

Caffeine as a Modulator in Oncology: Mechanisms of Action and Potential for Adjuvant Therapy
 , , and
, , and
Abstract
1. Introduction
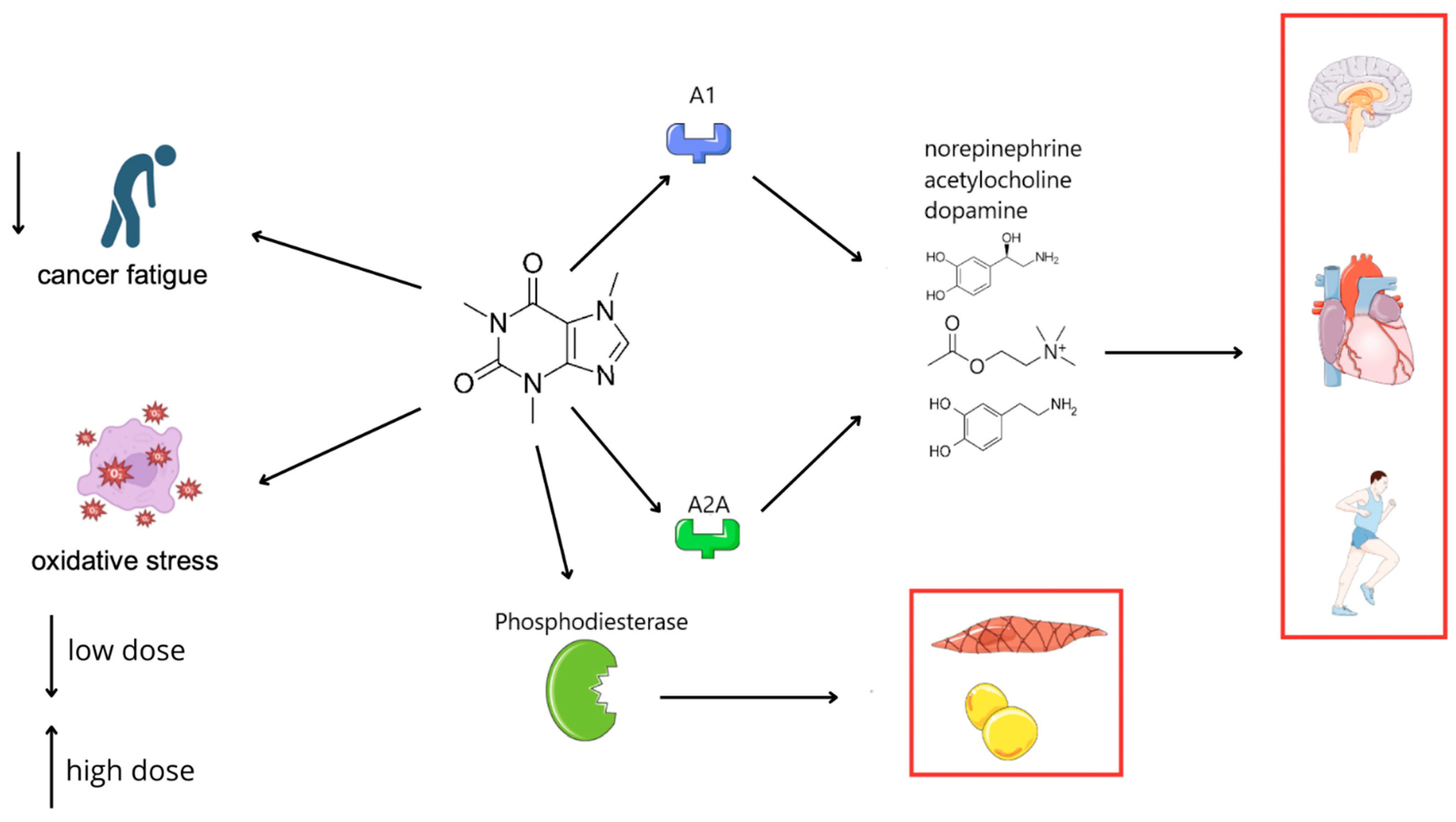
2. General Mechanisms of Caffeine Action
3. Genetic Polymorphisms and Individual Variability in Caffeine’s Effects
4. Caffeine in Cancer
4.1. Neuroendocrine Effects of Caffeine and Immune System Modulation in the Anticancer Therapy
4.2. Caffeine and Its Influence on the Appetite
4.3. Caffeine and Its Influence on Cancer Pain
4.4. Cancer-Related Fatigue
4.5. Caffeine Interactions with Chemotherapeutic Agents
4.6. Temperature of Caffeinated Beverages and Esophageal Risk
5. Influence on Psychiatric Disorders
5.1. Depression
5.2. Anxiety and Aggression Disorders
6. Effects on the Nervous System
6.1. Parkinson’s Disease
6.2. Migraine
6.3. Stroke
7. Effects on Cognitive Functions
7.1. Influence on Dementia
7.2. Influence on Alzheimer’s Disease
7.3. Cognitive Functions
8. Long-Term Caffeine Consumption and Its Effects
9. Limitations and Risks of Therapeutic Caffeine Use
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| A2AR | Adenosine A2A receptor |
| AD | Alzheimer’s disease |
| ADORA2A | Adenosine A2A receptor gene |
| ALS | Amyotrophic lateral sclerosis |
| ATM/ATR | Ataxia Telangiectasia Mutated/Ataxia Telangiectasia and Rad3-related kinases |
| ATR-Chk1 | Ataxia Telangiectasia and Rad3-related kinase–Checkpoint kinase 1 (DNA damage response pathway) |
| BRCA1 | Breast cancer gene 1 |
| CAF | Caffeine (1,3,7-trimethylxanthine) |
| cAMP | Cyclic adenosine monophosphate |
| CI | Confidence interval |
| CUD | Caffeine use disorder |
| CYP1A2 | Cytochrome P450 1A2 (liver enzyme metabolizing caffeine) |
| DASS | Depression, Anxiety, Stress Scale |
| EAC | Esophageal adenocarcinoma |
| EEG | Electroencephalography |
| ESCC | Esophageal squamous cell carcinoma |
| ESRD | End-stage renal disease |
| FDA | Food and Drug Administration |
| G2/M | G2/M phase cell cycle checkpoint |
| G6PD | Glucose-6-phosphate dehydrogenase |
| HIT-6 | Headache Impact Test-6 |
| HPA axis | Hypothalamic–pituitary–adrenal axis |
| MCI | Mild cognitive impairment |
| MDR | Multidrug resistance |
| NHANES | National Health and Nutrition Examination Survey |
| NK cell | Natural killer cell |
| OR | Odds ratio |
| PLGA | Poly(lactic-co-glycolic acid) |
| ROS | Reactive oxygen species |
| SIRT3 | Sirtuin 3 (mitochondrial deacetylase) |
| SNP | Single-nucleotide polymorphism |
| SOD2 | Superoxide dismutase 2 |
| Th1 | T-helper type 1 lymphocyte |
| TSD | Total sleep deprivation |
| UPDRS III | Unified Parkinson’s Disease Rating Scale, Part III (motor examination) |
| WM | Working memory |
| XO | Xanthine oxidase |
References
- Campagna, R.; Vignini, A. The Role of Xenobiotic Caffeine on Cardiovascular Health: Promises and Challenges. J. Xenobiotics 2025, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; He, B.; Wang, J.; Liu, J.; Hu, X. Risks of caffeine residues in the environment: Necessity for a targeted ecopharmacovigilance program. Chemosphere 2020, 243, 125343. [Google Scholar] [CrossRef] [PubMed]
- Quadra, G.R.; Paranaiba, J.R.; Vilas-Boas, J.; Roland, F.; Amado, A.M.; Barros, N.; Dias, R.J.P.; Cardoso, S.J. A global trend of caffeine consumption over time and related-environmental impacts. Environ. Pollut. 2020, 256, 113343. [Google Scholar] [CrossRef] [PubMed]
- Ősz, B.E.; Jîtcă, G.; Ștefănescu, R.E.; Pușcaș, A.; Tero-Vescan, A.; Vari, C.E. Caffeine and Its Antioxidant Properties—It Is All about Dose and Source. Int. J. Mol. Sci. 2022, 23, 13074. [Google Scholar] [CrossRef]
- van der Poll, T.; Coyle, S.M.; Barbosa, K.; Braxton, C.C.; Lowry, S.F. Epinephrine inhibits tumor necrosis factor-alpha and potentiates interleukin 10 production during human endotoxemia. J. Clin. Investig. 1996, 97, 713–719. [Google Scholar] [CrossRef]
