
Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. VNS Induced a Significant and Sustained Clinical Response in TRD Patients
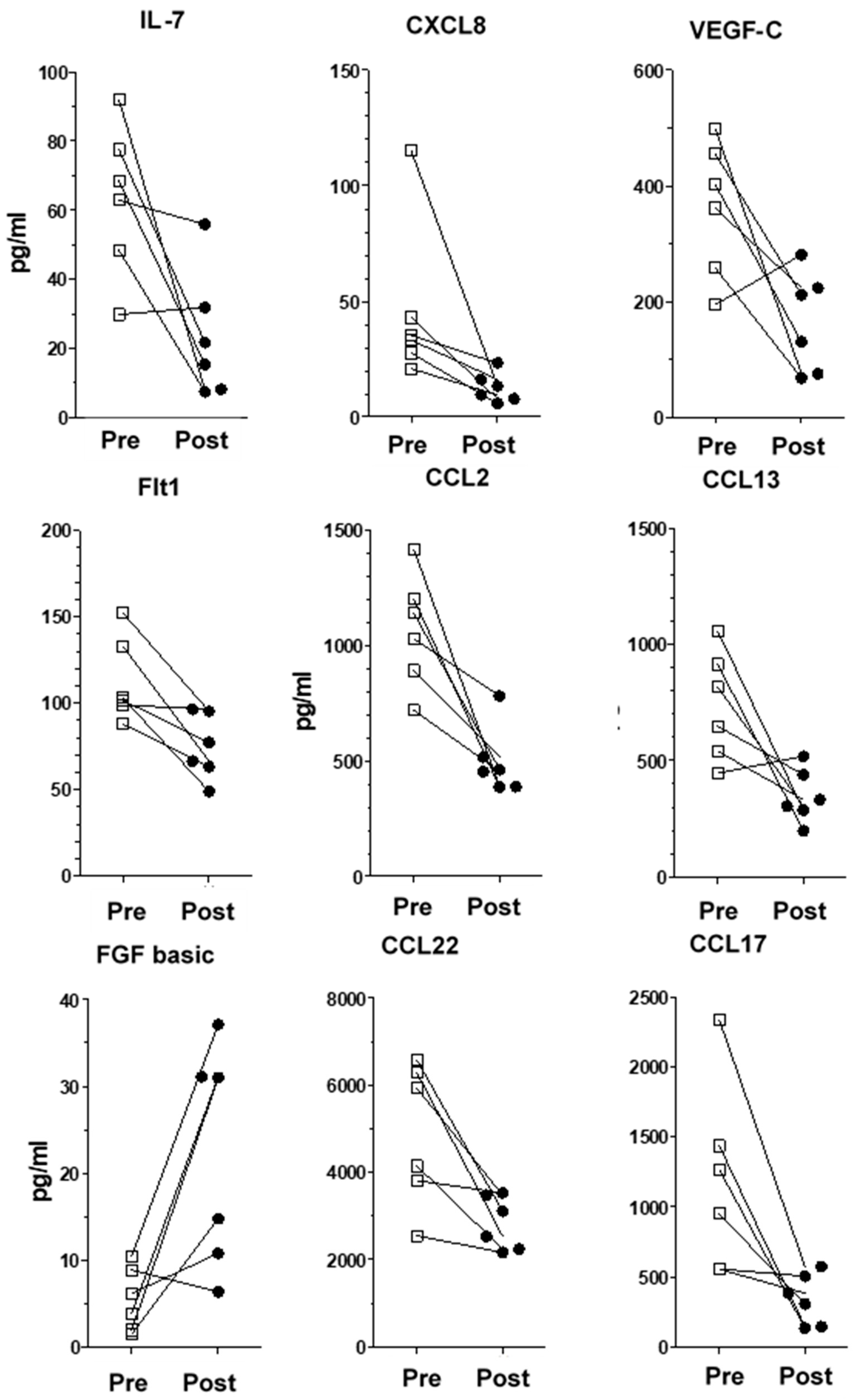
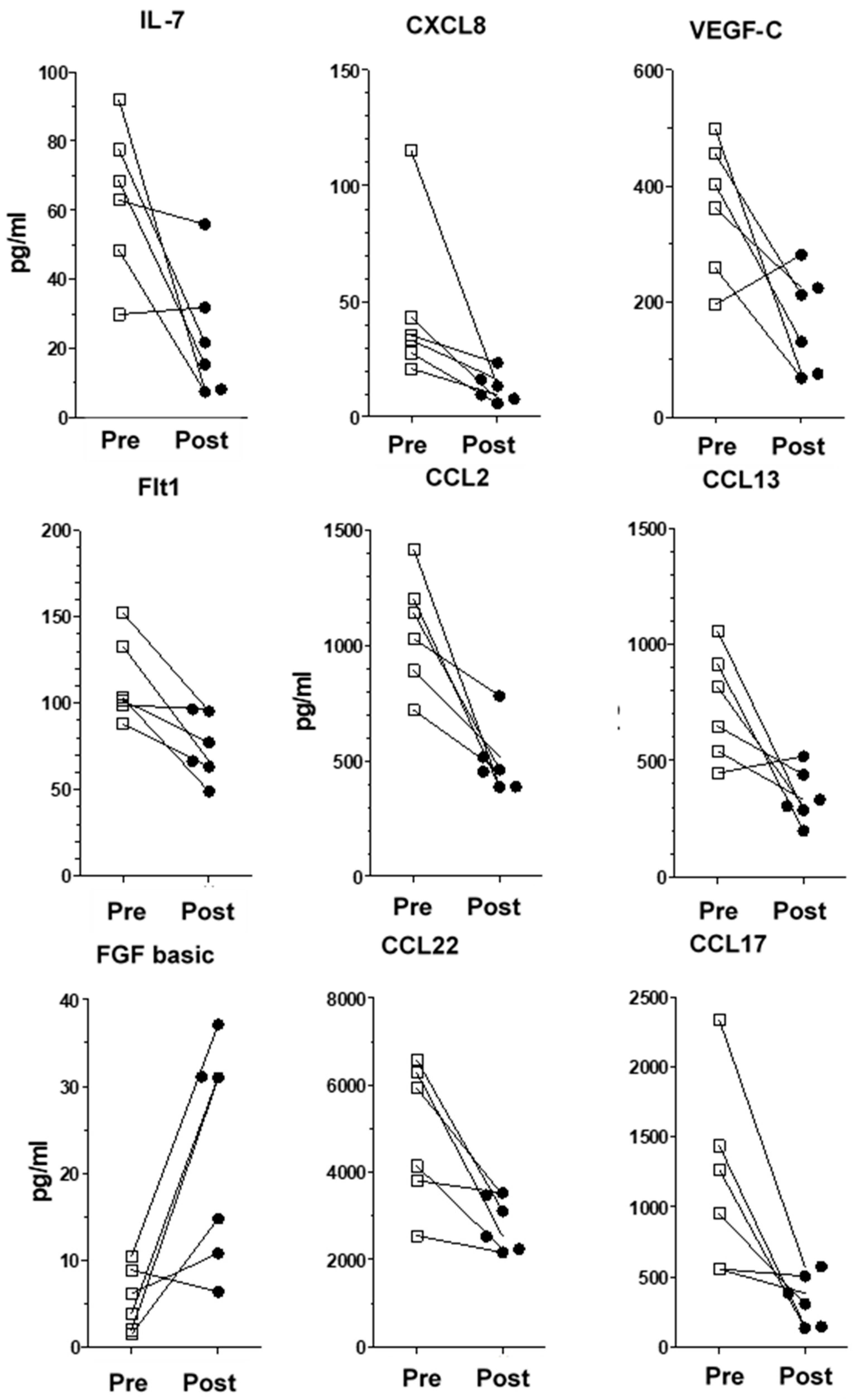
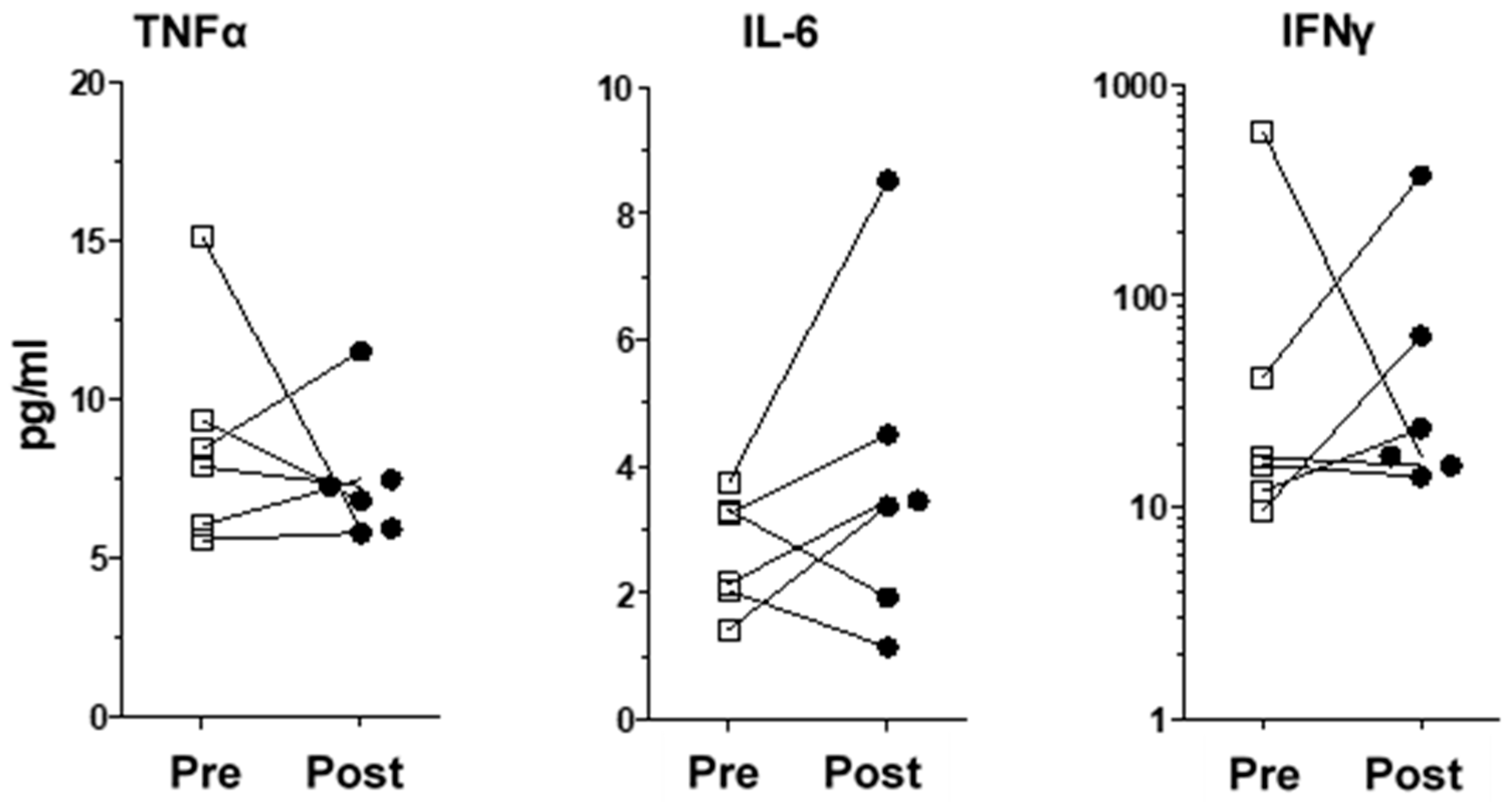
2.2. VNS Modulates Inflammatory Proteins in Sera of TRD Patients
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Measurement of Inflammatory Proteins in Plasma
4.3. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Himmerich, H.; Patsalos, O.; Lichtblau, N.; Ibrahim, M.A.A.; Dalton, B. Cytokine Research in Depression: Principles, Challenges, and Open Questions. Front. Psychiatry 2019, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Ay, I.; Nasser, R.; Simon, B.; Ay, H. Transcutaneous Cervical Vagus Nerve Stimulation Ameliorates Acute Ischemic Injury in Rats. Brain Stimul. 2016, 9, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B.L.; Bernstein, C.N. Brain-gut interactions in inflammatory bowel disease. Gastroenterology 2013, 144, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.; Ormstad, H.; Aass, H.C.; Malt, U.F.; Bendz, L.T.; Sandvik, L.; Brundin, L.; Andreassen, O.A. The plasma levels of various cytokines are increased during ongoing depression and are reduced to normal levels after recovery. Psychoneuroendocrinology 2014, 45, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Stuart, M.J.; Singhal, G.; Baune, B.T. Systematic Review of the Neurobiological Relevance of Chemokines to Psychiatric Disorders. Front. Cell. Neurosci. 2015, 9, 357. [Google Scholar] [CrossRef] [PubMed]
