
Effect of Low-Level Laser Therapy on Periodontal Host Cells and a Seven-Species Periodontitis Model Biofilm

 , , and
, , and
Abstract
1. Introduction
2. Results
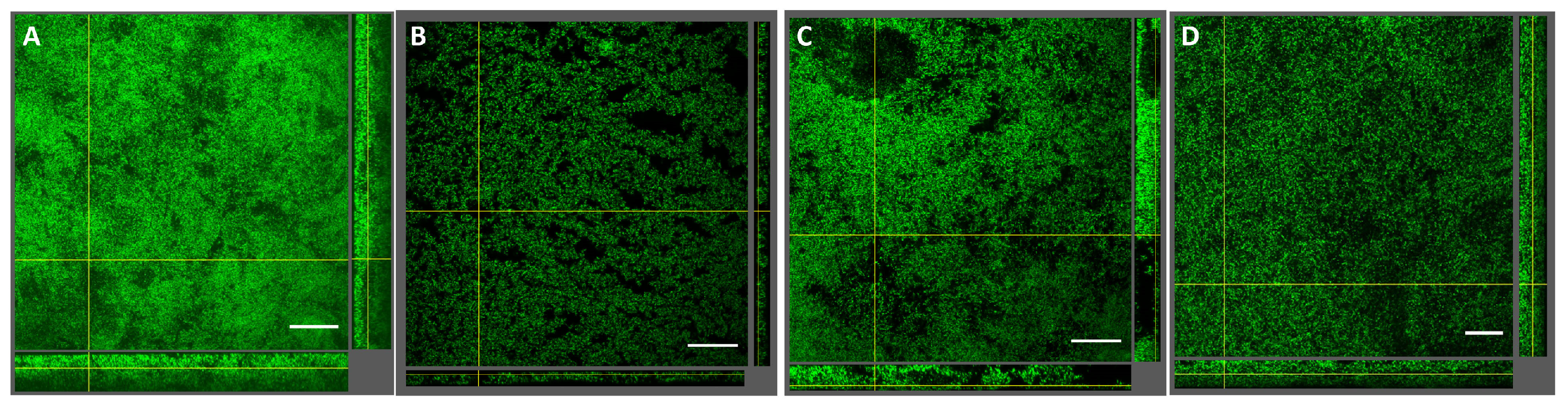
2.1. Effect of LLLT on Seven-Species Biofilms
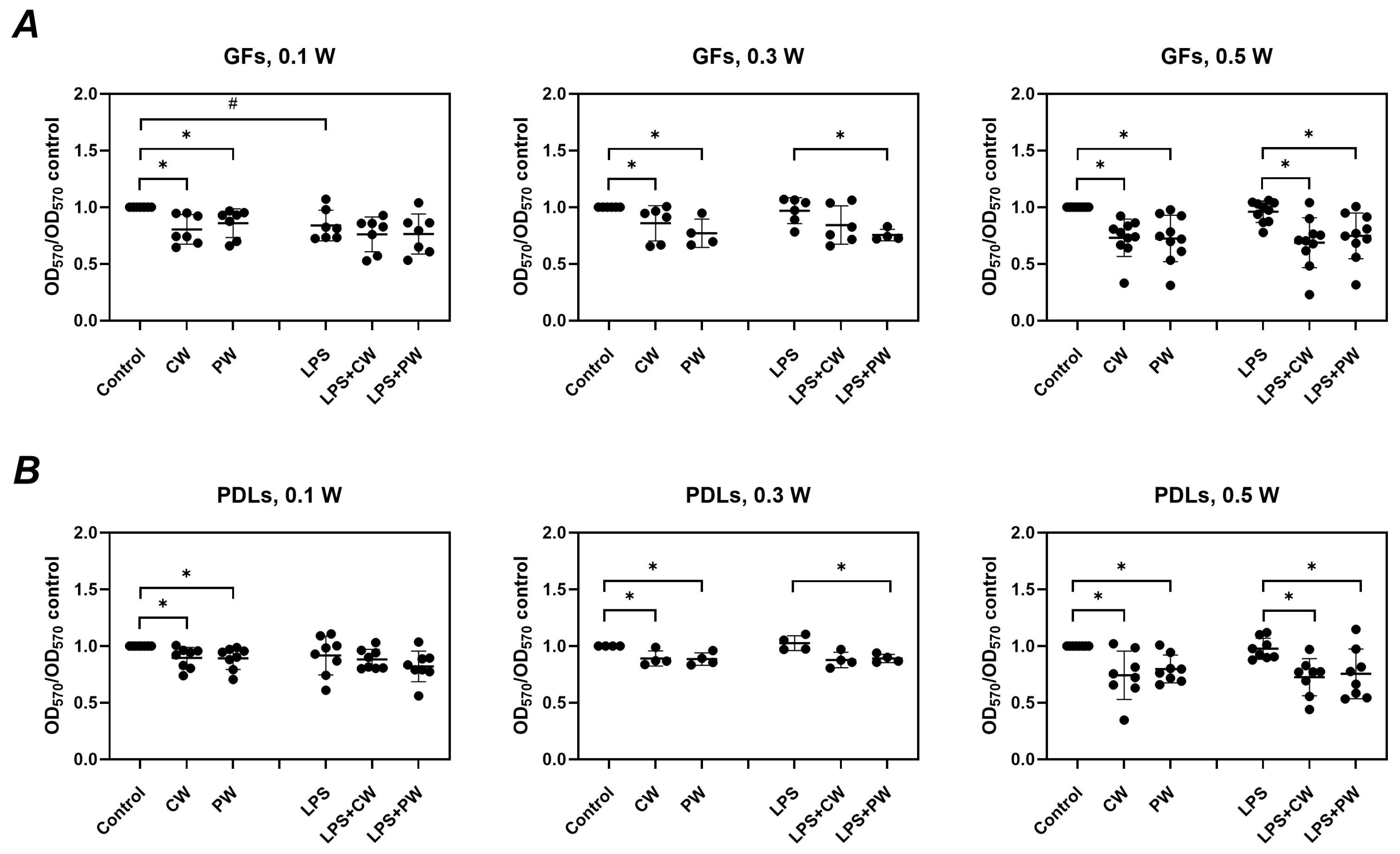
2.2. Effect of LLLT on Gingival Fibroblasts and Periodontal Ligament Cells
2.2.1. Cell Viability
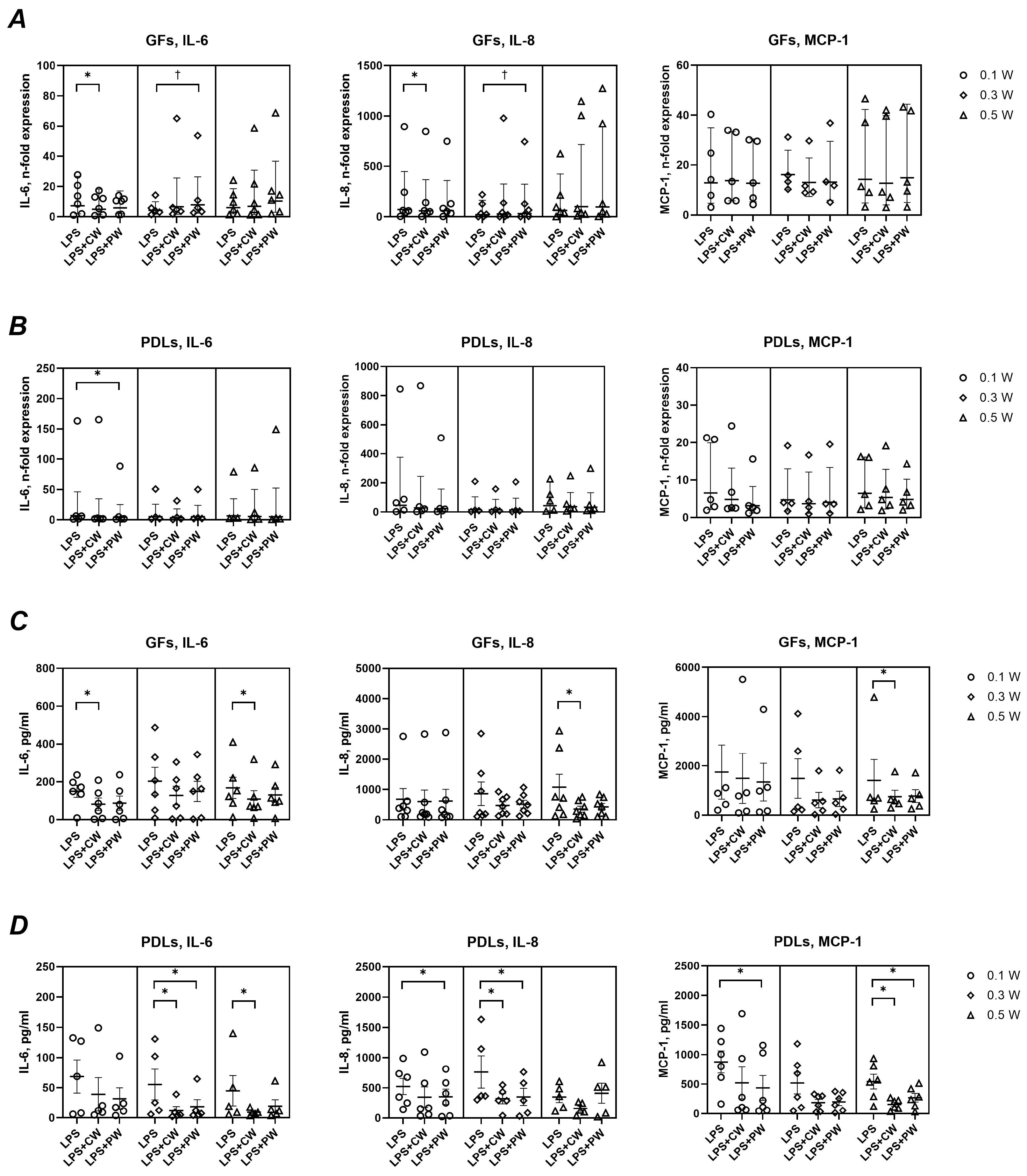
2.2.2. Basal Inflammatory Response
2.2.3. Inflammatory Response to P. gingivalis LPS
2.2.4. Mode Comparison
3. Discussion
4. Materials and Methods
4.1. Seven-Species Biofilm and Laser Treatment
4.2. Quantitative Analysis of Seven-Species Biofilm Composition by qPCR
4.3. Structural Analysis of Seven-Species Biofilms by Confocal Laser Scanning Microscopy
