
Identification of a Panel of miRNAs Associated with Resistance to Palbociclib and Endocrine Therapy

 , , , and
, , , and 
Abstract
1. Introduction
2. Results
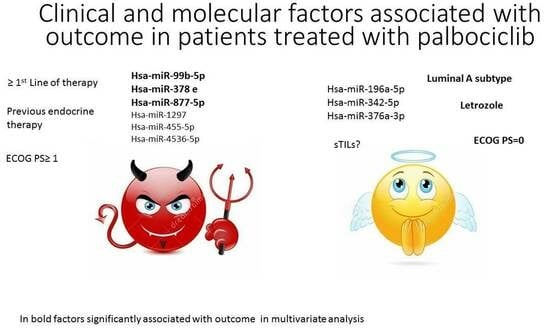
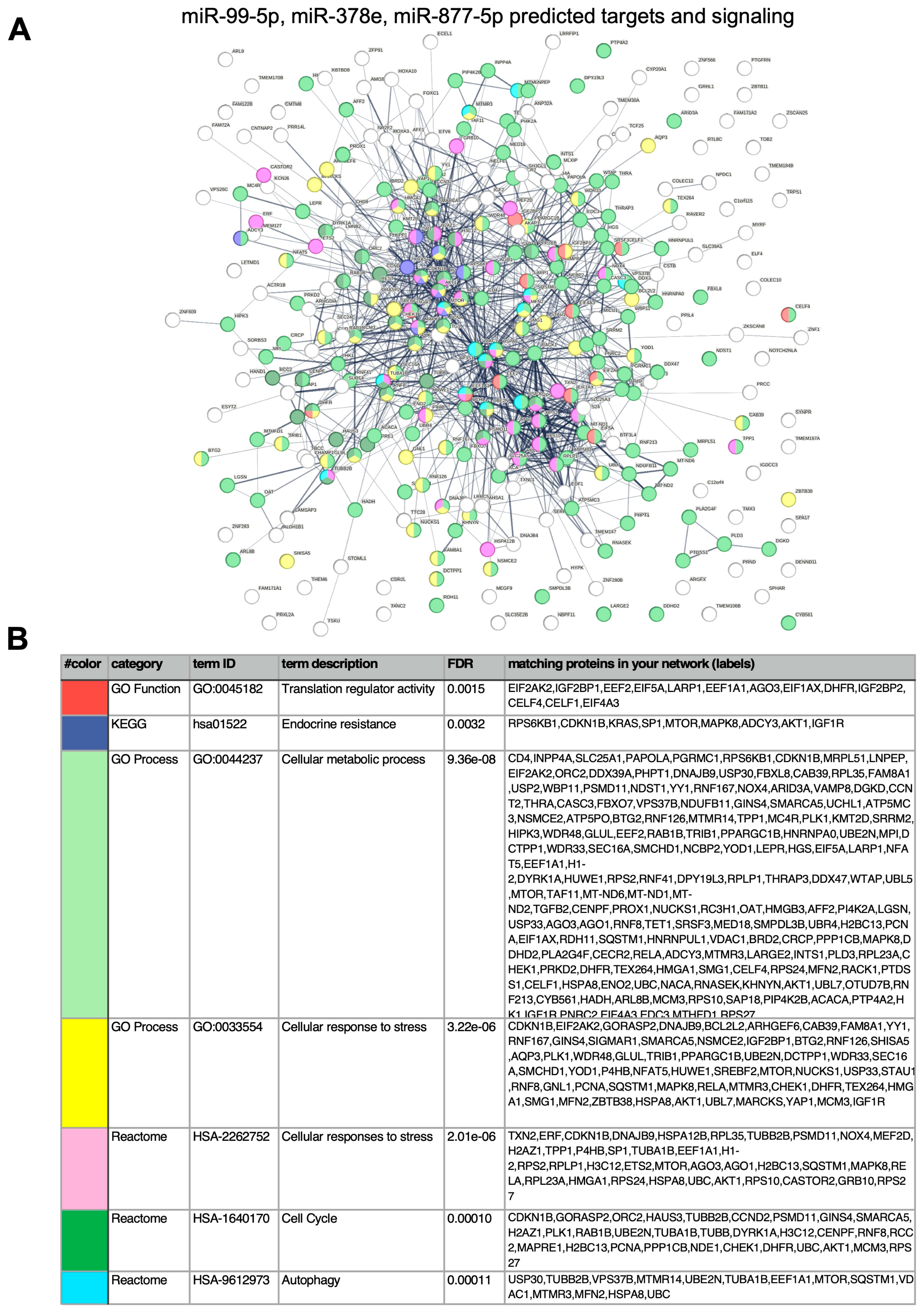
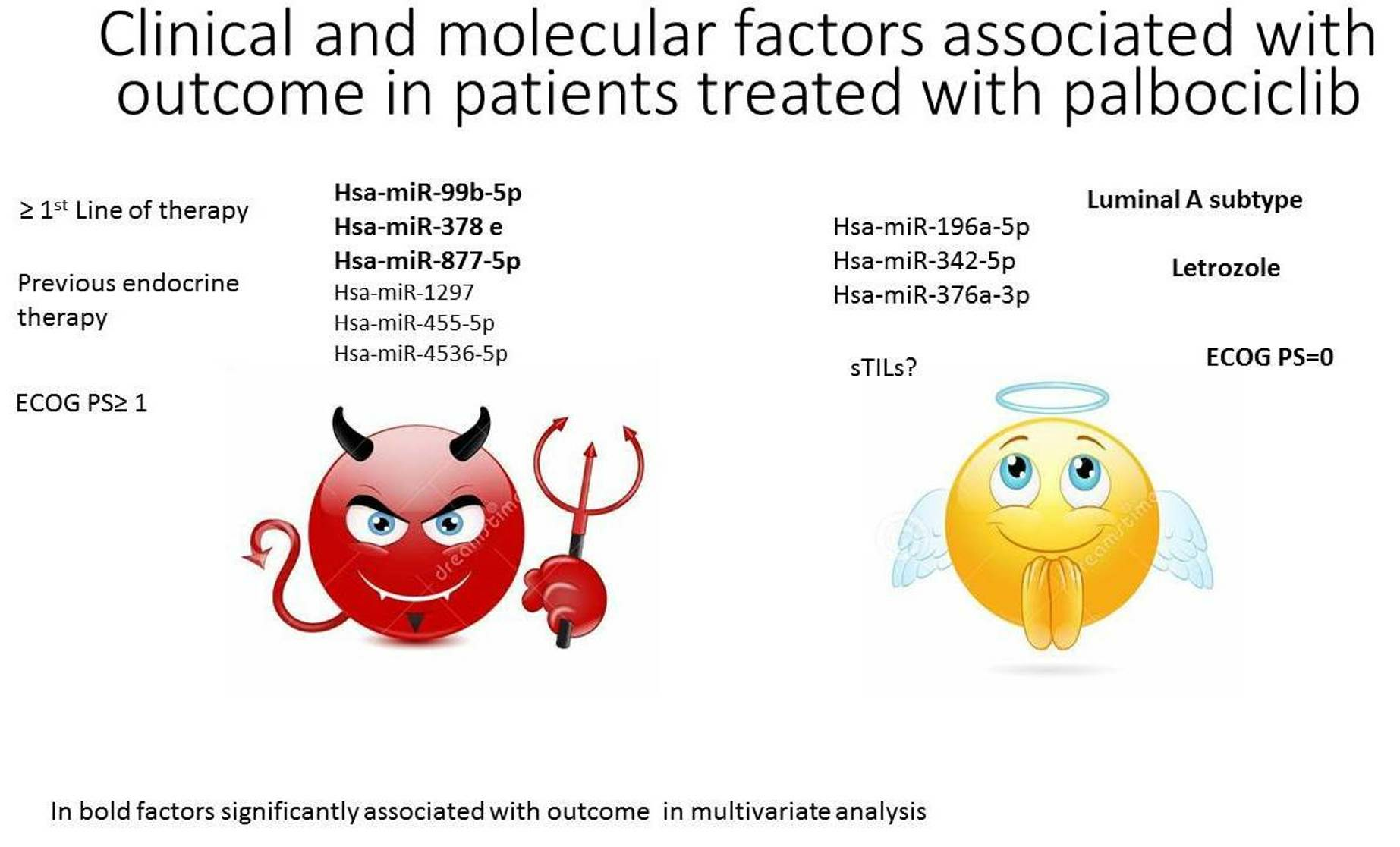
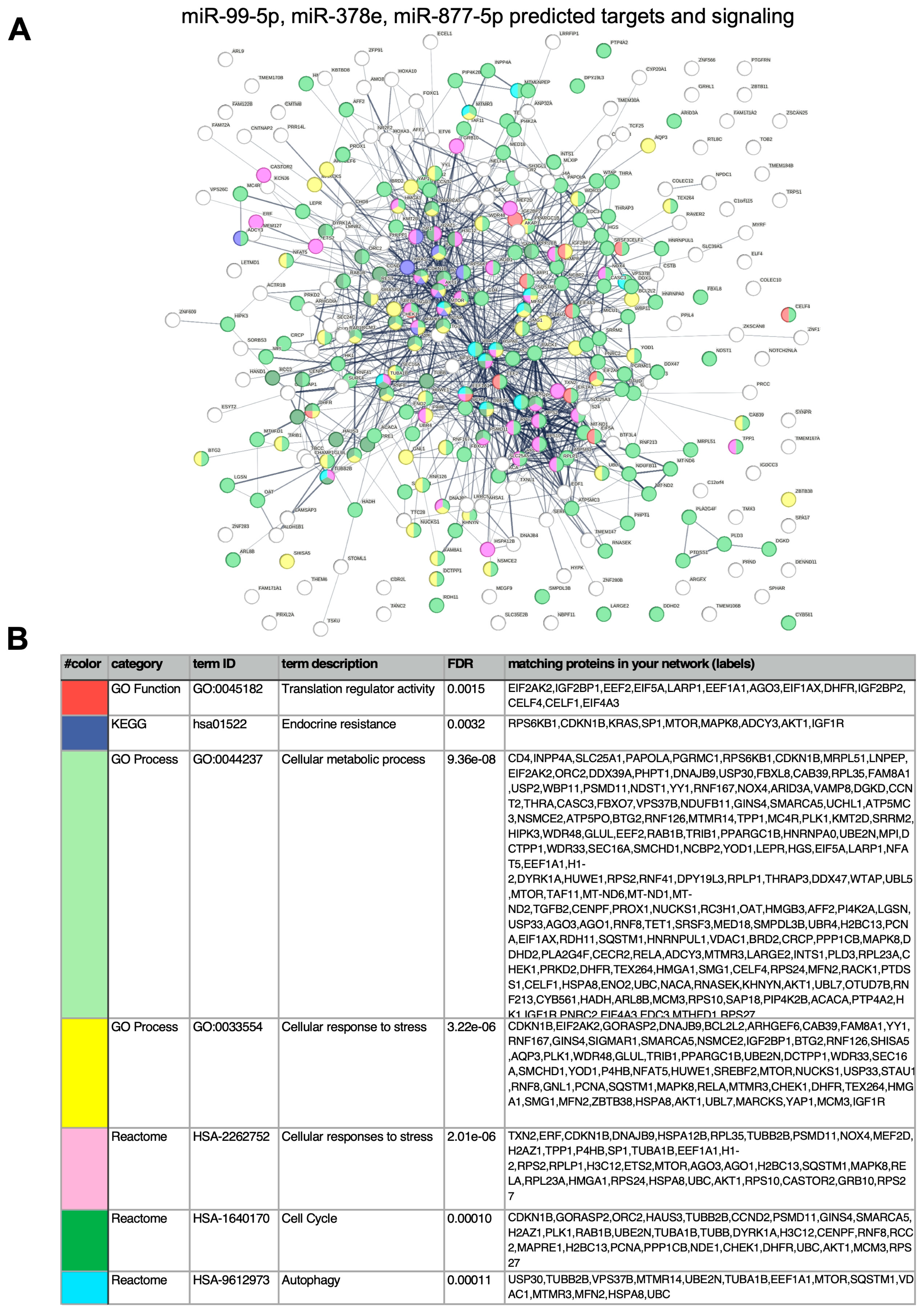
miRNA Analyses
3. Discussion
4. Materials and Methods
4.1. miRNA Analyses
4.2. sTILs Analyses
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.; Cronin, K.A. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl. Cancer Inst. 2014, 106, dju055. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall survival with Ribociclib plus Letrozole in advanced breast cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Neven, P.; Chia, S.; Jerusalem, G.; De Laurentiis, M.; Im, S.; Petrakova, K.; Bianchi, G.V.; Martín, M.; Nusch, A.; et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: Updated overall survival. Ann. Oncol. 2021, 32, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.-S.; Im, S.-A.; Colleoni, M.; Franke, F.; Bardia, A.; Cardoso, F.; Harbeck, N.; Hurvitz, S.; Chow, L.; Sohn, J.; et al. Updated overall survival of ribociclib plus endocrine therapy versus endocrine therapy alone in pre- and Peri-menopausal patients with HRþ/HER2_ advanced breast cancer in MONALEESA-7: A phase III randomized clinical trial. Clin. Cancer Res. 2022, 28, 851–859. [Google Scholar] [CrossRef]
- Rugo, H.S.; Finn, R.S.; Diéras, V.; Ettl, J.; Lipatov, O.; Joy, A.A.; Harbeck, N.; Castrellon, A.; Iyer, S.; Lu, D.R.; et al. Palbociclib plus letrozole as first-line therapy in estrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer with extended follow-up. Breast Cancer Res. Treat. 2019, 174, 719–729. [Google Scholar] [CrossRef]
- Johnston, S.; Martin, M.; Di Leo, A.; Im, S.-A.; Awada, A.; Forrester, T.; Frenzel, M.; Hardebeck, M.C.; Cox, J.; Barriga, S.; et al. MONARCH 3 final PFS: A randomized study of abemaciclib as initial therapy for advanced breast cancer. NPJ Breast Cancer 2019, 5, 5. [Google Scholar] [CrossRef]
