
Life-Threatening Macrophage Activation Syndrome in Pregnancy: First Manifestation of SLE Induced by Parvovirus B19

 , , and
, , and
Abstract
1. Introduction
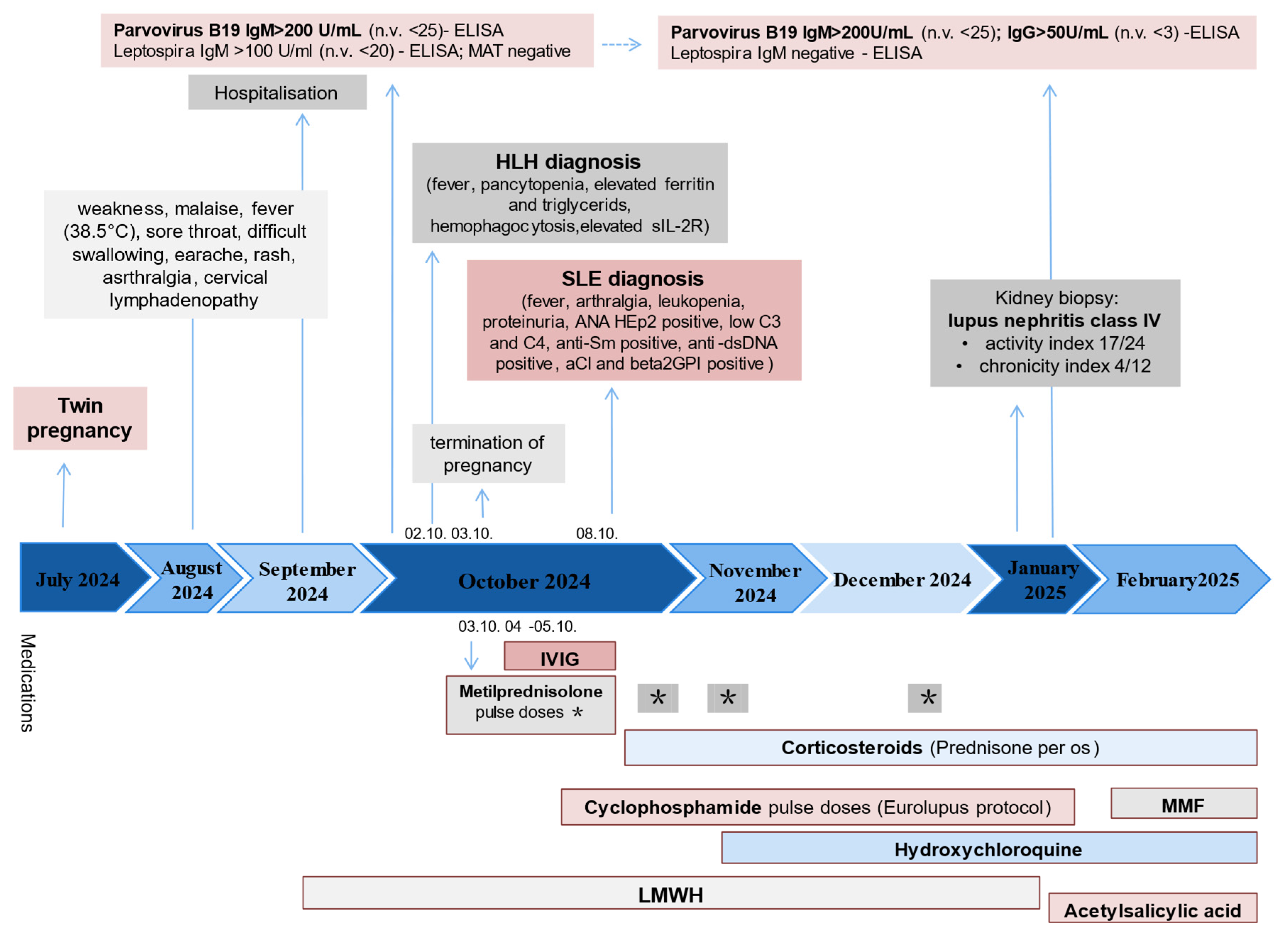
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, Y.; Wang, T.; Wu, H. Heterogeneity of macrophage activation syndrome and treatment progression. Front. Immunol. 2024, 15, 1389710. [Google Scholar] [CrossRef] [PubMed]
- Shakoory, B.; Geerlinks, A.; Wilejto, M.; Kernan, K.; Hines, M.; Romano, M.; Piskin, D.; Ravelli, A.; Sinha, R.; Aletaha, D.; et al. The 2022 EULAR/ACR points to consider at the early stages of diagnosis and management of suspected haemophagocytic lymphohistiocytosis/macrophage activation syndrome (HLH/MAS). Ann Rheum Dis. 2023, 82, 1271–1285. [Google Scholar] [CrossRef]
- Aziz, A.; Castaneda, E.E.; Ahmad, N.; Veerapalli, H.; Rockferry, A.G.; Lankala, C.R.; Hamid, P. Exploring macrophage activation syndrome secondary to systemic lupus erythematosus in adults: A systematic review of the literature. Cureus 2021, 13, e18822. [Google Scholar] [CrossRef]
- Kerr, J.R. The role of parvovirus B19 in the pathogenesis of autoimmunity and autoimmune disease. J. Clin. Pathol. 2016, 69, 279–291. [Google Scholar] [CrossRef]
- Thomas, G.; Rael, L.; Shimonkevitz, R.; Melamed, I.; Bar-Or, D. Autoantibody reaction to myelin basic protein by plasma parvovirus B19 IgG in MS patients. Protein Pept. Lett. 2006, 13, 109–111. [Google Scholar] [CrossRef]
- Thammasri, K.; Rauhamaki, S.; Wang, L.; Filippou, A.; Kivovich, V.; Marjomaki, V.; Naides, S.J.; Gilbert, L. Human parvovirus B19 induced apoptotic bodies contain altered self-antigens that are phagocytosed by antigen-presenting cells. PLoS ONE 2013, 8, e67179. [Google Scholar] [CrossRef]
- Trapani, S.; Ermini, M.; Falcini, F. Human parvovirus B19 infection: Its relationship with systemic lupus erythematosus. Semin. Arthritis Rheum. 1999, 28, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Griffin, G.; Shenoi, S.; Hughes, G.C. Hemophagocytic lymphohistiocytosis: An update on pathogenesis, diagnosis, and therapy. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101515. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, B.; Virelli, G.; Pedrollo, E.; Caprioli, M.; Riva, M.; Renna, D.; Tonutti, A.; Luciano, N.; Ceribelli, A.; Gremese, E.; et al. High risk of misclassification of acute Parvovirus B19 infection into a systemic rheumatic disease. Rheumatol. Adv. Pract. 2024, 8, rkae105. [Google Scholar] [CrossRef]
