
Assessment of the Impact of Carvedilol Administered Together with Dexrazoxan and Doxorubicin on Liver Structure and Function, Iron Metabolism, and Myocardial Redox System in Rats
 , ,
, ,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Results
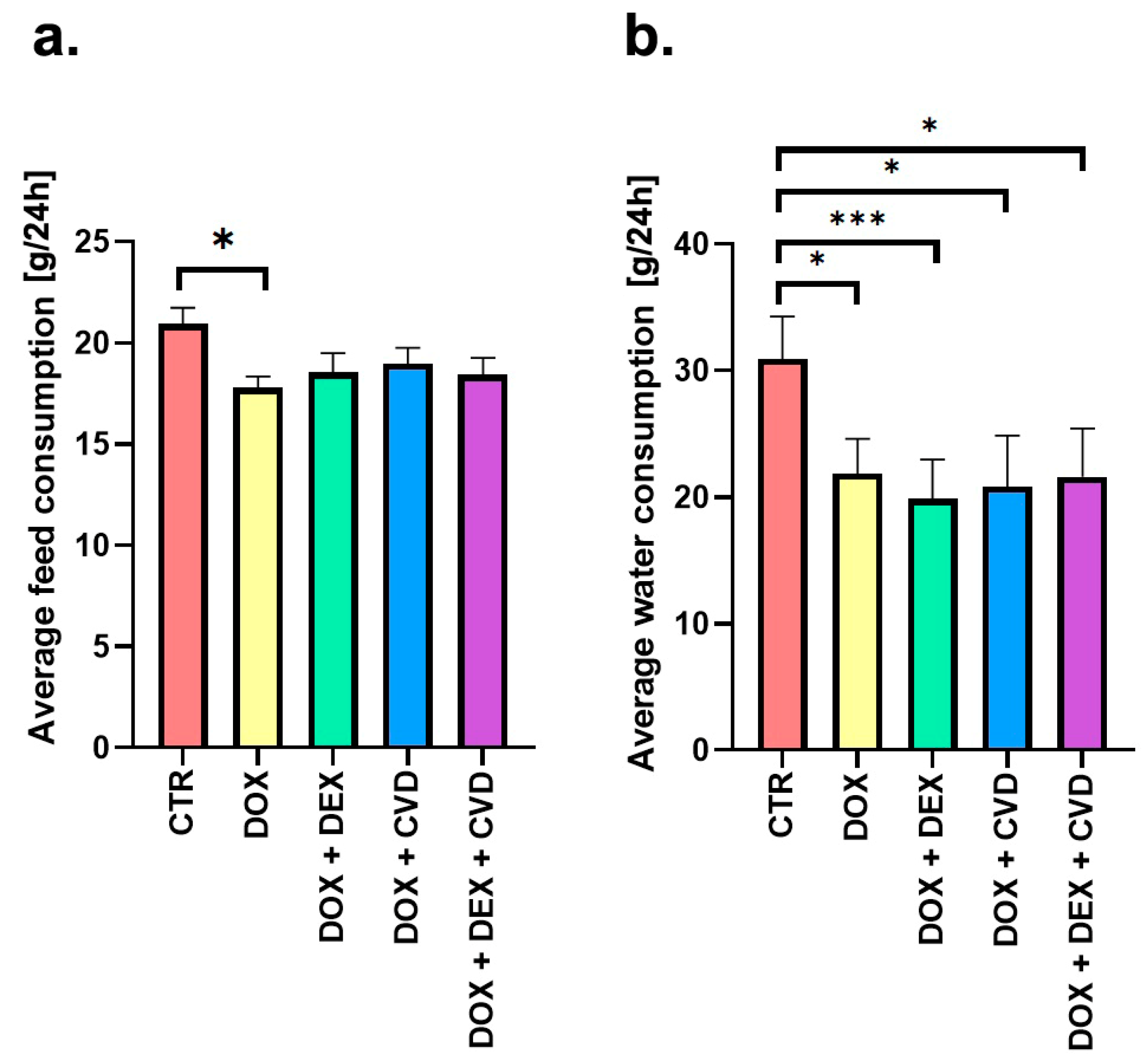
2.1. Body Mass Dynamics and Consumption Patterns
2.2. Biochemical Analyses
2.3. Assessment of Gene Expression
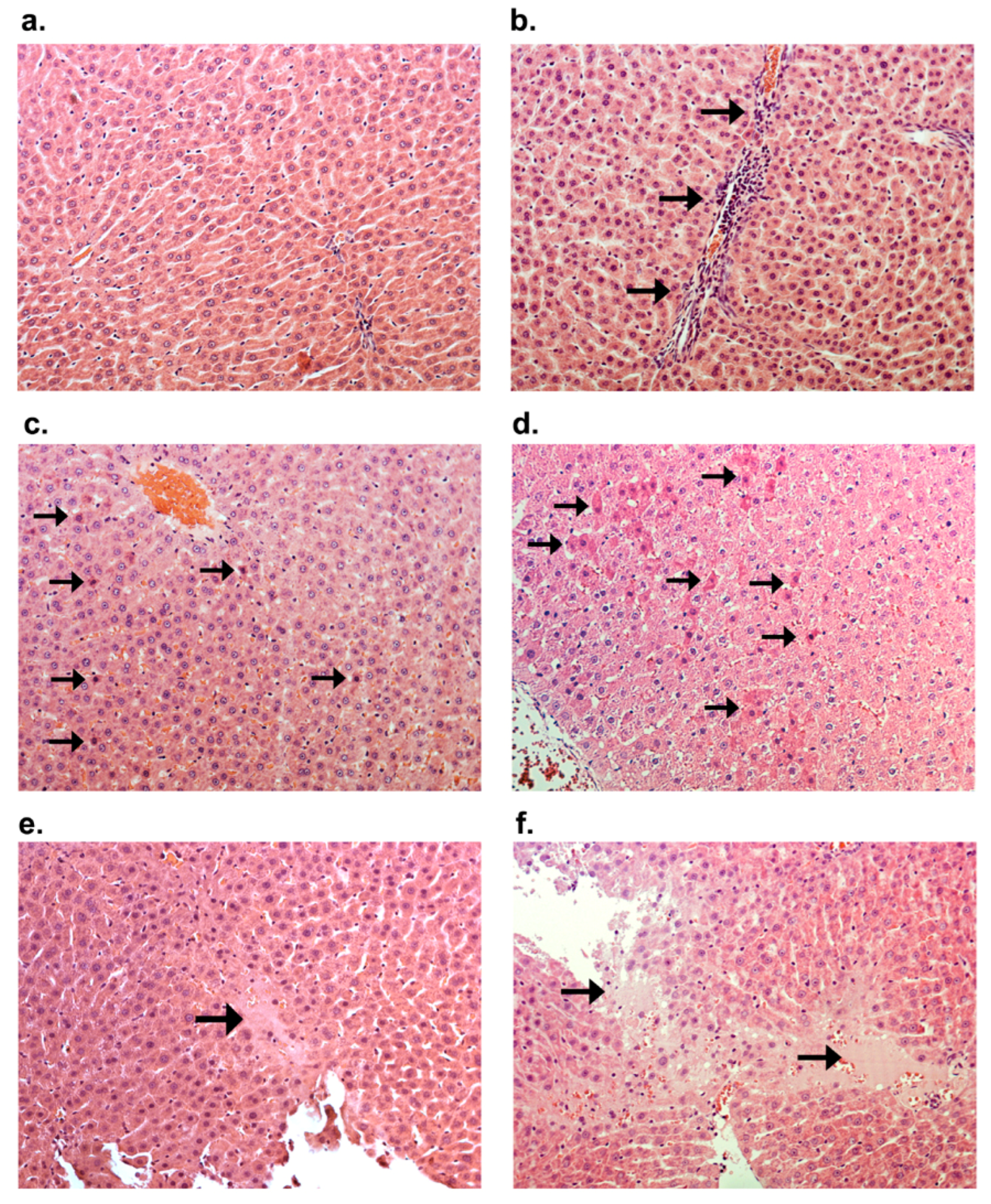
2.4. Histological Staining
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Experimental Design
4.3. Biochemical Analysis
4.4. Molecular Studies (qPCR Analysis)
4.5. Histological Staining
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CTR | control; |
| CVD | carvedilol; |
| DEX | dexrazoxane; |
| DOX | doxorubicin; |
| FDA | Food and Drug Administration; |
| IP | intraperitoneal |
| LVEF | left ventricular ejection fraction; |
| ROS | reactive oxygen species; |
| RQ | relative quantification; |
| TOP2β | topoisomerase 2β. |
References
- Kalyanaraman, B. Teaching the Basics of the Mechanism of Doxorubicin-Induced Cardiotoxicity: Have We Been Barking up the Wrong Tree? Redox Biol. 2020, 29, 101394. [Google Scholar] [CrossRef] [PubMed]
- Sritharan, S.; Sivalingam, N. A Comprehensive Review on Time-Tested Anticancer Drug Doxorubicin. Life Sci. 2021, 278, 119527. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Behnam Azad, B.; Nimmagadda, S. Chapter Two—The Intricate Role of CXCR4 in Cancer. In Advances in Cancer Research; Pomper, M.G., Fisher, P.B., Eds.; Emerging Applications of Molecular Imaging to Oncology; Academic Press: Cambridge, MA, USA, 2014; Volume 124, pp. 31–82. [Google Scholar]
- Minotti, G.; Menna, P.; Salvatorelli, E.; Cairo, G.; Gianni, L. Anthracyclines: Molecular Advances and Pharmacologic Developments in Antitumor Activity and Cardiotoxicity. Pharmacol. Rev. 2004, 56, 185–229. [Google Scholar] [CrossRef] [PubMed]
- Narezkina, A.; Nasim, K. Anthracycline Cardiotoxicity. Circ. Heart Fail. 2019, 12, e005910. [Google Scholar] [CrossRef] [PubMed]
- Ajaykumar, C. Overview on the Side Effects of Doxorubicin. In Advances in Precision Medicine Oncology; IntechOpen: London, UK, 2020; ISBN 978-1-83968-868-3. [Google Scholar]