- Lovallo, W.R.; Farag, N.H.; Vincent, A.S.; Thomas, T.L.; Wilson, M.F. Cortisol responses to mental stress, exercise, and meals following caffeine intake in men and women. Pharmacol. Biochem. Behav. 2006, 83, 441–447. [Google Scholar] [CrossRef]
- Ribeiro, J.A.; Sebastião, A.M. Caffeine and Adenosine. J. Alzheimer’s Dis. 2010, 20 (Suppl 1), S3–S15. [Google Scholar] [CrossRef]
- Bode, A.M.; Dong, Z. The enigmatic effects of caffeine in cell cycle and cancer. Cancer Lett. 2007, 247, 26–39. [Google Scholar] [CrossRef]
- Lu, Y.P.; Lou, Y.R.; Peng, Q.Y.; Xie, J.G.; Nghiem, P.; Conney, A.H. Effect of caffeine on the ATR/Chk1 pathway in the epidermis of UVB-irradiated mice. Cancer Res. 2008, 68, 2523–2529. [Google Scholar] [CrossRef]
- Rundle, S.; Bradbury, A.; Drew, Y.; Curtin, N.J. Targeting the ATR-CHK1 Axis in Cancer Therapy. Cancers 2017, 9, 41. [Google Scholar] [CrossRef]
- Wang, G.; Bhoopalan, V.; Wang, D.; Wang, L.; Xu, X. The effect of caffeine on cisplatin-induced apoptosis of lung cancer cells. Exp. Hematol. Oncol. 2015, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; Ghadirian, P.; El-Sohemy, A.; Lynch, H.T.; Snyder, C.; Daly, M.; Domchek, S.; Randall, S.; Karlan, B.; Zhang, P.; et al. The CYP1A2 genotype modifies the association between coffee consumption and breast cancer risk among BRCA1 mutation carriers. Cancer Epidemiol. Biomarkers Prev. 2007, 16, 912–916. [Google Scholar] [CrossRef]
- Low, J.J.L.; Tan, B.J.W.; Yi, L.X.; Zhou, Z.D.; Tan, E.K. Genetic susceptibility to caffeine intake and metabolism: A systematic review. J. Transl. Med. 2024, 22, 961. [Google Scholar] [CrossRef]
- Rahimi, M.; Semenova, E.; John, G.; Fallah, F.; Larin, A.; Generozov, E.; Ahmetov, I.I. Effect of ADORA2A Gene Polymorphism and Acute Caffeine Supplementation on Hormonal Response to Resistance Exercise: A Double-Blind, Crossover, Placebo-Controlled Study. Nutrients 2024, 16, 1803. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Z.; Han, S.; Lu, Y.; Feng, F.; Yuan, J. CYP1A2 rs762551 polymorphism contributes to cancer susceptibility: A meta-analysis from 19 case-control studies. BMC Cancer 2012, 12, 528. [Google Scholar] [CrossRef]
- Bartkiewicz, P.; Kunachowicz, D.; Filipski, M.; Stebel, A.; Ligoda, J.; Rembiałkowska, N. Hypercalcemia in Cancer: Causes, Effects, and Treatment Strategies. Cells 2024, 13, 1051. [Google Scholar] [CrossRef] [PubMed]
- Andryszkiewicz, W.; Misiąg, P.; Karwowska, A.; Resler, Z.; Wojno, A.; Kulbacka, J.; Szewczyk, A.; Rembiałkowska, N. Cancer Metastases to the Liver: Mechanisms of Tumor Cell Colonization. Pharmaceuticals 2024, 17, 1251. [Google Scholar] [CrossRef]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef]
- Wang, Z.; Gu, C.; Wang, X.; Lang, Y.; Wu, Y.; Wu, X.; Zhu, X.; Wang, K.; Yang, H. Caffeine enhances the anti-tumor effect of 5-fluorouracil via increasing the production of reactive oxygen species in hepatocellular carcinoma. Med. Oncol. 2019, 36, 97. [Google Scholar] [CrossRef]
- Tej, G.N.V.C.; Nayak, P.K. Mechanistic considerations in chemotherapeutic activity of caffeine. Biomed. Pharmacother. 2018, 105, 312–319. [Google Scholar] [CrossRef]
- Xu, H.; Hu, L.; Liu, T.; Chen, F.; Li, J.; Xu, J.; Jiang, L.; Xiang, Z.; Wang, X.; Sheng, J. Caffeine Targets G6PDH to Disrupt Redox Homeostasis and Inhibit Renal Cell Carcinoma Proliferation. Front. Cell Dev. Biol. 2020, 8, 556162. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.F.; Ouyang, S.H.; Tu, L.F.; Wang, X.; Yuan, W.L.; Wang, G.E.; Wu, Y.P.; Duan, W.J.; Yu, H.M.; Fang, Z.Z.; et al. Caffeine Protects Skin from Oxidative Stress-Induced Senescence through the Activation of Autophagy. Theranostics 2018, 8, 5713–5730. [Google Scholar] [CrossRef]
