
SGLT2 Inhibitors in Cancer Patients: A Comprehensive Review of Clinical, Biochemical, and Therapeutic Implications in Cardio-Oncology

 ,
,  , , , , ,
, , , , ,  , , , , and
, , , , and
Abstract

1. Introduction
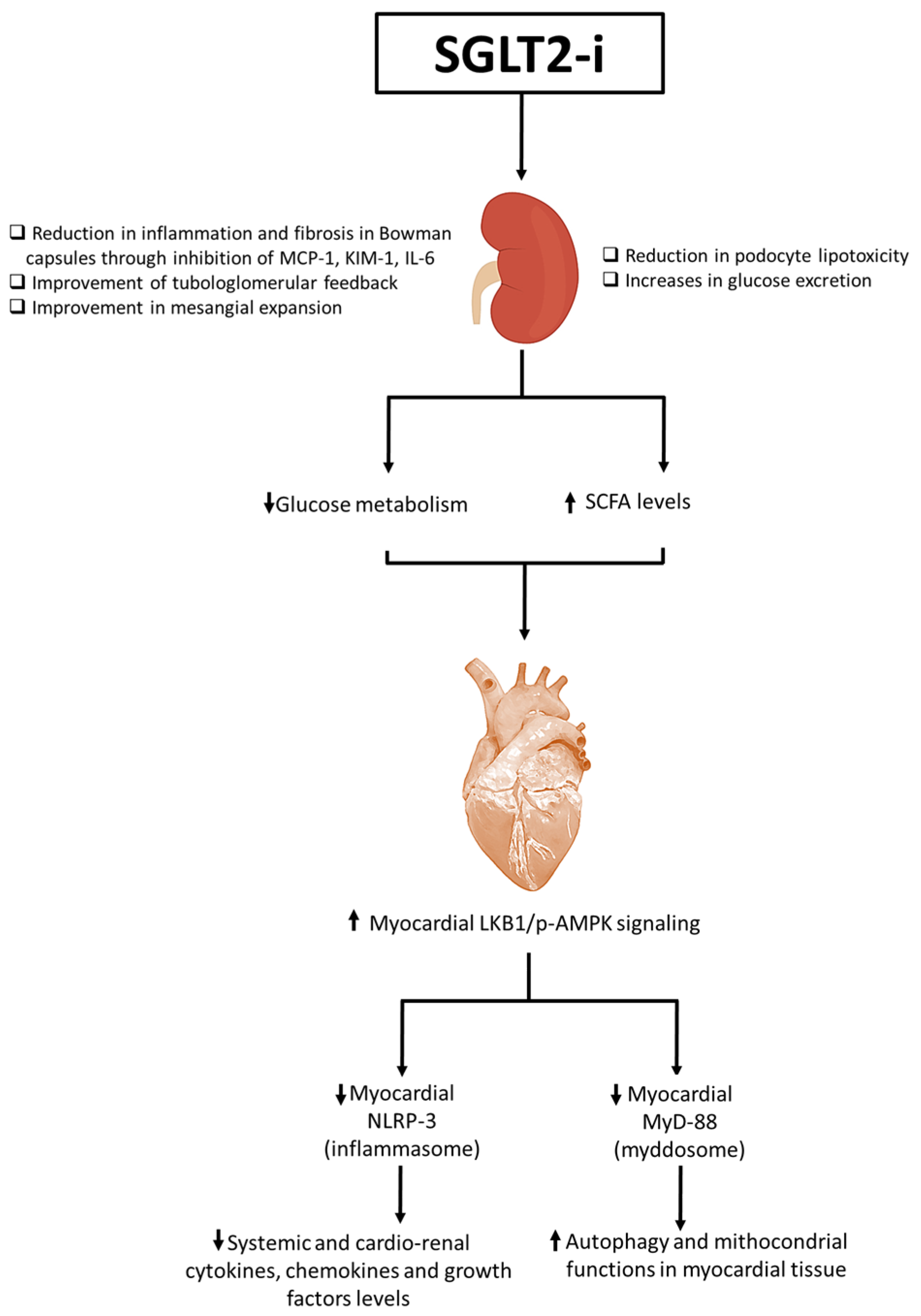
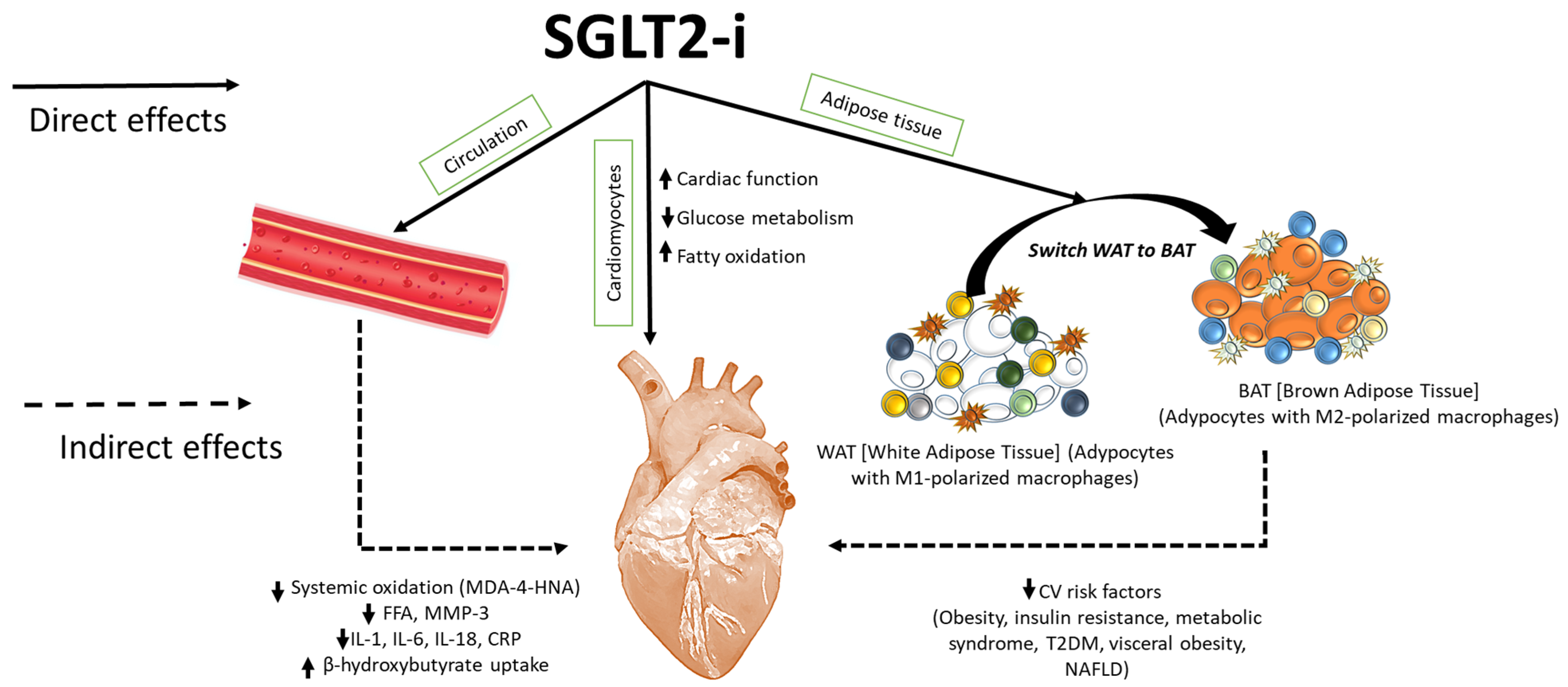
1.1. Biochemical Properties of SGLT2is: An Overview
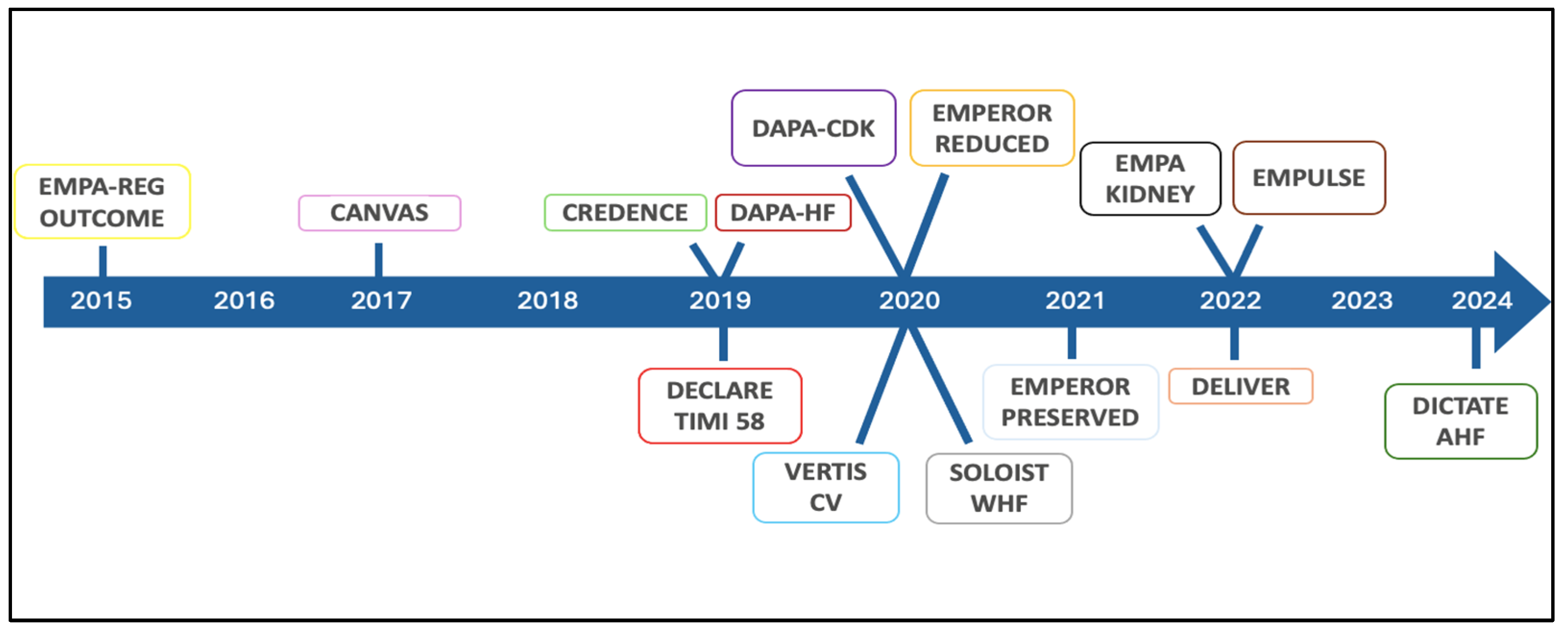
1.2. The Revolution of SGLT2is in Cardiology
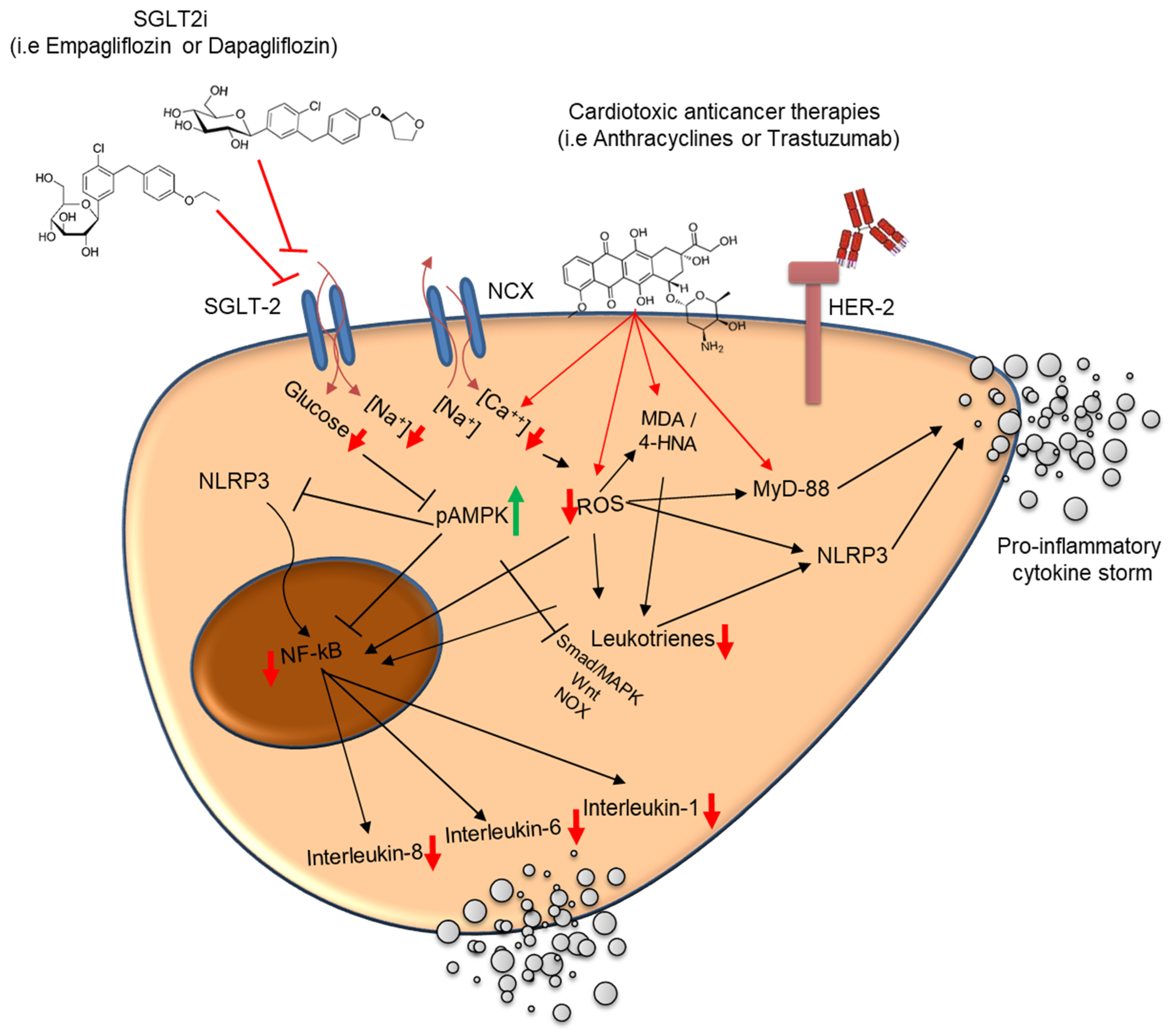
1.3. SGLT2is in the Treatment of Cancer Patients with Heart Failure or Cardiac Toxicity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Population | Cancer Therapy | SGLT2i Intervention | Key Findings |
|---|---|---|---|---|---|
| Case Series [62] | Prospective, single-arm | 7 patients with anthracycline-induced HF (CTRCD) | Anthracyclines | SGLT2is (empagliflozin or dapagliflozin) added to standard GDMT | –NYHA class improved in all patients (median III → I, p < 0.010) –LVEF improved (40% → 50%, p = 0.17) –LVEDVi reduced (82.5 → 53 mL/m2, p = 0.018) –No treatment discontinuations or major adverse effects |
