
Advances in Nanotechnology-Based Cisplatin Delivery for ORL Cancers: A Comprehensive Review

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
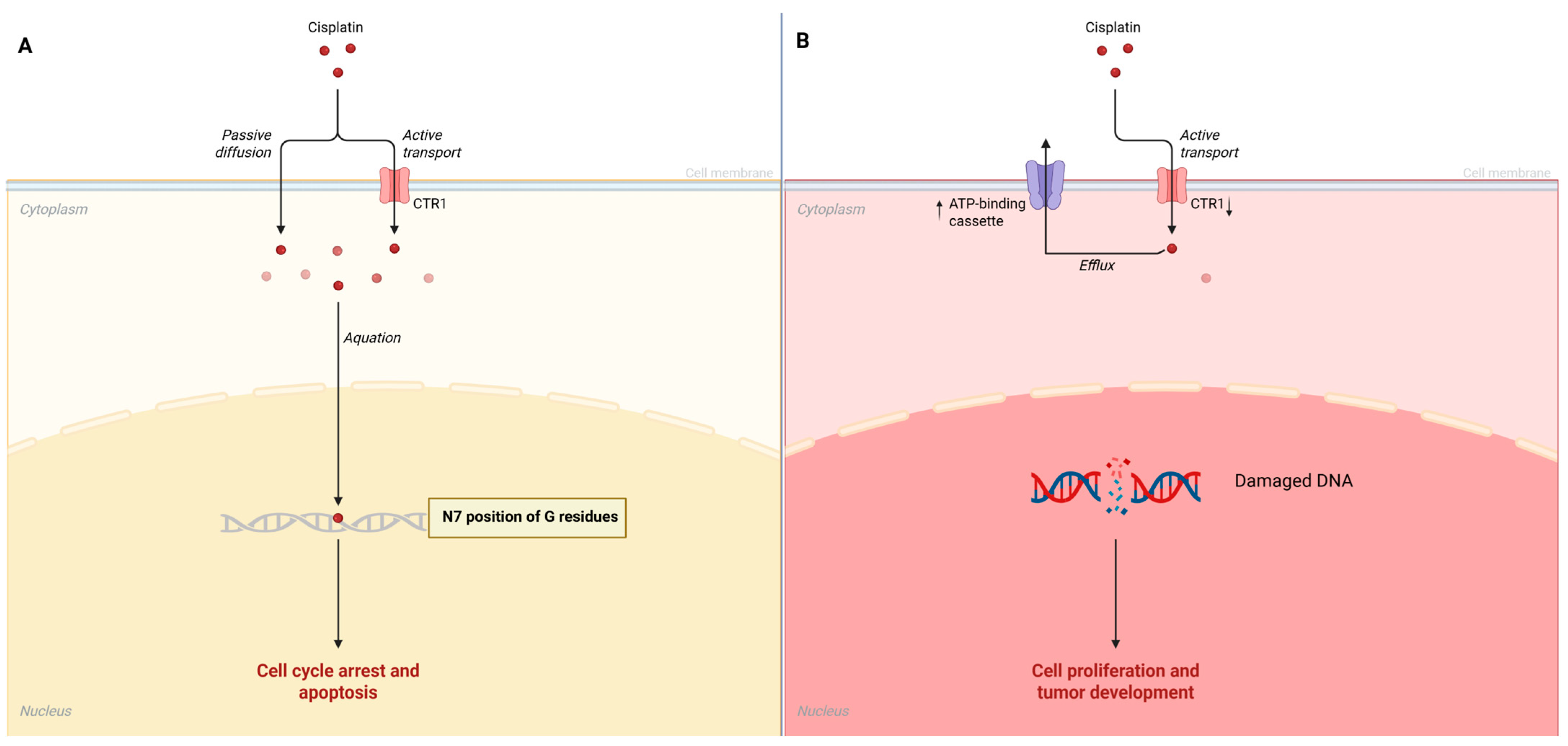
3. Mechanisms of Cisplatin Action and Resistance
4. Nanotechnology in Cisplatin Delivery
5. Current Clinical and Preclinical Studies

{kind=link}
{kind=link}
| Aspect | Nanotechnology-Based Approach | Nanocarrier Type | Study Model | Type of Cancer | Advantages | References |
|---|---|---|---|---|---|---|
| Drug Bioavailability and Pharmacokinetics | Nanoparticles encapsulating cisplatin | Lipid-based nanoparticles | In vitro, in vivo | ORL cancer, ovarian cancer | Protect cisplatin from degradation, prolong systemic circulation, and improve bioavailability at the tumor site, particularly in OSCC treatment. | [44,73,74] |
| Specificity and Targeting | Targeted delivery via functionalized nanoparticles (e.g., folic acid conjugation) | Polymeric particles, mesoporous silica particles | In vitro | Cervical cancer (HeLa cell line) | Enhanced drug delivery to cancer cells that overexpress receptors, improving efficacy while minimizing off-target effects and reducing systemic toxicity. | [46,75] |
| Overcoming Drug Resistance | Nanoparticle-based systems evading efflux pumps | Polymeric particles, mesoporous silica particles | In vitro | Oral cancer | Prevent drug resistance by facilitating drug accumulation inside cancer cells, bypassing efflux mechanisms like drug efflux pumps. | [29,43] |
| Controlled Release Systems | Redox-responsive mesoporous silica nanoparticles | Mesoporous silica nanoparticles | In vitro | Cervical cancer (HeLa cell line) | Release cisplatin in reducing environments of cancer cells, enhancing cytotoxicity against malignant cells while minimizing systemic exposure. | [46] |
| Biocompatibility and Pharmacokinetic Modulation | Custom nanoparticle systems (e.g., solid lipid nanoparticles) | Lipid nanoparticles, polymeric nanoparticles | In vitro | Various ORL cancer, ovarian cancer cell | Modify drug release profiles, enhance solubility and stability, and improve oral bioavailability, ensuring more efficient chemotherapy in oral cancer. | [47,74] |
| Combination Therapies | Combination of cisplatin with other therapeutic agents (antioxidants, immune modulators) | Organic nanoparticles, polymeric nanoparticles, lipid-based nanoparticles | In vitro, in vivo | Oral cancer, laryngeal cancers | Enhance overall cytotoxicity and counteract chemoresistance by integrating other therapeutic agents within nanoparticles, boosting the effectiveness of cisplatin. | [62,76,77] |
| Multifunctional Platforms for Diagnostics and Therapy | Nanoparticles integrating imaging agents | Gold nanoparticles, inorganic nanoparticles, polymeric nanoparticles | In vitro | Laryngeal cancer | Enable real-time monitoring of treatment efficacy, allowing adaptive strategies based on tumor response, optimizing treatment outcomes. | [43,78] |
| Stimuli-Responsive Release Mechanisms | Tumor-specific signal-responsive nanocarriers (e.g., pH-sensitive or enzyme-responsive systems) | Polymeric nanoparticles, drug-delivery platforms | In vitro | Various ORL cancers | Enable precise drug release within the tumor, enhancing therapeutic efficacy and minimizing systemic toxicity by evading healthy tissues. | [79] |
