

The Collapse of Brain Clearance: Glymphatic-Venous Failure, Aquaporin-4 Breakdown, and AI-Empowered Precision Neurotherapeutics in Intracranial Hypertension

Abstract
1. Introduction
1.1. Definition and Overview
1.2. Scope and Objectives
1.3. Clinical and Public Health Importance
A Call to Action
2. Fundamental Concepts of Intracranial Pressure
2.1. The Monro–Kellie Hypothesis Revisited
2.2. Normal vs. Pathological ICP
2.3. Cerebral Autoregulation and Compensation
3. Etiology and Risk Factors
3.1. Primary Intracranial Hypertension (Idiopathic Intracranial Hypertension—IIH)
3.2. Secondary Intracranial Hypertension
3.3. Rare and Novel Causes
3.3.1. Post-COVID-19 Neuroinflammatory Syndromes
3.3.2. High-Altitude Cerebral Edema (HACE)
4. Pathophysiology of Intracranial Hypertension
4.1. Cellular and Molecular Mechanisms
4.2. Cerebrospinal Fluid Dynamics
4.3. Cerebral Blood Flow and Autoregulatory Failure
4.4. Systemic Contributions to ICP Dysregulation
4.5. Emerging Insights and Future Directions
5. Advanced Diagnostics and Technologies in Intracranial Hypertension
5.1. Advanced Imaging Techniques
5.1.1. MR Elastography (MRE)
5.1.2. Quantitative Susceptibility Mapping (QSM)
5.1.3. Hybrid Imaging Systems: PET/MRI
5.2. Non-Invasive Monitoring Technologies
Smart Helmets with Transcranial Doppler (TCD) Sensors
5.3. Biomarkers and Molecular Diagnostics
5.4. Emerging Technologies and Innovations
6. Advanced Therapeutic Strategies in Intracranial Hypertension
6.1. Pharmacological Innovations
Implications for Low- and Middle-Income Countries:
6.2. Device-Based Therapeutic Innovations
Global Implementation and LMIC Scalability
6.3. Emerging Experimental Therapies
- Therapies for ICH have moved beyond CSF modulation by using epigenetic regulation, vascular remodeling, anti-fibrotic approaches, and personalized neurotechnologies.
- Many pharmacological agents show great potential for lowering ICP and preserving neurovascular integrity, but in transferral to practice, certain aspects are always limiting: off-target effects, limited cohort data, and uncollapse long-term safety considerations.
- Device-based approaches, which incorporate AI into common practices such as shunt placement and adaptive valves, as well as wearable smart devices and IoT, are working to improve the precision and equity of care for patients with ICH, though these need further validation in different patient populations.
- Emerging technologies such as CRISPR, nanorobots, and biohybrid implants are an exciting vision of the future; however, they remain mainly a theoretical consideration until we can resolve regulatory, ethical, and immunological barriers.
- In this regard, this section is focused not on solutions, but rather delineating where science and engineering could merge to fill persisting gaps in patient outcomes across contexts in which resources are scarce.
6.4. Multidisciplinary and Global Perspectives
7. Long-Term Outcomes and Patient-Centered Perspectives in Intracranial Hypertension
7.1. Long-Term Outcomes of Current Therapies
7.2. Rehabilitation and Quality of Life
7.3. Patient-Centered Care and Equity
7.4. Challenges and Future Directions
8. Future Directions and Innovations in Intracranial Hypertension Management
8.1. Emerging Technologies in ICH Management
8.2. Novel Therapeutic Strategies
8.3. Integrative and Global Approaches
8.4. Challenges and Ethical Considerations
9. Clinical Implications and Translational Pathways in Intracranial Hypertension Management
9.1. Translation of Innovations into Clinical Practice
9.2. Implications for Personalized Medicine
9.3. Training and Education in Advanced ICH Care
9.4. Addressing Challenges in Clinical Translation
9.5. Role of the Microbiota-Gut–Brain Axis in ICH
9.6. Sex and Hormonal Differences in ICH
10. Challenges, Unresolved Questions, and Future Perspectives in Intracranial Hypertension Management
10.1. Key Challenges in ICH Management
10.2. Unresolved Questions in ICH Research
10.3. Future Perspectives and Opportunities
10.4. Interdisciplinary Collaboration and Global Initiatives
10.5. Sustainability and Ethical Frameworks
10.6. Behavioral and Lifestyle Interventions
10.7. New Frontiers in Training and Education
11. Conclusions: Transforming Intracranial Hypertension Management—A Vision for the Future
11.1. A Tapestry of Progress
11.2. Confronting Persistent Challenges
11.3. Visionary Opportunities for the Future
11.4. Building a Future of Precision, Equity, and Sustainability
11.5. Closing Reflections
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chu, K.H. Mathematical Modelling of Brain Haemodynamics and Pressure-Volume Compensation. Ph.D. Thesis, University of Cambridge, Cambridge, UK, 2024. [Google Scholar] [CrossRef]
- Khiabani, E.; Kalisvaart, A.C.J.; Wilkinson, C.M.; Hurd, P.L.; Buck, B.H.; Colbourne, F. Evaluating the Monro-Kellie Doctrine: Contralateral Hemisphere Shrinkage in Intracerebral Hemorrhage Patients. Transl. Stroke Res. 2024. [Google Scholar] [CrossRef]
- Sloots, J.-J.; Biessels, G.J.; Amelink, G.J.; Zwanenburg, J.J.M. Abnormalities in cardiac-induced brain tissue deformations are now detectable with MRI: A case-report of a patient who underwent craniotomy after trauma. Magn. Reson. Imaging 2023, 98, 62–65. [Google Scholar] [CrossRef]
- Yang, J.; Cao, C.; Liu, J.; Liu, Y.; Lu, J.; Yu, H.; Li, X.; Wu, J.; Yu, Z.; Li, H.; et al. Dystrophin 71 deficiency causes impaired aquaporin-4 polarization contributing to glymphatic dysfunction and brain edema in cerebral ischemia. Neurobiol. Dis. 2024, 199, 106586. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Liu, J.; Liang, C.; Yang, L.; Wang, G. Aquaporin-4 in glymphatic system, and its implication for central nervous system disorders. Neurobiol. Dis. 2023, 179, 106035. [Google Scholar] [CrossRef]
- Cibelli, A.; Ballesteros-Gomez, D.; McCutcheon, S.; Yang, G.L.; Bispo, A.; Krawchuk, M.; Piedra, G.; Spray, D.C. Astrocytes sense glymphatic-level shear stress through the interaction of sphingosine-1-phosphate with Piezo1. iScience 2024, 27, 110069. [Google Scholar] [CrossRef]
- Santhoshkumar, S.; Varadarajan, V.; Gavaskar, S.; Amalraj, J.J.; Sumathi, A. Machine Learning Model for Intracranial Hemorrhage Diagnosis and Classification. Electronics 2021, 10, 2574. [Google Scholar] [CrossRef]
- Nischal, S.A.; Badejo, O.A.; Trillo-Ordonez, Y.; Oyemolade, T.A.; Seas, A.; Malomo, T.A.; Nwaribe, E.E.; Abu-Bonsrah, N.; Deng, D.D.; Okere, O.E.; et al. The Epidemiological Burden of Neurovascular Pathology in Nigeria: A Systematic Review and Pooled Patient-Level Analysis. World Neurosurg. 2024, 185, e243–e263. [Google Scholar] [CrossRef]
- Salari, N.; Ghasemi, H.; Fatahian, R.; Mansouri, K.; Dokaneheifard, S.; Shiri, M.H.; Hemmati, M.; Mohammadi, M. The global prevalence of primary central nervous system tumors: A systematic review and meta-analysis. Eur. J. Med. Res. 2023, 28, 39. [Google Scholar] [CrossRef]
- Natterson-Horowitz, B.; Baccouche, B.M.; Head, J.M.; Shivkumar, T.; Bertelsen, M.F.; Aalkjær, C.; Smerup, M.H.; Ajijola, O.A.; Hadaya, J.; Wang, T. Did giraffe cardiovascular evolution solve the problem of heart failure with preserved ejection fraction? Evol. Med. Public Health 2021, 9, 248–255. [Google Scholar] [CrossRef]
- Kameya, N.; Sakai, I.; Saito, K.; Hamabe-Horiike, T.; Shinmyo, Y.; Nakada, M.; Okuda, S.; Kawasaki, H. Evolutionary changes leading to efficient glymphatic circulation in the mammalian brain. Nat. Commun. 2024, 15, 10048. [Google Scholar] [CrossRef]
- Vasciaveo, V.; Iadarola, A.; Casile, A.; Dante, D.; Morello, G.; Minotta, L.; Tamagno, E.; Cicolin, A.; Guglielmotto, M. Sleep fragmentation affects glymphatic system through the different expression of AQP4 in wild type and 5xFAD mouse models. Acta Neuropathol. Commun. 2023, 11, 16. [Google Scholar] [CrossRef]
- Kahle, K.T.; Klinge, P.M.; Koschnitzky, J.E.; Kulkarni, A.V.; MacAulay, N.; Robinson, S.; Schiff, S.J.; Strahle, J.M. Paediatric hydrocephalus. Nat. Rev. Dis. Primer 2024, 10, 35. [Google Scholar] [CrossRef]
- Garcia, R.M.; Shlobin, N.A.; Baticulon, R.E.; Ghotme, K.A.; Lippa, L.; Borba, L.A.; Qureshi, M.; Thango, N.; Khan, T.; Hutchinson, P.; et al. Global Neurosurgery: An Overview. Neurosurgery 2024, 95, 501–508. [Google Scholar] [CrossRef]
- Cagnazzo, F.; Villain, M.; van Dokkum, L.E.; Radu, R.A.; Morganti, R.; Gascou, G.; Dargazanli, C.; Lefevre, P.-H.; Le Bars, E.; Risi, G.; et al. Concordance between venous sinus pressure and intracranial pressure in patients investigated for idiopathic intracranial hypertension. J. Headache Pain 2024, 25, 153. [Google Scholar] [CrossRef]
- Jung, J.W.; Kang, I.; Park, J.; Lee, S.; Jeon, S.-B. Intracranial pressure trends and clinical outcomes after decompressive hemicraniectomy in malignant middle cerebral artery infarction. Ann. Intensive Care 2024, 14, 176. [Google Scholar] [CrossRef]
- Yamada, S.; Otani, T.; Ii, S.; Ito, H.; Iseki, C.; Tanikawa, M.; Watanabe, Y.; Wada, S.; Oshima, M.; Mase, M. Modeling cerebrospinal fluid dynamics across the entire intracranial space through integration of four-dimensional flow and intravoxel incoherent motion magnetic resonance imaging. Fluids Barriers CNS 2024, 21, 47. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Zhang, Y.; Nasser, A.; Hong, T.; Wang, Z.; Sun, A.; Moldovan, L.; Edwards, L.S.; Passam, F.; Butcher, K.S.; et al. Movable typing of full-lumen personalized Vein-Chips to model cerebral venous sinus thrombosis. Aggregate 2023, 4, e386. [Google Scholar] [CrossRef]
- Farmer, J.; Mitchell, S.; Sherratt, P.; Miyazaki, Y. A human surrogate neck for traumatic brain injury research. Front. Bioeng. Biotechnol. 2022, 10, 854405. [Google Scholar] [CrossRef] [PubMed]
- Pavan, P.G.; Nasim, M.; Brasco, V.; Spadoni, S.; Paoloni, F.; d’Avella, D.; Khosroshahi, S.F.; de Cesare, N.; Gupta, K.; Galvanetto, U. Development of detailed finite element models for in silico analyses of brain impact dynamics. Comput. Methods Programs Biomed. 2022, 227, 107225. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, T.; Ono, K.; Honma, M.; Asano, M.; Mori, Y.; Futamura, A.; Yano, S.; Kanemoto, M.; Hieda, S.; Baba, Y.; et al. Cerebral white matter lesions and regional blood flow are associated with reduced cognitive function in early-stage cognitive impairment. Front. Aging Neurosci. 2023, 15, 1126618. [Google Scholar] [CrossRef]
- Yang, L.; Shu, J.; Yan, A.; Yang, F.; Xu, Z.; Wei, W. White matter hyperintensities-related cortical changes and correlation with mild behavioral impairment. Adv. Med. Sci. 2022, 67, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Gędek, A.; Koziorowski, D.; Szlufik, S. Assessment of factors influencing glymphatic activity and implications for clinical medicine. Front. Neurol. 2023, 14, 1232304. [Google Scholar] [CrossRef] [PubMed]
- Beirinckx, Q.; Jeurissen, B.; Nicastro, M.; Poot, D.H.J.; Verhoye, M.; den Dekker, A.J.; Sijbers, J. Model-based super-resolution reconstruction with joint motion estimation for improved quantitative MRI parameter mapping. Comput. Med. Imaging Graph. 2022, 100, 102071. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.J.; Kim, J.-M.; Choi, B.S.; Choi, J.-H.; Ryoo, N.; Song, Y.S.; Cho, S.J.; Kim, J.H. Glymphatic function assessment in Parkinson’s disease using diffusion tensor image analysis along the perivascular space. Parkinsonism Relat. Disord. 2023, 114, 105767. [Google Scholar] [CrossRef]
- Dong, Y.; Liu, X.; Tang, M.; Huo, H.; Chen, D.; Du, X.; Wang, J.; Tang, Z.; Qiao, X.; Guo, J.; et al. Age-related differences in upper limb motor performance and intrinsic motivation during a virtual reality task. BMC Geriatr. 2023, 23, 251. [Google Scholar] [CrossRef]
- Capogna, E.; Sneve, M.H.; Raud, L.; Folvik, L.; Ness, H.T.; Walhovd, K.B.; Fjell, A.M.; Vidal-Piñeiro, D. Whole-brain connectivity during encoding: Age-related differences and associations with cognitive and brain structural decline. Cereb. Cortex 2022, 33, 68–82. [Google Scholar] [CrossRef]
- Nestrasil, I.; Ahmed, A.; Utz, J.M.; Rudser, K.; Whitley, C.B.; Jarnes-Utz, J.R. Distinct progression patterns of brain disease in infantile and juvenile gangliosidoses: Volumetric quantitative MRI study. Mol. Genet. Metab. 2018, 123, 97–104. [Google Scholar] [CrossRef]
- Steffensen, A.B.; Edelbo, B.L.; Barbuskaite, D.; Andreassen, S.N.; Olsen, M.H.; Møller, K.; MacAulay, N. Nocturnal increase in cerebrospinal fluid secretion as a circadian regulator of intracranial pressure. Fluids Barriers CNS 2023, 20, 49. [Google Scholar] [CrossRef]
- Voumvourakis, K.I.; Sideri, E.; Papadimitropoulos, G.N.; Tsantzali, I.; Hewlett, P.; Kitsos, D.; Stefanou, M.; Bonakis, A.; Giannopoulos, S.; Tsivgoulis, G.; et al. The Dynamic Relationship between the Glymphatic System, Aging, Memory, and Sleep. Biomedicines 2023, 11, 2092. [Google Scholar] [CrossRef]
- Masalkhi, M.; Ong, J.; Waisberg, E.; Berdahl, J.; Lee, A.G. Intraocular Pressure during Spaceflight and Risk of Glaucomatous Damage in Prolonged Microgravity. Encyclopedia 2023, 3, 1187–1196. [Google Scholar] [CrossRef]
- Iaccarino, C.; Chibbaro, S.; Sauvigny, T.; Timofeev, I.; Zaed, I.; Franchetti, S.; Mee, H.; Belli, A.; Buki, A.; De Bonis, P.; et al. Consensus-based recommendations for diagnosis and surgical management of cranioplasty and post-traumatic hydrocephalus from a European panel. Brain Spine 2024, 4, 102761. [Google Scholar] [CrossRef]
- Müller, S.J.; Henkes, E.; Gounis, M.J.; Felber, S.; Ganslandt, O.; Henkes, H. Non-Invasive Intracranial Pressure Monitoring. J. Clin. Med. 2023, 12, 2209. [Google Scholar] [CrossRef] [PubMed]
