
Analysis of SIRT1 Gene SNPs and Clinical Characteristics in Medication-Related Osteonecrosis of the Jaw

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Results
2.1. Study Population
2.2. SIRT1 SNP Genotyping
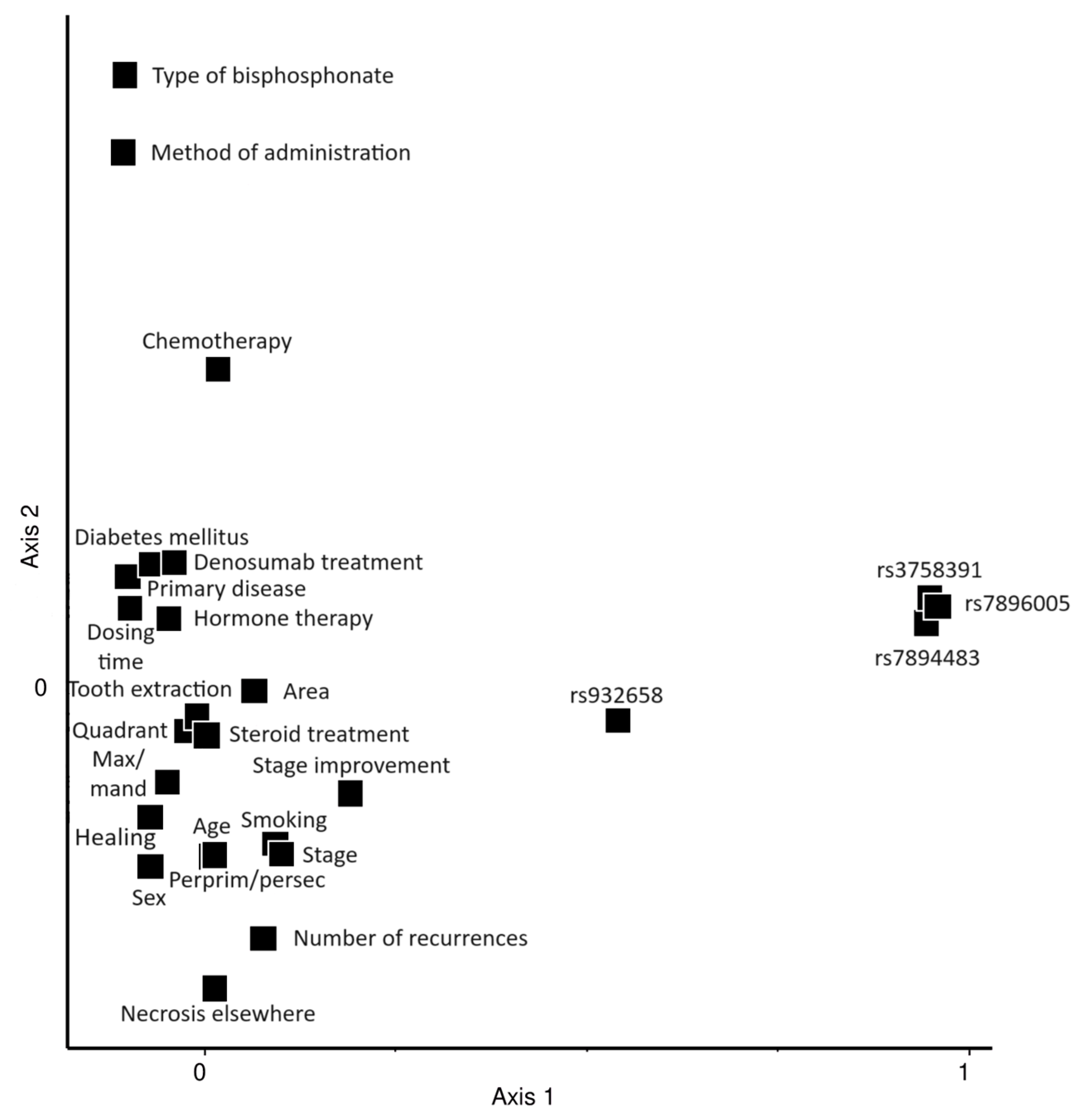
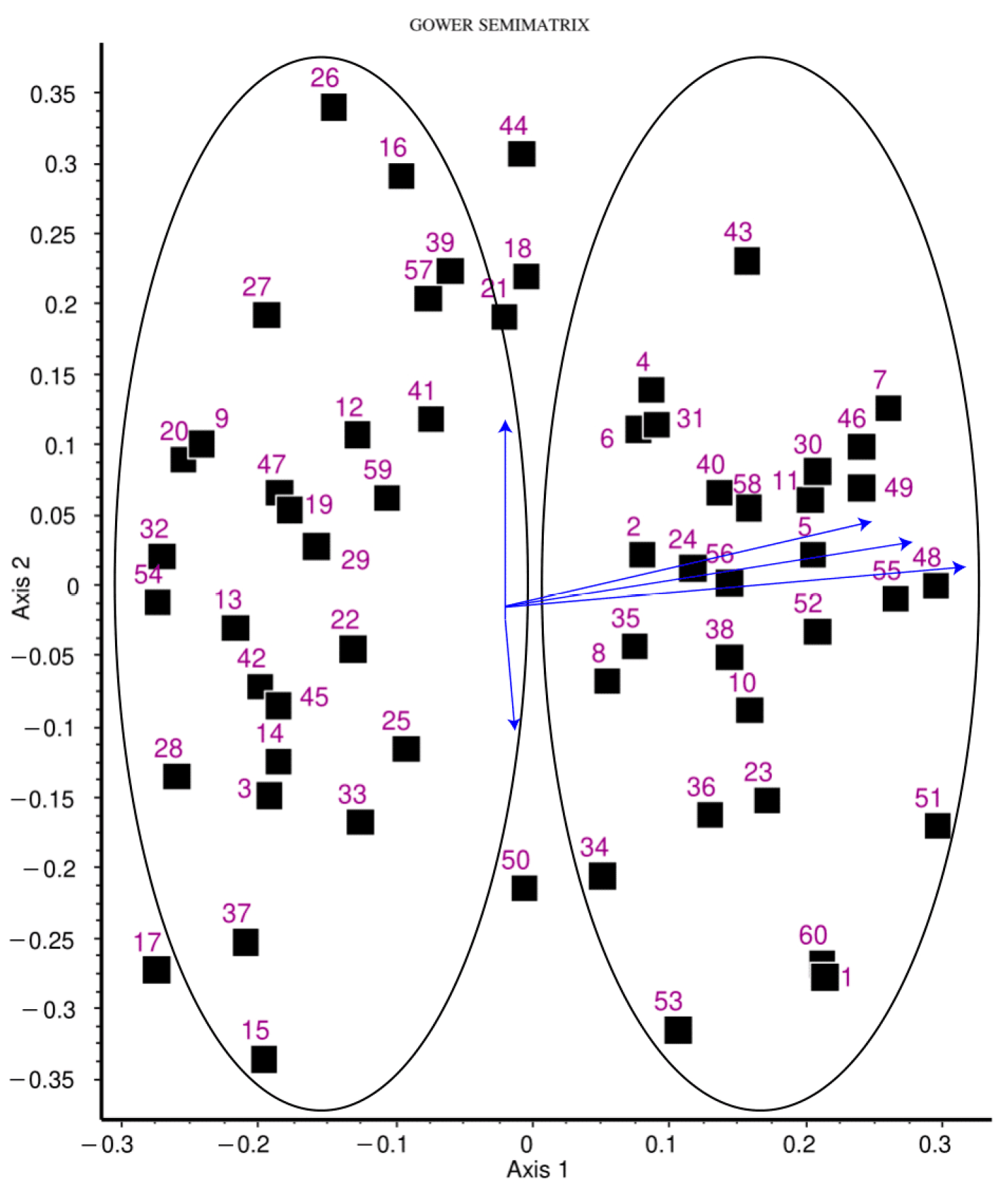
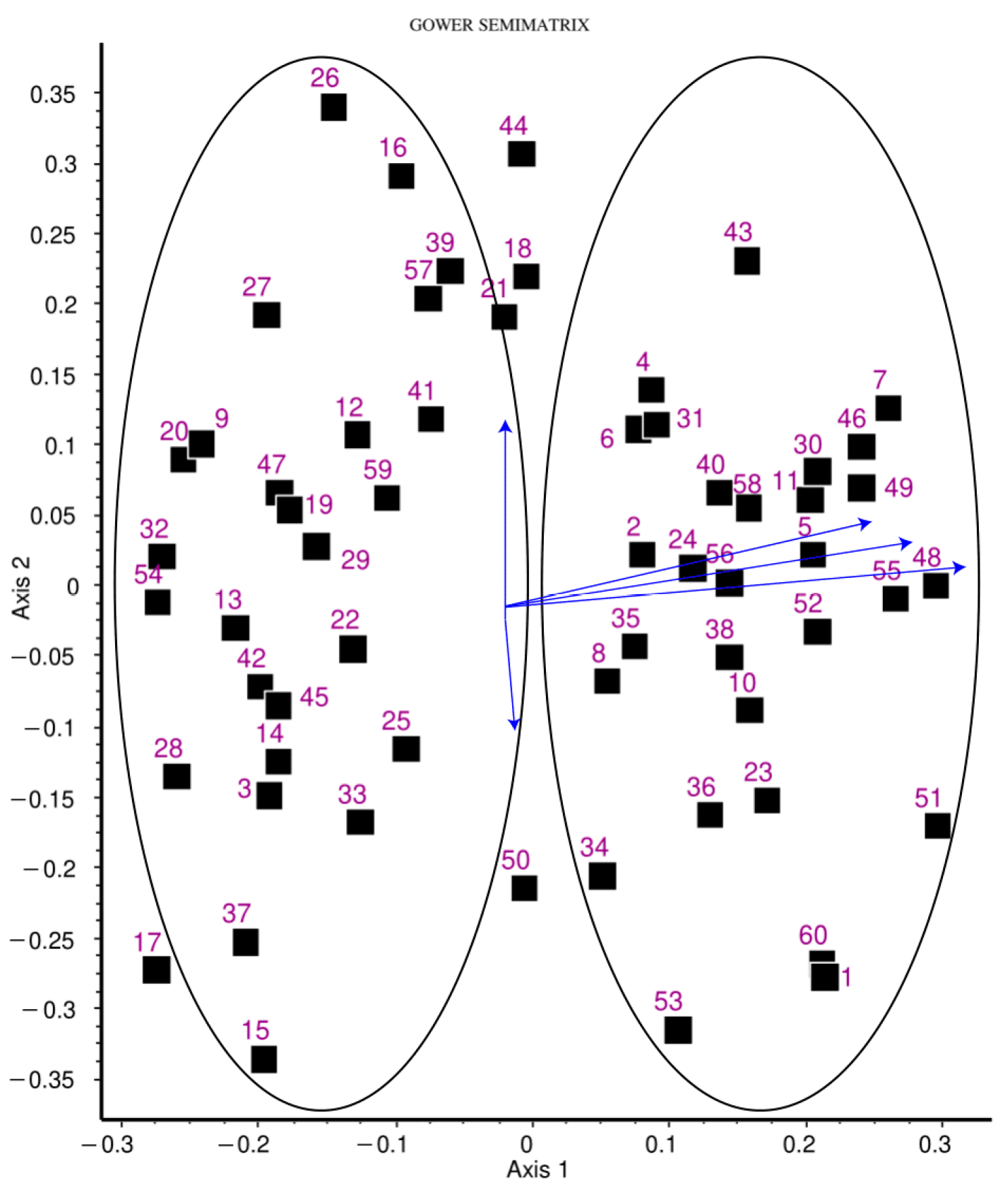
2.3. Multivariate Statistical Analysis
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Genotyping
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miksad, R.A.; Lai, K.C.; Dodson, T.B.; Woo, S.B.; Treister, N.S.; Akinyemi, O.; Bihrle, M.; Maytal, G.; August, M.; Gazelle, G.S.; et al. Quality of life implications of bisphosphonate-associated osteonecrosis of the jaw. Oncologist 2011, 16, 121–132. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral. Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Cadieux, B.; Coleman, R.; Jafarinasabian, P.; Lipton, A.; Orlowski, R.Z.; Saad, F.; Scagliotti, G.V.; Shimizu, K.; Stopeck, A. Experience with denosumab (XGEVA(R)) for prevention of skeletal-related events in the 10 years after approval. J. Bone Oncol. 2022, 33, 100416. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.R.; Saunders, Y.; Edmonds, P.M.; Patel, S.; Broadley, K.E.; Johnston, S.R. Systematic review of role of bisphosphonates on skeletal morbidity in metastatic cancer. BMJ 2003, 327, 469. [Google Scholar] [CrossRef]
- De Cicco, D.; Boschetti, C.E.; Santagata, M.; Colella, G.; Stagliano, S.; Gaggl, A.; Bottini, G.B.; Vitagliano, R.; D’Amato, S. Medication-Related Osteonecrosis of the Jaws: A Comparison of SICMF-SIPMO and AAOMS Guidelines. Diagnostics 2023, 13, 2137. [Google Scholar] [CrossRef]