4.4. Cultivation of Human Cells
4.5. Treatment of Human Cells with Laser and P. gingivalis LPS
4.6. Cell Viability and Proliferation Assay
4.7. Gene Expression and Protein Production Analysis
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CLSM | Confocal laser scanning microscopy |
| CW | Continuous wave |
| GFs | Gingival fibroblasts |
| IL | Interleukin |
| LLLT | Low-level laser therapy |
| LPS | Lipopolysaccharide |
| MCP | Monocyte chemoattractant protein |
| OD | Optical density |
| PDLs | Periodontal ligament cells |
| PW | Pulsed wave |
References
- Eke, P.I.; Thornton-Evans, G.O.; Wei, L.; Borgnakke, W.S.; Dye, B.A.; Genco, R.J. Periodontitis in US Adults: National Health and Nutrition Examination Survey 2009–2014. J. Am. Dent. Assoc. 2018, 149, 576–588.e6. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Belstrom, D.; Eick, S.; Gursoy, U.K.; Johansson, A.; Kononen, E. Periodontal microbiology and microbial etiology of periodontal diseases: Historical concepts and contemporary perspectives. Periodontol. 2000, 2023; Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Tay, F.R.; Niu, L.N.; Chen, J.H. Advancing antimicrobial strategies for managing oral biofilm infections. Int. J. Oral Sci. 2019, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Dental Scaling and Root Planing for Periodontal Health: A Review of the Clinical Effectiveness, Cost-effectiveness, and Guidelines. In CADTH Rapid Response Reports; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2016.
