
Changes in Inflammatory Cytokines in Responders and Non-Responders to TNFα Inhibitor and IL-17A Inhibitor: A Study Examining Psoriatic Arthritis Patients

 , and
, and
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Change in Clinical Outcome Measures in Responders and Non-Responders to Treatment
2.3. Change in Biomarker Level from Baseline to Follow-Up
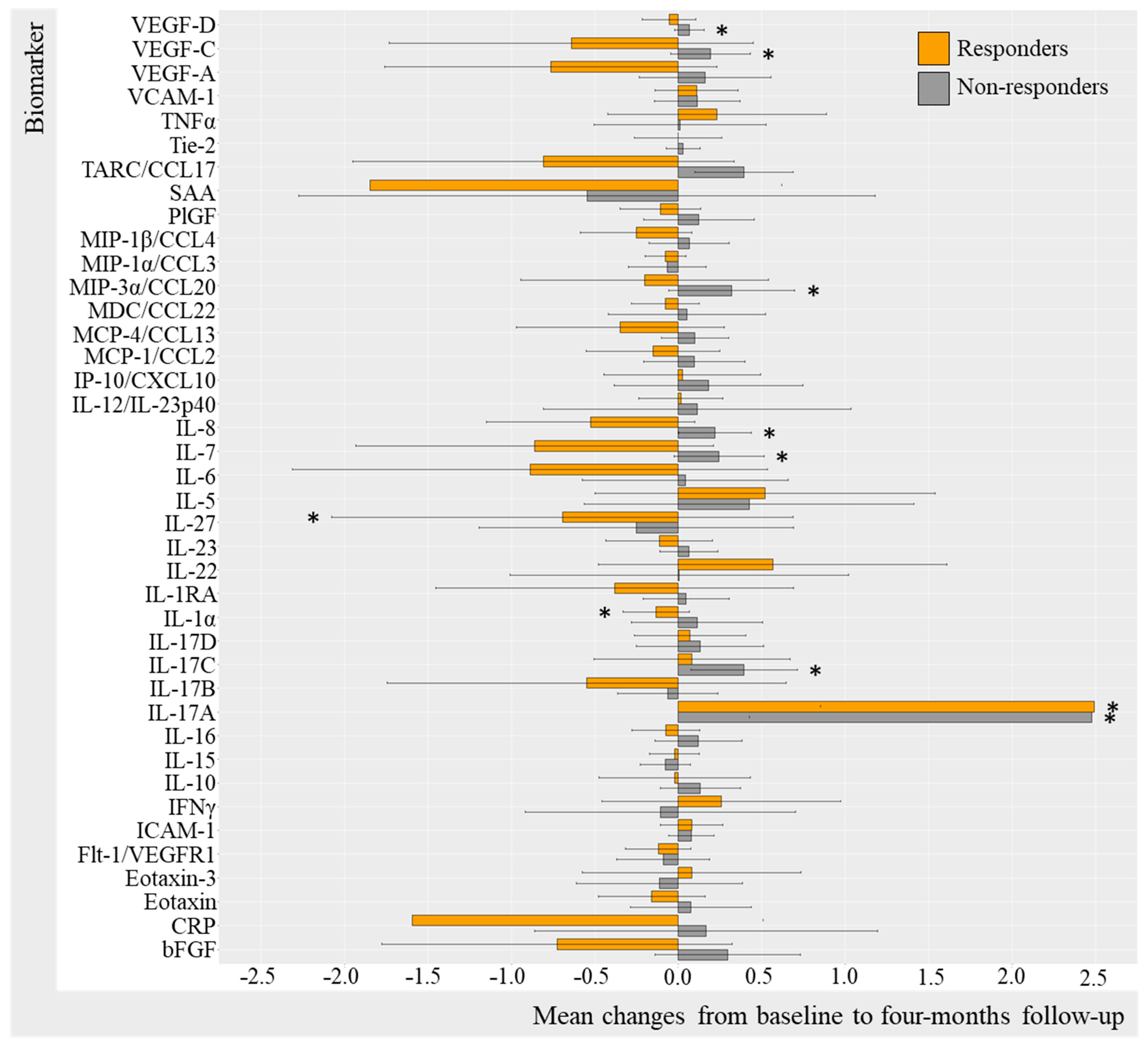
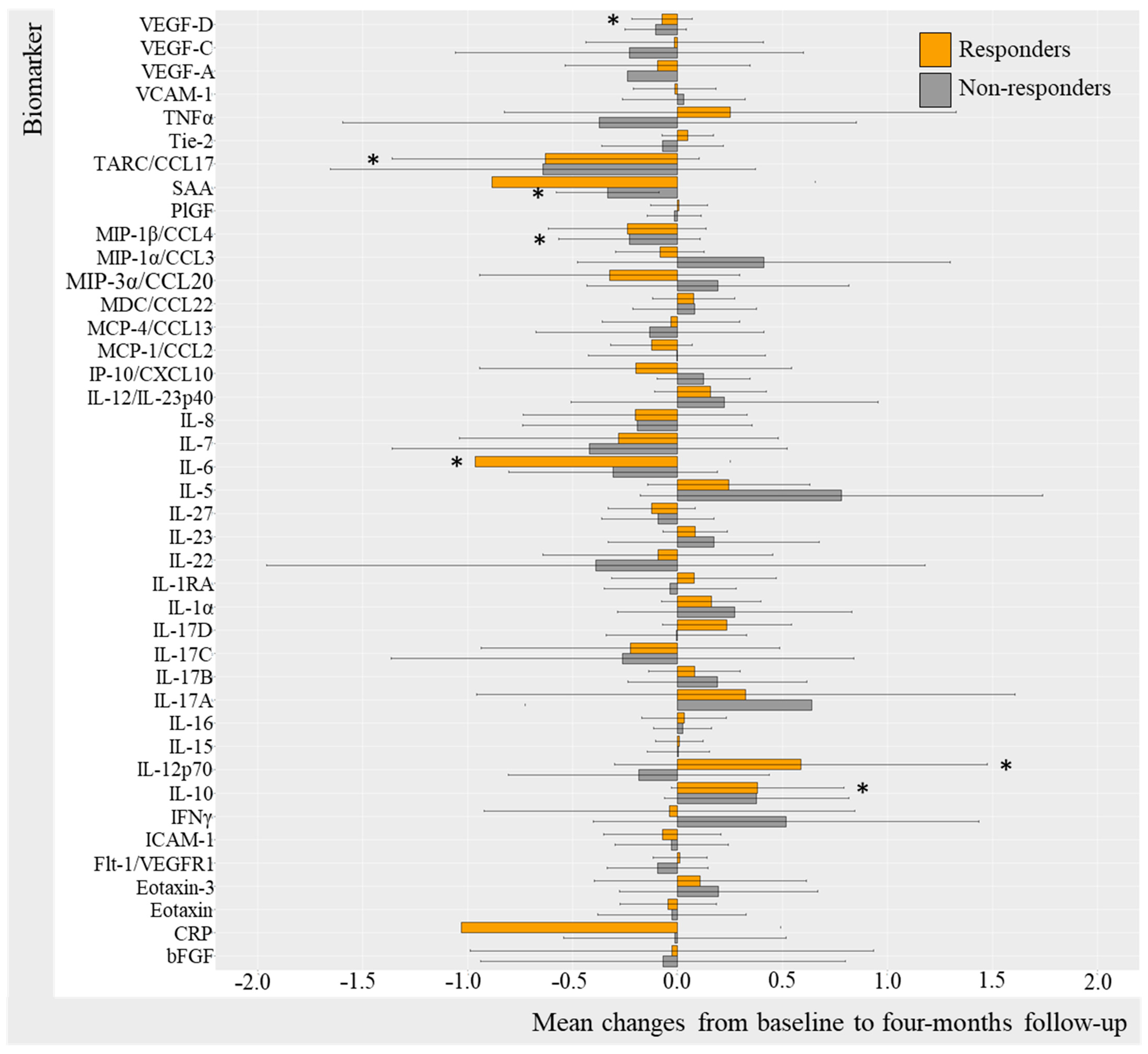
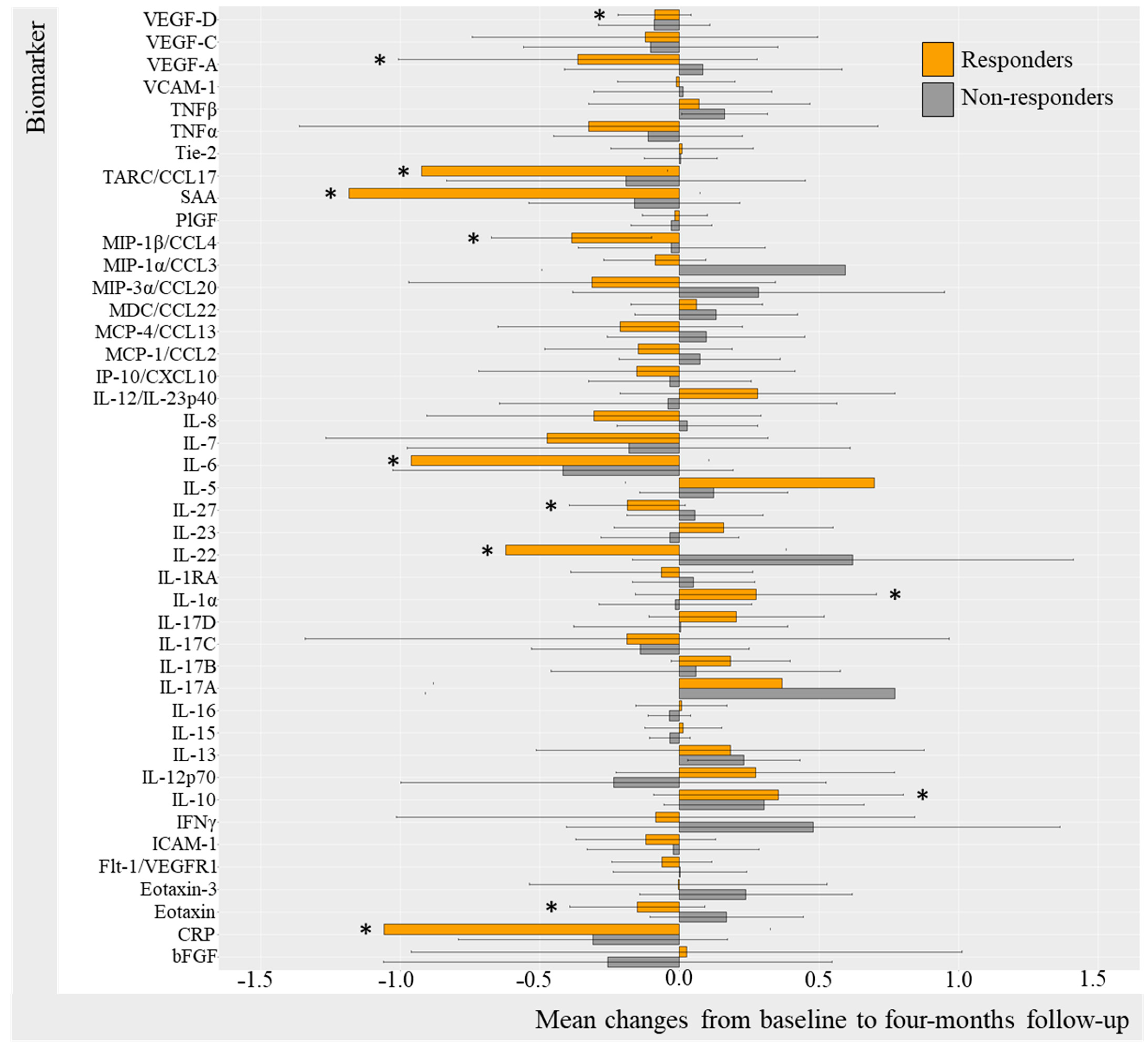
2.3.1. Change in Biomarkers in TNFi Responders and Non-Responders (DAPSA50 and PASI50)
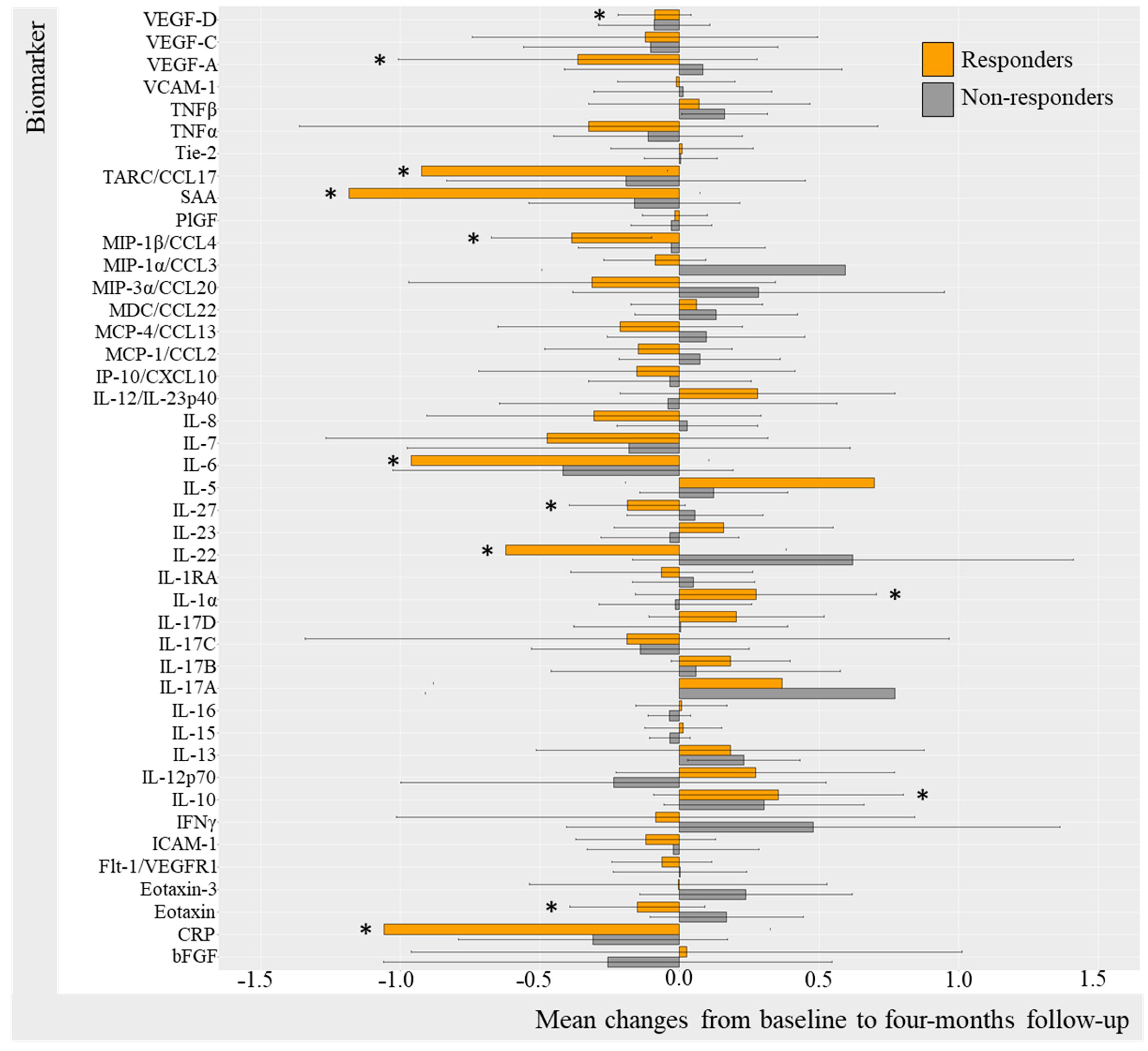
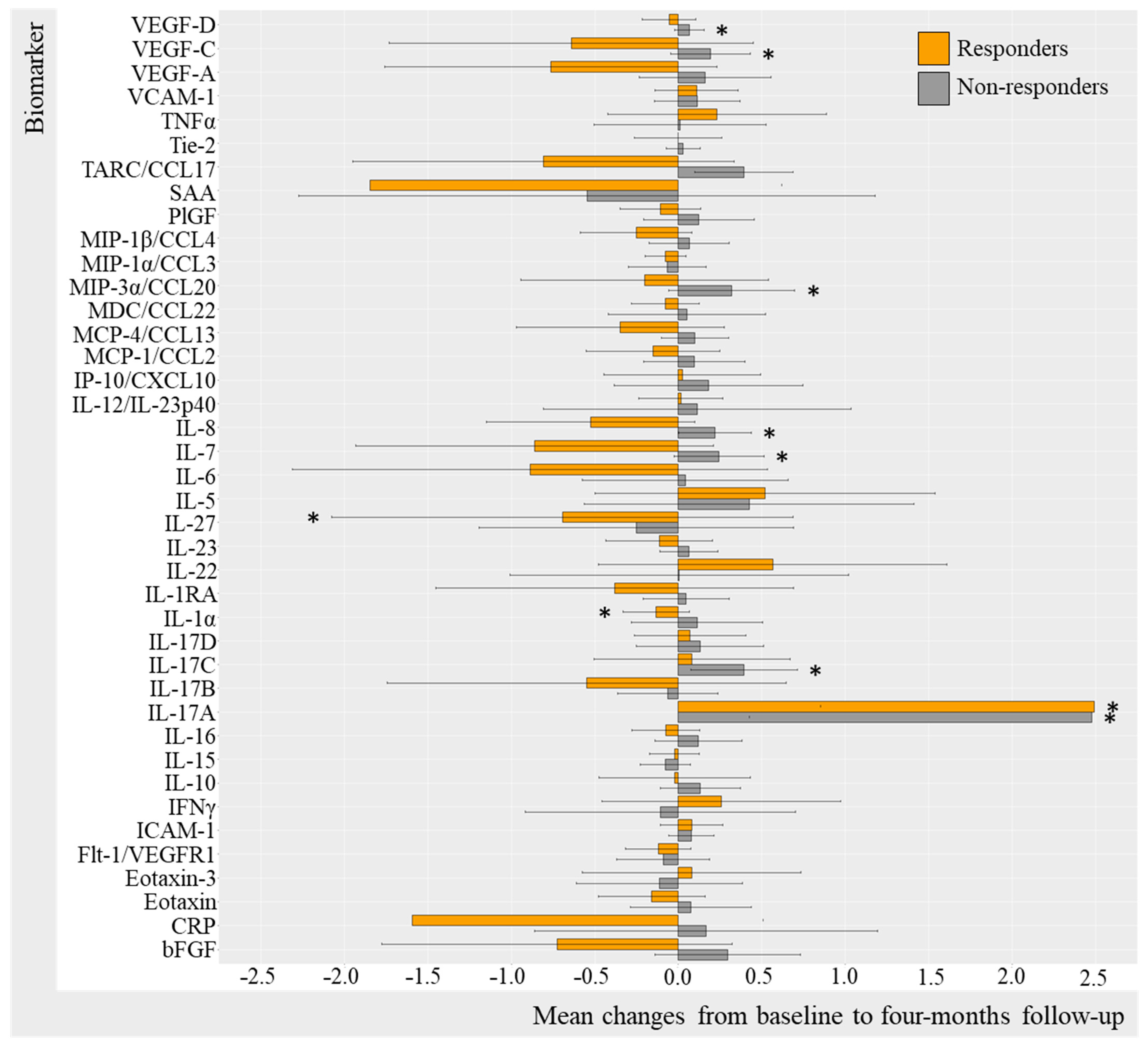
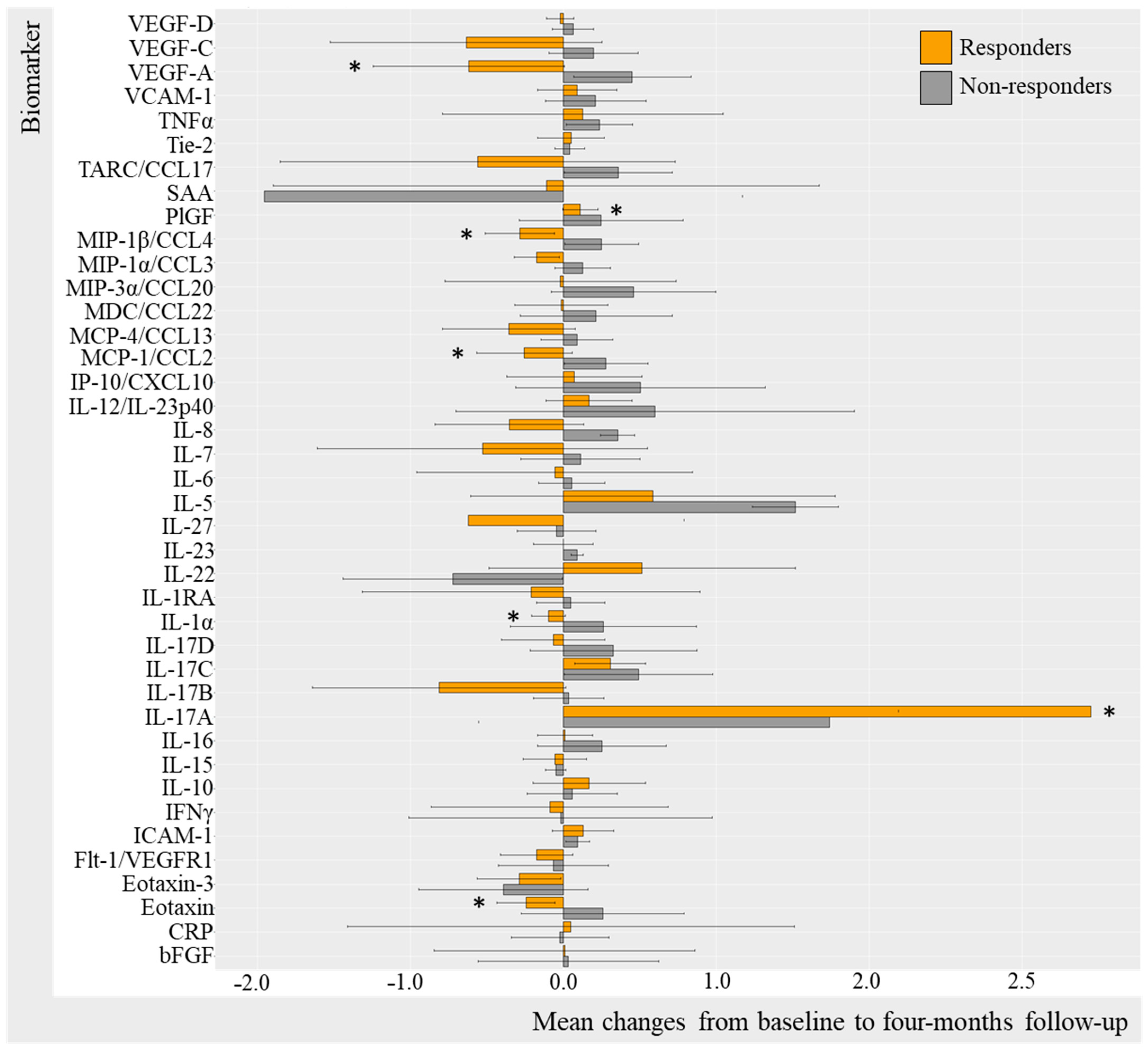
2.3.2. Change in Biomarkers in IL-17Ai Responders and Non-Responders (DAPSA50 and PASI50)
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Study Visits
4.3. Quantifying Biomarker Levels
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Husted, J.A.; Gladman, D.D.; Farewell, V.T.; Cook, R.J. Health-related quality of life of patients with psoriatic arthritis: A comparison with patients with rheumatoid arthritis. Arthritis Care Res. 2001, 45, 151–158. [Google Scholar] [CrossRef]
- Scott, D.L. Biologics-based therapy for the treatment of rheumatoid arthritis. Clin. Pharmacol. Ther. 2012, 91, 30–43. [Google Scholar] [CrossRef]
- Skougaard, M.; Jørgensen, T.S.; Jensen, M.J.; Ballegaard, C.; Guldberg-Møller, J.; Egeberg, A.; Christensen, R.; Benzin, P.; Stisen, Z.R.; Merola, J.F.; et al. Change in psoriatic arthritis outcome measures impacts SF-36 physical and mental component score differently: An observational cohort study. Rheumatol. Adv. Pract. 2021, 5, rkab076. