
Hemodialysis Intensifies NLRP3 Inflammasome Expression and Oxidative Stress in Patients with Chronic Kidney Disease

 , , and
, , and 
Abstract
1. Introduction
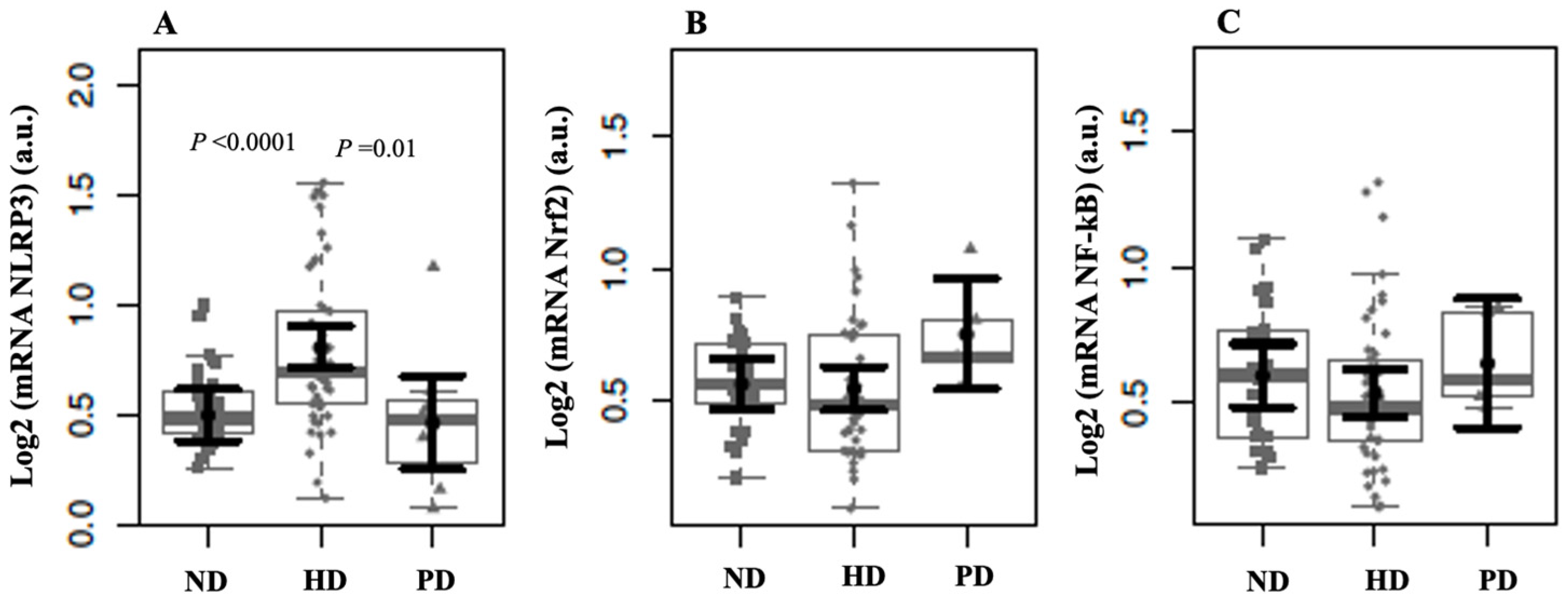
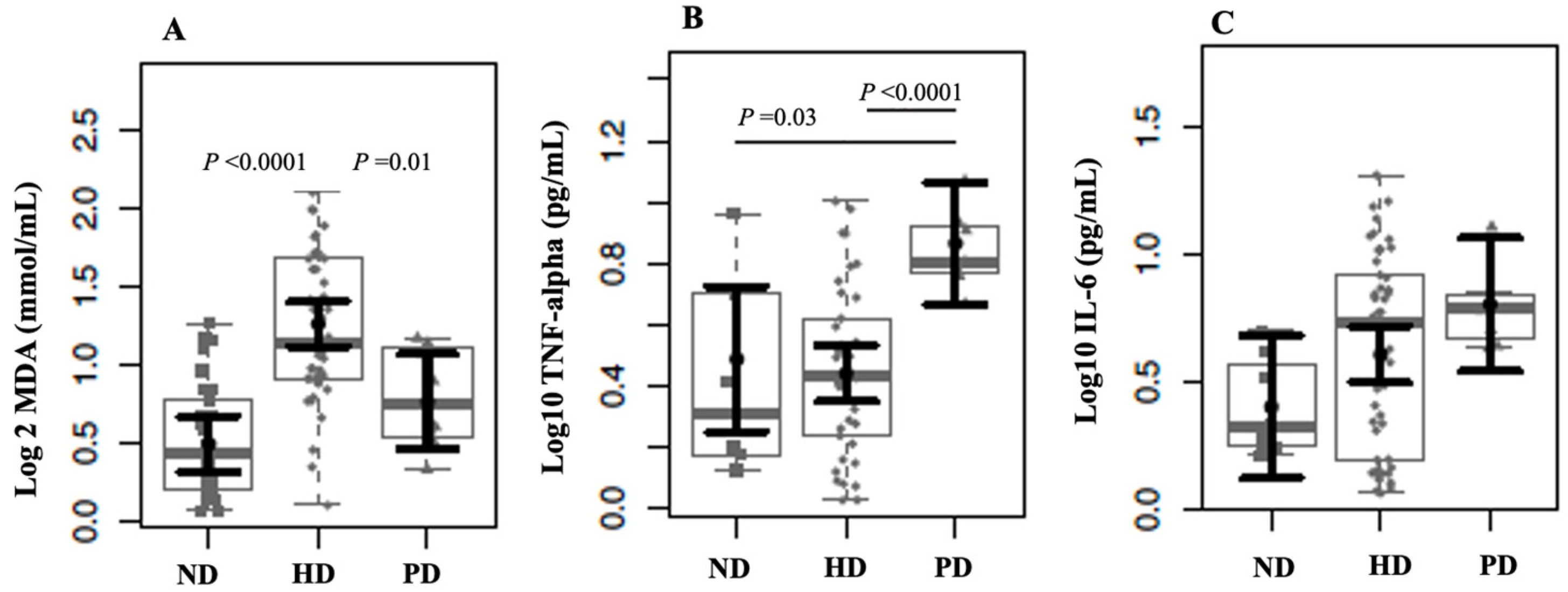
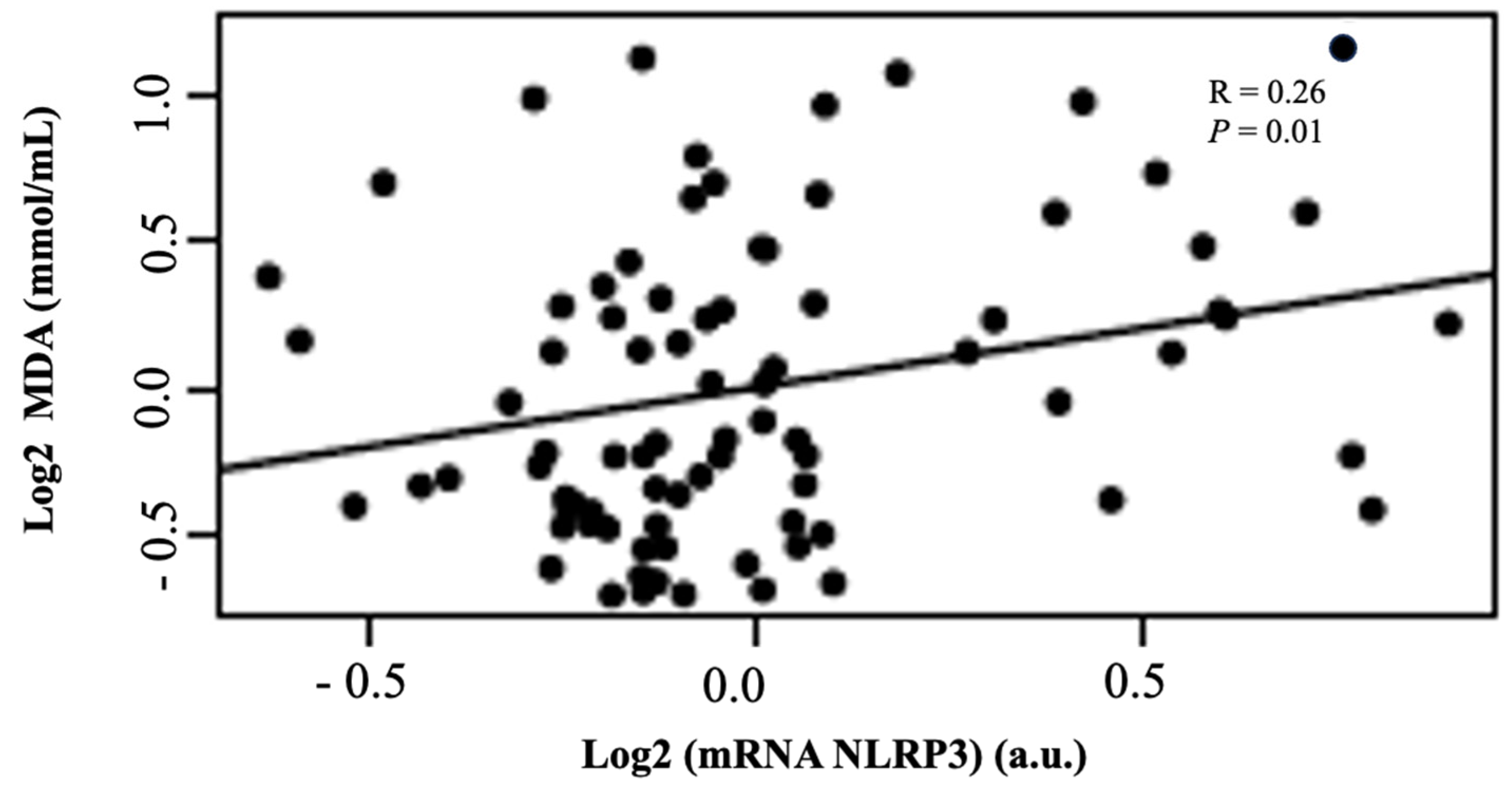
2. Results
3. Discussion
Limitations
4. Materials and Methods
4.1. Study Design and Patients
4.2. Analytic Procedures and Sample Processing
4.3. Quantitative Real-Time PCR Analyses
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CKD | chronic kidney disease |
| ND | non-dialysis |
| HD | hemodialysis |
| PD | peritoneal dialysis |
| MDA | malondialdehyde |
| NBD | nucleotide-binding domain |
| LRRs | leucine-rich repeats |
| GSDMD | gasdermin D |
| PRRs | pattern recognition receptors |
| PAMPs | pathogen-associated molecular patterns |
| DAMPs | damage-associated molecular patterns |
| GFR | glomerular filtration rate |
| RRT | renal replacement therapy |
| NLRP3 | nod-like receptor pyrin domain containing |
| NF-κB | nuclear factor kappa-B |
| Nrf2 | nuclear factor erythroid 2-related factor 2 |
| ROS | reactive oxygen species |
| TBARSs | thiobarbituric acid-reactive substances |
References
- Broz, P.; Dixit, V.M. Inflammasomes: Mechanism of assembly, regulation and signalling. Nat. Rev. Immunol. 2016, 16, 407–420. [Google Scholar] [CrossRef]
- Pandey, A.; Li, Z.; Gautam, M.; Ghosh, A.; Man, S.M. Molecular mechanisms of emerging inflammasome complexes and their activation and signaling in inflammation and pyroptosis. Immunol. Rev. 2025, 329, e13406. [Google Scholar] [CrossRef] [PubMed]
- Swanson, K.V.; Deng, M.; Ting, J.P.Y. The NLRP3 inflammasome: Molecular activation and regulation to therapeutics. Nat. Rev. Immunol. 2019, 19, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Gaidt, M.M.; Hornung, V. The NLRP3 Inflammasome Renders Cell Death Pro-inflammatory. J. Mol. Biol. 2018, 430, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Akbal, A.; Dernst, A.; Lovotti, M.; Mangan, M.S.J.; McManus, R.M.; Latz, E. How location and cellular signaling combine to activate the NLRP3 inflammasome. Cell. Mol. Immunol. 2022, 19, 1201–1214. [Google Scholar] [CrossRef]