- Doxorubicin. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Li, M.; Wang, L.; Du, J. Clinical Observation of Liposomal Doxorubicin on Liver and Renal Function in Patients with Breast Cancer. Toxicol. Res. 2023, 12, 807–813. [Google Scholar] [CrossRef]
- Salvatorelli, E.; Menna, P.; Minotti, G. Managing Anthracycline-Induced Cardiotoxicity: Beginning with the End in Mind. Future Cardiol. 2015, 11, 363–366. [Google Scholar] [CrossRef]
- Vejpongsa, P.; Yeh, E.T.H. Prevention of Anthracycline-Induced Cardiotoxicity: Challenges and Opportunities. J. Am. Coll. Cardiol. 2014, 64, 938–945. [Google Scholar] [CrossRef]
- Chen, Y.; Shi, S.; Dai, Y. Research Progress of Therapeutic Drugs for Doxorubicin-Induced Cardiomyopathy. Biomed. Pharmacother. Biomedecine Pharmacother. 2022, 156, 113903. [Google Scholar] [CrossRef]
- Reichardt, P.; Tabone, M.-D.; Mora, J.; Morland, B.; Jones, R.L. Risk-Benefit of Dexrazoxane for Preventing Anthracycline-Related Cardiotoxicity: Re-Evaluating the European Labeling. Future Oncol. 2018, 14, 2663–2676. [Google Scholar] [CrossRef]
- Simůnek, T.; Stérba, M.; Popelová, O.; Adamcová, M.; Hrdina, R.; Gersl, V. Anthracycline-Induced Cardiotoxicity: Overview of Studies Examining the Roles of Oxidative Stress and Free Cellular Iron. Pharmacol. Rep. 2009, 61, 154–171. [Google Scholar] [CrossRef]
- Milic, V.; Dragojevic, V. Doxorubicin-Induced Oxidative Injury of Cardiomyocytes—Do We Have Right Strategies for Prevention? In Cardiotoxicity of Oncologic Treatments; Fiuza, M., Ed.; InTech: London, UK, 2012; ISBN 978-953-51-0273-1. [Google Scholar]
- Jirkovský, E.; Jirkovská, A.; Bavlovič-Piskáčková, H.; Skalická, V.; Pokorná, Z.; Karabanovich, G.; Kollárová-Brázdová, P.; Kubeš, J.; Lenčová-Popelová, O.; Mazurová, Y.; et al. Clinically Translatable Prevention of Anthracycline Cardiotoxicity by Dexrazoxane Is Mediated by Topoisomerase II Beta and Not Metal Chelation. Circ. Heart Fail. 2021, 14, e008209. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, X.; Bawa-Khalfe, T.; Lu, L.-S.; Lyu, Y.L.; Liu, L.F.; Yeh, E.T.H. Identification of the Molecular Basis of Doxorubicin-Induced Cardiotoxicity. Nat. Med. 2012, 18, 1639–1642. [Google Scholar] [CrossRef] [PubMed]