| Retrospective Cohort Study [63] | Retrospective matched cohort (n = 1280) | Patients ≥ 18 years with cancer, T2DM, and HF post-cardiotoxic therapy | Anthracyclines, alkylating agents, antimetabolites, anti-HER2, TKIs, proteasome inhibitors, radiation | SGLT2is + GDMT vs. GDMT alone | –Reduced HF exacerbations: OR 0.483 (95% CI: 0.36–0.65, p < 0.001) –Lower all-cause mortality: OR 0.296 (95% CI: 0.22–0.40, p = 0.001) –Fewer hospitalizations and ED visits: OR 0.479 (95% CI: 0.383–0.599, p < 0.001) –Reduced atrial fibrillation, AKI, and RRT need |
| Observational Trial [64] | Mixed prospective/retrospective | 83 patients with active cancer (various types) | Various antineoplastic therapies | SGLT2is (unspecified type) + GDMT | –SGLT2is well tolerated with no new safety concerns –Confirmed effectiveness and clinical stability in oncology patients |
1.4. Safety Considerations and Contraindications in Oncology Settings
1.5. Cardioprotective Effects of SGLT2 Inhibitors in Cancer-Therapy-Related Cardiac Dysfunction (CTRCD): Preclinical and Clinical Evidence
1.6. Clinical Considerations for the Use of SGLT2 Inhibitors in Cardio-Oncology
- Patients with established HFrEF (LVEF ≤ 40%), where they confer well-documented reductions in cardiovascular mortality and heart failure hospitalization;
- Cancer patients receiving high-risk cardiotoxic therapies—such as high cumulative-dose anthracyclines (>250–300 mg/m2), HER2-targeted therapies (e.g., trastuzumab), or thoracic radiation—who are at an elevated risk for developing CTRCD;
- Patients with early signs of cardiac dysfunction, including abnormal global longitudinal strain (GLS), rising high-sensitivity troponin or NT-proBNP, or asymptomatic declines in LVEF (i.e., Stage B heart failure).
