
Altered Sweat Composition Due to Changes in Tight Junction Expression of Sweat Glands in Cholinergic Urticaria Patients

 , , ,
, , , 
Abstract
1. Introduction
2. Results
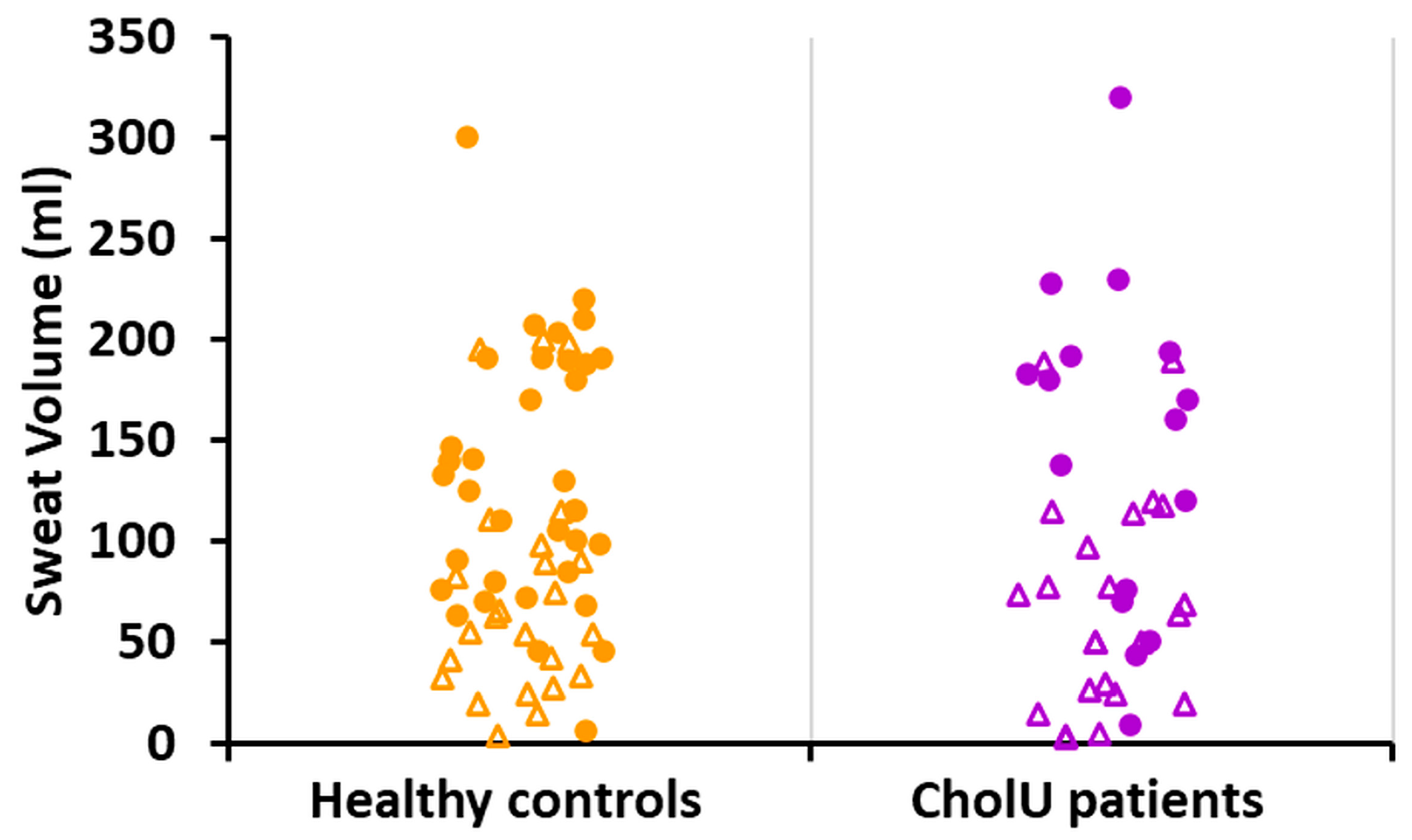
2.1. Reduced Sweating Can Be Observed in a Subgroup of CholU Patients
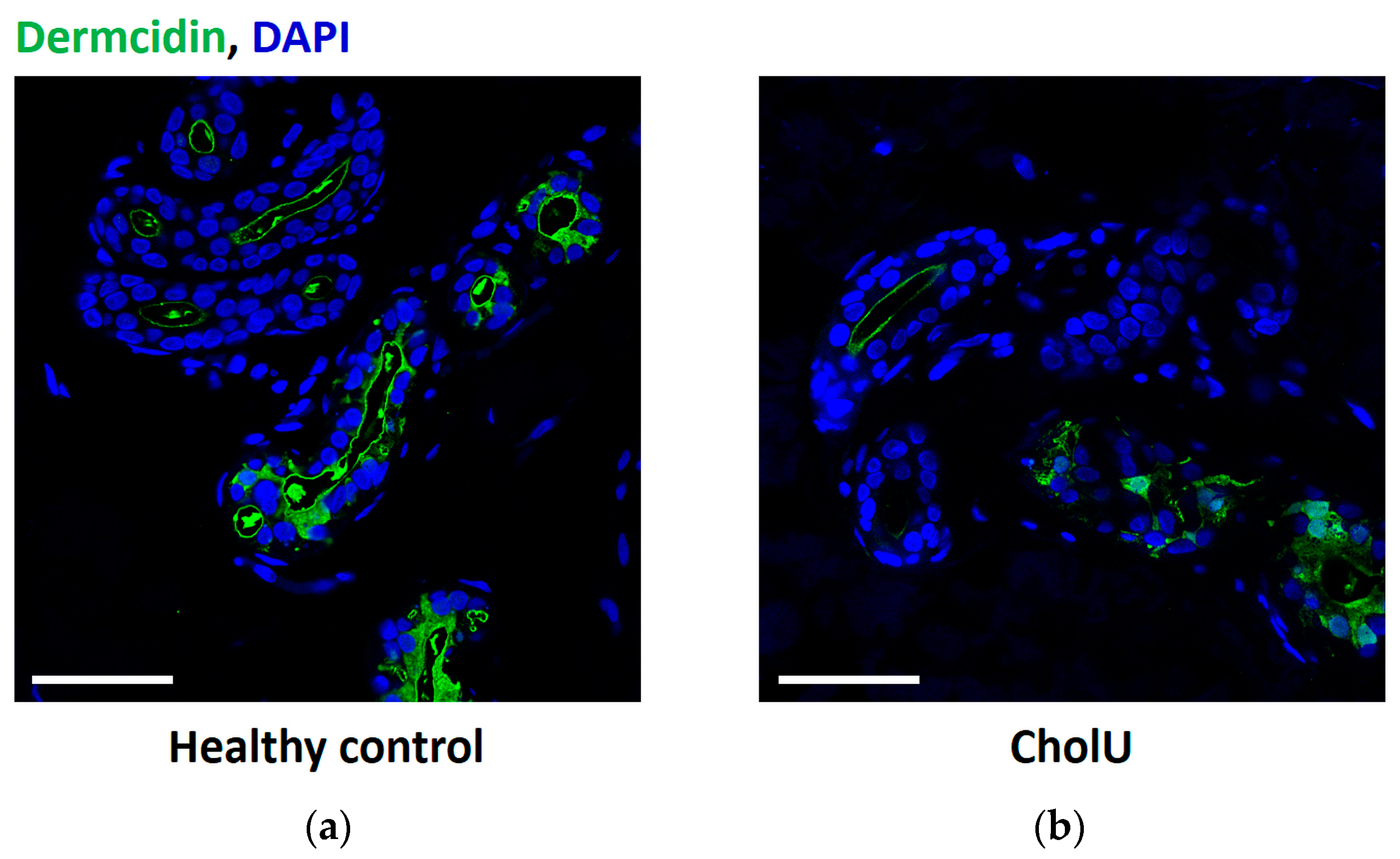
2.2. No Sweat Leakage from Sweat Glands in CholU Patients with Reduced Sweating
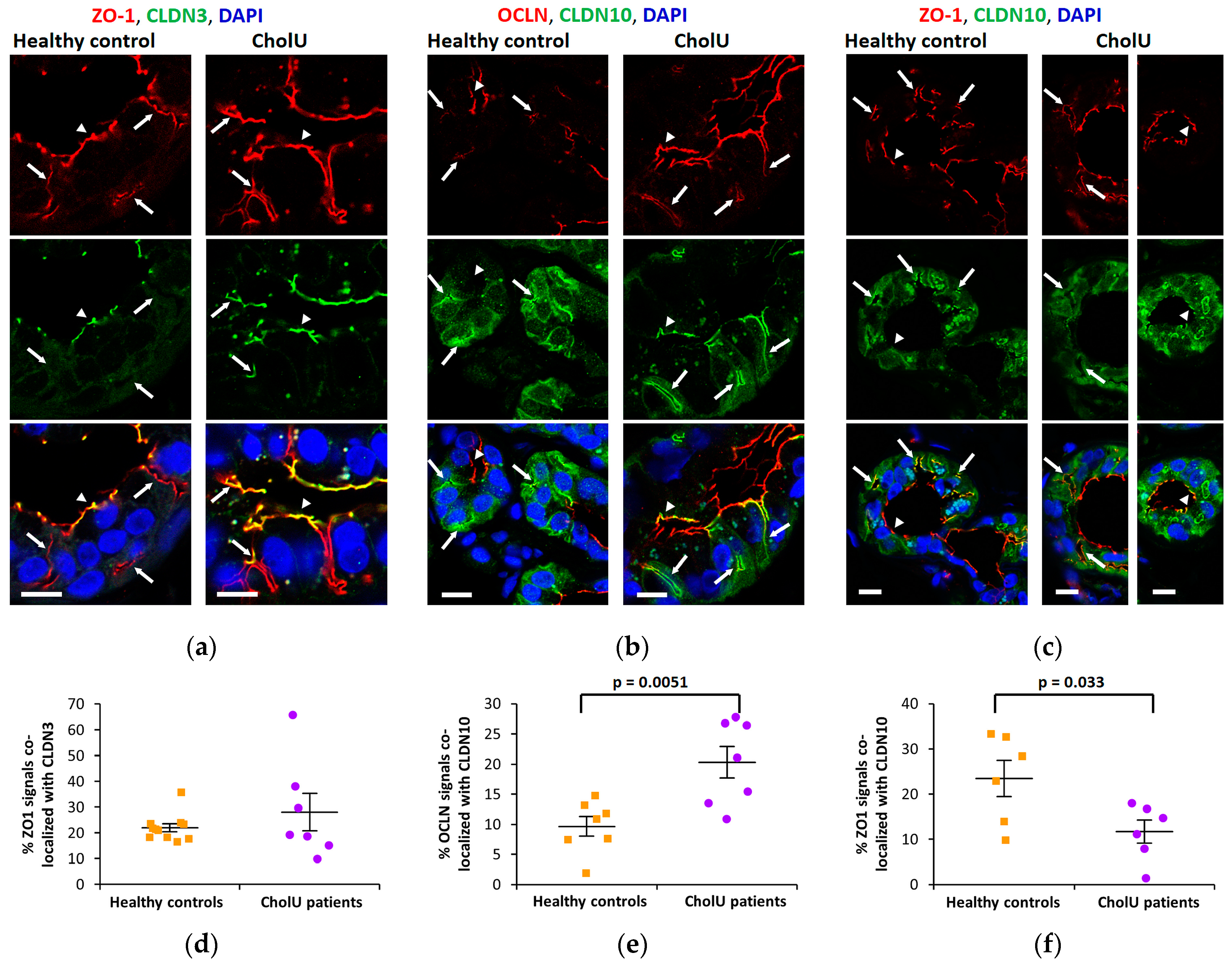
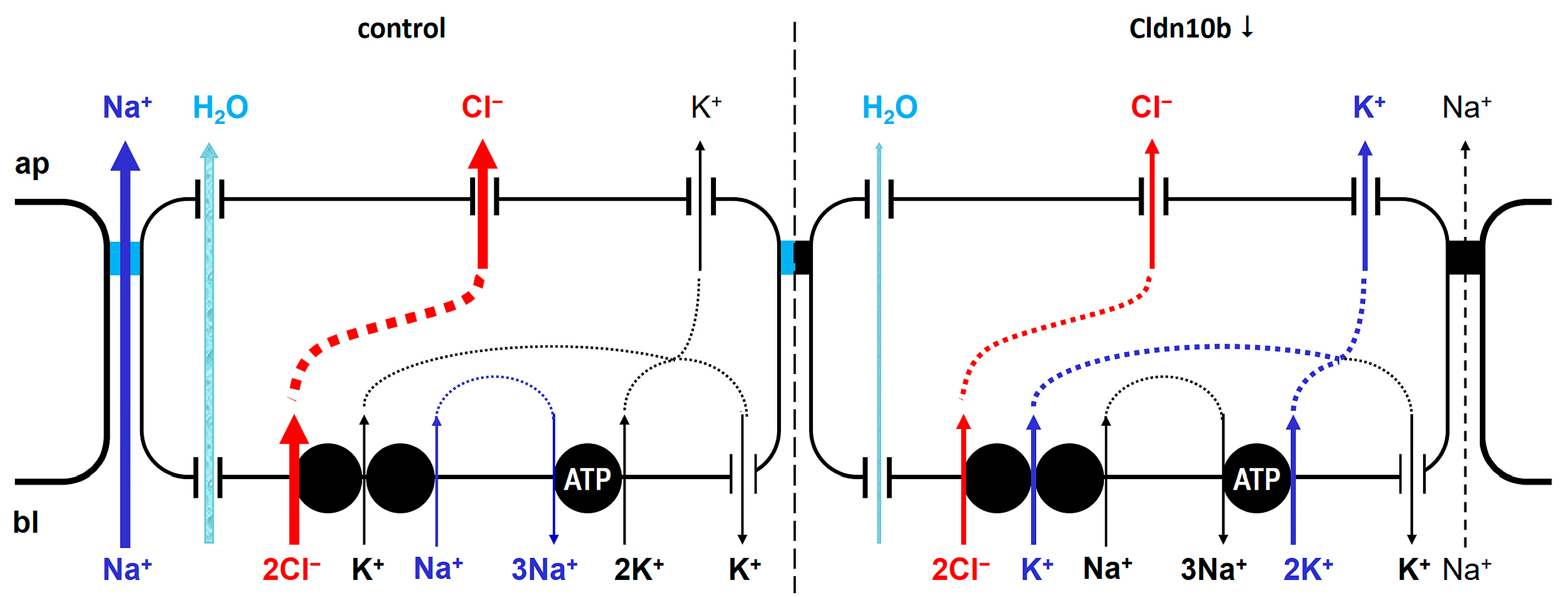
2.3. Altered TJ Protein Distribution in Sweat Gland Secretory Coils from CholU Patients
2.4. Altered Electrolyte Composition of Sweat from CholU Patients Compared to Healthy Controls
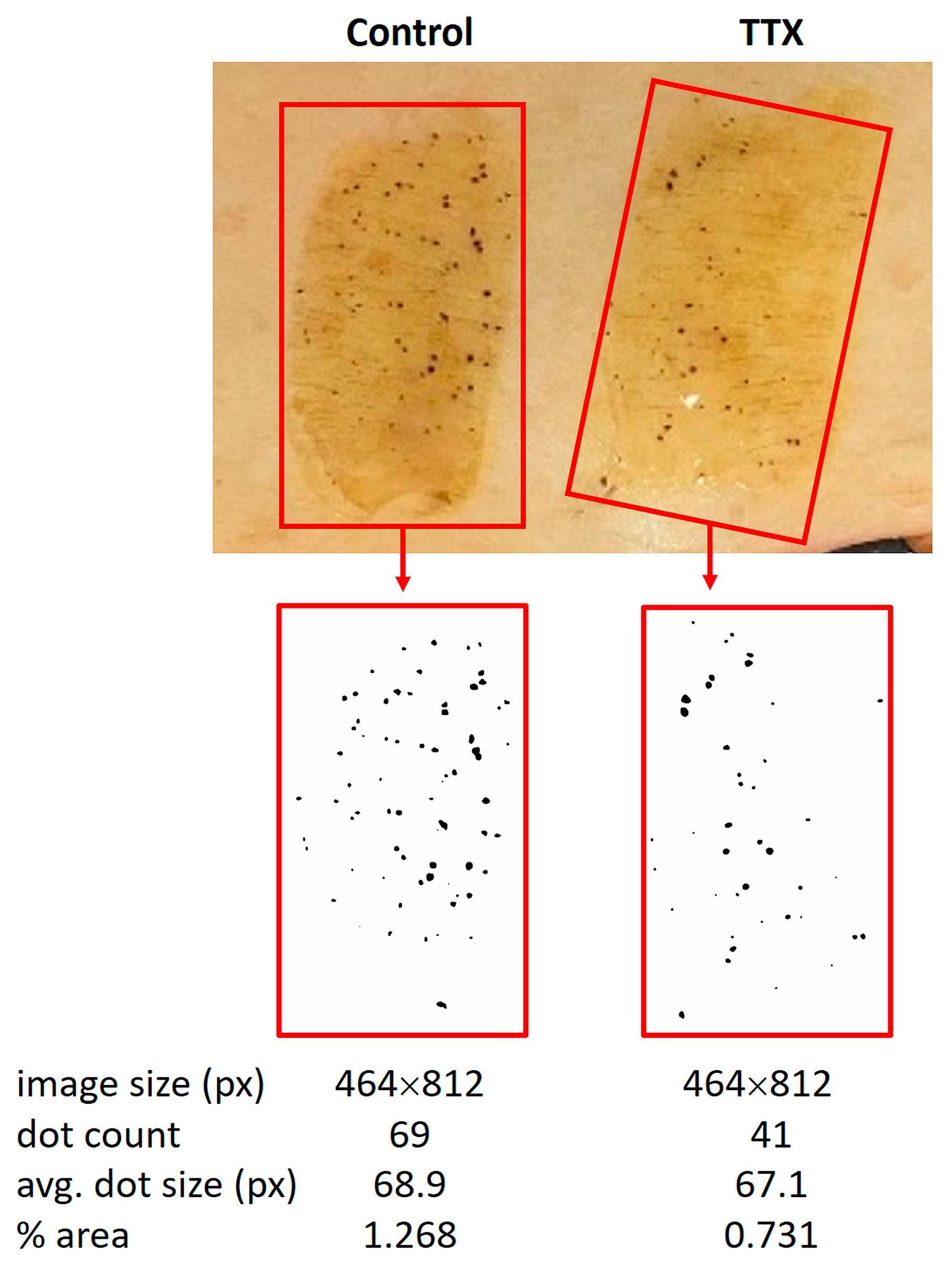
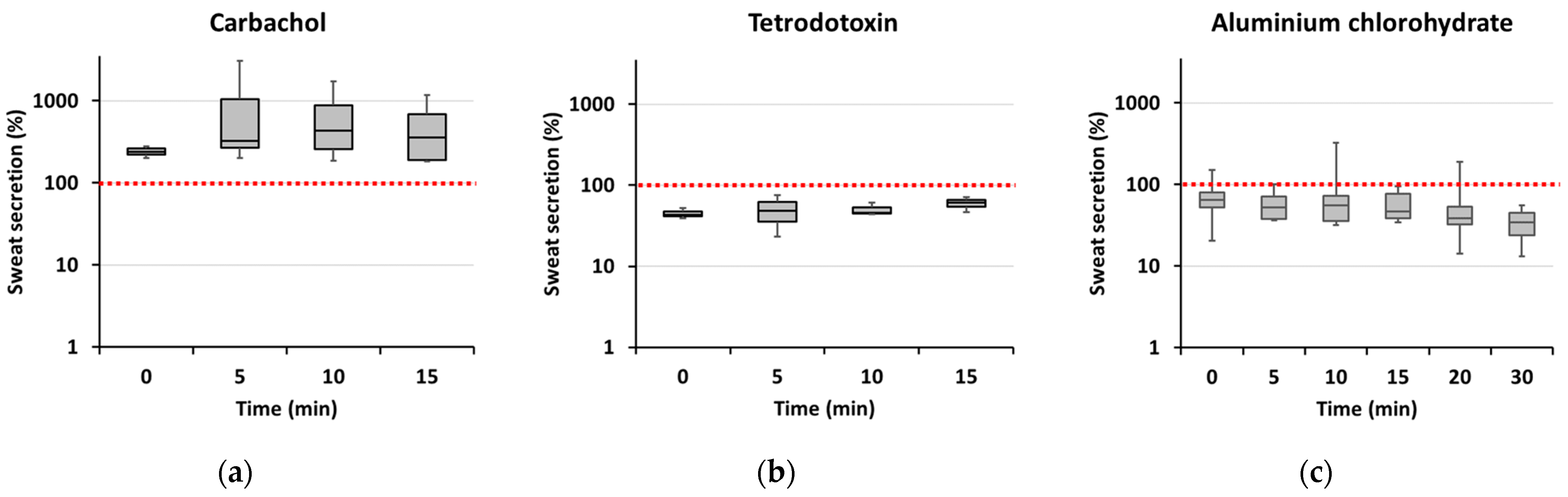
2.5. Establishing a Model for Sweat Provocation in Isolated Skin
3. Discussion
4. Materials and Methods
4.1. Cohorts of CholU Patients and Healthy Controls
4.2. Sweat Collection in CholU Patients and Healthy Controls
4.3. Immunofluorescence Staining
4.4. pH and Electrolyte Measurements
4.5. Ex Vivo Skin Model for Sweat Provocation and Inhibition
4.6. Evaluation of Sweat Production
4.7. Skin Explant Culture
4.8. Statistics
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pozderac, I.; Lugovic-Mihic, L.; Artukovic, M.; Stipic-Markovic, A.; Kuna, M.; Fercek, I. Chronic inducible urticaria: Classification and prominent features of physical and non-physical types. Acta Dermatovenerol. Alp. Pannonica Adriat. 2020, 29, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Abdul Latiff, A.H.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Ballmer-Weber, B.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; et al. The international EAACI/GA(2)LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022, 77, 734–766. [Google Scholar] [CrossRef] [PubMed]