- Ganatra, S.; Nohria, A.; Shah, S.; Groarke, J.D.; Sharma, A.; Venesy, D.; Patten, R.; Gunturu, K.; Zarwan, C.; Neilan, T.G.; et al. Upfront Dexrazoxane for the Reduction of Anthracycline-Induced Cardiotoxicity in Adults with Preexisting Cardiomyopathy and Cancer: A Consecutive Case Series. Cardio Oncol. 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Eneh, C.; Lekkala, M.R. Dexrazoxane. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Nabati, M.; Janbabai, G.; Baghyari, S.; Esmaili, K.; Yazdani, J. Cardioprotective Effects of Carvedilol in Inhibiting Doxorubicin-Induced Cardiotoxicity. J. Cardiovasc. Pharmacol. 2017, 69, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Tashakori Beheshti, A.; Mostafavi Toroghi, H.; Hosseini, G.; Zarifian, A.; Homaei Shandiz, F.; Fazlinezhad, A. Carvedilol Administration Can Prevent Doxorubicin-Induced Cardiotoxicity: A Double-Blind Randomized Trial. Cardiology 2016, 134, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.S.; Ayub-Ferreira, S.M.; de Barros Wanderley, M.R., Jr.; das Dores Cruz, F.; Gonçalves Brandão, S.M.; Rigaud, V.O.C.; Higuchi-dos-Santos, M.H.; Hajjar, L.A.; Filho, R.K.; Hoff, P.M.; et al. Carvedilol for Prevention of Chemotherapy-Related Cardiotoxicity. J. Am. Coll. Cardiol. 2018, 71, 2281–2290. [Google Scholar] [CrossRef] [PubMed]
- Bețiu, A.M.; Noveanu, L.; Hâncu, I.M.; Lascu, A.; Petrescu, L.; Maack, C.; Elmér, E.; Muntean, D.M. Mitochondrial Effects of Common Cardiovascular Medications: The Good, the Bad and the Mixed. Int. J. Mol. Sci. 2022, 23, 13653. [Google Scholar] [CrossRef]
- Szponar, J.; Ciechanski, E.; Ostrowska-Lesko, M.; Gorska, A.; Tchorz, M.; Dabrowska, A.; Dudka, J.; Murias, M.; Kowalczyk, M.; Korga-Plewko, A.; et al. The Lack of Synergy between Carvedilol and the Preventive Effect of Dexrazoxane in the Model of Chronic Anthracycline-Induced Cardiomyopathy. Int. J. Mol. Sci. 2023, 24, 10202. [Google Scholar] [CrossRef]
- Finn, N.A.; Findley, H.W.; Kemp, M.L. A Switching Mechanism in Doxorubicin Bioactivation Can Be Exploited to Control Doxorubicin Toxicity. PLoS Comput. Biol. 2011, 7, e1002151. [Google Scholar] [CrossRef]