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; Participants, E.F.P.W.; Methodological, C. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Winkler, P.C.; Benz, L.; Nickles, K.; Petsos, H.C.; Eickholz, P.; Dannewitz, B. Decision-making on systemic antibiotics in the management of periodontitis: A retrospective comparison of two concepts. J. Clin. Periodontol. 2024, 51, 1122–1133. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Tuner, J. Low-level laser therapy in dentistry. Dent. Clin. N. Am. 2004, 48, 1061–1076, viii. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; McGrath, C.; Jin, L.; Zhang, C.; Yang, Y. The effectiveness of low-level laser therapy as an adjunct to non-surgical periodontal treatment: A meta-analysis. J. Periodontal Res. 2017, 52, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Basso, F.G.; Oliveira, C.F.; Fontana, A.; Kurachi, C.; Bagnato, V.S.; Spolidorio, D.M.; Hebling, J.; de Souza Costa, C.A. In Vitro effect of low-level laser therapy on typical oral microbial biofilms. Braz. Dent. J. 2011, 22, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Robati, M.; Yousefimanesh, H.; Shokuhi Far, M.R.; Bagheri, S. Effect of low-level diode laser on streptococcus mutans and lactobacillus acidophilus growth: An invitro study. J. Oral Biol. Craniofac. Res. 2022, 12, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Tonin, M.H.; Brites, F.C.; Mariano, J.R.; Freitas, K.M.S.; Ortiz, M.A.L.; Salmeron, S. Low-Level Laser and Antimicrobial Photodynamic Therapy Reduce Peri-implantitis-related Microorganisms Grown In Vitro. Eur. J. Dent. 2022, 16, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Andrukhov, O. Toll-Like Receptors and Dental Mesenchymal Stromal Cells. Front. Oral Health 2021, 2, 648901. [Google Scholar] [CrossRef] [PubMed]
- Andrukhov, O.; Behm, C.; Blufstein, A.; Rausch-Fan, X. Immunomodulatory properties of dental tissue-derived mesenchymal stem cells: Implication in disease and tissue regeneration. World J. Stem Cells 2019, 11, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Lopes, L.; Rigau, J.; Zangaro, R.A.; Guidugli-Neto, J.; Jaeger, M.M. Comparison of the low level laser therapy effects on cultured human gingival fibroblasts proliferation using different irradiance and same fluence. Lasers Surg. Med. 2001, 29, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Pansani, T.N.; Basso, F.G.; Turirioni, A.P.; Kurachi, C.; Hebling, J.; de Souza Costa, C.A. Effects of low-level laser therapy on the proliferation and apoptosis of gingival fibroblasts treated with zoledronic acid. Int. J. Oral Maxillofac. Surg. 2014, 43, 1030–1034. [Google Scholar] [CrossRef] [PubMed]
- Frozanfar, A.; Ramezani, M.; Rahpeyma, A.; Khajehahmadi, S.; Arbab, H.R. The Effects of Low Level Laser Therapy on the Expression of Collagen Type I Gene and Proliferation of Human Gingival Fibroblasts (Hgf3-Pi 53): In vitro Study. Iran. J. Basic Med. Sci. 2013, 16, 1071–1074. [Google Scholar] [PubMed]
- Gkogkos, A.S.; Karoussis, I.K.; Prevezanos, I.D.; Marcopoulou, K.E.; Kyriakidou, K.; Vrotsos, I.A. Effect of Nd:YAG Low Level Laser Therapy on Human Gingival Fibroblasts. Int. J. Dent. 2015, 2015, 258941. [Google Scholar] [CrossRef] [PubMed]
- Salmani, Z.; Saberi, S.; Hodjat, M.; Tavakoli, M.; Eslaminia, M.; Sanchooli, S. Study the effect of low-level laser therapy on osteogenic capacity of periodontal ligament stem cell: An in vitro study. J. Laser Appl. 2025, 37, 012026. [Google Scholar] [CrossRef]
- Wang, L.; Liu, C.; Song, Y.; Wu, F. The effect of low-level laser irradiation on the proliferation, osteogenesis, inflammatory reaction, and oxidative stress of human periodontal ligament stem cells under inflammatory conditions. Lasers Med. Sci. 2022, 37, 3591–3599. [Google Scholar] [CrossRef] [PubMed]