- Gastaminza, G.; Azofra, J.; Nunez-Cordoba, J.M.; Baeza, M.L.; Echechipia, S.; Gaig, P.; Garcia, B.E.; Labrador-Horrillo, M.; Sala-Cunill, A.; Bresco, M.S.; et al. Efficacy and Safety of Omalizumab (Xolair) for Cholinergic Urticaria in Patients Unresponsive to a Double Dose of Antihistamines: A Randomized Mixed Double-Blind and Open-Label Placebo-Controlled Clinical Trial. J. Allergy Clin. Immunol. Pract. 2019, 7, 1599–1609.e1. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Munzberger, C.; Haustein, U.; Trippas, E.; Burtin, B.; Mariz, S.D.; Henz, B.M. Double-blind crossover study of high-dose cetirizine in cholinergic urticaria. Dermatology 1996, 193, 324–327. [Google Scholar] [CrossRef]
- Ghazanfar, M.N.; Holm, J.G.; Thomsen, S.F. Omalizumab for cholinergic urticaria: 6 months prospective study and systematic review of the literature. Dermatol. Ther. 2020, 33, e14010. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, H.S.; Ye, Y.M.; Shin, Y.S.; Kang, H.R.; Chung, S.J.; Choi, J.H. Omalizumab Treatment in Patients With Cholinergic Urticaria: A Real-World Retrospective Study in Korea. Allergy Asthma Immunol. Res. 2020, 12, 894–896. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, M.G. Cholinergic urticaria: More than a simple inducible urticaria. Australas. J. Dermatol. 2017, 58, e193–e198. [Google Scholar] [CrossRef]
- Fukunaga, A.; Washio, K.; Hatakeyama, M.; Oda, Y.; Ogura, K.; Horikawa, T.; Nishigori, C. Cholinergic urticaria: Epidemiology, physiopathology, new categorization, and management. Clin. Auton. Res. 2018, 28, 103–113. [Google Scholar] [CrossRef]
- Fukunaga, A.; Oda, Y.; Imamura, S.; Mizuno, M.; Fukumoto, T.; Washio, K. Cholinergic Urticaria: Subtype Classification and Clinical Approach. Am. J. Clin. Dermatol. 2023, 24, 41–54. [Google Scholar] [CrossRef]
- Tokura, Y. Direct and indirect action modes of acetylcholine in cholinergic urticaria. Allergol. Int. 2021, 70, 39–44. [Google Scholar] [CrossRef]