- Rajajee, V. Noninvasive Intracranial Pressure Monitoring: Are We There Yet? Neurocrit. Care 2024, 41, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Ragauskas, A.; Matijosaitis, V.; Zakelis, R.; Petrikonis, K.; Rastenyte, D.; Piper, I.; Daubaris, G. Clinical assessment of noninvasive intracranial pressure absolute value measurement method. Neurology 2012, 78, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Velle, F.; Lewén, A.; Howells, T.; Hånell, A.; Nilsson, P.; Enblad, P. Cerebral pressure autoregulation and optimal cerebral perfusion pressure during neurocritical care of children with traumatic brain injury. J. Neurosurg. Pediatr. 2023, 31, 503–513. [Google Scholar] [CrossRef]
- Kho, E.; Sperna Weiland, N.H.; Vlaar, A.P.J.; Veelo, D.P.; van der Ster, B.J.P.; Corsmit, O.T.; Koolbergen, D.R.; Dilai, J.; Immink, R.V. Cerebral hemodynamics during sustained intraoperative hypotension. J. Appl. Physiol. 2022, 132, 1560–1568. [Google Scholar] [CrossRef]
- Godoy, D.A.; Murillo-Cabezas, F.; Suarez, J.I.; Badenes, R.; Pelosi, P.; Robba, C. ‘‘THE MANTLE’’ bundle for minimizing cerebral hypoxia in severe traumatic brain injury. Crit. Care 2023, 27, 13. [Google Scholar] [CrossRef]
- Zhu, W.M.; Neuhaus, A.; Beard, D.J.; Sutherland, B.A.; DeLuca, G.C. Neurovascular coupling mechanisms in health and neurovascular uncoupling in Alzheimer’s disease. Brain 2022, 145, 2276–2292. [Google Scholar] [CrossRef]
- Acharya, D.; Ruesch, A.; Schmitt, S.; Yang, J.; Smith, M.A.; Kainerstorfer, J.M. Changes in neurovascular coupling with cerebral perfusion pressure indicate a link to cerebral autoregulation. J. Cereb. Blood Flow Metab. 2022, 42, 1247–1258. [Google Scholar] [CrossRef]
- Baselli, G.; Laganà, M.M. The intracranial Windkessel implies arteriovenous pulsatile coupling increased by venous resistances. Biomed. Signal Process. Control 2022, 71, 103092. [Google Scholar] [CrossRef]
- Thomale, U.W. Integrated understanding of hydrocephalus—A practical approach for a complex disease. Childs Nerv. Syst. 2021, 37, 3313–3324. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, S.O.; Adisa, A.O.; Okwuosa, C.U.; Mupparapu, M. Craniofacial disorders and dysplasias: Molecular, clinical, and management perspectives. Bone Rep. 2024, 20, 101747. [Google Scholar] [CrossRef] [PubMed]
- Nespoli, E.; Hakani, M.; Hein, T.M.; May, S.N.; Danzer, K.; Wirth, T.; Baumann, B.; Dimou, L. Glial cells react to closed head injury in a distinct and spatiotemporally orchestrated manner. Sci. Rep. 2024, 14, 2441. [Google Scholar] [CrossRef]
- Mitchell, J.L.; Lyons, H.S.; Walker, J.K.; Yiangou, A.; Grech, O.; Alimajstorovic, Z.; Greig, N.H.; Li, Y.; Tsermoulas, G.; Brock, K.; et al. The effect of GLP-1RA exenatide on idiopathic intracranial hypertension: A randomized clinical trial. Brain 2023, 146, 1821–1830. [Google Scholar] [CrossRef]
- Deveci, Ş.; Kabeloğlu, V. The Relationship between Idiopathic Intracranial Hypertension and Obstructive Sleep Apnea: Is Obesity the Only Mediating Factor between the Two? Duzce Med. J. 2024, 26, 122–128. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Bhatti, M.T.; Danesh-Meyer, H.V. Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management. J. Clin. Neurosci. 2022, 95, 172–179. [Google Scholar] [CrossRef]
- Ma, L.; Song, F. Obstructive sleep apnea-hypopnea syndrome complicated with idiopathic intracranial hypertension: A case report. Ann. Palliat. Med. 2022, 11, 3833839. [Google Scholar] [CrossRef]
- Song, Y.; Zhou, X.; Zhao, H.; Zhao, W.; Sun, Z.; Zhu, J.; Yu, Y. Characterizing the role of the microbiota-gut-brain axis in cerebral small vessel disease: An integrative multi-omics study. NeuroImage 2024, 303, 120918. [Google Scholar] [CrossRef]
- Barone, M.; Ramayo-Caldas, Y.; Estellé, J.; Tambosco, K.; Chadi, S.; Maillard, F.; Gallopin, M.; Planchais, J.; Chain, F.; Kropp, C.; et al. Gut barrier-microbiota imbalances in early life lead to higher sensitivity to inflammation in a murine model of C-section delivery. Microbiome 2023, 11, 140. [Google Scholar] [CrossRef]
- Thomas, R.K.; Padmanaban, E.; Raj, J.V.; Varadane, A.; Sambath, P. Normal variations in MR venography that may cause pitfalls in the diagnosis of cerebral venous sinus thrombosis. Glob. J. Health Sci. Res. 2023, 1, 22–26. [Google Scholar] [CrossRef]
- Tuță, S. Cerebral Venous Outflow Implications in Idiopathic Intracranial Hypertension—From Physiopathology to Treatment. Life 2022, 12, 854. [Google Scholar] [CrossRef]
- Hacein-Bey, L.; Varelas, P.N. Angioplasty and Stenting for Cerebrovascular Disease: Current Status. Neurosurg. Clin. N. Am. 2008, 19, 433–445. [Google Scholar] [CrossRef]
- Wiebe, J.; Byrne, R.A.; Bradaric, C.; Kuna, C.; Kessler, T.; Pfleiderer, M.; Kufner, S.; Xhepa, E.; Hoppmann, P.; Joner, M.; et al. A Prospective, Randomized Trial of Bioresorbable Polymer Drug-Eluting Stents versus Fully Bioresorbable Scaffolds in Patients Undergoing Coronary Stenting. J. Clin. Med. 2024, 13, 5949. [Google Scholar] [CrossRef]
- Bengueddache, S.; Cook, M.; Lehmann, S.; Arroyo, D.; Togni, M.; Puricel, S.; Cook, S. Ten-year clinical outcomes of everolimus- and biolimus-eluting coronary stents vs. everolimus-eluting bioresorbable vascular scaffolds—Insights from the EVERBIO-2 trial. Front. Cardiovasc. Med. 2024, 11, 1426348. [Google Scholar] [CrossRef]
- De Simone, R.; Sansone, M.; Curcio, F.; Russo, C.V.; Galizia, G.; Miele, A.; Stornaiuolo, A.; Piccolo, A.; Braca, S.; Abete, P. Recurrent reflex syncope in idiopathic intracranial hypertension patient resolved after lumbar puncture: Pathogenetic implications. BMC Neurol. 2023, 23, 416. [Google Scholar] [CrossRef] [PubMed]
- Eide, P.K.; Hansson, H.-A. A New Perspective on the Pathophysiology of Idiopathic Intracranial Hypertension: Role of the Glia-Neuro-Vascular Interface. Front. Mol. Neurosci. 2022, 15, 900057. [Google Scholar] [CrossRef] [PubMed]
- Ciurea, A.V.; Mohan, A.G.; Covache-Busuioc, R.-A.; Costin, H.P.; Saceleanu, V.M. The Brain’s Glymphatic System: Drawing New Perspectives in Neuroscience. Brain Sci. 2023, 13, 1005. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, S.; Olfati, M.; Ghaderi, M.; Hadizadeh, H.; Yazdanpanah, G.; Khodadadi, Z.; Karami, A.; Papi, Z.; Abdi, N.; Sharif Jalali, S.S.; et al. Neurological manifestation in COVID-19 disease with neuroimaging studies. Am. J. Neurodegener. Dis. 2023, 12, 42–84. [Google Scholar]
- Liu, J.; Hu, C.; Zhou, J.; Li, B.; Liao, X.; Liu, S.; Li, Y.; Yuan, D.; Jiang, W.; Yan, J. RNF213 rare variants and cerebral arteriovenous malformation in a Chinese population. Clin. Neurol. Neurosurg. 2021, 203, 106582. [Google Scholar] [CrossRef]
- Cuny, T.; Reynaud, R.; Raverot, G.; Coutant, R.; Chanson, P.; Kariyawasam, D.; Poitou, C.; Thomas-Teinturier, C.; Baussart, B.; Samara-Boustani, D.; et al. Diagnosis and management of children and adult craniopharyngiomas: A French Endocrine Society/French Society for Paediatric Endocrinology & Diabetes Consensus Statement. Ann. Endocrinol. 2025, 86, 101631. [Google Scholar] [CrossRef]
- Yang, Y.; Somani, S. Impact of obstructive sleep apnea on the expression of inflammatory mediators in diabetic macular edema. Eur. J. Ophthalmol. 2023, 33, 415–420. [Google Scholar] [CrossRef]
- Durduran, T.; Yodh, A.G. Diffuse correlation spectroscopy for non-invasive, micro-vascular cerebral blood flow measurement. NeuroImage 2014, 85, 51–63. [Google Scholar] [CrossRef]
- Wang, L.-W.; Cho, K.-H.; Chao, P.-Y.; Kuo, L.-W.; Chiang, C.-W.; Chao, C.-M.; Lin, M.-T.; Chang, C.-P.; Lin, H.-J.; Chio, C.-C. White and gray matter integrity evaluated by MRI-DTI can serve as noninvasive and reliable indicators of structural and functional alterations in chronic neurotrauma. Sci. Rep. 2024, 14, 7244. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Yu, H.; Zhao, H.; Wei, M.; Xing, H.; Pei, J.; Yang, Y.; Ren, K. Broadening horizons: Ferroptosis as a new target for traumatic brain injury. Burn. Trauma 2024, 12, tkad051. [Google Scholar] [CrossRef] [PubMed]
- Jing, J.; Wu, Z.; Wang, J.; Luo, G.; Lin, H.; Fan, Y.; Zhou, C. Hedgehog signaling in tissue homeostasis, cancers and targeted therapies. Signal Transduct. Target. Ther. 2023, 8, 315. [Google Scholar] [CrossRef] [PubMed]
- Kenney-Jung, D.L.; Collazo-Lopez, J.E.; Rogers, D.J.; Shanley, R.; Zatkalik, A.L.; Whitmarsh, A.E.; Roberts, A.E.; Zenker, M.; Pierpont, E.I. Epilepsy in cardiofaciocutaneous syndrome: Clinical burden and response to anti-seizure medication. Am. J. Med. Genet. A. 2024, 194, 301–310. [Google Scholar] [CrossRef]
- Sewell, M.T.; Legué, E.; Liem, K.F. Tubb4b is required for multi-ciliogenesis in the mouse. Development 2024, 151, dev201819. [Google Scholar] [CrossRef]
- Bunatyan, L.; Margineanu, A.; Boutin, C.; Montcouquiol, M.; Bachmann, S.; Ilsø Christensen, E.; Willnow, T.E.; Christ, A. LRP2 contributes to planar cell polarity-dependent coordination of motile cilia function. Cell Tissue Res. 2023, 392, 535–551. [Google Scholar] [CrossRef]
- Chowdhury, T.; Flexman, A.M.; Davis, M. Anesthetic considerations for endovascular treatment of acute ischemic stroke. Can. J. Anesth. Can. Anesth. 2022, 69, 658–673. [Google Scholar] [CrossRef]
- Li, P.; Liu, Q.; Huang, Z.; Liu, Y.; Tang, F.; Gao, S. miR-10b-5p regulates venous endothelial cells in deep venous thrombosis by targeting MFG-E8. Arch. Med. Sci. 2023, 1–16. [Google Scholar] [CrossRef]
- Tavares, V.; Savva-Bordalo, J.; Rei, M.; Liz-Pimenta, J.; Assis, J.; Pereira, D.; Medeiros, R. Plasma microRNA Environment Linked to Tissue Factor Pathway and Cancer-Associated Thrombosis: Prognostic Significance in Ovarian Cancer. Biomolecules 2024, 14, 928. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.M.; Sheth, K.N. Neurocritical Care Updates in Cerebrovascular Disease. Stroke 2022, 53, 2954–2957. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, A.H.; Adil, M.S.; Lin, X.; Chastain, D.B.; Henao-Martínez, A.F.; Franco-Paredes, C.; Somanath, P.R. Elevated Intracranial Pressure in Cryptococcal Meningoencephalitis: Examining Old, New, and Promising Drug Therapies. Pathogens 2022, 11, 783. [Google Scholar] [CrossRef] [PubMed]
- Toader, C.; Serban, M.; Covache-Busuioc, R.-A.; Radoi, M.P.; Aljboor, G.S.R.; Costin, H.P.; Corlatescu, A.D.; Glavan, L.-A.; Gorgan, R.M. Cerebellar Cavernoma Resection: Case Report with Long-Term Follow-Up. J. Clin. Med. 2024, 13, 7525. [Google Scholar] [CrossRef]
- del Campo, M.; Peeters, C.F.; Johnson, E.C.B.; Vermunt, L.; Hok-A-Hin, Y.S.; van Nee, M.; Chen-Plotkin, A.; Irwin, D.J.; Hu, W.T.; Lah, J.J.; et al. CSF proteome profiling reveals protein panels reflecting the pathophysiological diversity of Alzheimer’s disease. Nat. Aging 2022, 2, 1040–1053. [Google Scholar] [CrossRef]
- Manzano, G.; Eaton, J.; Levy, M.; Abbatemarco, J.; Aksamit, A.; Anand, P.; Balaban, D.; Barreras, P.; Baughman, R.; Bhattacharyya, S.; et al. Consensus Recommendations for the Management of Neurosarcoidosis: A Delphi Survey of Experts Across the US. Neurology 2024, 103, S24–S26. [Google Scholar] [CrossRef]
- Ajjeya, M.T.; Sudhakar, P. Role of Obstructive Sleep Apnea in Idiopathic Intracranial Hypertension (P10-4.004). Neurology 2023, 100, 122–128. [Google Scholar] [CrossRef]
- Rejas-González, R.; Montero-Calle, A.; Pastora Salvador, N.; Crespo Carballés, M.J.; Ausín-González, E.; Sánchez-Naves, J.; Pardo Calderón, S.; Barderas, R.; Guzman-Aranguez, A. Unraveling the nexus of oxidative stress, ocular diseases, and small extracellular vesicles to identify novel glaucoma biomarkers through in-depth proteomics. Redox Biol. 2024, 77, 103368. [Google Scholar] [CrossRef]
- Singh, M.; Pushpakumar, S.; Zheng, Y.; Smolenkova, I.; Akinterinwa, O.E.; Luulay, B.; Tyagi, S.C. Novel mechanism of the COVID-19 associated coagulopathy (CAC) and vascular thromboembolism. Npj Viruses 2023, 1, 3. [Google Scholar] [CrossRef]
- Mingoti, M.E.D.; Bertollo, A.G.; Simões, J.L.B.; Francisco, G.R.; Bagatini, M.D.; Ignácio, Z.M. COVID-19, Oxidative Stress, and Neuroinflammation in the Depression Route. J. Mol. Neurosci. 2022, 72, 1166–1181. [Google Scholar] [CrossRef]
- Brown, J.P.; Grocott, M.P. Humans at altitude: Physiology and pathophysiology. Contin. Educ. Anaesth. Crit. Care Pain 2013, 13, 17–22. [Google Scholar] [CrossRef]
- Vetrano, I.G.; Barbotti, A.; Erbetta, A.; Mariani, S.; Bova, S.M.; Colombo, L.; Caretti, V.; Marinoni, F.; Vestri, E.; Selvaggio, G.G.O.; et al. Multidisciplinary Management of Children with Occult Spinal Dysraphism: A Comprehensive Journey from Birth to Adulthood. Children 2022, 9, 1546. [Google Scholar] [CrossRef]
- Hopkins, C.D.; Wessel, C.; Chen, O.; El-Kersh, K.; Cathey, D.; Cave, M.C.; Cai, L.; Huang, J. A hypothesis: Potential contributions of metals to the pathogenesis of pulmonary artery hypertension. Life Sci. 2024, 336, 122289. [Google Scholar] [CrossRef]
- Mestre, H.; Du, T.; Sweeney, A.M.; Liu, G.; Samson, A.J.; Peng, W.; Mortensen, K.N.; Stæger, F.F.; Bork, P.A.R.; Bashford, L.; et al. Cerebrospinal fluid influx drives acute ischemic tissue swelling. Science 2020, 367, eaax7171. [Google Scholar] [CrossRef]
- Fang, Y.; Dai, S.; Jin, C.; Si, X.; Gu, L.; Song, Z.; Gao, T.; Chen, Y.; Yan, Y.; Yin, X.; et al. Aquaporin-4 Polymorphisms Are Associated With Cognitive Performance in Parkinson’s Disease. Front. Aging Neurosci. 2022, 13, 740491. [Google Scholar] [CrossRef]
- Andrews, M.J.; Salat, D.H.; Milberg, W.P.; McGlinchey, R.E.; Fortier, C.B. Poor sleep and decreased cortical thickness in veterans with mild traumatic brain injury and post-traumatic stress disorder. Mil. Med. Res. 2024, 11, 51. [Google Scholar] [CrossRef]