- Elenkov, I.J.; Kvetnansky, R.; Hashiramoto, A.; Bakalov, V.K.; Link, A.A.; Zachman, K.; Crane, M.; Jezova, D.; Rovensky, J.; Dimitrov, M.A.; et al. Low- versus High-Baseline Epinephrine Output Shapes Opposite Innate Cytokine Profiles: Presence of Lewis- and Fischer-Like Neurohormonal Immune Phenotypes in Humans? J. Immunol. 2008, 181, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Kovács, E.G.; Alatshan, A.; Budai, M.M.; Czimmerer, Z.; Bíró, E.; Benkő, S. Caffeine Has Different Immunomodulatory Effect on the Cytokine Expression and NLRP3 Inflammasome Function in Various Human Macrophage Subpopulations. Nutrients 2021, 13, 2409. [Google Scholar] [CrossRef]
- Ohta, A.; Gorelik, E.; Prasad, S.J.; Ronchese, F.; Lukashev, D.; Wong, M.K.K.; Huang, X.; Caldwell, S.; Liu, K.; Smith, P.; et al. A2A adenosine receptor protects tumors from antitumor T cells. Proc. Natl. Acad. Sci. USA 2006, 103, 13132–13137. [Google Scholar] [CrossRef] [PubMed]
- Eini, H.; Frishman, V.; Yulzari, R.; Kachko, L.; Lewis, E.C.; Chaimovitz, C.; Douvdevani, A. Caffeine promotes anti-tumor immune response during tumor initiation: Involvement of the adenosine A2A receptor. Biochem. Pharmacol. 2015, 98, 110–118. [Google Scholar] [CrossRef]
- Fu, J.; Antonioli, L.; Zheng, X.; El-Far, A.H. Editorial: Community series in adenosine pathways in cancer immunity and immunotherapy, volume II. Front. Immunol. 2025, 16, 1538930. [Google Scholar] [CrossRef]
- Strohbehn, G.W.; Ratain, M.J. Immunotherapy and the A2A Adenosine Receptor: A Confounding Brew. Clin. Pharmacol. Ther. 2019, 106, 498–500. [Google Scholar] [CrossRef]
- Schubert, M.M.; Irwin, C.; Seay, R.F.; Clarke, H.E.; Allegro, D.; Desbrow, B. Caffeine, coffee, and appetite control: A review. Int. J. Food Sci. Nutr. 2017, 68, 901–912. [Google Scholar] [CrossRef]
- Sweeney, P.; Levack, R.; Watters, J.; Xu, Z.; Yang, Y. Caffeine increases food intake while reducing anxiety-related behaviors. Appetite 2016, 101, 171–177. [Google Scholar] [CrossRef]
- Gavrieli, A.; Yannakoulia, M.; Fragopoulou, E.; Margaritopoulos, D.; Chamberland, J.P.; Kaisari, P.; Kavouras, S.A.; Mantzoros, C.S. Caffeinated Coffee Does Not Acutely Affect Energy Intake, Appetite, or Inflammation but Prevents Serum Cortisol Concentrations from Falling in Healthy Men1–4. J. Nutr. 2011, 141, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Panek-Shirley, L.M.; DeNysschen, C.; O’Brien, E.; Temple, J.L. Caffeine Transiently Affects Food Intake at Breakfast. J. Acad. Nutr. Diet. 2018, 118, 1832–1843. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.Y.; Choi, Y.S.; Oh, S.C.; Kim, Y.S.; Cho, K.; Bae, W.K.; Lee, J.H.; Seo, A.R.; Ahn, H.Y. Caffeine as an Adjuvant Therapy to Opioids in Cancer Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Pain Symptom Manag. 2013, 46, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Cornish, R.S.; Bolam, K.A.; Skinner, T.L. Effect of Caffeine on Exercise Capacity and Function in Prostate Cancer Survivors. Med. Sci. Sports Exerc. 2015, 47, 468–475. [Google Scholar] [CrossRef]
- Ferdaos, N.; Harada, A.; Masuda, E.; Kasai, S.; Horaguchi, T.; Yoshizawa, K. Caffeine-Supplemented Diet Prevents Fatigue-Like Behavior in Tumor-Bearing Mice. Nutr. Cancer 2023, 75, 1005–1013. [Google Scholar] [CrossRef]
- Xu, H.; Wang, L.; Shi, B.; Hu, L.; Gan, C.; Wang, Y.; Xiang, Z.; Wang, X.; Sheng, J. Caffeine inhibits the anticancer activity of paclitaxel via down-regulation of α-tubulin acetylation. Biomed Pharmacother. 2020, 129, 110441. [Google Scholar] [CrossRef]
- Yerragopu, A.K.; Chitra, V.; Kumar, K.R. Synergistic Effect of Caffeine in B16f10 Cells in Combination with Doxorubicin and Oxaliplatin. Toxicol. Int. 2023, 225–232. [Google Scholar] [CrossRef]
- Erzurumlu, Y.; Çataklı, D.; Doğan, H.K.; Aydoğdu, E. Caffeine May Improve the Chemotherapeutic Effect of Docetaxel by Inducing UPR and Autophagy in Breast Cancer Cells. Fabad J. Pharm. Sci. 2022, 48, 91–104. [Google Scholar] [CrossRef]