- Wang, Y.; Scheffel, J.; Vera, C.A.; Liu, W.; Günzel, D.; Terhorst-Molawi, D.; Maurer, M.; Altrichter, S. Impaired sweating in patients with cholinergic urticaria is linked to low expression of acetylcholine receptor CHRM3 and acetylcholine esterase in sweat glands. Front. Immunol. 2022, 13, 955161. [Google Scholar] [CrossRef] [PubMed]
- Blandina, P.; Fantozzi, R.; Mannaioni, P.F.; Masini, E. Characteristics of histamine release evoked by acetylcholine in isolated rat mast cells. J. Physiol. 1980, 301, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Aiba, S.; Yamagishi, T.; Tanita, M.; Hara, M.; Saito, H.; Tagami, H. Cholinergic urticaria, a new pathogenic concept: Hypohidrosis due to interference with the delivery of sweat to the skin surface. Dermatology 2002, 204, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Yamaga, K.; Murota, H.; Tamura, A.; Miyata, H.; Ohmi, M.; Kikuta, J.; Ishii, M.; Tsukita, S.; Katayama, I. Claudin-3 Loss Causes Leakage of Sweat from the Sweat Gland to Contribute to the Pathogenesis of Atopic Dermatitis. J. Invest. Dermatol. 2018, 138, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Tani, K.; Fujiyoshi, Y. Crystal structures of claudins: Insights into their intermolecular interactions. Ann. N. Y. Acad. Sci. 2017, 1397, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Furuse, M.; Takai, Y. Recent advances in understanding tight junctions. Fac. Rev. 2021, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.C.; Higashi, T.; Fukazawa, Y.; Otani, T.; Tauchi, M.; Higashi, A.Y.; Furuse, M.; Chiba, H. Occludin and tricellulin facilitate formation of anastomosing tight-junction strand network to improve barrier function. Mol. Biol. Cell 2021, 32, 722–738. [Google Scholar] [CrossRef] [PubMed]
- Klar, J.; Piontek, J.; Milatz, S.; Tariq, M.; Jameel, M.; Breiderhoff, T.; Schuster, J.; Fatima, A.; Asif, M.; Sher, M.; et al. Altered paracellular cation permeability due to a rare CLDN10B variant causes anhidrosis and kidney damage. PLoS Genet. 2017, 13, e1006897. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.S.; Hussein, M.; Alswailem, M.; Mouna, A.; Albalawi, L.; Moria, Y.; Jabbar, M.A.; Shi, Y.; Günzel, D.; Dasouki, M. A novel claudin-10 mutation with a unique mechanism in two unrelated families with HELIX syndrome. Kidney Int. 2021, 100, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Sewerin, S.; Piontek, J.; Schonauer, R.; Grunewald, S.; Rauch, A.; Neuber, S.; Bergmann, C.; Günzel, D.; Halbritter, J. Defective claudin-10 causes a novel variation of HELIX syndrome through compromised tight junction strand assembly. Genes. Dis. 2022, 9, 1301–1314. [Google Scholar] [CrossRef]
- Yanagida, N.; Takahagi, S.; Aoyama, Y.; Tanaka, A.; Hide, M. Anhidrosis accompanied by cholinergic urticaria-like rash and dermal pain in a patient with Sjogren’s syndrome. J. Dermatol. 2022, 49, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Qudair, A.; Hussein, M.; Alowain, M.; Al-Hassnan, Z.N.; Alfaifi, A.; Alfalah, A.; Al-Qahtani, M.; Alkuraya, F.S. Clinical and molecular features of four families with CLDN10-related HELIX syndrome. Eur. J. Med. Genet. 2023, 66, 104886. [Google Scholar] [CrossRef] [PubMed]
- Meyers, N.; Nelson-Williams, C.; Malaga-Dieguez, L.; Kaufmann, H.; Loring, E.; Knight, J.; Lifton, R.P.; Trachtman, H. Hypokalemia Associated With a Claudin 10 Mutation: A Case Report. Am. J. Kidney Dis. 2019, 73, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Hadj-Rabia, S.; Brideau, G.; Al-Sarraj, Y.; Maroun, R.C.; Figueres, M.L.; Leclerc-Mercier, S.; Olinger, E.; Baron, S.; Chaussain, C.; Nochy, D.; et al. Multiplex epithelium dysfunction due to CLDN10 mutation: The HELIX syndrome. Genet. Med. 2018, 20, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Milatz, S. A Novel Claudinopathy Based on Claudin-10 Mutations. Int. J. Mol. Sci. 2019, 20, 5396. [Google Scholar] [CrossRef] [PubMed]
