

Real-World Data and Clinical Implications of Next-Generation Sequencing (NGS)-Based Analysis in Metastatic Breast Cancer Patients
 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Results
2.1. Population Characteristics
2.2. Population Molecular Profile
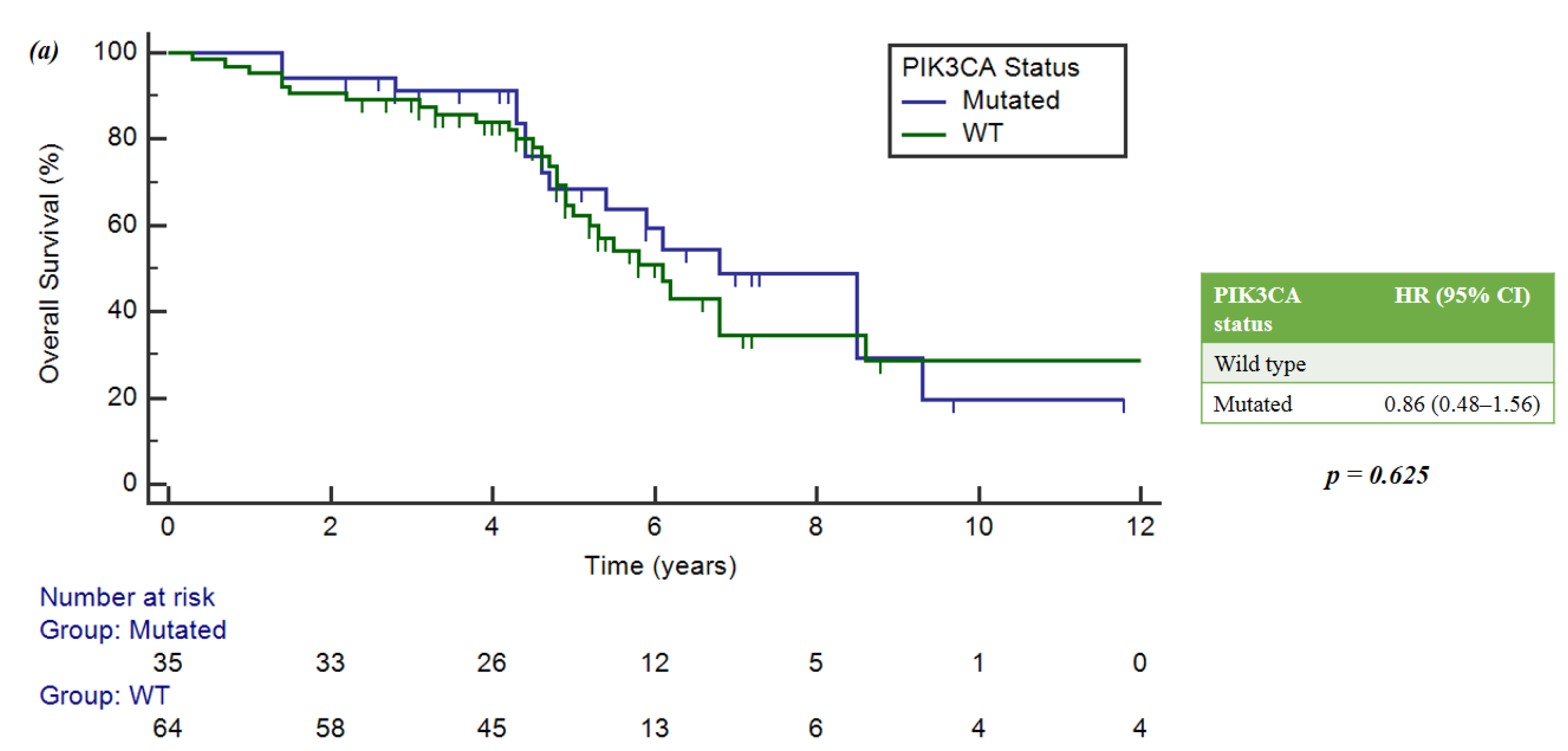
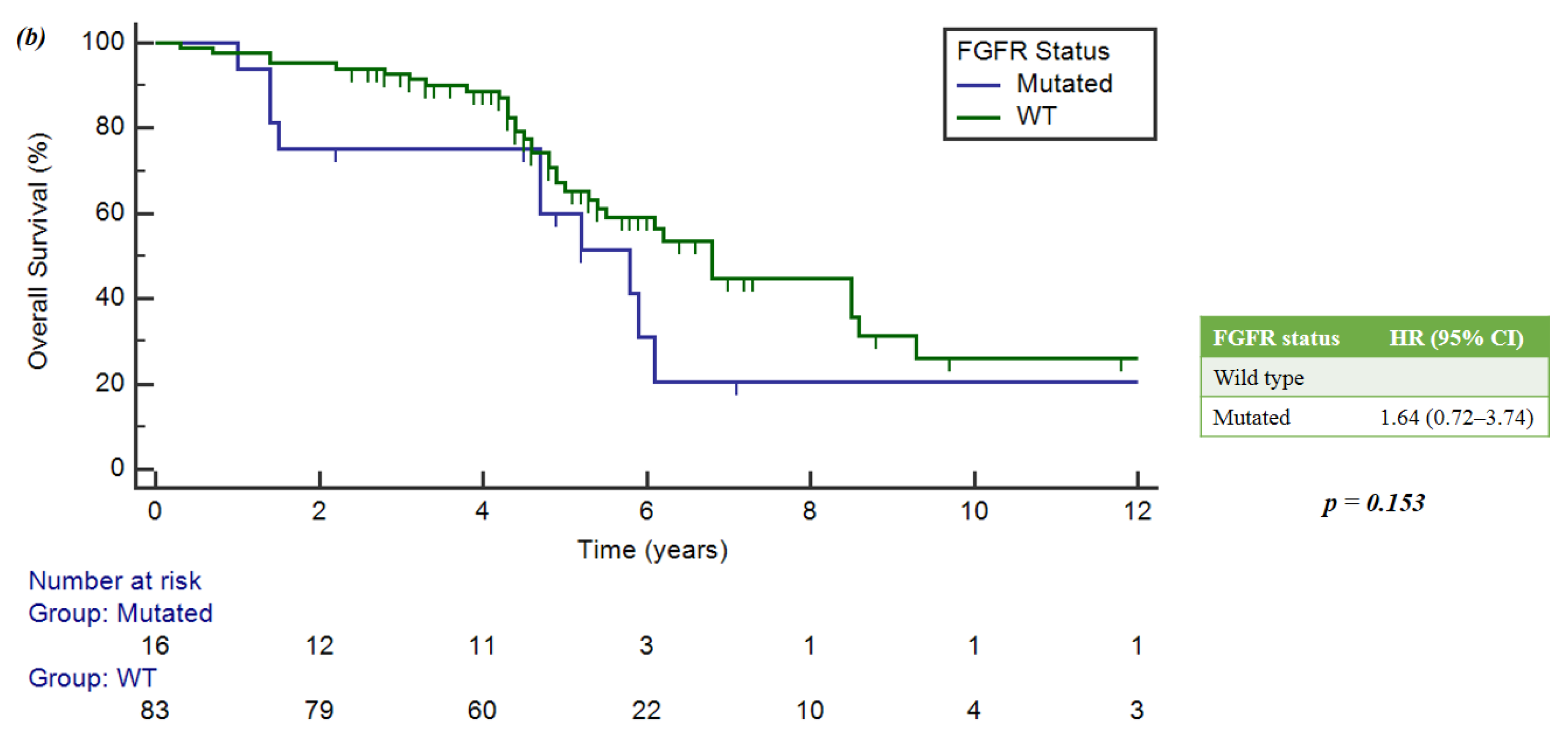
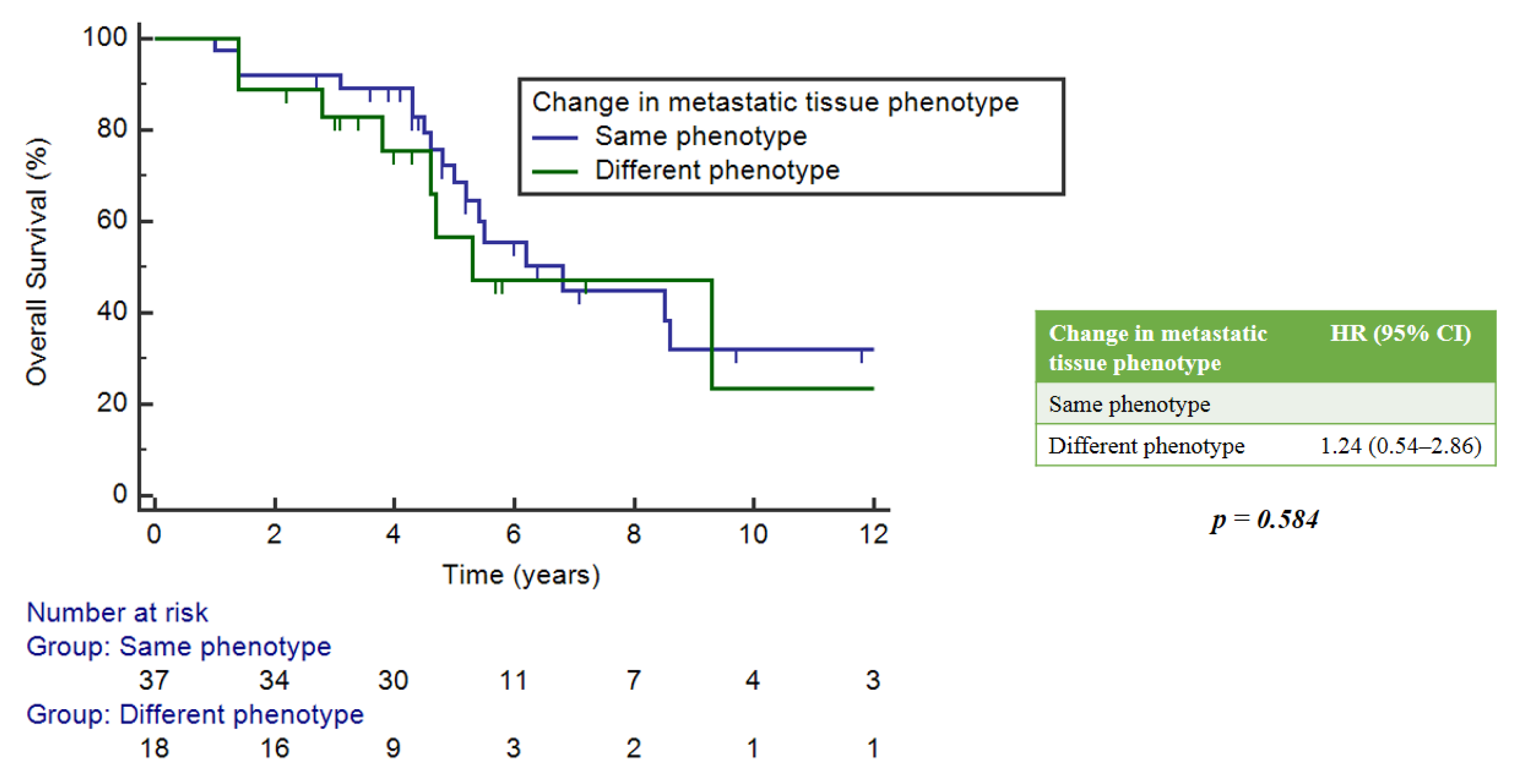