- Scheu, S.; Ali, S.; Ruland, C.; Arolt, V.; Alferink, J. The C-C Chemokines CCL17 and CCL22 and Their Receptor CCR4 in CNS Autoimmunity. Int. J. Mol. Sci. 2017, 18, 2306. [Google Scholar] [CrossRef] [PubMed]
- Leighton, S.P.; Nerurkar, L.; Krishnadas, R.; Johnman, C.; Graham, G.J.; Cavanagh, J. Chemokines in depression in health and in inflammatory illness: A systematic review and meta-analysis. Mol. Psychiatry 2018, 23, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, V.M.; Sarubin, N.; Hilbert, S.; Baghai, T.C.; Stoffler, F.; Lima-Ojeda, J.M.; Manook, A.; Almeqbaali, K.; Wetzel, C.H.; Rupprecht, R.; et al. Macrophage-Derived Chemokine: A Putative Marker of Pharmacological Therapy Response in Major Depression? Neuroimmunomodulation 2017, 24, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.G.; Cheng, Y.; Yu, X.C.; Ye, L.B.; Xia, Q.H.; Johnson, N.R.; Wei, X.; Chen, D.Q.; Cao, G.; Fu, X.B.; et al. bFGF Protects Against Blood-Brain Barrier Damage Through Junction Protein Regulation via PI3K-Akt-Rac1 Pathway Following Traumatic Brain Injury. Mol. Neurobiol. 2016, 53, 7298–7311. [Google Scholar] [CrossRef] [PubMed]
