
Exosomal Prostate-Specific Membrane Antigen (PSMA) and Caveolin-1 as Potential Biomarkers of Prostate Cancer—Evidence from Serbian Population
 , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
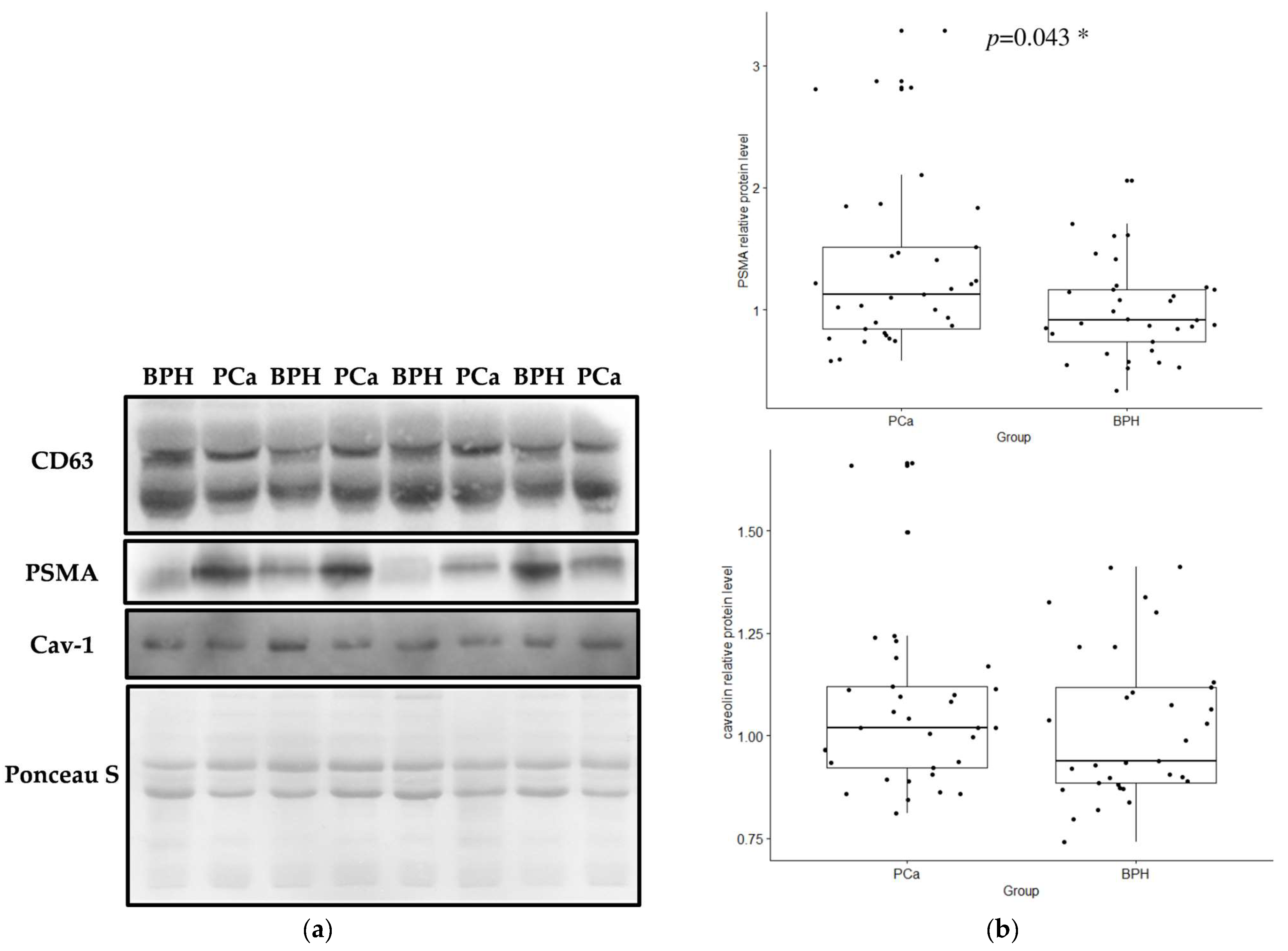
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Participants: Sample and Data Collection
4.2. Exosome Extraction
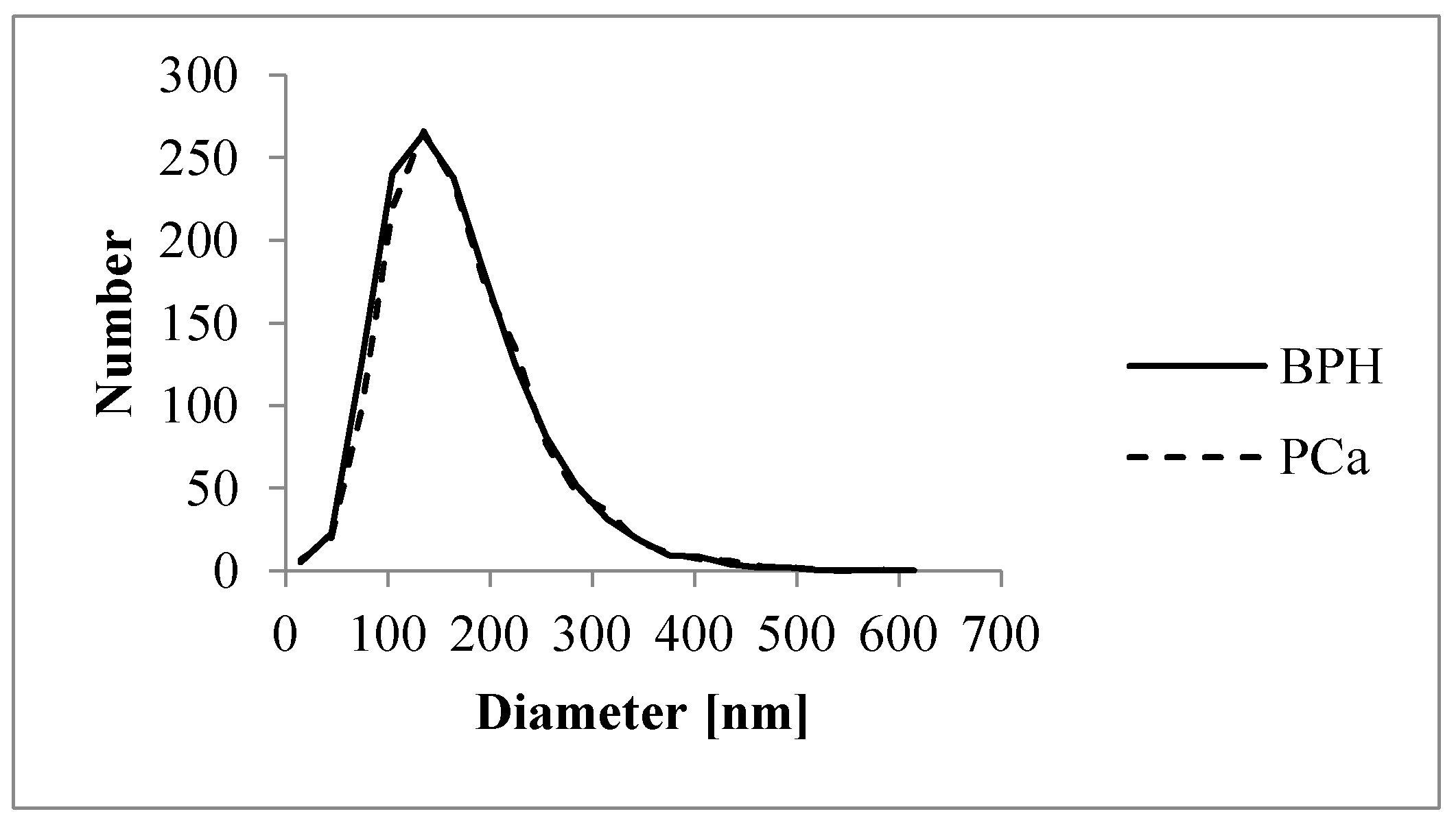
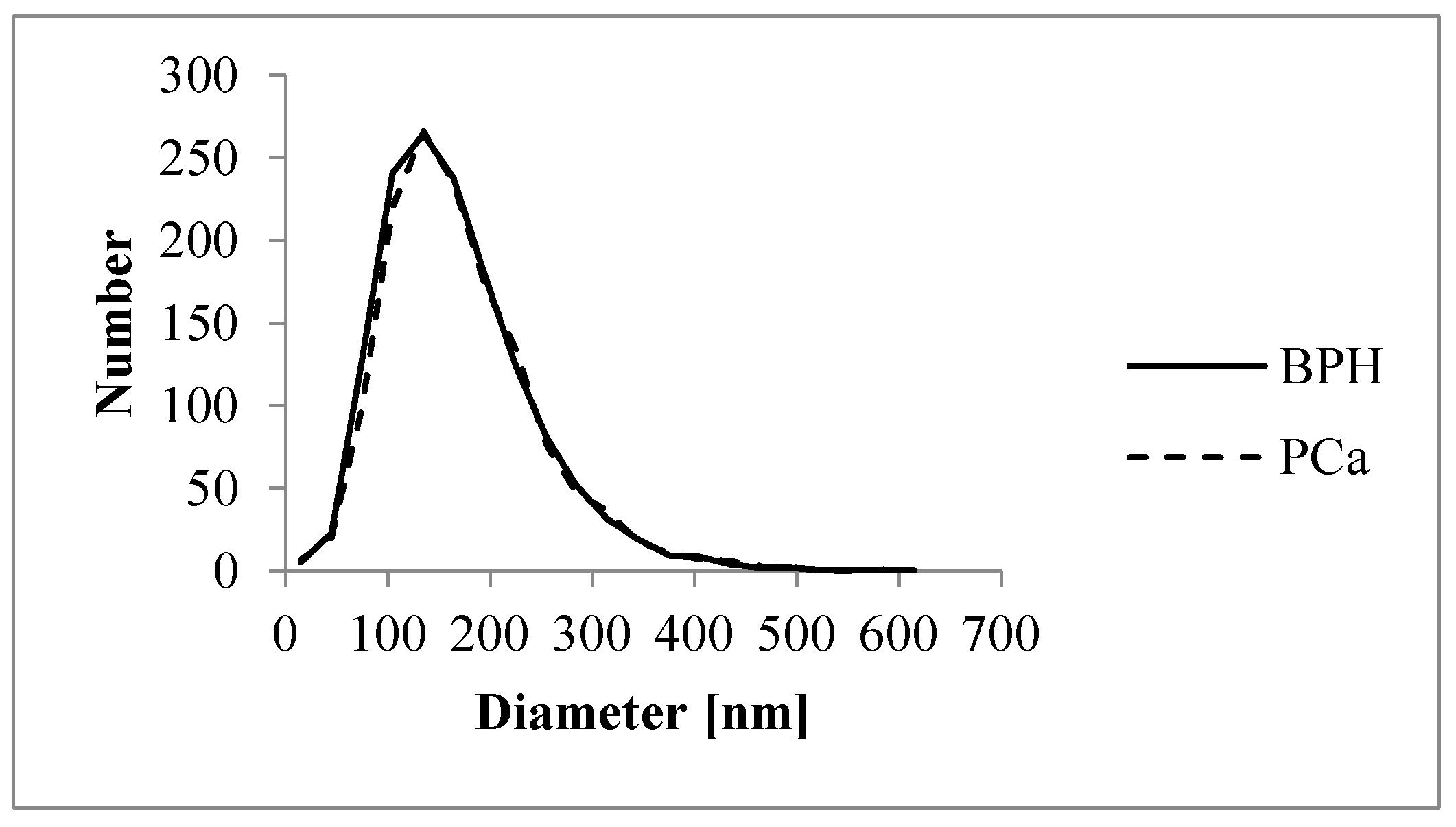
4.3. Nanoparticle-Tracking Analysis (NTA)
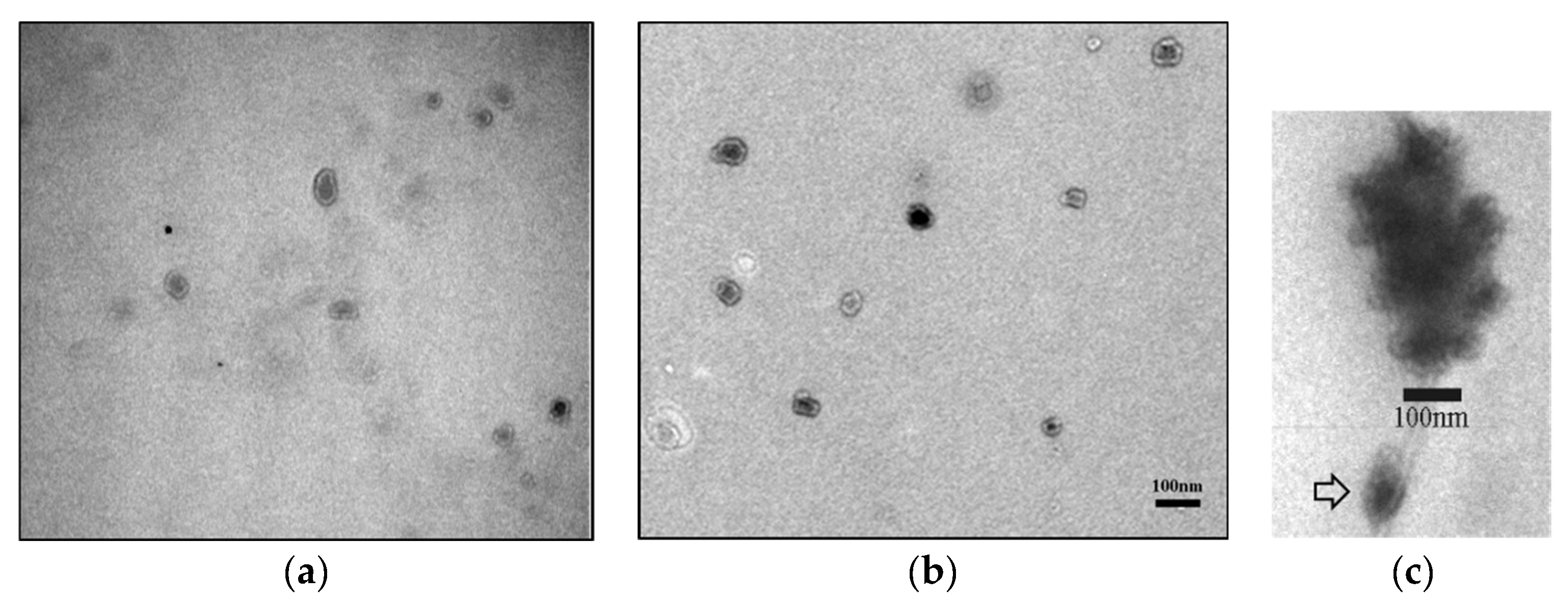
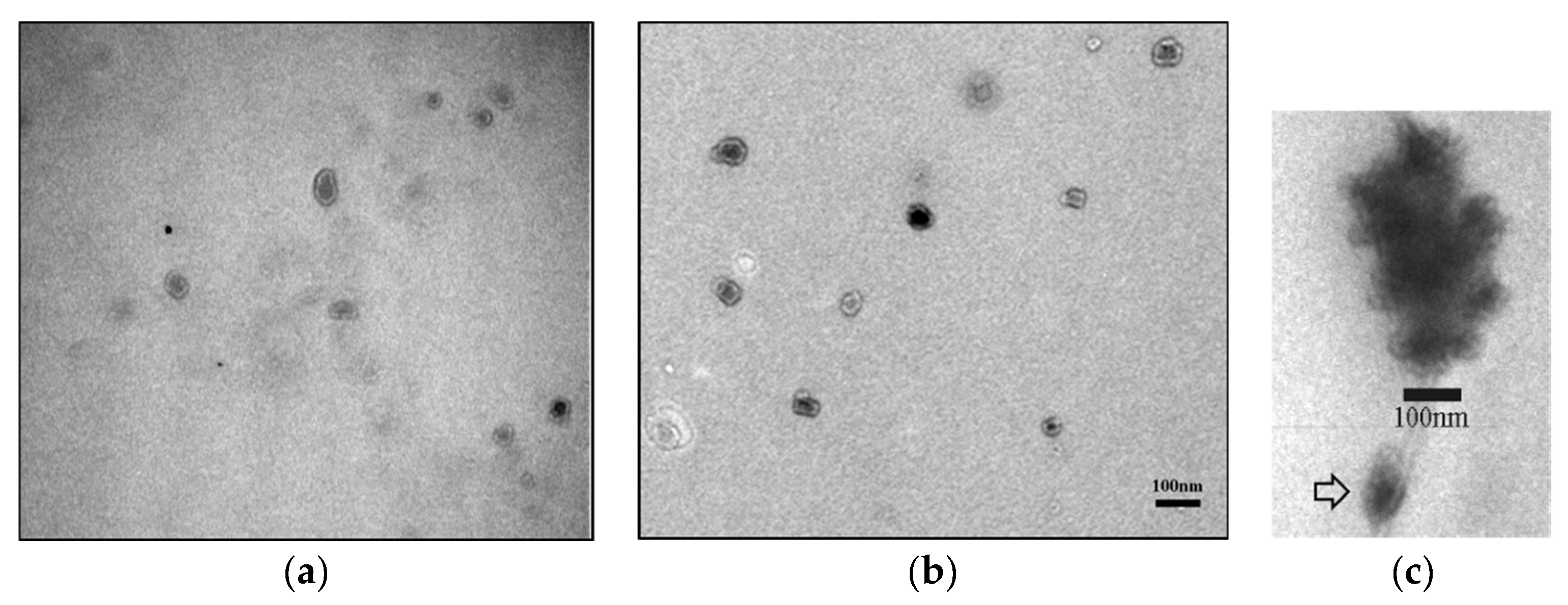
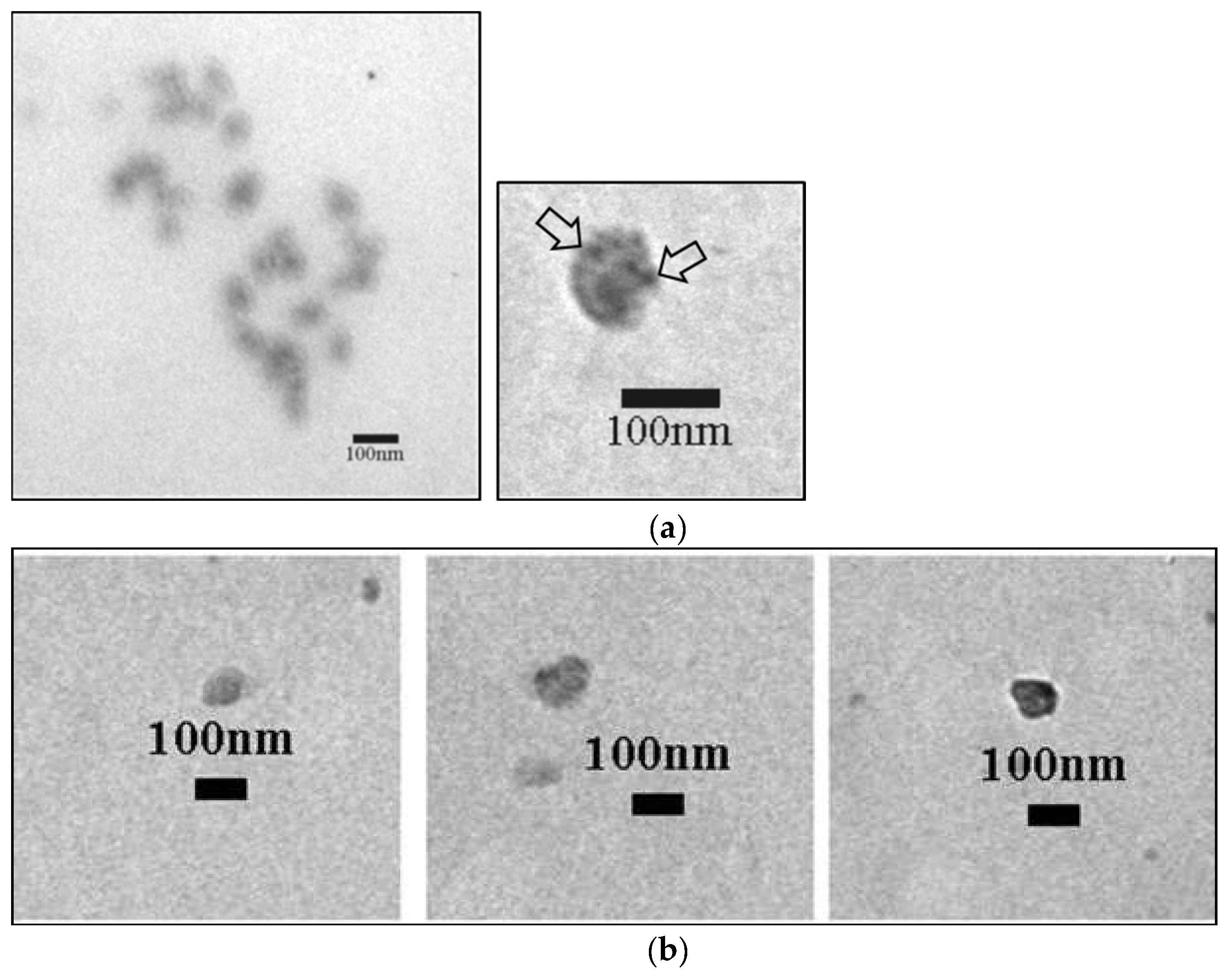
4.4. Transmission Electron Microscopy
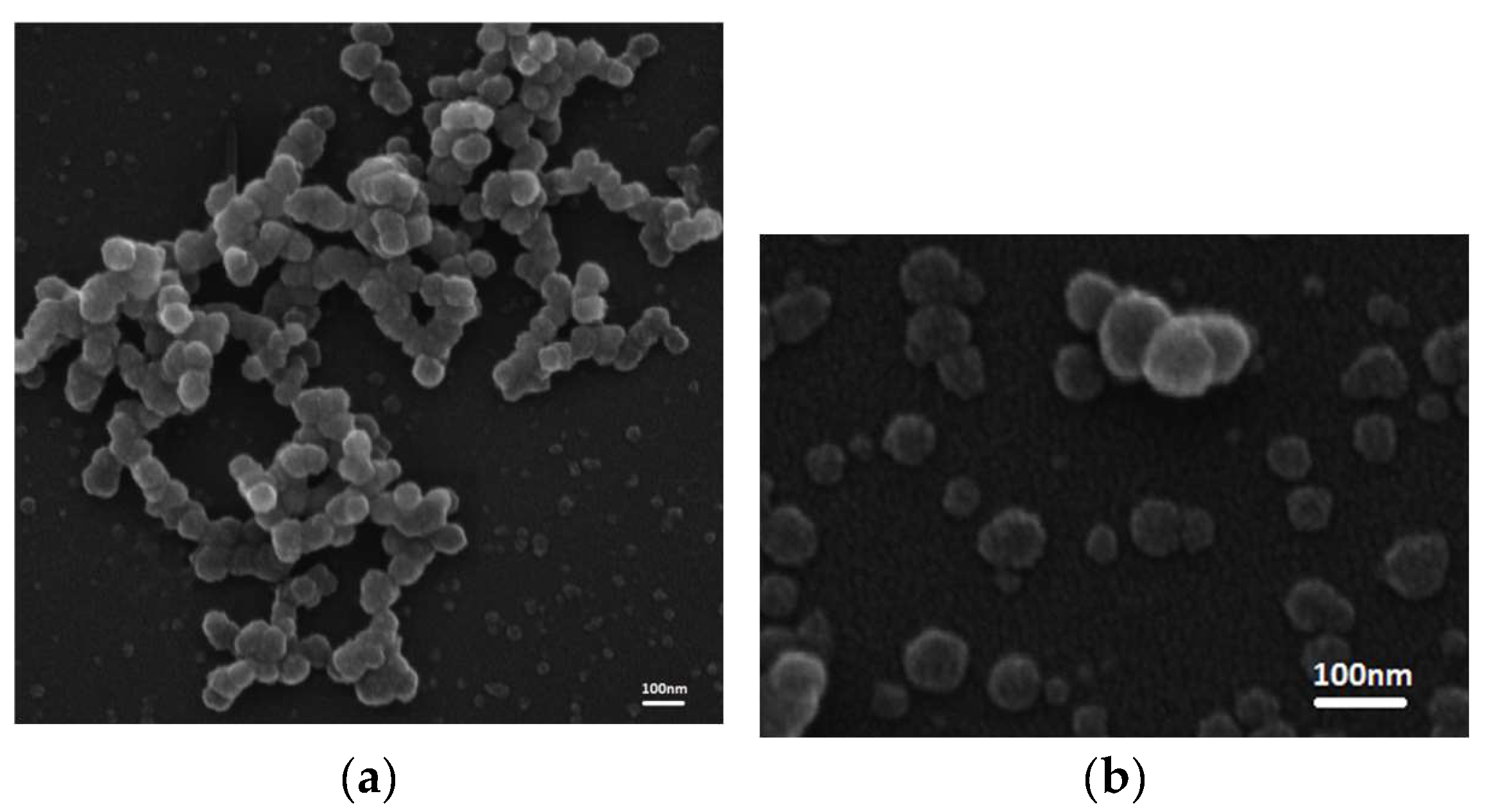
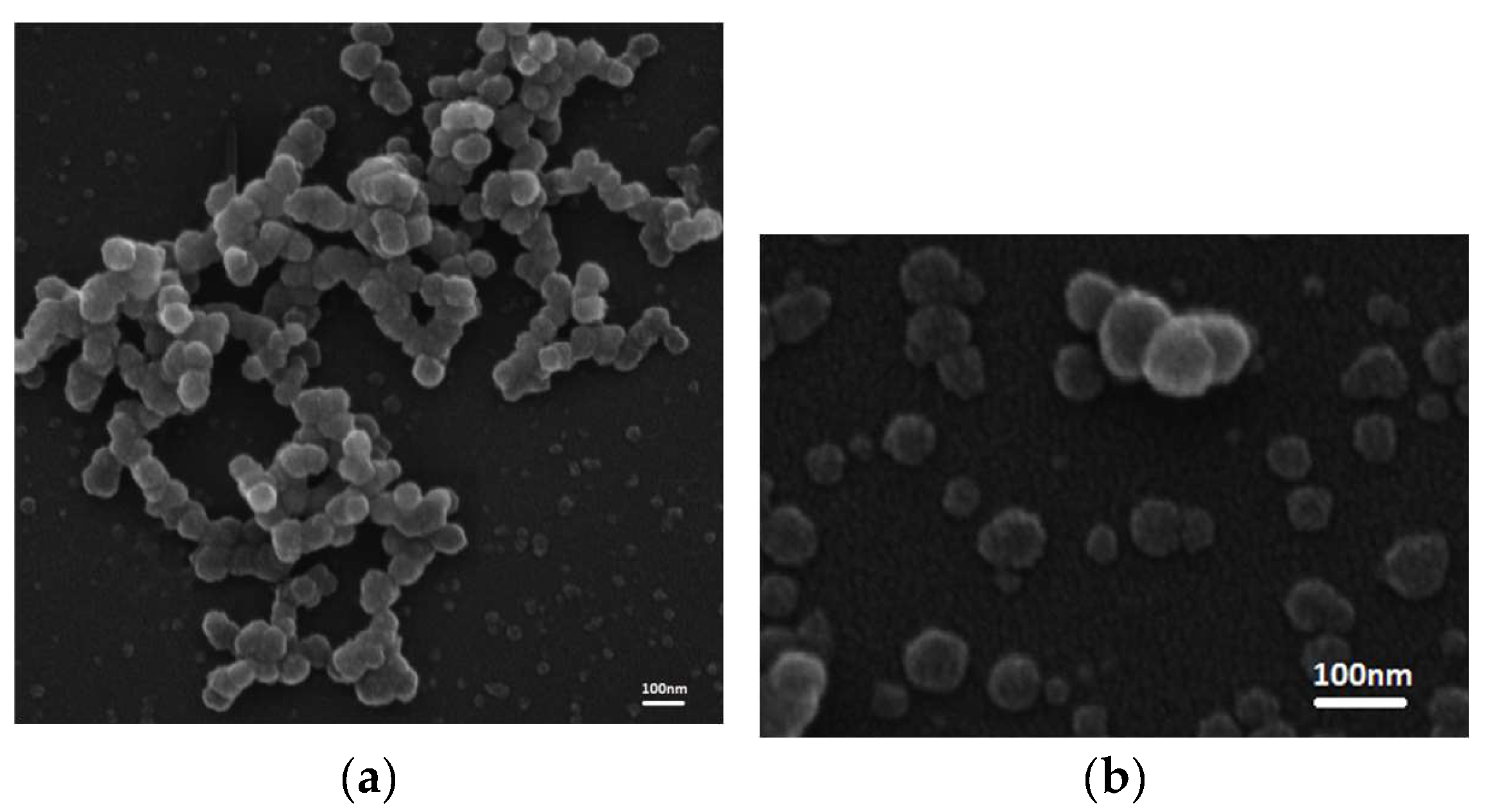
4.5. Scanning Electron Microscopy
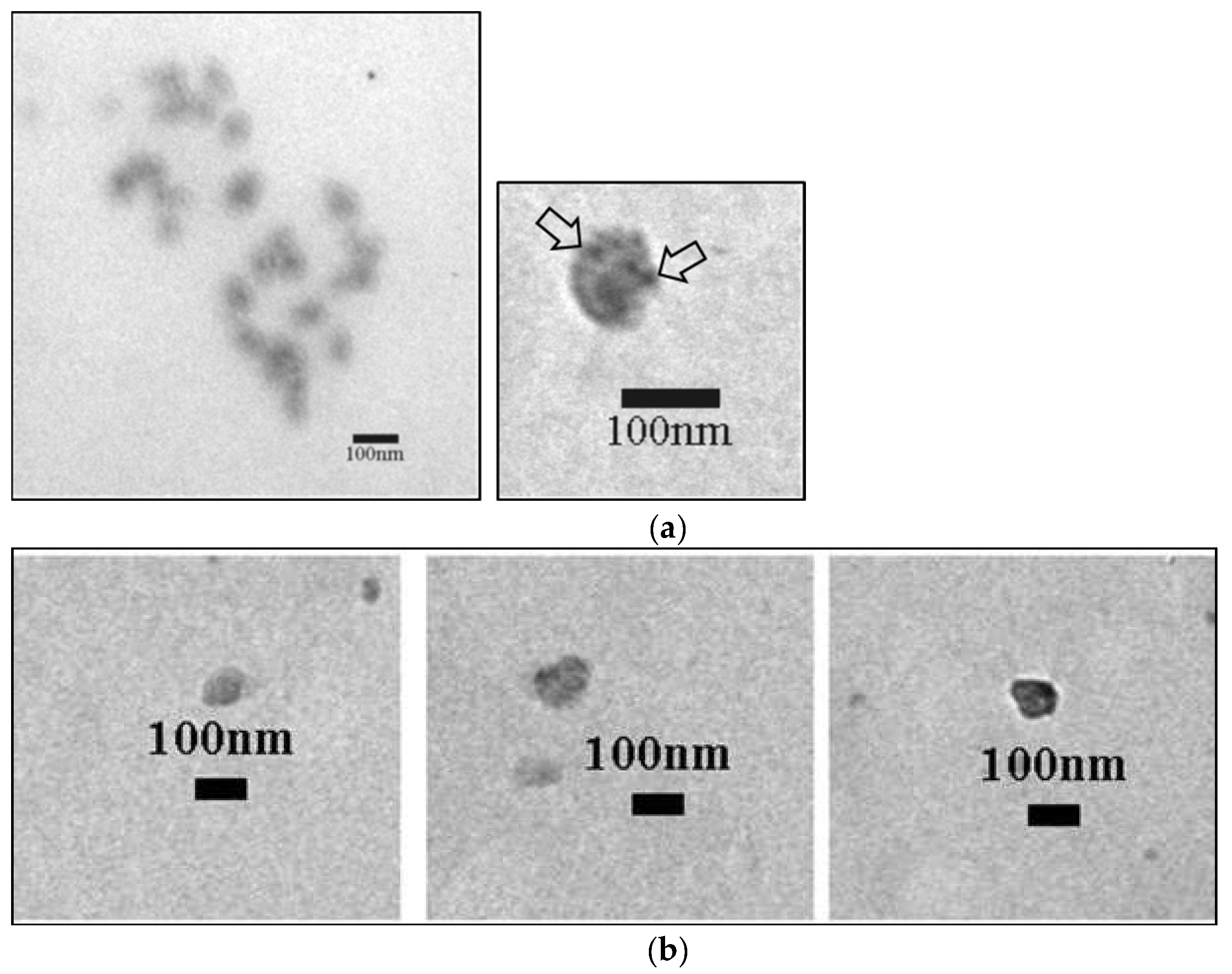
4.6. Immunogold Detection of PSMA
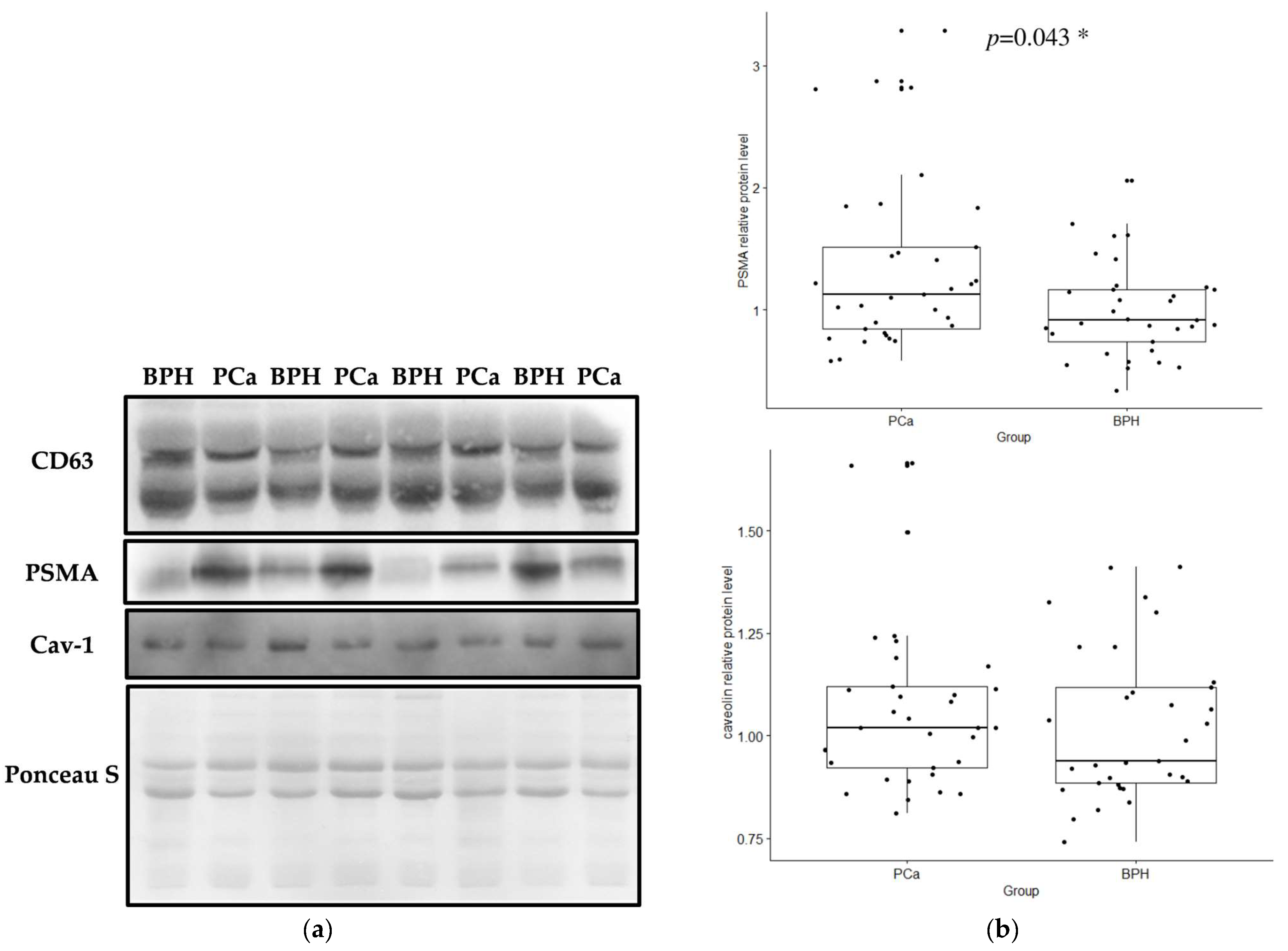
4.7. Western Blot Analysis
4.8. Flow Cytometry
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [PubMed]
- Institute of Public Health of Serbia. “Dr Milan Jovanović Batut” Cancer Incidence and Mortality in Central Serbia; Cancer Registry of Central Serbia: Belgrade, Serbia, 2021. [Google Scholar]
- Williams, I.S.; McVey, A.; Perera, S.; O’Brien, J.S.; Kostos, L.; Chen, K.; Siva, S.; Azad, A.A.; Murphy, D.G.; Kasivisvanathan, V.; et al. Modern paradigms for prostate cancer detection and management. Med. J. Aust. 2022, 217, 424–433. [Google Scholar]