- Barata, I.S.; Gomes, B.C.; Rodrigues, A.S.; Rueff, J.; Kranendonk, M.; Esteves, F. The Complex Dynamic of Phase I Drug Metabolism in the Early Stages of Doxorubicin Resistance in Breast Cancer Cells. Genes 2022, 13, 1977. [Google Scholar] [CrossRef]
- Deng, S.; Kruger, A.; Kleschyov, A.L.; Kalinowski, L.; Daiber, A.; Wojnowski, L. Gp91phox-Containing NAD(P)H Oxidase Increases Superoxide Formation by Doxorubicin and NADPH. Free Radic. Biol. Med. 2007, 42, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; McLaughlin, D.; Robinson, E.; Harvey, A.P.; Hookham, M.B.; Shah, A.M.; McDermott, B.J.; Grieve, D.J. Nox2 NADPH Oxidase Promotes Pathologic Cardiac Remodeling Associated with Doxorubicin Chemotherapy. Cancer Res. 2010, 70, 9287–9297. [Google Scholar] [CrossRef] [PubMed]
- Bolaman, Z.; Cicek, C.; Kadikoylu, G.; Barutca, S.; Serter, M.; Yenisey, C.; Alper, G. The Protective Effects of Amifostine on Adriamycin-Induced Acute Cardiotoxicity in Rats. Tohoku J. Exp. Med. 2005, 207, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Fadillioglu, E.; Oztas, E.; Erdogan, H.; Yagmurca, M.; Sogut, S.; Ucar, M.; Irmak, M.K. Protective Effects of Caffeic Acid Phenethyl Ester on Doxorubicin-Induced Cardiotoxicity in Rats. J. Appl. Toxicol. 2004, 24, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Danelisen, I.; Singal, P.K. Early Changes in Myocardial Antioxidant Enzymes in Rats Treated with Adriamycin. Mol. Cell. Biochem. 2002, 232, 19–26. [Google Scholar] [CrossRef]
- Tadokoro, T.; Ikeda, M.; Ide, T.; Deguchi, H.; Ikeda, S.; Okabe, K.; Ishikita, A.; Matsushima, S.; Koumura, T.; Yamada, K.; et al. Mitochondria-Dependent Ferroptosis Plays a Pivotal Role in Doxorubicin Cardiotoxicity. JCI Insight 2020, 5, e132747. [Google Scholar] [CrossRef]
- Dozic, S.; Howden, E.J.; Bell, J.R.; Mellor, K.M.; Delbridge, L.M.D.; Weeks, K.L. Cellular Mechanisms Mediating Exercise-Induced Protection against Cardiotoxic Anthracycline Cancer Therapy. Cells 2023, 12, 1312. [Google Scholar] [CrossRef]
- Wu, B.B.; Leung, K.T.; Poon, E.N.-Y. Mitochondrial-Targeted Therapy for Doxorubicin-Induced Cardiotoxicity. Int. J. Mol. Sci. 2022, 23, 1912. [Google Scholar] [CrossRef]