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, L.E.; Lie, E.; Jacobsson, L.T.; Christensen, R.; Mease, P.J.; Bliddal, H.; Geborek, P. Effectiveness and feasibility associated with switching to a second or third TNF inhibitor in patients with psoriatic arthritis: A cohort study from southern Sweden. J. Rheumatol. 2016, 43, 81–87. [Google Scholar] [CrossRef]
- McGonagle, D.; McDermott, M.F. A proposed classification of the immunological diseases. PLoS Med. 2006, 3, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.J.; Fearon, U. The pathogenesis of psoriatic arthritis. Lancet 2018, 391, 2273–2284. [Google Scholar] [CrossRef] [PubMed]
- Lubberts, E. The IL-23-IL-17 axis in inflammatory arthritis. Nat. Rev. Rheumatol. 2015, 11, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Tinazzi, I.; McGonagle, D.; Aydin, S.Z.; Chessa, D.; Marchetta, A.; Macchioni, P. ‘Deep Koebner’ phenomenon of the flexor tendon-associated accessory pulleys as a novel factor in tenosynovitis and dactylitis in psoriatic arthritis. Ann. Rheum. Dis. 2018, 77, 922–925. [Google Scholar] [CrossRef]
- McGonagle, D. Enthesitis: An autoinflammatory lesion linking nail and joint involvement in psoriatic disease. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 9–13. [Google Scholar] [CrossRef]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef]
- Grim, J.; Chládek, J.; Martínková, J. Pharmacokinetics and pharmacodynamics of methotrexate in non-neoplastic diseases. Clin. Pharmacokinet. 2003, 42, 139–151. [Google Scholar] [CrossRef]
- Chao, R.; Kavanaugh, A. Psoriatic Arthritis: Newer and Older Therapies. Curr. Rheumatol. Rep. 2019, 21, 75. [Google Scholar] [CrossRef]