- Severin, M.C.; Levy, Y.; Shoenfeld, Y. Systemic lupus erythematosus and parvovirus B-19: Casual coincidence or causative culprit? Clin. Rev. Allergy Immunol. 2003, 25, 41–48. [Google Scholar] [CrossRef]
- Vilaiyuk, S.; Sirachainan, N.; Wanitkun, S.; Pirojsakul, K.; Vaewpanich, J. Recurrent macrophage activation syndrome as the primary manifestation in systemic lupus erythematosus and the benefit of serial ferritin measurements: A case-based review. Clin. Rheumatol. 2013, 32, 899–900. [Google Scholar] [CrossRef] [PubMed]
- Lerkvaleekul, B.; Vilaiyuk, S. Macrophage activation syndrome: Early diagnosis is key. Open Access Rheumatol. Res. Rev. 2018, 10, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.M.; Márquez, A.M.B.; Cabada, I.A.B. Systemic lupus erythematosus and its association with hemophagocytic syndrome as an initial manifestation. Maedica 2020, 15, 556–560. [Google Scholar] [CrossRef]
- AlSheef, M.; Zaidi, A.R.Z.; AlAtmi, A.A.; AlSharif, L.H.; Mian, A. Hemophagocytic syndrome as an initial presentation of systemic lupus erythematosus: A case report. Cureus 2019, 11, e5261. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.L.; Yahaya, M.H.; Ahmad, N.S.; Lim, C.H. Macrophage activation syndrome as an initial presentation of systemic lupus erythematosus with sensorineural hearing loss in a young male patient. BMJ Case Rep. 2020, 13, e233330. [Google Scholar] [CrossRef]
- Abdelfattah, A.H.; Macpherson, A.; Javed, F. Macrophage activation syndrome presents as initial manifestation of lupus in an adult female. Cureus 2024, 16, e60567. [Google Scholar] [CrossRef]
- Wang, J.; Rong, W.; Yan, H. Eighty-six cases of clinical characteristics and outcomes of systemic lupus erythematosus-associated macrophage activation syndrome: A meta-analysis study. Immun. Inflamm. Dis. 2024, 12, e1364. [Google Scholar] [CrossRef]
- Ren, W.; Yang, S.; Liu, H.; Pan, Z.; Li, Z.; Qiao, P.; Ma, H. Case report and literature review: Hemophagocytic lymphohistiocytosis in a pregnant woman with systemic lupus erythematosus with Syntaxin 11 gene defect. Front. Oncol. 2022, 12, 937494. [Google Scholar] [CrossRef]
- Henter, J.I.; Horne, A.; Aricó, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef]
- Fardet, L.; Galicier, L.; Lambotte, O.; Marzac, C.; Aumont, C.; Chahwan, D.; Coppo, P.; Hejblum, G. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014, 66, 2613–2620. [Google Scholar] [CrossRef]