- Sripetchwandee, J.; KenKnight, S.B.; Sanit, J.; Chattipakorn, S.; Chattipakorn, N. Blockade of Mitochondrial Calcium Uniporter Prevents Cardiac Mitochondrial Dysfunction Caused by Iron Overload. Acta Physiol. 2014, 210, 330–341. [Google Scholar] [CrossRef]
- Vela, D. Keeping Heart Homeostasis in Check through the Balance of Iron Metabolism. Acta Physiol. 2020, 228, e13324. [Google Scholar] [CrossRef]
- Gulati, V.; Harikrishnan, P.; Palaniswamy, C.; Aronow, W.S.; Jain, D.; Frishman, W.H. Cardiac Involvement in Hemochromatosis. Cardiol. Rev. 2014, 22, 56–68. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week of Study | Study Group | ||||
|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | |
| 0 | 208.00 ± 12.31 | 206.60 ± 11.12 | 205.50 ± 11.91 | 204.66 ± 10.77 | 205.70 ± 22.67 |
| 1 | 234.80 ± 13.52 | 237.40 ± 16.58 | 230.80 ± 11.57 | 229.80 ± 13.56 | 230.20 ± 28.10 |
| 2 | 273.40 ± 18.99 | 271.60 ± 20.27 | 262.10 ± 18.62 | 258.20 ± 17.51 | 261.20 ± 33.81 |
| 3 | 297.10 ± 23.56 | 290.80 ± 20.61 | 275.70 ± 11.40 | 274.90 ± 20.24 | 277.20 ± 28.82 |
| 4 | 313.70 ± 27.20 | 299.80 ± 25.20 | 284.30 ± 22.54 | 286.30 ± 21.70 | 301.90 ± 28.21 |
| 5 | 331.70 ± 26.18 | 320.50 ± 33.68 | 301.20 ± 18.88 | 295.60 ± 20.50 | 305.00 ± 35.96 |
| 6 | 342.90 ± 28.63 | 316.40 ± 26.31 | 306.55 ± 14.73 | 297.20 ± 20.00 | 319.60 ± 27.90 |
| 7 | 355.40 ± 29.01 | 336.30 ± 33.70 | 312.10 ± 20.02 | 299.90 ± 21.71 | 337.30 ± 24.98 |
| 8 | 362.80 ± 28.11 | 326.50 ± 25.09 | 316.55 ± 21.70 | 311.80 ± 21.76 * | 330.30 ± 29.48 |
| 9 | 364.60 ± 37.81 | 331.10 ± 24.11 | 322.60 ± 20.31 | 320.90 ± 20.94 * | 338.70 ± 30.27 |
| 10 | 378.90 ± 31.13 | 331.00 ± 17.18 | 321.20 ± 17.93 | 317.70 ± 21.63 * | 334.33 ± 30.46 |
| 11 | 394.60 ± 33.41 | 331.20 ± 13.61 * | 324.30 ± 16.94 * | 323.60 ± 23.66 * | 336.00 ± 19.42 * |
| 21 | 540.50 ± 42.21 | 477.10 ± 24.23 * | 418.90 ± 22.56 *,# | 439.50 ± 28.74 * | 444.30 ± 27.32 * |
| The Differences in Body Weight | Study Group | ||||
|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | |
| Δ = T11–T0 | 186.6 ± 33.8 | 127.0 ± 13.49 * | 118.6 ± 10.7 * | 117.3 ± 21.36 * | 126.7 ± 14.1 * |
| Δ = T21–T11 | 145.9 ± 10.7 | 108.6 ± 7.75 * | 94.6 ± 6.89 * | 115.9 ± 12.84 * | 108.3 ± 11.45 * |
| Biochemical Parameter | Week of the Study | Study Group | ||||