- Krug, S.M.; Schulzke, J.D.; Fromm, M. Tight junction, selective permeability, and related diseases. Semin. Cell Dev. Biol. 2014, 36, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Van Itallie, C.M.; Rogan, S.; Yu, A.; Vidal, L.S.; Holmes, J.; Anderson, J.M. Two splice variants of claudin-10 in the kidney create paracellular pores with different ion selectivities. Am. J. Physiol. Renal Physiol. 2006, 291, F1288–F1299. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.B.; Wolfe, A.S. Physiological mechanisms determining eccrine sweat composition. Eur. J. Appl. Physiol. 2020, 120, 719–752. [Google Scholar] [CrossRef]
- Tamura, A.; Tsukita, S. Paracellular barrier and channel functions of TJ claudins in organizing biological systems: Advances in the field of barriology revealed in knockout mice. Semin. Cell Dev. Biol. 2014, 36, 177–185. [Google Scholar] [CrossRef]
- Anderson, J.M.; Van Itallie, C.M. Physiology and function of the tight junction. Cold Spring Harb. Perspect. Biol. 2009, 1, a002584. [Google Scholar] [CrossRef]
- Wickham, K.A.; McCarthy, D.G.; Spriet, L.L.; Cheung, S.S. Sex differences in the physiological responses to exercise-induced dehydration: Consequences and mechanisms. J. Appl. Physiol. (1985) 2021, 131, 504–510. [Google Scholar] [CrossRef]
- Sehl, P.L.; Leites, G.T.; Martins, J.B.; Meyer, F. Responses of obese and non-obese boys cycling in the heat. Int. J. Sports Med. 2012, 33, 497–501. [Google Scholar] [CrossRef]
- Nakamizo, S.; Egawa, G.; Miyachi, Y.; Kabashima, K. Cholinergic urticaria: Pathogenesis-based categorization and its treatment options. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 114–116. [Google Scholar] [CrossRef]
- Coyne, C.B.; Gambling, T.M.; Boucher, R.C.; Carson, J.L.; Johnson, L.G. Role of claudin interactions in airway tight junctional permeability. Am. J. Physiol. Lung Cell Mol. Physiol. 2003, 285, L1166–L1178. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Oshima, T.; Tomita, T.; Kim, Y.; Matsumoto, T.; Joh, T.; Miwa, H. Oxidative stress induces gastric epithelial permeability through claudin-3. Biochem. Biophys. Res. Commun. 2008, 376, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Van Itallie, C.M.; Fanning, A.S.; Holmes, J.; Anderson, J.M. Occludin is required for cytokine-induced regulation of tight junction barriers. J. Cell Sci. 2010, 123 Pt 16, 2844–2852. [Google Scholar] [CrossRef]
