

Current Knowledge of the Impact of Vitamin D in Coronary Artery Disease



Abstract
1. Introduction
1.1. Coronary Artery Disease (CAD)
1.2. Mechanisms of CAD Development
1.3. Current Treatment of CAD
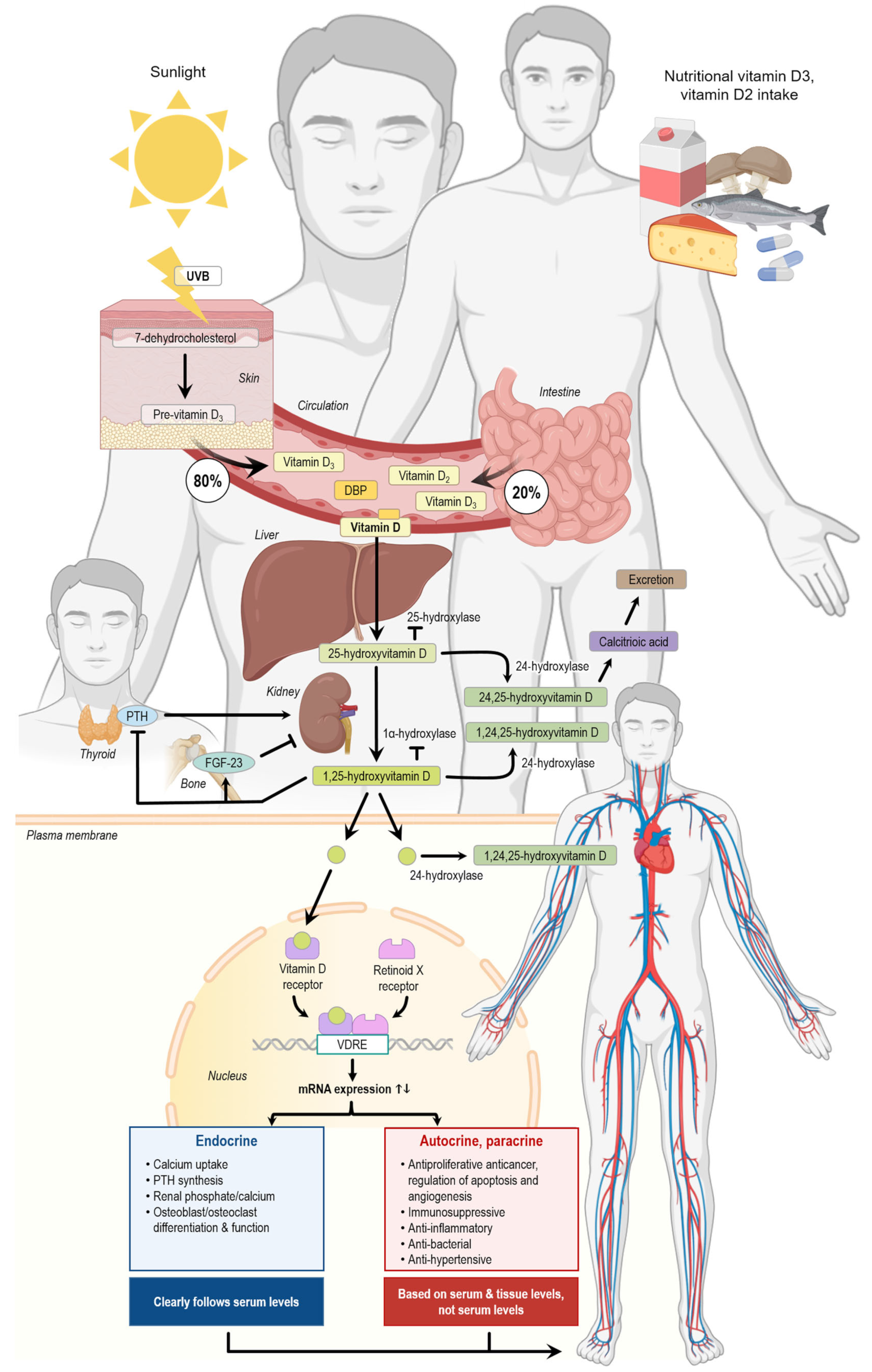
1.4. Vitamin D
1.5. The Effect of Vitamin D Supplementation on the Ca2+ Metabolism
1.6. Effect of Vitamin D on Cardiac Physiology
2. Results
2.1. Vitamin D and Hypertension
2.2. Vitamin D and Atherosclerosis
2.3. Vitamin D and Vascular Reactivity
2.4. Vitamin D and Myocardial Infarction
2.5. Randomized Controlled Trials
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AMI | Acute myocardial infarction |
| AVC | Aortic valve calcification |
| BMI | Body mass index |
| CAC | Coronary artery calcification |
| CAD | Coronary artery disease |
| CRP | C-reactive protein |
| CVD | Cardiovascular disease |
| DAG | Diacylglycerols |
| ER | Endoplasmic reticulum |
| FGF-23 | Fibroblast growth factor 23 |
| FGFR | fibroblast growth factor receptor |
| HDL | High-density lipoproteins |
| LDL | Low-density lipoprotein |
| MACE | Major cardiovascular events |
| NO | Nitric oxide |
| POAF | Postoperative atrial fibrillation |
| PTH | Parathyroid hormone |
| RCT | Randomized controlled trial |
| ROS | Reactive oxygen species |
| TG | Triglycerides |
| TRPC | Transient receptor potential channel |
| VDR | Vitamin D receptor |
References
- Mensah, G.A.; Fuster, V.; Murray, C.J.L.; Roth, G.A. Global Burden of Cardiovascular Diseases and Risks, 1990–2022. J. Am. Coll. Cardiol. 2023, 82, 2350–2473. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Dong, Z.; Liao, H.; Chen, Y.; Hu, L.; Yu, Z.; Xia, Y.; Zhao, Y.; Fan, K.; Ding, J.; et al. Lipid metabolism patterns and relevant clinical and molecular features of coronary artery disease patients: An integrated bioinformatic analysis. Lipids Health Dis. 2022, 21, 87. [Google Scholar] [CrossRef]
- Sinha, A.; Rahman, H.; Douiri, A.; Demir, O.M.; De Silva, K.; Clapp, B.; Webb, I.; Gulati, A.; Pinho, P.; Dutta, U.; et al. ChaMP-CMD: A Phenotype-Blinded, Randomized Controlled, Cross-Over Trial. Circulation 2024, 149, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Khan, M.U.; Aziz, S.; Iqtidar, K.; Zaher, G.F.; Alghamdi, S.; Gull, M. A two-stage classification model integrating feature fusion for coronary artery disease detection and classification. Multimed. Tools Appl. 2022, 81, 13661–13690. [Google Scholar] [CrossRef]
- Min, J.K.; Chang, H.J.; Andreini, D.; Pontone, G.; Guglielmo, M.; Bax, J.J.; Knaapen, P.; Raman, S.V.; Chazal, R.A.; Freeman, A.M.; et al. Coronary CTA plaque volume severity stages according to invasive coronary angiography and FFR. J. Cardiovasc. Comput. Tomogr. 2022, 16, 415–422. [Google Scholar] [CrossRef]
- Cury, R.C.; Leipsic, J.; Abbara, S.; Achenbach, S.; Berman, D.; Bittencourt, M.; Budoff, M.; Chinnaiyan, K.; Choi, A.D.; Ghoshhajra, B.; et al. CAD-RADSTM 2.0—2022 Coronary Artery Disease-Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR), and the North America Society of Cardiovascular Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2022, 16, 536–557. [Google Scholar] [CrossRef]
- Samaras, A.D.; Moustakidis, S.; Apostolopoulos, I.D.; Papandrianos, N.; Papageorgiou, E. Classification models for assessing coronary artery disease instances using clinical and biometric data: An explainable man-in-the-loop approach. Sci. Rep. 2023, 13, 6668. [Google Scholar] [CrossRef]
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef]
