
Comparative Evaluation of ARB Monotherapy and SGLT2/ACE Inhibitor Combination Therapy in the Renal Function of Diabetes Mellitus Patients: A Retrospective, Longitudinal Cohort Study

 ,
, 
Abstract
1. Introduction
2. Results
2.1. Physiological and Biochemical Markers: One-Sample t-Test
2.2. Physiological and Biochemical Markers: Analysis of Variance (ANOVA)
3. Discussion
3.1. Study Limitations
3.2. Future Implications and Perspectives
4. Methods
4.1. Study Design and Patient Selection
4.2. Clinical Parameters and Laboratory Measures
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEi | angiotensin-converting enzyme inhibitors |
| ACR | albumin-to-creatinine ratio |
| ADA | American Diabetes Association |
| ANOVA | Analysis of variance |
| ARBs | angiotensin receptor blockers |
| BP | blood pressure |
| CKD | chronic kidney disease |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| CVD | cardiovascular disease |
| DAPA-CKD | Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease |
| DBP | diastolic blood pressure |
| DKA | diabetic ketoacidosis |
| DM | diabetes mellitus |
| DN | diabetic nephropathy |
| eGFR | estimated glomerular filtration rate |
| EMPA-REG OUTCOME | Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes |
| ESRD | end-stage renal disease |
| HbA1c | hemoglobin A1c |
| IQR | interquartile range |
| JNC | Joint National Committee |
| K+ | potassium |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| KDOQI | National Kidney Foundation Kidney Disease Outcomes Quality Initiative |
| MAP | mean arterial pressure |
| MAU | microalbuminuria |
| MS | mean squares |
| NKF | National Kidney Foundation |
| NHBPEP | National High Blood Pressure Education Program |
| ONTARGET | Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial |
| RAAS | renin–angiotensin–aldosterone system |
| RAASi | renin–angiotensin–aldosterone system inhibitors |
| Rx | prescription/treatment |
| SBP | systolic blood pressure |
| sCr | serum creatinine |
| SD | standard deviation |
| SGLT2i | sodium-glucose cotransporter-2 inhibitors |
| SGLT2i/ACEi | sodium-glucose cotransporter-2 inhibitor/angiotensin-converting enzyme inhibitor |
| SS | sum of squares |
| T1DM | type 1 diabetes mellitus |
| T2DM | type 2 diabetes mellitus |
| UAE | urinary albumin excretion |
| UTIs | urinary tract infections |
References
- Zimbudzi, E.; Lo, C.; Ranasinha, S.; Gallagher, M.; Fulcher, G.; Kerr, P.G.; Russell, G.; Teed, H.; Usherwood, T.; Walker, R.; et al. Predictors of Health-Related Quality of Life in Patients with Co-Morbid Diabetes and Chronic Kidney Disease. PLoS ONE 2016, 11, e0168491. [Google Scholar] [CrossRef] [PubMed]
- Burrows, N.R.; Hora, I.; Geiss, L.S.; Gregg, E.W.; Albright, A. Incidence of End-Stage Renal Disease Attributed to Diabetes among Persons with Diagnosed Diabetes—United States and Puerto Rico, 2000–2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1165–1170. [Google Scholar] [CrossRef]
- Alsalemi, N.; Sadowski, C.A.; Elftouh, N.; Louis, M.; Kilpatrick, K.; Houle, S.K.D.; Lafrance, J.P. The Effect of Renin–Angiotensin–Aldosterone System Inhibitors on Continuous and Binary Kidney Outcomes in Subgroups of Patients with Diabetes: A Meta-Analysis of Randomized Clinical Trials. BMC Nephrol. 2022, 23, 161. [Google Scholar] [CrossRef] [PubMed]
- Sawaf, H.; Thomas, G.; Taliercio, J.J.; Nakhoul, G.; Vachharajani, T.J.; Mehdi, A. Therapeutic Advances in Diabetic Nephropathy. J. Clin. Med. 2022, 11, 378. [Google Scholar] [CrossRef]
- Selby, N.M.; Taal, M.W. An Updated Overview of Diabetic Nephropathy: Diagnosis, Prognosis, Treatment Goals and Latest Guidelines. Diabetes Obes. Metab. 2020, 22, 3–15. [Google Scholar] [CrossRef]