- Kaczoruk-Wieremczuk, M.; Adamska, P.; Adamski, L.J.; Wychowanski, P.; Jereczek-Fossa, B.A.; Starzynska, A. Oral Surgery Procedures in a Patient with Hajdu-Cheney Syndrome Treated with Denosumab—A Rare Case Report. Int. J. Environ. Res. Public Health 2021, 18, 9099. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.L.; Tu, M.M.; Ibrahim, M.F.K.; Basulaiman, B.; McGee, S.F.; Srikanthan, A.; Fernandes, R.; Vandermeer, L.; Stober, C.; Sienkiewicz, M.; et al. Long-term impact of bone-modifying agents for the treatment of bone metastases: A systematic review. Support. Care Cancer 2021, 29, 925–943. [Google Scholar] [CrossRef]
- Gnant, M.; Mlineritsch, B.; Stoeger, H.; Luschin-Ebengreuth, G.; Knauer, M.; Moik, M.; Jakesz, R.; Seifert, M.; Taucher, S.; Bjelic-Radisic, V.; et al. Zoledronic acid combined with adjuvant endocrine therapy of tamoxifen versus anastrozol plus ovarian function suppression in premenopausal early breast cancer: Final analysis of the Austrian Breast and Colorectal Cancer Study Group Trial 12. Ann. Oncol. 2015, 26, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Raje, N.; Terpos, E.; Willenbacher, W.; Shimizu, K.; Garcia-Sanz, R.; Durie, B.; Legiec, W.; Krejci, M.; Laribi, K.; Zhu, L.; et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: An international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018, 19, 370–381. [Google Scholar] [CrossRef]
- Saag, K.G.; Petersen, J.; Brandi, M.L.; Karaplis, A.C.; Lorentzon, M.; Thomas, T.; Maddox, J.; Fan, M.; Meisner, P.D.; Grauer, A. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef]
- Hallmer, F.; Andersson, G.; Gotrick, B.; Warfvinge, G.; Anderud, J.; Bjornland, T. Prevalence, initiating factor, and treatment outcome of medication-related osteonecrosis of the jaw-a 4-year prospective study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2018, 126, 477–485. [Google Scholar] [CrossRef]