- Kok, V.C.; Yu, C.C. Cancer-Derived Exosomes: Their Role in Cancer Biology and Biomarker Development. Int. J. Nanomed. 2020, 15, 8019–8036. [Google Scholar]
- Lucido, C.T.; Wynja, E.; Madeo, M.; Williamson, C.S.; Schwartz, L.E.; Imblum, B.A.; Drapkin, R.; Vermeer, P.D. Innervation of cervical carcinoma is mediated by cancer-derived exosomes. Gynecol. Oncol. 2019, 154, 228–235. [Google Scholar] [PubMed]
- Wei, H.; Chen, Q.; Lin, L.; Sha, C.; Li, T.; Liu, Y.; Yin, X.; Xu, Y.; Chen, L.; Gao, W.; et al. Regulation of exosome production and cargo sorting. Int. J. Biol. Sci. 2021, 17, 163–177. [Google Scholar] [PubMed]
- Valencia, K.; Montuenga, L.M. Exosomes in Liquid Biopsy: The Nanometric World in the Pursuit of Precision Oncology. Cancers 2021, 13, 2147. [Google Scholar] [PubMed]
- Chang, S.S. Overview of prostate-specific membrane antigen. Rev. Urol. 2004, 6 (Suppl. S10), S13–S18. [Google Scholar] [PubMed]
- Bravaccini, S.; Puccetti, M.; Bocchini, M.; Ravaioli, S.; Celli, M.; Scarpi, E.; De Giorgi, U.; Tumedei, M.M.; Raulli, G.; Cardinale, L.; et al. PSMA expression: A potential ally for the pathologist in prostate cancer diagnosis. Sci. Rep. 2018, 8, 4254. [Google Scholar]