- Vivian, E.; Mannebach, C. Therapeutic approaches to slowing the progression of diabetic nephropathy—Is less best? Drugs Context 2013, 212249. [Google Scholar] [CrossRef]
- Bailey, J. ACE inhibitors vs. ARBs for patients with diabetic kidney disease. Am. Fam. Physician 2007, 76, 68–69. [Google Scholar]
- Pathak, J.V.; Dass, E.E. A retrospective study of the effects of angiotensin receptor blockers and angiotensin converting enzyme inhibitors in diabetic nephropathy. Indian J. Pharmacol. 2015, 47, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Heerspink, H.J.L.; Sang, Y.; Matsushita, K.; Arnlov, J.; Astor, B.C.; Black, C.; Brunskill, N.J.; Carrero, J.J.; Feldman, H.I.; et al. Change in Albuminuria and Subsequent Risk of End-Stage Kidney Disease: An Individual Participant-Level Consortium Meta-Analysis of Observational Studies. Lancet Diabetes Endocrinol. 2019, 7, 115–127. [Google Scholar] [CrossRef]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). Hypertension 2014, 63, e136–e138. [Google Scholar] [CrossRef]
- Lee, C.J.; Kim, J.H.; Lee, E.K.; Jung, H.Y.; Ryu, D.R.; Lee, D.W.; Han, S.H.; Oh, D.J. Comparative efficacy of ACE inhibitors versus ARBs on renal outcomes in patients with diabetic kidney disease: A systematic review and meta-analysis. J. Clin. Hypertens. 2023, 25, 401–410. [Google Scholar] [CrossRef]
- Rodríguez-Morales, J.; Singh, A.K.; Khunti, K.; Kumar, A.; Verma, A.; Alvarado, M.M.; Bhatia, S. Long-term impact of RAAS blockade on diabetic nephropathy: Updated evidence from clinical trials. Diabetes Res. Clin. Pract. 2022, 188, 109941. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefansson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Green, T.; Hou, F.F.; Mann, J.F.E. Dapagliflozin in Patients with Chronic Kidney Disease. N. Eng. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.J.; Deedwania, P.; Acharya, T.; Aguilar, D.; Bhatt, D.L.; Chyun, D.A.; Di Palo, K.E.; Golden, S.H.; Sperling, L.S. Comprehensive Management of Cardiovascular Risk Factors for Adults with Type 2 Diabetes: A Scientific Statement from the American Heart Association. Circulation 2022, 145, e722–e759. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Winocour, P.; Chowdhury, T.A.; De, P.; Wahba, M.; Montero, R.; Fogarty, D.; Frankel, A.H.; Karalliedde, J.; Mark, P.B.; et al. Management of hypertension and renin-angiotensin-aldosterone system blockade in adults with diabetic kidney disease: Association of British Clinical Diabetologists and the Renal Association UK guideline update 2021. BMC Nephrol. 2022, 23, 9. [Google Scholar] [CrossRef]
- Jun, H.R.; Shin, Y.J.; Kim, S.J.; Cho, J.Y.; Kwon, H.Y. Onset of Hyperkalemia following the Administration of Angiotensin-Converting Enzyme Inhibitor or Angiotensin II Receptor Blocker. Cardiovasc. Ther. 2021, 2021, 5935149. [Google Scholar] [CrossRef]
- National High Blood Pressure Education Program. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7); NIH Publication No. 04-5230; U.S. Department of Health and Human Services; National Institutes of Health, National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 2004; p. 11. Available online: https://www.nhlbi.nih.gov/files/docs/guidelines/jnc7full.pdf (accessed on 4 December 2024).
- DiaTribe. Diabetes and High Potassium Levels. Available online: https://diatribe.org/diabetes-management/diabetes-and-high-potassium-levels (accessed on 9 December 2024).
- Eyth, E.; Naik, R. Hemoglobin A1C. In StatPearls; updated 13 March 2023; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK549816/ (accessed on 29 November 2024).