2. Discussion
3. Methods
- Published in English with an available abstract;
- Addressed at least one of the following topics: SGLT2 inhibitors, gliflozin, cardiotoxicity, cardiovascular diseases, cardio-oncology, cancer, cardioprotection, or cardiometabolic health.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SGLT2 | Sodium-Glucose Cotransporter 2 |
| SGLT2is | Sodium-Glucose Cotransporter 2 Inhibitors |
| T2DM | Type 2 Diabetes Mellitus |
| HF | Heart Failure |
| CTRCD | Cancer-Therapy-Related Cardiac Dysfunction |
| CTRCT | Cancer-Treatment-Related Cardiac Toxicity |
| BAT | Brown Adipose Tissue |
| WAT | White Adipose Tissue |
| MACE | Major Adverse Cardiovascular Events |
| CV | Cardiovascular |
| CVOTs | Cardiovascular Outcome Trials |
| NLRP3 | NOD-, LRR-, and Pyrin Domain-Containing Protein 3 |
| MyD-88 | Myeloid Differentiation Primary Response 88 |
| NF-kB | Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B cells |
| IL | Interleukin |
| IL-1β | Interleukin-1 beta |
| IL-6 | Interleukin-6 |
| IL-8 | Interleukin-8 |
| IL-10 | Interleukin-10 |
| IL-17α | Interleukin-17 alpha |
| IFN-γ | Interferon-gamma |
| TNF-α | Tumor Necrosis Factor alpha |
| G-CSF | Granulocyte Colony-Stimulating Factor |
| GM-CSF | Granulocyte–Macrophage Colony-Stimulating Factor |
| iROS | Intracellular Reactive Oxygen Species |
| MDA | Malondialdehyde |
| 4-HNA | 4-Hydroxynonenal |
| pAMPK | Phosphorylated AMP-Activated Protein Kinase |
| ATP | Adenosine Triphosphate |
| ADP | Adenosine Diphosphate |
| Th1 | T-helper 1 Cells |
| Th17 | T-helper 17 Cells |
| Treg | Regulatory T Cells |
| P/O ratio | Phosphate/Oxygen Ratio (measure of cardiac efficiency) |
| HER2 | Human Epidermal Growth Factor Receptor 2 |
| ERK | Extracellular Signal-Regulated Kinase |
| JNK | Janus Kinase |
| MAPKs | Mitogen-Activated Protein Kinases |
| DOX | Doxorubicin |
| EMPA | Empagliflozin |
| EMPA-DOXO | Empagliflozin + Doxorubicin Combination |
| LS | Longitudinal Strain |
| RS | Radial Strain |
| EMPACT | Empagliflozin in the Prevention of Cardiotoxicity in Cancer Patients Undergoing Chemotherapy Based on Anthracyclines Trial |
| PROTECT | Potential Protective Role of SGLT2 Inhibitors for Chemotherapy-Induced Cardiotoxicity Trial |
| PROTECTAA | CardioPROTECTion With Dapagliflozin in Breast Cancer Patients Treated with AnthrAcycline Trial |
| DM | Diabetes Mellitus |
| HR | Hazard Ratio |
| CI | Confidence Interval |
References
- Usman, M.S.; Siddiqi, T.J.; Anker, S.D.; Bakris, G.L.; Bhatt, D.L.; Filippatos, G.; Fonarow, G.C.; Greene, S.J.; Januzzi, J.L., Jr.; Khan, M.S.; et al. Effect of SGLT2 Inhibitors on Cardiovascular Outcomes Across Various Patient Populations. J. Am. Coll. Cardiol. 2023, 81, 2377–2387. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, A.M.; Awad, A.S.; Abdel-Rahman, E.M. Sodium-Glucose Co-Transporter 2 Inhibitors: Mechanism of Action and Efficacy in Non-Diabetic Kidney Disease from Bench to Bed-Side. J. Clin. Med. 2024, 13, 956. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scisciola, L.; Paolisso, P.; Belmonte, M.; Gallinoro, E.; Delrue, L.; Taktaz, F.; Fontanella, R.A.; Degrieck, I.; Pesapane, A.; Casselman, F.; et al. Myocardial sodium-glucose cotransporter 2 expression and cardiac remodelling in patients with severe aortic stenosis: The BIO-AS study. Eur. J. Heart Fail. 2024, 26, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Solini, A.; Baldi, S.; Scozzaro, T.; Polidori, D.; Natali, A.; Hansen, M.K. Role of Glycosuria in SGLT2 Inhibitor-Induced Cardiorenal Protection: A Mechanistic Analysis of the CREDENCE Trial. Diabetes 2024, 73, 250–259. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kommu, S. The Role of SGLT2 Inhibitors on Heart Failure Outcomes in Nondiabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Pharmacol. 2024, 83, 158–166. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, L.; Ota, T. Emerging roles of SGLT2 inhibitors in obesity and insulin resistance: Focus on fat browning and macrophage polarization. Adipocyte 2018, 7, 121–128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pereira, M.J.; Eriksson, J.W. Emerging Role of SGLT-2 Inhibitors for the Treatment of Obesity. Drugs 2019, 79, 219–230. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, P.C.; Ganguly, S.; Goh, S.Y. Weight loss associated with sodium-glucose cotransporter-2 inhibition: A review of evidence and underlying mechanisms. Obes. Rev. 2018, 19, 1630–1641. [Google Scholar] [CrossRef] [PubMed]