- Papadelli, A.; Kyriakidou, K.; Kotsakis, G.A.; Pepelassi, E.; Kallis, A.; Vrotsos, I.A.; Karoussis, I.K. Immunomodulatory effects of Nd:YAG (1064 nm) and diode laser (810 nm) wavelengths to LPS-challenged human gingival fibroblasts. Arch. Oral Biol. 2021, 122, 104982. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, C.; Pan, L.; Chen, Y.; Bian, Z.; Yang, Y.; Ke, T.; Sun, W.; Chen, L.; Tan, J. Low-level Nd:YAG laser inhibiting inflammation and oxidative stress in human gingival fibroblasts via AMPK/SIRT3 axis. J. Photochem. Photobiol. 2024, 251, 112845. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.H.; Liu, S.L.; Chen, C.L.; Shie, M.Y.; Kao, C.T. Low-level laser effects on simulated orthodontic tension side periodontal ligament cells. Photomed. Laser Surg. 2013, 31, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chiang, M.H.; Chen, P.H.; Ho, M.L.; Lee, H.E.; Wang, Y.H. Anti-inflammatory effects of low-level laser therapy on human periodontal ligament cells: In vitro study. Lasers Med. Sci. 2018, 33, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Iaria, R.; Vescovi, P.; De Francesco, P.; Giovannacci, I. Laser Photobiomodulation: What Are the Ideal Parameters for Each Type of Laser Used in Dental Practice to Promote Fibroblast Proliferation and Differentiation? A Systematic Review. Life 2025, 15, 853. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Liang, S.; Payne, M.A.; Hashim, A.; Jotwani, R.; Eskan, M.A.; McIntosh, M.L.; Alsam, A.; Kirkwood, K.L.; Lambris, J.D.; et al. Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe 2011, 10, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Pourhajibagher, M.; Gharibpour, F.; Nikparto, N.; Bahrami, R.; Bahador, A. The effect of photobiomodulation on oral microbiota dysbiosis: A literature review. Photodiagnosis Photodyn. Ther. 2025, 52, 104525. [Google Scholar] [CrossRef] [PubMed]
- Kendlbacher, F.L.; Bloch, S.; Hager-Mair, F.F.; Bacher, J.; Janesch, B.; Thurnheer, T.; Andrukhov, O.; Schaffer, C. Multispecies biofilm behavior and host interaction support the association of Tannerella serpentiformis with periodontal health. Mol. Oral Microbiol. 2023, 38, 115–133. [Google Scholar] [CrossRef] [PubMed]
- Ozkan Karasu, Y.; Oner, F.; Kantarci, A. Neutrophil response to Porphyromonas gingivalis is modulated by low-level laser application. Oral Dis. 2024, 30, 5268–5273. [Google Scholar] [CrossRef] [PubMed]
- Vinothkumar, T.S.; Apathsakayan, R.; FM, M.E.-S.; Homeida, H.E.; Hommedi, A.I.M.; MY, A.S.; Alsalhi, H.A.M. Antibacterial effect of diode laser on different cariogenic bacteria: An In-vitro study. Niger. J. Clin. Pract. 2020, 23, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Sher, B.M.; Mulder, R.; Gutknecht, N. The Photobiomodulation Effect of 940 nm Laser Irradiation on Enterococcus faecalis in Human Root Dentin Slices of Varying Thicknesses. J. Lasers Med. Sci. 2021, 12, e48. [Google Scholar] [CrossRef] [PubMed]
- Mazurek-Mochol, M.; Bonsmann, T.; Mochol, M.; Poniewierska-Baran, A.; Pawlik, A. The Role of Interleukin 6 in Periodontitis and Its Complications. Int. J. Mol. Sci. 2024, 25, 2146. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Imboden, M.A.; Lang, N.P. Neutrophil migration into the gingival sulcus is associated with transepithelial gradients of interleukin-8 and ICAM-1. J. Periodontol. 1998, 69, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Garlet, G.P.; Martins, W., Jr.; Ferreira, B.R.; Milanezi, C.M.; Silva, J.S. Patterns of chemokines and chemokine receptors expression in different forms of human periodontal disease. J. Periodontal Res. 2003, 38, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Behm, C.; Blufstein, A.; Abhari, S.Y.; Koch, C.; Gahn, J.; Schaffer, C.; Moritz, A.; Rausch-Fan, X.; Andrukhov, O. Response of Human Mesenchymal Stromal Cells from Periodontal Tissue to LPS Depends on the Purity but Not on the LPS Source. Mediat. Inflamm. 2020, 2020, 8704896. [Google Scholar] [CrossRef] [PubMed]