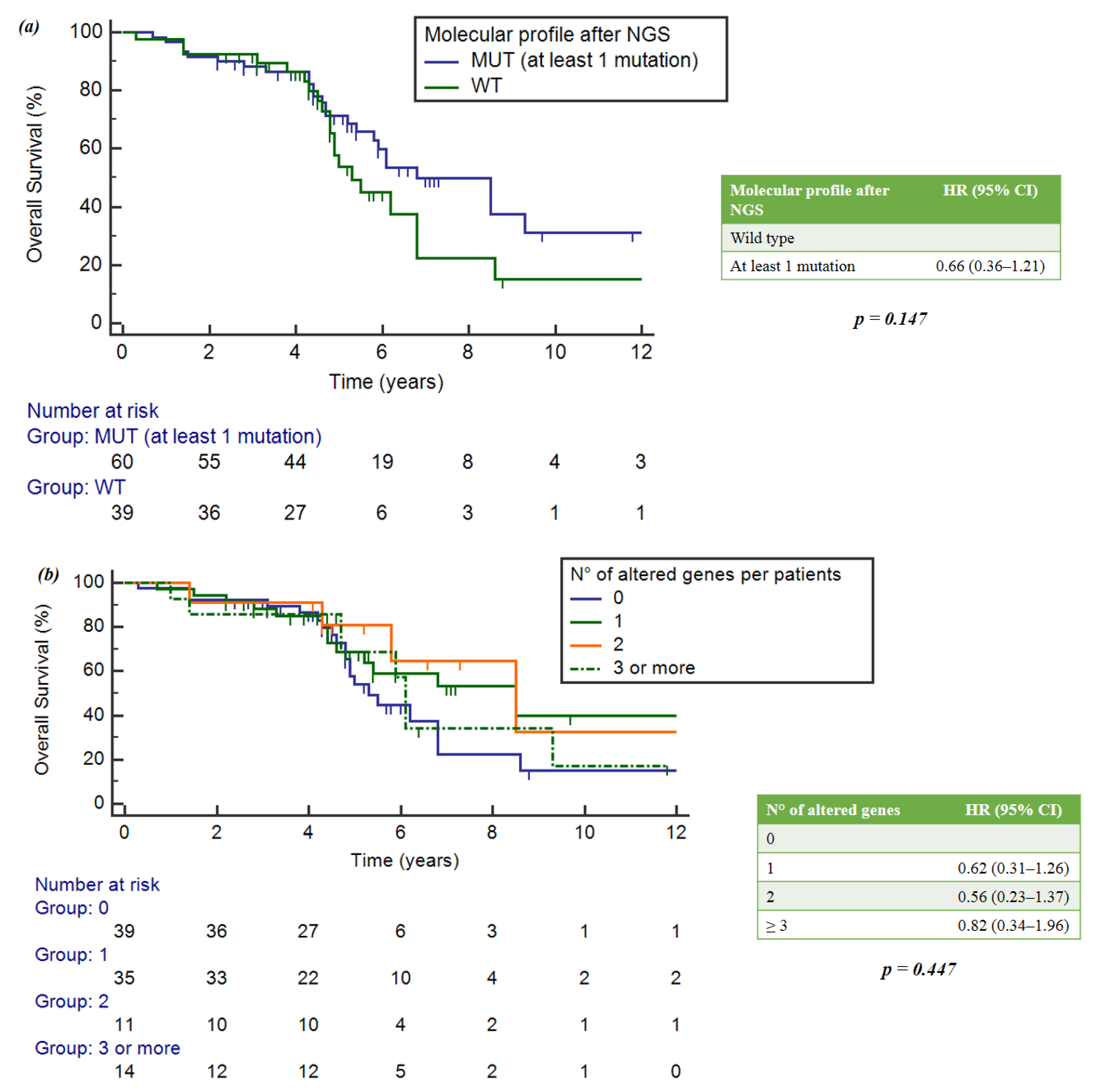
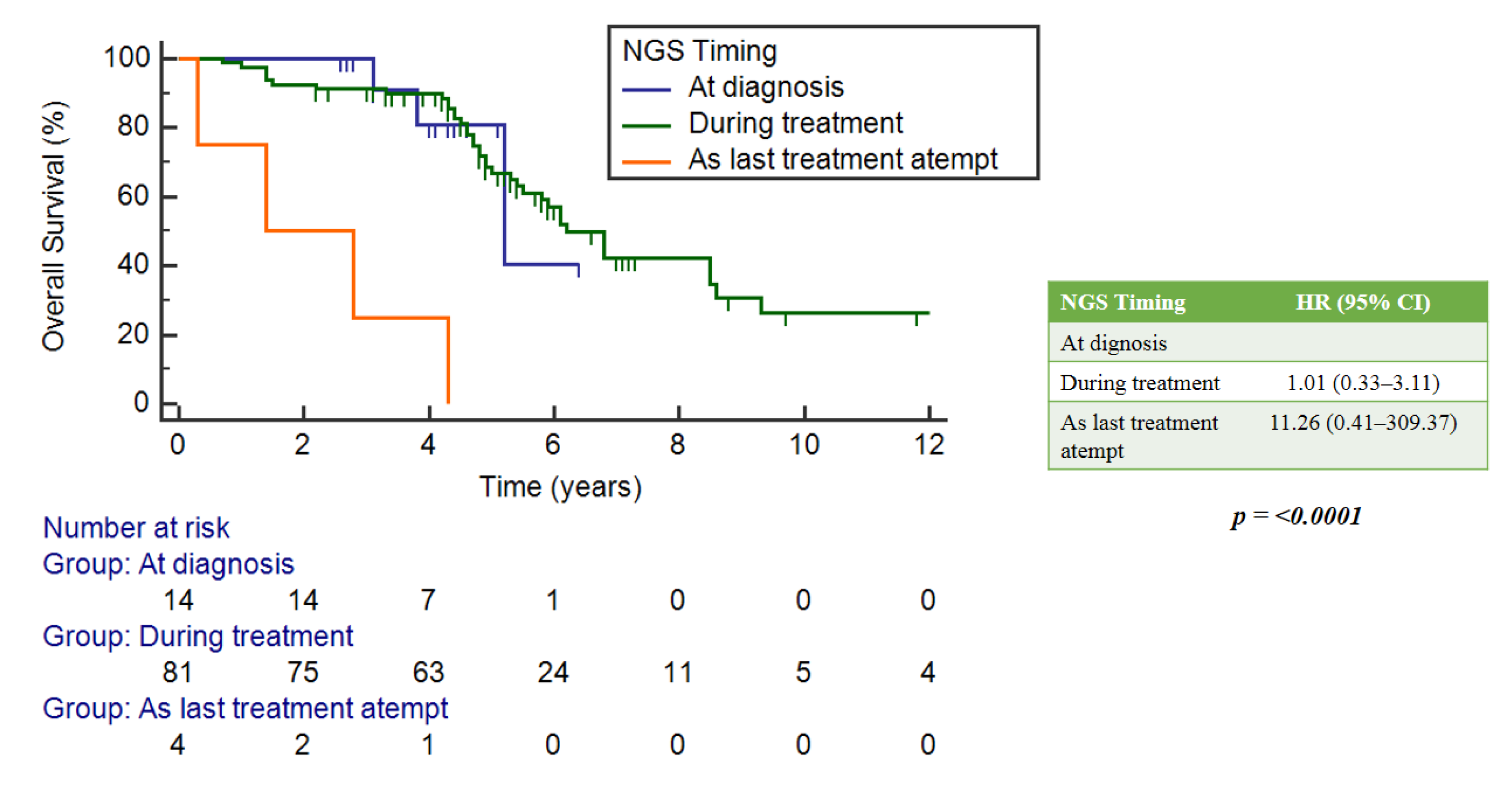
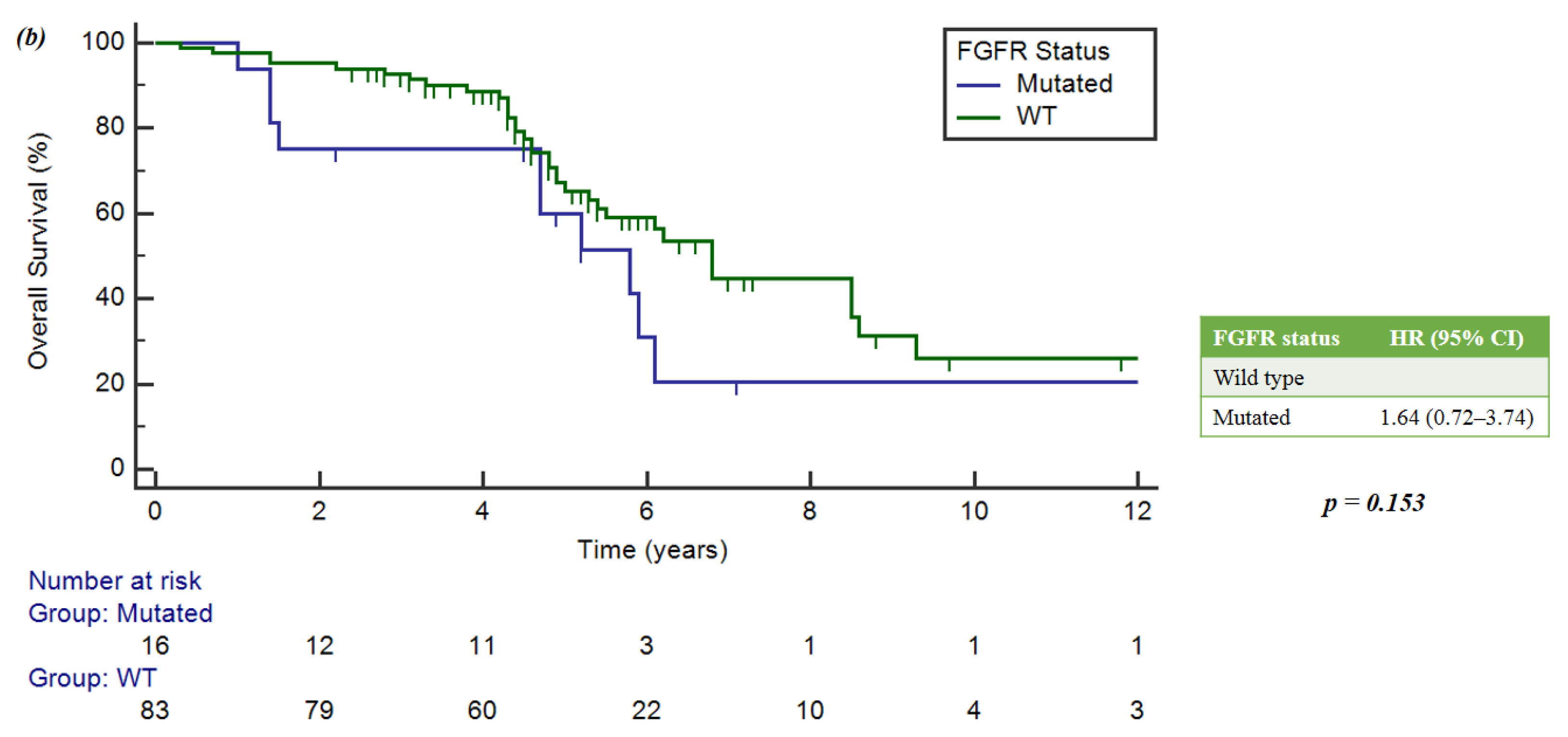
2.3. Prognostic Impact of NGS-Based Analysis
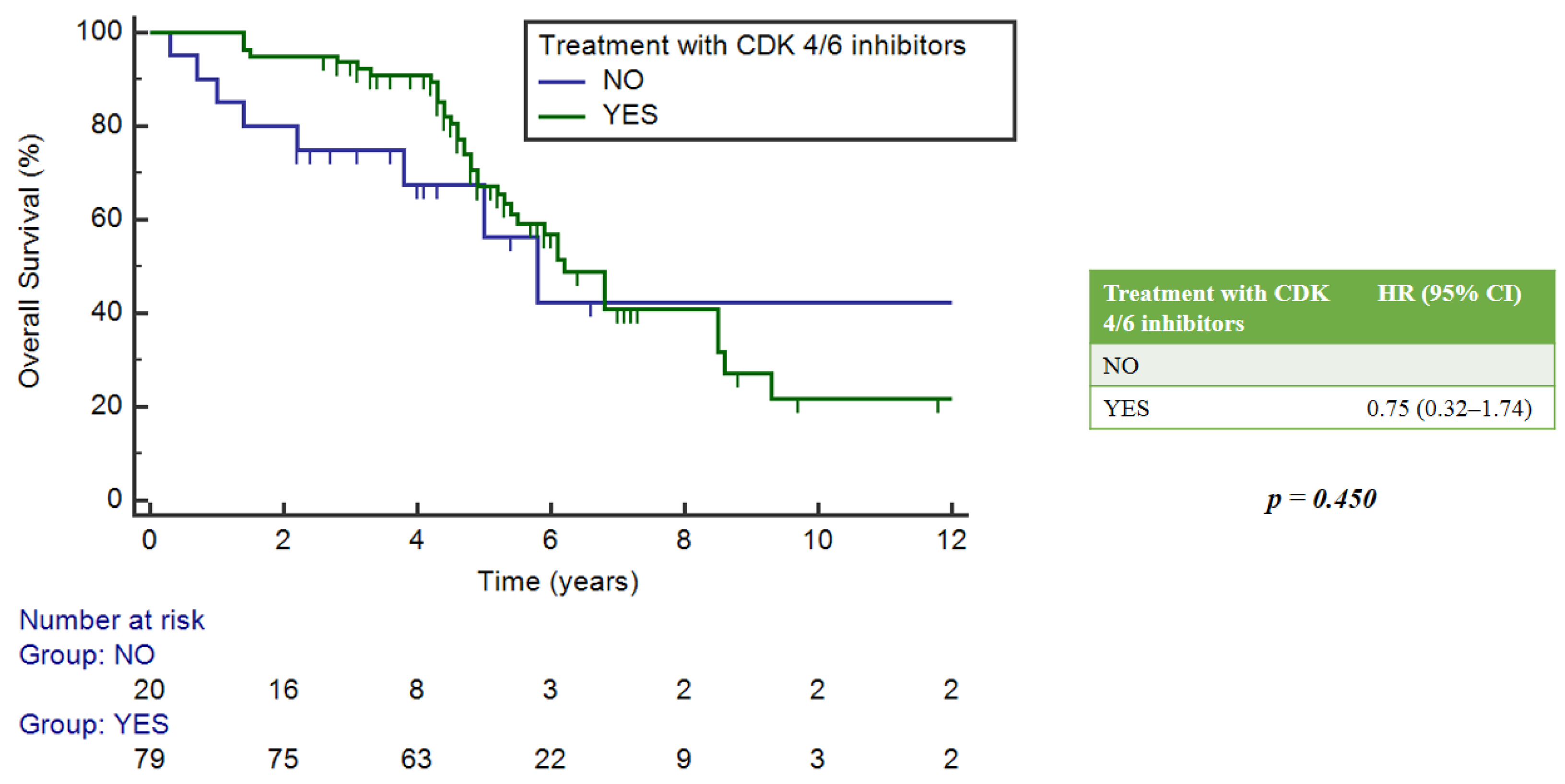
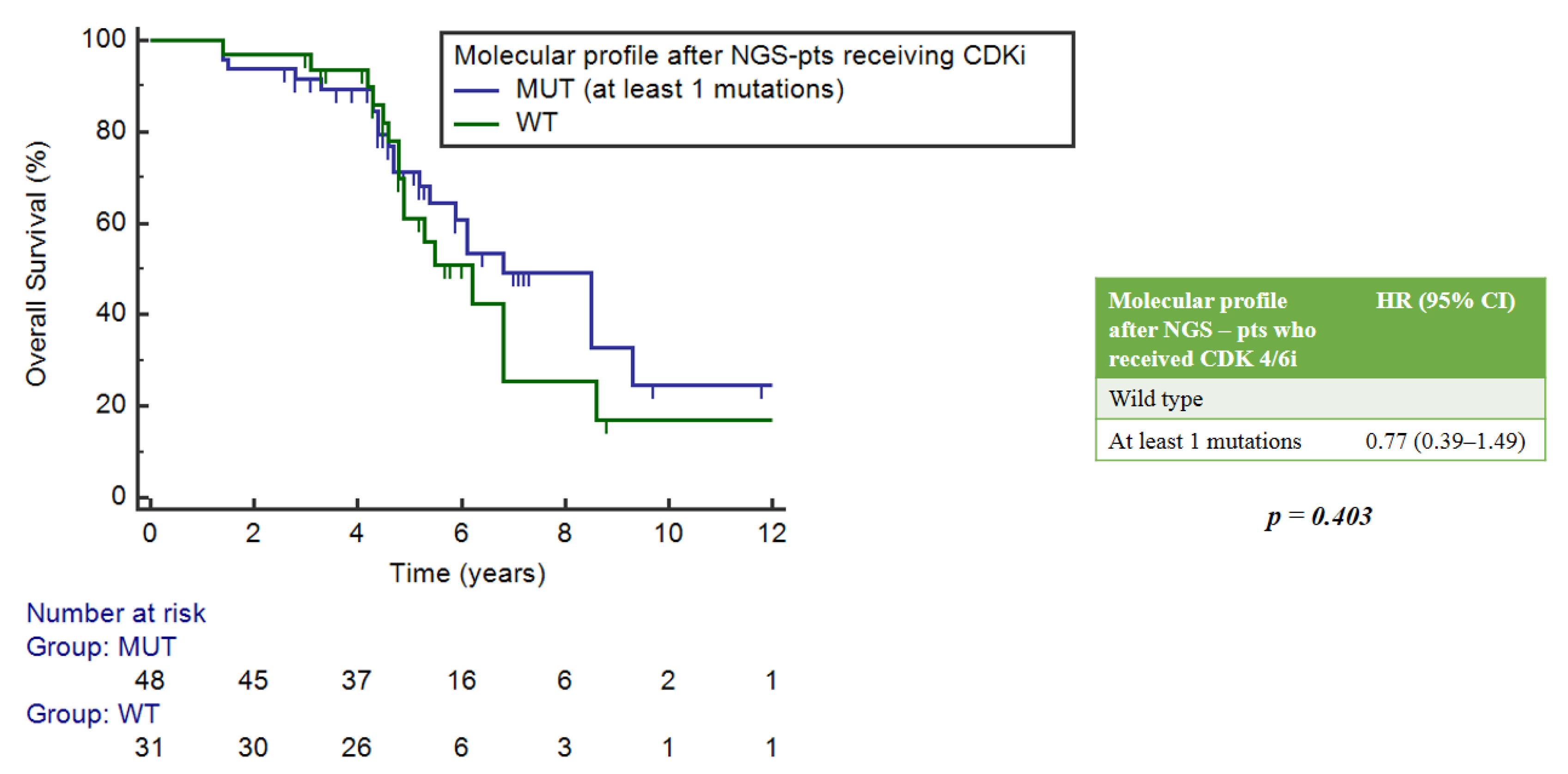
2.4. Role of the NGS Test in the Population Treated with CDK4/6 Inhibitors
2.5. Actionable Mutations
3. Discussion