- Kumai, Y.; Ooboshi, H.; Ibayashi, S.; Ishikawa, E.; Sugimori, H.; Kamouchi, M.; Kitazono, T.; Egashira, K.; Iida, M. Postischemic gene transfer of soluble Flt-1 protects against brain ischemia with marked attenuation of blood-brain barrier permeability. J. Cereb. Blood Flow Metab. 2007, 27, 1152–1160. [Google Scholar] [CrossRef] [PubMed]
- Xie, T.; Stathopoulou, M.G.; de Andres, F.; Siest, G.; Murray, H.; Martin, M.; Cobaleda, J.; Delgado, A.; Lamont, J.; Penas, L.E.; et al. VEGF-related polymorphisms identified by GWAS and risk for major depression. Transl. Psychiatry 2017, 7, e1055. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Deng, S.; Zhang, M.R.; Tang, M.M. Fibroblast Growth Factors in Depression. Front. Pharmacol. 2019, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, S.T.; Sears, P.; Ruvuna, F.; Bunker, M.; Conway, C.R.; Dougherty, D.D.; Reimherr, F.W.; Schwartz, T.L.; Zajecka, J.M. A 5-Year Observational Study of Patients with Treatment-Resistant Depression Treated with Vagus Nerve Stimulation or Treatment as Usual: Comparison of Response, Remission, and Suicidality. Am. J. Psychiatry 2017, 174, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Desbeaumes Jodoin, V.; Miron, J.P.; Lesperance, P. Safety and Efficacy of Accelerated Repetitive Transcranial Magnetic Stimulation Protocol in Elderly Depressed Unipolar and Bipolar Patients. Am. J. Geriatr. Psychiatry 2019, 27, 548–558. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Patients (n = 6) | Healthy Donors (n = 6) |