- Al-Sadi, R.; Khatib, K.; Guo, S.; Ye, D.; Youssef, M.; Ma, T. Occludin regulates macromolecule flux across the intestinal epithelial tight junction barrier. Am. J. Physiol. Gastrointest. Liver Physiol. 2011, 300, G1054–G1064. [Google Scholar] [CrossRef] [PubMed]
- Milatz, S.; Himmerkus, N.; Wulfmeyer, V.C.; Drewell, H.; Mutig, K.; Hou, J.; Breiderhoff, T.; Müller, D.; Fromm, M.; Bleich, M.; et al. Mosaic expression of claudins in thick ascending limbs of Henle results in spatial separation of paracellular Na+ and Mg2+ transport. Proc. Natl. Acad. Sci. USA 2017, 114, E219–E227. [Google Scholar] [CrossRef]
- Prot-Bertoye, C.; Griveau, C.; Skjodt, K.; Cheval, L.; Brideau, G.; Lievre, L.; Ferriere, E.; Arbaretaz, F.; Garbin, K.; Zamani, R.; et al. Differential localization patterns of claudin 10, 16, and 19 in human, mouse, and rat renal tubular epithelia. Am. J. Physiol. Renal Physiol. 2021, 321, F207–F224. [Google Scholar] [CrossRef] [PubMed]
- Klous, L.; Folkerts, M.; Daanen, H.; Gerrett, N. The effect of sweat sample storage condition on sweat content. Temperature 2021, 8, 254–261. [Google Scholar] [CrossRef]
- Ely, M.R.; Kenefick, R.W.; Cheuvront, S.N.; Chinevere, T.; Lacher, C.P.; Lukaski, H.C.; Montain, S.J. The effect of heat acclimation on sweat microminerals: Artifact of surface contamination. Int. J. Sport. Nutr. Exerc. Metab. 2013, 23, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.M.; Light, M.J.; Quinton, P.M. Activation of the epithelial Na+ channel (ENaC) requires CFTR Cl− channel function. Nature 1999, 402, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Klaka, P.; Grudl, S.; Banowski, B.; Giesen, M.; Sattler, A.; Proksch, P.; Welss, T.; Forster, T. A novel organotypic 3D sweat gland model with physiological functionality. PLoS ONE 2017, 12, e0182752. [Google Scholar] [CrossRef] [PubMed]