|---|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | ||
| NADPH2 [µM] | 11 | 1.00 ± 0.19 | 0.51 ± 0.12 * | 0.59 ± 0.11 * | 0.69 ± 0.15 * | 1.55 ± 0.73 # |
| 21 | 1.33 ± 0.37 | 0.83 ± 0.17 * | 0.55 ± 0.22 * | 0.29 ± 0.13 * | 0.30 ± 0.29 *,# | |
| NADP+ [µM] | 11 | 0.51 ± 0.12 | 0.47 ± 0.16 | 0.39 ± 0.19 | 0.60 ± 0.17 | 0.62 ± 0.44 |
| 21 | 0.96 ± 0.42 | 0.80 ± 0.27 | 0.82 ± 0.43 | 0.42 ± 0.48 | 0.55 ± 0.28 | |
| Ratio of NADPH2/NADP+ | 11 | 1.72 ± 0.34 | 1.02 ± 0.40 | 2.30 ± 2.17 | 1.05 ± 0.33 * | 1.86 ± 1.20 |
| 21 | 1.29 ± 0.32 | 1.03 ± 0.45 | 0.89 ± 0.72 | 0.69 ± 0.33 * | 0.70 ± 0.33 | |
| oxDNA [number/100kbp] | 11 | 0.50 ± 0.16 | 1.02 ± 0.49 | 2.66 ± 0.84 *,# | 3.42 ± 1.60 *,# | 2.30 ± 0.86 * |
| 21 | 0.62 ± 0.13 | 1.76 ± 0.69 * | 1.32 ± 0.79 | 1.18 ± 0.32 * | 1.54 ± 0.52 * | |
| LPO [µM MDA] | 11 | 7.54 ± 1.91 | 1.18 ± 0.66 * | 0.96 ± 0.32 * | 1.18 ± 0.66 * | 0.63 ± 0.31 * |
| 21 | 7.26 ± 1.23 | 3.77 ± 1.91 * | 2.22 ± 1.61 * | 4.92 ± 2.88 | 2.50 ± 1.94 * | |
| Biochemical Parameter | Time | Study Group | ||||
|---|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | ||
| AST [IU/L] | 11 | 63.24 ± 14.85 | 77.96 ± 21.90 | 60.09 ± 10.14 | 59.52 ± 9.38 | 68.74 ± 20.03 |
| 21 | 51.75 ± 6.32 | 63.40 ± 14.77 | 49.82 ± 10.38 | 51.35 ± 14.01 | 42.22 ± 11.63 | |
| ALT [IU/L] | 11 | 15.97 ± 2.19 | 21.78 ± 3.21 | 17.98 ± 2.09 | 17.94 ± 1.99 | 21.08 ± 3.26 |
| 21 | 15.27 ± 1.27 | 19.29 ± 4.44 | 16.59 ± 1.93 | 16.37 ± 3.58 | 20.73 ± 7.62 | |
| Albumin [g/dL] | 11 | 3.27 ± 0.37 | 3.47 ± 0.17 | 3.92 ± 0.46 | 3.70 ± 0.26 | 3.93 ± 0.31 |
| 21 | 3.36 ± 0.48 | 3.12 ± 0.38 | 3.11 ± 0.62 | 3.00 ± 0.40 | 3.24 ± 0.91 | |
| Biochemical Parameter | Time | Study Group | ||||
|---|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | ||
| Iron (Fe) [µg/dL] | 11 | 124.75 ± 10.11 | 105.16 ± 8.73 * | 96.04 ± 12.65 * | 95.54 ± 11.18 * | 99.109 ± 12.91 * |
| 21 | 121.75 ± 9.42 | 106.30 ± 15.50 | 103.55 ± 17.89 | 96.84 ± 9.51 * | 101.84 ± 32.76 | |
| Transferrin [mg/dL] | 11 | 424 ± 260 | 1049 ± 142 * | 898 ± 228 | 1059 ± 183* | 1033 ± 228 * |
| 21 | 516 ± 326 | 559 ± 209 | 507 ± 329 | 1040 ± 219 *,#,† | 636 ± 149 | |
| Ferritin [µg/L] | 11 | 3482 ± 1068 | 3740 ± 676 | 3918 ± 1325 | 3733 ± 1853 | 4317 ± 1426 |
