [PubMed]
- Plantone, D.; Pardini, M.; Rinaldi, G. Riboflavin in Neurological Diseases: A Narrative Review. Clin. Drug Investig. 2021, 41, 513–527. [Google Scholar] [CrossRef]
- Beathard, K.M.; Georghiades, N.; Goulart, J.B.; Riviere, A.J.; Sullivan, C.; Mascarro, M.; Riechman, S.E. The impact of nutrition on visual cognitive performance in the nutrition, vision, and cognition in sport study. Front. Nutr. 2023, 10, 1208890. [Google Scholar] [CrossRef]
- Depeint, F.; Bruce, W.R.; Shangari, N.; Mehta, R.; O’Brien, P.J. Mitochondrial function and toxicity: Role of the B vitamin family on mitochondrial energy metabolism. Chem. Biol. Interact. 2006, 163, 94–112. [Google Scholar] [CrossRef]
- Cunniffe, N.; Vuong, K.A.; Ainslie, D.; Baker, D.; Beveridge, J.; Bickley, S.; Camilleri, P.; Craner, M.; Fitzgerald, D.; de la Fuente, A.G.; et al. Systematic approach to selecting licensed drugs for repurposing in the treatment of progressive multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2020, 92, 295–302. [Google Scholar] [CrossRef]
- Morris, M.C.; Evans, D.A.; Bienias, J.L.; Scherr, P.A.; Tangney, C.C.; Hebert, L.E.; Bennett, D.A.; Wilson, R.S.; Aggarwal, N. Dietary niacin and the risk of incident Alzheimer’s disease and of cognitive decline. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1093–1099. [Google Scholar] [CrossRef]
- Klimova, N.; Kristian, T. Multi-targeted Effect of Nicotinamide Mononucleotide on Brain Bioenergetic Metabolism. Neurochem. Res. 2019, 44, 2280–2287. [Google Scholar] [CrossRef]
- Liu, Z.; Li, C.; Fan, X.; Kuang, Y.; Zhang, X.; Chen, L.; Song, J.; Zhou, Y.; Takahashi, E.; He, G.; et al. Nicotinamide, a vitamin B3 ameliorates depressive behaviors independent of SIRT1 activity in mice. Mol. Brain 2020, 13, 162. [Google Scholar] [CrossRef]
- Rawji, K.S.; Young, A.M.H.; Ghosh, T.; Michaels, N.J.; Mirzaei, R.; Kappen, J.; Kolehmainen, K.L.; Alaeiilkhchi, N.; Lozinski, B.; Mishra, M.K.; et al. Niacin-mediated rejuvenation of macrophage/microglia enhances remyelination of the aging central nervous system. Acta Neuropathol. 2020, 139, 893–909. [Google Scholar] [CrossRef]
- Wuerch, E.; Urgoiti, G.R.; Yong, V.W. The Promise of Niacin in Neurology. Neurotherapeutics 2023, 20, 1037–1054. [Google Scholar] [CrossRef]
- Stover, P.J.; Field, M.S. Vitamin B-6. Adv. Nutr. 2015, 6, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Hooshmand, B.; Solomon, A.; Kareholt, I.; Leiviskä, J.; Rusanen, M.; Ahtiluoto, S.; Winblad, B.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Homocysteine and holotranscobalamin and the risk of Alzheimer disease: A longitudinal study. Neurology 2010, 75, 1408–1414. [Google Scholar] [CrossRef]
- Modica, J.S.; Bonno, D.; Lizarraga, K.J. Pearls and oysters: Vitamin B6 deficiency presenting with new-onset epilepsy and status epilepticus in a patient with Parkinson disease. Neurology 2020, 94, e2605–e2607. [Google Scholar] [CrossRef]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: A randomized controlled trial. PLoS ONE 2010, 5, e12244. [Google Scholar] [CrossRef]
- Calderon-Ospina, C.A.; Nava-Mesa, M.O.; Paez-Hurtado, A.M. Update on Safety Profiles of Vitamins B1, B6, and B12: A Narrative Review. Ther. Clin. Risk Manag. 2020, 16, 1275–1288. [Google Scholar] [CrossRef]
- Sedel, F.; Bernard, D.; Mock, D.M.; Tourbah, A. Targeting demyelination and virtual hypoxia with high-dose biotin as a treatment for progressive multiple sclerosis. Neuropharmacology 2016, 110 Pt B, 644–653. [Google Scholar] [CrossRef]
- McCarty, M.F.; DiNicolantonio, J.J. Neuroprotective potential of high-dose biotin. Med. Hypotheses 2017, 109, 145–149. [Google Scholar] [CrossRef]
- León-Del-Río, A. Biotin in metabolism, gene expression, and human disease. J. Inherit. Metab. Dis. 2019, 42, 647–654. [Google Scholar] [CrossRef]