4. Methods
4.1. Ethical Committee
4.2. Patients
4.3. NGS Test
- (1)
- Myriapod NGS-IL 56G Onco Panel (Diatech Pharmacogenetics, Iesi, Italy): allows the analysis of hotspot variants on DNA in 56 cancer-related genes (ABL1, AKT1, ALK, APC, ATM, BRAF, CDH1, CDKN2A, CSF1R, CTNNB1, DDR2, DNMT3A, EGFR, ERBB2, ERBB4, EZH2, FBXW7, FGFR1, FGFR2, FGFR3, FLT3, FOXL2, GNA11, GNAQ, GNAS, HNF1A, HRAS, IDH1, IDH2, JAK2, JAK3, KDR, KIT, KRAS, MA2K1, MET, MLH1, MLP, MSH6, NOTCH, NPM1, NRAS, PDGFRA, PIK3CA, PTEN, PTPN11, RB1, RET, SKT11, SMAD4, SMARCB1, SMO, SRC, TP53, TSC1, VHL). It requires three days of manual work and then loading on the platform.
- (2)
- Myriapod NGS Cancer Panel DNA (Diatech Pharmacogenetics): includes DNA analysis of 16 genes with current clinical utility (ALK, BRAF, EGFR, ERBB2, FGFR3, HRAS, IDH1, IDH2, KIT, KRAS, MET, NRAS, PDFRA, PIK3CA, RET, ROS1). It requires 1–2 days of manual work, followed by loading on the platform.
- (1)
- DNA analysis of the hotspot variants (SNV, MNV, INDELs) of clinical relevance for 41 genes (AKT1, ALK, AR, BRAF, CCND1, CDK4, CDK6, CTNNB1, DDR2, EGFR, ERBB2, ERBB3, ERBB4, ESR1, FGFR1, FGFR2, FGFR3, FGFR4, GNA11, GNAQ, HRAS, IDH1, IDH2, JAK1, JAK2, JAK3, KIT, KRAS, MAP2K1, MAP2K2, MET, MTOR, MYC, MYCN, NRAS, PDGFRA, PIK3CA, RAF1, RET, ROS1, SMO);
- (2)
- RNA analysis of 23 gene fusion transcripts (ABL1, ALK, AKT3, AXL, BRAF, EGFR, ERBB2, ERG, ETV1, ETV4, ETV5, FGFR1, FGFR2, FGFR3, MET, NTRK1, NTRK2, NTRK3, PDGFRA, PPARG, RAF1, RET, ROS1).
