

Vitamin D/Bone Mineral Density and Triglyceride Paradoxes Seen in African Americans: A Cross-Sectional Study and Review of the Literature
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
4.1. Rationale behind the Use of 25(OH)VD to Total Serum TG Ratio
4.2. Brief Overview of Vitamin D Metabolism and Function
4.3. Possible Explanations for the Vitamin D and BMD Paradox in AA
4.3.1. Genetic Polymorphism and Vitamin D Binding Protein
4.3.2. Optimal Vitamin D Levels
4.3.3. Skeletal Resistance to PTH
4.3.4. Calcium Economy
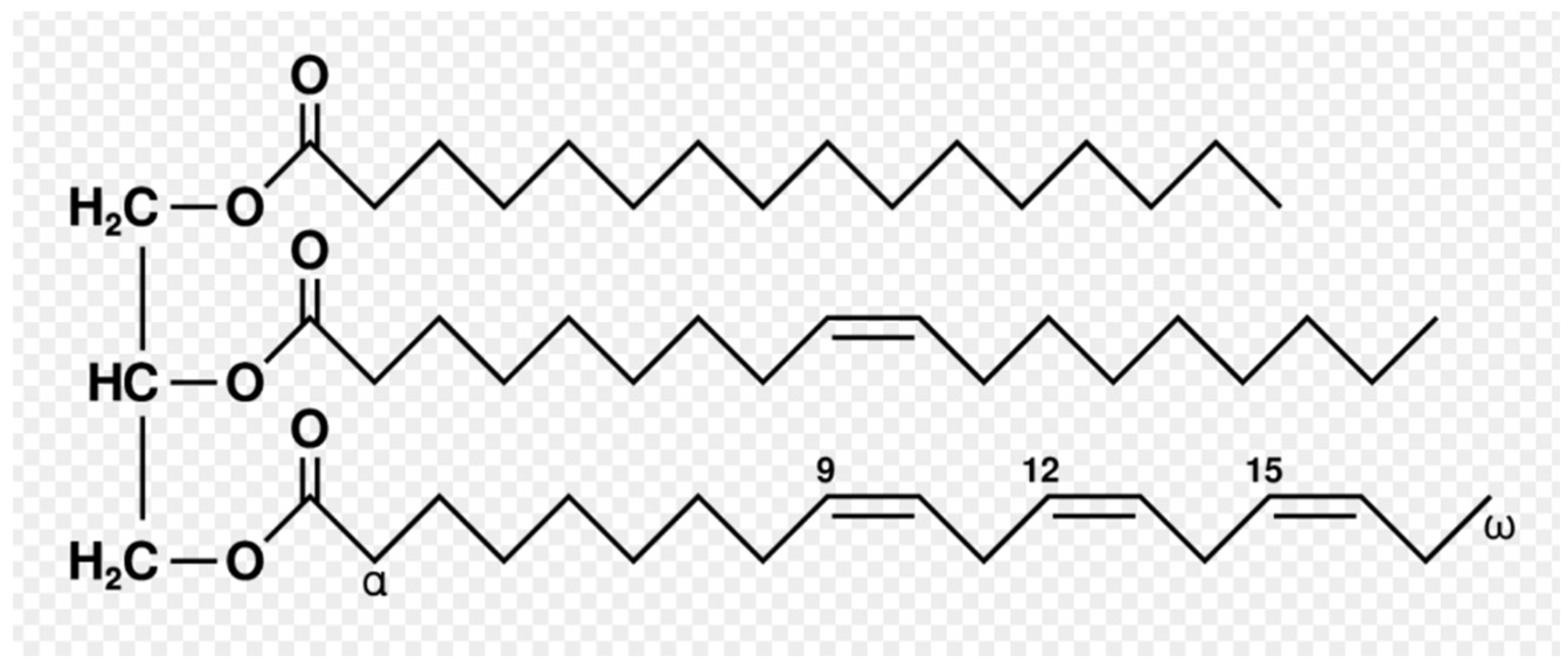
4.4. Brief Overview of Triglyceride Metabolism and Function
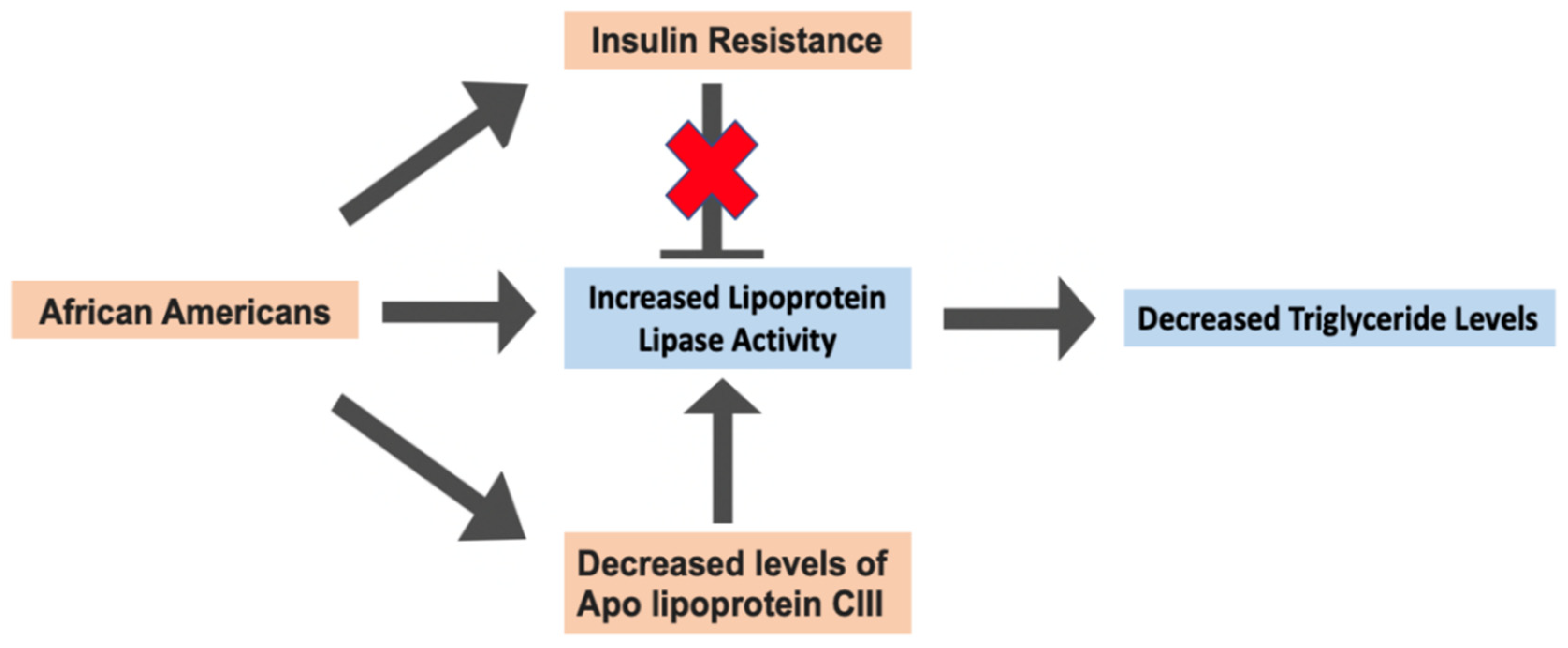
4.5. Possible Explanations for the Triglyceride Paradox in AA
4.6. Our First Novel Hypothesis: Could the Paradoxical Relationships Be Linked to Each Other?
4.7. Our Second Novel Hypothesis: Could Racial Differences in Estrogen Levels Be Responsible for the Vitamin D/BMD Paradox?
4.8. Our Third Novel Hypothesis: Could Racial Differences in Hydrogen Sulfide Levels Be a Potential Factor in the Vitamin D/BMD Paradox?
4.9. Our Fourth Novel Hypothesis: HMG-CoA Reductase as a Possible Contributor to the Triglyceride Paradox
4.10. Why Is Studying These Paradoxical Relationships Important?
5. Limitations of the Study
6. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Hofmann, B. The paradox of health care. Health Care Anal. 2001, 9, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Ames, B.N.; Grant, W.B.; Willett, W.C. Does the High Prevalence of Vitamin D Deficiency in African Americans Contribute to Health Disparities? Nutrients 2021, 13, 499. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.M.; Solway, J. Association of Vitamin D Levels, Race/Ethnicity, and Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open 2021, 4, e214117. [Google Scholar] [CrossRef] [PubMed]
- Varghese, S.B.; Benoit, J.; McIntyre, T. Vitamin D Levels in Ethnic Minority Adolescents in Primary Care. J. Pediatr. Health Care 2022, 36, 443–448. [Google Scholar] [CrossRef]
- Qiu, S.; Divine, G.; Rao, S.D. Effect of vitamin D metabolites on bone histomorphometry in healthy black and white women: An attempt to unravel the so-called vitamin D paradox in blacks. Bone Rep. 2023, 18, 101650. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.L.; Cohen, B.; Tabor, D.; Zappalà, G.; Maruvada, P.; Coates, P.M. The vitamin D paradox in Black Americans: A systems-based approach to investigating clinical practice, research, and public health—Expert panel meeting report. BMC Proc. 2018, 12 (Suppl. 6), 6. [Google Scholar] [CrossRef] [PubMed]
- Yellapragada, S.V.; Fillmore, N.R.; Frolov, A.; Zhou, Y.; Dev, P.; Yameen, H.; Ifeorah, C.; Do, N.V.; Brophy, M.T.; Munshi, N.C. Vitamin D deficiency predicts for poor overall survival in white but not African American patients with multiple myeloma. Blood Adv. 2020, 4, 1643–1646. [Google Scholar] [CrossRef]
- Vieth, R. Weaker bones and white skin as adaptions to improve anthropological “fitness” for northern environments. Osteoporos. Int. 2020, 31, 617–624. [Google Scholar] [CrossRef]
- Shieh, A.; Aloia, J.F. Assessing Vitamin D Status in African Americans and the Influence of Vitamin D on Skeletal Health Parameters. Endocrinol. Metab. Clin. North Am. 2017, 46, 135–152. [Google Scholar] [CrossRef]
- Yu, S.S.; Castillo, D.C.; Courville, A.B.; Sumner, A.E. The triglyceride paradox in people of African descent. Metab. Syndr. Relat. Disord. 2012, 10, 77–82. [Google Scholar] [CrossRef]
- Goedecke, J.H. Expanding Our Understanding of the Triglyceride Paradox in Populations of African Ancestry. Circ. Res. 2020, 126, 109–111. [Google Scholar] [CrossRef]