- Kushibiki, T.; Hirasawa, T.; Okawa, S.; Ishihara, M. Regulation of miRNA expression by low-level laser therapy (LLLT) and photodynamic therapy (PDT). Int. J. Mol. Sci. 2013, 14, 13542–13558. [Google Scholar] [CrossRef] [PubMed]
- Slezovic, M.O.; Saygun, I.; Bengi, V.U.; Serdar, M.; Kantarci, A. Antiproliferative effect of low-level laser/photobiomodulation on gingival fibroblasts derived from calcium channel blocker-induced gingival overgrowth. Lasers Med. Sci. 2024, 39, 194. [Google Scholar] [CrossRef] [PubMed]
- Hakki, S.S.; Bozkurt, S.B. Effects of different setting of diode laser on the mRNA expression of growth factors and type I collagen of human gingival fibroblasts. Lasers Med. Sci. 2012, 27, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Mylona, V.; Anagnostaki, E.; Chiniforush, N.; Barikani, H.; Lynch, E.; Grootveld, M. Photobiomodulation Effects on Periodontal Ligament Stem Cells: A Systematic Review of In Vitro Studies. Curr. Stem Cell Res. Ther. 2024, 19, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Gholami, L.; Parsamanesh, G.; Shahabi, S.; Jazaeri, M.; Baghaei, K.; Fekrazad, R. The Effect of Laser Photobiomodulation on Periodontal Ligament Stem Cells. Photochem. Photobiol. 2021, 97, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Etemadi, A.; Aghaie, M.; Sayar, F.; Chiniforush, N. Effect of photobiomodulation therapy with 660 and 980 nm diode lasers on differentiation of periodontal ligament mesenchymal stem cells. Sci. Rep. 2024, 14, 20587. [Google Scholar] [CrossRef] [PubMed]
- Al-Watban, F.A.; Zhang, X.Y. The comparison of effects between pulsed and CW lasers on wound healing. J. Clin. Laser Med. Surg. 2004, 22, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, J.T.; Huang, Y.Y.; Sharma, S.K.; Kurup, D.B.; De Taboada, L.; Carroll, J.D.; Hamblin, M.R. Effect of pulsing in low-level light therapy. Lasers Surg. Med. 2010, 42, 450–466. [Google Scholar] [CrossRef] [PubMed]
- Tribble, G.D.; Lamont, R.J. Bacterial invasion of epithelial cells and spreading in periodontal tissue. Periodontol. 2000 2010, 52, 68–83. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.J.; Yilmaz, O. In or out: The invasiveness of oral bacteria. Periodontol. 2000 2002, 30, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Alonso, B.; Leon, R.; Roldan, S.; Sanz, M. Antimicrobial therapy in periodontitis: The use of systemic antimicrobials against the subgingival biofilm. J. Clin. Periodontol. 2008, 35, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, T.; Mogi, M.; Okabe, I.; Okada, K.; Goto, H.; Sasaki, Y.; Fujimura, T.; Fukuda, M.; Mitani, A. Adjunctive Application of Antimicrobial Photodynamic Therapy in Nonsurgical Periodontal Treatment: A Review of Literature. Int. J. Mol. Sci. 2015, 16, 24111–24126. [Google Scholar] [CrossRef] [PubMed]
- ALHarthi, S.S.; Ali, D.; Alamry, N.Z.; Alshehri, M.K.; Divakar, D.D.; BinShabaib, M.S. Photobiomodulation for Managing “Dry Socket”: A Randomised Controlled Trial. Int. Dent. J. 2023, 73, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Rosa, A.; Pujia, A.M.; Arcuri, C. Investigation of alveolar osteitis and the effectiveness of laser treatment: A unified Meta-analysis and review of the literature. BMC Oral Health 2024, 24, 700. [Google Scholar] [CrossRef] [PubMed]
- Bardhoshi, M.; Qafmolla, A.; Gutknecht, N.; D’Amico, C.; Fiorillo, L. 980 nm diode laser for treatment of vascular lesions in oral district: A 5 years follow-up trial. Minerva Dent. Oral Sci. 2022; Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Guggenheim, B.; Giertsen, E.; Schupbach, P.; Shapiro, S. Validation of an in vitro biofilm model of supragingival plaque. J. Dent. Res. 2001, 80, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Tomek, M.B.; Neumann, L.; Nimeth, I.; Koerdt, A.; Andesner, P.; Messner, P.; Mach, L.; Potempa, J.S.; Schaffer, C. The S-layer proteins of Tannerella forsythia are secreted via a type IX secretion system that is decoupled from protein O-glycosylation. Mol. Oral Microbiol. 