- Razo, C.; Welgan, C.A.; Johnson, C.O.; McLaughlin, S.A.; Iannucci, V.; Rodgers, A.; Wang, N.; LeGrand, K.E.; Sorensen, R.J.D.; He, J.; et al. Effects of elevated systolic blood pressure on ischemic heart disease: A Burden of Proof study. Nat. Med. 2022, 28, 2056–2065. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Karamzad, N.; Singh, K.; Carson-Chahhoud, K.; Adams, C.; Nejadghaderi, S.A.; Almasi-Hashiani, A.; Sullman, M.J.M.; Mansournia, M.A.; Bragazzi, N.L.; et al. Burden of ischemic heart disease and its attributable risk factors in 204 countries and territories, 1990–2019. Eur. J. Prev. Cardiol. 2022, 29, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Biddinger, K.J.; Emdin, C.A.; Haas, M.E.; Wang, M.; Hindy, G.; Ellinor, P.T.; Kathiresan, S.; Khera, A.V.; Aragam, K.G. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw. Open 2022, 5, e223849. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Dorresteijn, J.A.; Janssen, A.; Lambrinou, E.; Scherrenberg, M.; Bonnefoy-Cudraz, E.; Cobain, M.; Piepoli, M.F.; Visseren, F.L.; Dendale, P. Risk prediction tools in cardiovascular disease prevention: A report from the ESC Prevention of CVD Programme led by the European Association of Preventive Cardiology (EAPC) in collaboration with the Acute Cardiovascular Care Association (ACCA) and the Association of Cardiovascular Nursing and Allied Professions (ACNAP). Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 522–532. [Google Scholar] [CrossRef]
- Khera, A.V.; Emdin, C.A.; Drake, I.; Natarajan, P.; Bick, A.G.; Cook, N.R.; Chasman, D.I.; Baber, U.; Mehran, R.; Rader, D.J.; et al. Genetic Risk, Adherence to a Healthy Lifestyle, and Coronary Disease. N. Engl. J. Med. 2016, 375, 2349–2358. [Google Scholar] [CrossRef]
- van de Hoef, T.P.; Echavarría-Pinto, M.; van Lavieren, M.A.; Meuwissen, M.; Serruys, P.W.; Tijssen, J.G.; Pocock, S.J.; Escaned, J.; Piek, J.J. Diagnostic and Prognostic Implications of Coronary Flow Capacity: A Comprehensive Cross-Modality Physiological Concept in Ischemic Heart Disease. JACC Cardiovasc. Interv. 2015, 8, 1670–1680. [Google Scholar] [CrossRef]
- Dasa, O.; Smith, S.M.; Pepine, C.J. Ischemic Heart Disease. In Hypertension: A Companion to Braunwalds’s Heart Disease, 4th ed.; Bakris, G.L., Sorrentino, M.J., Laffin, L.J., Eds.; Elsevier: Amsterdam, The Netherlands, 2024; pp. 363–376. [Google Scholar]
- Gutiérrez, E.; Flammer, A.J.; Lerman, L.O.; Elízaga, J.; Lerman, A.; Fernández-Avilés, F. Endothelial dysfunction over the course of coronary artery disease. Eur. Heart J. 2013, 34, 3175–3181. [Google Scholar] [CrossRef]
- Kłosowicz, M.; Leksa, D.; Bartusik-Aebisher, D.; Myśliwiec, A.; Dynarowicz, K.; Aebisher, D. Biomarkers That Seem to Have the Greatest Impact on Promoting the Formation of Atherosclerotic Plaque in Current Scientific Research. Curr. Issues Mol. Biol. 2024, 46, 9503–9522. [Google Scholar] [CrossRef]
- Stone, P.H.; Saito, S.; Takahashi, S.; Makita, Y.; Nakamura, S.; Kawasaki, T.; Takahashi, A.; Katsuki, T.; Nakamura, S.; Namiki, A.; et al. Prediction of progression of coronary artery disease and clinical outcomes using vascular profiling of endothelial shear stress and arterial plaque characteristics: The PREDICTION Study. Circulation 2012, 126, 172–181. [Google Scholar] [CrossRef]
- Xie, X.; Wang, F.; Zhu, L.; Yang, H.; Pan, D.; Liu, Y.; Qu, X.; Gu, Y.; Li, X.; Chen, S. Low shear stress induces endothelial cell apoptosis and monocyte adhesion by upregulating PECAM-1 expression. Mol. Med. Rep. 2020, 21, 2580–2588. [Google Scholar] [CrossRef]