6. Challenges and Future Perspectives
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Lee, S.C.; Tang, I.P.; Avatar, S.P.; Ahmad, N.; Selva, K.S.; Tay, K.K.; Vikneswaran, T.; Tan, T.Y. Head and Neck Cancer: Possible Causes for Delay in Diagnosis and Treatment. Med. J. Malays. 2011, 66, 101–104. [Google Scholar]
- Labani-Motlagh, A.; Ashja-Mahdavi, M.; Loskog, A. The Tumor Microenvironment: A Milieu Hindering and Obstructing Antitumor Immune Responses. Front. Immunol. 2020, 11, 940. [Google Scholar] [CrossRef]
- Zhao, Y.; Shen, M.; Wu, L.; Yang, H.; Yao, Y.; Yang, Q.; Du, J.; Liu, L.; Li, Y.; Bai, Y. Stromal Cells in the Tumor Microenvironment: Accomplices of Tumor Progression? Cell Death Dis. 2023, 14, 587. [Google Scholar] [CrossRef]
- Chen, Z.; Han, F.; Du, Y.; Shi, H.; Zhou, W. Hypoxic Microenvironment in Cancer: Molecular Mechanisms and Therapeutic Interventions. Sig. Transduct. Target Ther. 2023, 8, 70. [Google Scholar] [CrossRef]
- Babar, Q.; Saeed, A.; Tabish, T.A.; Sarwar, M.; Thorat, N.D. Targeting the Tumor Microenvironment: Potential Strategy for Cancer Therapeutics. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2023, 1869, 166746. [Google Scholar] [CrossRef]
- Seager, R.J.; Hajal, C.; Spill, F.; Kamm, R.D.; Zaman, M.H. Dynamic Interplay between Tumour, Stroma and Immune System Can Drive or Prevent Tumour Progression. Converg. Sci. Phys. Oncol. 2017, 3, 034002. [Google Scholar] [CrossRef]
- Marallano, V.; Ughetta, M.E.; Tejero, R.; Nanda, S.; Ramalingam, R.; Stalbow, L.; Sattiraju, A.; Huang, Y.; Ramakrishnan, A.; Shen, L.; et al. Hypoxia Drives Shared and Distinct Transcriptomic Changes in Two Invasive Glioma Stem Cell Lines. Sci. Rep. 2024, 14, 7246. [Google Scholar] [CrossRef]
- Noman, M.Z.; Hasmim, M.; Lequeux, A.; Xiao, M.; Duhem, C.; Chouaib, S.; Berchem, G.; Janji, B. Improving Cancer Immunotherapy by Targeting the Hypoxic Tumor Microenvironment: New Opportunities and Challenges. Cells 2019, 8, 1083. [Google Scholar] [CrossRef]
- Wang, L.; Mosel, A.J.; Oakley, G.G.; Peng, A. Deficient DNA Damage Signaling Leads to Chemoresistance to Cisplatin in Oral Cancer. Mol. Cancer Ther. 2012, 11, 2401–2409. [Google Scholar] [CrossRef]
- Bader, J.E.; Voss, K.; Rathmell, J.C. Targeting Metabolism to Improve the Tumor Microenvironment for Cancer Immunotherapy. Mol. Cell 2020, 78, 1019–1033. [Google Scholar] [CrossRef]
- Lin, W.; Wu, S.; Chen, X.; Ye, Y.; Weng, Y.; Pan, Y.; Chen, Z.; Chen, L.; Qiu, X.; Qiu, S. Characterization of Hypoxia Signature to Evaluate the Tumor Immune Microenvironment and Predict Prognosis in Glioma Groups. Front. Oncol. 2020, 15, 796. [Google Scholar] [CrossRef]
- Xu, Y.; Luo, C.; Wang, J.; Chen, L.; Chen, J.; Chen, T.; Zeng, Q. Application of Nanotechnology in the Diagnosis and Treatment of Bladder Cancer. J. Nanobiotechnol. 2021, 19, 393. [Google Scholar] [CrossRef]
- Khouzam, R.A.; Brodaczewska, K.; Filipiak-Duliban, A.; Zeinelabdin, N.A.; Buart, S.; Szczylik, C.; Kiéda, C.; Chouaib, S. Tumor Hypoxia Regulates Immune Escape/Invasion: Influence on Angiogenesis and Potential Impact of Hypoxic Biomarkers on Cancer Therapies. Front. Immunol. 2021, 11, 613114. [Google Scholar] [CrossRef]
