
Olfactory Perception in Parkinson’s Disease: The Impact of GBA1 Variants (Sidransky Syndrome)

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Results
2.1. Demography and Clinical Characteristics
2.2. Percentage of Identifications of the Different Smells Between the Groups
2.3. Difference in Smell Perception by Sex
2.4. Correlation Between Smell and Other Non-Motor Symptoms of PD
3. Discussion
4. Materials and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BSIT® | Brief Smell Identification Test |
| GD | Gaucher disease |
| GBA1 | Glucocerebrosidase type 1 |
| GBA1-PD | GBA1-associated PD |
| iPD | Idiopathic Parkinson’s disease |
| IRB | Institutional review |
| LDS | Least significant difference |
| LSD | Least significant difference |
| MDS-mUPDRS | motor part of the Movement Disorder Society Unified Parkinson’s Disease Rating Scale |
| PD | Parkinson’s disease |
| p-value | Probability value |
| REM | Rapid eye movement (REM) |
| RBD | REM sleep behavioral disorder |
| SiS | Sidransky syndrome |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
Appendix A
| Gene | Name |
| ADCY5 | Adenylate cyclase 5 |
| ANO3 | Anoctamin 3 |
| APOE | Apolipoprotein E |
| APP | Amyloid Beta Precursor Protein |
| ATP13A2 | ATPase Cation Transporting 13A2 |
| ATP1A3 | ATPase Na+/K+ Transporting Subunit Alpha 3 |
| ATP9A | ATPase Phospholipid Transporting 9A |
| C19orf12 | Chromosome 19 Open Reading Frame 12) |
| CHCHD2 | Coiled-Coil-Helix-Coiled-Coil-Helix Domain Containing 2 |
| CNEP1R1 | CTD Nuclear Envelope Phosphatase 1 Regulatory Subunit 1 |
| COX20 | Cytochrome c Oxidase Assembly Factor |
| CTDNEP1 | CTD Nuclear Envelope Phosphatase 1 |
| DCTN1 | Dynactin Subunit 1 |
| DJ1 (PARK7) | Parkinsonism-associated Deglycase |
| DNAJC13 | DnaJ Heat Shock Protein Family (Hsp40) Member C13 |
| DNAJC6 | DnaJ Heat Shock Protein Family (Hsp40) Member C6 |
| ELOVL7 | ELOVL Fatty Acid Elongase 7 |
| FBXO47 | F-Box Protein 47 |
| FBXO7 | F-Box Protein 7 |
| GAK | Cyclin G-Associated Kinase |
| GBA | Glucosylceramidase beta |
| GCDH | Glutaryl-CoA Dehydrogenase |
| GCH1 | GTP Cyclohydrolase 1 |
| GNAL | G Protein Subunit Alpha L |
| GNE | Glucosamine (UDP-N-Acetyl)-2-Epimerase/N-Acetylmannosamine Kinase |
| GRN | Granulin Precursor |
| HPCA | Hippocalcin |
| KCTD17 | Potassium Channel Tetramerization Domain Containing 17 |
| KMT2B | Lysine Methyltransferase 2B |
| LPIN1 | Lipin 1 |
| LPIN2 | Lipin 2 |
| LPIN3 | Lipin 3 |
| LRRK2 | Leucine-rich Repeat Kinase 2 |
| MAPT | Microtubule-associated Protein Tau |
| MCCC1 | Methylcrotonoyl-CoA Carboxylase 1 |
| MCOLN1 | Mucolipin 1 |
| NPC1 | NPC Intracellular Cholesterol Transporter 1 |