- Ravelli, A.; Minoia, F.; Davì, S.; Horne, A.; Bovis, F.; Pistorio, A.; Aricò, M.; Avcin, T.; Behrens, E.M.; De Benedetti, F.; et al. 2016 Classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: A EULAR/ACR/PRINTO collaborative initiative. Ann. Rheum. Dis. 2016, 75, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Debaugnies, F.; Mahadeb, B.; Nagant, C.; Meuleman, N.; De Bels, D.; Wolff, F.; Gottignies, P.; Salaroli, A.; Borde, P.; Voue, M.; et al. Biomarkers for early diagnosis of hemophagocytic lymphohistiocytosis in critically ill patients. J. Clin. Immunol. 2021, 41, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, M.; Borgia, R.E.; Dominguez, D.; Fetldman, B.M.; Liao, F.; Levy, D.M.; Ng, L.; Abdelhaleem, M.; Silverman, E.D.; Hiraki, L.T. Predicting macrophage activation syndrome in childhood-onset systemic lupus erythematosus patients at diagnosis. J. Rheumatol. 2020, 48, 1450–1457. [Google Scholar] [CrossRef]
- Liu, L.; Cui, Y.; Zhou, Q.; Zhao, H.; Li, X. Hemophagocytic lymphohistiocytosis during pregnancy: A review of the literature in epidemiology, pathogenesis, diagnosis and treatment. Orphanet J. Rare Dis. 2021, 16, 281. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.; Mishra, B.; Singh, N.; Das, A.; Jindal, S. Fulminant parvovirus B19-associated pancarditis with haemophagocytic lymphohistiocytosis in an immunocompetent adult. APMIS 2009, 117, 773–777. [Google Scholar] [CrossRef]
- Ardalan, M.R.; Shoja, M.M.; Tubbs, R.S.; Esmaili, H.; Keyvani, H. Postrenal transplant hemophagocytic lymphohistiocytosis and thrombotic microangiopathy associated with parvovirus B19 infection. Am. J. Transplant. 2008, 8, 1340–1344. [Google Scholar] [CrossRef]
- Kalmuk, J.; Matar, S.; Feng, G.; Kilb, E.; Lim, M.Y. Parvovirus B19-induced hemophagocytic lymphohistiocytosis: Case report and review of the literature. Clin. Case Rep. 2019, 7, 2076–2081. [Google Scholar] [CrossRef]
- Mayama, M.; Yoshihara, M.; Kokabu, T.; Oguchi, H. Hemophagocytic lymphohistiocytosis associated with a parvovirus B19 infection during pregnancy. Obstet. Gynecol. 2014, 124, 438–441. [Google Scholar] [CrossRef]
- Duenas, O.; Gupta, S.; Rico, H.; Agarwal, A. Parvovirus B19-associated hemophagocytic reactive syndrome during pregnancy. Fertil. Steril. 2007, 88, S228. [Google Scholar] [CrossRef]
- Arvia, R.; Stincarelli, M.A.; Manaresi, E.; Gallinella, G.; Zakrzewska, K. Parvovirus B19 in rheumatic diseases. Microorganisms 2024, 12, 1708. [Google Scholar] [CrossRef]