- Ramnaraign, B.; Sartor, O. PSMA-Targeted Radiopharmaceuticals in Prostate Cancer: Current Data and New Trials. Oncologist 2023, 28, 392–401. [Google Scholar]
- Chen, P.; Zhang, Y.L.; Xue, B.; Xu, G.Y. Association of Caveolin-1 Expression with Prostate Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 10, 562774. [Google Scholar]
- Wang, C.B.; Chen, S.H.; Zhao, L.; Jin, X.; Chen, X.; Ji, J.; Mo, Z.N.; Wang, F.B. Urine-derived exosomal PSMA is a promising diagnostic biomarker for the detection of prostate cancer on initial biopsy. Clin. Transl. Oncol. 2023, 25, 758–767. [Google Scholar]
- Li, S.; Yi, M.; Dong, B.; Tan, X.; Luo, S.; Wu, K. The role of exosomes in liquid biopsy for cancer diagnosis and prognosis prediction. Int. J. Cancer 2021, 148, 2640–2651. [Google Scholar]
- Yu, D.; Li, Y.; Wang, M.; Gu, J.; Xu, W.; Cai, H.; Fang, X.; Zhang, X. Exosomes as a new frontier of cancer liquid biopsy. Mol. Cancer 2022, 21, 56. [Google Scholar]
- Joković, S.M.; Dobrijević, Z.; Kotarac, N.; Filipović, L.; Popović, M.; Korać, A.; Vuković, I.; Savić-Pavićević, D.; Brajušković, G. MiR-375 and miR-21 as Potential Biomarkers of Prostate Cancer: Comparison of Matching Samples of Plasma and Exosomes. Genes 2022, 13, 2320. [Google Scholar] [CrossRef]