4.4. Bioinformatics Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamps, R.; Brandão, R.D.; van den Bosch, B.J.; Paulussen, A.D.C.; Xanthoulea, S.; Blok, M.J.; Romano, A. Next-Generation Sequencing in Oncology: Genetic Diagnosis, Risk Prediction and Cancer Classification. Int. J. Mol. Sci. 2017, 18, 308. [Google Scholar] [CrossRef]
- Morganti, S.; Tarantino, P.; Ferraro, E.; D’Amico, P.; Viale, G.; Trapani, D.; Duso, B.A.; Curigliano, G. Complexity of Genome Sequencing and Reporting: Next Generation Sequencing (NGS) Technologies and Implementation of Precision Medicine in Real Life. Crit. Rev. Oncol. Hematol. 2019, 133, 171–182. [Google Scholar] [CrossRef]
- Rodon, J.; Soria, J.-C.; Berger, R.; Miller, W.H.; Rubin, E.; Kugel, A.; Tsimberidou, A.; Saintigny, P.; Ackerstein, A.; Braña, I.; et al. Genomic and Transcriptomic Profiling Expands Precision Cancer Medicine: The WINTHER Trial. Nat. Med. 2019, 25, 751–758. [Google Scholar] [CrossRef]
- Karlovich, C.A.; Williams, P.M. Clinical Applications of Next-Generation Sequencing in Precision Oncology. Cancer J. 2019, 25, 264–271. [Google Scholar] [CrossRef]
- Shabani Azim, F.; Houri, H.; Ghalavand, Z.; Nikmanesh, B. Next Generation Sequencing in Clinical Oncology: Applications, Challenges and Promises: A Review Article. Iran J. Public Health 2018, 47, 1453–1457. [Google Scholar]
- Bianchi, V.; Ceol, A.; Ogier, A.G.E.; de Pretis, S.; Galeota, E.; Kishore, K.; Bora, P.; Croci, O.; Campaner, S.; Amati, B.; et al. Integrated Systems for NGS Data Management and Analysis: Open Issues and Available Solutions. Front. Genet. 2016, 7, 75. [Google Scholar] [CrossRef]
- Nekrutenko, A.; Taylor, J. Next-Generation Sequencing Data Interpretation: Enhancing Reproducibility and Accessibility. Nat. Rev. Genet. 2012, 13, 667–672. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.B.; Barlesi, F.; Lolkema, M.P.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the Use of Next-Generation Sequencing (NGS) for Patients with Metastatic Cancers: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef] [PubMed]
- Toss, A.; Piacentini, F.; Cortesi, L.; Artuso, L.; Bernardis, I.; Parenti, S.; Tenedini, E.; Ficarra, G.; Maiorana, A.; Iannone, A.; et al. Genomic Alterations at the Basis of Treatment Resistance in Metastatic Breast Cancer: Clinical Applications. Oncotarget 2018, 9, 31606–31619. [Google Scholar] [CrossRef] [PubMed]
- Zundelevich, A.; Dadiani, M.; Kahana-Edwin, S.; Itay, A.; Sella, T.; Gadot, M.; Cesarkas, K.; Farage-Barhom, S.; Saar, E.G.; Eyal, E.; et al. ESR1 Mutations Are Frequent in Newly Diagnosed Metastatic and Loco-Regional Recurrence of Endocrine-Treated Breast Cancer and Carry Worse Prognosis. Breast Cancer Res. 2020, 22, 16. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Lee, B.; Shim, J.H.; Lee, K.W.; Yun, J.W.; Kim, S.-Y.; Kim, T.-Y.; Kim, Y.H.; Ko, Y.H.; Chung, H.C.; et al. Landscape of Actionable Genetic Alterations Profiled from 1,071 Tumor Samples in Korean Cancer Patients. Cancer Res. Treat 2019, 51, 211–222. [Google Scholar] [CrossRef]
- Kwon, D.; Kim, B.; Shin, H.C.; Kim, E.J.; Ha, S.Y.; Jang, K.-T.; Kim, S.T.; Lee, J.; Kang, W.K.; Park, J.O.; et al. Cancer Panel Assay for Precision Oncology Clinic: Results from a 1-Year Study. Transl. Oncol. 2019, 12, 1488–1495. [Google Scholar] [CrossRef]
- Kim, J.H.; Yoon, S.; Lee, D.H.; Jang, S.J.; Chun, S.-M.; Kim, S.-W. Real-World Utility of next-Generation Sequencing for Targeted Gene Analysis and Its Application to Treatment in Lung Adenocarcinoma. Cancer Med. 2021, 10, 3197–3204. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Delord, J.-P.; Gonçalves, A.; Gavoille, C.; Dubot, C.; Isambert, N.; Campone, M.; Trédan, O.; Massiani, M.-A.; Mauborgne, C.; et al. Molecularly Targeted Therapy Based on Tumour Molecular Profiling versus Conventional Therapy for Advanced Cancer (SHIVA): A Multicentre, Open-Label, Proof-of-Concept, Randomised, Controlled Phase 2 Trial. Lancet Oncol. 2015, 16, 1324–1334. [Google Scholar] [CrossRef]
- Schwaederle, M.; Parker, B.A.; Schwab, R.B.; Daniels, G.A.; Piccioni, D.E.; Kesari, S.; Helsten, T.L.; Bazhenova, L.A.; Romero, J.; Fanta, P.T.; et al. Precision Oncology: The UC San Diego Moores Cancer Center PREDICT Experience. Mol. Cancer Ther. 2016, 15, 743–752. [Google Scholar] [CrossRef]
- Andre, F.; Filleron, T.; Kamal, M.; Mosele, F.; Arnedos, M.; Dalenc, F.; Sablin, M.-P.; Campone, M.; Bonnefoi, H.; Lefeuvre-Plesse, C.; et al. Genomics to Select Treatment for Patients with Metastatic Breast Cancer. Nature 2022, 610, 343–348. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [PubMed]