| PANK2 | Pantothenate Kinase 2 |
| PARK2 | Parkinson Disease 2 |
| PDE8B | Phosphodiesterase 8B |
| PDGFB | Platelet-derived Growth Factor Subunit B |
| PDGFRB | Platelet-derived Growth Factor Receptor Beta |
| PINK1 | Mitochondrial Serine/Threonine-protein Kinase |
| PLA2G6 | Phospholipase A2 Group VI |
| POLG | DNA Polymerase Subunit Gamma |
| SLC19A3 | Solute Carrier Family 19 Member 3 |
| SLC20A2 | Solute Carrier Family 20 Member 2 |
| SLC30A10 | Solute Carrier Family 30 Member 10 |
| SLC39A14 | Solute Carrier Family 9 Member 14 |
| SLC6A3 | Solute Carrier Family 6 Member 3 |
| SNCA | Synuclein Alpha |
| SNCB | Synuclein Beta |
| SYN1 | Synapsin I |
| SYNJ1 | Synaptojanin 1 |
| TAF1 | TATA-Box Binding Protein Associated Factor 1 |
| TDP43 | TAR DNA Binding Protein 43 |
| THAP1 | THAP Domain Containing 1 |
| TOR1A | Torsin Family 1 Member A |
| VAC14 | VAC14 Component Of PIKFYVE Complex |
| VPS13C | Vacuolar Protein Sorting 13 Homolog C |
| VPS35 | Vacuolar Protein Sorting-associated Protein 35 |
| XPR1 | Xenotropic And Polytropic Retrovirus Receptor 1 |
References
- Morley, J.F.; Duda, J.E. Olfaction as a Biomarker in Parkinson’s Disease. Biomark. Med. 2010, 4, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L. Biomarkers for Early Detection of Parkinson Disease: A Scent of Consistency with Olfactory Dysfunction. Neurology 2017, 89, 1432–1434. [Google Scholar] [CrossRef]
- Tarakad, A.; Jankovic, J. Anosmia and Ageusia in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 133, 541–556. [Google Scholar] [PubMed]
- Becker-Cohen, M.; Zimran, A.; Dinur, T.; Tiomkin, M.; Cozma, C.; Rolfs, A.; Arkadir, D.; Shulman, E.; Manor, O.; Paltiel, O.; et al. A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk. Int. J. Mol. Sci. 2022, 23, 12211. [Google Scholar] [CrossRef]
- Doty, R.L. Olfaction in Parkinson’s Disease and Related Disorders. Neurobiol. Dis. 2012, 46, 527–552. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Del Tredici, K.; Rüb, U.; de Vos, R.A.I.; Jansen Steur, E.N.H.; Braak, E. Staging of Brain Pathology Related to Sporadic Parkinson’s Disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Chen, S.; Tan, H.; Wu, Z.; Sun, C.; He, J.; Li, X.; Shao, M. Imaging of Olfactory Bulb and Gray Matter Volumes in Brain Areas Associated with Olfactory Function in Patients with Parkinson’s Disease and Multiple System Atrophy. Eur. J. Radiol. 2014, 83, 564–570. [Google Scholar] [CrossRef]
- Brodoehl, S.; Klingner, C.; Volk, G.F.; Bitter, T.; Witte, O.W.; Redecker, C. Decreased Olfactory Bulb Volume in Idiopathic Parkinson’s Disease Detected by 3.0-Tesla Magnetic Resonance Imaging. Mov. Disord. 2012, 27, 1019–1025. [Google Scholar] [CrossRef]