- Cao, M.; Xiao, L.; Chen, S.; Huang, J. Characterization of Hypoxia-Responsive States in Ovarian Cancer to Identify Hot Tumors and Aid Adjuvant Therapy. Discov. Oncol. 2024, 15, 23. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Y.; Chen, C.; Zhao, S.; Zhang, X.; Zhang, J.; Yan, Y. Hypoxia Score for Predicting Prognosis and Tumor Response to Immunotherapy in Bladder Urothelial Carcinoma. Res. Sq. 2022. preprint. [Google Scholar] [CrossRef]
- Jayaprakash, P.; Ai, M.; Liu, A.; Budhani, P.; Bartkowiak, T.; Sheng, J.; Ager, C.R.; Nicholas, C.; Jaiswal, A.R.; Sun, Y.; et al. Targeted Hypoxia Reduction Restores T Cell Infiltration and Sensitizes Prostate Cancer to Immunotherapy. J. Clin. Investig. 2018, 128, 5137–5149. [Google Scholar] [CrossRef]
- Ranasinghe, R.; Mathai, M.L.; Zulli, A. Cisplatin for Cancer Therapy and Overcoming Chemoresistance. Heliyon 2022, 8, e10608. [Google Scholar] [CrossRef]
- Brown, A.; Kumar, S.; Tchounwou, P.B. Cisplatin-Based Chemotherapy of Human Cancers. J. Cancer Sci. Ther. 2019, 11, 97. [Google Scholar]
- Dasari, S.; Bernard Tchounwou, P. Cisplatin in Cancer Therapy: Molecular Mechanisms of Action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef]
- Makovec, T. Cisplatin and beyond: Molecular Mechanisms of Action and Drug Resistance Development in Cancer Chemotherapy. Radiol. Oncol. 2019, 53, 148–158. [Google Scholar] [CrossRef]
- Aldossary, S.A. Review on Pharmacology of Cisplatin: Clinical Use, Toxicity and Mechanism of Resistance of Cisplatin. Biomed. Pharmacol. J. 2019, 12, 7–15. [Google Scholar] [CrossRef]
- Faig, J.; Haughton, M.; Taylor, R.C.; D’Agostino, R.B.J.; Whelen, M.J.; Porosnicu Rodriguez, K.A.; Bonomi, M.; Murea, M.; Porosnicu, M. Retrospective Analysis of Cisplatin Nephrotoxicity in Patients With Head and Neck Cancer Receiving Outpatient Treatment With Concurrent High-Dose Cisplatin and Radiotherapy. Am. J. Clin. Oncol. 2018, 41, 432. [Google Scholar] [CrossRef]
- Paken, J.; Govender, C.D.; Pillay, M.; Sewram, V. Cisplatin-Associated Ototoxicity: A Review for the Health Professional. J. Toxicol. 2016, 2016, 1–13. [Google Scholar] [CrossRef]
- Verstappen, C.C.P.; Heimans, J.J.; Hoekman, K.; Postma, T.J. Neurotoxic Complications of Chemotherapy in Patients with Cancer. Drugs 2003, 63, 1549–1563. [Google Scholar] [CrossRef]
- Chen, W.; Peng, L.; Zeng, X.; Wen, W.; Sun, W. Predictors of Myelosuppression for Patients with Head and Neck Squamous Cell Carcinoma After Induction Chemotherapy. Clin. Med. Insights Oncol. 2024, 18, 11795549231219497. [Google Scholar] [CrossRef]
- Stewart, D.J. Mechanisms of Resistance to Cisplatin and Carboplatin. Crit. Rev. Oncol. Hematol. 2007, 63, 12–31. [Google Scholar] [CrossRef]
- Chen, S.-H.; Chang, J.-Y. New Insights into Mechanisms of Cisplatin Resistance: From Tumor Cell to Microenvironment. Int. J. Mol. Sci. 2019, 20, 4136. [Google Scholar] [CrossRef]
- Chang, P.-Y.; Peng, S.-F.; Lee, C.-Y.; Lu, C.-C.; Tsai, S.-C.; Shieh, T.-M.; Wu, T.-S.; Tu, M.-G.; Chen, M.Y.; Yang, J.-S. Curcumin-Loaded Nanoparticles Induce Apoptotic Cell Death through Regulation of the Function of MDR1 and Reactive Oxygen Species in Cisplatin-Resistant CAR Human Oral Cancer Cells. Int. J. Oncol. 2013, 43, 1141–1150. [Google Scholar] [CrossRef]
- Kumbar, V.M.; Muddapur, U.; Bin Muhsinah, A.; Alshehri, S.A.; Alshahrani, M.M.; Almazni, I.A.; Kugaji, M.S.; Bhat, K.; Peram, M.R.; Mahnashi, M.H.; et al. Curcumin-Encapsulated Nanomicelles Improve Cellular Uptake and Cytotoxicity in Cisplatin-Resistant Human Oral Cancer Cells. J. Funct. Biomater. 2022, 13, 158. [Google Scholar] [CrossRef]