- Di Leo, A.; O’Shaughnessy, J.; Sledge, G.W., Jr.; Martin, M.; Lin, Y.; Frenzel, M.; Hardebeck, M.C.; Smith, I.C.; Llombart-Cussac, A.; Goetz, M.P.; et al. Prognostic characteristics in hormone receptor-positive advanced breast cancer and characterization of abemaciclib efficacy. NPJ Breast Cancer. 2018, 4, 41. [Google Scholar] [CrossRef]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Huang, J.; Zheng, L.; Sun, Z.; Li, J. CDK4/6 inhibitor resistance mechanisms and treatment strategies (Review). Int. J. Mol. Med. 2022, 50, 128–140. [Google Scholar] [CrossRef]
- Di Leva, G.; Garofalo, M.; Croce, C.M. MicroRNAs in Cancer. Annu. Rev. Pathol. Mech. Dis. 2014, 9, 287–314. [Google Scholar] [CrossRef]
- Campos-Parra, A.D.; Mitznahuatl, G.C.; Pedroza-Torres, A.; Romo, R.V.; Reyes, F.I.P.; López-Urrutia, E.; Pérez-Plasencia, C. Micro-RNA as potential predictors of response to breast cancer systemic therapy: Future clinical implications. Int. J. Mol. Sci. 2017, 18, 1182. [Google Scholar] [CrossRef] [PubMed]
- Andrikopoulou, A.; Shalit, A.; Zografos, E.; Koutsoukos, K.; Korakiti, A.M.; Liontos, M.; Dimopoulos, M.-A.; Zagouri, F. MicroRNAs as Potential Predictors of Response to CDK4/6 Inhibitor Treatment. Cancers. MicroRNAs as Potential Predictors of Response to CDK4/6 Inhibitor Treatment. Cancers 2021, 13, 4114. [Google Scholar] [CrossRef] [PubMed]
- Cornell, L.; Wander, S.A.; Visal, T.; Wagle, N.; Shapiro, G.I. Micro-RNA-mediated suppression of the TGF-β pathway confers transmissible and reversible CDK 4/6 inhibitor resistance. Cell Rep. 2019, 26, 2667–2680. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommen-dations by an Internationa TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- He, Y.L.; Ying, Y.; Xu, Y.L.; Su, J.F.; Luo, H.; Wang, H.F. Effects of Lycium barbarum polysaccharide on tumor microenvironment T-lymphocyte subsets and dendritic cells in H22-bearing mice. Zhong Xi Yi Jie He Xue Bao J. Chin. Integr. Med. 2005, 3, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Dieci, M.V.; Griguolo, G.; Miglietta, F.; Guarneri, V. The immune system and hormone-receptor positive breast cancer: Is it really a dead end? Cancer Treat. Rev. 2016, 46, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumor-infiltranting lymphocytes and prognosis in different subtypes of breast cancer: A pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018, 19, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, I.; Bonechi, M.; McCartney, A.; Guarducci, C.; Benelli, M.; Biganzoli, L.; Di Leo, A.; Malorni, L. CDK4/6 inhibitors: A focus on biomarkers of response and post-treatment therapeutic strategies in hormone receptor-positive HER2-negative breast cancer. Cancer Treat. Rev. 2021, 93, 102136. [Google Scholar] [CrossRef]
- O’Leary, B.; Cutts, R.J.; Huang, X.; Hrebien, S.; Liu, Y.; André, F.; Loibl, S.; Loi, S.; Garcia-Murillas, I.; Cristofanilli, M.; et al. Circulating tumor DNA markers for early progression on fulvestrant with or without palbociclib in ER+ advanced breast cancer. J. Natl. Cancer Ins. 2021, 113, 309–317. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [CrossRef]
- Eniafe, J.; Jiang, S. Micro-RNA family in cancer and immunity. Wiley Interdiscip Rev. RNA 2021, 12, e1635. [Google Scholar] [CrossRef]
- Gujrati, H.; Ha, S.; Waseem, M.; Wang, B.-D. Downregulation of miR-99b-5p and Upregulation of Nuclear mTOR Cooperatively Promotes the Tumor Aggressiveness and Drug Resistance in African American Prostate Cancer. Int. J. Mol. Sci. 2022, 23, 9643. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.; Tokumaru, Y.; Benesch, M.G.; Sugito, N.; Wu, R.; Yan, L.; Yamada, A.; Chishima, T.; Ishikawa, T.; Endo, I.; et al. High miR-99b expression is associated with cell proliferation and worse patient outcomes in breast cancer. Am. J. Cancer Res. 2022, 12, 4840–4852. [Google Scholar] [PubMed]