- Ben Aissa, M.; Lee, S.H.; Bennett, B.M.; Thatcher, G.R. Targeting NO/cGMP Signaling in the CNS for Neurodegeneration and Alzheimer’s Disease. Curr. Med. Chem. 2016, 23, 2770–2788. [Google Scholar] [CrossRef]
- Bennett, C.; Green, J.; Ciancio, M.; Goral, J.; Pitstick, L.; Pytynia, M.; Meyer, A.; Kwatra, N.; Jadavji, N.P. Dietary folic acid deficiency impacts hippocampal morphology and cortical acetylcholine metabolism in adult male and female mice. Nutr. Neurosci. 2022, 25, 2057–2065. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Zhang, M.; Yang, J.; Zhao, S.; Qin, S.; Chen, H.; Gao, Y.; Huang, G. Relationship between blood levels of methyl donor and folate and mild cognitive impairment in Chinese patients with type 2 diabetes: A case-control study. J. Clin. Biochem. Nutr. 2014, 54, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, S.; Ge, B.; Zhou, D.; Li, M.; Li, W.; Ma, F.; Liu, Z.; Ji, Y.; Huang, G. Effects of Folic Acid and Vitamin B12 Supplementation on Cognitive Impairment and Inflammation in Patients with Alzheimer’s Disease: A Randomized, Single-Blinded, Placebo-Controlled Trial. J. Prev. Alzheimer’s Dis. 2021, 8, 249–256. [Google Scholar] [CrossRef]
- Ho, P.I.; Ashline, D.; Dhitavat, S.; Ortiz, D.; Collins, S.C.; Shea, T.B.; Rogers, E. Folate deprivation induces neurodegeneration: Roles of oxidative stress and increased homocysteine. Neurobiol. Dis. 2003, 14, 32–42. [Google Scholar] [CrossRef]
- Liu, Y.; Gou, M.; Guo, X. Features of Plasma Homocysteine, Vitamin B12, and Folate in Parkinson’s Disease: An Updated Meta-Analysis. J. Integr. Neurosci. 2023, 22, 115. [Google Scholar] [CrossRef]
- Hu, N.; Wang, X. The level of homocysteine in amyotrophic lateral sclerosis: A systematic review and meta-analysis. Neurol. Sci. 2023, 44, 1185–1192. [Google Scholar] [CrossRef]
- Shemirani, F.; Titcomb, T.J.; Saxby, S.M.; Eyck, P.T.; Rubenstein, L.M.; Hoth, K.F.; Snetselaar, L.G.; Wahls, T.L. Association of serum homocysteine, folate, and vitamin B12 and mood following the Swank and Wahls elimination dietary interventions in relapsing-remitting multiple sclerosis: Secondary analysis of the WAVES trial. Mult. Scler. Relat. Disord. 2023, 75, 104743. [Google Scholar] [CrossRef]
- Lee, C.Y.; Chan, L.; Hu, C.J.; Hong, C.-T.; Chen, J.C. Role of vitamin B12 and folic acid in treatment of Alzheimer’s disease: A meta-analysis of randomized control trials. Aging 2024, 16, 7856–7869. [Google Scholar] [CrossRef]
- El-Mezayen, N.S.; Abd El Moneim, R.A.; El-Rewini, S.H. Vitamin B12 as a cholinergic system modulator and blood brain barrier integrity restorer in Alzheimer’s disease. Eur. J. Pharm. Sci. 2022, 174, 106201. [Google Scholar] [CrossRef]
- Cecchetti, L.; Lettieri, G.; Handjaras, G.; Leo, A.; Ricciardi, E.; Pietrini, P.; Pellegrini, S.; The Train the Brain Consortium. Brain Hemodynamic Intermediate Phenotype Links Vitamin B12 to Cognitive Profile of Healthyand Mild Cognitive Impaired Subjects. Neural Plast. 2019, 2019, 6874805. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Zhou, X.; Li, Q.; Zhao, J.; Song, A.; An, P.; Du, Y.; Xu, W.; Huang, G. Effects of folic acid and vitamin b12, alone and in combination on cognitive function and inflammatory factors in the elderly with mild cognitive impairment: A single-blind experimental design. Curr. Alzheimer Res. 2019, 16, 622–632. [Google Scholar] [CrossRef] [PubMed]
- McCarter, S.J.; Stang, C.; Turcano, P.; Mielke, M.M.; Ali, F.; Bower, J.H.; Savica, R. Higher vitamin B12 level at Parkinson’s disease diagnosis is associated with lower risk of future dementia. Park. Relat. Disord. 2020, 73, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Bagur, M.J.; Murcia, M.A.; Jiménez-Monreal, A.M.; Tur, J.A.; Bibiloni, M.M.; Alonso, G.L.; Martínez-Tomé, M. Influence of Diet in Multiple Sclerosis: A Systematic Review. Adv. Nutr. 2017, 8, 463–472. [Google Scholar] [CrossRef]