- Yamada, K. Multifaceted Roles of Aquaporins in the Pathogenesis of Alzheimer’s Disease. Int. J. Mol. Sci. 2023, 24, 6528. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Wu, M.; Tang, Q.; Yan, P.; Zhu, L. Age-Related Alterations in Immune Function and Inflammation: Focus on Ischemic Stroke. Aging Dis. 2024, 15, 1046–1074. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Bu, W.; Chen, H.; Liu, W.; Lu, X.; Zhang, G.; Liu, C.; Li, X.; Ren, H. Electroacupuncture reduces oxidative stress response and improves secondary injury of intracerebral hemorrhage in rats by activating the peroxisome proliferator-activated receptor-γ/nuclear factor erythroid2-related factor 2/γ-glutamylcysteine synthetase pathway. Neuroreport 2024, 35, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Y.; Lei, Y.; Wu, J.; Kang, Y.; Zheng, S.; Shao, L. MDM2 upregulation induces mitophagy deficiency via Mic60 ubiquitination in fetal microglial inflammation and consequently neuronal DNA damage caused by exposure to ZnO-NPs during pregnancy. J. Hazard. Mater. 2023, 457, 131750. [Google Scholar] [CrossRef]
- Li, J.; Xu, P.; Hong, Y.; Xie, Y.; Peng, M.; Sun, R.; Guo, H.; Zhang, X.; Zhu, W.; Wang, J.; et al. Lipocalin-2-mediated astrocyte pyroptosis promotes neuroinflammatory injury via NLRP3 inflammasome activation in cerebral ischemia/reperfusion injury. J. Neuroinflammation 2023, 20, 148. [Google Scholar] [CrossRef]
- Mathias, K.; Machado, R.S.; Stork, S.; Martins, C.D.; dos Santos, D.; Lippert, F.W.; Prophiro, J.S.; Petronilho, F. Short-chain fatty acid on blood-brain barrier and glial function in ischemic stroke. Life Sci. 2024, 354, 122979. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Wang, R.; Huang, Y.; Li, L.; Zhong, L.; Hu, Y.; Han, Z.; Fan, J.; Liu, P.; Zheng, Y.; et al. Elevated plasma syndecan-1 as glycocalyx injury marker predicts unfavorable outcomes after rt-PA intravenous thrombolysis in acute ischemic stroke. Front. Pharmacol. 2022, 13, 949290. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Xie, X.; Wang, L. Research Progress on Intracranial Lymphatic Circulation and Its Involvement in Disorders. Front. Neurol. 2022, 13, 865714. [Google Scholar] [CrossRef]
- Wei, Y.-C.; Hsu, C.-C.H.; Huang, W.-Y.; Lin, C.; Chen, C.-K.; Chen, Y.-L.; Chen, P.-Y.; Shyu, Y.-C.; Lin, C.-P. Vascular risk factors and astrocytic marker for the glymphatic system activity. Radiol. Med. 2023, 128, 1148–1161. [Google Scholar] [CrossRef]
- Xie, L.; Zhang, Y.; Hong, H.; Xu, S.; Cui, L.; Wang, S.; Li, J.; Liu, L.; Lin, M.; Luo, X.; et al. Higher intracranial arterial pulsatility is associated with presumed imaging markers of the glymphatic system: An explorative study. NeuroImage 2024, 288, 120524. [Google Scholar] [CrossRef]
- Lim, J.; Monteiro, A.; Kuo, C.C.; Jacoby, W.T.; Cappuzzo, J.M.; Becker, A.B.; Davies, J.M.; Snyder, K.V.; Levy, E.I.; Siddiqui, A.H. Stenting for Venous Sinus Stenosis in Patients with Idiopathic Intracranial Hypertension: An Updated Systematic Review and Meta-Analysis of the Literature. Neurosurgery 2024, 94, 648–656. [Google Scholar] [CrossRef]
- Stoklund Dittlau, K.; Terrie, L.; Baatsen, P.; Kerstens, A.; De Swert, L.; Janky, R.; Corthout, N.; Masrori, P.; Van Damme, P.; Hyttel, P.; et al. FUS-ALS hiPSC-derived astrocytes impair human motor units through both gain-of-toxicity and loss-of-support mechanisms. Mol. Neurodegener. 2023, 18, 5. [Google Scholar] [CrossRef]
- Grewal, S.; Gonçalves de Andrade, E.; Kofoed, R.H.; Matthews, P.M.; Aubert, I.; Tremblay, M.-È.; Morse, S.V. Using focused ultrasound to modulate microglial structure and function. Front. Cell Neurosci. 2023, 17, 1290628. [Google Scholar] [CrossRef]
- Plog, B.A.; Nedergaard, M. The glymphatic system in CNS health and disease: Past, present and future. Annu. Rev. Pathol. 2018, 13, 379–394. [Google Scholar] [CrossRef]
- Simon, M.; Wang, M.X.; Ismail, O.; Braun, M.; Schindler, A.G.; Reemmer, J.; Wang, Z.; Haveliwala, M.A.; O’Boyle, R.P.; Han, W.Y.; et al. Loss of perivascular aquaporin-4 localization impairs glymphatic exchange and promotes amyloid β plaque formation in mice. Alzheimers Res. Ther. 2022, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.; Garcia, T.; Aniqa, M.; Ali, S.; Ally, A.; Nauli, S. Endothelial Nitric Oxide Synthase (eNOS) and the Cardiovascular System: In Physiology and in Disease States. Am. J. Biomed. Sci. Res. 2022, 15, 153–177. [Google Scholar] [CrossRef] [PubMed]
- Gusev, E.; Solomatina, L.; Bochkarev, P.; Zudova, A.; Chereshnev, V. The Role of Systemic Inflammation in the Pathogenesis of Spontaneous Intracranial Hemorrhage in the Presence or Absence of Effective Cerebral Blood Flow. J. Clin. Med. 2024, 13, 4454. [Google Scholar] [CrossRef] [PubMed]
- Shang, P.; Zheng, R.; Wu, K.; Yuan, C.; Pan, S. New Insights on Mechanisms and Therapeutic Targets of Cerebral Edema. Curr. Neuropharmacol. 2024, 22, 2330–2352. [Google Scholar] [CrossRef]
- Wittenberg, P.; McBryde, F.D.; Korsak, A.; Rodrigues, K.L.; Paton, J.F.R.; Marina, N.; Gourine, A.V. On the regulation of arterial blood pressure by an intracranial baroreceptor mechanism. J. Physiol. 2025, 603, 2517–2532. [Google Scholar] [CrossRef]
- Zhang, Q.; Niu, Y.; Li, Y.; Xia, C.; Chen, Z.; Chen, Y.; Feng, H. Meningeal lymphatic drainage: Novel insights into central nervous system disease. Signal Transduct. Target. Ther. 2025, 10, 142. [Google Scholar] [CrossRef]
- De Simone, R.; Sansone, M.; Russo, C.; Miele, A.; Stornaiuolo, A.; Braca, S. The putative role of trigemino-vascular system in brain perfusion homeostasis and the significance of the migraine attack. Neurol. Sci. 2022, 43, 5665–5672. [Google Scholar] [CrossRef]
- Li, Y.; Zhou, H.; Xie, J.; Yu, M.; Ye, G.; Zhang, Y.; Li, Z.; Zhang, K.; Wu, J.; Xiao, S.; et al. Targeting TRPV4 to restore glymphatic system function and alleviate cerebral edema in ischemic stroke. Brain Pathol. 2025, e70022. [Google Scholar] [CrossRef]
- Delamere, N.A.; Shahidullah, M.; Mathias, R.T.; Gao, J.; Sun, X.; Sellitto, C.; White, T.W. Signaling Between TRPV1/TRPV4 and Intracellular Hydrostatic Pressure in the Mouse Lens. Investig. Ophthalmol. Vis. Sci. 2020, 61, 58. [Google Scholar] [CrossRef]
- Abbrescia, P.; Signorile, G.; Valente, O.; Palazzo, C.; Cibelli, A.; Nicchia, G.P.; Frigeri, A. Crucial role of Aquaporin-4 extended isoform in brain water Homeostasis and Amyloid-β clearance: Implications for Edema and neurodegenerative diseases. Acta Neuropathol. Commun. 2024, 12, 159. [Google Scholar] [CrossRef]
- Serrano-Pozo, A.; Li, H.; Li, Z.; Muñoz-Castro, C.; Jaisa-aad, M.; Healey, M.A.; Welikovitch, L.A.; Jayakumar, R.; Bryant, A.G.; Noori, A.; et al. Astrocyte transcriptomic changes along the spatiotemporal progression of Alzheimer’s disease. Nat. Neurosci. 2024, 27, 2384–2400. [Google Scholar] [CrossRef]
- Kopaliani, I.; Elsaid, B.; Speier, S.; Deussen, A. Immune and Metabolic Mechanisms of Endothelial Dysfunction. Int. J. Mol. Sci. 2024, 25, 13337. [Google Scholar] [CrossRef]
- Rodriguez, F.; Seta, F. Editorial: The Role of Sirtuin-1 in Cardiovascular and Renal Pathophysiology. Front. Physiol. 2021, 12, 770386. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Leskova, W.; Harris, N.R. The Endothelial Glycocalyx and Retinal Hemodynamics. Pathophysiology 2022, 29, 663–677. [Google Scholar] [CrossRef] [PubMed]
- Desantis, V.; Potenza, M.A.; Sgarra, L.; Nacci, C.; Scaringella, A.; Cicco, S.; Solimando, A.G.; Vacca, A.; Montagnani, M. microRNAs as Biomarkers of Endothelial Dysfunction and Therapeutic Target in the Pathogenesis of Atrial Fibrillation. Int. J. Mol. Sci. 2023, 24, 5307. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Barbur, I.; Calderon, A.; Banerjee, S.; Proweller, A. Notch signaling regulates arterial vasoreactivity through opposing functions of Jagged1 and Dll4 in the vessel wall. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1835–H1850. [Google Scholar] [CrossRef]
- Drew, D.; North, R.A.; Nagarathinam, K.; Tanabe, M. Structures and General Transport Mechanisms by the Major Facilitator Superfamily (MFS). Chem. Rev. 2021, 121, 5289–5335. [Google Scholar] [CrossRef]
- Orfali, R.; AlFaiz, A.; Alanazi, M.; Alabdulsalam, R.; Alharbi, M.; Alromaih, Y.; Dallak, I.; Alrahal, M.; Alwatban, A.; Saud, R. TRPV4 Channel Modulators as Potential Drug Candidates for Cystic Fibrosis. Int. J. Mol. Sci. 2024, 25, 10551. [Google Scholar] [CrossRef]
- Giamello, J.D.; Savioli, G.; Longhitano, Y.; Ferrari, F.; D’Agnano, S.; Esposito, C.; Tesauro, M.; Zanza, C. The role of acetazolamide in critical care and emergency medicine. J. Geriatr. Cardiol. JGC 2024, 21, 1085–1095. [Google Scholar] [CrossRef]
- Xiao-qun, Z.; Xian-li, M.; Ariffin, N.S. The potential of carbonic anhydrase enzymes as a novel target for anti-cancer treatment. Eur. J. Pharmacol. 2024, 976, 176677. [Google Scholar] [CrossRef]
- ter Horst, L.; van Zeggeren, I.E.; Olie, S.E.; van de Beek, D.; Brouwer, M.C. Predictors of unfavourable outcome in adults with suspected central nervous system infections: A prospective cohort study. Sci. Rep. 2023, 13, 21250. [Google Scholar] [CrossRef]
- Manto, C.; Castro-Gordon, A.; Goujard, C.; Meyer, L.; Lambotte, O.; Essat, A.; Shaiykova, A.; Boufassa, F.; Noël, N. Non-AIDS-Defining Events in Human Immunodeficiency Virus Controllers Versus Antiretroviral Therapy–Controlled Patients: A Cohort Collaboration From the French National Agency for Research on AIDS CO21 (CODEX) and CO06 (PRIMO) Cohorts. Open Forum Infect. Dis. 2023, 10, ofad067. [Google Scholar] [CrossRef]
- Marcut, L.; Mohan, A.G.; Corneschi, I.; Grosu, E.; Paltanea, G.; Avram, I.; Badaluta, A.V.; Vasilievici, G.; Nicolae, C.-A.; Ditu, L.M. Improving the Hydrophobicity of Plasticized Polyvinyl Chloride for Use in an Endotracheal Tube. Materials 2023, 16, 7089. [Google Scholar] [CrossRef]
- Lundy, P.; Barkley, A.; Rahman, A.K.M.F.; Arynchyna-Smith, A.; Thrower, J.; Stewart, A.; Dziugan, K.; Lam, S.; Hall, K.; Hauptman, J.; et al. Pediatric CSF diversion procedures for treatment of hydrocephalus during the COVID-19 pandemic. J. Neurosurg. Pediatr. 2024, 35, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Hale, A.T.; Bastarache, L.; Morales, D.M.; Wellons, J.C.; Limbrick, D.D.; Gamazon, E.R. Multi-omic analysis elucidates the genetic basis of hydrocephalus. Cell Rep. 2021, 35, 109085. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Hou, P.; Chen, Y.; Dai, Y.; Ji, Y.; Shen, Y.; Su, Y.; Liu, B.; Wang, Y.; Sun, D.; et al. Preclinical evaluation of 3D185, a novel potent inhibitor of FGFR1/2/3 and CSF-1R, in FGFR-dependent and macrophage-dominant cancer models. J. Exp. Clin. Cancer Res. 2019, 38, 372. [Google Scholar] [CrossRef]
- Tabassum, S.; Ruesch, A.; Acharya, D.; Yang, J.; Relander, F.A.J.; Scammon, B.; Wolf, M.S.; Rakkar, J.; Clark, R.S.B.; McDowell, M.M.; et al. Clinical translation of noninvasive intracranial pressure sensing with diffuse correlation spectroscopy. J. Neurosurg. 2022, 139, 184–193. [Google Scholar] [CrossRef]
- Toader, C.; Radoi, M.P.; Brehar, F.-M.; Serban, M.; Glavan, L.-A.; Covache-Busuioc, R.-A.; Ciurea, A.V.; Dobrin, N. Mirror Aneurysms of the Pericallosal Artery Clipped During a Single Surgical Procedure: Case Report and Literature Review. J. Clin. Med. 2024, 13, 6719. [Google Scholar] [CrossRef]
- Al-Bachari, S.; Naish, J.H.; Parker, G.J.M.; Emsley, H.C.A.; Parkes, L.M. Blood–Brain Barrier Leakage Is Increased in Parkinson’s Disease. Front. Physiol. 2020, 11, 593026. [Google Scholar] [CrossRef]
- Shaaban, C.E.; Rosano, C.; Cohen, A.D.; Huppert, T.; Butters, M.A.; Hengenius, J.; Parks, W.T.; Catov, J.M. Cognition and Cerebrovascular Reactivity in Midlife Women with History of Preeclampsia and Placental Evidence of Maternal Vascular Malperfusion. Front. Aging Neurosci. 2021, 13, 637574. [Google Scholar] [CrossRef]
- Rundfeldt, H.C.; Lee, C.M.; Lee, H.; Jung, K.-H.; Chang, H.; Kim, H.J. Cerebral perfusion simulation using realistically generated synthetic trees for healthy and stroke patients. Comput. Methods Programs Biomed. 2024, 244, 107956. [Google Scholar] [CrossRef]
- Vliora, M.; Ravelli, C.; Grillo, E.; Corsini, M.; Flouris, A.D.; Mitola, S. The impact of adipokines on vascular networks in adipose tissue. Cytokine Growth Factor Rev. 2023, 69, 61–72. [Google Scholar] [CrossRef]
- Alimajstorovic, Z.; Mitchell, J.L.; Yiangou, A.; Hancox, T.; Southam, A.D.; Grech, O.; Ottridge, R.; Winder, C.L.; Tahrani, A.A.; Tan, T.M.; et al. Determining the role of novel metabolic pathways in driving intracranial pressure reduction after weight loss. Brain Commun. 2023, 5, fcad272. [Google Scholar] [CrossRef]
- Taghizadeh Ghassab, F.; Shamlou Mahmoudi, F.; Taheri Tinjani, R.; Emami Meibodi, A.; Zali, M.R.; Yadegar, A. Probiotics and the microbiota-gut-brain axis in neurodegeneration: Beneficial effects and mechanistic insights. Life Sci. 2024, 350, 122748. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, J.V.; Ackrivo, J.; Hsu, J.Y.; Wilson, M.W.; Labaki, W.W.; Hansen-Flaschen, J.; Hyzy, R.C.; Choi, P.J. Lowering PCO2 With Noninvasive Ventilation Is Associated with Improved Survival in Chronic Hypercapnic Respiratory Failure. Respir. Care 2023, 68, 1613–1622. [Google Scholar] [CrossRef] [PubMed]
- Kolesnikova, T.O.; Demin, K.A.; Costa, F.V.; de Abreu, M.S.; Kalueff, A.V. Zebrafish models for studying cognitive enhancers. Neurosci. Biobehav. Rev. 2024, 164, 105797. [Google Scholar] [CrossRef] [PubMed]
- Vallée, A. Envisioning the Future of Personalized Medicine: Role and Realities of Digital Twins. J. Med. Internet Res. 2024, 26, e50204. [Google Scholar] [CrossRef]
- Hu, W.; Yao, X.; Li, Y.; Li, J.; Zhang, J.; Zou, Z.; Kang, F.; Dong, S. Injectable hydrogel with selenium nanoparticles delivery for sustained glutathione peroxidase activation and enhanced osteoarthritis therapeutics. Mater. Today Bio 2023, 23, 100864. [Google Scholar] [CrossRef]
- AbuAlrob, M.A.; Mesraoua, B. Harnessing artificial intelligence for the diagnosis and treatment of neurological emergencies: A comprehensive review of recent advances and future directions. Front. Neurol. 2024, 15, 1485799. [Google Scholar] [CrossRef]