- Gounden, V.; Bhatt, H.; Jialal, I. Renal Function Tests. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507821/ (accessed on 5 December 2024).
- Asmamaw, T.; Genet, S.; Menon, M.; Tarekegn, G.; Chekol, E.; Geto, Z.; Lejisa, T.; Habtu, W.; Getahun, T.; Tolcha, Y. Early Detection of Renal Impairment Among Patients with Type 2 Diabetes Mellitus Through Evaluation of Serum Cystatin C in Comparison with Serum Creatinine Levels: A Cross-Sectional Study. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 4727–4735. [Google Scholar] [CrossRef]
- National Kidney Foundation. Kidney Failure Risk Factor: Urine Albumin-Creatinine Ratio (uACR). Available online: https://www.kidney.org/kidney-failure-risk-factor-urine-albumin-creatinine-ratio-uacr (accessed on 9 December 2024).
- Haider, M.Z.; Aslam, A. Proteinuria. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564390/ (accessed on 9 December 2024).
- Vaidya, S.R.; Narothama, R.A. Chronic Kidney Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024; Available online: https://www.statpearls.com/point-of-care/28357 (accessed on 9 December 2024).
- Bhandari, S.; Mehta, S.; Khwaja, A.; Cleland, J.G.F.; Ives, N.; Brettell, E.; Chadburn, M.; Cockwell, P.; STOP ACEi Trial Investigators. Renin-Angiotensin System Inhibition in Advanced Chronic Kidney Disease. N. Eng. J. Med. 2022, 387, 2021–2032. [Google Scholar] [CrossRef]
- Onuigbo, M.A.C.; Agbasi, N. Diabetic Nephropathy and CKD-Analysis of Individual Patient Serum Creatinine Trajectories: A Forgotten Diagnostic Methodology for Diabetic CKD Prognostication and Prediction. J. Clin. Med. 2015, 4, 1348–1368. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am. J. Kidney Dis. 2002, 39 (Suppl. S1), S1–S266. [Google Scholar]
- Vallon, V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu. Rev. Med. 2015, 66, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Eng. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Vejakama, P.; Thakkinstian, A.; Lertrattananon, D.; Ingsathit, A.; Ngarmukos, C.; Attia, J. Reno-protective effects of renin-angiotensin system blockade in type 2 diabetic patients: A systematic review and network meta-analysis. Diabetologia 2024, 47, 15–23. [Google Scholar] [CrossRef]