- Bone, H.G.; Wagman, R.B.; Brandi, M.L.; Brown, J.P.; Chapurlat, R.; Cummings, S.R.; Czerwinski, E.; Fahrleitner-Pammer, A.; Kendler, D.L.; Lippuner, K.; et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: Results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol. 2017, 5, 513–523. [Google Scholar] [CrossRef]
- Soundia, A.; Hadaya, D.; Esfandi, N.; de Molon, R.S.; Bezouglaia, O.; Dry, S.M.; Pirih, F.Q.; Aghaloo, T.; Tetradis, S. Osteonecrosis of the jaws (ONJ) in mice after extraction of teeth with periradicular disease. Bone 2016, 90, 133–141. [Google Scholar] [CrossRef]
- Soma, T.; Iwasaki, R.; Sato, Y.; Kobayashi, T.; Nakamura, S.; Kaneko, Y.; Ito, E.; Okada, H.; Watanabe, H.; Miyamoto, K.; et al. Tooth extraction in mice administered zoledronate increases inflammatory cytokine levels and promotes osteonecrosis of the jaw. J. Bone Miner. Metab. 2021, 39, 372–384. [Google Scholar] [CrossRef]
- Mawardi, H.; Giro, G.; Kajiya, M.; Ohta, K.; Almazrooa, S.; Alshwaimi, E.; Woo, S.B.; Nishimura, I.; Kawai, T. A role of oral bacteria in bisphosphonate-induced osteonecrosis of the jaw. J. Dent. Res. 2011, 90, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Hamadeh, I.S.; Katz, J.; Riva, A.; Lakatos, P.; Balla, B.; Kosa, J.; Vaszilko, M.; Pelliccioni, G.A.; Davis, N.; et al. SIRT1/HERC4 Locus Associated With Bisphosphonate-Induced Osteonecrosis of the Jaw: An Exome-Wide Association Analysis. J. Bone Miner. Res. 2018, 33, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Collins, J.M.; Rafiee, R.; Singh, S.; Langaee, T.; McDonough, C.W.; Holliday, L.S.; Wang, D.; Lamba, J.K.; Kim, Y.S.; et al. SIRT1 Gene SNP rs932658 Is Associated With Medication-Related Osteonecrosis of the Jaw. J. Bone Miner. Res. 