- Wattendorf, E.; Welge-Lüssen, A.; Fiedler, K.; Bilecen, D.; Wolfensberger, M.; Fuhr, P.; Hummel, T.; Westermann, B. Olfactory Impairment Predicts Brain Atrophy in Parkinson’s Disease. J. Neurosci. 2009, 29, 15410–15413. [Google Scholar] [CrossRef]
- Skrahin, A.; Horowitz, M.; Istaiti, M.; Skrahina, V.; Lukas, J.; Yahalom, G.; Cohen, M.E.; Revel-Vilk, S.; Goker-Alpan, O.; Becker-Cohen, M.; et al. GBA1-Associated Parkinson’s Disease Is a Distinct Entity. Int. J. Mol. Sci. 2024, 25, 7102. [Google Scholar] [CrossRef]
- Smith, L.; Schapira, A.H.V. GBA Variants and Parkinson Disease: Mechanisms and Treatments. Cells 2022, 11, 1261. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Zhan, X.; Zhou, H.; Guo, Z.; Xing, Y.; Yin, H.; Xue, C.; Wu, J.; Liu, W. Comparing the Effects of GBA Variants and Onset Age on Clinical Features and Progression in Parkinson’s Disease. CNS Neurosci. Ther. 2024, 30, e14387. [Google Scholar] [CrossRef] [PubMed]
- Yahalom, G.; Greenbaum, L.; Israeli-Korn, S.; Fay-Karmon, T.; Livneh, V.; Ruskey, J.A.; Roncière, L.; Alam, A.; Gan-Or, Z.; Hassin-Baer, S. Carriers of Both GBA and LRRK2 Mutations, Compared to Carriers of Either, in Parkinson’s Disease: Risk Estimates and Genotype-Phenotype Correlations. Park. Relat. Disord. 2019, 62, 179–184. [Google Scholar] [CrossRef]
- Cilia, R.; Tunesi, S.; Marotta, G.; Cereda, E.; Siri, C.; Tesei, S.; Zecchinelli, A.L.; Canesi, M.; Mariani, C.B.; Meucci, N.; et al. Survival and Dementia in GBA-Associated Parkinson’s Disease: The Mutation Matters. Ann. Neurol. 2016, 80, 662–673. [Google Scholar] [CrossRef]
- Brockmann, K.; Srulijes, K.; Hauser, A.-K.; Schulte, C.; Csoti, I.; Gasser, T.; Berg, D. GBA-Associated PD Presents with Nonmotor Characteristics. Neurology 2011, 77, 276–280. [Google Scholar] [CrossRef]
- Nishioka, K.; Ross, O.A.; Vilariño-Güell, C.; Cobb, S.A.; Kachergus, J.M.; Mann, D.M.A.; Snowden, J.; Richardson, A.M.T.; Neary, D.; Robinson, C.A.; et al. Glucocerebrosidase Mutations in Diffuse Lewy Body Disease. Park. Relat. Disord. 2011, 17, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Parkkinen, L.; Neumann, J.; O’Sullivan, S.S.; Holton, J.L.; Revesz, T.; Hardy, J.; Lees, A.J. Glucocerebrosidase Mutations Do Not Cause Increased Lewy Body Pathology in Parkinson’s Disease. Mol. Genet. Metab. 2011, 103, 410–412. [Google Scholar] [CrossRef]
- McNeill, A.; Duran, R.; Proukakis, C.; Bras, J.; Hughes, D.; Mehta, A.; Hardy, J.; Wood, N.W.; Schapira, A.H.V. Hyposmia and Cognitive Impairment in Gaucher Disease Patients and Carriers. Mov. Disord. 2012, 27, 526–532. [Google Scholar] [CrossRef]