- Ontarget Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N. Engl. J. Med. 2008, 358, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. Stages of Chronic Kidney Disease (CKD). Available online: https://www.kidney.org/kidney-topics/stages-chronic-kidney-disease-ckd (accessed on 9 December 2024).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic(s) | Totals | Active ARB Rx | SGLT2i/ACEi Rx |
|---|---|---|---|
| n = 126 | 74 | 52 | |
| Age | |||
| Mean (years) | 61.8 ± 11.0 | 62.1 ± 10.16 | 61.5 ± 12.11 |
| Sex | |||
| Female | 54 | 29 | 25 |
| Male | 72 | 45 | 27 |
| Insulin status | |||
| Insulin-dependent | 20 | 12 | 8 |
| Non-insulin dependent | 106 | 62 | 44 |
| Race/Ethnicity | |||
| Black, non-Hispanic | 47 | 33 | 14 |
| Hispanic | 37 | 19 | 18 |
| Asian | 29 | 16 | 13 |
| White | 13 | 6 | 7 |
| Chronic kidney disease (CKD) stage | |||
| No CKD/CKD1 | 52 | 32 | 20 |
| CKD2 | 38 | 23 | 15 |
| CKD3a/3b | 32 | 16 | 16 |
| CKD4 | 4 | 3 | 1 |
| CKD5 | 0 | 0 | 0 |
| Predictor | df | SS/MS * | F-Value | p-Value |
|---|---|---|---|---|
| HbA1c | 1 | 1224 | 5.276 | 0.0236 |
| Potassium | 1 | 2783 | 12.037 | 0.0008 |
| Creatinine | 1 | 31,800 | 137.540 | <2.0 × 10−16 |
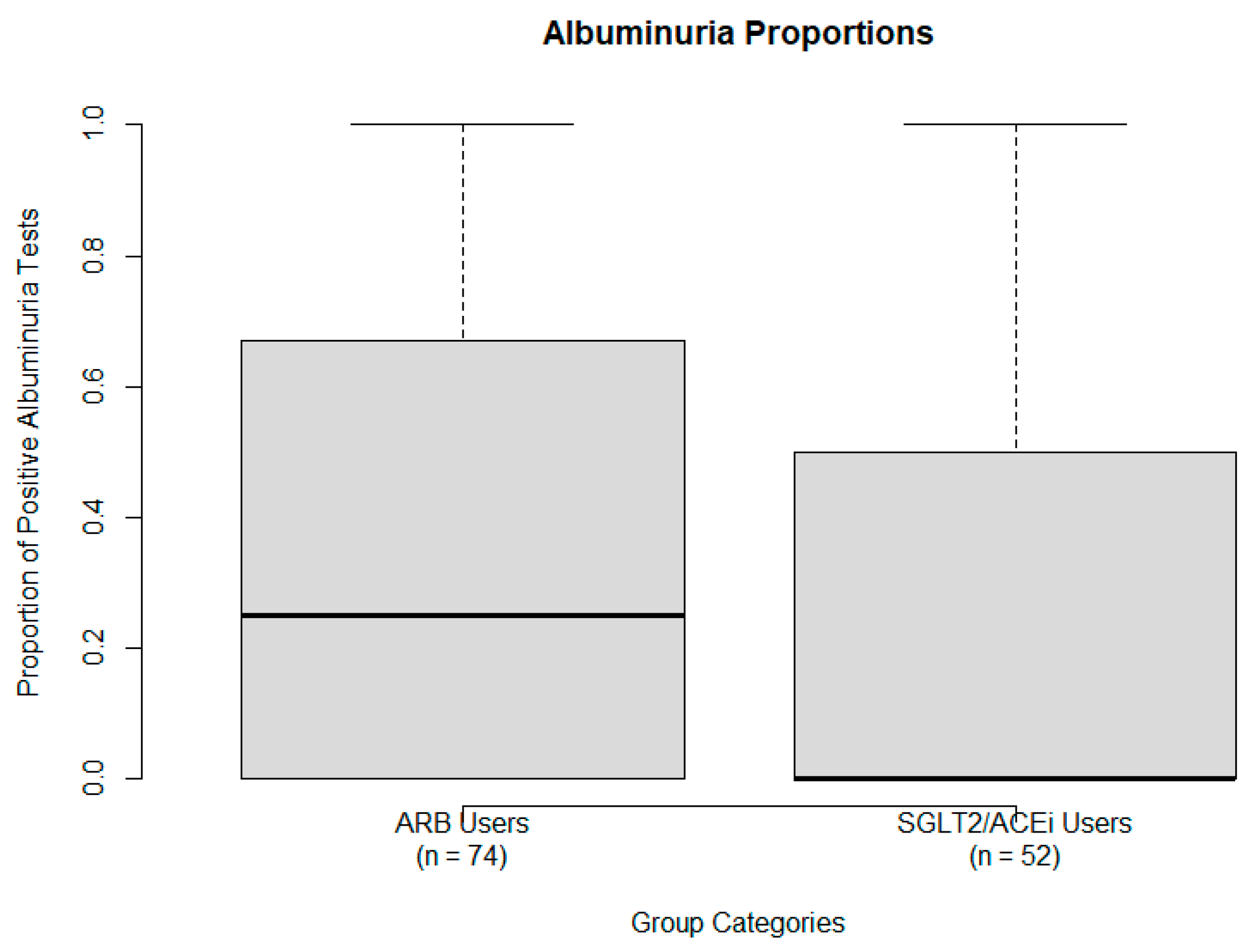