2021, 36, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Balla, B.; Vaszilko, M.; Kosa, J.P.; Podani, J.; Takacs, I.; Tobias, B.; Nagy, Z.; Lazary, A.; Lakatos, P. New approach to analyze genetic and clinical data in bisphosphonate-induced osteonecrosis of the jaw. Oral. Dis. 2012, 18, 580–585. [Google Scholar] [CrossRef]
- Sarasquete, M.E.; Garcia-Sanz, R.; Marin, L.; Alcoceba, M.; Chillon, M.C.; Balanzategui, A.; Santamaria, C.; Rosinol, L.; de la Rubia, J.; Hernandez, M.T.; et al. Bisphosphonate-related osteonecrosis of the jaw is associated with polymorphisms of the cytochrome P450 CYP2C8 in multiple myeloma: A genome-wide single nucleotide polymorphism analysis. Blood 2008, 112, 2709–2712. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, Y.; Wang, Y.; Chao, Y.; Zhang, J.; Jia, Y.; Tie, J.; Hu, D. Regulation of SIRT1 and Its Roles in Inflammation. Front. Immunol. 2022, 13, 831168. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhou, M.; Ge, Y.; Wang, X. SIRT1 and aging related signaling pathways. Mech. Ageing Dev. 2020, 187, 111215. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, F.; Liu, H.; Li, J.; Che, H.; Shen, J.; Luo, E. SIRT1, a promising regulator of bone homeostasis. Life Sci. 2021, 269, 119041. [Google Scholar] [CrossRef]
- Yang, G.; Singh, S.; McDonough, C.W.; Lamba, J.K.; Hamadeh, I.; Holliday, L.S.; Wang, D.; Katz, J.; Lakatos, P.A.; Balla, B.; et al. Genome-wide Association Study Identified Chromosome 8 Locus Associated with Medication-Related Osteonecrosis of the Jaw. Clin. Pharmacol. Ther. 2021, 110, 1558–1569. [Google Scholar] [CrossRef]