- Diallo, A.; Carlos-Bolumbu, M.; Galtier, F. Blood pressure-lowering effects of SGLT2 inhibitors and GLP-1 receptor agonists for preventing of cardiovascular events and death in type 2 diabetes: A systematic review and meta-analysis. Acta Diabetol. 2023, 60, 1651–1662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhou, S.; Liu, L. Efficacy and safety evaluation of SGLT2i on blood pressure control in patients with type 2 diabetes and hypertension: A new meta-analysis. Diabetol. Metab. Syndr. 2023, 15, 118. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koh, E.S.; Kim, G.H.; Chung, S. Intrarenal Mechanisms of Sodium-Glucose Cotransporter-2 Inhibitors on Tubuloglomerular Feedback and Natriuresis. Endocrinol. Metab. 2023, 38, 359–372. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jasleen, B.; Vishal, G.K.; Sameera, M.; Fahad, M.; Brendan, O.; Deion, S.; Pemminati, S. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors: Benefits Versus Risk. Cureus 2023, 15, e33939. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kalra, S.; Jain, A.; Ved, J.; Unnikrishnan, A.G. Sodium-glucose cotransporter 2 inhibition and health benefits: The Robin Hood effect. Indian J. Endocrinol. Metab. 2016, 20, 725–729. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhu, X.; Lin, C.; Li, L.; Hu, S.; Cai, X.; Ji, L. SGLT2i increased the plasma fasting glucagon level in patients with diabetes: A meta-analysis. Eur. J. Pharmacol. 2021, 903, 174145. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A. SGLT2 inhibitors: Cardiorenal metabolic drugs for the ages. J. Clin. Investig. 2024, 134, e177625. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ekanayake, P.; Hupfeld, C.; Mudaliar, S. Sodium-Glucose Cotransporter Type 2 (SGLT-2) Inhibitors and Ketogenesis: The Good and the Bad. Curr. Diabetes Rep. 2020, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Birnbaum, Y.; Ye, R.; Yang, H.C.; Bajaj, M.; Ye, Y. SGLT2 Inhibition by Dapagliflozin Attenuates Diabetic Ketoacidosis in Mice with Type-1 Diabetes. Cardiovasc. Drugs Ther. 2022, 36, 1091–1108. [Google Scholar] [CrossRef] [PubMed]
- Poynten, A.M.; Markovic, T.P.; Maclean, E.L.; Furler, S.M.; Freund, J.; Chisholm, D.J.; Campbell, L.V. Fat oxidation, body composition and insulin sensitivity in diabetic and normoglycaemic obese adults 5 years after weight loss. Int. J. Obes. 2003, 27, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Paccone, A.; Iovine, M.; Cavalcanti, E.; Berretta, M.; Maurea, C.; Canale, M.L.; Maurea, N. Interleukin-1 blocking agents as promising strategy for prevention of anticancer drug-induced cardiotoxicities: Possible implications in cancer patients with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6797–6812. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.R.; Lee, S.G.; Kim, S.H.; Kim, J.H.; Choi, E.; Cho, W.; Rim, J.H.; Hwang, I.; Lee, C.J.; Lee, M.; et al. SGLT2 inhibition modulates NLRP3 inflammasome activity via ketones and insulin in diabetes with cardiovascular disease. Nat. Commun. 2020, 11, 2127. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boeder, S.; Davies, M.J.; McGill, J.B.; Pratley, R.; Girard, M.; Banks, P.; Pettus, J.; Garg, S. Beta-Hydroxybutyrate Levels and Risk of Diabetic Ketoacidosis in Adults with Type 1 Diabetes Treated with Sotagliflozin. Diabetes Technol. Ther. 2024, 26, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Herring, R.A.; Shojaee-Moradie, F.; Stevenage, M.; Parsons, I.; Jackson, N.; Mendis, J.; Middleton, B.; Umpleby, A.M.; Fielding, B.A.; Davies, M.; et al. The SGLT2 Inhibitor Dapagliflozin Increases the Oxidation of Ingested Fatty Acids to Ketones in Type 2 Diabetes. Diabetes Care 2022, 45, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Wallenius, K.; Kroon, T.; Hagstedt, T.; Löfgren, L.; Sörhede-Winzell, M.; Boucher, J.; Lindén, D.; Oakes, N.D. The SGLT2 inhibitor dapagliflozin promotes systemic FFA mobilization, enhances hepatic β-oxidation, and induces ketosis. J. Lipid Res. 2022, 63, 100176. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rastogi, A.; Bhansali, A. SGLT2 Inhibitors Through the Windows of EMPA-REG and CANVAS Trials: A Review. Diabetes Ther. 2017, 8, 1245–1251. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeng, X.C.; Tian, Y.; Liang, X.M.; Wu, X.B.; Yao, C.M.; Chen, X.M. SGLT2i relieve proteinuria in diabetic nephropathy patients potentially by inhibiting renal oxidative stress rather than through AGEs pathway. Diabetol. Metab. Syndr. 