| Albuminuria | 1 | 301 | 1.301 | 0.2569 |
| Residuals | 95 | 21,964 |
| Predictor | df | SS/MS * | F-Value | p-Value |
|---|---|---|---|---|
| HbA1c | 1 | 610 | 2.706 | 0.1045 |
| Potassium | 1 | 1956 | 8.676 | 0.0044 |
| Creatinine | 1 | 23,813 | 105.629 | 1.49 × 10−15 |
| Albuminuria | 1 | 108 | 0.479 | 0.4912 |
| Residuals | 69 | 15,555 |
| Predictor | df | SS/MS * | F-Value | p-Value |
|---|---|---|---|---|
| HbA1c | 1 | 1915 | 13.895 | 0.0005 |
| Potassium | 1 | 558 | 4.045 | 0.0500 |
| Creatinine | 1 | 20,563 | 149.186 | 3.44 × 10−16 |
| Albuminuria | 1 | 941 | 6.830 | 0.0120 |
| Residuals | 47 | 6478 |
| Marker | Mean ± SD | t-Statistic | p-Value | Effect Size (d) | |
|---|---|---|---|---|---|
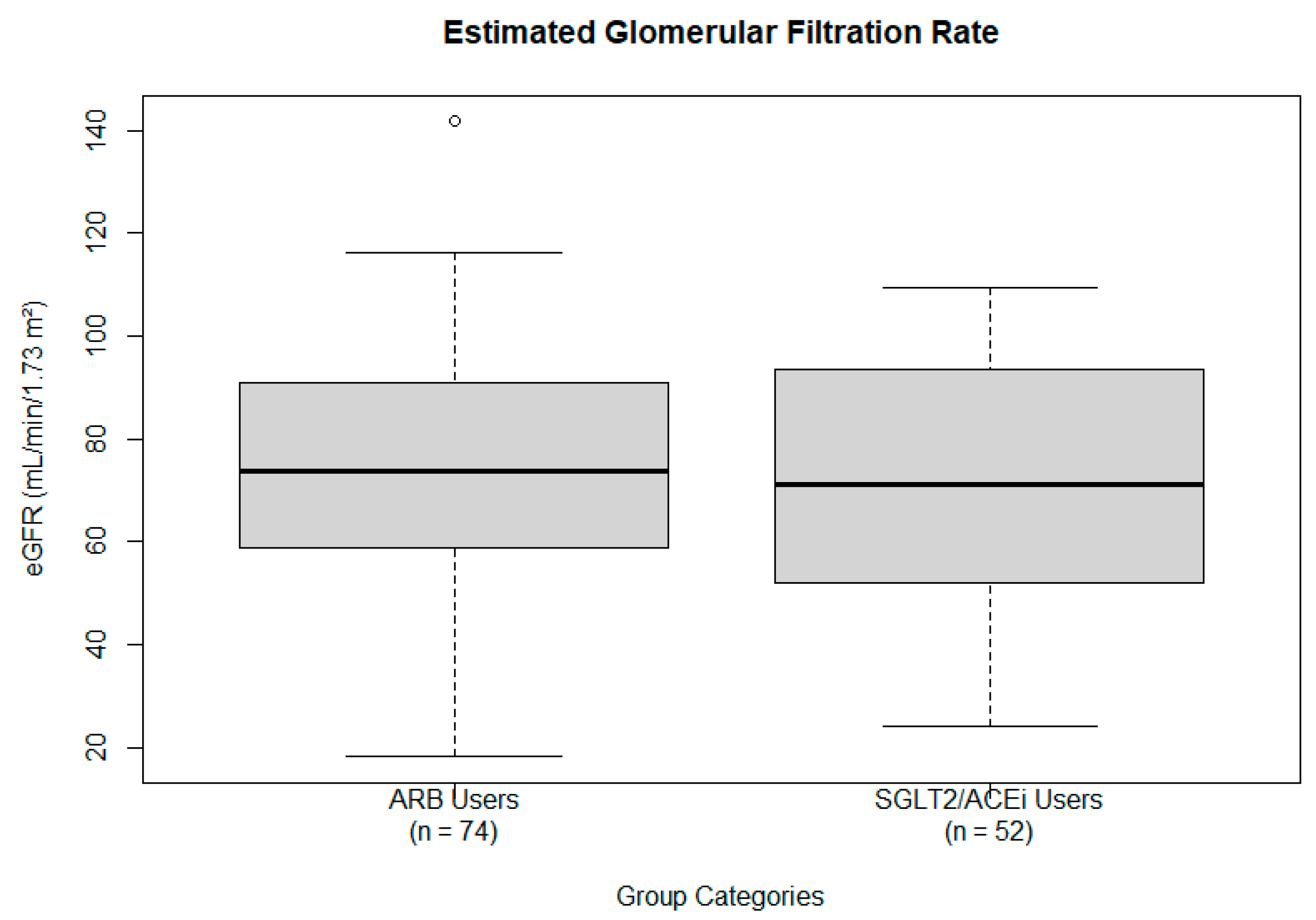
| eGFR (mL/min/1.73 m2) | Overall | 73.37 ± 24.22 | −14.09 | 2.14 × 10−25 | −1.41 |
| ARB Users | 73.57 ± 24.00 | −12.16 | 3.15 × 10−19 | −1.41 | |
| SGLT2/ACEi Users | 71.74 ± 24.44 | −10.55 | 2.00 × 10−14 | −1.46 | |
| HbA1c (%) | Overall | 7.23 ± 1.54 | 4.74 | 7.11 × 10−6 | 0.47 |
| ARB Users | 7.36 ± 1.68 | 4.40 | 3.58 × 10−5 | 0.51 | |
| SGLT2/ACEi Users | 7.02 ± 0.92 | 4.08 | 1.60 × 10−4 | 0.57 | |