- Meeks, K.A.C.; Bentley, A.R.; Agyemang, C.; Galenkamp, H.; Born, B.-J.H.v.D.; Hanssen, N.M.; Doumatey, A.P.; Adeyemo, A.A.; Rotimi, C.N. Ancestral and environmental patterns in the association between triglycerides and other cardiometabolic risk factors. EBioMedicine 2023, 91, 104548. [Google Scholar] [CrossRef]
- Bentley, A.R.; Rotimi, C.N. Interethnic Differences in Serum Lipids and Implications for Cardiometabolic Disease Risk in African Ancestry Populations. Glob. Heart 2017, 12, 141–150. [Google Scholar] [CrossRef]
- Gao, Y.; Chen, Z.; Ma, Z. Vitamin D is Positively Associated with Bone Mineral Density Muscle Mass and Negatively with Insulin Resistance in Senile Diabetes Mellitus. Dis. Markers 2022, 2022, 9231408. [Google Scholar] [CrossRef]
- Zhang, J.; Li, Y.; Lai, D.; Lu, D.; Lan, Z.; Kang, J.; Xu, Y.; Cai, S. Vitamin D Status Is Negatively Related to Insulin Resistance and Bone Turnover in Chinese Non-Osteoporosis Patients With Type 2 Diabetes: A Retrospective Cross-Section Research. Front. Public. Health 2021, 9, 727132. [Google Scholar] [CrossRef]
- Tirosh, A.; Shai, I.; Bitzur, R.; Kochba, I.; Tekes-Manova, D.; Israeli, E.; Shochat, T.; Rudich, A. Changes in triglyceride levels over time and risk of type 2 diabetes in young men. Diabetes Care 2008, 31, 2032–2037. [Google Scholar] [CrossRef]
- Jain, S.K.; Kahlon, G.; Morehead, L.; Dhawan, R.; Lieblong, B.; Stapleton, T.; Caldito, G.; Hoeldtke, R.; Levine, S.N.; Bass, P.F. Effect of chromium dinicocysteinate supplementation on circulating levels of insulin, TNF-alpha, oxidative stress, and insulin resistance in type 2 diabetic subjects: Randomized, double-blind, placebo-controlled study. Mol. Nutr. Food Res. 2012, 56, 1333–1341. [Google Scholar] [CrossRef]
- Karanchi, H.; Muppidi, V.; Wyne, K. Hypertriglyceridemia; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Rygiel, K. Hypertriglyceridemia—Common Causes, Prevention and Treatment Strategies. Curr. Cardiol. Rev. 2018, 14, 67–76. [Google Scholar] [CrossRef]
- Rychter, A.M.; Hryhorowicz, S.; Słomski, R.; Dobrowolska, A.; Krela-Kaźmierczak, I. Antioxidant effects of vitamin E and risk of cardiovascular disease in women with obesity—A narrative review. Clin. Nutr. 2022, 41, 1557–1565. [Google Scholar] [CrossRef]
- Jain, S.K.; Wise, R.; Yanamandra, K.; Dhanireddy, R.; Bocchini, J.A. The effect of maternal and cord-blood vitamin C, vitamin E and lipid peroxide levels on newborn birth weight. Mol. Cell Biochem. 2008, 309, 217–221. [Google Scholar] [CrossRef]
- Jain, S.K.; McVie, R.; Smith, T. Vitamin E supplementation restores glutathione and malondialdehyde to normal concentrations in erythrocytes of type 1 diabetic children. Diabetes Care 2000, 23, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Ogbera, A.O.; Ezeobi, E.; Unachukwu, C.; Oshinaike, O. Treatment of diabetes mellitus-associated neuropathy with vitamin E and Eve primrose. Indian. J. Endocrinol. Metab. 2014, 18, 846–849. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Li, R.; Chen, D.; Hu, J.; Chen, Y.; Xu, C.; Wen, Z. Protective Effects of Vitamin E on Chemotherapy-Induced Peripheral Neuropathy: A Meta-Analysis of Randomized Controlled Trials. Ann. Nutr. Metab. 2021, 77, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Pace, A.; Giannarelli, D.; Galie, E.; Savarese, A.; Carpano, S.; Della Giulia, M.; Pozzi, A.; Silvani, A.; Gaviani, P.; Scaioli, V.; et al. Vitamin E neuroprotection for cisplatin neuropathy: A randomized, placebo-controlled trial. Neurology 2010, 74, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Chroni, E.; Koutras, A.; Ellul, J.; Papapetropoulos, S.; Katsoulas, G.; Iconomou, G.; Kalofonos, H.P. Vitamin E for prophylaxis against chemotherapy-induced neuropathy: A randomized controlled trial. Neurology 2005, 64, 26–31. [Google Scholar] [CrossRef]