- Angelucci, F.; Ai, A.R.; Piendel, L.; Cerman, J.; Hort, J. Integrating AI in fighting advancing Alzheimer: Diagnosis, prevention, treatment, monitoring, mechanisms, and clinical trials. Curr. Opin. Struct. Biol. 2024, 87, 102857. [Google Scholar] [CrossRef]
- Ozturk, B.; Koundal, S.; Al Bizri, E.; Chen, X.; Gursky, Z.; Dai, F.; Lim, A.; Heerdt, P.; Kipnis, J.; Tannenbaum, A.; et al. Continuous positive airway pressure increases CSF flow and glymphatic transport. JCI Insight 2023, 8, e170270. [Google Scholar] [CrossRef]
- Hirzallah, M.I.; Bose, S.; Hu, J.; Maltz, J.S. Automation of ultrasonographic optic nerve sheath diameter measurement using convolutional neural networks. J. Neuroimaging 2023, 33, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Campero-Jurado, I.; Márquez-Sánchez, S.; Quintanar-Gómez, J.; Rodríguez, S.; Corchado, J.M. Smart Helmet 5.0 for Industrial Internet of Things Using Artificial Intelligence. Sensors 2020, 20, 6241. [Google Scholar] [CrossRef] [PubMed]
- Guedj, E.; Varrone, A.; Boellaard, R.; Albert, N.L.; Barthel, H.; van Berckel, B.; Brendel, M.; Cecchin, D.; Ekmekcioglu, O.; Garibotto, V.; et al. EANM procedure guidelines for brain PET imaging using [18F]FDG, version 3. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 632–651. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hu, Y.; Liu, Q.; Lou, K.; Wang, S.; Zhang, N.; Jiang, N.; Yetisen, A.K. Multiplexed optical fiber sensors for dynamic brain monitoring. Matter 2022, 5, 3947–3976. [Google Scholar] [CrossRef]
- Rasulo, F.A.; Calza, S.; Robba, C.; Taccone, F.S.; Biasucci, D.G.; Badenes, R.; Piva, S.; Savo, D.; Citerio, G.; Dibu, J.R.; et al. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: The IMPRESSIT-2 prospective multicenter international study. Crit. Care 2022, 26, 110. [Google Scholar] [CrossRef]
- Meyer, T.; Castelein, J.; Schattenfroh, J.; Sophie Morr, A.; Vieira da Silva, R.; Tzschätzsch, H.; Reiter, R.; Guo, J.; Sack, I. Magnetic resonance elastography in a nutshell: Tomographic imaging of soft tissue viscoelasticity for detecting and staging disease with a focus on inflammation. Prog. Nucl. Magn. Reson. Spectrosc. 2024, 144–145, 1–14. [Google Scholar] [CrossRef]
- Elsawaf, Y.; Jaklitsch, E.; Belyea, M.; Rodriguez, L.; Silverman, A.; Valley, H.; Koleilat, I.; Yaghi, N.K.; Jaeggli, M. Implantable Intracranial Pressure Sensor with Continuous Bluetooth Transmission via Mobile Application. J. Pers. Med. 2023, 13, 1318. [Google Scholar] [CrossRef]
- Hao, J.; Kwapong, W.R.; Shen, T.; Fu, H.; Xu, Y.; Lu, Q.; Liu, S.; Zhang, J.; Liu, Y.; Zhao, Y.; et al. Early detection of dementia through retinal imaging and trustworthy AI. Npj Digit. Med. 2024, 7, 294. [Google Scholar] [CrossRef]
- Issa, A.S.I.; Ibrahim, R.; Ayad, M.S.; Nagy, M.; Zaher, A.M.A.; Yassin, A.M. Ultrasound-guided foam sclerotherapy versus four-layer compression only for treatment of chronic venous ulcers. Egypt. J. Radiol. Nucl. Med. 2024, 55, 113. [Google Scholar] [CrossRef]
- Bachnas, M.A.; Andonotopo, W.; Dewantiningrum, J.; Pramono, M.B.A.; Stanojevic, M.; Kurjak, A. The utilization of artificial intelligence in enhancing 3D/4D ultrasound analysis of fetal facial profiles. J. Perinat. Med. 2024, 52, 899–913. [Google Scholar] [CrossRef]
- Moro, V.; Canals, J.; Moreno, S.; Higgins-Wood, S.; Alonso, O.; Waag, A.; Prades, J.D.; Dieguez, A. Fluorescence Multi-Detection Device Using a Lensless Matrix Addressable microLED Array. Biosensors 2024, 14, 264. [Google Scholar] [CrossRef]
- Golemati, S.; Cokkinos, D.D. Recent advances in vascular ultrasound imaging technology and their clinical implications. Ultrasonics 2022, 119, 106599. [Google Scholar] [CrossRef]
- Billot, B.; Greve, D.N.; Puonti, O.; Thielscher, A.; Van Leemput, K.; Fischl, B.; Dalca, A.V.; Iglesias, J.E. SynthSeg: Segmentation of brain MRI scans of any contrast and resolution without retraining. Med. Image Anal. 2023, 86, 102789. [Google Scholar] [CrossRef]
- Khalifa, M.; Albadawy, M. AI in diagnostic imaging: Revolutionising accuracy and efficiency. Comput. Methods Programs Biomed. Update 2024, 5, 100146. [Google Scholar] [CrossRef]
- Lei, S.; Zhang, J.; Blum, N.T.; Li, M.; Zhang, D.-Y.; Yin, W.; Zhao, F.; Lin, J.; Huang, P. In vivo three-dimensional multispectral photoacoustic imaging of dual enzyme-driven cyclic cascade reaction for tumor catalytic therapy. Nat. Commun. 2022, 13, 1298. [Google Scholar] [CrossRef] [PubMed]
- Amelard, R.; Flannigan, N.; Patterson, C.A.; Heigold, H.; Hughson, R.L.; Robertson, A.D. Assessing jugular venous compliance with optical hemodynamic imaging by modulating intrathoracic pressure. J. Biomed. Opt. 2022, 27, 116005. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wang, G.; Kolluru, C.; Gu, Y.; Gao, H.; Zhang, J.; Wang, Y.; Wilson, D.L.; Zhu, X.; Flask, C.A.; et al. Transport pathways and kinetics of cerebrospinal fluid tracers in mouse brain observed by dynamic contrast-enhanced MRI. Sci. Rep. 2023, 13, 13882. [Google Scholar] [CrossRef] [PubMed]
- Biousse, V.; Danesh-Meyer, H.V.; Saindane, A.M.; Lamirel, C.; Newman, N.J. Imaging of the optic nerve: Technological advances and future prospects. Lancet Neurol. 2022, 21, 1135–1150. [Google Scholar] [CrossRef]
- Díaz-Fernández, A.; de-los-Santos-Álvarez, N.; Lobo-Castañón, M.J. Capacitive spectroscopy as transduction mechanism for wearable biosensors: Opportunities and challenges. Anal. Bioanal. Chem. 2024, 416, 2089–2095. [Google Scholar] [CrossRef]
- Li, Y.; Chen, H.; Yang, X.; Peng, A.; Wang, S.; Wang, H.; Jiang, Z.; Zhang, J.; Peng, Y.; Li, L.; et al. An Artificial Intelligence-Driven Approach for Automatic Evaluation of Right-to-Left Shunt Grades in Saline-Contrasted Transthoracic Echocardiography. Ultrasound Med. Biol. 2024, 50, 1134–1142. [Google Scholar] [CrossRef]
- Scagliusi, S.F.; Giménez-Miranda, L.; Pérez-García, P.; Fernández, D.M.; Medrano, F.J.; Huertas, G.; Yúfera, A. Bioimpedance Spectroscopy-Based Edema Supervision Wearable System for Noninvasive Monitoring of Heart Failure. IEEE Trans. Instrum. Meas. 2023, 72, 1–8. [Google Scholar] [CrossRef]
- Van Bostraeten, P.; Aertgeerts, B.; Bekkering, G.; Delvaux, N.; Haers, A.; Vanheeswyck, M.; Vandekendelaere, A.; Van der Auwera, N.; Dijckmans, C.; Ostyn, E.; et al. Digital encounter decision aids linked to clinical practice guidelines: Results from user testing SHARE-IT decision aids in primary care. BMC Med. Inform. Decis. Mak. 2023, 23, 97. [Google Scholar] [CrossRef]
- Lim, F.Y.; Neo, T.H.; Guo, H.; Goh, S.Z.; Ong, S.L.; Hu, J.; Lee, B.C.Y.; Ong, G.S.; Liou, C.X. Pilot and Field Studies of Modular Bioretention Tree System with Talipariti tiliaceum and Engineered Soil Filter Media in the Tropics. Water 2021, 13, 1817. [Google Scholar] [CrossRef]
- Wilson, M.H.; Ashworth, E.; Hutchinson, P.J. A proposed novel traumatic brain injury classification system—An overview and inter-rater reliability validation on behalf of the Society of British Neurological Surgeons. Br. J. Neurosurg. 2022, 36, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Yang, Y.; Zhou, Y. Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning. Brain Sci. 2024, 14, 1175. [Google Scholar] [CrossRef] [PubMed]
- Vandenbulcke, S.; De Pauw, T.; Dewaele, F.; Degroote, J.; Segers, P. Computational fluid dynamics model to predict the dynamical behavior of the cerebrospinal fluid through implementation of physiological boundary conditions. Front. Bioeng. Biotechnol. 2022, 10, 1040517. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, W.; Bai, X.; Zhang, X.; Yuan, Z.; Jiao, B.; Zhang, Y.; Li, Z.; Zhang, P.; Tang, H.; et al. Increased glymphatic system activity in migraine chronification by diffusion tensor image analysis along the perivascular space. J. Headache Pain 2023, 24, 147. [Google Scholar] [CrossRef]
- Wu, C.-H.; Kuo, Y.; Ling, Y.-H.; Wang, Y.-F.; Fuh, J.-L.; Lirng, J.-F.; Wu, H.-M.; Wang, S.-J.; Chen, S.-P. Dynamic changes in glymphatic function in reversible cerebral vasoconstriction syndrome. J. Headache Pain 2024, 25, 17. [Google Scholar] [CrossRef]
- Hagiwara, A.; Fujita, S.; Kurokawa, R.; Andica, C.; Kamagata, K.; Aoki, S. Multiparametric MRI. Investig. Radiol. 2023, 58, 548–560. [Google Scholar] [CrossRef]
- Leary, O.P.; Zhong, Z.; Bi, L.; Jiao, Z.; Dai, Y.-W.; Ma, K.; Sayied, S.; Kargilis, D.; Imami, M.; Zhao, L.-M.; et al. MRI-Based Prediction of Clinical Improvement after Ventricular Shunt Placement for Normal Pressure Hydrocephalus: Development and Evaluation of an Integrated Multisequence Machine Learning Algorithm. AJNR Am. J. Neuroradiol. 2024, 45, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Zheng, X.; Yang, Z.; Li, H.; Fei, H.; Zhang, C. Machine learning for clustering and postclosure outcome of adult CHD-PAH patients with borderline hemodynamics. J. Heart Lung Transplant. 2023, 42, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Pleșa, F.C.; Jijie, A.; Toma, G.S.; Ranetti, A.E.; Manole, A.M.; Rotaru, R.; Caloianu, I.; Anghel, D.; Dulămea, O.A. Challenges in Cerebral Venous Thrombosis Management—Case Reports and Short Literature Review. Life 2023, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Renslo, J.; Wong, K.; Clifford, T.G.; Beutler, B.D.; Kim, P.E.; Gholamrezanezhad, A. Current Trends and Applications of PET/MRI Hybrid Imaging in Neurodegenerative Diseases and Normal Aging. Diagnostics 2024, 14, 585. [Google Scholar] [CrossRef]
- Roshan, M.P.; Al-Shaikhli, S.A.; Linfante, I.; Antony, T.T.; Clarke, J.E.; Noman, R.; Lamy, C.; Britton, S.; Belnap, S.C.; Abrams, K.; et al. Revolutionizing Intracranial Hemorrhage Diagnosis: A Retrospective Analytical Study of Viz.ai ICH for Enhanced Diagnostic Accuracy. Cureus 2024, 16, e66449. [Google Scholar] [CrossRef]
- Li, M.; Wu, S.; Liang, X.; Gao, C.; Hu, M.; Chen, Z.; He, P.; Jia, T.; Xiong, L. The role of 4D flow MRI in deep vein thrombosis research. Meta-Radiology 2024, 3, 100123. [Google Scholar] [CrossRef]
- Thomaides-Brears, H.B.; Lepe, R.; Banerjee, R.; Duncker, C. Multiparametric MR mapping in clinical decision-making for diffuse liver disease. Abdom. Radiol. 2020, 45, 3507–3522. [Google Scholar] [CrossRef]
- Zhan, J.-L.; Lu, W.-B.; Ding, C.; Sun, Z.; Yu, B.-Y.; Ju, L.; Liang, X.-H.; Chen, Z.-M.; Chen, H.; Jia, Y.-H.; et al. Flexible and wearable battery-free backscatter wireless communication system for colour imaging. Npj Flex. Electron. 2024, 8, 19. [Google Scholar] [CrossRef]
- Priyadarshi, R.; Ranjan, R.; Kumar Vishwakarma, A.; Yang, T.; Singh Rathore, R. Exploring the Frontiers of Unsupervised Learning Techniques for Diagnosis of Cardiovascular Disorder: A Systematic Review. IEEE Access 2024, 12, 139253–139272. [Google Scholar] [CrossRef]
- Zhang, B.; Huang, Z.; Song, H.; Kim, H.S.; Park, J. Wearable Intracranial Pressure Monitoring Sensor for Infants. Biosensors 2021, 11, 213. [Google Scholar] [CrossRef]
- Childs, A.; Mayol, B.; Lasalde-Ramírez, J.A.; Song, Y.; Sempionatto, J.R.; Gao, W. Diving into Sweat: Advances, Challenges, and Future Directions in Wearable Sweat Sensing. ACS Nano 2024, 18, 24605–24616. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.S.; Gatti, A.A.; Farrokhyar, F.; Xie, F.; Hanna, W.C. Clinical utility of artificial intelligence–augmented endobronchial ultrasound elastography in lymph node staging for lung cancer. JTCVS Tech. 2024, 27, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Kim, H.; Zitouni, M.S.; Khandoker, A.; Jelinek, H.F.; Hadjileontiadis, L.; Lee, U.; Jeong, Y. Trends in Smart Helmets with Multimodal Sensing for Health and Safety: Scoping Review. JMIR MHealth UHealth 2022, 10, e40797. [Google Scholar] [CrossRef] [PubMed]
- Viarasilpa, T. Managing Intracranial Pressure Crisis. Curr. Neurol. Neurosci. Rep. 2025, 25, 12. [Google Scholar] [CrossRef]
- Chen, Y.; Mateski, J.; Gerace, L.; Wheeler, J.; Burl, J.; Prakash, B.; Svedin, C.; Amrick, R.; Adams, B.D. Non-coding RNAs and neuroinflammation: Implications for neurological disorders. Exp. Biol. Med. 2024, 249, 10120. [Google Scholar] [CrossRef]
- Sharma, P.; Roy, A.; Dhamija, R.K.; Bhushan, S.; Baswal, K.; Kulandaisamy, R.; Yadav, S.; Kumar, S.; Inampudi, K.K. A comprehensive proteomic profiling of urinary exosomes and the identification of early non-invasive biomarker in patients with coronary artery disease. J. Proteom. 2024, 293, 105059. [Google Scholar] [CrossRef]
- Yoon, J.H.; Seo, Y.; Jo, Y.S.; Lee, S.; Cho, E.; Cazenave-Gassiot, A.; Shin, Y.-S.; Moon, M.H.; An, H.J.; Wenk, M.R.; et al. Brain lipidomics: From functional landscape to clinical significance. Sci. Adv. 2022, 8, eadc9317. [Google Scholar] [CrossRef]
- Ghouneimy, A.; Mahas, A.; Marsic, T.; Aman, R.; Mahfouz, M. CRISPR-Based Diagnostics: Challenges and Potential Solutions toward Point-of-Care Applications. ACS Synth. Biol. 2022, 12, 1–16. [Google Scholar] [CrossRef]
- Huang, Z.; Lyon, C.J.; Wang, J.; Lu, S.; Hu, T.Y. CRISPR Assays for Disease Diagnosis: Progress to and Barriers Remaining for Clinical Applications. Adv. Sci. 2023, 10, 2301697. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Liu, Y.; Wu, Y.; Bian, B.; Shang, J.; Li, R. Recent Progress in Wearable Near-Sensor and In-Sensor Intelligent Perception Systems. Sensors 2024, 24, 2180. [Google Scholar] [CrossRef]
- Bhardwaj, H.; Archana; Noumani, A.; Himanshu, J.K.; Chakravorty, S.; Solanki, P.R. Recent advancement in the detection of potential cancer biomarkers using the nanomaterial integrated electrochemical sensing technique: A detailed review. Mater. Adv. 2024, 5, 475–503. [Google Scholar] [CrossRef]