| 21 | 3112 ± 931 | 2607 ± 550 | 2736 ± 1217 | 2380 ± 670 | 1732 ± 641 | |
| Gene | Week of the Study | Study Group | ||||
|---|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | ||
| Sod2 | 11 | 1.01 ± 0.18 | 0.67 ± 0.11 * | 1.92 ± 0.25 *,# | 0.71 ± 0.08 *,† | 1.52 ± 0.20 *,# |
| 21 | 1.02 ± 0.22 | 0.85 ± 0.10 | 0.92 ± 0.12 | 0.84 ± 0.12 | 1.32 ± 0.17 # | |
| Cat | 11 | 1.05 ± 0.25 | 6.77 ± 1.86 * | 32.29 ± 8.72 *,# | 8.02 ± 2.34 *,† | 21.96 ± 5.76 *,# |
| 21 | 1.01 ± 0.29 | 1.43 ± 0.38 | 1.07 ± 0.22 | 1.39 ± 0.43 | 1.67 ± 0.45 | |
| Morphological Feature | Week of the Study | Study Group | ||||
|---|---|---|---|---|---|---|
| CTR | DOX | DOX + DEX | DOX + DEX + CVD | DOX + CVD | ||
| Glycogen accumulation | 11 | + (7) | +++ (10) | - | ++(7) | + (8) |
| 21 | + (7) | - | - | + (7) | + (7) | |
| Foci of inflammatory cells | 11 | - | + (9) | - | + (6) | + (8) |
| 21 | - | + (10) | - | ++ (8) | + (9) | |
| Single cell death (apoptosis) | 11 | - | + (6) | - | - | - |
| 21 | - | - | - | + (5) | - | |
| Necrosis | 11 | - | + (6) | - | - | ++ (7) |
| 21 | - | - | - | - | - | |
| Symbol of Group | Type of Group | Administration |
|---|---|---|
| CTR | Control (n = 20) | 0.01 mL 0.9% NaCl per g body weight IP administration once a week for 10 weeks; |
| DOX | Experimental (n = 20) | 1.6 mg DOX per kg of body weight IP administration once a week for 10 weeks; |
| DOX + DEX + CVD | Experimental (n = 20) | 1 mg CVD per kg of body weight IP administration 30 min prior DOX; 25 mg DEX per kg of body weight IP administration 30 min prior DOX; 1.6 mg DOX per kg of body weight IP administration once a week for 10 weeks; |
| DOX + DEX | Experimental (n = 20) | 1.6 mg DOX per kg of body weight IP administration once a week for 10 weeks; 25 mg DEX per kg of body weight IP administration 30 min prior DOX; |
| DOX + CVD | Experimental (n = 20) | 1.6 mg DOX per kg of body weight IP administration once a week for 10 weeks; 1 mg CVD per kg of body weight IP administration 30 min prior DOX. |
| Gene Name | Gene Symbol | Primer Sequence (5′ → 3′) | NCBI Reference Sequence | |
|---|---|---|---|---|
| Left | Right | |||