2024, 16, 46. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; De Laurentiis, M.; Rea, D.; Barbieri, A.; Monti, M.G.; Carbone, A.; Paccone, A.; Altucci, L.; Conte, M.; Canale, M.L.; et al. The SGLT-2 inhibitor empagliflozin improves myocardial strain, reduces cardiac fibrosis and pro-inflammatory cytokines in non-diabetic mice treated with doxorubicin. Cardiovasc. Diabetol. 2021, 20, 150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; Canale, M.L.; Bisceglia, I.; Iovine, M.; Paccone, A.; Maurea, C.; Scherillo, M.; Merola, A.; Giordano, V.; Palma, G.; et al. Sodium-glucose cotransporter 2 inhibitor dapagliflozin prevents ejection fraction reduction, reduces myocardial and renal NF-κB expression and systemic pro-inflammatory biomarkers in models of short-term doxorubicin cardiotoxicity. Front Cardiovasc. Med. 2024, 11, 1289663. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Toldo, S.; Mezzaroma, E.; Buckley, L.F.; Potere, N.; Di Nisio, M.; Biondi-Zoccai, G.; Van Tassell, B.W.; Abbate, A. Targeting the NLRP3 inflammasome in cardiovascular diseases. Pharmacol Ther. 2022, 236, 108053. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Safaie, N.; Masoumi, S.; Alizadeh, S.; Mirzajanzadeh, P.; Nejabati, H.R.; Hajiabbasi, M.; Alivirdiloo, V.; Basmenji, N.C.; Derakhshi Radvar, A.; Majidi, Z.; et al. SGLT2 inhibitors and AMPK: The road to cellular housekeeping? Cell Biochem. Funct. 2024, 42, e3922. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.S.; Miller, E.J.; Young, L.H. AMP-activated protein kinase: A core signalling pathway in the heart. Acta Physiol. 2009, 196, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.; Herat, L.; Schlaich, M.P.; Matthews, V. The Impact of SGLT2 Inhibitors in the Heart and Kidneys Regardless of Diabetes Status. Int. J. Mol. Sci. 2023, 24, 14243. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Matthews, J.R.; Herat, L.Y.; Magno, A.L.; Gorman, S.; Schlaich, M.P.; Matthews, V.B. SGLT2 Inhibitor-Induced Sympathoexcitation in White Adipose Tissue: A Novel Mechanism for Beiging. Biomedicines 2020, 8, 514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morciano, C.; Gugliandolo, S.; Capece, U.; Di Giuseppe, G.; Mezza, T.; Ciccarelli, G.; Soldovieri, L.; Brunetti, M.; Avolio, A.; Splendore, A.; et al. SGLT2 inhibition and adipose tissue metabolism: Current outlook and perspectives. Cardiovasc Diabetol. 2024, 23, 449. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peres Valgas da Silva, C.; Shettigar, V.K.; Baer, L.A.; Abay, E.; Madaris, K.L.; Mehling, M.R.; Hernandez-Saavedra, D.; Pinckard, K.M.; Seculov, N.P.; Ziolo, M.T.; et al. Brown adipose tissue prevents glucose intolerance and cardiac remodeling in high-fat-fed mice after a mild myocardial infarction. Int. J. Obes. 2022, 46, 350–358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, L.; Nagata, N.; Nagashimada, M.; Zhuge, F.; Ni, Y.; Chen, G.; Mayoux, E.; Kaneko, S.; Ota, T. SGLT2 Inhibition by Empagliflozin Promotes Fat Utilization and Browning and Attenuates Inflammation and Insulin Resistance by Polarizing M2 Macrophages in Diet-induced Obese Mice. EBioMedicine 2017, 20, 137–149. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Mannucci, E.; Mosenzon, O.; Avogaro, A. Analyses of results from cardiovascular safety trials with DPP-4 Inhibitors: Cardiovascular outcomes, predefined safety outcomes, and pooled analysis and meta-analysis. Diabetes Care 2016, 39 (Suppl. S2), S196–S204. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. VERTIS CV Investigators. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. EMPEROR-Reduced Trial Investigators. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: A meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. EMPEROR-Preserved Trial Investigators. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.; Martinez, F.; et al. DELIVER Trial Committees and Investigators. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.S.; Jamal, W.; Salsali, A.; Schnee, J.; Kimura, K.; Zeller, C.; George, J.; Brueckmann, M.; et al. Evaluation of the effects of sodium-glu-cose co-transporter 2 inhibition with empagliflozin on morbidity and mortality in patients with chronic heart failure and a preserved ejection fraction: Rationale for and design of the EMPEROR-Preserved trial. Eur. J. Heart Fail. 2019, 21, 1279–1287. [Google Scholar] [CrossRef]