- Fan, X.; Wang, T.; Ji, Z.; Li, Q.; Shen, H.; Wang, J. Synergistic Combination Therapy of Lung Cancer Using Lipid-Layered Cisplatin and Oridonin Co-Encapsulated Nanoparticles. Biomed. Pharmacother. 2021, 141, 111830. [Google Scholar] [CrossRef]
- Tchounwou, P.B.; Dasari, S.; Noubissi, F.K.; Ray, P.C.; Kumar, S. Advances in Our Understanding of the Molecular Mechanisms of Action of Cisplatin in Cancer Therapy. J. Exp. Pharmacol. 2021, 13, 303–328. [Google Scholar] [CrossRef]
- Lugones, Y.; Loren, P.; Salazar, L.A. Cisplatin Resistance: Genetic and Epigenetic Factors Involved. Biomolecules 2022, 12, 1365. [Google Scholar] [CrossRef]
- Schoeberl, A.; Gutmann, M.; Theiner, S.; Corte-Rodríguez, M.; Braun, G.; Vician, P.; Berger, W.; Koellensperger, G. The Copper Transporter CTR1 and Cisplatin Accumulation at the Single-Cell Level by LA-ICP-TOFMS. Front. Mol. Biosci. 2022, 9, 1055356. [Google Scholar] [CrossRef]
- Wang, S.; Yuan, S.; Hu, H.; Zhang, J.; Cao, K.; Wang, Y.; Liu, Y. Reactions of Cisplatin With Thioredoxin-1 Regulate Intracellular Redox Homeostasis. Inorg. Chem. 2024, 63, 11779–11787. [Google Scholar] [CrossRef]
- Dasari, S.; Njiki, S.; Mbemi, A.; Yedjou, C.G.; Tchounwou, P.B. Pharmacological Effects of Cisplatin Combination With Natural Products in Cancer Chemotherapy. Int. J. Mol. Sci. 2022, 23, 1532. [Google Scholar] [CrossRef]
- Raji, G.R.; Poyyakkara, A.; Krishnan, A.K.; Maurya, A.K.; Changmai, U.; Shankar, S.S.; Sameer Kumar, V.B. Horizontal Transfer of miR-643 From Cisplatin-Resistant Cells Confers Chemoresistance to Recipient Drug-Sensitive Cells by Targeting APOL6. Cells 2021, 10, 1341. [Google Scholar] [CrossRef]
- Balyapan, H.; Ak, G. Nanoparticle Targeting Strategies in Cancer Therapy. In Recent Progress in Pharmaceutical Nanobiotechnology: A Medical Perspective; Bentham Science Publishers: Sharjah, United Arab Emirates, 2023; Volume 8, pp. 223–238. [Google Scholar]
- Davoudi, M.; Jadidi, Y.; Moayedi, K.; Farrokhi, V.; Afrisham, R. Ameliorative Impacts of Polymeric and Metallic Nanoparticles on Cisplatin-Induced Nephrotoxicity: A 2011–2022 Review. J. Nanobiotechnol. 2022, 20, 504. [Google Scholar] [CrossRef]
- Soni, A.; Bhandari, M.P.; Tripathi, G.K.; Bundela, P.; Khiriya, P.K.; Khare, P.S.; Kashyap, M.K.; Dey, A.; Vellingiri, B.; Suresh, S.; et al. Nano-biotechnology in Tumour and Cancerous Disease: A Perspective Review. J. Cell. Mol. Med. 2023, 27, 737–762. [Google Scholar] [CrossRef]
- Wu, J.; Hu, Y.; Ye, H.; Zhang, S.; Zhu, J.; Ji, D.; Zhang, Y.; Ding, Y.; Huang, Z. One Stone Two Birds: Redox-Sensitive Colocalized Delivery of Cisplatin and Nitric Oxide Through Cascade Reactions. JACS Au 2022, 2, 2339–2351. [Google Scholar] [CrossRef]
- Motelică, L.; Voicu, G.; Chircov, C.; Surdu, V.-A.; Truşcă, R.; Vasile, B.Ș.; Ficai, D.; Oprea, O.; Marta, D.; Peteu, V.E.; et al. Aspartic Acid Functionalized Magnetic Nanoparticles for Enhanced Internalization in Tumoral Cell. J. Aust. Ceram. Soc. 2025, 61, 265–283. [Google Scholar] [CrossRef]
- Farooq, M.A.; Aquib, M.; Farooq, A.; Haleem Khan, D.; Joelle Maviah, M.B.; Sied Filli, M.; Kesse, S.; Boakye-Yiadom, K.O.; Mavlyanova, R.; Parveen, A.; et al. Recent Progress in Nanotechnology-Based Novel Drug Delivery Systems in Designing of Cisplatin for Cancer Therapy: An Overview. Artif. Cells Nanomed. Biotechnol. 2019, 47, 1674–1692. [Google Scholar] [CrossRef]