- Kazanskiy, N.L.; Butt, M.A.; Khonina, S.N. Recent Advances in Wearable Optical Sensor Automation Powered by Battery versus Skin-like Battery-Free Devices for Personal Healthcare—A Review. Nanomaterials 2022, 12, 334. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liang, C.; Peng, S.; Bao, S.; Xue, F.; Lian, X.; Liu, Y.; Wang, G. Aquaporin-4 activation facilitates glymphatic system function and hematoma clearance post-intracerebral hemorrhage. Glia 2025, 73, 368–380. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Liu, T.; Wang, X.; Sharma, A.; Schmidt-Wolf, I.G.H.; Jiang, L.; Hou, J. Exploring the role of histone deacetylase and histone deacetylase inhibitors in the context of multiple myeloma: Mechanisms, therapeutic implications, and future perspectives. Exp. Hematol. Oncol. 2024, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Pu, T.; Wang, L.; Marshall, C.; Wu, T.; Xiao, M. Astroglial water channel aquaporin 4-mediated glymphatic clearance function: A determined factor for time-sensitive treatment of aerobic exercise in patients with Alzheimer’s disease. Med. Hypotheses 2018, 119, 18–21. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Canney, M.; Carpentier, A.; Idbaih, A. Overcoming the blood brain barrier in glioblastoma: Status and future perspective. Rev. Neurol. 2023, 179, 430–436. [Google Scholar] [CrossRef]
- Arms, L.M.; Duchatel, R.J.; Jackson, E.R.; Sobrinho, P.G.; Dun, M.D.; Hua, S. Current status and advances to improving drug delivery in diffuse intrinsic pontine glioma. J. Control. Release 2024, 370, 835–865. [Google Scholar] [CrossRef]
- Rufai, S.R.; Thomas, M.G.; Purohit, R.; Bowman, R.; Bunce, C.; Panteli, V.; Gottlob, I.; Patel, C.K.; Hayward, R.; Dunaway, D.J.; et al. Recognition of Intracranial Hypertension in Children using Handheld Optical Coherence Tomography: The RIO Diagnostic Accuracy Study. Invest. Ophthalmol. Vis. Sci. 2023, 64, 4404. [Google Scholar] [CrossRef]
- Lee, W.T.; Lee, H.; Kim, J.; Jung, Y.; Choi, E.; Jeong, J.H.; Jeong, J.-H.; Lee, J.H.; Youn, Y.S. Alveolar macrophage phagocytosis-evading inhaled microgels incorporating nintedanib-PLGA nanoparticles and pirfenidone-liposomes for improved treatment of pulmonary fibrosis. Bioact. Mater. 2024, 33, 262–278. [Google Scholar] [CrossRef]
- Li, B.; Bai, W.-W.; Guo, T.; Tang, Z.-Y.; Jing, X.-J.; Shan, T.-C.; Yin, S.; Li, Y.; Wang, F.; Zhu, M.-L.; et al. Statins improve cardiac endothelial function to prevent heart failure with preserved ejection fraction through upregulating circRNA-RBCK1. Nat. Commun. 2024, 15, 2953. [Google Scholar] [CrossRef]
- Mei, J.; Li, Y.; Niu, L.; Liang, R.; Tang, M.; Cai, Q.; Xu, J.; Zhang, D.; Yin, X.; Liu, X.; et al. SGLT2 inhibitors: A novel therapy for cognitive impairment via multifaceted effects on the nervous system. Transl. Neurodegener. 2024, 13, 41. [Google Scholar] [CrossRef]
- Tang, H.; Xu, C.; Zhang, P.; Luo, T.; Huang, Y.; Yang, X. A profile of SGLT-2 inhibitors in hyponatremia: The evidence to date. Eur. J. Pharm. Sci. 2023, 184, 106415. [Google Scholar] [CrossRef]
- Sim, A.Y.; Choi, D.H.; Kim, J.Y.; Kim, E.R.; Goh, A.-R.; Lee, Y.-H.; Lee, J.E. SGLT2 and DPP4 inhibitors improve Alzheimer’s disease-like pathology and cognitive function through distinct mechanisms in a T2D-AD mouse model. Biomed. Pharmacother. 2023, 168, 115755. [Google Scholar] [CrossRef]
- Li, C.; Spencer, G.; Husain, M.J.; Nugent, R.; Auzenne, D.; Kostova, D.; Richter, P. Barriers to accessibility of medicines for hyperlipidemia in low- and middle-income countries. PLoS Glob. Public Health 2024, 4, e0002905. [Google Scholar] [CrossRef]
- Chesnut, R.M.; Temkin, N.; Videtta, W.; Petroni, G.; Lujan, S.; Pridgeon, J.; Dikmen, S.; Chaddock, K.; Barber, J.; Machamer, J.; et al. Consensus-Based Management Protocol (CREVICE Protocol) for the Treatment of Severe Traumatic Brain Injury Based on Imaging and Clinical Examination for Use When Intracranial Pressure Monitoring Is Not Employed. J. Neurotrauma 2020, 37, 1291–1299. [Google Scholar] [CrossRef]
- Knudsen, J.E.; Ghaffar, U.; Ma, R.; Hung, A.J. Clinical applications of artificial intelligence in robotic surgery. J. Robot. Surg. 2024, 18, 102. [Google Scholar] [CrossRef]
- Toader, C.; Serban, M.; Covache-Busuioc, R.-A.; Radoi, M.P.; Aljboor, G.S.R.; Costin, H.P.; Ilie, M.-M.; Popa, A.A.; Gorgan, R.M. Single-Stage Microsurgical Clipping of Multiple Intracranial Aneurysms in a Patient with Cerebral Atherosclerosis: A Case Report and Review of Surgical Management. J. Clin. Med. 2025, 14, 269. [Google Scholar] [CrossRef]
- Karabacak, M.; Margetis, K. Natural language processing reveals research trends and topics in The Spine Journal over two decades: A topic modeling study. Spine J. 2024, 24, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Govindarajan, V.; Marshall, L.; Sahni, A.; Cetatoiu, M.; Eickhoff, E.; Davee, J.; St Clair, N.; Schulz, N.; Hoganson, D.M.; Hammer, P.E.; et al. Impact of Age-related change in Caval Flow Ratio on Hepatic Flow Distribution in Fontan. MedRxiv 2023. [CrossRef] [PubMed]
- Tzeis, S.; Gerstenfeld, E.P.; Kalman, J.; Saad, E.B.; Sepehri Shamloo, A.; Andrade, J.G.; Barbhaiya, C.R.; Baykaner, T.; Boveda, S.; Calkins, H.; et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2024, 26, euae043. [Google Scholar] [CrossRef] [PubMed]
- Goertz, L.; Pieczewski, J.; Zopfs, D.; Kabbasch, C.; Timmer, M.; Goldbrunner, R.; Wetzel, C. Prospective evaluation of flow-regulated valves for idiopathic normal pressure hydrocephalus: 1-year results. J. Clin. Neurosci. 2024, 124, 94–101. [Google Scholar] [CrossRef]
- Zhang, S.; Sun, J.; Guo, S.; Wang, Y.; Zhang, Y.; Lei, J.; Liu, X.; Chen, H. Balancing functions of antifouling, nitric oxide release and vascular cell selectivity for enhanced endothelialization of assembled multilayers. Regen. Biomater. 2024, 11, rbae096. [Google Scholar] [CrossRef]
- Alam, S.N.; Ghosh, A.; Shrivastava, P.; Shukla, U.; Garg, K.; Edara, A.C.; Sahoo, N. An introduction to triboelectric nanogenerators. Nano-Struct. Nano-Objects 2023, 34, 100980. [Google Scholar] [CrossRef]
- Ghadi, Y.Y.; Mazhar, T.; Shahzad, T.; Amir Khan, M.; Abd-Alrazaq, A.; Ahmed, A.; Hamam, H. The role of blockchain to secure internet of medical things. Sci. Rep. 2024, 14, 18422. [Google Scholar] [CrossRef]
- Mutanu, L.; Gupta, K.; Gohil, J. Leveraging IoT solutions for enhanced health information exchange. Technol. Soc. 2022, 68, 101882. [Google Scholar] [CrossRef]
- Barile, B.; Mola, M.G.; Formaggio, F.; Saracino, E.; Cibelli, A.; Gargano, C.D.; Mogni, G.; Frigeri, A.; Caprini, M.; Benfenati, V.; et al. AQP4-independent TRPV4 modulation of plasma membrane water permeability. Front. Cell. Neurosci. 2023, 17, 1247761. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Ojha, R.; Chamlagain, R.; Chhetri, S.; Prasad, P.; Baral, B.; Gyawali, B.; Shrestha, A.; Yadav, J.K. Therapeutic drug level of tacrolimus causing intracranial hemorrhage in a patient with renal transplant. Clin. Case Rep. 2022, 10, e05788. [Google Scholar] [CrossRef] [PubMed]
- Bassi, S.T.; Pamu, R.; Ambika, S.; Praveen, S.; Priyadarshini, D.; Dharini, V.; Padmalakshmi, K. Optical coherence tomography in papilledema: A probe into the intracranial pressure correlation. Indian J. Ophthalmol. 2024, 72, 672. [Google Scholar] [CrossRef]
- Proietti, R.; Rivera-Caravaca, J.M.; López-Gálvez, R.; Harrison, S.L.; Marín, F.; Underhill, P.; Shantsila, E.; McDowell, G.; Vinciguerra, M.; Davies, R.; et al. Cerebrovascular, Cognitive and Cardiac Benefits of SGLT2 Inhibitors Therapy in Patients with Atrial Fibrillation and Type 2 Diabetes Mellitus: Results from a Global Federated Health Network Analysis. J. Clin. Med. 2023, 12, 2814. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, X.; Zhang, J. Pirfenidone and nintedanib attenuate pulmonary fibrosis in mice by inhibiting the expression of JAK2. J. Thorac. Dis. 2024, 16, 1128–1140. [Google Scholar] [CrossRef]
- Han, Y.; Chen, L.; Guo, Y.; Wang, C.; Zhang, C.; Kong, L.; Ma, H. Class I HDAC Inhibitor Improves Synaptic Proteins and Repairs Cytoskeleton Through Regulating Synapse-Related Genes In vitro and In vivo. Front. Aging Neurosci. 2021, 12, 619866. [Google Scholar] [CrossRef]
- Jeong, J.-H.; Koo, J.-H.; Yook, J.S.; Cho, J.-Y.; Kang, E.-B. Neuroprotective Benefits of Exercise and MitoQ on Memory Function, Mitochondrial Dynamics, Oxidative Stress, and Neuroinflammation in D-Galactose-Induced Aging Rats. Brain Sci. 2021, 11, 164. [Google Scholar] [CrossRef]
- Westgate, C.S.J.; Kamp-Jensen, C.; Israelsen, I.M.E.; Toft-Bertelsen, T.; Wardman, J.H.; Jensen, C.A.; Styrishave, B.; MacAulay, N.; Jensen, R.H.; Eftekhari, S. Acetazolamide and topiramate lower intracranial pressure through differential mechanisms: The effect of acute and chronic administration. Br. J. Pharmacol. 2024, 181, 70–86. [Google Scholar] [CrossRef]
- Camilleri, E.; van Rein, N.; van Vlijmen, B.J.M.; Biedermann, J.S.; Kruip, M.J.H.A.; Leebeek, F.W.; van der Meer, F.J.; Cobbaert, C.M.; Cannegieter, S.C.; Lijfering, W.M. Influence of rosuvastatin on apolipoproteins and coagulation factor levels: Results from the STAtin Reduce Thrombophilia trial. Res. Pract. Thromb. Haemost. 2023, 7, 100063. [Google Scholar] [CrossRef]
- Smith, A.G.; Singleton, J.R.; Aperghis, A.; Coffey, C.S.; Creigh, P.; Cudkowicz, M.; Conwit, R.; Ecklund, D.; Fedler, J.K.; Gudjonsdottir, A.; et al. Safety and Efficacy of Topiramate in Individuals with Cryptogenic Sensory Peripheral Neuropathy With Metabolic Syndrome: The TopCSPN Randomized Clinical Trial. JAMA Neurol. 2023, 80, 1334–1343. [Google Scholar] [CrossRef]
- Pittock, S.J.; Barnett, M.; Bennett, J.L.; Berthele, A.; de Sèze, J.; Levy, M.; Nakashima, I.; Oreja-Guevara, C.; Palace, J.; Paul, F.; et al. Ravulizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder. Ann. Neurol. 2023, 93, 1053–1068. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, P.; Macleod, T.; Wong, C.; Harland, M.; McGonagle, D. Revisiting p38 Mitogen-Activated Protein Kinases (MAPK) in Inflammatory Arthritis: A Narrative of the Emergence of MAPK-Activated Protein Kinase Inhibitors (MK2i). Pharmaceuticals 2023, 16, 1286. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, L.; Menon, V.; Arnold, A.C.; Mollan, S.P. Managing idiopathic intracranial hypertension in the eye clinic. Eye 2024, 38, 2472–2481. [Google Scholar] [CrossRef]
- Notten, P.; ten Cate, H.; ten Cate-Hoek, A.J. Postinterventional antithrombotic management after venous stenting of the iliofemoral tract in acute and chronic thrombosis: A systematic review. J. Thromb. Haemost. 2021, 19, 753–796. [Google Scholar] [CrossRef]
- Rajeswaran, A.B.; Ali, A.; Safi, S.; Abdulghani Saleh, A.E. Efficacy and safety of local fibrinolytic therapy in intracranial hemorrhages: A systematic review and meta-analysis of randomised controlled trials. World Neurosurg. X 2024, 22, 100316. [Google Scholar] [CrossRef]
- Beretta, S.; Versace, A.; Fiore, G.; Piola, M.; Martini, B.; Bigiogera, V.; Coppadoro, L.; Mariani, J.; Tinti, L.; Pirovano, S.; et al. Selective Cerebrospinal Fluid Hypothermia: Bioengineering Development and In Vivo Study of an Intraventricular Cooling Device (V-COOL). Neurotherapeutics 2022, 19, 1942–1950. [Google Scholar] [CrossRef]
- Eraky, A.M.; Yerramalla, Y.; Khan, A.; Mokhtar, Y.; Alamrosy, M.; Farag, A.; Wright, A.; Grounds, M.; Gregorich, N.M. Beta-Blockers as an Immunologic and Autonomic Manipulator in Critically Ill Patients: A Review of the Recent Literature. Int. J. Mol. Sci. 2024, 25, 8058. [Google Scholar] [CrossRef]
- Sami, A.; Xue, Z.; Tazein, S.; Arshad, A.; He Zhu, Z.; Ping Chen, Y.; Hong, Y.; Tian Zhu, X.; Jin Zhou, K. CRISPR–Cas9-based genetic engineering for crop improvement under drought stress. Bioengineered 2021, 12, 5814–5829. [Google Scholar] [CrossRef]
- Egunlusi, A.O.; Joubert, J. NMDA Receptor Antagonists: Emerging Insights into Molecular Mechanisms and Clinical Applications in Neurological Disorders. Pharmaceuticals 2024, 17, 639. [Google Scholar] [CrossRef]
- Rodriguez-Almaraz, J.E.; Butowski, N. Therapeutic and Supportive Effects of Cannabinoids in Patients with Brain Tumors (CBD Oil and Cannabis). Curr. Treat. Options Oncol. 2023, 24, 30–44. [Google Scholar] [CrossRef]
- Do, C.; Vasquez, P.C.; Soleimani, M. Metabolic Alkalosis Pathogenesis, Diagnosis, and Treatment: Core Curriculum 2022. Am. J. Kidney Dis. 2022, 80, 536–551. [Google Scholar] [CrossRef]
- Sharma, S.; Mohler, J.; Mahajan, S.D.; Schwartz, S.A.; Bruggemann, L.; Aalinkeel, R. Microbial Biofilm: A Review on Formation, Infection, Antibiotic Resistance, Control Measures, and Innovative Treatment. Microorganisms 2023, 11, 1614. [Google Scholar] [CrossRef]
- Morris-Blanco, K.C.; Chokkalla, A.K.; Arruri, V.; Jeong, S.; Probelsky, S.M.; Vemuganti, R. Epigenetic mechanisms and potential therapeutic targets in stroke. J. Cereb. Blood Flow Metab. 2022, 42, 2000–2016. [Google Scholar] [CrossRef] [PubMed]
- Gohari, S.; Reshadmanesh, T.; Khodabandehloo, H.; Karbalaee-Hasani, A.; Ahangar, H.; Arsang-Jang, S.; Ismail-Beigi, F.; Dadashi, M.; Ghanbari, S.; Taheri, H.; et al. The effect of EMPAgliflozin on markers of inflammation in patients with concomitant type 2 diabetes mellitus and Coronary ARtery Disease: The EMPA-CARD randomized controlled trial. Diabetol. Metab. Syndr. 2022, 14, 170. [Google Scholar] [CrossRef] [PubMed]
- Alam, F.; Ashfaq Ahmed, M.; Jalal, A.H.; Siddiquee, I.; Adury, R.Z.; Hossain, G.M.M.; Pala, N. Recent Progress and Challenges of Implantable Biodegradable Biosensors. Micromachines 2024, 15, 475. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Hu, C.; Wang, Z.; Wang, L. Silk-based wearable devices for health monitoring and medical treatment. iScience 2024, 27, 109604. [Google Scholar] [CrossRef]
- Latifi-Navid, H.; Mokhtari, S.; Taghizadeh, S.; Moradi, F.; Poostforoush-Fard, D.; Alijanpour, S.; Aghanoori, M.-R. AI-assisted multi-OMICS analysis reveals new markers for the prediction of AD. Biochim. Biophys. Acta Mol. Basis Dis. 2025, 1871, 167925. [Google Scholar] [CrossRef]