- Foruzandeh, Z.; Alivand, M.R.; Ghiami-Rad, M.; Zaefizadeh, M.; Ghorbian, S. Identification and validation of miR-583 and mir-877-5p as biomarkers in patients with breast cancer: An integrated experimental and bioinformatics research. BMC Res. Notes 2023, 16, 72. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Dai, H.; Li, X.; Guo, L.; Sun, X.; Zheng, Z.; Xu, C. LncRNA TRG-AS1 inhibits bone metastasis of breast cancer by the miR-877–5p/WISP2 axis. Pathol. Res. Pract. 2023, 243, 154360. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Huang, Z.; Tian, S.; Chen, Y.; Yuan, Y.; Yuan, J.; Zou, X.; Zhou, F. MicroRNA-877-5p alleviates ARDS via enhancing PI3K/Akt path by targeting CDKN1B both in vivo and in vitro. Int. Immunopharmacol. 2021, 95, 107530. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Zhu, C.; Liu, Y.; Muckenhuber, A.; Bronger, H.; Scorilas, A.; Kiechle, M.; Dorn, J.; Magdolen, V.; Dreyer, T.; et al. Elevated levels of both microRNA 378 (miR-378) and kallikrein-related peptidase 4 (KLK4) mRNA are associated with an unfavorable prognosis in triple-negative breast cancer. Am. J. Transl. Res. 2021, 13, 1594–1606. [Google Scholar] [PubMed]
- Cocco, S.; Leone, A.; Piezzo, M.; Caputo, R.; Di Lauro, V.; Di Rella, F.; Fusco, G.; Capozzi, M.; di Gioia, G.; Budillon, A.; et al. Targeting Autophagy in Breast Cancer. Int. J. Mol. Sci. 2020, 21, 7836. [Google Scholar] [CrossRef]
- Wen, N.; Lv, Q.; Du, Z.-G. MicroRNAs involved in drug resistance of breast cancer by regulating autophagy. J. Zhejiang Univ. Sci. B 2020, 21, 690–702. [Google Scholar] [CrossRef]
- Vijayaraghavan, S.; Karakas, C.; Doostan, I.; Chen, X.; Bui, T.; Yi, M.; Raghavendra, A.S.; Zhao, Y.; Bashour, S.I.; Ibrahim, N.K.; et al. CDK4/6 and Autophagy Inhibitors Synergistically Induce Senescence in Rb Positive Cytoplasmic Cyclin E Negative Cancers. Nat. Commun. 2017, 8, 15916. [Google Scholar] [CrossRef]