- Yu, H.; Tang, Z.; Zhang, D.; Song, W.; Zhang, Y.; Yang, Y.; Ahmad, Z.; Chen, X. Pharmacokinetics, Biodistribution and in Vivo Efficacy of Cisplatin Loaded Poly(l-Glutamic Acid)-g-Methoxy Poly(Ethylene Glycol) Complex Nanoparticles for Tumor Therapy. J. Control. Release 2015, 205, 89–97. [Google Scholar] [CrossRef]
- Liang, X.-J.; Meng, H.; Wang, Y.; He, H.; Meng, J.; Lu, J.; Wang, P.C.; Zhao, Y.; Gao, X.; Sun, B.; et al. Metallofullerene Nanoparticles Circumvent Tumor Resistance to Cisplatin by Reactivating Endocytosis. Proc. Natl. Acad. Sci. USA 2010, 107, 7449–7454. [Google Scholar] [CrossRef]
- Alvarez-Berríos, M.P.; Vivero-Escoto, J.L. In Vitro Evaluation of Folic Acid-Conjugated Redox-Responsive Mesoporous Silica Nanoparticles for the Delivery of Cisplatin. Int. J. Nanomed. 2016, 11, 6251–6265. [Google Scholar] [CrossRef]
- Shah, A.S.; Surnar, B.; Kolishetti, N.; Dhar, S. Intersection of Inorganic Chemistry and Nanotechnology for the Creation of New Cancer Therapies. Acc. Mater. Res. 2022, 3, 283–296. [Google Scholar] [CrossRef]
- Mensah, L.B.; Morton, S.W.; Li, J.; Xiao, H.; Quadir, M.A.; Elias, K.M.; Penn, E.; Richson, A.K.; Ghoroghchian, P.P.; Liu, J.; et al. Layer-by-layer Nanoparticles for Novel Delivery of Cisplatin and PARP Inhibitors for Platinum-based Drug Resistance Therapy in Ovarian Cancer. Bioeng Transl. Med. 2019, 4, e10131. [Google Scholar] [CrossRef]
- Hernández-Gil, J.; Cobaleda-Siles, M.; Zabaleta, A.; Salassa, L.; Calvo, J.; Mareque-Rivas, J.C. An Iron Oxide Nanocarrier Loaded With a Pt(IV) Prodrug and Immunostimulatory dsRNA for Combining Complementary Cancer Killing Effects. Adv. Healthc. Mater. 2015, 4, 1034–1042. [Google Scholar] [CrossRef]
- Bozeman, E.N.; Gao, N.; Qian, W.; Wang, A.Z.; Yang, L. Abstract 3635: Enhanced Intra-Tumoral Immune Cell Infiltration Following Tumor Targeted Delivery of Chemotherapy Using Theranostic Nanoparticles in an Orthotopic Mouse Pancreatic Model. Cancer Res. 2014, 74, 3635. [Google Scholar] [CrossRef]
- Hoffmann, C.; Shen, C.; Tourneau, C.L. Nanoparticle Therapy for Head and Neck Cancers. Curr. Opin. Oncol. 2022, 34, 177–184. [Google Scholar] [CrossRef]
- Xu, C.; Yu, Y.; Sun, Y.; Kong, L.; Yang, C.; Hu, M.; Yang, T.; Zhang, J.; Hu, Q.; Zhang, Z. Transformable Nanoparticle-Enabled Synergistic Elicitation and Promotion of Immunogenic Cell Death for Triple-Negative Breast Cancer Immunotherapy. Adv. Funct. Mater. 2019, 29, 1905213. [Google Scholar] [CrossRef]
- Fu, G.; Wu, Y.; Zhao, G.; Chen, X.; Xu, Z.; Sun, J.; Tian, J.; Cheng, Z.; Shi, Y.; Jin, B. Activation of cGAS-STING Signal to Inhibit the Proliferation of Bladder Cancer: The Immune Effect of Cisplatin. Cells 2022, 11, 3011. [Google Scholar] [CrossRef] [PubMed]
- Fu, G.; Chen, X.; Xu, Z.; Su, J.; Tian, J.; Shi, Y.; Xu, C.; Pan, H.; Jin, B. Cisplatin Inhibits Bladder Cancer Proliferation Through cGAS-STING Pathway. 2020. Available online: https://www.researchgate.net/publication/347859388_Cisplatin_Inhibits_Bladder_Cancer_Proliferation_Through_cGAS-STING_Pathway/fulltext/5fed0030a6fdccdcb81ae3e7/Cisplatin-Inhibits-Bladder-Cancer-Proliferation-Through-cGAS-STING-Pathway.pdf (accessed on 27 May 2025).