- Danelakis, A.; Stubberud, A.; Tronvik, E.; Matharu, M. The Emerging Clinical Relevance of Artificial Intelligence, Data Science, and Wearable Devices in Headache: A Narrative Review. Life 2025, 15, 909. [Google Scholar] [CrossRef]
- Becatti, M.; Mozafari, M.; Risoluti, R. Editorial: Advancements and future challenges in molecular diagnostics and therapeutics. Front. Mol. Biosci. 2025, 12, 1620909. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.S.; Khandelwal, S.; Thakre, Y.; Rangole, J.; Kulkarni, M.B.; Bhaiyya, M. A Review on 3D-Printed Miniaturized Devices for Point-of-Care-Testing Applications. Biosensors 2025, 15, 340. [Google Scholar] [CrossRef] [PubMed]
- Agbeyangi, A.O.; Lukose, J.M. Telemedicine Adoption and Prospects in Sub-Sahara Africa: A Systematic Review with a Focus on South Africa, Kenya, and Nigeria. Healthcare 2025, 13, 762. [Google Scholar] [CrossRef] [PubMed]
- Dodoo, J.E.; Al-Samarraie, H.; Alsswey, A. The development of telemedicine programs in Sub-Saharan Africa: Progress and associated challenges. Health Technol. 2022, 12, 33–46. [Google Scholar] [CrossRef]
- Huang, Y.; Guo, X.; Wu, Y.; Chen, X.; Feng, L.; Xie, N.; Shen, G. Nanotechnology’s frontier in combatting infectious and inflammatory diseases: Prevention and treatment. Signal Transduct. Target. Ther. 2024, 9, 34. [Google Scholar] [CrossRef]
- Won, S.; An, J.; Song, H.; Im, S.; You, G.; Lee, S.; Koo, K.-I.; Hwang, C.H. Transnasal targeted delivery of therapeutics in central nervous system diseases: A narrative review. Front. Neurosci. 2023, 17, 1137096. [Google Scholar] [CrossRef]
- Bellavite, P. Neuroprotective Potentials of Flavonoids: Experimental Studies and Mechanisms of Action. Antioxidants 2023, 12, 280. [Google Scholar] [CrossRef]
- Hu, Y.; Hu, S.; Zhang, S.; Dong, S.; Hu, J.; Kang, L.; Yang, X. A double-layer hydrogel based on alginate-carboxymethyl cellulose and synthetic polymer as sustained drug delivery system. Sci. Rep. 2021, 11, 9142. [Google Scholar] [CrossRef]
- Hu, B.; Gao, J.; Lu, Y.; Wang, Y. Applications of Degradable Hydrogels in Novel Approaches to Disease Treatment and New Modes of Drug Delivery. Pharmaceutics 2023, 15, 2370. [Google Scholar] [CrossRef]
- Li, M.; Zhou, S.; Zhang, S.; Xie, X.; Nie, J.; Wang, Q.; Ma, L.; Cheng, Y.; Luo, J. Transdermal delivery of CRISPR/Cas9-mediated melanoma gene therapy via polyamines-modified thermosensitive hydrogels. J. Nanobiotechnol. 2025, 23, 441. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Y. Personalized dynamic transport of magnetic nanorobots inside the brain vasculature. Nanotechnology 2020, 31, 495706. [Google Scholar] [CrossRef]
- Watson, C.J.; Monstad-Rios, A.T.; Bhimani, R.M.; Gistelinck, C.; Willaert, A.; Coucke, P.; Hsu, Y.-H.; Kwon, R.Y. Phenomics-based quantification of CRISPR-induced mosaicism in zebrafish. Cell Syst. 2020, 10, 275.e5–286.e5. [Google Scholar] [CrossRef]
- BenDavid, E.; Ramezanian, S.; Lu, Y.; Rousseau, J.; Schroeder, A.; Lavertu, M.; Tremblay, J.P. Emerging Perspectives on Prime Editor Delivery to the Brain. Pharmaceuticals 2024, 17, 763. [Google Scholar] [CrossRef]
- Toader, C.; Tataru, C.P.; Munteanu, O.; Covache-Busuioc, R.-A.; Serban, M.; Ciurea, A.V.; Enyedi, M. Revolutionizing Neuroimmunology: Unraveling Immune Dynamics and Therapeutic Innovations in CNS Disorders. Int. J. Mol. Sci. 2024, 25, 13614. [Google Scholar] [CrossRef]
- Aqel, S.; Al-Thani, N.; Haider, M.Z.; Abdelhady, S.; Al Thani, A.A.; Kobeissy, F.; Shaito, A.A. Biomaterials in Traumatic Brain Injury: Perspectives and Challenges. Biology 2023, 13, 21. [Google Scholar] [CrossRef]
- Binsar, F.; Arief, M.; Tjhin, V.U.; Susilowati, I. Exploring consumer sentiments in telemedicine and telehealth services: Towards an integrated framework for innovation. J. Open Innov. Technol. Mark. Complex. 2025, 11, 100453. [Google Scholar] [CrossRef]
- Huanbutta, K.; Burapapadh, K.; Kraisit, P.; Sriamornsak, P.; Ganokratanaa, T.; Suwanpitak, K.; Sangnim, T. Artificial intelligence-driven pharmaceutical industry: A paradigm shift in drug discovery, formulation development, manufacturing, quality control, and post-market surveillance. Eur. J. Pharm. Sci. 2024, 203, 106938. [Google Scholar] [CrossRef]
- Li, S.; Qiu, N.; Ni, A.; Hamblin, M.H.; Yin, K.-J. Role of regulatory non-coding RNAs in traumatic brain injury. Neurochem. Int. 2024, 172, 105643. [Google Scholar] [CrossRef]
- Toader, C.; Serban, M.; Munteanu, O.; Covache-Busuioc, R.-A.; Enyedi, M.; Ciurea, A.V.; Tataru, C.P. From Synaptic Plasticity to Neurodegeneration: BDNF as a Transformative Target in Medicine. Int. J. Mol. Sci. 2025, 26, 4271. [Google Scholar] [CrossRef]
- Duan, M.; Xu, Y.; Li, Y.; Feng, H.; Chen, Y. Targeting brain-peripheral immune responses for secondary brain injury after ischemic and hemorrhagic stroke. J. Neuroinflammation 2024, 21, 102. [Google Scholar] [CrossRef]
- Agarwal, N.; Lewis, L.D.; Hirschler, L.; Rivera, L.R.; Naganawa, S.; Levendovszky, S.R.; Ringstad, G.; Klarica, M.; Wardlaw, J.; Iadecola, C.; et al. Current Understanding of the Anatomy, Physiology, and Magnetic Resonance Imaging of Neurofluids: Update From the 2022 “ISMRM Imaging Neurofluids Study group” Workshop in Rome. J. Magn. Reson. Imaging 2024, 59, 431–449. [Google Scholar] [CrossRef]
- Ringstad, G. Glymphatic imaging: A critical look at the DTI-ALPS index. Neuroradiology 2024, 66, 157–160. [Google Scholar] [CrossRef]
- Mehryab, F.; Taghizadeh, F.; Goshtasbi, N.; Merati, F.; Rabbani, S.; Haeri, A. Exosomes as cutting-edge therapeutics in various biomedical applications: An update on engineering, delivery, and preclinical studies. Biochimie 2023, 213, 139–167. [Google Scholar] [CrossRef]
- Shoraka, Z.B. Biomedical Engineering Literature: Advanced Reading Skills for Research and Practice. Int. J. Sci. Res. Manag. 2024, 12, 1270–1284. [Google Scholar] [CrossRef]
- Wu, Y.; Li, L.; Xin, B.; Hu, Q.; Dong, X.; Li, Z. Application of machine learning in personalized medicine. Intell. Pharm. 2023, 1, 152–156. [Google Scholar] [CrossRef]
- Wang, Y.; Zhai, W.; Cheng, S.; Li, J.; Zhang, H. Surface-functionalized design of blood-contacting biomaterials for preventing coagulation and promoting hemostasis. Friction 2023, 11, 1371–1394. [Google Scholar] [CrossRef]
- Guan, H.; Yang, R.; Li, W.; Tao, Y.; Chen, C.; Tai, H.; Su, Y.; Wang, Y.; Jiang, Y.; Li, W. Self-powered multifunctional flexible sensor for wearable biomonitoring. Sens. Actuators B Chem. 2023, 377, 132996. [Google Scholar] [CrossRef]
- Millarch, A.S.; Bonde, A.; Bonde, M.; Klein, K.V.; Folke, F.; Rudolph, S.S.; Sillesen, M. Assessing optimal methods for transferring machine learning models to low-volume and imbalanced clinical datasets: Experiences from predicting outcomes of Danish trauma patients. Front. Digit. Health 2023, 5, 1249258. [Google Scholar] [CrossRef]
- Toader, C.; Munteanu, O.; Radoi, M.P.; Crivoi, C.; Covache-Busuioc, R.-A.; Serban, M.; Ciurea, A.V.; Dobrin, N. AI-Driven Prediction of Glasgow Coma Scale Outcomes in Anterior Communicating Artery Aneurysms. J. Clin. Med. 2025, 14, 2672. [Google Scholar] [CrossRef]
- Vostrý, M.; Pešatová, I.; Lanková, B.; Štolová, I.; Fleischmann, O. Supervised Combined Therapy for a Pediatric Patient After a Cerebral Stroke: Selected Special Pedagogical, Occupational Therapy, and Psychological Approaches in a Case Study of the Czech Republic. Neuro Endocrinol. Lett. 2024, 45, 157–166. [Google Scholar]
- Santilli, G.; Mangone, M.; Agostini, F.; Paoloni, M.; Bernetti, A.; Diko, A.; Tognolo, L.; Coraci, D.; Vigevano, F.; Vetrano, M.; et al. Evaluation of Rehabilitation Outcomes in Patients with Chronic Neurological Health Conditions Using a Machine Learning Approach. J. Funct. Morphol. Kinesiol. 2024, 9, 176. [Google Scholar] [CrossRef]
- Manser, P.; Michels, L.; Schmidt, A.; Barinka, F.; de Bruin, E.D. Effectiveness of an Individualized Exergame-Based Motor-Cognitive Training Concept Targeted to Improve Cognitive Functioning in Older Adults with Mild Neurocognitive Disorder: Study Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2023, 12, e41173. [Google Scholar] [CrossRef]
- Wang, Y.; Ye, M.; Tong, Y.; Xiong, L.; Wu, X.; Geng, C.; Zhang, W.; Dai, Z.; Tian, W.; Rong, J. Effects of robot-assisted therapy on upper limb and cognitive function in patients with stroke: Study protocol of a randomized controlled study. Trials 2022, 23, 538. [Google Scholar] [CrossRef]
- Bremner, J.D.; Gazi, A.H.; Lambert, T.P.; Nawar, A.; Harrison, A.B.; Welsh, J.W.; Vaccarino, V.; Walton, K.M.; Jaquemet, N.; Mermin-Bunnell, K.; et al. Noninvasive Vagal Nerve Stimulation for Opioid Use Disorder. Ann. Depress. Anxiety 2023, 10, 1117. [Google Scholar]
- Ge, X.; Zhang, Y.; Xin, T.; Luan, X. Effects of 10 Hz repetitive transcranial magnetic stimulation of the right dorsolateral prefrontal cortex in the vegetative state. Exp. Ther. Med. 2021, 21, 206. [Google Scholar] [CrossRef]
- Heydari, A.; Manzari, Z.S.; Mohammadpourhodki, R. Peer-support interventions and related outcomes in patients with myocardial infarction: A systematic review. Heliyon 2024, 10, e25314. [Google Scholar] [CrossRef]
- Nimmagadda, N.; Aboian, E.; Kiang, S.; Fischer, U. The Role of Artificial Intelligence in Vascular Care. JVS-Vasc. Insights 2024, 3, 100179. [Google Scholar] [CrossRef]
- Huma, T.; Peng, Z. Introduction to Regulatory Affairs and Different Regulatory Bodies for Pharmaceutical Products and Impact of Digitalization on Regulatory Affairs. Pharmacol. Pharm. 2023, 14, 463–477. [Google Scholar] [CrossRef]
- Stahl, B.C.; Eke, D. The ethics of ChatGPT—Exploring the ethical issues of an emerging technology. Int. J. Inf. Manag. 2024, 74, 102700. [Google Scholar] [CrossRef]
- Frączek, W.; Kotela, A.; Kotela, I.; Grodzik, M. Nanostructures in Orthopedics: Advancing Diagnostics, Targeted Therapies, and Tissue Regeneration. Materials 2024, 17, 6162. [Google Scholar] [CrossRef]
- Farasati Far, B.; Safaei, M.; Nahavandi, R.; Gholami, A.; Naimi-Jamal, M.R.; Tamang, S.; Ahn, J.E.; Ramezani Farani, M.; Huh, Y.S. Hydrogel Encapsulation Techniques and Its Clinical Applications in Drug Delivery and Regenerative Medicine: A Systematic Review. ACS Omega 2024, 9, 29139–29158. [Google Scholar] [CrossRef]
- Demblon, A.; Karakoc, O.; Sam, J.; Zhao, D.; Atli, K.C.; Mabe, J.H.; Karaman, I. Compositional and microstructural sensitivity of the actuation fatigue response in NiTiHf high temperature shape memory alloys. Mater. Sci. Eng. A 2022, 838, 142786. [Google Scholar] [CrossRef]
- Boulingre, M.; Portillo-Lara, R.; Green, R.A. Biohybrid neural interfaces: Improving the biological integration of neural implants. Chem. Commun. 2023, 59, 14745–14758. [Google Scholar] [CrossRef]
- Aslam, N.; Zhou, H.; Urbach, E.K.; Turner, M.J.; Walsworth, R.L.; Lukin, M.D.; Park, H. Quantum sensors for biomedical applications. Nat. Rev. Phys. 2023, 5, 157–169. [Google Scholar] [CrossRef]
- Li, J.; Zhang, F.; Xia, X.; Zhang, K.; Wu, J.; Liu, Y.; Zhang, C.; Cai, X.; Lu, J.; Xu, L.; et al. An ultrasensitive multimodal intracranial pressure biotelemetric system enabled by exceptional point and iontronics. Nat. Commun. 2024, 15, 9557. [Google Scholar] [CrossRef]
- Li, T.; Shen, Y.; Li, Y.; Zhang, Y.; Wu, S. The status quo and future prospects of digital twins for healthcare. EngMedicine 2024, 1, 100042. [Google Scholar] [CrossRef]
- Yang, X.; Yu, P.; Zhang, H.; Zhang, R.; Liu, Y.; Li, H.; Sun, P.; Liu, X.; Wu, Y.; Jia, X.; et al. Deep Learning Algorithm Enables Cerebral Venous Thrombosis Detection with Routine Brain Magnetic Resonance Imaging. Stroke 2023, 54, 1357–1366. [Google Scholar] [CrossRef]
- Hołubowicz, R.; Du, S.W.; Felgner, J.; Smidak, R.; Choi, E.H.; Palczewska, G.; Menezes, C.R.; Dong, Z.; Gao, F.; Medani, O.; et al. Safer and efficient base editing and prime editing via ribonucleoproteins delivered through optimized lipid-nanoparticle formulations. Nat. Biomed. Eng. 2024, 9, 57–78. [Google Scholar] [CrossRef]
- Kong, X.; Gao, P.; Wang, J.; Fang, Y.; Hwang, K.C. Advances of medical nanorobots for future cancer treatments. J. Hematol. Oncol. 2023, 16, 74. [Google Scholar] [CrossRef]
- Ahamed, J.; Jaswanth Gowda, B.H.; Almalki, W.H.; Gupta, N.; Sahebkar, A.; Kesharwani, P. Recent advances in nanoparticle-based approaches for the treatment of brain tumors: Opportunities and challenges. Eur. Polym. J. 2023, 193, 112111. [Google Scholar] [CrossRef]
- Srihagulang, C.; Vongsfak, J.; Vaniyapong, T.; Chattipakorn, N.; Chattipakorn, S.C. Potential roles of vagus nerve stimulation on traumatic brain injury: Evidence from in vivo and clinical studies. Exp. Neurol. 2022, 347, 113887. [Google Scholar] [CrossRef]
- Gomolka, R.S.; Hablitz, L.M.; Mestre, H.; Giannetto, M.; Du, T.; Hauglund, N.L.; Xie, L.; Peng, W.; Martinez, P.M.; Nedergaard, M.; et al. Loss of aquaporin-4 results in glymphatic system dysfunction via brain-wide interstitial fluid stagnation. eLife 2023, 12, e82232. [Google Scholar] [CrossRef]
- Namatame, C.; Abe, Y.; Miyasaka, Y.; Takai, Y.; Matsumoto, Y.; Takahashi, T.; Mashimo, T.; Misu, T.; Fujihara, K.; Yasui, M.; et al. Humanized-Aquaporin-4-Expressing Rat Created by Gene-Editing Technology and Its Use to Clarify the Pathology of Neuromyelitis Optica Spectrum Disorder. Int. J. Mol. Sci. 2024, 25, 8169. [Google Scholar] [CrossRef]
- Rhomberg, T.; Trivik-Barrientos, F.; Hakim, A.; Raabe, A.; Murek, M. Applied deep learning in neurosurgery: Identifying cerebrospinal fluid (CSF) shunt systems in hydrocephalus patients. Acta Neurochir. 2024, 166, 69. [Google Scholar] [CrossRef]