- Lanceta, L.; O’Neill, C.; Lypova, N.; Li, X.; Rouchka, E.; Waigel, S.; Gomez-Gutierrez, J.G.; Chesney, J.; Imbert-Fernandez, Y. Transcriptomic Profiling Identifies Differentially Expressed Genes in Palbociclib-Resistant ER+ MCF7 Breast Cancer Cells. Genes 2020, 11, 467. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, Z.; Li, X.; Tang, X.; He, J.; Lu, S. MicroRNA-1297 contributes to tumor growth of human breast cancer by targeting PTEN/PI3K/AKT signaling. Oncol. Rep. 2017, 38, 2435–2443. [Google Scholar] [CrossRef] [PubMed]
- Aili, T.; Paizula, X.; Ayoufu, A. miR-455-5p promotes cell invasion and migration in breast cancer. Mol. Med. Rep. 2018, 17, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Torrisi, R.; Jacobs, F.; Miggiano, C.; De Sanctis, R.; Santoro, A. HR+/HER2– de novo metastatic breast cancer: A true peculiar entity? Drugs Context 2023, 12, 2022-12-2. [Google Scholar] [CrossRef] [PubMed]
- mRNA Vaccine Slows Melanoma Recurrence. Cancer Discov. 2023, 13, 1278. [CrossRef] [PubMed]
- Torrisi, R.; Vaira, V.; Giordano, L.; Destro, A.; Basilico, V.; Mazzara, S.; Salvini, P.; Gaudioso, G.; Fernandes, B.; Rudini, N.; et al. Predictors of fulvestrant long-term benefit in hormone receptor-positive/HER2 negative advanced breast cancer. Sci. Rep. 2022, 12, 12789. [Google Scholar] [CrossRef] [PubMed]
- Kern, F.; Aparicio-Puerta, E.; Li, Y.; Fehlmann, T.; Kehl, T.; Wagner, V.; Ray, K.; Ludwig, N.; Lenhof, H.-P.; Meese, E.; et al. miRTargetLink 2.0—Interactive miRNA target gene and target pathway networks. Nucleic Acids Res. 2021, 49, W409–W416. [Google Scholar] [CrossRef] [PubMed]
- Szklarczyk, D.; Kirsch, R.; Koutrouli, M.; Nastou, K.; Mehryary, F.; Hachilif, R.; Gable, A.L.; Fang, T.; Doncheva, N.T.; Pyysalo, S.; et al. The STRING database in 2023: Protein–protein association networks and functional enrichment analyses for any sequenced genome of interest. Nucleic Acids Res. 2023, 51, D638–D646. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Age in years, median (range) | 64.5 | (33–84) |