- Anoushirvani, A.A.; Poorsaadat, L.; Aghabozorgi, R.; Kasravi, M. Comparison of the Effects of Omega 3 and Vitamin E on Palcitaxel-Induced Peripheral Neuropathy. Open Access Maced. J. Med. Sci. 2018, 6, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Chroni, E.; Koutras, A.; Iconomou, G.; Papapetropoulos, S.; Polychronopoulos, P.; Kalofonos, H.P. Preventing paclitaxel-induced peripheral neuropathy: A phase II trial of vitamin E supplementation. J. Pain. Symptom Manag. 2006, 32, 237–244. [Google Scholar] [CrossRef]
- Eum, S.; Choi, H.-D.; Chang, M.-J.; Choi, H.-C.; Ko, Y.-J.; Ahn, J.-S.; Shin, W.-G.; Lee, J.-Y. Protective effects of vitamin E on chemotherapy-induced peripheral neuropathy: A meta-analysis of randomized controlled trials. Int. J. Vitam. Nutr. Res. 2013, 83, 101–111. [Google Scholar] [CrossRef]
- Farrell, P.M.; Mischler, E.H.; Gutcher, G.R. Evaluation of vitamin E deficiency in children with lung disease. Ann. N. Y Acad. Sci. 1982, 393, 96–108. [Google Scholar] [CrossRef]
- Heubi, J.E.; Sokol, R.J.; McGraw, C.A. Comparison of total serum lipids measured by two methods. J. Pediatr. Gastroenterol. Nutr. 1990, 10, 468–472. [Google Scholar]
- Laditan, A.A.; Ette, S.I. Plasma alpha-tocopherol (vitamin E) levels and tocopherol-lipid ratio among children with protein-energy malnutrition (PEM). Ann. Trop. Paediatr. 1982, 2, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, Y.; Pincemail, J.; Hanique, G.; Denis, B.; Leenaerts, L.; Vankeerberghen, L.; Deby, C. Differences in tocopherol-lipid ratios in ARDS and non-ARDS patients. Intensive Care Med. 1989, 15, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Sokol, R.J.; Heubi, J.E.; Iannaccone, S.T.; Bove, K.E.; Balistreri, W.F. Vitamin E deficiency with normal serum vitamin E concentrations in children with chronic cholestasis. N. Engl. J. Med. 1984, 310, 1209–1212. [Google Scholar] [CrossRef] [PubMed]
- Horwitt, M.K.; Harvey, C.C.; Dahm, C.H.; Searcy, M.T. Relationship between tocopherol and serum lipid levels for determination of nutritional adequacy. Ann. N. Y. Acad. Sci. 1972, 203, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Krueger, K.S.; McVie, R.; Jaramillo, J.J.; Palmer, M.; Smith, T. Relationship of blood thromboxane-B2 (TxB2) with lipid peroxides and effect of vitamin E and placebo supplementation on TxB2 and lipid peroxide levels in type 1 diabetic patients. Diabetes Care 1998, 21, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; McVie, R.; Jaramillo, J.J.; Palmer, M.; Smith, T. Effect of modest vitamin E supplementation on blood glycated hemoglobin and triglyceride levels and red cell indices in type I diabetic patients. J. Am. Coll. Nutr. 1996, 15, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Wise, R. Relationship between elevated lipid peroxides, vitamin E deficiency and hypertension in preeclampsia. Mol. Cell Biochem. 1995, 151, 33–38. [Google Scholar] [CrossRef]
- Barebring, L.; Amberntsson, A.; Augustin, H. A validated screening tool correctly identifies the majority of pregnant women at high risk of vitamin D deficiency. Clin. Nutr. ESPEN 2022, 49, 301–306. [Google Scholar] [CrossRef]
- de la Guia-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef]
- Kapala, A.; Szlendak, M.; Grochowska, E. Cross-sectional observational study—Investigation of vitamin D concentration in Caucasian cancer patients. What is the adequate dose of vitamin D for these patients? Clin. Nutr. 2021, 40, 3852–3858. [Google Scholar] [CrossRef]