- Merlin, J.; Udayakumar, R.; Pandian, S.; Veerappan, K. Multidrug resistance for cancer treatment: Delivery of ursolic acid and caffeine by poly (lactic-co-glycolic acid) nanoparticles. J. Cancer Sci. Res. 2017, 3, S2. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Drinking Coffee, Mate, and Very Hot Beverages; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar] [PubMed]
- Islami, F.; Boffetta, P.; Ren, J.; Pedoeim, L.; Khatib, D.; Kamangar, F. High-temperature beverages and foods and esophageal cancer risk—A systematic review. Int. J. Cancer 2009, 125, 491–524. [Google Scholar] [CrossRef]
- Chen, Y.; Tong, Y.; Yang, C.; Gan, Y.; Sun, H.; Bi, H.; Cao, S.; Yin, X.; Lu, Z. Consumption of hot beverages and foods and the risk of esophageal cancer: A meta-analysis of observational studies. BMC Cancer 2015, 15, 449. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Zeng, R.; Cao, W.; Luo, R.; Chen, J.; Lin, Y. Hot beverage and food intake and esophageal cancer in southern China. Asian Pac. J. Cancer Prev. 2011, 12, 2189–2192. [Google Scholar] [PubMed]
- Luo, H.; Ge, H. Hot Tea Consumption and Esophageal Cancer Risk: A Meta-Analysis of Observational Studies. Front. Nutr. 2022, 9, 831567. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhang, L.; Du, W.; Tang, J.; Yang, L.; Geng, D.; Cheng, Y. Caffeine alleviate lipopolysaccharide-induced neuroinflammation and depression through regulating p-AKT and NF-κB. Neurosci Lett. 2024, 837, 137923. [Google Scholar] [CrossRef]
- Bodur, M.; Kaya, S.; Ilhan-Esgin, M.; Çakiroğlu, F.P.; Özçelik, A.Ö. The caffeine dilemma: Unraveling the intricate relationship between caffeine use disorder, caffeine withdrawal symptoms and mental well-being in adults. Public. Health Nutr. 2024, 27, e57. [Google Scholar] [CrossRef]
- Abdoli, F.; Davoudi, M.; Momeni, F.; Djafari, F.; Dolatshahi, B.; Hosseinzadeh, S.; Aliyaki, H.; Khalili, Z. Estimate the prevalence of daily caffeine consumption, caffeine use disorder, caffeine withdrawal and perceived harm in Iran: A cross-sectional study. Sci. Rep. 2024, 14, 7644. [Google Scholar] [CrossRef]
- Cole, E.L.; Grillo, A.R.; Vrshek-Schallhorn, S. Habitual Caffeine Use Is Associated With Heightened Cortisol Reactivity to Lab-Based Stress in Two Samples. Psychosom. Med. 2024, 86, 730–737. [Google Scholar] [CrossRef]
- Yang, L.S.; Zhang, Z.Y.; Yan, L.J.; Yan, Y.C.; Tan, S.Y.; Wang, D.X.; Dong, Z.R.; Li, T. Caffeine intake is associated with less severe depressive symptoms in noncancer populations: An analysis based on NHANES 2007–2016. Nutr. Res. 2023, 118, 1–11. [Google Scholar] [CrossRef]
- Makki, N.M.; Alharbi, S.T.; Alharbi, A.M.; Alsharif, A.S.; Aljabri, A.M. Caffeine Consumption and Depression, Anxiety, and Stress Levels Among University Students in Medina: A Cross-Sectional Study. Cureus 2023, 15, e48018. [Google Scholar] [CrossRef]
- Yin, J.; Ding, Y.; Xu, F.; Zhao, L.; Gong, R.; Yang, J.; Liu, Y. Does the timing of intake matter? Association between caffeine intake and depression: Evidence from the National Health and Nutrition Examination Survey. J. Affect. Disord. 2023, 340, 362–368. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Z.; Gui, P.; Zhang, B.; Xie, Y. Coffee and caffeine intake and depression in postpartum women: A cross-sectional study from the National Health and Nutrition Examination Survey 2007–2018. Front. Psychol. 2023, 14, 1134522. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wang, L.; Zhang, C.; Hu, Z.; Tang, J.; Xue, J.; Lu, W. Caffeine intake and anxiety: A meta-analysis. Front. Psychol. 2024, 1, 15. [Google Scholar] [CrossRef]
- Cho, J.A.; Kim, S.; Shin, H.; Kim, H.; Park, E.C. The Association between High-Caffeine Drink Consumption and Anxiety in Korean Adolescents. Nutrients 2024, 16, 794. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhou, Z.D.; Yi, L.; Tan, B.J.W.; Tan, E.K. Interaction between caffeine consumption & genetic susceptibility in Parkinson’s disease: A systematic review. Ageing Res. Rev. 2024, 99, 102381. [Google Scholar] [CrossRef]