|---|---|---|
| Age | 48.83 (41.0–57.0) | 32.67 (24–51) |
| Sex | ||
| Men | 2 (33.3%) | 2 (33.3%) |
| Women | 4 (66.6%) | 4 (66.6%) |
| Initial diagnosis | - | |
| Bipolar disorder | 2 (33.33%) | |
| Unipolar disorder | 4 (66.66%) | |
| Baseline clinical evaluation | - | |
| MADRS score | 24.5 (14–34) | |
| HAM-A score | 16.2 (9–29) |
| Baseline Score | Post-Treatment Score | Change (%) | p | |
|---|---|---|---|---|
| MADRS Score | 24.5 (14–34) | 5.8 (1–8) | 76.3 | 0.00074 |
| HAM-A Score | 16.2 (9–29) | 6.5 (2–13) | 59.9 | 0.0031 |
| Cytokine/Chemokine | Healthy Controls (pg/mL) | Baseline (pg/mL) | Post-Treatment (pg/mL) | Change (%) | p |
|---|---|---|---|---|---|
| IL-7 | 4.0 (0.97) | 63.2 (21.9) | 23.4 (18.4) | −63.0 | 0.029 |
| CXCL8 | 2.0 (0.5) | 40.5 (31.8) | 5.8 (2.0) | −85.7 | 0.041 |
| CCL2 | 40.0 (11.2) | 1065.2 (244.3) | 498.2 (146.5) | −53.2 | 0.007 |
| CCL13 | 63.0 (22.6) | 736.4 (232.6) | 346.3 (114.3) | −53.0 | 0.034 |
| CCL17 | 100.0 (25.0) | 1182.4 (669.7) | 340.1 (181.9) | −71.2 | 0.028 |
| CCL22 | 1162.0 (265.0) | 4882.8 (1615.7) | 2843.4 (610.4) | −41.8 | 0.020 |
| Flt-1 | 40.0 (5.0) | 112.7 (24.5) | 74.5 (18.8) | −32.8 | 0.013 |
| VEGF-C | 37.0 (25.0) | 361.9 (116.6) | 165.2 (86.8) | −54.4 | 0.036 |