- Wang, W.; Yang, F.; Zhang, L.; Wang, M.; Yin, L.; Dong, X.; Xiao, H.; Xing, N. Targeting DNA Damage and Repair Machinery via Delivering WEE1 Inhibitor and Platinum (IV) Prodrugs to Stimulate STING Pathway for Maximizing Chemo-Immunotherapy in Bladder Cancer. Adv. Mater. 2024, 36, 2308762. [Google Scholar] [CrossRef] [PubMed]
- Pathak, R.; Wen, R.; Kolishetti, N.; Dhar, S. A Prodrug of Two Approved Drugs, Cisplatin and Chlorambucil, for Chemo War Against Cancer. Mol. Cancer Ther. 2017, 16, 625–636. [Google Scholar] [CrossRef]
- Zhao, Q.; Liang, G.; Guo, B.; Wang, W.; Yang, C.; Chen, D.; Yang, F.; Xiao, H.; Xing, N. Polyphotosensitizer-Based Nanoparticles With Michael Addition Acceptors Inhibiting GST Activity and Cisplatin Deactivation for Enhanced Chemotherapy and Photodynamic Immunotherapy. Adv. Sci. 2023, 10, 2300175. [Google Scholar] [CrossRef]
- Afrin, H.; Geetha Bai, R.; Kumar, R.; Ahmad, S.S.; Agarwal, S.K.; Nurunnabi, M. Oral Delivery of RNAi for Cancer Therapy. Cancer Metastasis Rev. 2023, 42, 699–724. [Google Scholar] [CrossRef]
- Tolue Ghasaban, F.; Maharati, A.; Zangouei, A.S.; Zangooie, A.; Moghbeli, M. MicroRNAs as the Pivotal Regulators of Cisplatin Resistance in Head and Neck Cancers. Cancer Cell Int. 2023, 23, 170. [Google Scholar] [CrossRef]
- Kumar, K.; Rani, V.; Mishra, M.; Chawla, R. New Paradigm in Combination Therapy of siRNA with Chemotherapeutic Drugs for Effective Cancer Therapy. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100103. [Google Scholar] [CrossRef]
- Vivero-Escoto, J.L.; Elnagheeb, M. Mesoporous Silica Nanoparticles Loaded with Cisplatin and Phthalocyanine for Combination Chemotherapy and Photodynamic Therapy in Vitro. Nanomaterials 2015, 5, 2302–2316. [Google Scholar] [CrossRef]
- Duan, X.; He, C.; Kron, S.J.; Lin, W. Nanoparticle Formulations of Cisplatin for Cancer Therapy. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2016, 8, 776–791. [Google Scholar] [CrossRef]
- Mohammadinezhad, F.; Talebi, A.; Allahyartorkaman, M.; Nahavandi, R.; Vesal, M.; Akbarzadeh, A. Preparation, Characterization and Cytotoxic Studies of Cisplatin-Containing Nanoliposomes on Breast Cancer Cell Lines. Asian Pac. J. Cancer Biol. 2023, 8, 155–159. [Google Scholar] [CrossRef]
- Zhao, C.; Cheng, R.; Yang, Z.; Tian, Z. Nanotechnology for Cancer Therapy Based on Chemotherapy. Molecules 2018, 23, 826. [Google Scholar] [CrossRef] [PubMed]
- Amreddy, N.; Babu, A.; Panneerselvam, J.; Srivastava, A.; Muralidharan, R.; Chen, A.; Zhao, Y.D.; Munshi, A.; Ramesh, R. Chemo-Biologic Combinatorial Drug Delivery Using Folate Receptor-Targeted Dendrimer Nanoparticles for Lung Cancer Treatment. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Ramani, S.M.; Penchalaneni, J.; Padma, K.R. Emerging Updates on Tracking New Landscapes in Nanotechnology for the Diagnosis and Ovarian Cancer Therapy. J. Assoc. Med. Sci. 2024, 57, 124–134. [Google Scholar] [CrossRef]
- Qiu, S.; Sun, L.; Zhang, Y.; Han, S. Downregulation of BAG3 Attenuates Cisplatin Resistance by Inhibiting Autophagy in Human Epithelial Ovarian Cancer Cells. Oncol. Lett. 2019, 18, 1969–1978. [Google Scholar] [CrossRef]
- Liu, H.-T.; Wang, T.; Hsu, Y.; Chou, C.; Huang, K.; Hsu, C.; Liang, H.; Chang, H.; Lee, T.; Tsai, P. Nanoparticulated Honokiol Mitigates Cisplatin-Induced Chronic Kidney Injury by Maintaining Mitochondria Antioxidant Capacity and Reducing Caspase 3-Associated Cellular Apoptosis. Antioxidants 2019, 8, 466. [Google Scholar] [CrossRef]
- Bei, M.F.; Domocoș, D.; Szilagyi, G.; Varga, D.M.; Pogan, M.D. Influence of Vitamins and Antioxidants in Oral Carcinogenesis – A Review. Pharmacophore 2023, 14, 39–45. [Google Scholar] [CrossRef]