- Meyer, O. Parvovirus B19 and autoimmune diseases. Jt. Bone Spine 2003, 70, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Aslanidis, S.; Pyrpasopoulou, A.; Kontotasios, K.; Doumas, S.; Zamboulis, C. Parvovirus B19 infection and systemic lupus erythematosus: Activation of an aberrant pathway? Eur. J. Intern. Med. 2008, 19, 314–318. [Google Scholar] [CrossRef]
- Young, N.S.; Brown, K.E. Parvovirus B19. N. Engl. J. Med. 2004, 350, 586–597. [Google Scholar] [CrossRef]
- Gallinella, G. The clinical use of parvovirus B19 assays: Recent advances. Expert Rev. Mol. Diagn. 2018, 18, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R.; Cunniffe, V.S.; Kelleher, P.; Coats, A.J.; Mattey, D.L. Circulating cytokines and chemokines in acute symptomatic parvovirus B19 infection: Negative association between levels of pro-inflammatory cytokines and development of B19-associated arthritis. J. Med. Virol. 2004, 74, 147–155. [Google Scholar] [CrossRef]
- Moffatt, S.; Tanaka, N.; Tada, K.; Nose, M.; Nakamura, M.; Muraoka, O.; Hirano, T.; Sugamura, K. A cytotoxic nonstructural protein, NS1, of human parvovirus B19 induces activation of interleukin-6 gene expression. J. Virol. 1996, 70, 8485–8491. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; López-Guillermo, A.; Khamashta, M.A.; Bosch, X. Adult haemophagocytic syndrome. Lancet 2014, 383, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hu, Z.; Cai, S.; Shen, G.; Zhong, J.; Dong, L. Efficacy of plasma exchange on top of standard immunosuppressive therapy in adult autoimmune inflammatory rheumatic diseases-associated macrophage activation syndrome, a single center real-world analysis. Semin. Arthritis Rheum. 2022, 55, 152043. [Google Scholar] [CrossRef]
- Summerlin, J.; Wells, D.A.; Anderson, M.K.; Halford, Z. A Review of Current and Emerging Therapeutic Options for Hemophagocytic Lymphohistiocytosis. Ann. Pharmacother. 2023, 57, 867–879. [Google Scholar] [CrossRef]
- Chen, J.; Xiao, Z.-Z.; Shi, Q.; Wang, H.-M.; He, F.; Zhang, J.-Y. Risk factors associated with adverse pregnancy outcomes in patients with new-onset systemic lupus erythematosus during pregnancy. Lupus 2021, 30, 393–402. [Google Scholar] [CrossRef]
- Lu, J.; Xu, D.; Wan, Q.; Chen, H. Pregnancy outcomes and risk factors analysis in patients with systemic lupus erythematous. BMC Pregnancy Childbirth 2024, 24, 495. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Committee Opinion No. 819: Informed Consent and Shared Decision Making in Obstetrics and Gynecology. Obstet. Gynecol. 2021, 137, e34–e42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Analysis | On Admission | Before CS Therapy | After 6th CYC Pulse | Reference Range | |