- Oki, R.; Izumi, Y.; Fujita, K.; Miyamoto, R.; Nodera, H.; Sato, Y.; Sakaguchi, S.; Nokihara, H.; Kanai, K.; Tsunemi, T.; et al. Japan Early-Stage Trial of Ultrahigh-Dose Methylcobalamin for ALS (JETALS) Collaborators. Efficacy and Safety of Ultrahigh-Dose Methylcobalamin in Early-Stage Amyotrophic Lateral Sclerosis: A Randomized Clinical Trial. JAMA Neurol. 2022, 79, 575–583. [Google Scholar] [CrossRef]
- Hansen, S.N.; Tveden-Nyborg, P.; Lykkesfeldt, J. Does vitamin C deficiency affect cognitive development and function? Nutrients 2014, 6, 3818–3846. [Google Scholar] [CrossRef]
- Eldridge, C.F.; Bunge, M.B.; Bunge, R.P.; Wood, P.M. Differentiation of axon-related Schwann cells in vitro. I. Ascorbic acid regulates basal lamina assembly and myelin formation. J. Cell Biol. 1987, 105, 1023–1034. [Google Scholar] [CrossRef]
- Harrison, F.E.; May, J.M. Vitamin C function in the brain: Vital role of the ascorbate transporter SVCT2. Free Radic. Biol. Med. 2009, 46, 719–730. [Google Scholar] [CrossRef]
- Chang, C.Y.; Chen, J.Y.; Wu, M.H.; Hu, M.L. Therapeutic treatment with vitamin C reduces focal cerebral ischemia-induced brain infarction in rats by attenuating disruptions of blood brain barrier and cerebral neuronal apoptosis. Free Radic. Biol. Med. 2020, 155, 29–36. [Google Scholar] [CrossRef]
- Choudhry, F.; Howlett, D.R.; Richardson, J.C.; Francis, P.T.; Williams, R.J. Pro-oxidant diet enhances beta/gamma secretase-mediated APP processing in APP/PS1 transgenic mice. Neurobiol. Aging 2012, 33, 960–968. [Google Scholar] [CrossRef]
- Nualart, F.; Mack, L.; Garcia, A.; Cisternas, P.; Bongarzone, E.R.; Heitzer, M.; Jara, N.; Martinez, F.; Ferrada, L.; Espinoza, F.; et al. Vitamin C transporters, recycling and the bystander effect in the nervous system: SVCT2 versus gluts. J. Stem Cell Res. Ther. 2014, 4, 209. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wang, X. Antioxidant therapies for Alzheimer’s disease. Oxidative Med. Cell Longev. 2012, 2012, 472932. [Google Scholar] [CrossRef] [PubMed]
- Kook, S.-Y.; Lee, K.-M.; Kim, Y.; Cha, M.-Y.; Kang, S.; Baik, S.H.; Lee, H.; Park, R.; Mook-Jung, I. High-dose of vitamin C supplementation reduces amyloid plaque burden and ameliorates pathological changes in the brain of 5XFAD mice. Cell Death Dis. 2014, 5, e1083. [Google Scholar] [CrossRef] [PubMed]
- Hamid, M.; Mansoor, S.; Amber, S.; Zahid, S. A quantitative meta-analysis of vitamin C in the pathophysiology of Alzheimer’s disease. Front. Aging Neurosci. 2022, 14, 970263. [Google Scholar] [CrossRef]
- Koduah, P.; Paul, F.; Dörr, J.M. Vitamin D in the Prevention, Prediction and Treatment of Neurodegenerative and Neuroinflammatory Diseases. EPMA J. 2017, 8, 313–325. [Google Scholar] [CrossRef]
- Habib, A.M.; Nagi, K.; Thillaiappan, N.B.; Sukumaran, V.; Akhtar, S. Vitamin D and Its Potential Interplay With Pain Signaling Pathways. Front. Immunol. 2020, 11, 820. [Google Scholar] [CrossRef]
- Moretti, R.; Morelli, M.E.; Caruso, P. Vitamin D in Neurological Diseases: A Rationale for a Pathogenic Impact. Int. J. Mol. Sci. 2018, 19, 2245. [Google Scholar] [CrossRef]
- Caccamo, D.; Ricca, S.; Curro, M.; Ientile, R. Health risks of hypovitaminosis D: A review of new molecular insights. Int. J. Mol. Sci. 2018, 19, 892. [Google Scholar] [CrossRef]
- Grimm, M.O.W.; Thiel, A.; Lauer, A.A.; Winkler, J.; Lehmann, J.; Regner, L.; Nelke, C.; Janitschke, D.; Benoist, C.; Streidenberger, O.; et al. Vitamin D and Its Analogues Decrease Amyloid-β (Aβ) Formation and Increase Aβ-Degradation. Int. J. Mol. Sci. 2017, 18, 2764. [Google Scholar] [CrossRef]
- Pignolo, A.; Mastrilli, S.; Davì, C.; Arnao, V.; Aridon, P.; Dos Santos Mendes, F.A.; Gagliardo, C.; D’Amelio, M. Vitamin D and Parkinson’s Disease. Nutrients 2022, 14, 1220. [Google Scholar] [CrossRef]
- Sangha, A.; Quon, M.; Pfeffer, G.; Orton, S.M. The Role of Vitamin D in Neuroprotection in Multiple Sclerosis: An Update. Nutrients 2023, 15, 2978. [Google Scholar] [CrossRef] [PubMed]