- Asuku, A.O.; Ayinla, M.T.; Olajide, T.S.; Oyerinde, T.O.; Yusuf, J.A.; Bayo-Olugbami, A.A.; Fajemidagba, G.A. Coffee and Parkinson’s disease. Prog. Brain Res. 2024, 289, 1–19. [Google Scholar]
- Hamdan, M.; Suharto, A.P.; Nugraha, P.; Islamiyah, W.R. Motor improvement in Parkinson’s disease patients receiving caffeine adjuvants: A double-blind randomized controlled trial in Indonesia. Narra J. 2024, 4, e826. [Google Scholar] [CrossRef]
- Reddy, V.S.; Shiva, S.; Manikantan, S.; Ramakrishna, S. Pharmacology of caffeine and its effects on the human body. Eur. J. Med. Chem. Rep. 2024, 10, 100138. [Google Scholar] [CrossRef]
- de Bem Alves, A.C.; Aguiar, A.S. Caffeine plus haloperidol reduces fatigue in an experimental model of Parkinson’s disease—A prospective to A2AR-D2R heterodimer antagonism. Purinergic Signal. 2024, 20, 29–34. [Google Scholar] [CrossRef]
- Zhao, Y.; Lai, Y.; Konijnenberg, H.; Huerta, J.M.; Vinagre-Aragon, A.; Sabin, J.A.; Hansen, J.; Petrova, D.; Sacerdote, C.; Zamora-Ros, R.; et al. Association of Coffee Consumption and Prediagnostic Caffeine Metabolites With Incident Parkinson Disease in a Population-Based Cohort. Neurology 2024, 102, e209201. [Google Scholar] [CrossRef]
- Barbanti, P.; Allais, G.; Cevoli, S.; Guerzoni, S.; Valeriani, M.; Vernieri, F. The Role of the Combination Paracetamol/Caffeine in Treatment of Acute Migraine Pain: A Narrative Review. Pain Ther. 2024, 13, 319–346. [Google Scholar] [CrossRef]
- Diener, H.; Peil, H.; Aicher, B. The efficacy and tolerability of a fixed combination of acetylsalicylic acid, paracetamol, and caffeine in patients with severe headache: A post-hoc subgroup analysis from a multicentre, randomized, double-blind, single-dose, placebo-controlled parallel group study. Cephalalgia 2011, 31, 1466–1476. [Google Scholar]
- Cho, S.; Kim, K.M.; Chu, M.K. Coffee consumption and migraine: A population-based study. Sci. Rep. 2024, 14, 6007. [Google Scholar] [CrossRef]
- Zduńska, A.; Cegielska, J.; Zduński, S.; Domitrz, I. Caffeine for Headaches: Helpful or Harmful? A Brief Review of the Literature. Nutrients 2023, 15, 3170. [Google Scholar] [CrossRef] [PubMed]
- Charles, A. The role of caffeine in headache disorders. Curr. Opin. Neurol. 2024, 37, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Nowaczewska, M.; Wiciński, M.; Kaźmierczak, W. The Ambiguous Role of Caffeine in Migraine Headache: From Trigger to Treatment. Nutrients 2020, 12, 2259. [Google Scholar] [CrossRef]
- Hikita, T.; Goda, H.; Ogawa, Y.; Kudo, T.; Ito, K. Caffeine consumption as a risk factor for childhood and adolescence migraine. Pediatr. Int. 2023, 65, e15429. [Google Scholar] [CrossRef] [PubMed]
- Mostofsky, E.; Mittleman, M.A.; Buettner, C.; Li, W.; Bertisch, S.M. Prospective Cohort Study of Caffeinated Beverage Intake as a Potential Trigger of Headaches among Migraineurs. Am. J. Med. 2019, 132, 984–991. [Google Scholar] [CrossRef]
- Mostofsky, E.; Schlaug, G.; Mukamal, K.J.; Rosamond, W.D.; Mittleman, M.A. Coffee and acute ischemic stroke onset. Neurology 2010, 75, 1583–1588. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.E.; Kim, Y. Relationship between coffee consumption and stroke risk in Korean population: The Health Examinees (HEXA) Study. Nutr. J. 2017, 16, 7. [Google Scholar] [CrossRef]
- Shao, C.; Tang, H.; Wang, X.; He, J. Coffee Consumption and Stroke Risk: Evidence from a Systematic Review and Meta-Analysis of more than 2.4 Million Men and Women. J. Stroke Cerebrovasc. Dis. 2021, 30, 105452. [Google Scholar] [CrossRef]
- Fan, J.; Yuan, Y.; Zhang, X.; Li, W.; Ma, W.; Wang, W.; Gu, J.; Zhou, B. Association between urinary caffeine and caffeine metabolites and stroke in American adults: A cross-sectional study from the NHANES, 2009–2014. Sci. Rep. 2023, 13, 11855. [Google Scholar] [CrossRef]