2014, 29, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Gmur, R.; Guggenheim, B. Antigenic heterogeneity of Bacteroides intermedius as recognized by monoclonal antibodies. Infect. Immun. 1983, 42, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Ammann, T.W.; Bostanci, N.; Belibasakis, G.N.; Thurnheer, T. Validation of a quantitative real-time PCR assay and comparison with fluorescence microscopy and selective agar plate counting for species-specific quantification of an in vitro subgingival biofilm model. J. Periodontal Res. 2013, 48, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Ammann, T.W.; Belibasakis, G.N.; Thurnheer, T. Impact of early colonizers on in vitro subgingival biofilm formation. PLoS ONE 2013, 8, e83090. [Google Scholar] [CrossRef] [PubMed]
- Thurnheer, T.; van der Ploeg, J.R.; Giertsen, E.; Guggenheim, B. Effects of Streptococcus mutans gtfC deficiency on mixed oral biofilms in vitro. Caries Res. 2006, 40, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Behm, C.; Milek, O.; Schwarz, K.; Kovar, A.; Derdak, S.; Rausch-Fan, X.; Moritz, A.; Andrukhov, O. Heterogeneity in Dental Tissue-Derived MSCs Revealed by Single-Cell RNA-seq. J. Dent. Res. 2024, 103, 1141–1152. [Google Scholar] [CrossRef] [PubMed]
- An, N.; Holl, J.; Wang, X.; Rausch, M.A.; Andrukhov, O.; Rausch-Fan, X. Potential Suppressive Effect of Nicotine on the Inflammatory Response in Oral Epithelial Cells: An In Vitro Study. Int. J. Environ. Res. Public Health 2021, 18, 483. [Google Scholar] [CrossRef] [PubMed]
- Blufstein, A.; Behm, C.; Nguyen, P.Q.; Rausch-Fan, X.; Andrukhov, O. Human periodontal ligament cells exhibit no endotoxin tolerance upon stimulation with Porphyromonas gingivalis lipopolysaccharide. J. Periodontal Res. 2018, 53, 589–597. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organism | Sequence (5′-3′) | Reference |
|---|---|---|
| S. oralis | ACCAGGTCTTGACATCCCTCTGACC | [54] |
| ACCACCTGTCACCTCTGTCCCG | ||
| S. anginosus | ACCAGGTCTTGACATCCCGATGCTA | [54] |
| CCATGCACCACCTGTCACCGA | ||
| A. oris | GCCTGTCCCTTTGTGGGTGGG | [54] |
| GCGGCTGCTGGCACGTAGTT | ||
| V. dispar | CCCGGGCCTTGTACACACCG | [54] |
| CCCACCGGCTTTGGGCACTT | ||
| F. nucleatum | CGCCCGTCACACCACGAGA | [54] |
| ACACCCTCGGAACATCCCTCCTTAC | ||
| T. forsythia | CGATGATACGCGAGGAACCTTACCC | [54] |
| CCGAAGGGAAGAAAGCTCTCACTCT | ||
| P. gingivalis | GCGAGAGCCTGAACCAGCCA | [54] |
| ACTCGTATCGCCCGTTATTCCCGTA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dervisbegovic, S.; Bloch, S.; Maierhofer, V.; Behm, C.; Rausch-Fan, X.; Moritz, A.; Schäffer, C.; Andrukhov, O. Effect of Low-Level Laser Therapy on Periodontal Host Cells and a Seven-Species Periodontitis Model Biofilm. Int. J. Mol. Sci. 2025, 26, 6803. https://doi.org/10.3390/ijms26146803
Dervisbegovic S, Bloch S, Maierhofer V, Behm C, Rausch-Fan X, Moritz A, Schäffer C, Andrukhov O. Effect of Low-Level Laser Therapy on Periodontal Host Cells and a Seven-Species Periodontitis Model Biofilm. International Journal of Molecular Sciences. 2025; 26(14):6803. https://doi.org/10.3390/ijms26146803
Chicago/Turabian StyleDervisbegovic, Selma, Susanne Bloch, Vera Maierhofer, Christian Behm, Xiaohui Rausch-Fan, Andreas Moritz, Christina Schäffer, and Oleh Andrukhov. 2025. "Effect of Low-Level Laser Therapy on Periodontal Host Cells and a Seven-Species Periodontitis Model Biofilm" International Journal of Molecular Sciences 26, no. 14: 6803. https://doi.org/10.3390/ijms26146803
APA StyleDervisbegovic, S., Bloch, S., Maierhofer, V., Behm, C., Rausch-Fan, X., Moritz, A., Schäffer, C., & Andrukhov, O. (2025). Effect of Low-Level Laser Therapy on Periodontal Host Cells and a Seven-Species Periodontitis Model Biofilm. International Journal of Molecular Sciences, 26(14), 6803. https://doi.org/10.3390/ijms26146803