- Wang, X.; Xiong, T.; Cui, M.; Li, N.; Li, Q.; Zhu, L.; Duan, S.; Wang, Y.; Guo, Y. A Novel Targeted Co-Delivery Nanosystem for Enhanced Ovarian Cancer Treatment via Multidrug Resistance Reversion and mTOR-Mediated Signaling Pathway. J. Nanobiotechnol. 2021, 19, 444. [Google Scholar] [CrossRef]
- Duan, Y.; Shen, C.; Zhang, Y.; Luo, Y. Advanced Diagnostic and Therapeutic Strategies in Nanotechnology for Lung Cancer. Front. Oncol. 2022, 12, 1031000. [Google Scholar] [CrossRef]
- Aftab, Z.; Bukhari, S.M.; Abubakar, M.; Sultan, H.M.; Zubair, M.; Abou Niaaj, M.A. Innovative Nanoparticle Synthesis and Multifaceted Applications in Medicine and Cancer Therapy. J. Clin. Nurs. Res. 2024, 8, 21–35. [Google Scholar] [CrossRef]
- Bortot, B.; Mongiat, M.; Valencic, E.; Dal Monego, S.; Licastro, D.; Crosera, M.; Adami, G.; Rampazzo, E.; Ricci, G.; Romano, F.; et al. Nanotechnology-Based Cisplatin Intracellular Delivery to Enhance Chemo-Sensitivity of Ovarian Cancer. Int. J. Nanomed. 2020, 15, 4793–4810. [Google Scholar] [CrossRef] [PubMed]
- Catanzaro, D.; Nicolosi, S.; Cocetta, V.; Salvalaio, M.; Pagetta, A.; Ragazzi, E.; Montopoli, M.; Pasut, G. Cisplatin Liposome and 6-Amino Nicotinamide Combination to Overcome Drug Resistance in Ovarian Cancer Cells. Oncotarget 2018, 9, 16847–16860. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Du, X.; Kleitz, F.; Qiao, S.Z. Cancer-Cell-Specific Nuclear-Targeted Drug Delivery by Dual-Ligand-Modified Mesoporous Silica Nanoparticles. Small 2015, 11, 5919–5926. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.M.; Madni, A.; Tahir, N.; Parveen, F.; Khan, S.; Jan, N.; Ali, A.; Abdurrahim, M.; Farooq, U.; Khan, M.I. Co-Delivery of Curcumin and Cisplatin to Enhance Cytotoxicity of Cisplatin Using Lipid-Chitosan Hybrid Nanoparticles. Int. J. Nanomed. 2020, 15, 2207–2217. [Google Scholar] [CrossRef]
- Tsvetkova, D.; Ivanova, S. Application of Approved Cisplatin Derivatives in Combination Therapy against Different Cancer Diseases. Molecules 2022, 27, 2466. [Google Scholar] [CrossRef]
- Sun, J.; Li, L.; Cai, W.; Chen, A.; Zhang, R. Multifunctional Hybrid Nanoprobe for Photoacoustic/PET/MR Imaging-Guided Photothermal Therapy of Laryngeal Cancer. ACS Appl. Bio Mater. 2021, 4, 5312–5323. [Google Scholar] [CrossRef]
- Rahim, M.A.; Jan, N.; Khan, S.; Shah, H.; Madni, A.; Khan, A.; Jabar, A.; Khan, S.; Elhissi, A.; Hussain, Z.; et al. Recent Advancements in Stimuli Responsive Drug Delivery Platforms for Active and Passive Cancer Targeting. Cancers 2021, 13, 670. [Google Scholar] [CrossRef]
- Xu, B.; Zeng, M.; Zeng, J.; Feng, J.; Yu, L. Meta-Analysis of Clinical Trials Comparing the Efficacy and Safety of Liposomal Cisplatin Versus Conventional Nonliposomal Cisplatin in Nonsmall Cell Lung Cancer (NSCLC) and Squamous Cell Carcinoma of the Head and Neck (SCCHN). Medicine 2018, 97, e13169. [Google Scholar] [CrossRef]
- Browning, R.J.; Thomas Reardon, P.J.; Parhizkar, M.; Pedley, R.; Edirisinghe, M.; Knowles, J.C.; Stride, E. Drug Delivery Strategies for Platinum-Based Chemotherapy. Acs Nano 2017, 11, 8560–8578. [Google Scholar] [CrossRef]
- Poy, D.; Akbarzadeh, A.; Shahmabadi, H.E.; Ebrahimifar, M.; Farhangi, A.A.; Zarabi, M.F.; Akbari, A.; Saffari, Z.; Siami, F. Preparation, Characterization, and Cytotoxic Effects of Liposomal Nanoparticles Containing Cisplatin: An in Vitro Study. Chem. Biol. Drug Des. 2016, 88, 568–573. [Google Scholar] [CrossRef]