- Driscoll, I.; Shumaker, S.A.; Snively, B.M.; Margolis, K.L.; Manson, J.E.; Vitolins, M.Z.; Rossom, R.C.; Espeland, M.A. Relationships Between Caffeine Intake and Risk for Probable Dementia or Global Cognitive Impairment: The Women’s Health Initiative Memory Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1596–1602. [Google Scholar] [CrossRef]
- Haskell-Ramsay, C.F.; Jackson, P.A.; Forster, J.S.; Dodd, F.L.; Bowerbank, S.L.; Kennedy, D.O. The Acute Effects of Caffeinated Black Coffee on Cognition and Mood in Healthy Young and Older Adults. Nutrients 2018, 10, 1386. [Google Scholar] [CrossRef] [PubMed]
- Carman, A.J.; Dacks, P.A.; Lane, R.F.; Shineman, D.W.; Fillit, H.M. Current evidence for the use of coffee and caffeine to prevent age-related cognitive decline and Alzheimer’s disease. J. Nutr. Health Aging 2014, 18, 383–392. [Google Scholar] [CrossRef]
- Eskelinen, M.H.; Kivipelto, M. Caffeine as a protective factor in dementia and Alzheimer’s disease. J. Alzheimers Dis. 2010, 20 (Suppl. 1), S167–S174. [Google Scholar] [CrossRef]
- Tira, R.; Viola, G.; Barracchia, C.G.; Parolini, F.; Munari, F.; Capaldi, S.; Assfalg, M.; D’Onofrio, M. Espresso Coffee Mitigates the Aggregation and Condensation of Alzheimer′s Associated Tau Protein. J. Agric. Food Chem. 2023, 71, 11429–11441. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, M.C.; Bennett, D.A.; Weintraub, S.; Schneider, J.A.; Morris, M.C. Caffeine Consumption and Dementia: Are Lewy Bodies the Link? Ann. Neurol. 2022, 91, 834–846. [Google Scholar] [CrossRef]
- MYelanchezian, Y.M.; Waldvogel, H.J.; Faull, R.L.M.; Kwakowsky, A. Neuroprotective Effect of Caffeine in Alzheimer’s Disease. Molecules 2022, 27, 3737. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, H.; Li, S.; Li, W.-D.; Wang, y. Consumption of coffee and tea and risk of developing stroke, dementia, and poststroke dementia: A cohort study in the UK Biobank. PLoS Med. 2021, 18, e1003830. [Google Scholar] [CrossRef]
- Lefèvre-Arbogast, S.; Helmer, C.; Berr, C.; Debette, S.; Samieri, C. Habitual coffee consumption and risk of dementia in older persons: Modulation by CYP1A2 polymorphism. Eur. J. Epidemiol. 2024, 39, 81–86. [Google Scholar] [CrossRef]
- Chen, J.Q.A.; Scheltens, P.; Groot, C.; Ossenkoppele, R. Associations Between Caffeine Consumption, Cognitive Decline, and Dementia: A Systematic Review. J. Alzheimer’s Disease 2020, 78, 1519–1546. [Google Scholar] [CrossRef]
- Uchida, K.; Meno, K.; Korenaga, T.; Liu, S.; Suzuki, H.; Baba, Y.; Tagata, C.; Araki, Y.; Tsunemi, S.; Aso, K.; et al. Effect of matcha green tea on cognitive functions and sleep quality in older adults with cognitive decline: A randomized controlled study over 12 months. PLoS ONE 2024, 19, e0309287. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Hu, C.X.; Liu, X.; Zhu, R.X.; Wang, B.Q. Moderate coffee or tea consumption decreased the risk of cognitive disorders: An updated dose–response meta-analysis. Nutr. Rev. 2024, 82, 738–748. [Google Scholar] [CrossRef]
- Lin, Y.S.; Weibel, J.; Landolt, H.P.; Santini, F.; Slawik, H.; Borgwardt, S.; Cajochen, C.; Reichert, C.F. Brain activity during a working memory task after daily caffeine intake and caffeine withdrawal: A randomized double-blind placebo-controlled trial. Sci. Rep. 2023, 13, 1002. [Google Scholar] [CrossRef] [PubMed]
- Mabrey, G.; Koozehchian, M.S.; Newton, A.T.; Naderi, A.; Forbes, S.C.; Haddad, M. The Effect of Creatine Nitrate and Caffeine Individually or Combined on Exercise Performance and Cognitive Function: A Randomized, Crossover, Double-Blind, Placebo-Controlled Trial. Nutrients 2024, 16, 766. [Google Scholar] [CrossRef]