- Lopez, G.J.; Lichtenberg, J.; Tayebi, N.; Ryan, E.; Lecker, A.L.; Sidransky, E. Longitudinal Evaluation of Olfactory Function in Individuals with Gaucher Disease and GBA1 Mutation Carriers with and without Parkinson’s Disease. Front. Neurol. 2022, 13, 1039214. [Google Scholar] [CrossRef]
- Cao, M.; Li, Y.; Gu, Z.; Mi, T.; Xu, X.; Ma, C.; Chen, M.; Wu, M.; Chan, P. Validation of the Utility of the Brief Smell Identification Test in Chinese Patients with Parkinson’s Disease. J. Clin. Neurosci. 2019, 60, 68–72. [Google Scholar] [CrossRef]
- Double, K.L.; Rowe, D.B.; Hayes, M.; Chan, D.K.Y.; Blackie, J.; Corbett, A.; Joffe, R.; Fung, V.S.; Morris, J.; Halliday, G.M. Identifying the Pattern of Olfactory Deficits in Parkinson Disease Using the Brief Smell Identification Test. Arch. Neurol. 2003, 60, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Daum, R.F.; Sekinger, B.; Kobal, G.; Lang, C.J. Olfactory Testing with “Sniffin’’ Sticks” for Clinical Diagnosis of Parkinson Disease. Nervenarzt 2000, 71, 643–650. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| GD or GBA1 Healthy Carriers | Sidransky Syndrome | iPD | Healthy Controls | Total | p-Value | |
|---|---|---|---|---|---|---|
| N | 41 | 18 | 30 | 30 | 119 | |
| Males | 21 | 12 | 21 | 13 | 67 | |
| Age, years (SD) | 53.6 (9.8) | 58.0 (11.0) | 70.6 (8.2) | 56.2 (9.7) | 59.2 (11.7) | p < 0.001 |
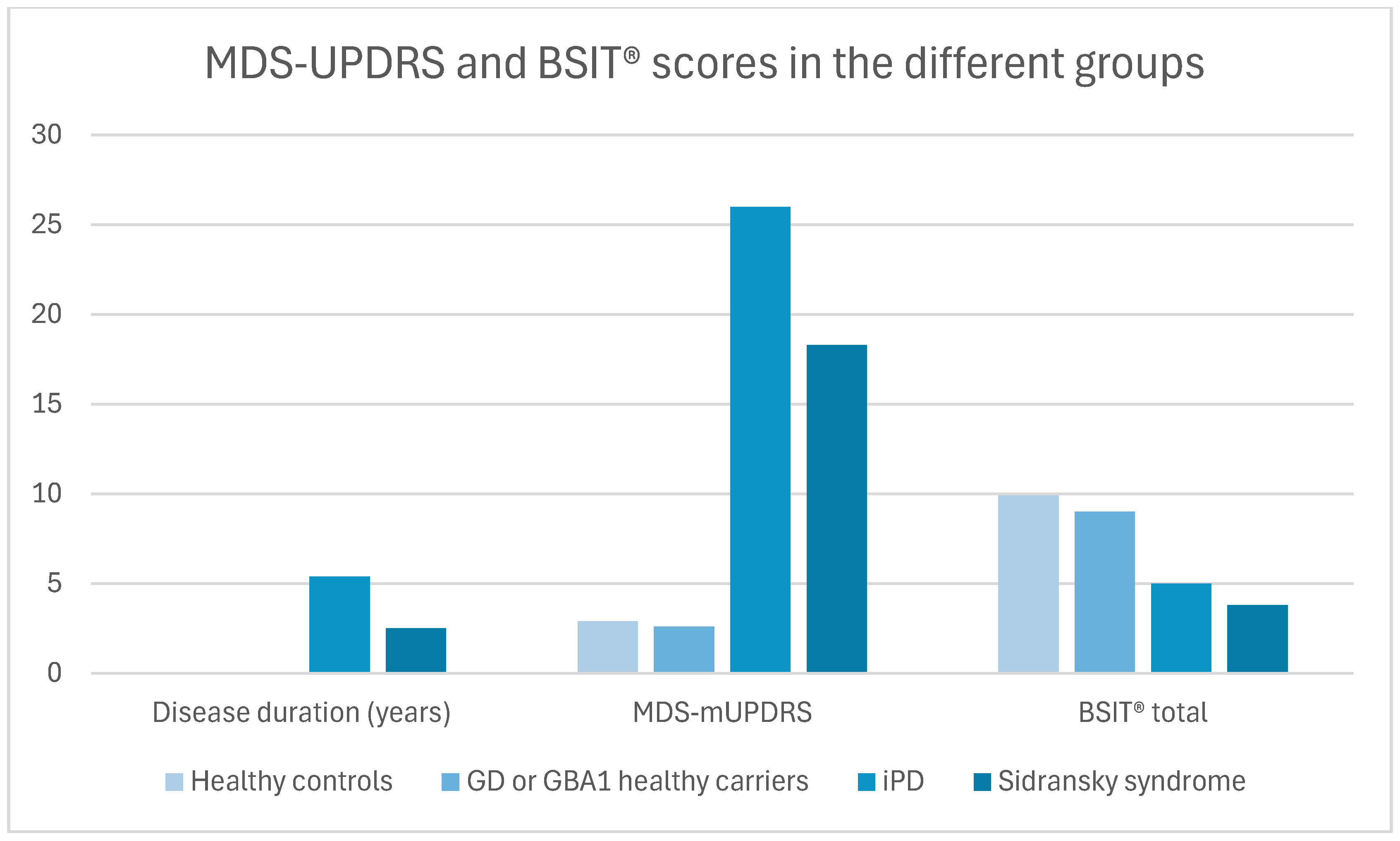
| Disease duration, years (SD) | NA | 2.5 (2.2) | 5.4 (4.9) | NA | 4.6 (4.5) | 0.12 |
| MDS-mUPDRS | 2.6 (3.8) | 18.3 (8.5) | 26.0 (9.5) | 2.9 (3.3) | 11.5 (12.3) | p < 0.001 * p = 0.02 |
| BSIT® total | 9.0 (2.6) | 3.8 (3.5) | 5.0 (3.1) | 9.9 (1.8) | 7.4 (3.6) | p < 0.001 * p = 0.13 ** p = 0.02 |
| GD or GBA1 Healthy Carriers | Sidransky Syndrome | iPD | Healthy Controls | Total | p-Value | Adjusted for Age and Sex | |
|---|---|---|---|---|---|---|---|
| Menthol | 63.4 | 38.9 | 53.3 | 90.0 | 63.9 | 0.002 | 0.01 |
| Cherry | 78.0 | 27.8 | 46.7 | 80.0 | 63.0 | <0.001 | 0.006 |
| Clove | 80.5 | 33.3 | 60.0 | 86.7 | 69.7 | <0.001 | 0.003 |
| Leather | 87.8 | 44.4 | 40.0 | 93.3 | 70.6 | <0.001 | <0.001 |
| Strawberry | 58.5 | 33.3 | 26.7 | 76.7 | 51.3 | <0.001 | 0.02 |
| Lilac | 73.2 | 27.8 | 43.3 | 76.7 | 59.7 | <0.001 | 0.01 |
| Pineapple | 85.4 | 33.3 | 50.0 | 93.3 | 70.6 | <0.001 | <0.001 |
| Smoke | 95.1 | 38.9 | 46.7 | 90.0 | 73.1 | <0.001 | <0.001 |
| Lemon | 61.0 | 11.1 | 13.3 | 50.0 | 38.7 | <0.001 | <0.001 |
| Soap | 65.9 | 27.8 | 63.3 | 76.7 | 62.2 | 0.007 | 0.02 |
| Natural gas | 85.4 | 22.2 | 30.0 | 96.7 | 64.7 | <0.001 | <0.001 |
| Rose | 63.4 | 33.3 | 30.0 | 80.0 | 54.6 | <0.001 | 0.004 |