| bFGF | 39.0 (42.0) | 5.5 (3.7) | 21.9 (12.7) | 298.2 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lespérance, P.; Desbeaumes Jodoin, V.; Drouin, D.; Racicot, F.; Miron, J.-P.; Longpré-Poirier, C.; Fournier-Gosselin, M.-P.; Thebault, P.; Lapointe, R.; Arbour, N.; et al. Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study. Int. J. Mol. Sci. 2024, 25, 2679. https://doi.org/10.3390/ijms25052679
Lespérance P, Desbeaumes Jodoin V, Drouin D, Racicot F, Miron J-P, Longpré-Poirier C, Fournier-Gosselin M-P, Thebault P, Lapointe R, Arbour N, et al. Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study. International Journal of Molecular Sciences. 2024; 25(5):2679. https://doi.org/10.3390/ijms25052679
Chicago/Turabian StyleLespérance, Paul, Véronique Desbeaumes Jodoin, David Drouin, Frédéric Racicot, Jean-Philippe Miron, Christophe Longpré-Poirier, Marie-Pierre Fournier-Gosselin, Paméla Thebault, Réjean Lapointe, Nathalie Arbour, and et al. 2024. "Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study" International Journal of Molecular Sciences 25, no. 5: 2679. https://doi.org/10.3390/ijms25052679
APA StyleLespérance, P., Desbeaumes Jodoin, V., Drouin, D., Racicot, F., Miron, J.-P., Longpré-Poirier, C., Fournier-Gosselin, M.-P., Thebault, P., Lapointe, R., Arbour, N., & Cailhier, J.-F. (2024). Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study. International Journal of Molecular Sciences, 25(5), 2679. https://doi.org/10.3390/ijms25052679