- Solomon, S.D.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; Shah, S.J.; Lindholm, D.; et al. Dapagliflozin in heart failure with preserved and mildly reduced ejection fraction: Rationale and design of the DELIVER trial. Eur. J. Heart Fail. 2021, 23, 1217–1225. [Google Scholar] [CrossRef]
- Vukadinović, D.; Abdin, A.; Anker, S.D.; Rosano, G.M.; Mahfoud, F.; Packer, M.; Butler, J.; Böhm, M. Side effects and treatment initiation barriers of sodium-glucose cotransporter 2 inhibitors in heart failure: A systematic review and meta-analysis. Eur. J. Heart Fail. 2022, 24, 1625–1632. [Google Scholar] [CrossRef]
- Van der Aart-van der Beek, A.B.; de Boer, R.A.; Heerspink, H.J.L. Kidney and heart failure outcomes associated with SGLT2 inhibitor use. Nat. Rev. Nephrol. 2022, 18, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. DAPA-CKD Trial Committees and Investigators. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; Ng, S.Y.A.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hsia, D.S.; Grove, O.; Cefalu, W.T. An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Vaduganathan, M.; Lewis, E.F.; Claggett, B.L.; Rizkala, A.R.; Wang, W.; Lefkowitz, M.P.; Shi, V.C.; Anand, I.S.; Ge, J.; et al. Health-related quality of life in heart failure with preserved ejection fraction: The PARAGON-HF trial. J. Am. Coll. Cardiol. Heart Fail. 2019, 7, 862–874. [Google Scholar]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Lenneman, C.G.; Sawyer, D.B. Cardio-oncology: An update on cardiotoxicity of cancer-related treatment. Circ. Res. 2016, 118, 1008–1020. [Google Scholar] [CrossRef]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef]
- Henson, K.; McGale, P.; Taylor, C.; Darby, S. Radiation-related mortality from heart disease and lung cancer more than 20 years after radiotherapy for breast cancer. Br. J. Cancer 2013, 108, 179–182. [Google Scholar] [CrossRef]
- De Azambuja, E.; Procter, M.J.; van Veldhuisen, D.J.; Agbor-Tarh, D.; Metzger-Filho, O.; Steinseifer, J.; Untch, M.; Smith, I.E.; Gianni, L.; Baselga, J.; et al. Trastuzumab-associated cardiac events at 8 years of median follow-up in the Herceptin adjuvant trial (BIG 1-01). J. Clin. Oncol. 2014, 32, 2159–2165. [Google Scholar] [CrossRef]
- Catino, A.B.; Hubbard, R.A.; Chirinos, J.A.; Townsend, R.; Keefe, S.; Haas, N.B.; Puzanov, I.; Fang, J.C.; Agarwal, N.; Hyman, D.; et al. Longitudinal assessment of vascular function with sunitinib in patients with metastatic renal cell carcinoma. Circ. Heart Fail. 2018, 11, e004408. [Google Scholar] [CrossRef]
- Waxman, A.J.; Clasen, S.; Hwang, W.T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-associated cardiovascular adverse events: A systematic review and meta-analysis. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef] [PubMed]
- Giangiacomi, F.; Faggiano, A.; Cardinale, D.; Rossi, F.G.; Pollina, A.; Gherbesi, E.; Gnan, E.; Carugo, S.; Vicenzi, M. Case report: Sodium-glucose cotransporter 2 inhibitors induce left ventricular reverse remodeling in anthracycline-related cardiac dysfunction-a case series. Front. Cardiovasc Med. 2023, 10, 1250185. [Google Scholar] [CrossRef] [PubMed]
- Avula, V.; Sharma, G.; Kosiborod, M.N.; Vaduganathan, M.; Neilan, T.G.; Lopez, T.; Dent, S.; Baldassarre, L.; Scherrer-Crosbie, M.; Barac, A.; et al. SGLT2 inhibitor use risk of clinical events inpatients with cancer therapy-related cardiacdysfunction. J. Am. Coll. Cardiol. Heart Fail. 2024, 12, 67–78. [Google Scholar]
- Canale, M.; Fabiani, J.; Donne, M.D.; Colombi, L.; Lupo, A.; Barletta, V.; Capati, E.; Orso, F.; Arena, G.; Frediani, L.; et al. Safety of Sglt2 Inhibitors in Active Cancer Patients: Rationale and Study Design of Tosca Trial. Eur. Hear. J. Suppl. 2024, 26, ii120. [Google Scholar] [CrossRef]
- Packer, M. Cardioprotective Effects of Sirtuin-1 and Its Downstream Effectors: Potential Role in Mediating the Heart Failure Benefits of SGLT2 (Sodium-Glucose Cotransporter 2) Inhibitors. Circ. Heart Fail. 2020, 13, e007197. [Google Scholar] [CrossRef]
- Sabatino, J.; De Rosa, S.; Tammè, L.; Iaconetti, C.; Sorrentino, S.; Polimeni, A.; Mignogna, C.; Amorosi, A.; Spaccarotella, C.; Yasuda, M.; et al. Empagliflozin prevents doxorubicin-induced myocardial dysfunction. Cardiovasc. Diabetol. 2020, 19, 66. [Google Scholar] [CrossRef]