- Takase, T.; Tsugawa, N.; Sugiyama, T.; Ikesue, H.; Eto, M.; Hashida, T.; Tomii, K.; Muroi, N. Association between 25-hydroxyvitamin D levels and COVID-19 severity. Clin. Nutr. ESPEN 2022, 49, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Bizzaro, G.; Antico, A.; Fortunato, A.; Bizzaro, N. Vitamin D and Autoimmune Diseases: Is Vitamin D Receptor (VDR) Polymorphism the Culprit? Isr. Med. Assoc. J. 2017, 19, 438–443. [Google Scholar] [PubMed]
- Jean, G.; Souberbielle, J.C.; Chazo, C. Vitamin D in Chronic Kidney Disease and Dialysis Patients. Nutrients 2017, 9, 328. [Google Scholar] [CrossRef] [PubMed]
- de la Puente Yague, M.; Yurrita, L.C.; Cabañas, M.J.C.; Cenzual, M.A.C. Role of Vitamin D in Athletes and Their Performance: Current Concepts and New Trends. Nutrients 2020, 12, 579. [Google Scholar] [CrossRef] [PubMed]
- Khazai, N.; Judd, S.E.; Tangpricha, V. Calcium and vitamin D: Skeletal and extraskeletal health. Curr. Rheumatol. Rep. 2008, 10, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Uenishi, K. Phosphorus intake and bone health. Clin. Calcium. 2009, 19, 1822–1828. [Google Scholar] [PubMed]
- Cashman, K.D. Calcium intake, calcium bioavailability and bone health. Br. J. Nutr. 2002, 87 (Suppl. 2), S169–S177. [Google Scholar] [CrossRef]
- Fukumoto, S. Phosphate metabolism and vitamin D. Bonekey Rep. 2014, 3, 497. [Google Scholar] [CrossRef]
- Wasserman, R. Vitamin D and the Intestinal Absorption of Calcium: A View and Overview; Elsevier Acad. Press: San Diego, CA, USA, 2005; Chapter 24; pp. 411–428. [Google Scholar]
- Bouillon, R.; Norman, A.W.; Lips, P. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar]
- Khan, M.; Jose, A.; Sharma, S. Physiology, Parathyroid Hormone; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Powe, C.E.; Evans, M.K.; Wenger, J.; Zonderman, A.B.; Berg, A.H.; Nalls, M.; Tamez, H.; Zhang, D.; Bhan, I.; Karumanchi, S.A.; et al. Vitamin D-binding protein and vitamin D status of black Americans and white Americans. N. Engl. J. Med. 2013, 369, 1991–2000. [Google Scholar] [CrossRef]
- Powe, C.E.; Ricciardi, C.; Berg, A.H.; Erdenesanaa, D.; Collerone, G.; Ankers, E.; Wenger, J.; Karumanchi, S.A.; Thadhani, R.; Bhan, I. Vitamin D-binding protein modifies the vitamin D-bone mineral density relationship. J. Bone Miner. Res. 2011, 26, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.M.; Henao, M.P.; Finkelstein, J.S.; Burnett-Bowie, S.A.M. Prevalence and predictors of vitamin D deficiency in healthy adults. Endocr. Pract. 2012, 18, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, O.M.; Farwell, W.R.; Kermah, D.; Taylor, E.N. Racial differences in the relationship between vitamin D, bone mineral density, and parathyroid hormone in the National Health and Nutrition Examination Survey. Osteoporos. Int. 2011, 22, 1745–1753. [Google Scholar] [CrossRef]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Wright, N.C.; Chen, L.; Niu, J.; Neogi, T.; Javiad, K.; Nevitt, M.A.; Lewis, C.E.; Curtis, J.R. Defining physiologically “normal” vitamin D in African Americans. Osteoporos. Int. 2012, 23, 2283–2291. [Google Scholar] [CrossRef] [PubMed]
- Sizar, O.; Khare, S.; Goyal, A.; Givler, A. Vitamin D Deficiency; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cauley, J.A.; Danielson, M.E.; Boudreau, R.; Barbour, K.E.; Horwitz, M.J.; Bauer, D.C.; Ensrud, K.E.; Manson, J.E.; Wactawski-Wende, J.; Shikany, J.M.; et al. Serum 25-hydroxyvitamin D and clinical fracture risk in a multiethnic cohort of women: The Women’s Health Initiative (WHI). J. Bone Miner. Res. 2011, 26, 2378–2388. [Google Scholar] [CrossRef]
- Aloia, J.F. African Americans, 25-hydroxyvitamin D, and osteoporosis: A paradox. Am. J. Clin. Nutr. 2008, 88, 545S–550S. [Google Scholar] [CrossRef]