- Payne, M.E.; Anderson, J.J.; Steffens, D.C. Calcium and vitamin D intakes may be positively associated with brain lesions in de-pressed and nondepressed elders. Nutr. Res. 2008, 28, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lara, S.Q.; Cardona-Muñoz, E.G.; Ramírez-Lizardo, E.J.; Totsuka-Sutto, S.E.; Castillo-Romero, A.; García-Cobián, T.A.; García-Benavides, L. Alternative Interventions to Prevent Oxidative Damage following Ischemia/Reperfusion. Oxidative Med. Cell Longev. 2016, 2016, 7190943. [Google Scholar] [CrossRef] [PubMed]
- Ulatowski, L.M.; Manor, D. Vitamin E and neurodegeneration. Neurobiol. Dis. 2015, 84, 78–83. [Google Scholar] [CrossRef]
- Cassidy, L.; Fernandez, F.; Johnson, J.B.; Naiker, M.; Owoola, A.G.; Broszczak, D.A. Oxidative stress in alzheimer’s disease: A review on emergent natural polyphenolic therapeutics. Complement. Ther. Med. 2020, 49, 102294. [Google Scholar] [CrossRef]
- Hao, X.; Li, H.; Li, Q.; Gao, D.; Wang, X.; Wu, C.; Wang, Q.; Zhu, M. Dietary vitamin E intake and risk of Parkinson’s disease: A cross-sectional study. Front. Nutr. 2024, 10, 1289238. [Google Scholar] [CrossRef]
- Guan, J.Z.; Guan, W.P.; Maeda, T. Vitamin E administration erases an enhanced oxidation in multiple sclerosis. Can. J. Physiol. Pharmacol. 2018, 96, 1181–1183. [Google Scholar] [CrossRef]
- Nolan, J.M.; Power, R.; Howard, A.N.; Bergin, P.; Roche, W.; Prado-Cabrero, A.; Pope, G.; Cooke, J.; Power, T.; Mulcahy, R. Supplementation With Carotenoids, Omega-3 Fatty Acids, and Vitamin E Has a Positive Effect on the Symptoms and Progression of Alzheimer’s Disease. J. Alzheimer’s Dis. 2022, 90, 233–249. [Google Scholar] [CrossRef]
- Mangialasche, F.; Kivipelto, M.; Mecocci, P.; Rizzuto, D.; Palmer, K.; Winblad, B. High plasma levels of vitamin E forms and reduced Alzheimer’s disease risk in advanced age. J. Alzheimers Dis. 2010, 20, 1029–1037. [Google Scholar] [CrossRef]
- Yang, F.; Wolk, A.; Håkansson, N.; Pedersen, N.L.; Wirdefeldt, K. Dietary antioxidants and risk of Parkinson’s disease in two population-based cohorts. Mov. Disord. 2017, 32, 1631–1636. [Google Scholar] [CrossRef]
- Xia, K.; Wang, Y.; Zhang, L.; Tang, L.; Zhang, G.; Huang, T.; Huang, N.; Fan, D. Dietary-Derived Essential Nutrients and Amyotrophic Lateral Sclerosis: A Two-Sample Mendelian Randomization Study. Nutrients 2022, 14, 920. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Morel, A.; Saso, L.; Saluk, J. Isoprostanes and neuroprostanes as biomarkers of oxidative stress in neurodegenerative diseases. Oxidative Med. Cell Longev. 2014, 2014, 572491. [Google Scholar] [CrossRef] [PubMed]
- Regner-Nelke, L.; Nelke, C.; Schroeter, C.B.; Dziewas, R.; Warnecke, T.; Ruck, T.; Meuth, S.G. Enjoy Carefully: The Multifaceted Role of Vitamin E in Neuro-Nutrition. Int. J. Mol. Sci. 2021, 22, 10087. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.N.; Whiting, A.; McCaffery, P. Retinoic acid receptor-targeted drugs in neurodegenerative disease. Expert Opin. Drug Metab. Toxicol. 2020, 16, 1097–1108. [Google Scholar] [CrossRef]
- Joshi, P.; Chia, S.; Yang, X.; Perni, M.; Gabriel, J.M.; Gilmer, M.; Limbocker, R.; Habchi, J.; Vendruscolo, M. Combinations of Vitamin A and Vitamin E Metabolites Confer Resilience against Amyloid-β Aggregation. ACS Chem. Neurosci. 2023, 14, 657–666. [Google Scholar] [CrossRef]
- Marie, A.; Darricau, M.; Touyarot, K.; Parr-Brownlie, L.C.; Bosch-Bouju, C. Role and Mechanism of Vitamin A Metabolism in the Pathophysiology of Parkinson’s Disease. J. Park. Dis. 2021, 11, 949–970. [Google Scholar] [CrossRef]
- Fragoso, Y.D.; Stoney, P.N.; McCaffery, P.J. The evidence for a beneficial role of vitamin A in multiple sclerosis. CNS Drugs 2014, 28, 291–299. [Google Scholar] [CrossRef]
- Lane, M.A.; Bailey, S.J. Role of retinoid signaling in the adult brain. Prog. Neurobiol. 2005, 75, 275–293. [Google Scholar] [CrossRef]