- Mizutani, K.; Terazawa, R.; Kameyama, K.; Kato, T.; Horie, K.; Tsuchiya, T.; Seike, K.; Ehara, H.; Fujita, Y.; Kawakami, K.; et al. Isolation of prostate cancer-related exosomes. Anticancer Res. 2014, 34, 3419–3423. [Google Scholar] [PubMed]
- Allelein, S.; Aerchlimann, K.; Rösch, G.; Khajehamiri, R.; Kölsch, A.; Freese, C.; Kuhlmeier, D. Prostate-Specific Membrane Antigen (PSMA)-Positive Extracellular Vesicles in Urine-A Potential Liquid Biopsy Strategy for Prostate Cancer Diagnosis? Cancers 2022, 14, 2987. [Google Scholar]
- Paschalis, A.; Sheehan, B.; Riisnaes, R.; Rodrigues, D.N.; Gurel, B.; Bertan, C.; Ferreira, A.; Lambros, M.B.K.; Seed, G.; Yuan, W.; et al. Prostate-specific Membrane Antigen Heterogeneity and DNA Repair Defects in Prostate Cancer. Eur. Urol. 2019, 76, 469–478. [Google Scholar]
- Liu, T.; Mendes, D.E.; Berkman, C.E. Functional prostate-specific membrane antigen is enriched in exosomes from prostate cancer cells. Int. J. Oncol. 2014, 44, 918–922. [Google Scholar]
- Ariotti, N.; Wu, Y.; Okano, S.; Gambin, Y.; Follett, J.; Rae, J.; Ferguson, C.; Teasdale, R.D.; Alexandrov, K.; Meunier, F.A.; et al. An inverted CAV1 (caveolin 1) topology defines novel autophagy-dependent exosome secretion from prostate cancer cells. Autophagy 2021, 17, 2200–2216. [Google Scholar] [PubMed]