- Kastritis, E.; Melea, P.; Bagratuni, T.; Melakopoulos, I.; Gavriatopoulou, M.; Roussou, M.; Migkou, M.; Eleutherakis-Papaiakovou, E.; Terpos, E.; Dimopoulos, M.A. Genetic factors related with early onset of osteonecrosis of the jaw in patients with multiple myeloma under zoledronic acid therapy. Leuk. Lymphoma 2017, 58, 2304–2309. [Google Scholar] [CrossRef]
- Guo, Z.; Cui, W.; Que, L.; Li, C.; Tang, X.; Liu, J. Pharmacogenetics of medication-related osteonecrosis of the jaw: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2020, 49, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Mun, S.; Shin, W.; Han, K.; Kim, M.Y. Identification of Potentially Pathogenic Variants Associated with Recurrence in Medication-Related Osteonecrosis of the Jaw (MRONJ) Patients Using Whole-Exome Sequencing. J. Clin. Med. 2022, 11, 2145. [Google Scholar] [CrossRef] [PubMed]
- Stockmann, P.; Nkenke, E.; Englbrecht, M.; Schlittenbauer, T.; Wehrhan, F.; Rauh, C.; Beckmann, M.W.; Fasching, P.A.; Kreusch, T.; Mackensen, A.; et al. Major histocompatibility complex class II polymorphisms are associated with the development of anti-resorptive agent-induced osteonecrosis of the jaw. J. Craniomaxillofac Surg. 2013, 41, 71–75. [Google Scholar] [CrossRef]
- Li, Q.; Cheng, J.C.; Jiang, Q.; Lee, W.Y. Role of sirtuins in bone biology: Potential implications for novel therapeutic strategies for osteoporosis. Aging Cell 2021, 20, e13301. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral. Dis. 2018, 24, 527–536. [Google Scholar] [CrossRef]
- SDCEP. Oral health management of patients at risk of medication-related osteonecrosis of the jaw. Br. Dent. J. 2017, 222, 930. [Google Scholar] [CrossRef]
- Drudge-Coates, L.; Van den Wyngaert, T.; Schiodt, M.; van Muilekom, H.A.M.; Demonty, G.; Otto, S. Preventing, identifying, and managing medication-related osteonecrosis of the jaw: A practical guide for nurses and other allied healthcare professionals. Support. Care Cancer 2020, 28, 4019–4029. [Google Scholar] [CrossRef] [PubMed]