- de Oliveira, M.R.; da Rocha, R.F.; Pasquali, M.A.; Moreira, J.C. The effects of vitamin A supplementation for 3 months on adult rat nigrostriatal axis: Increased monoamine oxidase enzyme activity, mitochondrial redox dysfunction, increased β-amyloid(1-40) peptide and TNF-α contents, and susceptibility of mitochondria to an in vitro H2O2 challenge. Brain Res. Bull. 2012, 87, 432–444. [Google Scholar]
- Lionikaite, V.; Gustafsson, K.L.; Westerlund, A.; Windahl, S.H.; Koskela, A.; Tuukkanen, J.; Johansson, H.; Ohlsson, C.; Cona-way, H.H.; Henning, P.; et al. Clinically relevant doses of vitamin A decrease cortical bone mass in mice. J. Endocrinol. 2018, 239, 389–402. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Gluud, C. Antioxidant supplements and mortality. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Diachenko, A.I.; Rodin, I.A.; Krasnova, T.N.; Klychnikov, O.I.; Nefedova, L.N. The Role of Vitamin K in the Development of Neurodegenerative Diseases. Biochemistry 2024, 89, S57–S70. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.; German, M. Vitamin K2 Holds Promise for Alzheimer’s Prevention and Treatment. Nutrients 2021, 13, 2206. [Google Scholar] [CrossRef] [PubMed]
- Denisova, N.A.; Booth, S.L. Vitamin K and sphingolipid metabolism: Evidence to date. Nutrit. Rev. 2005, 63, 111–121. [Google Scholar] [CrossRef]
- Lin, X.; Wen, X.; Wei, Z.; Guo, K.; Shi, F.; Huang, T.; Wang, W.; Zheng, J. Vitamin K2 Protects against A 42-Induced Neurotoxicity by Activating Autophagy and Improving Mitochondrial Function in Drosophila. NeuroReport 2021, 32, 431–437. [Google Scholar] [CrossRef]
- Booth, S.L.; Shea, M.K.; Barger, K.; Leurgans, S.E.; James, B.D.; Holland, T.M.; Agarwal, P.; Fu, X.; Wang, J.; Matuszek, G.; et al. Association of Vitamin K with cognitive decline and neuropathology in community-dwelling older persons. Alzheimer’s Dement. 2022, 8, e12255. [Google Scholar] [CrossRef]
- Alam, P.; Chaturvedi, S.K.; Siddiqi, M.K.; Rajpoot, R.K.; Ajmal, M.R.; Zaman, M.; Khan, R.H. Vitamin K3 inhibits protein aggregation: Implication in the treatment of amyloid diseases. Sci. Rep. 2016, 6, 26759. [Google Scholar] [CrossRef]
- Vos, M.; Esposito, G.; Edirisinghe, J.N.; Vilain, S.; Haddad, D.M.; Slabbaert, J.R.; Van Meensel, S.; Schaap, O.; De Strooper, B.; Meganathan, R.; et al. Vitamin K2 is a mitochondrial electron carrier that rescues pink1 deficiency. Science 2012, 8, 1306–1310. [Google Scholar] [CrossRef]
- Yu, Y.X.; Yu, X.D.; Cheng, Q.Z.; Tang, L.; Shen, M.Q. The association of serum vitamin K2 levels with Parkinson’s disease: From basic case-control study to big data mining analysis. Aging 2020, 12, 16410–16419. [Google Scholar] [CrossRef]
- Moriya, M.; Nakatsuji, Y.; Okuno, T.; Hamasaki, T.; Sawada, M.; Sakoda, S. Vitamin K2 ameliorates experimental autoimmune encephalomyelitis in Lewis rats. J. Neuroimmunol. 2005, 170, 11–20. [Google Scholar] [CrossRef]
- De Oliveira, L.G.; Angelo, Y.D.S.; Iglesias, A.H.; Peron, J.P.S. Unraveling the Link between Mitochondrial Dynamics and Neuroinflammation. Front. Immunol. 2021, 12, 624919. [Google Scholar] [CrossRef] [PubMed]
- Lasemi, R.; Kundi, M.; Moghadam, N.B.; Moshammer, H.; Hainfellner, J.A. Vitamin K2 in Multiple Sclerosis Patients. Wien. Klin. Wochenschr. 2018, 130, 307–313. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on foods. Off. J. Eur. Union 2006, 404, 9–25. [Google Scholar]
- Duttaroy, A.K. Chapter 19—Regulation of functional foods in European Union: Assessment of health claim by the European Food Safety Authority. In Nutraceutical and Functional Food Regulations in the United States and Around the World, 3rd ed.; Bagchi, D., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 267–276. ISBN 9780128164679. [Google Scholar]
- Available online: https://food.ec.europa.eu/food-safety/labelling-and-nutrition/nutrition-and-health-claims/eu-register-health-claims_en (accessed on 27 November 2024).