- Mortensen, M.B.; Dzaye, O.; Steffensen, F.H.; Bøtker, H.E.; Jensen, J.M.; Rønnow Sand, N.P.; Kragholm, K.H.; Sørensen, H.T.; Leipsic, J.; Mæng, M.; et al. Impact of Plaque Burden Versus Stenosis on Ischemic Events in Patients With Coronary Atherosclerosis. J. Am. Coll. Cardiol. 2020, 76, 2803–2813. [Google Scholar] [CrossRef]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef] [PubMed]
- Turck, D.; Bohn, T.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Pentieva, K.; et al. Scientific opinion on the tolerable upper intake level for vitamin D, including the derivation of a conversion factor for calcidiol monohydrate. Efsa J. 2023, 21, e08145. [Google Scholar] [CrossRef] [PubMed]
- Carbone, F.; Liberale, L.; Libby, P.; Montecucco, F. Vitamin D in atherosclerosis and cardiovascular events. Eur. Heart J. 2023, 44, 2078–2094. [Google Scholar] [CrossRef]
- Cosentino, N.; Campodonico, J.; Milazzo, V.; De Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. [Google Scholar] [CrossRef]
- Jiang, H.; Horst, R.L.; Koszewski, N.J.; Goff, J.P.; Christakos, S.; Fleet, J.C. Targeting 1,25(OH)(2)D-mediated calcium absorption machinery in proximal colon with calcitriol glycosides and glucuronides. J. Steroid Biochem. Mol. Biol. 2020, 198, 105574. [Google Scholar] [CrossRef]
- Chankamngoen, W.; Thammayon, N.; Suntornsaratoon, P.; Nammultriputtar, K.; Kitiyanant, N.; Donpromma, N.; Chaichanan, J.; Supcharoen, P.; Teerapo, K.; Teerapornpuntakit, J.; et al. Fibroblast growth factor-21 potentiates the stimulatory effects of 1,25-dihydroxyvitamin D3 on transepithelial calcium transport and TRPV6 Ca2+ channel expression. Biochem. Biophys. Res. Commun. 2024, 733, 150429. [Google Scholar] [CrossRef]
- Matikainen, N.; Pekkarinen, T.; Ryhänen, E.M.; Schalin-Jäntti, C. Physiology of Calcium Homeostasis: An Overview. Endocrinol. Metab. Clin. N. Am. 2021, 50, 575–590. [Google Scholar] [CrossRef]
- Nakamichi, Y.; Liu, Z.; Mori, T.; He, Z.; Yasuda, H.; Takahashi, N.; Udagawa, N. The vitamin D receptor in osteoblastic cells but not secreted parathyroid hormone is crucial for soft tissue calcification induced by the proresorptive activity of 1,25(OH)2D3. J. Steroid Biochem. Mol. Biol. 2023, 232, 106351. [Google Scholar] [CrossRef]
- Dutta, P.; Layton, A.T. Modeling calcium and magnesium balance: Regulation by calciotropic hormones and adaptations under varying dietary intake. iScience 2024, 27, 111077. [Google Scholar] [CrossRef] [PubMed]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.C.; Sloan, A.; Isakova, T.; Gutiérrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J. Clin. Investig. 2011, 121, 4393–4408. [Google Scholar] [CrossRef] [PubMed]
- Stratford, K.; Haykal-Coates, N.; Thompson, L.; Farraj, A.; Hazari, M. Early-life persistent vitamin D deficiency-induced cardiovascular dysfunction in mice is mediated by transient receptor potential C channels. J. Steroid Biochem. Mol. Biol. 2021, 206, 105804. [Google Scholar] [CrossRef] [PubMed]
- Philouze, C.; Martin, J.C.; Riva, C.; Marziou, A.; Defoort, C.; Couturier, C.; Berton, T.; Astier, J.; Jover, B.; Gayrard, N.; et al. Vitamin D3 Supplementation Alleviates Left Ventricular Dysfunction in a Mouse Model of Diet-Induced Type 2 Diabetes: Potential Involvement of Cardiac Lipotoxicity Modulation. Cardiovasc. Drugs Ther. 2022, 36, 245–256. [Google Scholar] [CrossRef]
- Ivkovic, T.; Tepavcevic, S.; Romic, S.; Stojiljkovic, M.; Kostic, M.; Stanisic, J.; Koricanac, G.; Culafic, T. Cholecalciferol affects cardiac proteins regulating malonyl-CoA availability and intracellular calcium level. Gen. Physiol. Biophys. 2023, 42, 241–250. [Google Scholar] [CrossRef]