| Potassium (mEq/L) | Overall | 4.31 ± 0.33 | 3.37 | 1.07 × 10−3 | 0.33 |
| ARB Users | 4.27 ± 0.33 | 1.83 | 7.11 × 10−2 | 0.21 | |
| SGLT2/ACEi Users | 4.38 ± 0.30 | 4.36 | 6.30 × 10−5 | 0.60 | |
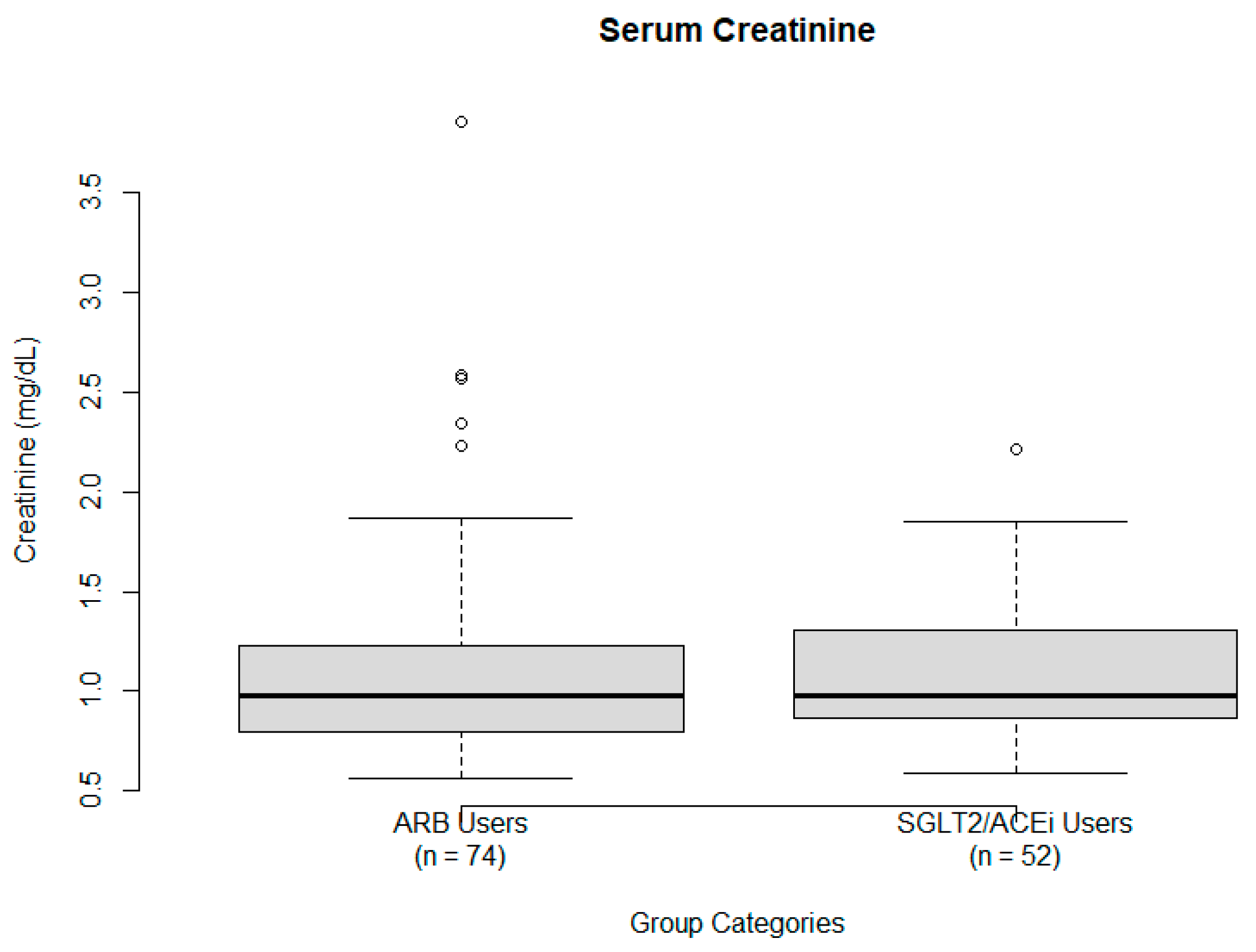
| Creatinine (mg/dL) | Overall | 1.10 ± 0.48 | 4.77 | 6.38 × 10−6 | 0.48 |
| ARB Users | 1.12 ± 0.53 | 4.00 | 1.48 × 10−4 | 0.47 | |
| SGLT2/ACEi Users | 1.10 ± 0.36 | 4.56 | 3.24 × 10−5 | 0.64 | |
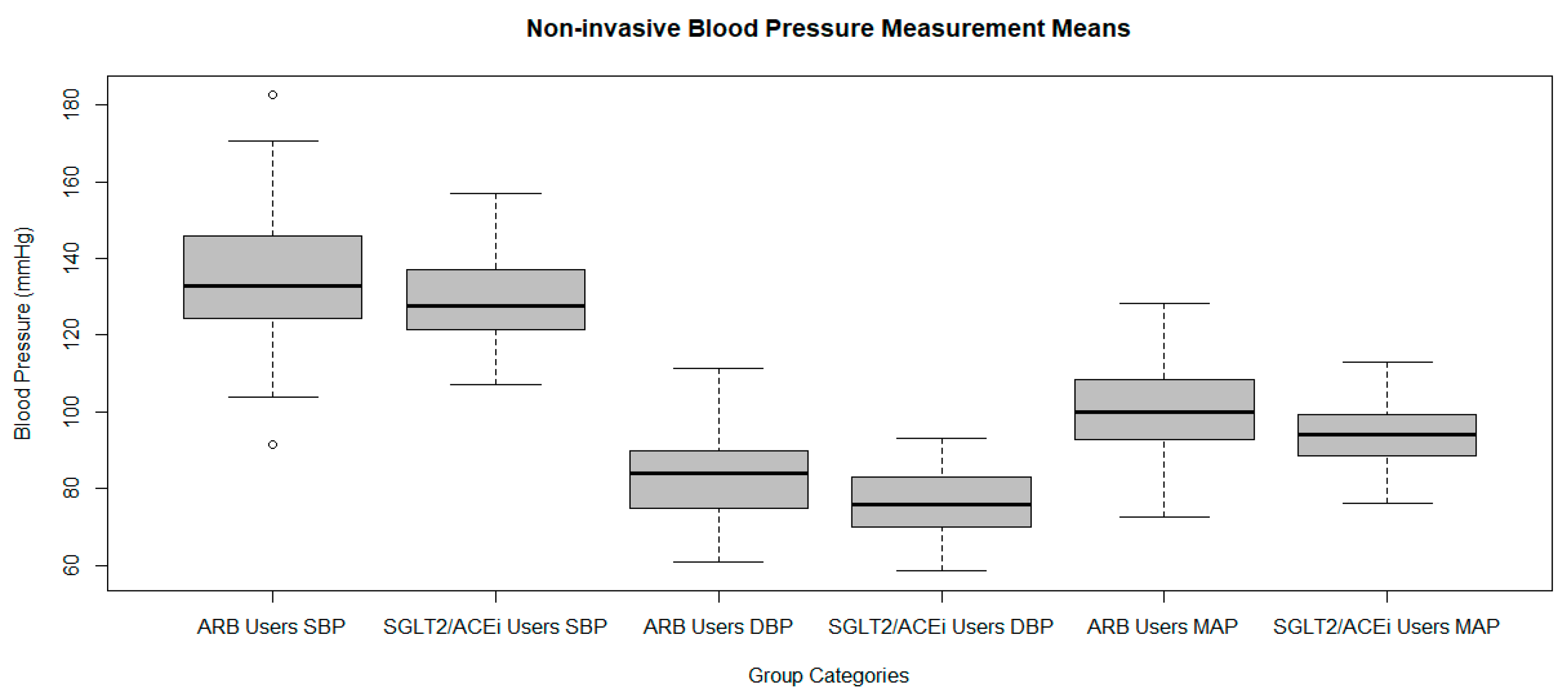
| Systolic Blood Pressure (mmHg) | Overall | 133.1 ± 16.2 | 8.09 | 1.52 × 10−12 | 0.81 |
| ARB Users | 135.1 ± 17.2 | 7.59 | 8.15 × 10−11 | 0.88 | |
| SGLT2/ACEi Users | 129.1 ± 12.8 | 5.16 | 4.02 × 10−6 | 0.71 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngai, A.W.; Baig, A.; Zia, M.; Arca-Contreras, K.; Haque, N.U.; Livetsky, V.; Rokicki, M.; Sukhram, S.D. Comparative Evaluation of ARB Monotherapy and SGLT2/ACE Inhibitor Combination Therapy in the Renal Function of Diabetes Mellitus Patients: A Retrospective, Longitudinal Cohort Study. Int. J. Mol. Sci. 2025, 26, 7412. https://doi.org/10.3390/ijms26157412