- Zhong, L.; Wang, J.; Wang, P.; Liu, X.; Liu, P.; Cheng, X.; Cao, L.; Wu, H.; Chen, J.; Zhou, L. Neural stem cell-derived exosomes and regeneration: Cell-free therapeutic strategies for traumatic brain injury. Stem Cell Res. Ther. 2023, 14, 198. [Google Scholar] [CrossRef]
- Aragón-Navas, A.; López-Cano, J.J.; Johnson, M.; Sigen, A.; Vicario-de-la-Torre, M.; Andrés-Guerrero, V.; Tai, H.; Wang, W.; Bravo-Osuna, I.; Herrero-Vanrell, R. Smart biodegradable hydrogels: Drug-delivery platforms for treatment of chronic ophthalmic diseases affecting the back of the eye. Int. J. Pharm. 2024, 649, 123653. [Google Scholar] [CrossRef]
- Baldwin, A.; States, G.; Pikov, V.; Gunalan, P.; Elyahoodayan, S.; Kilgore, K.; Meng, E. Recent advances in facilitating the translation of bioelectronic medicine therapies. Curr. Opin. Biomed. Eng. 2024, 33, 100575. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, Q.; Dong, Q.; Shen, J.; Hao, J.; Li, D.; Xu, T.; Cai, X.; Bai, W.; Ying, T.; et al. Nanoarchitectonic Engineering of Thermal-Responsive Magnetic Nanorobot Collectives for Intracranial Aneurysm Therapy. Small 2024, 20, 2400408. [Google Scholar] [CrossRef]
- Yoo, S.-S.; Kim, E.; Kowsari, K.; Van Reet, J.; Kim, H.-C.; Yoon, K. Non-invasive enhancement of intracortical solute clearance using transcranial focused ultrasound. Sci. Rep. 2023, 13, 12339. [Google Scholar] [CrossRef]
- Sempionatto, J.R.; Lasalde-Ramírez, J.A.; Mahato, K.; Wang, J.; Gao, W. Wearable chemical sensors for biomarker discovery in the omics era. Nat. Rev. Chem. 2022, 6, 899–915. [Google Scholar] [CrossRef]
- Ahmed, Z. Precision medicine with multi-omics strategies, deep phenotyping, and predictive analysis. Prog. Mol. Biol. Transl. Sci. 2022, 190, 101–125. [Google Scholar] [CrossRef]
- Kamya, P.; Ozerov, I.V.; Pun, F.W.; Tretina, K.; Fokina, T.; Chen, S.; Naumov, V.; Long, X.; Lin, S.; Korzinkin, M.; et al. PandaOmics: An AI-Driven Platform for Therapeutic Target and Biomarker Discovery. J. Chem. Inf. Model. 2024, 64, 3961–3969. [Google Scholar] [CrossRef]
- Sikander, S.; Biswas, P.; Kulkarni, P. Recent advancements in telemedicine: Surgical, diagnostic and consultation devices. Biomed. Eng. Adv. 2023, 6, 100096. [Google Scholar] [CrossRef]
- Lamem, M.F.H.; Sahid, M.I.; Ahmed, A. Artificial intelligence for access to primary healthcare in rural settings. J. Med. Surg. Public Health 2025, 5, 100173. [Google Scholar] [CrossRef]
- Barrit, S.; Al Barajraji, M.; El Hadwe, S.; Niset, A.; Foreman, B.; Park, S.; Lazaridis, C.; Shutter, L.; Appavu, B.; Kirschen, M.P.; et al. Intracranial multimodal monitoring in neurocritical care (Neurocore-iMMM): An open, decentralized consensus. Crit. Care 2024, 28, 427. [Google Scholar] [CrossRef]
- Shim, Y.; Kim, J.; Kim, H.S.; Oh, J.; Lee, S.; Ha, E.J. Intracranial Pressure Monitoring for Acute Brain Injured Patients: When, How, What Should We Monitor. Korean J. Neurotrauma 2023, 19, 149–161. [Google Scholar] [CrossRef]
- Palaniyandi, T.; Kanagavalli, B.; Prabhakaran, P.; Viswanathan, S.; Rahaman Abdul Wahab, M.; Natarajan, S.; Kumar Kaliya Moorthy, S.; Kumarasamy, S. Nanosensors for the diagnosis and therapy of neurodegenerative disorders and inflammatory bowel disease. Acta Histochem. 2023, 125, 151997. [Google Scholar] [CrossRef]
- Cascella, M.; Montomoli, J.; Bellini, V.; Vittori, A.; Biancuzzi, H.; Dal Mas, F.; Bignami, E.G. Crossing the AI Chasm in Neurocritical Care. Computers 2023, 12, 83. [Google Scholar] [CrossRef]
- Petrella, R.J. The AI Future of Emergency Medicine. Ann. Emerg. Med. 2024, 84, 139–153. [Google Scholar] [CrossRef]
- Munusamy, T.; Karuppiah, R.; Bahuri, N.F.A.; Sockalingam, S.; Cham, C.Y.; Waran, V. Telemedicine via Smart Glasses in Critical Care of the Neurosurgical Patient—COVID-19 Pandemic Preparedness and Response in Neurosurgery. World Neurosurg. 2021, 145, e53–e60. [Google Scholar] [CrossRef]
- Molla, G.; Bitew, M. Revolutionizing Personalized Medicine: Synergy with Multi-Omics Data Generation, Main Hurdles, and Future Perspectives. Biomedicines 2024, 12, 2750. [Google Scholar] [CrossRef]
- Hu, C.; Jia, W. Multi-omics profiling: The way toward precision medicine in metabolic diseases. J. Mol. Cell Biol. 2021, 13, 576–593. [Google Scholar] [CrossRef]
- Zhao, Z.; Liu, R.; Groner, J.I.; Xiang, H.; Zhang, P. Data Imputation for Clinical Trial Emulation: A Case Study on Impact of Intracranial Pressure Monitoring for Traumatic Brain Injury. AMIA Summits Transl. Sci. Proc. 2023, 2023, 612–621. [Google Scholar]
- Liu, D.; Zusman, B.E.; Shaffer, J.R.; Li, Y.; Arockiaraj, A.I.; Liu, S.; Weeks, D.E.; Desai, S.M.; Kochanek, P.M.; Puccio, A.M.; et al. Decreased DNA Methylation of RGMA is Associated with Intracranial Hypertension After Severe Traumatic Brain Injury: An Exploratory Epigenome-Wide Association Study. Neurocrit. Care 2022, 37, 26–37. [Google Scholar] [CrossRef]
- Martínez-Iglesias, O.; Naidoo, V.; Carrera, I.; Corzo, L.; Cacabelos, R. Natural Bioactive Products as Epigenetic Modulators for Treating Neurodegenerative Disorders. Pharmaceuticals 2023, 16, 216. [Google Scholar] [CrossRef]
- Giralt-Steinhauer, E.; Jiménez-Balado, J.; Fernández-Pérez, I.; Rey Álvarez, L.; Rodríguez-Campello, A.; Ois, Á.; Cuadrado-Godia, E.; Jiménez-Conde, J.; Roquer, J. Genetics and Epigenetics of Spontaneous Intracerebral Hemorrhage. Int. J. Mol. Sci. 2022, 23, 6479. [Google Scholar] [CrossRef]
- Griñán-Ferré, C.; Bellver-Sanchis, A.; Guerrero, A.; Pallàs, M. Advancing personalized medicine in neurodegenerative diseases: The role of epigenetics and pharmacoepigenomics in pharmacotherapy. Pharmacol. Res. 2024, 205, 107247. [Google Scholar] [CrossRef]
- Basnawi, A.; Koshak, A. Application of Artificial Intelligence in Advanced Training and Education of Emergency Medicine Doctors: A Narrative Review. Emerg. Care Med. 2024, 1, 247–259. [Google Scholar] [CrossRef]
- Gulamali, F.; Jayaraman, P.; Sawant, A.S.; Desman, J.; Fox, B.; Chang, A.; Soong, B.Y.; Arivazagan, N.; Reynolds, A.S.; Duong, S.Q.; et al. Derivation, external and clinical validation of a deep learning approach for detecting intracranial hypertension. Npj Digit. Med. 2024, 7, 233. [Google Scholar] [CrossRef]
- Tran, S.; Smith, L.; Carter, S. Understanding Patient Perspectives on the Use of Gamification and Incentives in mHealth Apps to Improve Medication Adherence: Qualitative Study. JMIR MHealth UHealth 2024, 12, e50851. [Google Scholar] [CrossRef]
- Weidmann, A.E.; Sonnleitner-Heglmeier, A.; Dartsch, D.C. Effect of patient education videos on modifying medication-related health behaviours: A systematic review using the behaviour intervention functions. Patient Educ. Couns. 2023, 117, 107992. [Google Scholar] [CrossRef]
- Birru, E.; Ndayizigiye, M.; Wanje, G.; Marole, T.; Smith, P.D.; Koto, M.; McBain, R.; Hirschhorn, L.R.; Mokoena, M.; Michaelis, A.; et al. Healthcare workers’ views on decentralized primary health care management in Lesotho: A qualitative study. BMC Health Serv. Res. 2024, 24, 801. [Google Scholar] [CrossRef]
- Klassen, S.L.; Okello, E.; Ferrer, J.M.E.; Alizadeh, F.; Barango, P.; Chillo, P.; Chimalizeni, Y.; Dagnaw, W.W.; Eiselé, J.-L.; Eberly, L.; et al. Decentralization and Integration of Advanced Cardiac Care for the Worlds Poorest Billion Through the PEN-Plus Strategy for Severe Chronic Non-Communicable Disease. Glob. Heart 2024, 19, 33. [Google Scholar] [CrossRef]
- Akhtar, M.N.; Haleem, A.; Javaid, M. Scope of health care system in rural areas under Medical 4.0 environment. Intell. Pharm. 2023, 1, 217–223. [Google Scholar] [CrossRef]
- Niazi, S.K. The Dawn of In Vivo Gene Editing Era: A Revolution in the Making. Biologics 2023, 3, 253–295. [Google Scholar] [CrossRef]
- Kaupbayeva, B.; Tsoy, A.; Safarova (Yantsen), Y.; Nurmagambetova, A.; Murata, H.; Matyjaszewski, K.; Askarova, S. Unlocking Genome Editing: Advances and Obstacles in CRISPR/Cas Delivery Technologies. J. Funct. Biomater. 2024, 15, 324. [Google Scholar] [CrossRef]
- Cavazza, A.; Hendel, A.; Bak, R.O.; Rio, P.; Güell, M.; Lainšček, D.; Arechavala-Gomeza, V.; Peng, L.; Hapil, F.Z.; Harvey, J.; et al. Progress and harmonization of gene editing to treat human diseases: Proceeding of COST Action CA21113 GenE-HumDi. Mol. Ther. Nucleic Acids 2023, 34, 102066. [Google Scholar] [CrossRef]
- Anand, N.; Gorantla, V.R.; Chidambaram, S.B. The Role of Gut Dysbiosis in the Pathophysiology of Neuropsychiatric Disorders. Cells 2022, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Lv, L. Mechanistic insights into the role of probiotics in modulating immune cells in ulcerative colitis. Immun. Inflamm. Dis. 2023, 11, e1045. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Rao, T.; Wei, S.; Cheng, J.; Zhan, Y.; Lin, T.; Chen, J.; Zhong, X.; Jiang, Y.; Yang, S. Role of inflammatory cytokines and the gut microbiome in vascular dementia: Insights from Mendelian randomization analysis. Front. Microbiol. 2024, 15, 1398618. [Google Scholar] [CrossRef] [PubMed]
- Pansell, J.; Rudberg, P.C.; Friman, O.; Bell, M.; Cooray, C. Sex differences in the diagnostic value of optic nerve sheath diameter for assessing intracranial pressure. Sci. Rep. 2024, 14, 9553. [Google Scholar] [CrossRef]
- Wan, Y.; Holste, K.G.; Hua, Y.; Keep, R.F.; Xi, G. Brain edema formation and therapy after intracerebral hemorrhage. Neurobiol. Dis. 2023, 176, 105948. [Google Scholar] [CrossRef]
- Chrzanowski, S.; Batra, R. CRISPR-Based Gene Editing Techniques in Pediatric Neurological Disorders. Pediatr. Neurol. 2024, 153, 166–174. [Google Scholar] [CrossRef]
- Oh, S.; Jekal, J.; Liu, J.; Kim, J.; Park, J.-U.; Lee, T.; Jang, K.-I. Bioelectronic Implantable Devices for Physiological Signal Recording and Closed-Loop Neuromodulation. Adv. Funct. Mater. 2024, 34, 2403562. [Google Scholar] [CrossRef]
- Subica, A.M. CRISPR in Public Health: The Health Equity Implications and Role of Community in Gene-Editing Research and Applications. Am. J. Public Health 2023, 113, 874–882. [Google Scholar] [CrossRef]
- Kim, H.; Rigo, B.; Wong, G.; Lee, Y.J.; Yeo, W.-H. Advances in Wireless, Batteryless, Implantable Electronics for Real-Time, Continuous Physiological Monitoring. Nano-Micro Lett. 2023, 16, 52. [Google Scholar] [CrossRef]
- Peralta, G.; Sánchez-Santiago, B. Navigating the challenges of clinical trial professionals in the healthcare sector. Front. Med. 2024, 11, 1400585. [Google Scholar] [CrossRef]
- Liu, W.; Jia, L.; Xu, L.; Yang, F.; Cheng, H.; Li, H.; Hou, J.; Zhang, D.; Liu, Y. Idiopathic intracranial hypertension in patients with cerebral small vessel disease: A case report. Medicine 2023, 102, e32639. [Google Scholar] [CrossRef]
- Sulaimon, L.A.; Afolabi, L.O.; Adisa, R.A.; Ayankojo, A.G.; Afolabi, M.O.; Adewolu, A.M.; Wan, X. Pharmacological significance of MitoQ in ameliorating mitochondria-related diseases. Adv. Redox Res. 2022, 5, 100037. [Google Scholar] [CrossRef]
- Reel, P.S.; Reel, S.; van Kralingen, J.C.; Langton, K.; Lang, K.; Erlic, Z.; Larsen, C.K.; Amar, L.; Pamporaki, C.; Mulatero, P.; et al. Machine learning for classification of hypertension subtypes using multi-omics: A multi-centre, retrospective, data-driven study. eBioMedicine 2022, 84, 104276. [Google Scholar] [CrossRef]
- Katusic, Z.S.; d’Uscio, L.V.; He, T. Emerging Roles of Endothelial Nitric Oxide in Preservation of Cognitive Health. Stroke 2023, 54, 686–696. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, J.; Wang, W.; Lin, W.; Ahmed, W.; Duan, W.; Huang, S.; Zhu, Z.; Chen, L. The role of exosomes derived from stem cells in nerve regeneration: A contribution to neurological repair. Exp. Neurol. 2024, 380, 114882. [Google Scholar] [CrossRef] [PubMed]
- Lyu, J.; Wang, X.; Duan, Q.; Wang, W.; Li, R.; Wang, X.; Lou, X. Progress in magnetic resonance imaging of the glymphatic system. Magn. Reson. Lett. 2024, 4, 200154. [Google Scholar] [CrossRef]
- Hirai, T.; Yasuda, S.; Umezawa, A.; Sato, Y. Country-specific regulation and international standardization of cell-based therapeutic products derived from pluripotent stem cells. Stem Cell Rep. 2023, 18, 1573–1591. [Google Scholar] [CrossRef]
- Gareev, I.; Beylerli, O.; Ilyasova, T.; Mashkin, A.; Shi, H. The use of bioinformatic analysis to study intracerebral hemorrhage. Brain Hemorrhages 2024, 5, 188–196. [Google Scholar] [CrossRef]
- Ma, L.; Hu, X.; Song, L.; Chen, X.; Ouyang, M.; Billot, L.; Li, Q.; Malavera, A.; Li, X.; Muñoz-Venturelli, P.; et al. The third Intensive Care Bundle with Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT3): An international, stepped wedge cluster randomised controlled trial. Lancet 2023, 402, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.P.; Kasa, V.P.; Dubey, B.K.; Sen, R.; Sarmah, A.K. Synthesis and commercialization of bioplastics: Organic waste as a sustainable feedstock. Sci. Total Environ. 2023, 904, 167243. [Google Scholar] [CrossRef]
- Tilala, M.H.; Chenchala, P.K.; Choppadandi, A.; Kaur, J.; Naguri, S.; Saoji, R.; Devaguptapu, B. Ethical Considerations in the Use of Artificial Intelligence and Machine Learning in Health Care: A Comprehensive Review. Cureus 2024, 16, e62443. [Google Scholar] [CrossRef]
- Nojadeh, J.N.; Eryilmaz, N.S.B.; Ergüder, B.I. CRISPR/Cas9 genome editing for neurodegenerative diseases. EXCLI J. 2023, 22, 567–582. [Google Scholar] [CrossRef]
- Yiangou, A.; Weaver, S.R.C.; Thaller, M.; Mitchell, J.L.; Lyons, H.S.; Tsermoulas, G.; Mollan, S.P.; Lucas, S.J.E.; Sinclair, A.J. The Impact of Valsalva Manoeuvres and Exercise on Intracranial Pressure and Cerebrovascular Dynamics in Idiopathic Intracranial Hypertension. Neuro-Ophthalmology 2023, 48, 122–133. [Google Scholar] [CrossRef]
- Abeltino, A.; Riente, A.; Bianchetti, G.; Serantoni, C.; De Spirito, M.; Capezzone, S.; Esposito, R.; Maulucci, G. Digital applications for diet monitoring, planning, and precision nutrition for citizens and professionals: A state of the art. Nutr. Rev. 2024, 83, e574–e601. [Google Scholar] [CrossRef]