- Bravo, A.; Kavanaugh, A. Bedside to bench: Defining the immunopathogenesis of psoriatic arthritis. Nat. Rev. Rheumatol. 2019, 15, 645–656. [Google Scholar] [CrossRef]
- Skougaard, M.; Ditlev, S.B.; Søndergaard, M.F.; Kristensen, L.E. Cytokine Signatures in Psoriatic Arthritis Patients Indicate Different Phenotypic Traits Comparing Responders and Non-Responders of IL-17A and TNFα Inhibitors. Int. J. Mol. Sci. 2023, 24, 6343. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 104: Correlational Analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Walters, H.M.; Pan, N.; Lehman, T.J.A.; Adams, A.; Kalliolias, G.D.; Zhu, Y.; Santiago, F.; Nguyen, J.; Sitaras, L.; Cunningham-Rundles, S.; et al. The impact of disease activity and tumour necrosis factor-α inhibitor therapy on cytokine levels in juvenile idiopathic arthritis. Clin. Exp. Immunol. 2016, 184, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Rudwaleit, M.; Brandt, J.; Thiel, A.; Braun, J.; Sieper, J. Up regulation of the production of tumour necrosis factor α and interferon γ by T cells in ankylosing spondylitis during treatment with etanercept. Ann. Rheum. Dis. 2003, 62, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Hueber, A.J.; McInnes, I.B. Immune regulation in psoriasis and psoriatic arthritis-Recent developments. Immunol. Lett. 2007, 114, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Herrera, L.A.; De la Cruz-Mosso, U.; Román-Fernández, I.V.; Parra-Rojas, I.; Soñanez-Organis, J.; Hernández-Bello, J.; Morales-Zambrano, R.; Villanueva-Quintero, G.; Muñoz-Valle, J. A potential inflammatory role of IL-31 in psoriatic arthritis: A correlation with Th17 cytokine profile. Int. J. Immunopathol. Pharmacol. 2020, 34, 2058738420907186. [Google Scholar] [CrossRef]