- Oh, J.; Matkovich, S.J.; Riek, A.E.; Bindom, S.M.; Shao, J.S.; Head, R.D.; Barve, R.A.; Sands, M.S.; Carmeliet, G.; Osei-Owusu, P.; et al. Macrophage secretion of miR-106b-5p causes renin-dependent hypertension. Nat. Commun. 2020, 11, 4798. [Google Scholar] [CrossRef]
- Kumar, S.; Nanduri, R.; Bhagyaraj, E.; Kalra, R.; Ahuja, N.; Chacko, A.P.; Tiwari, D.; Sethi, K.; Saini, A.; Chandra, V.; et al. Vitamin D3-VDR-PTPN6 axis mediated autophagy contributes to the inhibition of macrophage foam cell formation. Autophagy 2021, 17, 2273–2289. [Google Scholar] [CrossRef]
- Elseweidy, M.M.; Aly, S.I.; Hammad, S.K.; Shershir, N.I. Early myocardial injury biomarkers in diabetic hyperlipidemic rats: Impact of 10-dehydrogingerdione and vitamin D3. Exp. Biol. Med. 2020, 245, 1326–1334. [Google Scholar] [CrossRef]
- Fontányi, Z.; Sziva, R.E.; Pál, É.; Hadjadj, L.; Monori-Kiss, A.; Horváth, E.M.; Benkő, R.; Magyar, A.; Heinzlmann, A.; Benyó, Z.; et al. Vitamin D Deficiency Reduces Vascular Reactivity of Coronary Arterioles in Male Rats. Curr. Issues Mol. Biol. 2021, 43, 79–92. [Google Scholar] [CrossRef]
- Wei, Y.X.; Dong, S.M.; Wang, Y.Y.; Zhang, P.; Sun, M.Y.; Wei, Y.X.; Meng, X.C.; Wang, Y. Autophagy participates in the protection role of 1,25-dihydroxyvitamin D3 in acute myocardial infarction via PI3K/AKT/mTOR pathway. Cell Biol. Int. 2021, 45, 394–403. [Google Scholar] [CrossRef]
- Mehdipoor, M.; Damirchi, A.; Razavi Tousi, S.M.T.; Babaei, P. Concurrent vitamin D supplementation and exercise training improve cardiac fibrosis via TGF-β/Smad signaling in myocardial infarction model of rats. J. Physiol. Biochem. 2021, 77, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Wang, C.; Ruan, C.; Chen, M.; Cao, R.; Sheng, L.; Chang, N.; Xu, T.; Zhao, P.; Liu, X.; et al. Novel Insights into the Cardioprotective Effects of Calcitriol in Myocardial Infarction. Cells 2022, 11, 1676. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Waterhouse, M.; English, D.R.; McLeod, D.S.; Armstrong, B.K.; Baxter, C.; Duarte Romero, B.; Ebeling, P.R.; Hartel, G.; Kimlin, M.G.; et al. Vitamin D supplementation and major cardiovascular events: D-Health randomised controlled trial. BMJ 2023, 381, e075230. [Google Scholar] [CrossRef]
- Neale, R.E.; Baxter, C.; Romero, B.D.; McLeod, D.S.A.; English, D.R.; Armstrong, B.K.; Ebeling, P.R.; Hartel, G.; Kimlin, M.G.; O’Connell, R.; et al. The D-Health Trial: A randomised controlled trial of the effect of vitamin D on mortality. Lancet Diabetes Endocrinol. 2022, 10, 120–128. [Google Scholar] [CrossRef]
- Waterhouse, M.; English, D.R.; Armstrong, B.K.; Baxter, C.; Duarte Romero, B.; Ebeling, P.R.; Hartel, G.; Kimlin, M.G.; McLeod, D.S.A.; O’Connell, R.L.; et al. A randomized placebo-controlled trial of vitamin D supplementation for reduction of mortality and cancer: Statistical analysis plan for the D-Health Trial. Contemp. Clin. Trials Commun. 2019, 14, 100333. [Google Scholar] [CrossRef]
- Morrone, L.; Palmer, S.C.; Saglimbene, V.M.; Perna, A.; Cianciolo, G.; Russo, D.; Gesualdo, L.; Natale, P.; Santoro, A.; Mazzaferro, S.; et al. Calcifediol supplementation in adults on hemodialysis: A randomized controlled trial. J. Nephrol. 2022, 35, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Joseph, P.; Pais, P.; Gao, P.; Teo, K.; Xavier, D.; Lopez-Jaramillo, P.; Yusoff, K.; Santoso, A.; Gamra, H.; Talukder, S.H.; et al. Vitamin D supplementation and adverse skeletal and non-skeletal outcomes in individuals at increased cardiovascular risk: Results from the International Polycap Study (TIPS)-3 randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 434–440. [Google Scholar] [CrossRef]