- Piemontese, L.; Brunetti, L.; Leuci, R. Can foods influence the onset and progress of neurodegenerative diseases? Neural Regen. Res. 2022, 17, 2443–2444. [Google Scholar] [CrossRef] [PubMed]
- Wolak, N.; Zawrotniak, M.; Gogol, M.; Kozik, A.; Rapala-Kozik, M. Vitamins B1, B2, B3 and B9-Occurrence, Biosynthesis Pathways and Functions in Human Nutrition. Mini Rev. Med. Chem. 2017, 17, 1075–1111. [Google Scholar] [CrossRef]
- Hrubša, M.; Siatka, T.; Nejmanová, I.; Vopršalová, M.; Kujovská Krčmová, L.; Matoušová, K.; Javorská, L.; Macáková, K.; Mercolini, L.; Remião, F.; et al. Biological Properties of Vitamins of the B-Complex, Part 1: Vitamins B1, B2, B3, and B5. Nutrients 2022, 14, 484. [Google Scholar] [CrossRef]
- Benedik, E. Sources of vitamin D for humans. Int. J. Vitam. Nutr. Res. 2022, 92, 118–125. [Google Scholar] [CrossRef]
- Watanabe, F.; Bito, T. Vitamin B12 sources and microbial interaction. Exp. Biol. Med. 2018, 243, 148–158. [Google Scholar] [CrossRef]
- Zaaboul, F.; Liu, Y. Vitamin E in foodstuff: Nutritional, analytical, and food technology aspects. Compr. Rev. Food Sci. Food Saf. 2022, 21, 964–998. [Google Scholar] [CrossRef]
- Regulska-Ilow, B.; Różańska, D.; Zatońska, K.; Szuba, A. Estimation of Vitamin K Content and Its Sources in the Diet of the Polish Participants of the PURE Study. Nutrients 2022, 14, 1917. [Google Scholar] [CrossRef]
- Zeng, J.; Chen, L.; Wang, Z.; Chen, Q.; Fan, Z.; Jiang, H.; Wu, Y.; Ren, L.; Chen, J.; Li, T.; et al. Marginal vitamin A deficiency facilitates Alzheimer’s pathogenesis. Acta Neuropathol. 2017, 133, 967–982. [Google Scholar] [CrossRef] [PubMed]
- Létondor, A.; Buaud, B.; Vaysse, C.; Richard, E.; Layé, S.; Pallet, V.; Alfos, S. EPA/DHA and vitamin A supplementation improves spatial memory and alleviates the age-related decrease in hippocampal RXRγ and kinase expression in rats. Front. Aging Neurosci. 2016, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Hu, J.; Huo, X.; Miao, R.; Zhang, Y.; Ma, F. Effects of vitamin D supplementation on cognitive function and blood Aβ-related biomarkers in older adults with Alzheimer’s disease: A randomised, double-blind, placebo-controlled trial. J. Neurol. Neurosurg. Psychiatry 2019, 90, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Latimer, C.S.; Brewer, L.D.; Searcy, J.L.; Chen, K.-C.; Popovi’c, J.; Kraner, S.D.; Thibault, O.; Blalock, E.M.; Landfield, P.W.; Porter, N.M. Vitamin D prevents cognitive decline and enhances hippocampal synaptic function in aging rats. Proc. Natl. Acad. Sci. USA 2014, 111, E4359–E4366. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, M.; Li, C.; Jiang, X.; Su, Y.; Zhang, Y. Benefits of Vitamins in the Treatment of Parkinson’s Disease. Oxidative Med. Cell Longev. 2019, 2019, 9426867. [Google Scholar] [CrossRef]
- Paganini-Hill, A.; Bukhari, S.; Montine, T.J.; Corrada, M.M.; Kawas, C.H. Alzheimer’s Disease Neuropathologic Change and Vitamin Supplement Use Decades Earlier: The 90+ Study. Alzheimer Dis. Assoc. Disord. 2023, 37, 1–6. [Google Scholar] [CrossRef]
- Gong, X.; Shi, L.; Wu, Y.; Luo, Y.; Kwok, T. B Vitamin Supplementation Slows Cognitive Decline in Mild Cognitive Impairment Patients with Frontal Lobe Atrophy. J. Alzheimer’s Dis. 2022, 89, 1453–1461. [Google Scholar] [CrossRef]
- Douaud, G.; Refsum, H.; de Jager, C.A.; Jacoby, R.; Nichols, T.E.; Smith, S.M.; Smith, A.D. Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc. Natl. Acad. Sci. USA 2013, 110, 9523–9528. [Google Scholar] [CrossRef]
- Kontush, A.; Mann, U.; Arlt, S.; Ujeyl, A.; Lührs, C.; Müller-Thomsen, T.; Beisiegel, U. Influence of vitamin E and C supplementation on lipoprotein oxidation in patients with Alzheimer’s disease. Free Radic. Biol. Med. 2001, 31, 345–354. [Google Scholar] [CrossRef]
- Arlt, S.; Müller-Thomsen, T.; Beisiegel, U.; Kontush, A. Effect of one-year vitamin C-and E-supplementation on cerebrospinalfluid oxidation parameters and clinical course in Alzheimer’s disease. Neurochem. Res. 2012, 37, 2706–2714. [Google Scholar] [CrossRef]
- Crivello, N.A.; Casseus, S.L.; Peterson, J.W.; Smith, D.E.; Booth, S.L. Age-and brain region-specific effects of dietary vitamin K on myelin sulfatides. J. Nutr. Biochem. 2010, 21, 1083–1088. [Google Scholar] [CrossRef]
| Vitamin | Claim | Health Relationship |
|---|---|---|
| Vitamin B2 | Contributes to normal functioning of the nervous system | Maintenance of the normal function of the nervous system |
| Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage | |
| Contributes to the reduction of tiredness and fatigue | Reduction of tiredness and fatigue | |
| Vitamin B12 | Contributes to normal functioning of the nervous system | Contribution to neurological and psychological function |
| Contributes to normal homocysteine metabolism | Contribution to normal homocysteine metabolism | |
| Contributes to normal psychological function | Contribution to neurological and psychological function | |
| Vitamin B6 | Contributes to normal homocysteine metabolism | Contribution to normal homocysteine metabolism |
| Contributes to normal psychological function | Contribution to normal psychological functions | |
| Contributes to normal functioning of the nervous system | Function of the nervous system | |
| Vitamin D | Contributes to the normal function of the immune system | Normal function of the immune system and inflammation response |
| Vitamin E | Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage |
| Vitamin C | Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage |
| Contributes to normal functioning of the nervous system | Function of the nervous system | |
| Contributes to normal psychological function | Contribution to normal psychological functions |
| Vitamin | Claim | Health Relationship |
|---|---|---|
| Vitamin B2 | Contributes to normal energy-yielding metabolism | Contribution to normal energy-yielding metabolism |
| Contributes to normal functioning of the nervous system | Maintenance of the normal function of the nervous system | |
| Contributes to the maintenance of normal mucous membranes | Maintenance of normal skin and mucous membranes | |
| Contributes to the maintenance of normal red blood cells | Maintenance of normal red blood cells | |
| Contributes to the maintenance of normal skin | Maintenance of normal skin and mucous membranes | |
| Contributes to the maintenance of normal vision | Maintenance of normal vision | |
| Contributes to the normal metabolism of iron | Contribution to normal metabolism of iron | |
| Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage | |
| Contributes to the reduction of tiredness and fatigue | Reduction of tiredness and fatigue | |
| Vitamin B12 | Contributes to normal energy-yielding metabolism | Energy-yielding metabolism |
| Contributes to normal functioning of the nervous system | Contribution to neurological and psychological function | |
| Contributes to normal homocysteine metabolism | Contribution to normal homocysteine metabolism | |
| Contributes to normal psychological function | Contribution to neurological and psychological function | |
| Contributes to normal red blood cell formation | Red blood cell formation | |
| Contributes to the normal function of the immune system | Function of the immune system | |
| Contributes to the reduction of tiredness and fatigue | Reduction of tiredness and fatigue | |
| Has a role in the process of cell division | Cell division | |
| Vitamin B6 | Contributes to normal homocysteine metabolism | Contribution to normal homocysteine metabolism |
| Contributes to normal protein and glycogen metabolism | Protein and glycogen metabolism | |
| Contributes to normal psychological function | Contribution to normal psychological functions | |
| Contributes to normal red blood cell formation | Red blood cell formation | |
| Contributes to the normal function of the immune system | Function of the immune system | |
| Contributes to the reduction of tiredness and fatigue | Reduction of tiredness and fatigue | |
| Contributes to the regulation of hormonal activity | Regulation of hormonal activity | |
| Contributes to normal cysteine synthesis | Contribution to normal cysteine synthesis | |
| Contributes to normal energy-yielding metabolism | Contribution to normal energy-yielding metabolism | |
| Contributes to normal functioning of the nervous system | Function of the nervous system | |
| Calcium and Vitamin D | Needed for normal growth and development of bone in children | -/- |
| Help to reduce loss of bone mineral in post-menopausal women | -/- | |
| Vitamin D | Needed for normal growth and development of bone in children | -/- |
| Helps reduce the risk of falling associated with postural instability and muscle weakness | -/- | |
| Contributes to normal absorption/utilization of calcium and phosphorus | Absorption and utilization of calcium and phosphorus, maintenance of blood calcium levels | |