- Gower, J.C. A general coefficient of similarity and some of its properties. Biometrics 1971, 27, 857–871. [Google Scholar] [CrossRef]
- Podani, J.; Schmera, D.; Bagella, S. Correlating variables with different scale types: A new framework based on matrix comparisons. Methods Ecol. Evol. 2023, 14, 1049–1060. [Google Scholar] [CrossRef]
- Podani, J. SYN-TAX 2000. Computer programs for data analysis in ecology and systematics. In User’s Manual Scientia, Budapest; Scientia Publishing: Budapest, Hungary, 2001. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MRONJ Patients n = 63 |
|---|---|
| Age (years) (mean ± SD) * | 69.33 ± 11.06 |
| Sex | |
| Female | 46 |
| Male | 17 |
| Duration of treatment (months) (mean ± SD) * | 46.42 ± 39.77 |
| Disorder * | |
| Breast cancer | 26 |
| Prostate cancer | 11 |
| Myeloma multiplex | 11 |
| Osteoporosis | 7 |
| Lung cancer | 2 |
| Melanoma malignum | 1 |
| Colon cancer | 1 |
| Cervical cancer | 1 |
| Chemotherapy * | |
| Yes | 38 |
| No | 22 |
| Hormone deprivation therapy | |
| Yes | 32 |
| No | 28 |
| Antiresorptive agent *, ** | |
| Alendronate (p.o.) | 1 |
| Ibandronate (p.o.) | 4 |
| Risedronate (p.o.) | 1 |
| Zoledronate (iv./inj.) | 29 |
| Denosumab (inj.) | 29 |
| MRONJ localization *, *** | |
| Maxilla | 19 |
| Mandibula | 42 |
| MRONJ stage *, **** | |
| 1 | 1 |
| 2 | 44 |
| 3 | 15 |
| SNP | Genotype 1 | Genotype 2 | Genotype 3 | Allele Frequency | ALFA | p-Value |
|---|---|---|---|---|---|---|
| rs932658 | CC: 65.1% (n = 41) | CA: 25.4% (n = 16) | AA: 9.5% (n = 6) | C:A 77.8:22.2 | C:A 59.9:40.1 | p = 4.5 × 10−5 |
| rs7896005 * | GG: 47.4% (n = 27) | GA: 40.3% (n = 23) | AA: 12.3% (n = 7) | G:A 67.5:32.5 | G:A 65.5:34.5 | ns. (p = 0.64) |