- Miao, N.; Yin, F.; Xie, H.; Wang, Y.; Xu, Y.; Shen, Y.; Xu, D.; Yin, J.; Wang, B.; Zhou, Z.; et al. The cleavage of gasdermin D by caspase-11 promotes tubular epithelial cell pyroptosis and urinary IL-18 excretion in acute kidney injury. Kidney Int. 2019, 96, 1105–1120. [Google Scholar] [CrossRef]
- Evans, M.; Lewis, R.D.; Morgan, A.R.; Whyte, M.B.; Hanif, W.; Bain, S.C.; Davies, S.; Dashora, U.; Yousef, Z.; Patel, D.C.; et al. A Narrative Review of Chronic Kidney Disease in Clinical Practice: Current Challenges and Future Perspectives. Adv. Ther. 2022, 39, 33–43. [Google Scholar] [CrossRef]
- Rispoli, R.M.; Popolo, A.; de Fabrizio, V.; Bianca, R.D.d.V.; Autore, G.; Dalli, J.; Marzocco, S. Targeting Inflammatory Imbalance in Chronic Kidney Disease: Focus on Anti-Inflammatory and Resolution Mediators. Int. J. Mol. Sci. 2025, 26, 3072. [Google Scholar] [CrossRef]
- Huang, G.; Zhang, Y.; Zhang, Y.; Ma, Y. Chronic kidney disease and NLRP3 inflammasome: Pathogenesis, development and targeted therapeutic strategies. Biochem. Biophys. Rep. 2022, 33, 101417. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Y.; Dong, Y.; Chen, Z.; Eckols, T.K.; Kasembeli, M.M.; Tweardy, D.J.; Mitch, W.E. Pharmacokinetics and pharmacodynamics of TTI-101, a STAT3 inhibitor that blocks muscle proteolysis in rats with chronic kidney disease. Am. J. Physiol. Renal Physiol. 2020, 319, F84–F92. [Google Scholar] [CrossRef]
- Leal, V.O.; Saldanha, J.F.; Stockler-Pinto, M.B.; Cardozo, L.F.; Santos, F.R.; Albuquerque, A.S.; Leite, M., Jr.; Mafra, D. NRF2 and NF-κB mRNA expression in chronic kidney disease: A focus on nondialysis patients. Int. Urol. Nephrol. 2015, 47, 1985–1991. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, A.; Bigdeli, R.; Shahnazari, M.; Oruji, F.; Fattahi, S.; Panahnejad, E.; Ghadri, A.; Movahedi-Asl, E.; Mahdavi-Ourtakand, M.; Asgary, V.; et al. Evaluation of Inflammasome Activation in Peripheral Blood Mononuclear Cells of Hemodialysis Treated Patients with Glomerulonephritis. Iran. J. Pharm Res. 2021, 20, 609–617. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hishida, E.; Ito, H.; Komada, T.; Karasawa, T.; Kimura, H.; Watanabe, S.; Kamata, R.; Aizawa, E.; Kasahara, T.; Morishita, Y.; et al. Crucial Role of NLRP3 Inflammasome in the Development of Peritoneal Dialysis-related Peritoneal Fibrosis. Sci. Rep. 2019, 9, 10363. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hautem, N.; Morelle, J.; Sow, A.; Corbet, C.; Feron, O.; Goffin, E.; Huaux, F.; Devuyst, O. The NLRP3 Inflammasome Has a Critical Role in Peritoneal Dialysis-Related Peritonitis. J. Am. Soc. Nephrol. 2017, 28, 2038–2052. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Granata, S.; Masola, V.; Zoratti, E.; Scupoli, M.T.; Baruzzi, A.; Messa, M.; Sallustio, F.; Gesualdo, L.; Lupo, A.; Zaza, G. NLRP3 inflammasome activation in dialyzed chronic kidney disease patients. PLoS ONE 2015, 10, e0122272. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sahib, A.; Choudhury, C.; Wani, I.A.; Wani, M.M. Evaluation of Inflammatory Status in Chronic Kidney Disease Patients and a Comparison Between Hemodialysis and Peritoneal Dialysis Patients. Cureus 2024, 16, e69443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, H.; Zhang, X.; Liao, N.; Mi, L.; Peng, Y.; Liu, B.; Zhang, S.; Wen, F. Enhanced Expression of NLRP3 Inflammasome-Related Inflammation in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2018, 59, 978–985. [Google Scholar] [CrossRef]
- Ekiner, S.A.; Gęgotek, A.; Skrzydlewska, E. Inflammasome activity regulation by PUFA metabolites. Front. Immunol. 2024, 15, 1452749. [Google Scholar] [CrossRef]