| Menopausal status | ||
| Pre/peri-menopausal | 7 | 13.5 |
| Post-menopausal | 44 | 84.6 |
| Not applicable | 1 | 1.9 |
| Occurrence of MBC | ||
| De novo | 13 | 25 |
| rMBC | 39 | 75 |
| PgR% (biopsy) | ||
| High (≥50%) | 18 | 34.6 |
| Low (10–49%) | 13 | 25 |
| Negative (<10%) | 21 | 40.4 |
| Ki67% (biopsy) | ||
| ≤20 | 35 | 67.3 |
| >20 | 16 | 30.8 |
| Unknown | 1 | 1.9 |
| Tumor subtype | ||
| Luminal A | 27 | 51.9 |
| Luminal B | 25 | 48.1 |
| Metastatic sites (number) | ||
| ≤2 | 28 | 53.9 |
| >2 | 24 | 46.1 |
| Metastatic sites | ||
| Bone | 26 | 50 |
| Visceral | 33 | 63.5 |
| Other | 38 | 73.1 |
| Endocrine resistance | ||
| Endocrine naïve * | 11 | 21.2 |
| Endocrine sensitive ** | 23 | 44.2 |
| Endocrine resistance primary | 2 | 3.8 |
| Endocrine resistance secondary | 16 | 30.8 |
| Prior lines of therapy for metastatic disease | ||
| 0 | 41 | 78.8 |
| 1 | 6 | 11.5 |
| ≥2 | 5 | 9.6 |
| Endocrine therapy | ||
| Letrozole | 29 | 55.8 |
| Fulvestrant | 23 | 44.2 |
| ECOG Performance status | ||
| 0 | 35 | 67.3 |
| ≥1 | 17 | 32.7 |
| Dose reduction | ||
| No | 27 | 51.9 |
| yes | 24 | 46.2 |
| unknown | 1 | 1.9 |
| N | mPFS Months (95% CI) | p-Value | |
|---|---|---|---|
| Overall. | 52 | 20.8 (12.6–21.6) | |
| Menopausal status, n | |||
| Pre/peri-menopausal | 7 | 25.4 (3.4–NR) | |
| Post-menopausal | 44 | 20.9 (12.4–36) | NS |
| Not applicable | 1 | - | |
| Occurence of MBC | |||
| De novo | 13 | 23.8 (15.8-NR) | |
| Recurrent | 39 | 18 (8.7–36.2) | NS |
| Tumor subtype (biopsy), n | |||
| Luminal A | 27 | 31.6 (15.8–NR) | |
| Luminal B | 25 | 16.6 (5.1–23.8) | <0.05 |
| Ki67% (biopsy) | |||
| ≤20 | 35 | 25.4 (12.4–36.2) | |
| >20 | 16 | 18.4 (4.2–28.3) | NS |
| Unknown | 1 | - | |
| Metastatic sites | |||
| Visceral | 33 | 19.4 (8.5–31.6) | |
| Non visceral | 19 | 36.2 (12.4–NR) | NS |
| Metastatic sites (number) | |||
| ≤2 | 28 | 23.8 (15.8–36) | |