| rs7894483 ** | AA: 9.9% (n = 6) | AT: 39.3% (n = 24) | TT: 50.8% (n = 31) | A:T 29.5:70.5 | A:T 32.9:67.1 | ns. (p = 0.43) |
| rs3758391 ** | CC: 50.8% (n = 31) | CT: 37.7% (n = 23) | TT: 11.5% (n = 7) | C:T 69.7:30.3 | C:T 67.7:32.3 | ns. (p = 0.64) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bojtor, B.; Vaszilko, M.; Armos, R.; Tobias, B.; Podani, J.; Szentpeteri, S.; Balla, B.; Lengyel, B.; Piko, H.; Illes, A.; et al. Analysis of SIRT1 Gene SNPs and Clinical Characteristics in Medication-Related Osteonecrosis of the Jaw. Int. J. Mol. Sci. 2024, 25, 3646. https://doi.org/10.3390/ijms25073646
Bojtor B, Vaszilko M, Armos R, Tobias B, Podani J, Szentpeteri S, Balla B, Lengyel B, Piko H, Illes A, et al. Analysis of SIRT1 Gene SNPs and Clinical Characteristics in Medication-Related Osteonecrosis of the Jaw. International Journal of Molecular Sciences. 2024; 25(7):3646. https://doi.org/10.3390/ijms25073646
Chicago/Turabian StyleBojtor, Bence, Mihaly Vaszilko, Richard Armos, Balint Tobias, Janos Podani, Szofia Szentpeteri, Bernadett Balla, Balazs Lengyel, Henriett Piko, Anett Illes, and et al. 2024. "Analysis of SIRT1 Gene SNPs and Clinical Characteristics in Medication-Related Osteonecrosis of the Jaw" International Journal of Molecular Sciences 25, no. 7: 3646. https://doi.org/10.3390/ijms25073646
APA StyleBojtor, B., Vaszilko, M., Armos, R., Tobias, B., Podani, J., Szentpeteri, S., Balla, B., Lengyel, B., Piko, H., Illes, A., Kiss, A., Putz, Z., Takacs, I., Kosa, J. P., & Lakatos, P. (2024). Analysis of SIRT1 Gene SNPs and Clinical Characteristics in Medication-Related Osteonecrosis of the Jaw. International Journal of Molecular Sciences, 25(7), 3646. https://doi.org/10.3390/ijms25073646