- Elizondo, R.S. Primate models to study eccrine sweating. Am. J. Primatol. 1988, 14, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Ban, C.; Kwoen, D.H. Objective Quantitation of Focal Sweating Areas Using a Mouse Sweat-assay Model. Bio-Protocol 2021, 11, e4047. [Google Scholar] [CrossRef] [PubMed]
- Altrichter, S.; Salow, J.; Ardelean, E.; Church, M.K.; Werner, A.; Maurer, M. Development of a standardized pulse-controlled ergometry test for diagnosing and investigating cholinergic urticaria. J. Dermatol. Sci. 2014, 75, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Altrichter, S.; Wang, Y.; Schumacher, P.; Alraboni, O.; Church, M.K.; Maurer, M. Acetylcholine-induced whealing in cholinergic urticaria—What does it tell us? J. Dermatol. Sci. 2021, 103, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Minor, V. Ein neues Verfahren zu der klinischen Untersuchung der Schweißabsonderung. Dtsch. Z. Nervenheilkd. 1928, 101, 302–308. [Google Scholar] [CrossRef]
- Hexsel, D.; Rodrigues, T.C.; Soirefmann, M.; Zechmeister-Prado, D. Recommendations for performing and evaluating the results of the minor test according to a sweating intensity visual scale. Dermatol. Surg. 2010, 36, 120–122. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Control | CholU Patient | p-Value (t-Test) | |
|---|---|---|---|
| Number (m/f) | 59 (31, 28) | 39 (16, 23) | |
| Age ([years]; mean ± SEM; n) | 30.76 ± 0.99; 59 | 34.74 ± 1.93; 39 | 0.05 |
| BMI ([kg/m2]; mean ± SEM; n) | 23.27 ± 0.43; 55 | 24.69 ± 0.66; 39 | 0.06 |
| Sweat volume ([mL]; mean ± SEM; n) | |||
| all | 108.12 ± 8.59; 59 | 101.10 ± 12.27; 39 | 0.63 |
| male | 131.44 ± 9.65; 31 | 147.50 ± 20.57; 16 | 0.42 |
| female | 82.30 ± 13.15; 28 | 68.83 ± 11.16; 23 | 0.53 |
| pH | Na+ [mM] | Cl− [mM] | K+ [mM] | Ca2+ [mM] | Mg2+ [mM] | |