- Cao, W.; Zeng, Y.; Su, Y.; Gong, H.; He, J.; Liu, Y.; Li, C. The involvement of oxidative stress and the TLR4/NF-κB/NLRP3 pathway in acute lung injury induced by high-altitude hypoxia. Immunobiology 2024, 229, 152809. [Google Scholar] [CrossRef]
- Capusa, C.; Stoian, I.; Rus, E.; Lixandru, D.; Barbulescu, C.; Mircescu, G. Does dialysis modality influence the oxidative stress of uremic patients? Kidney Blood Press. Res. 2012, 35, 220–225. [Google Scholar] [CrossRef]
- Ajala, M.O.; Ogunro, P.S.; Odun, A. Effect of hemodialysis on total antioxidant status of chronic renal failure patients in government hospitals in Lagos Nigeria. Niger. J. Clin. Pract. 2011, 14, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Dounousi, E.; Mertens, P.R. Oxidative Stress in Hemodialysis Patients: A Review of the Literature. Oxid. Med. Cell. Longev. 2017, 2017, 3081856. [Google Scholar] [CrossRef] [PubMed]
- Tbahriti, H.F.; Kaddous, A.; Bouchenak, M.; Mekki, K. Effect of different stages of chronic kidney disease and renal replacement therapies on oxidant-antioxidant balance in uremic patients. Biochem. Res. Int. 2013, 2013, 358985. [Google Scholar] [CrossRef] [PubMed]
- Vida, C.; Oliva, C.; Yuste, C.; Ceprián, N.; Caro, P.J.; Valera, G.; de Pablos, I.G.; Morales, E.; Carracedo, J. Oxidative Stress in Patients with Advanced CKD and Renal Replacement Therapy: The Key Role of Peripheral Blood Leukocytes. Antioxidants 2021, 10, 1155. [Google Scholar] [CrossRef]
- Chermut, T.R.; Fonseca, L.; Figueiredo, N.; Leal, V.d.O.; Borges, N.A.; Cardozo, L.F.; Correa Leite, P.E.; Alvarenga, L.; Regis, B.; Delgado, A.; et al. Effects of propolis on inflammation markers in patients undergoing hemodialysis: A randomized, double-blind controlled clinical trial. Complement. Ther. Clin. Pract. 2023, 51, 101732. [Google Scholar] [CrossRef] [PubMed]