- Mateo, J.; Chakravarty, D.; Dienstmann, R.; Jezdic, S.; Gonzalez-Perez, A.; Lopez-Bigas, N.; Ng, C.K.Y.; Bedard, P.L.; Tortora, G.; Douillard, J.-Y.; et al. A Framework to Rank Genomic Alterations as Targets for Cancer Precision Medicine: The ESMO Scale for Clinical Actionability of Molecular Targets (ESCAT). Ann. Oncol. 2018, 29, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Condorelli, R.; Mosele, F.; Verret, B.; Bachelot, T.; Bedard, P.L.; Cortes, J.; Hyman, D.M.; Juric, D.; Krop, I.; Bieche, I.; et al. Genomic Alterations in Breast Cancer: Level of Evidence for Actionability According to ESMO Scale for Clinical Actionability of Molecular Targets (ESCAT). Ann. Oncol. 2019, 30, 365–373. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Bachelot, T.; Commo, F.; Campone, M.; Arnedos, M.; Dieras, V.; Lacroix-Triki, M.; Lacroix, L.; Cohen, P.; Gentien, D.; et al. Comparative Genomic Hybridisation Array and DNA Sequencing to Direct Treatment of Metastatic Breast Cancer: A Multicentre, Prospective Trial (SAFIR01/UNICANCER). Lancet Oncol. 2014, 15, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Van Geelen, C.T.; Savas, P.; Teo, Z.L.; Luen, S.J.; Weng, C.-F.; Ko, Y.-A.; Kuykhoven, K.S.; Caramia, F.; Salgado, R.; Francis, P.A.; et al. Clinical Implications of Prospective Genomic Profiling of Metastatic Breast Cancer Patients. Breast Cancer Res. 2020, 22, 91. [Google Scholar] [CrossRef] [PubMed]
- Sultova, E.; Westphalen, C.B.; Jung, A.; Kumbrink, J.; Kirchner, T.; Mayr, D.; Rudelius, M.; Ormanns, S.; Heinemann, V.; Metzeler, K.H.; et al. Implementation of Precision Oncology for Patients with Metastatic Breast Cancer in an Interdisciplinary MTB Setting. Diagnostics 2021, 11, 733. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 101 | (%) | |
| Median Age at diagnosis | ||
| 52 years | [29–82 years] | |
| Stage at diagnosis | ||
| I | 9 | (8.9%) |
| II | 32 | (31.7%) |
| III | 24 | (23.8%) |
| IV | 36 | (35.6%) |
| Tumor phenotype at diagnosis | ||
| Luminal A-like | 52 | (51.5%) |
| Luminal B-like | 34 | (33.7%) |
| HER2-positive | 10 | (9.9%) |
| Triple-negative | 5 | (4.9%) |
| N° of metastatic sites at diagnosis of mBC | ||
| 1 | 48 | (47.5%) |
| 2 | 46 | (45.5%) |
| ≥3 | 7 | (7%) |
| Type of metastatic sites at diagnosis of mBC | ||
| Bone only | 15 | (14.8%) |
| Visceral only | 32 | (31.7%) |
| CNS only | 1 | (1%) |
| Bone and visceral | 53 | (52.5%) |
| Concordance in tumor phenotype between metastases and primary * (N = 52 biopsies on metastatic site) | ||
| Same tumor phenotype | 35 | (67.3%) |
| Change in tumor phenotype | 17 | (32.7%) |
| Prior (neo)adjuvant treatments | ||
| Chemotherapy | 61 | (60.4%) |
| Endocrine therapy | 59 | (58.4%) |
| Systemic treatments for metastatic disease (N° of lines) | ||
| 1 | 31 | (30.7%) |
| 2 | 19 | (18.8%) |
| ≥3 | 51 | (50.5%) |
| N = 101 | (%) | |
| Origin of tumor tissue tested for NGS | ||
| Primary tumor | 47 | (46.5%) |
| Metastatic site | 52 | (51.5%) |
| 7 | (7%) |
| 8 | (7.9%) |
| 3 | (3%) |
| 21 | (20.8%) |
| 8 | (7.9%) |
| 5 | (5%) |
| Liquid biopsy | 2 | (2%) |
| N° of mutations per patients | ||
| Wild type | 40 | (39.6%) |
| Mutated | 61 | (60.4%) |
| 35 | (34.7%) |
| 11 | (10.9%) |
| 15 | (14.9%) |
| Mutation classification according to ESCAT scale | ||
| 35 | (57.4%) |
| 11 | (18.0%) |
| 15 | (24.6%) |
| Patients | N° Prior Systemic Treatments For Mbc | Mutations | Target Treatment | PFS (Months) | State of Patient |
|---|---|---|---|---|---|
| 1 | 14 | PIK3CA | Alpelisib + Fulvestrant | 3.8 | Dead |
| 2 | 9 | PIK3CA | Alpelisib + Fulvestrant | 0.5 | Dead |
| 3 | 2 | PIK3CA | Alpelisib + Fulvestrant | 1.6 | Alive |
| 4 | 2 | PIK3CA | Alpelisib + Fulvestrant | 24.2 | Alive |
| 5 | 5 | PIK3CA | Alpelisib + Fulvestrant | 13.1 | Dead |
| 6 | 6 | PIK3CA | Alpelisib + Fulvestrant | 8.5 | Dead |
| 7 | 3 | PIK3CA | Alpelisib + Fulvestrant | 1.0 | Alive |
| 8 | 6 | PIK3CA | Alpelisib + Fulvestrant | 2.1 | Alive |
| 9 | 3 | FGFR1/2 | TAS-120 | 11.7 | Dead |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canino, F.; Tornincasa, A.; Bettelli, S.; Manfredini, S.; Barbolini, M.; Moscetti, L.; Omarini, C.; Toss, A.; Tamburrano, F.; Antonelli, G.; et al. Real-World Data and Clinical Implications of Next-Generation Sequencing (NGS)-Based Analysis in Metastatic Breast Cancer Patients. Int. J. Mol. Sci. 2024, 25, 2490. https://doi.org/10.3390/ijms25052490
Canino F, Tornincasa A, Bettelli S, Manfredini S, Barbolini M, Moscetti L, Omarini C, Toss A, Tamburrano F, Antonelli G, et al. Real-World Data and Clinical Implications of Next-Generation Sequencing (NGS)-Based Analysis in Metastatic Breast Cancer Patients. International Journal of Molecular Sciences. 2024; 25(5):2490. https://doi.org/10.3390/ijms25052490
Chicago/Turabian StyleCanino, Fabio, Antonio Tornincasa, Stefania Bettelli, Samantha Manfredini, Monica Barbolini, Luca Moscetti, Claudia Omarini, Angela Toss, Fabio Tamburrano, Giuseppina Antonelli, and et al. 2024. "Real-World Data and Clinical Implications of Next-Generation Sequencing (NGS)-Based Analysis in Metastatic Breast Cancer Patients" International Journal of Molecular Sciences 25, no. 5: 2490. https://doi.org/10.3390/ijms25052490
APA StyleCanino, F., Tornincasa, A., Bettelli, S., Manfredini, S., Barbolini, M., Moscetti, L., Omarini, C., Toss, A., Tamburrano, F., Antonelli, G., Baglio, F., Belluzzi, L., Martinelli, G., Natalizio, S., Ponzoni, O., Dominici, M., & Piacentini, F. (2024). Real-World Data and Clinical Implications of Next-Generation Sequencing (NGS)-Based Analysis in Metastatic Breast Cancer Patients. International Journal of Molecular Sciences, 25(5), 2490. https://doi.org/10.3390/ijms25052490