| Catalase | Cat | ACA TGG TCT GGG ACT TCT GG | CAA GTT TTT GAT GCC CTG GT | NM_012520.2 |
| Superoxide dismutase 2 | Sod2 | CAC TGT GGC TGA GCT GTT GT | TCC AAG CAA TTC AAG CCT CT | NM_017051.2 |
| Ribosomal Protein L32 | Rpl32 | AGA TTC AAG GGC CAG ATC CT | CGA TGG CTT TTC GGT TCT TA | NM_013226 |
| TATA box binding protein | Tbp | CCT CTG AGA GCT CTG GGA TTG TA | GCC AAG ATT CAC GGT GGA TAC A | NM_001004198.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szponar, J.; Gorska, A.; Ostrowska-Lesko, M.; Korga-Plewko, A.; Tchorz, M.; Ciechanski, E.; Dabrowska, A.; Poleszak, E.; Burdan, F.; Dudka, J.; et al. Assessment of the Impact of Carvedilol Administered Together with Dexrazoxan and Doxorubicin on Liver Structure and Function, Iron Metabolism, and Myocardial Redox System in Rats. Int. J. Mol. Sci. 2024, 25, 2219. https://doi.org/10.3390/ijms25042219
Szponar J, Gorska A, Ostrowska-Lesko M, Korga-Plewko A, Tchorz M, Ciechanski E, Dabrowska A, Poleszak E, Burdan F, Dudka J, et al. Assessment of the Impact of Carvedilol Administered Together with Dexrazoxan and Doxorubicin on Liver Structure and Function, Iron Metabolism, and Myocardial Redox System in Rats. International Journal of Molecular Sciences. 2024; 25(4):2219. https://doi.org/10.3390/ijms25042219
Chicago/Turabian StyleSzponar, Jaroslaw, Agnieszka Gorska, Marta Ostrowska-Lesko, Agnieszka Korga-Plewko, Michal Tchorz, Erwin Ciechanski, Anna Dabrowska, Ewa Poleszak, Franciszek Burdan, Jaroslaw Dudka, and et al. 2024. "Assessment of the Impact of Carvedilol Administered Together with Dexrazoxan and Doxorubicin on Liver Structure and Function, Iron Metabolism, and Myocardial Redox System in Rats" International Journal of Molecular Sciences 25, no. 4: 2219. https://doi.org/10.3390/ijms25042219
APA StyleSzponar, J., Gorska, A., Ostrowska-Lesko, M., Korga-Plewko, A., Tchorz, M., Ciechanski, E., Dabrowska, A., Poleszak, E., Burdan, F., Dudka, J., Murias, M., & Mandziuk, S. (2024). Assessment of the Impact of Carvedilol Administered Together with Dexrazoxan and Doxorubicin on Liver Structure and Function, Iron Metabolism, and Myocardial Redox System in Rats. International Journal of Molecular Sciences, 25(4), 2219. https://doi.org/10.3390/ijms25042219