- Sarhan, N.; Essam Abou Warda, A.; Alsahali, S.; Alanazi, A.S. Impact of Vitamin D Supplementation on the Clinical Outcomes and Epigenetic Markers in Patients with Acute Coronary Syndrome. Pharmaceuticals 2023, 16, 262. [Google Scholar] [CrossRef]
- Hasific, S.; Oevrehus, K.A.; Lindholt, J.S.; Mejldal, A.; Dey, D.; Dahl, J.S.; Frandsen, N.E.; Auscher, S.; Lambrechtsen, J.; Hosbond, S.; et al. Effects of Vitamin K2 and D Supplementation on Coronary Artery Disease in Men: A RCT. JACC Adv. 2023, 2, 100643. [Google Scholar] [CrossRef]
- Tasdighi, E.; Hekmat, M.; Beheshti, M.; Baghaei, R.; Mirhosseini, S.M.; Torbati, P.; Pourmotahari, F.; Foroughi, M. Vitamin D Treatment Attenuates Heart Apoptosis After Coronary Artery Bypass Surgery: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. J. Cardiovasc. Pharmacol. Ther. 2020, 25, 338–345. [Google Scholar] [CrossRef]
- Alirezaei, T.; Ansari Aval, Z.; Karamian, A.; Hayati, A. Effect of preoperative vitamin D on postoperative atrial fibrillation incidence after coronary artery bypass grafting. Gen. Thorac. Cardiovasc. Surg. 2024, 72, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Limonte, C.P.; Zelnick, L.R.; Hoofnagle, A.N.; Thadhani, R.; Melamed, M.L.; Mora, S.; Cook, N.R.; Luttmann-Gibson, H.; Sesso, H.D.; Lee, I.M.; et al. Effects of Vitamin D(3) Supplementation on Cardiovascular and Cancer Outcomes by eGFR in VITAL. Kidney360 2022, 3, 2095–2105. [Google Scholar] [CrossRef]
- Gaengler, S.; Sadlon, A.; De Godoi Rezende Costa Molino, C.; Willett, W.C.; Manson, J.E.; Vellas, B.; Steinhagen-Thiessen, E.; Von Eckardstein, A.; Ruschitzka, F.; Rizzoli, R.; et al. Effects of vitamin D, omega-3 and a simple strength exercise programme in cardiovascular disease prevention: The DO-HEALTH randomized controlled trial. J. Nutr. Health Aging 2024, 28, 100037. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; da Silva, J.A.P.; Blauth, M.; Felson, D.T.; McCloskey, E.V.; Watzl, B.; Hofbauer, L.C.; et al. Effect of Vitamin D Supplementation, Omega-3 Fatty Acid Supplementation, or a Strength-Training Exercise Program on Clinical Outcomes in Older Adults: The DO-HEALTH Randomized Clinical Trial. JAMA 2020, 324, 1855–1868. [Google Scholar] [CrossRef]
- Sadeghi, M.; Momeni, A.; Mirsaeidi, F.S.; Jamalian, M.; Amirpour, A.; Hadavi, M.M.; Tavassoli, P.; Taheri, M.; Azizi, E.; Rouhani, S.; et al. The Effect of Vitamin D Deficiency Treatment on Lipid Profile and C-reactive Protein in Patients with Ischemic Heart Disease: Double-blind Randomized Clinical Trial. Adv. Biomed. Res. 2024, 13, 79. [Google Scholar] [CrossRef] [PubMed]
- Johny, E.; Jala, A.; Nath, B.; Alam, M.J.; Kuladhipati, I.; Das, R.; Borkar, R.M.; Adela, R. Vitamin D Supplementation Modulates Platelet-Mediated Inflammation in Subjects With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Front. Immunol. 2022, 13, 869591. [Google Scholar] [CrossRef]
- Imanparast, F.; Mashayekhi, F.J.; Kamankesh, F.; Rafiei, F.; Mohaghegh, P.; Alimoradian, A. Improving the endothelial dysfunction in type 2 diabetes with chromium and vitamin D(3) byreducing homocysteine and oxidative stress: A randomized placebo-controlled trial. J. Trace Elem. Med. Biol. 2020, 62, 126639. [Google Scholar] [CrossRef]
- Rizzoli, R. Vitamin D supplementation: Upper limit for safety revisited? Aging Clin. Exp. Res. 2021, 33, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef]