Ngai AW, Baig A, Zia M, Arca-Contreras K, Haque NU, Livetsky V, Rokicki M, Sukhram SD. Comparative Evaluation of ARB Monotherapy and SGLT2/ACE Inhibitor Combination Therapy in the Renal Function of Diabetes Mellitus Patients: A Retrospective, Longitudinal Cohort Study. International Journal of Molecular Sciences. 2025; 26(15):7412. https://doi.org/10.3390/ijms26157412
Chicago/Turabian StyleNgai, Andrew W., Aqsa Baig, Muhammad Zia, Karen Arca-Contreras, Nadeem Ul Haque, Veronica Livetsky, Marcelina Rokicki, and Shiryn D. Sukhram. 2025. "Comparative Evaluation of ARB Monotherapy and SGLT2/ACE Inhibitor Combination Therapy in the Renal Function of Diabetes Mellitus Patients: A Retrospective, Longitudinal Cohort Study" International Journal of Molecular Sciences 26, no. 15: 7412. https://doi.org/10.3390/ijms26157412
APA StyleNgai, A. W., Baig, A., Zia, M., Arca-Contreras, K., Haque, N. U., Livetsky, V., Rokicki, M., & Sukhram, S. D. (2025). Comparative Evaluation of ARB Monotherapy and SGLT2/ACE Inhibitor Combination Therapy in the Renal Function of Diabetes Mellitus Patients: A Retrospective, Longitudinal Cohort Study. International Journal of Molecular Sciences, 26(15), 7412. https://doi.org/10.3390/ijms26157412