| >2 | 24 | 16.8 (5.8–NR) | NS |
| Endocrine therapy | |||
| Letrozole | 29 | 31.6 (18–NR) | |
| Fulvestrant | 23 | 8.7 (5.1–19) | <0.005 |
| Prior lines of therapy for metastatic disease | |||
| 0 | 41 | 25.4 (16.6–36.4) | |
| ≥1 | 11 | 8.5 (3.1–17.6) | <0.005 |
| Endocrine resistance | |||
| Endocrine naive * | 11 | 28.3 (15.8–NR) | |
| Endocrine sensitive ** | 23 | 36.2 (12.4–NR) | |
| Endocrine resistant | 16 | 8.5 (3.5–19) | <0.05 |
| sTILs | |||
| Negative | 35 | 19 (8.7–25.4) | |
| Positive | 15 | 36 (3.5–NR) | NS |
| Unknown | 2 | - | |
| ECOG Performance Status | |||
| 0 | 35 | 25.4 (16–36.4) | |
| ≥1 | 17 | 12.6 (4.2–20.9) | NS |
| PFS | ≥18 Months PFS | <6 Months PFS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| mmirRNA | HR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value |
| miR-216a-5p | 1.025 | 1.000–1.051 | 0.053 | 0.951 | 0.910–0.994 | 0.026 | |||
| miR-378e | 1.017 | 1.001–1.032 | 0.034 | 0.961 | 0.929–0.994 | 0.022 | 1.060 | 1.019–1.102 | 0.004 |
| miR-1233–3p | 1.011 | 1.003–1.019 | 0.009 | 0.989 | 0.975–1.002 | 0.097 | |||
| miR-99b-5p | 1.004 | 1.001–1.008 | 0.013 | 0.993 | 0.986–1.000 | 0.046 | 1.009 | 1.002–1.017 | 0.014 |
| miR-1260b | 1.002 | 1.001–1.004 | 0.015 | 0.994 | 0.989–1.000 | 0.034 | |||
| miR-448 | 1.038 | 1.003–1.075 | 0.032 | ||||||
| miR-1252–5p | 1.029 | 1.001–1.058 | 0.041 | ||||||
| miR-324–3p | 1.027 | 1.001–1.053 | 0.04 | ||||||
| miR-132–3p | 1.004 | 1.000–1.008 | 0.050 | ||||||
| miR-19a-3p | 0.991 | 0.981–1.001 | 0.067 | ||||||
| miR-196a-5p | 1.001 | 1.000–1.001 | 0.023 | ||||||
| miR-342–5p | 1.057 | 1.001–1.116 | 0.046 | ||||||
| miR-410–3p | 0.902 | 0.808–1.006 | 0.064 | ||||||
| miR-3161 | 1.067 | 0.944–1.144 | 0.071 | ||||||
| miR-424–5p | 1.002 | 1.000–1.003 | 0.070 | ||||||
| miR-1297 | 1.013 | 1.001–1.026 | 0.041 | ||||||
| miR-877–5p | 1.065 | 1.005–1.129 | 0.032 | ||||||