- Park, Y.H.; Shin, H.W.; Jung, A.R.; Kwon, O.S.; Choi, Y.J.; Park, J.; Lee, J.Y. Prostate-specific extracellular vesicles as a novel biomarker in human prostate cancer. Sci. Rep. 2016, 6, 30386. [Google Scholar] [PubMed]
- Kawakami, K.; Fujita, Y.; Kato, T.; Horie, K.; Koie, T.; Umezawa, K.; Tsumoto, H.; Miura, Y.; Katagiri, Y.; Miyazaki, T.; et al. Diagnostic potential of serum extracellular vesicles expressing prostate-specific membrane antigen in urologic malignancies. Sci. Rep. 2021, 11, 15000. [Google Scholar]
- Bakht, M.K.; Derecichei, I.; Li, Y.; Ferraiuolo, R.M.; Dunning, M.; Oh, S.W.; Hussein, A.; Youn, H.; Stringer, K.F.; Jeong, C.W.; et al. Neuroendocrine differentiation of prostate cancer leads to PSMA suppression. Endocr. Relat. Cancer 2018, 26, 131–146. [Google Scholar]
- Bakht, M.K.; Yamada, Y.; Ku, S.Y.; Venkadakrishnan, V.B.; Korsen, J.A.; Kalidindi, T.M.; Mizuno, K.; Ahn, S.H.; Seo, J.H.; Garcia, M.M.; et al. Landscape of prostate-specific membrane antigen heterogeneity and regulation in AR-positive and AR-negative metastatic prostate cancer. Nat. Cancer 2023, 4, 699–715. [Google Scholar]
- Vykoukal, J.; Fahrmann, J.F.; Gregg, J.R.; Tang, Z.; Basourakos, S.; Irajizad, E.; Park, S.; Yang, G.; Creighton, C.J.; Fleury, A.; et al. Caveolin-1-mediated sphingolipid oncometabolism underlies a metabolic vulnerability of prostate cancer. Nat. Commun. 2020, 11, 4279. [Google Scholar] [PubMed]