- Ruiz-Garcia, A.; Pallares-Carratala, V.; Turegano-Yedro, M.; Torres, F.; Sapena, V.; Martin-Gorgojo, A.; Martin-Moreno, J.M. Vitamin D Supplementation and Its Impact on Mortality and Cardiovascular Outcomes: Systematic Review and Meta-Analysis of 80 Randomized Clinical Trials. Nutrients 2023, 15, 1810. [Google Scholar] [CrossRef]
- Djousse, L.; Cook, N.R.; Kim, E.; Bodar, V.; Walter, J.; Bubes, V.; Luttmann-Gibson, H.; Mora, S.; Joseph, J.; Lee, I.M.; et al. Supplementation With Vitamin D and Omega-3 Fatty Acids and Incidence of Heart Failure Hospitalization: VITAL-Heart Failure. Circulation 2020, 141, 784–786. [Google Scholar] [CrossRef] [PubMed]
- Albert, C.M.; Cook, N.R.; Pester, J.; Moorthy, M.V.; Ridge, C.; Danik, J.S.; Gencer, B.; Siddiqi, H.K.; Ng, C.; Gibson, H.; et al. Effect of Marine Omega-3 Fatty Acid and Vitamin D Supplementation on Incident Atrial Fibrillation: A Randomized Clinical Trial. JAMA 2021, 325, 1061–1073. [Google Scholar] [CrossRef] [PubMed]
- Tikkanen, J.T.; Soliman, E.Z.; Pester, J.; Danik, J.S.; Gomelskya, N.; Copeland, T.; Lee, I.M.; Buring, J.E.; Manson, J.E.; Cook, N.R.; et al. A randomized clinical trial of omega-3 fatty acid and vitamin D supplementation on electrocardiographic risk profiles. Sci. Rep. 2023, 13, 11454. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Study, Identifier | Design | Intervention | Results |
|---|---|---|---|
| Vitamin D supplementation and major cardiovascular events: D-health randomized controlled trial [44,45,46] ACTRN12613000743763 | Phase 3, randomized, double blinded, placebo-controlled trial n = 21,315 (60–84 years old) follow-up: 5 years endpoint: major cardiovascular event (Myocardial infarction, stroke or coronary revascularization) | One monthly dose of 60,000 IU vitamin D vs. soya oil placebo data | The rate of major cardiovascular events was lower in vitamin D group than in placebo group (HR = 0.91, 95% CI: 0.81–1.01) The rate of major cardiovascular events was even lower in patients taking cardiovascular drugs (HR = 0.84, 95% CI: 0.74–0.97, p = 0.12) The hazard ratio was lower when looking at incidents of myocardial infarction (HR = 0.81, 95% CI = 0.67–0.98) and coronary revascularization (HR = 0.89, 95% CI: 0.78–1.01) However, all differences were not statistically significant |
| Calcifediol supplementation in adults on hemodialysis: a randomized controlled trial [47] NCT01457001 | Phase 3, multicenter, randomized controlled trial n = 284 (≥18 years) follow-up period = 24 months Endpoint: composite of nonfatal myocardial infarction, nonfatal stroke and death | 40 µg calcifediol 3 times a week vs. no additional treatment | Calcifediol did not have effect on cardiovascular death (HR: 1.06, 95% CI: 0.41–2.74) or nonfatal myocardial infarction (HR: 0.20, 95% CI: 0.02–1.67) The intervention did not show an effect on the composite of nonfatal myocardial infarction, nonfatal stroke, and death (HR = 1.03 95% CI: 0.63–1.67) |
| The International Polycap Study 3 (TIPS-3) [48] NCT01646437 | Phase 3, double-blind, placebo-controlled, randomized trial n = 5670 (men aged ≥ 50 years and women aged ≥ 55 years) Mean follow-up: 4.6 years Endpoint: fracture and composite of CV death, myocardial infarction stroke, cancer, fracture or fall | One monthly dose of 60,000 IU of vitamin D3 vs. placebo | High dose vitamin D did not reduce non-skeletal outcomes (HR = 1.13, 95% CI: 0.93–1.37, p = 0.22) More people in the vitamin D group died (HR = 1.29, 95% CI: 1.03–1.61, p = 0.03) |