- Zhu, H.; Bai, S.; Ma, W.; Qian, H.; Du, P. A combined effect of fish-originated collagen peptides and caffeine on the cognitive function of sleep-deprived mice. Food Funct. 2024, 15, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.J.; Wang, Z.G.; Gong, J.H.; Gong, J.P.; Li, J.H. Role of alanine aminotransferase in the effects of urinary caffeine concentration and its primary metabolite concentration on cognitive function in older adults: Bayesian Kernel Machine regression analysis and mediation analysis. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 721–733. [Google Scholar]
- Wu, S.H.; Chen, Y.C.; Chen, C.H.; Liu, H.S.; Liu, Z.X.; Chiu, C.H. Caffeine supplementation improves the cognitive abilities and shooting performance of elite e-sports players: A crossover trial. Sci. Rep. 2024, 14, 2074. [Google Scholar] [CrossRef]
- Huin, V.; Blum, D.; Delforge, V.; Cailliau, E.; Djeziri, S.; Dujardin, K.; Genet, A.; Viard, R.; Attarian, S.; Bruneteau, G.; et al. Caffeine consumption outcomes on amyotrophic lateral sclerosis disease progression and cognition. Neurobiol Dis. 2024, 199, 106603. [Google Scholar] [CrossRef]
- Nadam, I.S.; Bellamine, A.; Salom, R.; Guilera, S.; Inarejos-Garcia, A.M.; Pillar, G. Effects of the active botanical blend “WKUP GT” on attention and cognitive functions after lunch in healthy volunteers. Hum. Psychopharmacol.: Clin. Exp. 2024, 39, e2895. [Google Scholar] [CrossRef]
- dos Santos, M.K.F.; Gavioli, E.C.; Rosa, L.S.; de Paula Soares-Rachetti, V.; Lobão-Soares, B. Craving espresso: The dialetics in classifying caffeine as an abuse drug. Naunyn Schmiedebergs Arch. Pharmacol. 2018, 391, 1301–1318. [Google Scholar] [CrossRef] [PubMed]
- Heinz, A.; Daedelow, L.S.; Wackerhagen, C.; Di Chiara, G. Addiction theory matters—Why there is no dependence on caffeine or antidepressant medication. Addict. Biol. 2020, 25, e12735. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Mikulic, P. Acute effects of caffeine supplementation on resistance exercise, jumping, and Wingate performance: No influence of habitual caffeine intake. Eur. J. Sport Sci. 2021, 21, 1165–1175. [Google Scholar] [CrossRef]
- Tallis, J.; Guimaraes-Ferreira, L.; Clarke, N.D. Not Another Caffeine Effect on Sports Performance Study—Nothing New or More to Do? Nutrients 2022, 14, 4696. [Google Scholar] [CrossRef]
- Willson, C. The clinical toxicology of caffeine: A review and case study. Toxicol. Rep. 2018, 5, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Grgic, J. Is Coffee a Useful Source of Caffeine Preexercise? Int. J. Sport. Nutr. Exerc. Metab. 2020, 30, 69–82. [Google Scholar] [CrossRef]
- Zhang, B.; Liu, Y.; Wang, X.; Deng, Y.; Zheng, X. Cognition and Brain Activation in Response to Various Doses of Caffeine: A Near-Infrared Spectroscopy Study. Front Psychol. 2020, 11, 1393. [Google Scholar] [CrossRef]
- Pina Cabral, J.; Sousa, D.L.; Carvalho, C.; Girao, A.; Pacheco Mendes, A.; Pina, R. Caffeine Intoxication: Unregulated, Over-the-Counter Sale of Potentially Deadly Supplements. Cureus 2022, 14, e21045. [Google Scholar] [CrossRef]

{kind=link}
| Area of Interest | Effect of Caffeine | Cited Studies |
|---|---|---|
| DNA Damage Response and Cell Cycle Regulation | Inhibits ATR-Chk1 signaling, sensitizing cancer cells to DNA-damaging agents by impairing DNA repair and promoting mitotic catastrophe. | [8,9,10,11] |
| Cancer Treatment | Low doses: anti-oxidant protection and cancer prevention. High doses: oxidative stress and enhanced cell death. | [8,18,19,20,21,22] |
| Neuroendocrine Effects and Immune System Modulation | CAF modulates immune response by elevating cortisol (mild immunosuppression) and blocking A2A adenosine receptors, enhancing T and NK cell activity. Demonstrated tumor protection in vivo; may synergize with immunotherapy. | [5,23,24,25,26,27,28] |
| Influence of Caffeine on the Appetite | Mixed findings; possible appetite increase in animals (dose-dependent), no significant effect in humans; CAF may raise cortisol levels. | [29,30,31,32] |