- Cosman, F.; Morgan, D.C.; Nieves, J.W.; Shen, V.; Luckey, M.M.; Dempster, D.W.; Lindsay, R.; Parisien, M. Resistance to bone resorbing effects of PTH in black women. J. Bone Miner. Res. 1997, 12, 958–966. [Google Scholar] [CrossRef]
- Cosman, F.; Shen, V.; Morgan, D.; Gordon, S.; Parisien, M.; Nieves, J.; Lindsay, R. Biochemical responses of bone metabolism to 1,25-dihydroxyvitamin D administration in black and white women. Osteoporos. Int. 2000, 11, 271–277. [Google Scholar] [CrossRef]
- Valcour, A.; Blocki, F.; Hawkins, D.M.; Rao, S.D. Effects of age and serum 25-OH-vitamin D on serum parathyroid hormone levels. J. Clin. Endocrinol. Metab. 2012, 97, 3989–3995. [Google Scholar] [CrossRef]
- Heaney, R.P. Ethnicity, bone status, and the calcium requirement. Nutr. Res. 2002, 22, 153–178. [Google Scholar] [CrossRef]
- Aloia, J.; Mikhail, M.; Dhaliwal, R.; Shieh, A.; Usera, G.; Stolberg, A.; Ragolia, L.; Islam, S. Free 25(OH)D and the Vitamin D Paradox in African Americans. J. Clin. Endocrinol. Metab. 2015, 100, 3356–3363, Erratum in J. Clin. Endocrinol. Metab. 2016, 101, 3250. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.J.; Wastney, M.E.; Martin, B.R.; Wood, O.; McCabe, G.P.; Morshidi, M.; Smith, D.L.; Peacock, M.; Weaver, C.M. Racial differences in bone turnover and calcium metabolism in adolescent females. J. Clin. Endocrinol. Metab. 2003, 88, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Bell, N.H.; Yergey, A.L.; Vieira, N.E.; Oexmann, M.J.; Shary, J.R. Demonstration of a difference in urinary calcium, not calcium absorption, in black and white adolescents. J. Bone Miner. Res. 1993, 8, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Abrams, S.A.; O’Brien, K.O.; Liang, L.K.; Stuff, J.E. Differences in calcium absorption and kinetics between black and white girls aged 5–16 years. J. Bone Miner. Res. 1995, 10, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Mendez, A.; Álvarez-Delgado, C.; Hernández-Godinez, D.; Fernandez-Mejia, C. Hepatic diseases related to triglyceride metabolism. Mini Rev. Med. Chem. 2013, 13, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Demignot, S.; Beilstein, F.; Morel, E. Triglyceride-rich lipoproteins and cytosolic lipid droplets in enterocytes: Key players in intestinal physiology and metabolic disorders. Biochimie 2014, 96, 48–55. [Google Scholar] [CrossRef]
- Pirahanchi, Y.; Anoruo, M.; Sharma, S. Biochemistry, Lipoprotein Lipase; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Despres, J.P.; Couillard, C.; Gagnon, J.; Bergeron, J.; Leon, A.S.; Rao, D.C.; Skinner, J.S.; Wilmore, J.H.; Bouchard, C. Race, visceral adipose tissue, plasma lipids, and lipoprotein lipase activity in men and women: The Health, Risk Factors, Exercise Training, and Genetics (HERITAGE) family study. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1932–1938. [Google Scholar] [CrossRef]
- Chung, S.T.; Cravalho, C.K.; Meyers, A.G.; Courville, A.B.; Yang, S.; Matthan, N.R.; Mabundo, L.; Sampson, M.; Ouwerkerk, R.; Gharib, A.M.; et al. Triglyceride Paradox Is Related to Lipoprotein Size, Visceral Adiposity and Stearoyl-CoA Desaturase Activity in Black Versus White Women. Circ. Res. 2020, 126, 94–108. [Google Scholar] [CrossRef]
- Florez, H.; Mendez, A.; Casanova-Romero, P.; Larreal-Urdaneta, C.; Castillo-Florez, S.; Lee, D.; Goldberg, R. Increased apolipoprotein C-III levels associated with insulin resistance contribute to dyslipidemia in normoglycemic and diabetic subjects from a triethnic population. Atherosclerosis 2006, 188, 134–141. [Google Scholar] [CrossRef]