| Impact of Vitamin D supplementation on the Clinical Outcomes and Epigenetic Markers in Patients with Acute Coronary Syndrome [49] Trial registration not given | Randomized controlled trial n = 250 Follow up: 2 years Endpoints: cardiac fibrosis markers, echocardiographic parameters, epigenetic markers | Intervention arm: Vitamin D based on serum vitamin D level at baseline. The intervention was: 50,000 IU/week for 8 weeks followed by 10,000 IU/week for 4 months if serum vitamin D was 12 ng/mL and 10,000 IU/week for 6 months if serum vitamin D was above 12 ng/mL | The intervention lowered ejection fraction (p = 1.1 × 10−4), end systolic volume (p = 0.0075), and end diastolic volume (p = 0.002) There was a decrease in cardiac fibrosis markers There were fewer events of MACE (p = 0.043) Taq I (rs731236) was a predictor of heart failure, Bsm I (rs1544410) was a predictor of MACE, Fok I (rs2228570) protected against MACE |
| The Aortic Valve DECalcification Trial (AVADEC) [50] NCT03243890 | Randomized, controlled, double blinded trial n = 304 (men, 65–75 years old) Follow-up time: 2 years Endpoint: absolute change in CAC score and changes in plaque volume | Menaquinone-7 720 µg/day including the recommended daily dose of vitamin D (25 µg/day) vs. placebo | There was no overall reduction in mean CAC progression (mean difference = 51 AU, p = 0.089) Participants with CAC scores ≥400 AU had a smaller progression in CAC (380 AU vs. 288 AU, p = 0.047) Participants with statin use also had a smaller progression in CAC (p = 0.048) |
| Can Vitamin D Reduce Heart Muscle Damage After Bypass Surgery? [51] NCT04323852 | Phase 4, double blind, randomized, placebo-controlled trial n = 70 (≥18 years) follow-up: 30 days Endpoint: caspases 2, 3 and 7 activity, IL-10 serum level, IGF-I serum levels and pro-BNP | 3 doses of vitamin D (50,000 U) a day for 3 days before surgery vs. placebo | Lower average number of caspases 2 and 3 in the vitamin D group (p = 0.006) Increased levels of IL-10 in the vitamin D group before surgery (p = 0.001). It remained elevated after surgery compared to the intervention group (p < 0.001) No difference in pro-BNP |
| Effect of preoperative Vitamin D on postoperative atrial fibrillation incidence after coronary artery bypass graft [52] IRCT20230506058103N1 | Phase 3, randomized controlled clinical trial n = 246 follow-up = 5 days Endpoints: POAF up to 5 days after surgery, duration of hospitalization, duration of intubation | Starting 3 days before the surgery, patients receive 50,000 units of vitamin D three times a day vs. placebo | There was no significant difference in the duration of the hospital stay (p = 0.975) or intubation period (p = 0.886) Decrease in POAF incidence in the intervention group (p = 0.003) |
| Vitamin D and Omega-3 Trial (VITAL) [53] NCT01169259 | Phase 3, double-blind, placebo-controlled trial n = 15,917 (men ≥ 50 years and women ≥ 55 years) Endpoint: major cardiovascular events, invasive cancer | Daily doses of: 2000 IU vitamin D3 + 840 mg of marine omega-3 fatty acids vs. 2000 IU vitamin D3 + fish oil placebo vs. vitamin D placebo + 840 mg of marine omega-3 fatty acids vs. vitamin D placebo + fish oil placebo | There was no significant difference in major cardiovascular events between the intervention and control group There was no significant interaction between eGFR, vitamin D, and major cardiovascular events |