- Wang, X.; Liu, Z.; Yang, Z. Expression and clinical significance of Caveolin-1 in prostate Cancer after transurethral surgery. BMC Urol. 2018, 18, 102. [Google Scholar]
- Ketteler, J.; Klein, D. Caveolin-1, cancer and therapy resistance. Int. J. Cancer 2018, 143, 2092–2104. [Google Scholar] [PubMed]
- Mathieu, R.; Klatte, T.; Lucca, I.; Mbeutcha, A.; Seitz, C.; Karakiewicz, P.I.; Fajkovic, H.; Sun, M.; Lotan, Y.; Scherr, D.S.; et al. Prognostic value of Caveolin-1 in patients treated with radical prostatectomy: A multicentric validation study. BJU Int. 2016, 118, 243–249. [Google Scholar] [PubMed]
- Heidenreich, A.; Bastian, P.J.; Bellmunt, J.; Bolla, M.; Joniau, S.; van der Kwast, T.; Mason, M.; Matveev, V.; Wiegel, T.; Zattoni, F.; et al. EAU guidelines on prostate cancer. part 1: Screening, diagnosis, and local treatment with curative intent-update 2013. Eur. Urol. 2014, 65, 124–137. [Google Scholar] [PubMed]
- Filipović, L.; Spasojević, M.; Prodanović, R.; Korać, A.; Matijaševic, S.; Brajušković, G.; de Marco, A.; Popović, M. Affinity-based isolation of extracellular vesicles by means of single-domain antibodies bound to macroporous methacrylate-based copolymer. New Biotechnol. 2022, 69, 36–48. [Google Scholar]