| Males | Females | Total | p-Value | |
| Menthol | 53.7 | 76.9 | 63.9 | 0.007 |
| Cherry | 52.2 | 76.9 | 56.6 | 0.005 |
| Clove | 65.7 | 75.0 | 69.7 | 0.19 |
| Leather | 62.7 | 80.8 | 70.6 | 0.03 |
| Strawberry | 46.3 | 57.7 | 51.3 | 0.15 |
| Lilac | 55.2 | 65.4 | 59.7 | 0.18 |
| Pineapple | 56.7 | 88.5 | 70.6 | <0.001 |
| Smoke | 61.2 | 88.5 | 73.1 | <0.001 |
| Lemon | 34.3 | 44.2 | 38.7 | 0.18 |
| Soap | 55.2 | 71.2 | 62.2 | 0.06 |
| Natural gas | 55.2 | 76.9 | 64.7 | 0.01 |
| Rose | 38.8 | 75.0 | 54.6 | <0.001 |
| Total BSIT® | Constipation | Urinary COMPLAINTS | RBD | MDS-mUPDRS | ||
|---|---|---|---|---|---|---|
| Hyposmia | Pearson correlation | −0.672 | 0.172 | 0.063 | 0.100 | 0.185 |
| p-value | <0.001 | 0.354 | 0.733 | 0.620 | 0.320 | |
| N | 32 | 31 | 32 | 27 | 31 | |
| Total BSIT® | Pearson correlation | 1 | −0.354 | −0.197 | −0.313 | −0.573 |
| p-value | <0.001 | 0.043 | 0.002 | <0.001 | ||
| N | 119 | 113 | 106 | 91 | 103 | |
| Constipation | Pearson correlation | 1 | 0.273 | 0.447 | 0.483 | |
| p-value | 0.005 | <0.001 | <0.001 | |||
| N | 113 | 103 | 89 | 98 | ||
| Urinary complaints | Pearson correlation | 1 | 0.312 | 0.371 | ||
| p-value | 0.005 | <0.001 | ||||
| N | 106 | 81 | 91 | |||
| RBD | Pearson correlation | 1 | 0.245 | |||
| p-value | 0.034 | |||||
| N | 91 | 75 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen, M.E.; Shechter, Y.; Dominko, M.; Shulman, E.; Dinur, T.; Revel-Vilk, S.; Eichel, R.; Yahalom, G.; Becker-Cohen, M. Olfactory Perception in Parkinson’s Disease: The Impact of GBA1 Variants (Sidransky Syndrome). Int. J. Mol. Sci. 2025, 26, 5258. https://doi.org/10.3390/ijms26115258
Cohen ME, Shechter Y, Dominko M, Shulman E, Dinur T, Revel-Vilk S, Eichel R, Yahalom G, Becker-Cohen M. Olfactory Perception in Parkinson’s Disease: The Impact of GBA1 Variants (Sidransky Syndrome). International Journal of Molecular Sciences. 2025; 26(11):5258. https://doi.org/10.3390/ijms26115258
Chicago/Turabian StyleCohen, Mikhal E., Yosef Shechter, Melania Dominko, Elena Shulman, Tama Dinur, Shoshana Revel-Vilk, Roni Eichel, Gilad Yahalom, and Michal Becker-Cohen. 2025. "Olfactory Perception in Parkinson’s Disease: The Impact of GBA1 Variants (Sidransky Syndrome)" International Journal of Molecular Sciences 26, no. 11: 5258. https://doi.org/10.3390/ijms26115258
APA StyleCohen, M. E., Shechter, Y., Dominko, M., Shulman, E., Dinur, T., Revel-Vilk, S., Eichel, R., Yahalom, G., & Becker-Cohen, M. (2025). Olfactory Perception in Parkinson’s Disease: The Impact of GBA1 Variants (Sidransky Syndrome). International Journal of Molecular Sciences, 26(11), 5258. https://doi.org/10.3390/ijms26115258