- Fromm, S.; Cunningham, C.C.; Dunne, M.R.; Veale, D.J.; Fearon, U.; Wade, S.M. Enhanced angiogenic function in response to fibroblasts from psoriatic arthritis synovium compared to rheumatoid arthritis. Arthritis Res. Ther. 2019, 21, 297. [Google Scholar] [CrossRef] [PubMed]
- Skougaard, M.; Jørgensen, T.S.; Rifbjerg-Madsen, S.; Coates, L.C.; Egeberg, A.; Amris, K.; Dreyer, L.; Højgaard, P.; Guldberg-Møller, J.; Merola, J.F.; et al. Relationship between Fatigue and Inflammation, Disease Duration, and Chronic Pain in Psoriatic Arthritis: An Observational DANBIO Registry Study. J. Rheumatol. 2020, 47, 548–552. [Google Scholar] [CrossRef] [PubMed]
- McInnes, I.B.; Mease, P.J.; Kirkham, B.; Kavanaugh, A.; Ritchlin, C.T.; Rahman, P.; van der Heijde, D.; Landewé, R.; Conaghan, P.G.; Gottlieb, A.B.; et al. Secukinumab, a human anti-interleukin-17A monoclonal antibody, in patients with psoriatic arthritis (FUTURE 2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2015, 386, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.J.; Van Der Heijde, D.; Ritchlin, C.T.; Okada, M.; Cuchacovich, R.S.; Shuler, C.L.; Lin, C.-Y.; Braun, D.K.; Lee, C.H.; Gladman, D.D. Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: Results from the 24-week randomised, double-blind, placebocontrolled and active (adalimumab)-controlled period of th. Ann. Rheum. Dis. 2017, 76, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Furue, K.; Ito, T.; Furue, M. Differential efficacy of biologic treatments targeting the TNF-α/IL-23/IL-17 axis in psoriasis and psoriatic arthritis. Cytokine 2018, 111, 182–188. [Google Scholar] [CrossRef]