- Lowry, O.H.; Rosebrough, N.J.; Farr, A.L.; Randall, R.J. Protein measurement with the Folin phenol reagent. J. Biol. Chem. 1951, 193, 265–275. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups of Patients | Relative Protein Level ± SD | p Value |
|---|---|---|
| exosomal PSMA | ||
| PSA < 20 ng/mL/PSA > 20 ng/mL | 1.05 ± 0.69/1.35 ± 0.85 | 0.26 |
| T1 and T2 stage/T3 and T4 stage | 1.07 ± 0.74/1.24 ± 0.77 | 0.49 |
| GS < 7/GS ≥ 7 | 1.15 ± 0.85/1.10 ± 0.70 | 0.93 |
| low risk/high risk | 1.13 ± 0.83/1.29 ± 0.74 | 0.52 |
| exosomal caveolin-1 | ||
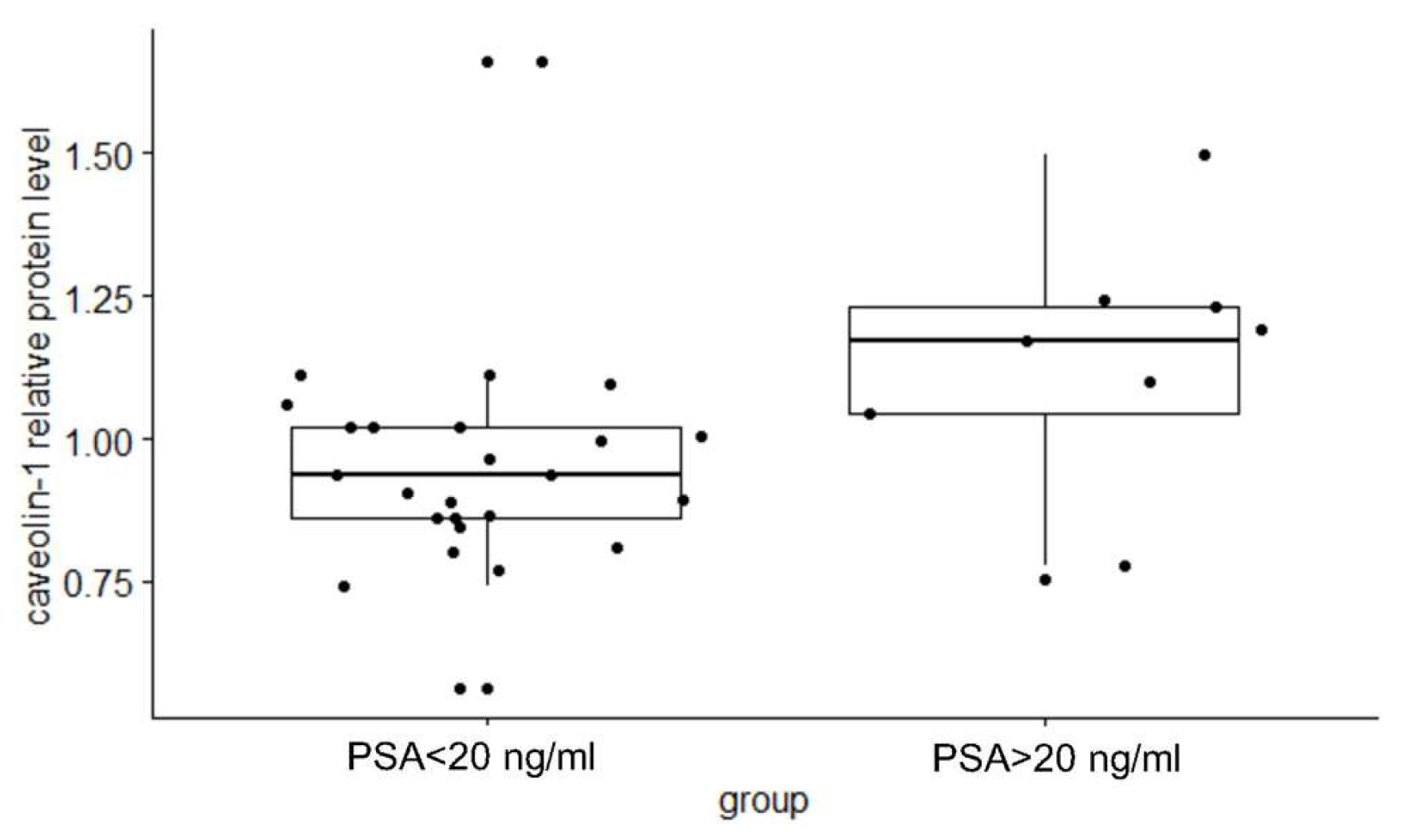
| PSA < 20 ng/mL/PSA > 20 ng/mL | 0.93 ± 0.20/1.08 ± 0.23 | 0.033 |
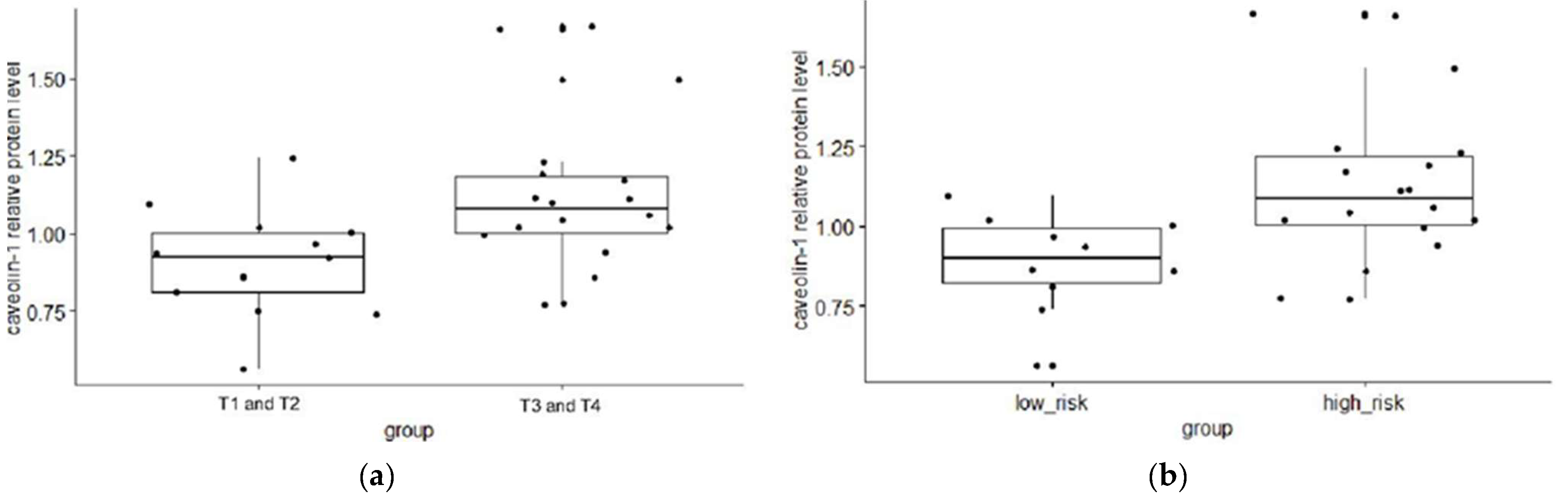
| T1 and T2 stage/T3 and T4 stage | 0.89 ± 0.17/1.09 ± 0.26 | 0.008 |
| GS < 7/GS ≥ 7 | 1.00 ± 0.32/0.98 ± 0.21 | 0.51 |
| low risk/high risk | 0.87 ± 0.15/1.10 ± 0.26 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matijašević Joković, S.; Korać, A.; Kovačević, S.; Djordjević, A.; Filipović, L.; Dobrijević, Z.; Brkušanin, M.; Savić-Pavićević, D.; Vuković, I.; Popović, M.; et al. Exosomal Prostate-Specific Membrane Antigen (PSMA) and Caveolin-1 as Potential Biomarkers of Prostate Cancer—Evidence from Serbian Population. Int. J. Mol. Sci. 2024, 25, 3533. https://doi.org/10.3390/ijms25063533