|---|---|---|---|---|---|---|
| Healthy Controls | ||||||
| MW ± SEM | 7.33 ± 0.25 | 42.51 ± 3.13 | 41.47 ± 1.99 | 6.19 ± 0.61 | 1.04 ± 0.11 | 0.27 ± 0.06 |
| n | 20 | 39 | 39 | 39 | 39 | 25 |
| CholU patients | ||||||
| MW ± SEM | 7.58 ± 0.21 | 47.60 ± 3.34 | 45.58 ± 2.23 | 8.54 ± 0.57 | 1.40 ± 0.10 | 0.27 ± 0.04 |
| n | 20 | 36 | 36 | 36 | 36 | 25 |
| p-value | 0.46 | 0.27 | 0.17 | 0.01 | 0.02 | 0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daci, D.; Altrichter, S.; Grillet, F.M.; Dib, S.; Mouna, A.; Suresh Kumar, S.; Terhorst-Molawi, D.; Maurer, M.; Günzel, D.; Scheffel, J. Altered Sweat Composition Due to Changes in Tight Junction Expression of Sweat Glands in Cholinergic Urticaria Patients. Int. J. Mol. Sci. 2024, 25, 4658. https://doi.org/10.3390/ijms25094658
Daci D, Altrichter S, Grillet FM, Dib S, Mouna A, Suresh Kumar S, Terhorst-Molawi D, Maurer M, Günzel D, Scheffel J. Altered Sweat Composition Due to Changes in Tight Junction Expression of Sweat Glands in Cholinergic Urticaria Patients. International Journal of Molecular Sciences. 2024; 25(9):4658. https://doi.org/10.3390/ijms25094658
Chicago/Turabian StyleDaci, Denisa, Sabine Altrichter, François Marie Grillet, Selma Dib, Ahmad Mouna, Sukashree Suresh Kumar, Dorothea Terhorst-Molawi, Marcus Maurer, Dorothee Günzel, and Jörg Scheffel. 2024. "Altered Sweat Composition Due to Changes in Tight Junction Expression of Sweat Glands in Cholinergic Urticaria Patients" International Journal of Molecular Sciences 25, no. 9: 4658. https://doi.org/10.3390/ijms25094658
APA StyleDaci, D., Altrichter, S., Grillet, F. M., Dib, S., Mouna, A., Suresh Kumar, S., Terhorst-Molawi, D., Maurer, M., Günzel, D., & Scheffel, J. (2024). Altered Sweat Composition Due to Changes in Tight Junction Expression of Sweat Glands in Cholinergic Urticaria Patients. International Journal of Molecular Sciences, 25(9), 4658. https://doi.org/10.3390/ijms25094658