- Sumner, A.E.; Vega, G.L.; Genovese, D.J.; Finley, K.B.; Bergman, R.N.; Boston, R.C. Normal triglyceride levels despite insulin resistance in African Americans: Role of lipoprotein lipase. Metabolism 2005, 54, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.A. Evolutionary Origins of the Differences in Osteoporosis Risk in US Populations. J. Clin. Densitom. 2019, 22, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Speeckaert, M.M.; Taes, Y.E.; De Buyzere, M.L.; Christophe, A.B.; Kaufman, J.-M.; Delanghe, J.R. Investigation of the potential association of vitamin D binding protein with lipoproteins. Ann. Clin. Biochem. 2010, 47, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Speeckaert, M.M.; Wehlou, C.; Vandewalle, S.; Taes, Y.E.; Robberecht, E.; Delanghe, J.R. Vitamin D binding protein, a new nutritional marker in cystic fibrosis patients. Clin. Chem. Lab. Med. 2008, 46, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Parsanathan, R.; Jain, S.K. Hydrogen Sulfide Regulates Irisin and Glucose Metabolism in Myotubes and Muscle of HFD-Fed Diabetic Mice. Antioxidants 2022, 11, 1369. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Manna, P.; Micinski, D.; Lieblong, B.J.; Kahlon, G.; Morehead, L.; Hoeldtke, R.; Bass, P.F., 3rd; Levine, S.N. In African American type 2 diabetic patients, is vitamin D deficiency associated with lower blood levels of hydrogen sulfide and cyclic adenosine monophosphate, and elevated oxidative stress? Antioxid. Redox. Signal 2013, 18, 1154–1158. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, S.; Katikaneni, P.; Deshotels, M.; Pardue, S.; Glawe, J.; Shen, X.; Akkus, N.; Modi, K.; Bhandari, R.; Dominic, P.; et al. Total sulfane sulfur bioavailability reflects ethnic and gender disparities in cardiovascular disease. Redox Biol. 2018, 15, 480–489. [Google Scholar] [CrossRef]
- Dominic, P.; Ahmad, J.; Bhandari, R.; Pardue, S.; Solorzano, J.; Jaisingh, K.; Watts, M.; Bailey, S.R.; Orr, A.W.; Kevil, C.G.; et al. Decreased availability of nitric oxide and hydrogen sulfide is a hallmark of COVID-19. Redox Biol. 2021, 43, 101982. [Google Scholar] [CrossRef]
- Jain, S.K.; McLean, W.E.; Stevens, C.M.; Dhawan, R. The Positive Association of Plasma Levels of Vitamin C and Inverse Association of VCAM-1 and Total Adiponectin with Bone Mineral Density in Subjects with Diabetes. Nutrients 2022, 14, 3893. [Google Scholar] [CrossRef]
- Peng, X.D.; Xie, H.; Zhao, Q.; Wu, X.-P.; Sun, Z.-Q.; Liao, E.-Y. Relationships between serum adiponectin, leptin, resistin, visfatin levels and bone mineral density, and bone biochemical markers in Chinese men. Clin. Chim. Acta 2008, 387, 31–35. [Google Scholar] [CrossRef]
- Nakamura, Y.; Nakano, M.; Suzuki, T.; Sato, J.; Kato, H.; Takahashi, J.; Shiraki, M. Two adipocytokines, leptin and adiponectin, independently predict osteoporotic fracture risk at different bone sites in postmenopausal women. Bone 2020, 137, 115404. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Micinski, D.; Lieblong, B.J.; Stapleton, T. Relationship between hydrogen sulfide levels and HDL-cholesterol, adiponectin, and potassium levels in the blood of healthy subjects. Atherosclerosis 2012, 225, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.M.; He, D.-W.; Gao, Y.; Fang, L.-N.; Zhang, P.-P.; Lu, K.; Lu, R.-Z.; Li, C. Association of Hydrogen Sulfide with Femoral Bone Mineral Density in Osteoporosis Patients: A Preliminary Study. Med. Sci. Monit. 2021, 27, e929389. [Google Scholar] [CrossRef]
- Hao, Y.; Wang, H.; Fang, L.; Bian, J.; Gao, Y.; Li, C. H2S Donor and Bone Metabolism. Front. Pharmacol. 2021, 12, 661601. [Google Scholar] [CrossRef] [PubMed]