| DO-HEALTH/Vitamin D3—Omega3—Home Exercise—Healthy Ageing and Longevity Trial (DO-HEALTH)) [54,55] NCT01745263 | Phase 3, double-blind, randomized placebo-controlled trial n (biomarkers) = 2157 n (MACE) = 2089 age ≥ 70 years Endpoint: lipid and CVD biomarkers, incident hypertension, and major cardiovascular events. Follow-up: 3 years | 2000 IU/d of vitamin D3, 1 g/d of omega-3s, and a strength-training exercise program vs. vitamin D3 and omega-3s vs. vitamin D3 and vs. vitamin D3 alone vs. omega-3s and exercise vs. omega-3s alone vs. exercise alone vs. placebo | Vitamin D3 did not change the lipid profile significantly Vitamin D3 supplements showed no effect on MACE (HR = 1.37, 95% CI: 0.88–2.14), there were also no effects on hypertension (HR = 1.05, 95% CI: 0.76–1.44) |
| The effect of vitamin D deficiency treatment on lipid profile in ischemic heart diseases: a double blinded randomized clinical trial [56] IRCT20200905048622N1 | Phase 3, double-blind, randomized controlled trial n = 44 (40–65 years) Follow-up time: 5 weeks Endpoints: serum levels of TGs, LDL-C, HDL-C, TC and CRP | 50,000 IU vitamin D3 weekly up to 2 months vs. placebo | A significant increase in HDL (p = 0.048) and a significant decrease in TG (p = 0.008) in the intervention group No correlation between vitamin D and CRP levels |
| Vitamin D supplementation modulates platelet-mediated inflammation in subjects with type 2 diabetes: A randomized double-blind, placebo-controlled trial [57] CTRI/2019/01/016921 | Randomized, double-blind, placebo-controlled trial n = 59 (25–65 years) follow-up = 12 months endpoint: platelet activation, platelet-immune-cell aggregation, immune profile, vitamin D metabolite levels | Vitamin D 60,000 IU/week for 3 months followed by 60,000/month for 9 months | No improvement of glycemic control or a difference in immune cells between the groups Platelet activation was reduced, and platelet-immune cell aggregates were altered (p < 0.05) Reduced levels of cytokines such as IL-18, TNF-alpha, IFN-gamma, etc. Reduction in intracellular reactive oxygen species |
| Simultaneous use of chromium picolinate and vitamin D reconstruction or prevention of endothelial dysfunction in patients with type 2 diabetes by examining the pattern of changes in metabolic markers of oxidative stress, inflammation, and endothelial dysfunction [58] IRCT2017052034038N1 | Phase 3, randomized, single-blind, placebo-controlled trial n = 92 (25–60 years) Follow-up time: 4 months Endpoints: Hct, MDA, total antioxidant capacity, total thiol groups, vascular cell adhesion molecule-1, plasminogen activator inhibitor-1 | 6 months of: 400 mg of chromium picolinate daily vs. 50,000 IU vitamin D per week vs. combination of 50,000 IU per week vitamin D and 400 mg of chromium picolinate per day vs. placebo | Vitamin D3 significantly reduced homocysteine Vitamin D3 significantly changed the mean concentration of MDA Vitamin D3 significantly decreased the expression of PAI-1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jespersen, F.E.; Grimm, D.; Krüger, M.; Wehland, M. Current Knowledge of the Impact of Vitamin D in Coronary Artery Disease. Int. J. Mol. Sci. 2025, 26, 5002. https://doi.org/10.3390/ijms26115002
Jespersen FE, Grimm D, Krüger M, Wehland M. Current Knowledge of the Impact of Vitamin D in Coronary Artery Disease. International Journal of Molecular Sciences. 2025; 26(11):5002. https://doi.org/10.3390/ijms26115002
Chicago/Turabian StyleJespersen, Freja Esager, Daniela Grimm, Marcus Krüger, and Markus Wehland. 2025. "Current Knowledge of the Impact of Vitamin D in Coronary Artery Disease" International Journal of Molecular Sciences 26, no. 11: 5002. https://doi.org/10.3390/ijms26115002
APA StyleJespersen, F. E., Grimm, D., Krüger, M., & Wehland, M. (2025). Current Knowledge of the Impact of Vitamin D in Coronary Artery Disease. International Journal of Molecular Sciences, 26(11), 5002. https://doi.org/10.3390/ijms26115002