- Schulz, M.; Dotzlaw, H.; Neeck, G. Ankylosing spondylitis and rheumatoid arthritis: Serum levels of TNF- α and its soluble receptors during the course of therapy with etanercept and infliximab. Biomed. Res. Int. 2014, 2014, 675108. [Google Scholar] [CrossRef]
- Gane, J.M.; Stockley, R.A.; Sapey, E. TNF- α Autocrine Feedback Loops in Human Monocytes: The Pro- and Anti-Inflammatory Roles of the TNF- α Receptors Support the Concept of Selective TNFR1 Blockade in vivo. J. Immunol. Res. 2016, 2016, 1079851. [Google Scholar] [CrossRef]
- Miossec, P. Local and systemic effects of IL-17 in joint inflammation: A historical perspective from discovery to targeting. Cell. Mol. 2021, 18, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Mc Ardle, A.; Flatley, B.; Pennington, S.R.; FitzGerald, O. Early biomarkers of joint damage in rheumatoid and psoriatic arthritis. Arthritis Res. Ther. 2015, 17, 141. [Google Scholar] [CrossRef]
- Meka, R.R.; Venkatesha, S.H.; Dudics, S.; Acharya, B.; Moudgil, K.D. IL-27-induced modulation of autoimmunity and its therapeutic potential. Autoimmun. Rev. 2015, 14, 1131–1141. [Google Scholar] [CrossRef]
- van Roon, J.A.G.; Glaudemans, K.A.F.M.; Bijilsma, J.W.J.; Lafeber FP, J.G. Interleukin 7 stimulates tumour necrosis factor α and Th 1 cytokine production in joints of patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 113–119. [Google Scholar] [CrossRef]
- Ogata, A.; Kumanogoh, A.; Tanaka, T. Pathological Role of Interleukin-6 in Psoriatic Arthritis. Arthritis 2012, 2012, 1713618. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, B.W.; Kavanaugh, A.; Reich, K. Interleukin-17A: A unique pathway in immune-mediated diseases: Psoriasis, psoriatic arthritis and rheumatoid arthritis. Immunology 2014, 141, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Schoels, M.M.; Aletaha, D.; Alasti, F.; Smolen, J.S. Disease activity in psoriatic arthritis (PsA): Defining remission and treatment success using the DAPSA score. Ann. Rheum. Dis. 2016, 75, 811–818. [Google Scholar] [CrossRef]
- Højgaard, P.; Christensen, R.; Dreyer, L.; Mease, P.; de Wit, M.; Skov, L.; Glintborg, B.; Christensen, A.W.; Ballegaard, C.; Bliddal, H.; et al. Pain mechanisms and ultrasonic inflammatory activity as prognostic factors in patients with psoriatic arthritis: Protocol for a prospective, exploratory cohort study. BMJ Open 2016, 6, e010650. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 68) | TNFi Initiators (n = 29) | IL17Ai Initiators (n = 19) | MTX Initiators (n = 20) | p Value | |
|---|---|---|---|---|---|
| Female, n (%) | 38 (55.88) | 16 (55.17) | 12 (63.16) | 10 (20.00) | 0.707 |
| Age, years | 51.50 (45.27–60.88) | 49.60 (56.20–59.30) | 49.80 (45.05–61.10) | 56.80 (51.35–62.38) | 0.173 |
| Disease duration, years | 4.00 (1.58–10.00) | 4.00 (1.75–8.42) | 6.00 (1.63–14.5) | 4.73 (1.44–10.75) | 0.794 |
| bDMARD monotherapy, n (%) | 27 (56.25) § | 17 (58.62) | 10 (52.63) | - | 0.911 |
| Methotrexate, n (%) | 15 (31.25) § | 10 (34.48) § | 5 (26.32) § | - | 0.319 |
| Leflunomide, n (%) | 4 (8.33) § | 1 (3.45) § | 3 (15.79) § | - | |
| Salazopyrin, n (%) | 2 (4.17) § | 1 (3.34) § | 1 (5.26) § | - | |
| Previous bDMARD, n (%) | |||||
| - 0 | 39 (57.35) | 19 (65.52) | 2 (10.53) | 18 (0.90) | <0.001 |
| - 1 | 14 (20.59) | 7 (24.14) | 5 (26.32) | 2 (0.10) | |
| - 2 | 8 (11.77) | 2 (5.90) | 6 (31.58) | 0 (0.00) | |
| - ≥3 | 7 (10.29) | 1 (3.45) | 6 (31.58) | 0 (0.00) | |