- Behera, J.; George, A.K.; Voor, M.J.; Tyagi, S.C.; Tyagi, N. Hydrogen sulfide epigenetically mitigates bone loss through OPG/RANKL regulation during hyperhomocysteinemia in mice. Bone 2018, 114, 90–108. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, R.; Liu, X.; Zhou, Y.; Qu, C.; Kikuiri, T.; Wang, S.; Zandi, E.; Du, J.; Ambudkar, I.S.; et al. Hydrogen sulfide maintains mesenchymal stem cell function and bone homeostasis via regulation of Ca(2+) channel sulfhydration. Cell Stem Cell 2014, 15, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen YD, I.; Li, X.; Post, W.; Herrington, D.; Polak, J.F.; Rotter, J.I.; Taylor, K.D. The HMG-CoA reductase gene and lipid and lipoprotein levels: The multi-ethnic study of atherosclerosis. Lipids 2009, 44, 733–743. [Google Scholar] [CrossRef]
- Rooney, M.R.; Harnack, L.; Michos, E.D.; Ogilvie, R.P.; Sempos, C.T.; Lutsey, P.L. Trends in Use of High-Dose Vitamin D Supplements Exceeding 1000 or 4000 International Units Daily, 1999–2014. J. Am. Med. Assoc. 2017, 317, 2448–2450. [Google Scholar] [CrossRef]
- Mishra, S.; Stierman, B.; Gahche, J.J.; Potischman, N. Dietary Supplement Use Among Adults: United States, 2017–2018; NCHS Data Brief; NCHS: Atlanta, GA, USA, 2021; pp. 1–8.
- Parikh, R.M.; Mohan, V. Changing definitions of metabolic syndrome. Indian. J. Endocrinol. Metab. 2012, 16, 7–12. [Google Scholar] [CrossRef]
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation; Part 1, Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999.
- Balkau, B.; Charles, M.A. Comment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistance (EGIR). Diabet. Med. 1999, 16, 442–443. [Google Scholar]
- National Institutes of Health. National Institutes of Health Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III); Executive Summary; Lung, and Blood Institute: Bethesda, MD, USA, 2001.
- Einhorn, D. American College of Endocrinology position statement on the insulin resistance syndrome. Endocr. Pract. 2003, 9, 237–252. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Sumner, A.E.; Cowie, C.C. Ethnic differences in the ability of triglyceride levels to identify insulin resistance. Atherosclerosis 2008, 196, 696–703. [Google Scholar] [CrossRef]
- Sumner, A.E.; Finley, K.B.; Genovese, D.J.; Criqui, M.H.; Boston, R.C. Fasting triglyceride and the triglyceride-HDL cholesterol ratio are not markers of insulin resistance in African Americans. Arch. Intern. Med. 2005, 165, 1395–1400. [Google Scholar] [CrossRef]
- Sumner, A.E. “Half the dsylipidemia of insulin resistance” is the dyslipidemia [corrected] of insulin-resistant Blacks. Ethn. Dis. 2009, 19, 462–465. [Google Scholar]
- Goedecke, J.H.; Utzschneider, K.; Faulenbach, M.V.; Rizzo, M.; Berneis, K.; Spinas, G.A.; Dave, J.A.; Levitt, N.S.; Lambert, E.V.; Olsson, T.; et al. Ethnic differences in serum lipoproteins and their determinants in South African women. Metabolism 2010, 59, 1341–1350. [Google Scholar] [CrossRef]
- Ervin, R.B. Prevalence of Metabolic Syndrome among Adults 20 Years of Age and Over, by Sex, Age, Race and Ethnicity, and Body Mass Index: United States, 2003–2006; National Health Statistics Reports; DHHS: Cincinnati, OH, USA, 2009; pp. 1–7. [Google Scholar]
- Park, Y.W.; Zhu, S.; Palaniappan, L.; Heshka, S.; Carnethon, M.R.; Heymsfield, S.B. The metabolic syndrome: Prevalence and associated risk factor findings in the US population from the Third National Health and Nutrition Examination Survey, 1988–1994. Arch. Intern. Med. 2003, 163, 427–436. [Google Scholar] [CrossRef]
- Gaillard, T.R. The Metabolic Syndrome and Its Components in African-American Women: Emerging Trends and Implications. Front. Endocrinol. 2017, 8, 383. [Google Scholar] [CrossRef]
- Sun, L.; Yuan, J.-L.; Chen, Q.-C.; Xiao, W.-K.; Ma, G.-P.; Liang, J.-H.; Chen, X.-K.; Wang, S.; Zhou, X.-X.; Wu, H.; et al. Red meat consumption and risk for dyslipidaemia and inflammation: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 996467. [Google Scholar] [CrossRef]