| miR-4536-5p | 1.050 | 1.007–1.096 | 0.023 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| ECOG PS (≥1 vs. 0) | 3.90 | 1.40–10.93 | 0.010 |
| Endocrine agent (Fulvestrant vs. letrozole) | 2.94 | 1.25–6.94 | 0.014 |
| Tumor subtype (Luminal A vs. B) | 0.25 | 0.10–0.66 | 0.005 |
| miR-410-3p | 1.05 | 1.00–1.10 | 0.041 |
| miR-448 | 1.06 | 1.00–1.13 | 0.035 |
| miR-1252-5p | 1.03 | 1.00–1.06 | 0.047 |
| miR-216a-5p | 1.03 | 1.00–1.06 | 0.047 |
| miR-335-5p | 0.98 | 0.97–1.00 | 0.048 |
| miR-1260b | 1.00 | 1.00–1.01 | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torrisi, R.; Vaira, V.; Giordano, L.; Fernandes, B.; Saltalamacchia, G.; Palumbo, R.; Carnaghi, C.; Basilico, V.; Gentile, F.; Masci, G.; et al. Identification of a Panel of miRNAs Associated with Resistance to Palbociclib and Endocrine Therapy. Int. J. Mol. Sci. 2024, 25, 1498. https://doi.org/10.3390/ijms25031498
Torrisi R, Vaira V, Giordano L, Fernandes B, Saltalamacchia G, Palumbo R, Carnaghi C, Basilico V, Gentile F, Masci G, et al. Identification of a Panel of miRNAs Associated with Resistance to Palbociclib and Endocrine Therapy. International Journal of Molecular Sciences. 2024; 25(3):1498. https://doi.org/10.3390/ijms25031498
Chicago/Turabian StyleTorrisi, Rosalba, Valentina Vaira, Laura Giordano, Bethania Fernandes, Giuseppe Saltalamacchia, Raffaella Palumbo, Carlo Carnaghi, Vera Basilico, Francesco Gentile, Giovanna Masci, and et al. 2024. "Identification of a Panel of miRNAs Associated with Resistance to Palbociclib and Endocrine Therapy" International Journal of Molecular Sciences 25, no. 3: 1498. https://doi.org/10.3390/ijms25031498
APA StyleTorrisi, R., Vaira, V., Giordano, L., Fernandes, B., Saltalamacchia, G., Palumbo, R., Carnaghi, C., Basilico, V., Gentile, F., Masci, G., De Sanctis, R., & Santoro, A. (2024). Identification of a Panel of miRNAs Associated with Resistance to Palbociclib and Endocrine Therapy. International Journal of Molecular Sciences, 25(3), 1498. https://doi.org/10.3390/ijms25031498