| DAPSA | 29.20 (21.90–38.85) † | 28.80 (22.00–39.80) | 33.25 (25.80–46.65) † | 27.55 (20.50–36.83) | 0.277 |
| DAS28CRP | 4.12 (3.70–4.90) † | 4.12 (3.58–4.85) | 4.36 (3.77–5.30) † | 4.06 (3.61–4.57) | 0.274 |
| PASI (0–72) | 1.20 (0.00–3.08) | 1.50 (0.30–3.40) | 0.40 (0.00–2.00) | 0.95 (0.00–2.93) | 0.453 |
| VAS fatigue (0–100 mm) | 67.00 (50.00–82.00) † | 60.00 (48.00–79.00) | 85.00 (75.00–91.50) | 62.00 (46.50–75.50) | 0.007 |
| VAS pain (0–100 mm) | 59.00 (31.00–78.00) † | 57.00 (27.00–77.00) | 75.00 (50.75–83.75) | 47.00 (31.50–64.25) | 0.176 |
| Baseline | Follow-Up | Mean Change | p-Value | |
|---|---|---|---|---|
| DAPSA50 Responders | ||||
| TNFi (n = 11) | ||||
| DAPSA | 35.80 ± 23.76 | 7.05 ± 9.48 | −28.75 (−81.81; 24.32) | <0.001 |
| PASI | 2.16 ± 2.72 | 0.56 ± 1.22 | −1.60 (−7.79; 4.59) | 0.024 |
| IL17Ai (n = 7) | ||||
| DAPSA | 33.93 ± 14.01 | 12.28 ± 7.18 | −21.65 (−55.95; 12.65) | 0.031 |
| PASI | 1.51 ± 1.88 | 0.21 ± 0.45 | −1.30 (−5.45; 2.85) | 0.106 |
| PASI50 Responders | ||||
| TNFi (n = 12) | ||||
| DAPSA | 36.58 ± 23.70 | 15.53 ± 17.80 | −21.04 (−82.21; 40.13) | <0.001 |
| PASI | 4.33 ± 5.55 | 0.25 ± 0.60 | −4.08 (−15.61; 7.45) | 0.003 |
| IL17Ai (n = 7) | ||||
| DAPSA | 38.40 ± 11.06 | 26.30 ± 17.06 | −12.1 (−56.41; 32.21) | 0.156 |
| PASI | 5.14 ± 8.37 | 0.17 ± 0.34 | −4.97 (−22.95; 13.00) | 0.016 |
| DAPSA50 Non-responders | ||||
| TNFi (n = 9) | ||||
| DAPSA | 34.73 ± 13.08 | 27.58 ± 15.59 | −7.16 (−49.90; 35.59) | 0.039 |
| PASI | 4.56 ± 6.22 | 5.09 ± 8.14 | 0.53 (−20.99; 22.05) | 1.000 |
| IL17Ai (n = 12) | ||||
| DAPSA | 38.53 ± 17.87 | 39.68 ± 22.31 | 1.15 (−57.84; 60.14) | 0.850 |
| PASI | 3.70 ± 7.32 | 1.95 ± 4.60 | −1.75 (19.59; 16.09) | 0.834 |
| PASI50 Non-responders | ||||