- Naamati-Schneider, L. Enhancing AI competence in health management: Students’ experiences with ChatGPT as a learning Tool. BMC Med. Educ. 2024, 24, 598. [Google Scholar] [CrossRef]
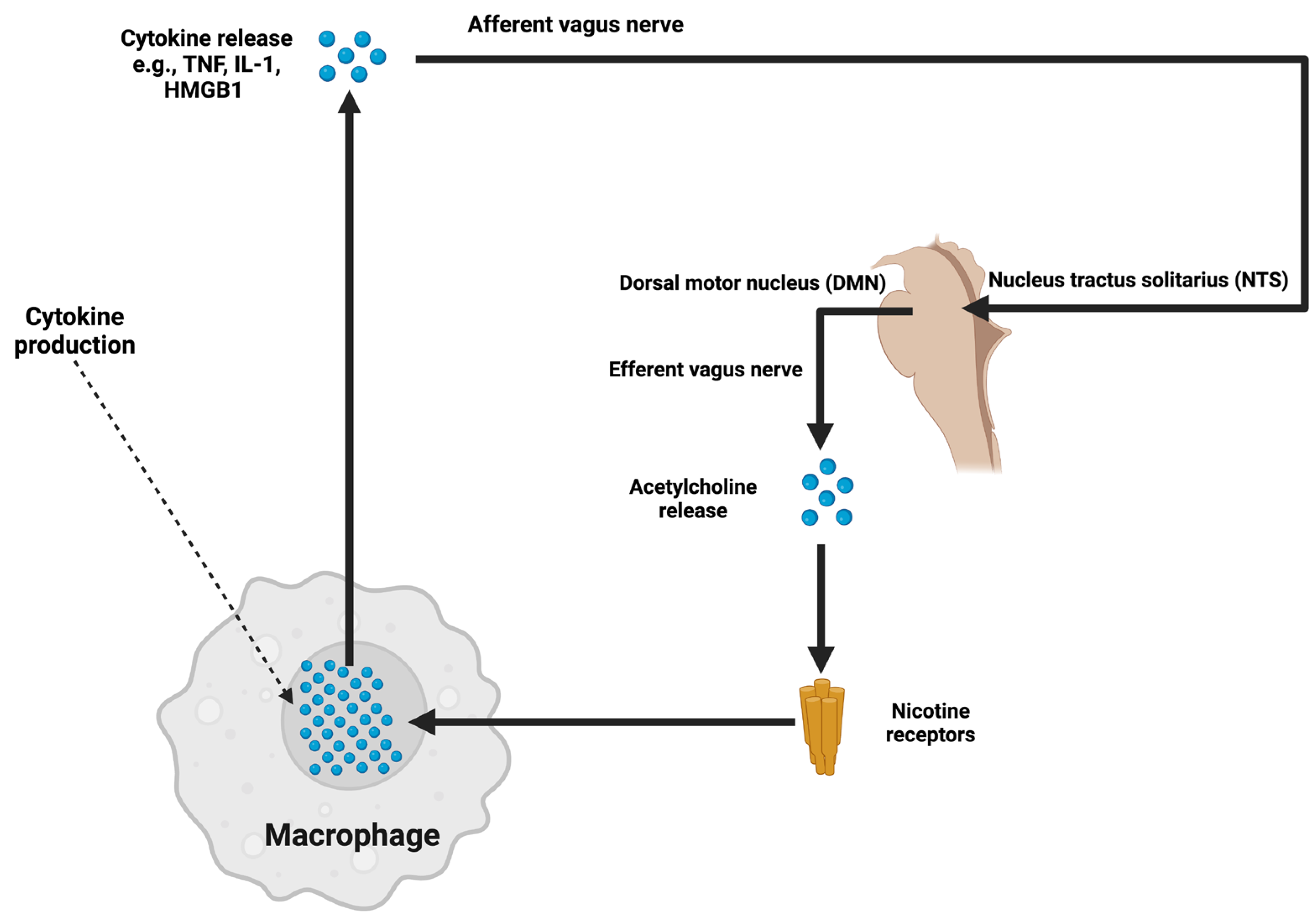


{kind=link}
{kind=link}
| Reference | Imaging/Monitoring Modality | Patient Population | Endpoints Measured | Outcome | Limitations |
|---|---|---|---|---|---|
| Glymphatic Mapping with DCE-MRI (2023) [142] | Dynamic contrast-enhanced MRI | IIH, glymphatic dysfunction | ICP variation, glymphatic flow dynamics | 80% diagnostic accuracy improvement | Small sample size |
| AI-Augmented ONSD Ultrasonography (2023) [143] | AI-integrated optic nerve sheath diameter | Acute TBI, IIH | ICP correlation, diagnostic precision | 97% diagnostic accuracy | Limited generalizability |
| 4D Flow MRI and Glymphatic–Vascular Coupling (2024) [97] | 4D Flow MRI | Chronic ICP, venous stenosis | Venous outflow, ICP variability | Identified 35% more venous sinus collapsibility cases | Expensive equipment |
| Smart Helmets for ICP Detection (2020) [144] | Wearable transcranial Doppler sensors | Emergency care patients | Time-to-diagnosis, ICP trends | Reduced diagnostic time by 40% in emergencies | Limited chronic ICP data |
| Hybrid Imaging: PET/MRI (2021) [145] | PET and MRI integration | IIH with vascular anomalies | Metabolic markers, BBB integrity | Microglial activation detected in 88% of IIH patients | Small, single-center study |
| Biophotonic ICP Sensors (2022) [146] | Biophotonic nanosensors | IIH, refractory ICP | ICP sensitivity | Detected nocturnal surges in 92% | High cost, early-phase trial |
| Transcranial Doppler in Rural Care (2022) [147] | Portable transcranial Doppler (TCD) | Low-resource trauma patients | Accessibility, diagnostic accuracy | Increased ICP detection by 60% in resource-limited settings | Non-comparative design |
| Ocular MRI Elastography (2024) [148] | MRI elastography | IIH, chronic ICP | Optic nerve compliance, ICP trends | Enhanced optic nerve-related ICP diagnostics | Time-consuming imaging process |
| Miniaturized ICP Monitors (2023) [149] | Wearable nanosensors | Chronic ICP | Real-time ICP tracking, usability | Hospital visits reduced by 25% | Long-term adherence unknown |
| AI-Coupled Retinal Scanning (2024) [150] | Retinal scanning with AI algorithms | Chronic IIH patients | Papilledema severity, ICP correlation | Reliable ICP estimation without invasive monitoring | Limited availability of retinal scanners |
| QSM-Guided Venous Hypertension Study (2024) [151] | Quantitative susceptibility mapping | IIH, venous stenosis | Venous congestion markers | High correlation between QSM and venous ICP trends | Validation in diverse cohorts needed |
| AI-Driven 4D Ultrasound Diagnostics (2024) [152] | AI-enhanced ultrasonography | IIH, emergency trauma | Real-time ICP dynamics | Improved early ICP detection, reduced intervention time by 30% | No long-term patient outcome data |
| Portable ICP Sensors in LMICs (2024) [153] | Low-cost, portable ICP sensors | Rural trauma care | Accessibility, diagnostic efficiency | Detected 80% of acute ICP elevation cases | Durability in tropical climates is questionable |
| Vascular Flow with Ultrasonic Imaging (2022) [154] | Handheld ultrasonic imaging devices | Chronic venous stenosis | Vascular flow markers | Identified venous hypertension in 90% of stenosis patients | Limited flow resolution |
| CRISP-Aided MRI Analysis (2023) [155] | CRISP software-enhanced MRI | IIH with glymphatic dysfunction | Glymphatic efficiency | Visualized glymphatic disruption 60% better than traditional imaging | Requires computational infrastructure |
| AI-Augmented Phase-Contrast Imaging (2024) [156] | Phase-contrast MRI | Hydrocephalus patients | CSF flow dynamics | Higher sensitivity to CSF blockages | Costly MRI enhancements |
| Multi-Spectral ICP Monitoring (2022) [157] | Multi-spectral optics | Chronic IIH | Light wave changes due to ICP surges | Accurate ICP monitoring in 80% of participants | Dependent on robust calibration systems |
| Venous Compliance Imaging (2022) [158] | MRI compliance mapping | Venous stenosis | Wall stiffness, ICP correlation | High sensitivity for venous wall abnormalities | Small-scale study |
| Glymphatic Function with Contrast MRI (2023) [159] | Contrast-enhanced MRI | IIH, BBB impairment | CSF flow markers | Enhanced glymphatic markers provided actionable ICP data | High imaging costs |
| Optic Nerve-Specific Imaging (2024) [160] | High-res optic nerve imaging | IIH with optic involvement | Optic nerve and ICP correlation | 30% improvement in optic nerve-related ICP diagnosis | Limited global availability |
| Wearable Spectroscopic Devices (2024) [161] | Non-invasive spectroscopic ICP monitor | IIH, chronic ICP | ICP trends, compliance usability | High adherence rates for daily monitoring | Limited sensitivity in highly mobile patients |
| AI-Driven Shunt Monitoring (2024) [162] | AI-monitored shunt function | Hydrocephalus, IIH | ICP trends | Significant improvement in shunt-related complication detection | Expensive to integrate |
| Bioimpedance Monitoring Trials (2023) [163] | Bioimpedance nanosensors | IIH, TBI | ICP-related fluid volume dynamics | Promising early results for tracking subclinical ICP surges | Limited commercial deployment |
| Digital ICP Decision Aids (2023) [164] | Digital platforms with predictive tools | IIH patients, rural clinics | Diagnostic reliability | AI-aided diagnostics reduced misdiagnosis rates by 20% | Validation across global clinics needed |
| Modular ICP Systems Study (2021) [165] | Modular, wearable ICP monitors | IIH, venous stenosis | ICP tracking, user feedback | High usability and adherence rates among outpatient participants | Early-stage development |
| Reference | Drug/Class | Target Pathway | Population Studied | Primary Outcome | Adverse Events |
|---|---|---|---|---|---|
| AQP4 Modulator Trial (2023) [217] | AQP4 upregulators (Vorinostat) | Glymphatic clearance | IIH, glymphatic dysfunction | Reduced ICP surges by 40% | Mild fatigue in 10% |
| Everolimus in IIH (2022) [218] | mTOR inhibitors | CSF production, homeostasis | Obese IIH patients | 35% decrease in CSF overproduction | GI symptoms in 15% |
| Anti-VEGF Therapy for Venous ICP (2023) [219] | Bevacizumab | BBB stabilization | IIH with venous congestion | Improved BBB integrity by 30% | Thrombosis in 5% |
| SGLT2 Inhibitors in ICH (2023) [220] | Empagliflozin | Astrocytic metabolism | Obese IIH | 25% improvement in glymphatic clearance | No significant events |
| Pirfenidone for Fibrosis (2024) [221] | Anti-fibrotic agents | Preventing shunt occlusions | Refractory hydrocephalus | Reduced shunt blockages by 30% | Nausea in 15% |
| HDAC Inhibitors for Glymphatic Function (2021) [222] | Class I HDAC inhibitors | Epigenetic modulation | Chronic ICP, IIH patients | Increased glymphatic clearance by 50% | Mild leukopenia in 8% |
| MitoQ Neuroprotection (2021) [223] | Mitochondrial antioxidants | Oxidative stress | Chronic ICP | Reduced neuroinflammation by 25% | Minimal side effects |
| Combination Therapy in Hydrocephalus (2023) [224] | Acetazolamide + Topiramate | CSF secretion | Chronic hydrocephalus | Sustained ICP reduction for 12 months | Cognitive blunting in 5% |
| Statins in Venous Tone Modulation (2023) [225] | Rosuvastatin | Endothelial function | Venous sinus stenosis | Reduced ICP fluctuations by 15% | None reported |
| Topiramate Neuroprotection Trial (2023) [226] | Topiramate | Ion channel modulation | IIH with vision symptoms | Reduced headache frequency by 35% | Dizziness in 8% |
| Aquaporin Therapy Trial (2023) [227] | Aquaporin-targeted small molecules | Glymphatic clearance | IIH, glymphatic dysfunction | Enhanced CSF dynamics in 70% | Early-stage results |
| Anti-Inflammatory Drug Study (2023) [228] | p38 MAPK inhibitors | Neuroinflammation suppression | Chronic ICP | Decreased pro-inflammatory cytokines (IL-6, TNF-α) | Fatigue in 12% |
| Progesterone Modulation in IIH (2024) [229] | Progesterone analogs | CSF absorption | Obese IIH patients | Improved vision in 60%, reduced ICP by 20% | Limited by sample size |
| Venous Stenting with Drugs (2021) [230] | Anti-thrombotics | Venous stenosis and flow | IIH, venous sinus stenosis | Combined stenting and anti-thrombotics reduced ICP by 30% | Bleeding risk in 5% |
| Fibrinolytic Therapy in ICP Control (2024) [231] | Plasminogen activators | Venous thrombi dissolution | Acute IIH | 80% efficacy in reducing venous sinus occlusion | Mild bleeding in 10% |
| Hypothermia Combined with Anti-Edema Drugs (2022) [232] | Osmotic agents + cooling | Cerebral edema reduction | TBI patients with ICP | ICP reduction by 50%, improved survival rates | Hypothermia-related infection risk |
| Beta-Blockers for ICP Modulation (2024) [233] | Beta-blockers | Autoregulation improvement | IIH | Reduced ICP by 15% | Bradycardia in 10% |
| CRISPR-Edited Genetic Targets (2021) [234] | Gene-edited aquaporin pathways | Glymphatic-targeted clearance | IIH, hydrocephalus | Reduced glymphatic disruptions by 40% | Safety still under evaluation |
| NMDA Antagonists for Neuroprotection (2024) [235] | NMDA receptor antagonists | Excitotoxicity mitigation | ICP spikes | Improved cognitive recovery by 20% | Early-phase trial |
| Cannabinoids in ICP Control (2024) [236] | Cannabinoid receptor agonists | Anti-inflammatory pathways | Chronic IIH patients | Reduced headache frequency by 30% | Mild sedation reported |
| Spironolactone in IIH (2023) [237] | Mineralocorticoid receptor antagonists | Hormonal modulation | IIH, PCOS patients | Reduced ICP surges during menstrual cycle | Few side effects reported |
| Biofilm-Resistant Shunt Therapy (2023) [238] | Antibiotic-embedded shunts | Shunt durability | Pediatric hydrocephalus | Reduced shunt infection rates by 50% | No adverse effects noted |
| Epigenetic Drugs in ICP Regulation (2022) [239] | DNA methylation modifiers | CSF flow | IIH, obesity-related ICP | Enhanced therapeutic response in 40% | Transient fatigue |
| SGLT2 and Anti-inflammatory Combination (2023) [240] | Empagliflozin + TNF-α blockers | Glymphatic flow and inflammation | Chronic ICP patients | Synergistic improvement in ICP and cytokine reduction | Early clinical phase |
| Reference | Technology/Innovation | Population Studied | Outcome Measured | Results | Challenges/Limitations |
|---|---|---|---|---|---|
| CRISPR-AQP4 Modulation (2024) [297] | CRISPR gene editing | IIH, refractory hydrocephalus | Glymphatic flow improvement | Enhanced glymphatic function in 70% of patients | Safety monitoring needed |
| Closed-Loop AI Shunts (2023) [298] | Adaptive CSF drainage systems | Hydrocephalus patients | Real-time ICP adjustment, reliability | Reduced over-drainage complications by 30% | High device costs |
| Neural Progenitor Exosomes (2023) [299] | Stem cell-derived exosomes | Chronic ICP with neuroinflammation | BBB repair | Significant BBB repair in 60% of participants | High production costs |
| Biodegradable ICP Hydrogels (2024) [300] | Steroid-loaded hydrogels | Refractory ICP patients | Sustained ICP reduction | Sustained ICP control for 6 months | Repeat applications needed |
| Vagus Nerve Stimulation (2024) [301] | Non-invasive bioelectronics | IIH patients | Cerebrovascular tone improvement | Improved ICP control in 80% | Poor adherence to regimen |
| Nanorobots in CSF Therapy (2024) [302] | Molecular nanorobots | Refractory IIH | Targeted drug delivery | Reduced inflammation at focal sites | Prototype stage |
| Smart Helmets with Nanosensors (2022) [184] | Wearable ICP monitors | IIH, emergency use | ICP monitoring | Reduced diagnostic latency | High manufacturing costs |
| AI-Guided Therapeutic Robotics (2024) [207] | AI-integrated surgical robotics | Chronic hydrocephalus | Shunt placement precision | Improved accuracy by 20% | Scalability unclear |
| Focused Ultrasound with Microbubbles (2023) [303] | Ultrasound-assisted CSF clearance | IIH, hydrocephalus | Glymphatic flow enhancement | 25% ICP reduction in pilot trial | Limited operator availability |
| Gene-Integrated Wearables (2022) [304] | Wearables with epigenetic sensors | Chronic ICP patients | Real-time genetic variation tracking | Improved personalized ICP management | High complexity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Șerban, M.; Toader, C.; Covache-Busuioc, R.-A. The Collapse of Brain Clearance: Glymphatic-Venous Failure, Aquaporin-4 Breakdown, and AI-Empowered Precision Neurotherapeutics in Intracranial Hypertension. Int. J. Mol. Sci. 2025, 26, 7223. https://doi.org/10.3390/ijms26157223
Șerban M, Toader C, Covache-Busuioc R-A. The Collapse of Brain Clearance: Glymphatic-Venous Failure, Aquaporin-4 Breakdown, and AI-Empowered Precision Neurotherapeutics in Intracranial Hypertension. International Journal of Molecular Sciences. 2025; 26(15):7223. https://doi.org/10.3390/ijms26157223
Chicago/Turabian StyleȘerban, Matei, Corneliu Toader, and Răzvan-Adrian Covache-Busuioc. 2025. "The Collapse of Brain Clearance: Glymphatic-Venous Failure, Aquaporin-4 Breakdown, and AI-Empowered Precision Neurotherapeutics in Intracranial Hypertension" International Journal of Molecular Sciences 26, no. 15: 7223. https://doi.org/10.3390/ijms26157223
APA StyleȘerban, M., Toader, C., & Covache-Busuioc, R.-A. (2025). The Collapse of Brain Clearance: Glymphatic-Venous Failure, Aquaporin-4 Breakdown, and AI-Empowered Precision Neurotherapeutics in Intracranial Hypertension. International Journal of Molecular Sciences, 26(15), 7223. https://doi.org/10.3390/ijms26157223