Matijašević Joković S, Korać A, Kovačević S, Djordjević A, Filipović L, Dobrijević Z, Brkušanin M, Savić-Pavićević D, Vuković I, Popović M, et al. Exosomal Prostate-Specific Membrane Antigen (PSMA) and Caveolin-1 as Potential Biomarkers of Prostate Cancer—Evidence from Serbian Population. International Journal of Molecular Sciences. 2024; 25(6):3533. https://doi.org/10.3390/ijms25063533
Chicago/Turabian StyleMatijašević Joković, Suzana, Aleksandra Korać, Sanja Kovačević, Ana Djordjević, Lidija Filipović, Zorana Dobrijević, Miloš Brkušanin, Dušanka Savić-Pavićević, Ivan Vuković, Milica Popović, and et al. 2024. "Exosomal Prostate-Specific Membrane Antigen (PSMA) and Caveolin-1 as Potential Biomarkers of Prostate Cancer—Evidence from Serbian Population" International Journal of Molecular Sciences 25, no. 6: 3533. https://doi.org/10.3390/ijms25063533
APA StyleMatijašević Joković, S., Korać, A., Kovačević, S., Djordjević, A., Filipović, L., Dobrijević, Z., Brkušanin, M., Savić-Pavićević, D., Vuković, I., Popović, M., & Brajušković, G. (2024). Exosomal Prostate-Specific Membrane Antigen (PSMA) and Caveolin-1 as Potential Biomarkers of Prostate Cancer—Evidence from Serbian Population. International Journal of Molecular Sciences, 25(6), 3533. https://doi.org/10.3390/ijms25063533