- Gongora, C.A.; Drobni, Z.D.; Quinaglia Araujo Costa Silva, T.; Zafar, A.; Gong, J.; Zlotoff, D.A.; Gilman, H.K.; Hartmann, S.E.; Sama, S.; Nikolaidou, S.; et al. Sodium-Glucose Co-Transporter-2 Inhibitors and Cardiac Outcomes Among Patients Treated with Anthracyclines. JACC Heart Fail. 2022, 10, 559–567. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef]
- Lee, T.M.; Chang, N.C.; Lin, S.Z. Dapagliflozin, a selective SGLT2 inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free. Radic. Biol. Med. 2017, 104, 298–310. [Google Scholar] [CrossRef]
- Bhatti, A.W.; Patel, R.; Dani, S.S.; Khadke, S.; Makwana, B.; Lessey, C.; Shah, J.; Al-Husami, Z.; Yang, E.H.; Thavendiranathan, P.; et al. SGLT2i and Primary Prevention of Cancer Therapy–Related Cardiac Dysfunction in Patients with Diabetes. J. Am. Coll. Cardiol. CardioOncol. 2024; in press. [Google Scholar] [CrossRef]
| Step | Assessment Domain | Clinical Consideration | Recommended Action |
|---|---|---|---|
| 1 | Baseline Cardiovascular Risk | History of HfrEF *, ASCVD, hypertension, diabetes, CKD, prior cardiotoxic therapy | Consider SGLT2is in patients with established HFrEF (LVEF ≤ 40%) or high baseline CV risk |
| 2 | Planned or Ongoing Cancer Therapy | Anthracyclines (>250 mg/m2), HER2 inhibitors, thoracic radiation, TKi | High-risk regimens may benefit from early prophylactic SGLT2i initiation if no contraindications |
| 3 | Subclinical Cardiac Dysfunction | Elevated troponin, NT-proBNP, abnormal GLS, asymptomatic ↓ LVEF | Consider SGLT2is for cardioprotection in patients showing early cardiac injury markers, even in absence of symptoms |
| 4 | Renal Function | eGFR ≥ 20–25 mL/min/1.73 m2 | Safe to initiate empagliflozin or dapagliflozin (10 mg QD); monitor renal function regularly |
| 5 | Volume and Nutritional Status | Risk of dehydration (e.g., mucositis, vomiting, diarrhea), poor oral intake | Delay or withhold SGLT2is during active volume depletion or acute illness; reinitiate once stable |
| 6 | Glycemic Status | T2DM, risk for ketoacidosis | Monitor for euglycemic DKA, especially in T2DM or during fasting states; educate patient on warning symptoms |
| 7 | Multidisciplinary Review | Oncology, cardiology, nephrology input | Confirm indication and timing; integrate into broader cardio-oncology treatment plan |
| 8 | Monitoring Plan | Cardiac biomarkers, echocardiography, renal function | Monitor response and side effects every 4–6 weeks initially; adjust based on clinical status and cancer treatment course |
| Database | Search String |
|---|---|
| Medline | (“SGLT2 inhibitors” OR “gliflozin”) AND (“cancer” OR “cardio-oncology”) AND (“cardiotoxicity” OR “cardiovascular disease” OR “cardioprotection”) |
| EMBASE | (“SGLT2 inhibitors” OR “gliflozin”) AND (“cancer” OR “oncology”) AND (“cardiotoxicity” OR “cardiovascular disease” OR “heart failure”) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, A.; Canale, M.L.; Quagliariello, V.; Oliva, S.; Tedeschi, A.; Inno, A.; De Biasio, M.; Bisceglia, I.; Tarantini, L.; Maurea, N.; et al. SGLT2 Inhibitors in Cancer Patients: A Comprehensive Review of Clinical, Biochemical, and Therapeutic Implications in Cardio-Oncology. Int. J. Mol. Sci. 2025, 26, 4780. https://doi.org/10.3390/ijms26104780
Greco A, Canale ML, Quagliariello V, Oliva S, Tedeschi A, Inno A, De Biasio M, Bisceglia I, Tarantini L, Maurea N, et al. SGLT2 Inhibitors in Cancer Patients: A Comprehensive Review of Clinical, Biochemical, and Therapeutic Implications in Cardio-Oncology. International Journal of Molecular Sciences. 2025; 26(10):4780. https://doi.org/10.3390/ijms26104780
Chicago/Turabian StyleGreco, Alessandra, Maria Laura Canale, Vincenzo Quagliariello, Stefano Oliva, Andrea Tedeschi, Alessandro Inno, Marzia De Biasio, Irma Bisceglia, Luigi Tarantini, Nicola Maurea, and et al. 2025. "SGLT2 Inhibitors in Cancer Patients: A Comprehensive Review of Clinical, Biochemical, and Therapeutic Implications in Cardio-Oncology" International Journal of Molecular Sciences 26, no. 10: 4780. https://doi.org/10.3390/ijms26104780
APA StyleGreco, A., Canale, M. L., Quagliariello, V., Oliva, S., Tedeschi, A., Inno, A., De Biasio, M., Bisceglia, I., Tarantini, L., Maurea, N., Navazio, A., Corda, M., Iacovoni, A., Colivicchi, F., Grimaldi, M., & Oliva, F. (2025). SGLT2 Inhibitors in Cancer Patients: A Comprehensive Review of Clinical, Biochemical, and Therapeutic Implications in Cardio-Oncology. International Journal of Molecular Sciences, 26(10), 4780. https://doi.org/10.3390/ijms26104780