|---|---|---|---|---|---|
| Complete blood count | WBC | 2.9 | 2.8 | 4.3 | 3.4–9.7 × 109/L |
| th | 2.3 | 2.2 | 2.5 | 2.1–6.5 × 109/L | |
| Ly | 0.4 | 0.05 | 1.2 | 1.2–3.4 × 109/L | |
| RBC | 3.26 | 3.22 | 3.95 | 3.86–5.08 × 1012/L | |
| Hb | 92 | 82 | 114 | 119–157 g/L | |
| PLT | 259 | 113 | 277 | 150–450 × 109/L | |
| Markers of inflammation | ESR | - | 100 | 42 | <10 mm/h |
| CRP | 51.7 | 55.5 | 10.3 | <5 mg/L | |
| Ferritin | 1262.3 | 1648.3 | 163.5 | 4.6–204 µg/L | |
| Liver function | AST | 145 | 189 | 47 | <37 U/L |
| ALT | 85 | 91 | 74 | <41 U/L | |
| GGT | 277 | 255 | 113 | <38 U/L | |
| ALP | 342 | - | 98 | 40–120 U/L | |
| TGs | - | 2.11 | 1.92 | 0–1.7 mmol/L | |
| Kidney function | Urea | 1.9 | 2.1 | 4.7 | 2.5–7.5 mmol/L |
| Creatinine | 40 | 41 | 60 | 45–84 umol/L | |
| eGFR | >60 | >60 | >60 | >60 mL/min/ 1.73 m2 | |
| Urine sediment | - | Erythrocytes leucocytes | Proteins, hemoglobin erythrocyte leucocytes | - | |
| 24 h-proteiuria (g/24 h) | - | 2.03 | 3.83 | <0.5 g/day | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plavsic, A.; Miskovic, R.; Jovanovic, D.; Karic, U.; Jovicic, Z.; Radovic, S.; Drazic, A.; Dasic, A.; Arandjelovic, S. Life-Threatening Macrophage Activation Syndrome in Pregnancy: First Manifestation of SLE Induced by Parvovirus B19. Int. J. Mol. Sci. 2025, 26, 5406. https://doi.org/10.3390/ijms26115406
Plavsic A, Miskovic R, Jovanovic D, Karic U, Jovicic Z, Radovic S, Drazic A, Dasic A, Arandjelovic S. Life-Threatening Macrophage Activation Syndrome in Pregnancy: First Manifestation of SLE Induced by Parvovirus B19. International Journal of Molecular Sciences. 2025; 26(11):5406. https://doi.org/10.3390/ijms26115406
Chicago/Turabian StylePlavsic, Aleksandra, Rada Miskovic, Dragana Jovanovic, Uros Karic, Zikica Jovicic, Sara Radovic, Ana Drazic, Aleksandra Dasic, and Snezana Arandjelovic. 2025. "Life-Threatening Macrophage Activation Syndrome in Pregnancy: First Manifestation of SLE Induced by Parvovirus B19" International Journal of Molecular Sciences 26, no. 11: 5406. https://doi.org/10.3390/ijms26115406
APA StylePlavsic, A., Miskovic, R., Jovanovic, D., Karic, U., Jovicic, Z., Radovic, S., Drazic, A., Dasic, A., & Arandjelovic, S. (2025). Life-Threatening Macrophage Activation Syndrome in Pregnancy: First Manifestation of SLE Induced by Parvovirus B19. International Journal of Molecular Sciences, 26(11), 5406. https://doi.org/10.3390/ijms26115406