- Reis, D.C.M.V.; Alvarenga, L.; Cardozo, L.F.M.F.; Baptista, B.G.; Fanton, S.; Paiva, B.R.; Ribeiro-Alves, M.; Fortunato, R.S.; Vasconcelos, A.L.; Nakao, L.S.; et al. Can curcumin supplementation break the vicious cycle of inflammation, oxidative stress, and uremia in patients undergoing peritoneal dialysis? Clin. Nutr. ESPEN 2024, 59, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for Lipid Peroxides in Animal Tissues by Thiobarbituric Acid Reaction. Anal. Biochem. 1979, 95, 351–358. [Google Scholar] [CrossRef]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameters | ND (N = 32) | HD (N = 50) | PD (N = 8) | p Values |
|---|---|---|---|---|
| Sex (male/female) | 14/18 | 20/30 | 5/3 | 0.490 |
| Age (years) | 63 (11.2) | 48.5 (16.5) | 56.5 (8.5) | 0.000 |
| Time on dialysis (months) | - | 60.5 (50) | 40.5 (41.2) | 0.187 |
| eGFR (mL/min/1.72 m2) | 43.5 (22.0) | - | - | - |
| BMI (kg/m2) | 29.5 (10.0) | 24.2 (4.9) | 28.8 (2.6) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, M.; Cardozo, L.F.M.F.; Coutinho-Wolino, K.S.; Ribeiro-Alves, M.; Mafra, D. Hemodialysis Intensifies NLRP3 Inflammasome Expression and Oxidative Stress in Patients with Chronic Kidney Disease. Int. J. Mol. Sci. 2025, 26, 6933. https://doi.org/10.3390/ijms26146933
Ribeiro M, Cardozo LFMF, Coutinho-Wolino KS, Ribeiro-Alves M, Mafra D. Hemodialysis Intensifies NLRP3 Inflammasome Expression and Oxidative Stress in Patients with Chronic Kidney Disease. International Journal of Molecular Sciences. 2025; 26(14):6933. https://doi.org/10.3390/ijms26146933
Chicago/Turabian StyleRibeiro, Marcia, Ludmila F. M. F. Cardozo, Karen Salve Coutinho-Wolino, Marcelo Ribeiro-Alves, and Denise Mafra. 2025. "Hemodialysis Intensifies NLRP3 Inflammasome Expression and Oxidative Stress in Patients with Chronic Kidney Disease" International Journal of Molecular Sciences 26, no. 14: 6933. https://doi.org/10.3390/ijms26146933
APA StyleRibeiro, M., Cardozo, L. F. M. F., Coutinho-Wolino, K. S., Ribeiro-Alves, M., & Mafra, D. (2025). Hemodialysis Intensifies NLRP3 Inflammasome Expression and Oxidative Stress in Patients with Chronic Kidney Disease. International Journal of Molecular Sciences, 26(14), 6933. https://doi.org/10.3390/ijms26146933