| Contributes to normal blood calcium levels | Absorption and utilization of calcium and phosphorus, maintenance of blood calcium levels | |
| Contributes to the maintenance of normal bones | Maintenance of bones and teeth | |
| Contributes to the maintenance of normal muscle function | Normal muscle function | |
| Contributes to the maintenance of normal teeth | Maintenance of bones and teeth | |
| Contributes to the normal function of the immune system | Normal function of immune system and inflammation response | |
| Has a role in the process of cell division | Cell division | |
| Contributes to the normal function of the immune system in children | -/- | |
| Vitamin E | Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage |
| Vitamin A | Contributes to normal iron metabolism | -/- |
| Contributes to the maintenance of normal mucous membranes | Maintenance of normal skin and mucous membranes | |
| Contributes to the maintenance of normal skin | Maintenance of normal skin and mucous membranes | |
| Contributes to the maintenance of normal vision | Maintenance of normal vision | |
| Contributes to the normal function of the immune system | Maintenance of the normal function of the immune system | |
| Has a role in the process of cell specialization | Cell differentiation | |
| Vitamin K | Contributes to normal blood clotting | Blood coagulation |
| Contributes to the maintenance of normal bones | Maintenance of bones | |
| Vitamin C | Contributes to maintain the normal function of the immune system during and after intense physical exercise | Function of the immune system during and after extreme physical exercise |
| Contributes to normal collagen formation for the normal function of blood vessels | Collagen formation | |
| Contributes to normal collagen formation for the normal function of bones | Collagen formation | |
| Contributes to normal collagen formation for the normal function of cartilage | Collagen formation | |
| Contributes to normal collagen formation for the normal function of gums | Collagen formation | |
| Contributes to normal collagen formation for the normal function of skin | Collagen formation | |
| Contributes to normal collagen formation for the normal function of teeth | Collagen formation | |
| Contributes to normal energy-yielding metabolism | Contribution to normal energy-yielding metabolism | |
| Contributes to normal functioning of the nervous system | Function of the nervous system | |
| Contributes to normal psychological function | Contribution to normal psychological functions | |
| Contributes to the normal function of the immune system | Maintenance of the normal function of the immune system | |
| Contributes to the protection of cells from oxidative stress | Protection of DNA, proteins, and lipids from oxidative damage | |
| Contributes to the reduction of tiredness and fatigue | Reduction of tiredness and fatigue | |
| Contributes to the regeneration of the reduced form of vitamin E | Regeneration of the reduced form of vitamin E | |
| Increases iron absorption | Non-haem iron absorption |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orywal, K.; Socha, K.; Iwaniuk, P.; Kaczyński, P.; Farhan, J.A.; Zoń, W.; Łozowicka, B.; Perkowski, M.; Mroczko, B. Vitamins in the Prevention and Support Therapy of Neurodegenerative Diseases. Int. J. Mol. Sci. 2025, 26, 1333. https://doi.org/10.3390/ijms26031333
Orywal K, Socha K, Iwaniuk P, Kaczyński P, Farhan JA, Zoń W, Łozowicka B, Perkowski M, Mroczko B. Vitamins in the Prevention and Support Therapy of Neurodegenerative Diseases. International Journal of Molecular Sciences. 2025; 26(3):1333. https://doi.org/10.3390/ijms26031333
Chicago/Turabian StyleOrywal, Karolina, Katarzyna Socha, Piotr Iwaniuk, Piotr Kaczyński, Jakub Ali Farhan, Wojciech Zoń, Bożena Łozowicka, Maciej Perkowski, and Barbara Mroczko. 2025. "Vitamins in the Prevention and Support Therapy of Neurodegenerative Diseases" International Journal of Molecular Sciences 26, no. 3: 1333. https://doi.org/10.3390/ijms26031333
APA StyleOrywal, K., Socha, K., Iwaniuk, P., Kaczyński, P., Farhan, J. A., Zoń, W., Łozowicka, B., Perkowski, M., & Mroczko, B. (2025). Vitamins in the Prevention and Support Therapy of Neurodegenerative Diseases. International Journal of Molecular Sciences, 26(3), 1333. https://doi.org/10.3390/ijms26031333