| TNFi (n = 6) | ||||
| DAPSA | 33.03 ± 10.28 | 20.65 ± 15.33 | −12.38 (−52.61; 27.84) | 0.094 |
| PASI | 2.13 ± 2.44 | 8.17 ± 8.68 | 6.03 (−13.61; 25.68) | 0.094 |
| IL17Ai (n = 4) | ||||
| DAPSA | 34.20 ± 14.26 | 34.15 ± 21.98 | −0.05 (−60.47; 60.37) | 1.000 |
| PASI | 4.75 ± 5.65 | 5.85 ± 6.86 | 1.10 (−19.38; 21.58) | 0.414 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skougaard, M.; Søndergaard, M.F.; Ditlev, S.B.; Kristensen, L.E. Changes in Inflammatory Cytokines in Responders and Non-Responders to TNFα Inhibitor and IL-17A Inhibitor: A Study Examining Psoriatic Arthritis Patients. Int. J. Mol. Sci. 2024, 25, 3002. https://doi.org/10.3390/ijms25053002
Skougaard M, Søndergaard MF, Ditlev SB, Kristensen LE. Changes in Inflammatory Cytokines in Responders and Non-Responders to TNFα Inhibitor and IL-17A Inhibitor: A Study Examining Psoriatic Arthritis Patients. International Journal of Molecular Sciences. 2024; 25(5):3002. https://doi.org/10.3390/ijms25053002
Chicago/Turabian StyleSkougaard, Marie, Magnus Friis Søndergaard, Sisse Bolm Ditlev, and Lars Erik Kristensen. 2024. "Changes in Inflammatory Cytokines in Responders and Non-Responders to TNFα Inhibitor and IL-17A Inhibitor: A Study Examining Psoriatic Arthritis Patients" International Journal of Molecular Sciences 25, no. 5: 3002. https://doi.org/10.3390/ijms25053002
APA StyleSkougaard, M., Søndergaard, M. F., Ditlev, S. B., & Kristensen, L. E. (2024). Changes in Inflammatory Cytokines in Responders and Non-Responders to TNFα Inhibitor and IL-17A Inhibitor: A Study Examining Psoriatic Arthritis Patients. International Journal of Molecular Sciences, 25(5), 3002. https://doi.org/10.3390/ijms25053002