| Caffeine and Cancer Pain | Modest reduction in pain and drowsiness as an adjuvant to opioids; not clinically significant. | [33] |
| Cancer-Related Fatigue | Improved physical performance and muscle strength; no significant effect on perceived fatigue | [34,35] |
| Caffeine Interactions with Chemotherapeutic Agents | Enhances cytotoxicity of agents like doxorubicin, oxaliplatin, and docetaxel via apoptosis/autophagy. Additionally, abrogates G2/M checkpoint arrest by inhibiting ATM/ATR, sensitizing cancer cells to DNA-damaging agents. | [8,20,36,37,38,39] |
| Temperature Beverages and Esophageal Cancer Risk | Not CAF itself, but consumption of hot caffeinated beverages (>65 °C) is associated with an increased risk of esophageal squamous cell carcinoma (ESCC), likely due to thermal injury to the esophageal mucosa leading to chronic inflammation and carcinogenesis. | [40,41,42,43,44] |
| Area of Interest | Effect of Caffeine | Cited Studies |
|---|---|---|
| Psychiatric Disorders: Depression | Reduces depressive symptoms in moderate amounts; timing of intake affects depression risk; excessive intake and withdrawal are linked to increased depressive tendencies. | [45,46,47,48,49,50,51,52] |
| Psychiatric Disorders | Increases risk of anxiety, especially at higher doses; dose-dependent effects noted across populations, including adolescents. | [53,54] |
| Parkinson’s Disease | Reduces risk; improves motor functions and cognitive outcomes. | [55,56,57,58,59,60] |
| Migraine and Headaches | Enhances the effect of analgesics; beneficial in moderate amounts; excessive consumption or acute withdrawal can trigger or exacerbate migraines. | [61,62,63,64,65,66,67,68] |
| Stroke | Reduces stroke risk in certain populations; potential diagnostic value based on CAF metabolites. | [69,70,71,72] |
| Cognitive Performance and Dementia | Enhances alertness, attention, and memory; improves reaction time in certain contexts; may impair working memory due to increased metabolic demand; reduces prevalence and risk of dementia and Alzheimer’s; has neuroprotective effects due to anti-inflammatory and anti-oxidant properties. | [73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91] |
| Long-Term Caffeine Consumption | Associated with potential for tolerance and withdrawal symptoms but lacks classical addiction profile; ergogenic effects vary with habitual intake and dosing. | [92,93,94,95,96,97,98] |
| Limitations and Risks of Therapeutic Caffeine Use | Effective anticancer doses of caffeine in vitro exceed safe levels in humans. High doses may cause arrhythmias, seizures, or toxicity, especially in slow metabolizers. Metabolic variability, scarce clinical data, and side effects limit its use. | [1,99] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rembiałkowska, N.; Demiy, A.; Dąbrowska, A.; Mastalerz, J.; Szlasa, W. Caffeine as a Modulator in Oncology: Mechanisms of Action and Potential for Adjuvant Therapy. Int. J. Mol. Sci. 2025, 26, 6252. https://doi.org/10.3390/ijms26136252
Rembiałkowska N, Demiy A, Dąbrowska A, Mastalerz J, Szlasa W. Caffeine as a Modulator in Oncology: Mechanisms of Action and Potential for Adjuvant Therapy. International Journal of Molecular Sciences. 2025; 26(13):6252. https://doi.org/10.3390/ijms26136252
Chicago/Turabian StyleRembiałkowska, Nina, Alina Demiy, Alicja Dąbrowska, Jakub Mastalerz, and Wojciech Szlasa. 2025. "Caffeine as a Modulator in Oncology: Mechanisms of Action and Potential for Adjuvant Therapy" International Journal of Molecular Sciences 26, no. 13: 6252. https://doi.org/10.3390/ijms26136252
APA StyleRembiałkowska, N., Demiy, A., Dąbrowska, A., Mastalerz, J., & Szlasa, W. (2025). Caffeine as a Modulator in Oncology: Mechanisms of Action and Potential for Adjuvant Therapy. International Journal of Molecular Sciences, 26(13), 6252. https://doi.org/10.3390/ijms26136252