- Deshpande, N.; Jayakannan, M. Cisplatin-Stitched Polysaccharide Vesicles for Synergistic Cancer Therapy of Triple Antagonistic Drugs. Biomacromolecules 2016, 18, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.; Ji, X.; Luo, J. Rational Nanocarrier Design Towards Clinical Translation of Cancer Nanotherapy. Biomed. Mater. 2021, 16, 032005. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.J.; Ciura, K.; Ma, Y.; Mikołajczyk, A.; Jagiełło, K.; Wan, Y.; Gao, Y.; Zheng, J.; Zhong, S.; Puzyn, T.; et al. Toward the Integration of Machine Learning and Molecular Modeling for Designing Drug Delivery Nanocarriers. Adv. Mater. 2024, 36, e2407793. [Google Scholar] [CrossRef] [PubMed]
| Feature | Lipid-Based NPs | Polymeric NPs | Inorganic NPs | Mesoporous Silica NPs | Extracellular Vesicles | Hybrid/Composite NPs |
|---|---|---|---|---|---|---|
| Biocompatibility | Excellent; reduced nephrotoxicity | Generally good; potential polymer toxicity | Moderate; long-term metal accumulation concerns | Moderate; biodegradability issues | Intrinsic; immune evasive | Variable, depending on component materials |
| Drug-loading capacity | Limited | High | Moderate | Very high (large pore volume for co-loading) | Low yield; heterogeneous cargo | Tunable via choice of polymer/lipid/metal blends |
| Release profile | Passive EPR-mediated accumulation | Controlled/sustained | Multifunctional (imaging + therapy) | Stimuli responsive | Natural cargo delivery; endogenous release cues | Synergistic release modes (e.g., burst + sustained) |
| Circulation stability | Challenged (stability in blood) | Batch-to-batch variability | Very high | Fine surface engineering | Moderate; stability varies with isolation method | Depends on formulation and core–shell architecture |
| Manufacturing complexity | Moderate | Moderate | High | Moderate | High (low yield, scalability issues) | High (multiple components and processing steps) |
| Safety/toxicity concerns | Generally low systemic toxicity | Polymer-related toxicity possible | Metal accumulation; unclear long-term fate | Silicosis risk; slow biodegradation | Low immunogenicity; cargo heterogeneity risks | Regulatory pathway often unclear |
| Tumor-targeting specificity | Passive (EPR)—moderate; active with ligands possible | Passive + ligand-directed active targeting | Mostly passive; some active via surface chemistry | Passive; active via folate or antibody conjugates | Highly specific via native membrane proteins | Depends entirely on the chosen targeting ligands |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgovan, A.I.; Boia, E.R.; Motofelea, A.C.; Orasan, A.; Negru, M.C.; Guran, K.; Para, D.M.; Sandu, D.; Ciocani, S.; Sitaru, A.M.; et al. Advances in Nanotechnology-Based Cisplatin Delivery for ORL Cancers: A Comprehensive Review. Int. J. Mol. Sci. 2025, 26, 5261. https://doi.org/10.3390/ijms26115261
Morgovan AI, Boia ER, Motofelea AC, Orasan A, Negru MC, Guran K, Para DM, Sandu D, Ciocani S, Sitaru AM, et al. Advances in Nanotechnology-Based Cisplatin Delivery for ORL Cancers: A Comprehensive Review. International Journal of Molecular Sciences. 2025; 26(11):5261. https://doi.org/10.3390/ijms26115261
Chicago/Turabian StyleMorgovan, Anda Ioana, Eugen Radu Boia, Alexandru Catalin Motofelea, Alexandru Orasan, Mihaela Cristina Negru, Kristine Guran, Diana Maria Para, Daniela Sandu, Sonja Ciocani, Adrian Mihail Sitaru, and et al. 2025. "Advances in Nanotechnology-Based Cisplatin Delivery for ORL Cancers: A Comprehensive Review" International Journal of Molecular Sciences 26, no. 11: 5261. https://doi.org/10.3390/ijms26115261
APA StyleMorgovan, A. I., Boia, E. R., Motofelea, A. C., Orasan, A., Negru, M. C., Guran, K., Para, D. M., Sandu, D., Ciocani, S., Sitaru, A. M., & Balica, N. C. (2025). Advances in Nanotechnology-Based Cisplatin Delivery for ORL Cancers: A Comprehensive Review. International Journal of Molecular Sciences, 26(11), 5261. https://doi.org/10.3390/ijms26115261