- Kim, S.A.; Shin, S. Red meat and processed meat consumption and the risk of dyslipidemia in Korean adults: A prospective cohort study based on the Health Examinees (HEXA) study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1714–1727. [Google Scholar] [CrossRef]
- Choi, S.E.; Lee, K.J. Ethnic differences in attitudes, beliefs, and patterns of meat consumption among American young women meat eaters. Nutr. Res. Pract. 2023, 17, 73–90. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Youssef, G.; Procter-Gray, E.; Olendzki, B.; Cornish, T.; Hayes, R.; Churchill, L.; Kane, K.; Brown, K.; Magee, M.F. Racial Differences in Eating Patterns and Food Purchasing Behaviors among Urban Older Women. J. Nutr. Health Aging 2017, 21, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Lee-Kwan, S.H.; Moore, L.V.; Blanck, H.M.; Harris, D.M.; Galuska, D. Disparities in State-Specific Adult Fruit and Vegetable Consumption—United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Brown-Riggs, C. Nutrition and Health Disparities: The Role of Dairy in Improving Minority Health Outcomes. Int. J. Environ. Res. Public. Health 2015, 13, 28. [Google Scholar] [CrossRef]
- Richards Adams, I.K.; Figueroa, W.; Hatsu, I.; Odei, J.B.; Sotos-Prieto, M.; Leson, S.; Huling, J.; Joseph, J.J. An Examination of Demographic and Psychosocial Factors, Barriers to Healthy Eating, and Diet Quality Among African American Adults. Nutrients 2019, 11, 519. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AA | White | AA | White | AA | White | |
|---|---|---|---|---|---|---|
| Male + Female | Female | Male | ||||
| n | 56 | 26 | 43 | 20 | 13 | 6 |
| Age (yrs) | 48 ± 1.3 | 53 ± 1.5 | 47 ± 1.5 | 52 ± 1.9 | 48 ± 3.2^ | 55 ± 0.8 ^^ |
| BMI (kg/m2) | 37 ± 1.2 | 38 ± 2.1 | 38 ± 1.3 | 37 ± 2.2 | 31 ± 1.8 | 40 ± 6.1 |
| Diabetes duration (yrs) | 3.7 ± 0.4 | 4.7 ± 0.9 | 3.6 ± 0.5 | 4.2 ± 1.0 | 3.7 ± 1.0 | 6.4 ± 2.4 |
| HbA1c (%) | 7.9 ± 0.3 | 7.4 ± 0.3 | 7.8 ± 0.3 | 7.0 ± 0.2 | 8.3 ± 0.5 | 8.5 ± 0.8 |
| Triglycerides(mg/dL) | 135 ± 15 * | 243 ± 32 ** | 117 ± 7 # | 242 ± 40 ## | 196 ± 59 | 245 ± 53 |
| 25(OH)D (μM/mL) | 15 ± 1.1 * | 19 ± 1.9 ** | 15 ± 1.4 # | 20 ± 2.2 ## | 15 ± 1.5 | 15 ± 3.6 |
| 25(OH)D/Triglycerides | 14 ± 1.8 | 8.6 ± 1.0 | 13 ± 2.0 | 9.0 ± 1.2 | 16 ± 4.0 | 6.9 ± 1.4 |
| L1-L4 BMD (g/cm2) | 1.3 ± 0.0 * | 1.2 ± 0.0 ** | 1.3 ± 0.0 # | 1.2 ± 0.0 ## | 1.4 ± 0.0 ^ | 1.2 ± 0.0 ^^ |
| Calcium (mg/dL) | 9.4 ± 0.1 | 9.2 ± 0.1 | 9.3 ± 0.0 | 9.3 ± 0.1 | 9.6 ± 0.1 ^ | 9.2 ± 0.1 ^^ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stevens, C.M.; Jain, S.K. Vitamin D/Bone Mineral Density and Triglyceride Paradoxes Seen in African Americans: A Cross-Sectional Study and Review of the Literature. Int. J. Mol. Sci. 2024, 25, 1305. https://doi.org/10.3390/ijms25021305
Stevens CM, Jain SK. Vitamin D/Bone Mineral Density and Triglyceride Paradoxes Seen in African Americans: A Cross-Sectional Study and Review of the Literature. International Journal of Molecular Sciences. 2024; 25(2):1305. https://doi.org/10.3390/ijms25021305
Chicago/Turabian StyleStevens, Christopher M., and Sushil K. Jain. 2024. "Vitamin D/Bone Mineral Density and Triglyceride Paradoxes Seen in African Americans: A Cross-Sectional Study and Review of the Literature" International Journal of Molecular Sciences 25, no. 2: 1305. https://doi.org/10.3390/ijms25021305
APA StyleStevens, C. M., & Jain, S. K. (2024). Vitamin D/Bone Mineral Density and Triglyceride Paradoxes Seen in African Americans: A Cross-Sectional Study and Review of the Literature. International Journal of Molecular Sciences, 25(2), 1305. https://doi.org/10.3390/ijms25021305