Abstract
Cutaneous wound healing consists of four stages: hemostasis, inflammation, proliferation/repair, and remodeling. While healthy wounds normally heal in four to six weeks, a variety of underlying medical conditions can impair the progression through the stages of wound healing, resulting in the development of chronic, non-healing wounds. Great progress has been made in developing wound dressings and improving surgical techniques, yet challenges remain in finding effective therapeutics that directly promote healing. This review examines the current understanding of the pro-healing effects of targeted pharmaceuticals, re-purposed drugs, natural products, and cell-based therapies on the various cell types present in normal and chronic wounds. Overall, despite several promising studies, there remains only one therapeutic approved by the United States Food and Drug Administration (FDA), Becaplermin, shown to significantly improve wound closure in the clinic. This highlights the need for new approaches aimed at understanding and targeting the underlying mechanisms impeding wound closure and moving the field from the management of chronic wounds towards resolving wounds.
1. Introduction
1.1. Normal Wound Healing
Wound healing is a complex process classified into four defined stages: hemostasis, inflammation, proliferation/repair and remodeling (Figure 1A). Immediately after injury, hemostasis occurs through the formation of a fibrin and platelet plug which trigger a coagulation cascade to stop the bleeding at the site of injury and promote recruitment of cells from the surrounding tissue and bloodstream. The fibrin plug, from platelet-derived fibrinogen, acts as a matrix for fibroblasts and macrophages []. Damage to endothelial cells exposes collagen which stimulates platelets to undergo activation, adhesion, and aggregation. Platelets produce chemotactic factors including transforming growth factor-β (TGF-β) and platelet-derived growth factor (PDGF). These growth factors attract neutrophils, macrophages and fibroblasts, which are essential for the initiation and completion of the inflammatory and proliferative stages of healing. In addition, changes in osmolarity and an increase in hydrogen peroxide contribute to leukocyte recruitment to the wound site [,].
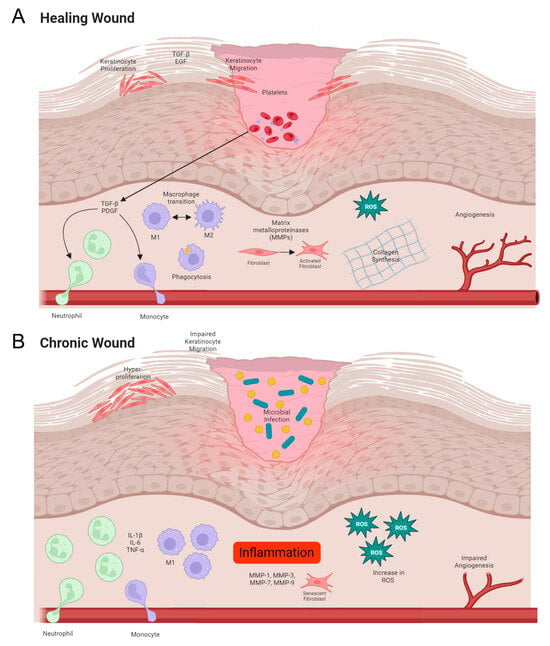
Figure 1.
Normal versus chronic wound healing. (A) In normal wounds, there is an orderly progression from hemostasis to inflammation, proliferation/repair and, finally, remodeling. (B) Chronic wounds demonstrate increased inflammation, reduced keratinocyte migration associated with hyperproliferation and the presence of bacterial biofilms.
The inflammatory phase starts within minutes of wound formation when neutrophils adhere to the endothelium. Neutrophils use collagen and elastase to facilitate migration into the extracellular space where they degrade matrix proteins, phagocytose microbes, and further attract additional neutrophils as well as macrophages. Macrophages play a key role in the acute healing process and are the predominant cell type during the inflammatory stage. Macrophage differentiation exists on a spectrum, commonly delineated as either M1 leaning or M2 leaning. The phenotype of macrophages changes as wounds progress through the stages of healing, towards a resolved healed response. During the early stages of wound healing, macrophages differentiate into an M1 phenotype, which infiltrates the wound site and removes bacteria, debris, and dead cells. Then, as the wound begins to repair the macrophage population transitions to an M2 phenotype which promotes resolution of inflammation and enables migration and proliferation of fibroblasts and keratinocytes and rebuilding of the tissue architecture [,].
The proliferation phase begins within 24 h of wounding and comprises fibroplasia, granulation, epithelialization and angiogenesis. The fibrin matrix created during hemostasis enables keratinocyte migration from the wound edge and hair follicles across the keratinocytes within the wound bed. In addition to TGF-β and Interleukin-6 (IL-6), the production of key molecules Epidermal Growth Factor (EGF) and Tumor Necrosis Factor-α (TNF-α) are essential to balance keratinocyte proliferation and migration []. Interestingly, disruption of the epithelium generates a directional electrical field, which also helps orient keratinocytes for directed migration []. Angiogenesis is induced by the presence of Vascular Endothelial Growth Factor (VEGF), which is upregulated by low oxygen tension []. Endothelial cells are recruited and stimulated to proliferate by VEGF, which induces smooth muscle cell migration [].
Fibroblasts migrate to the wound site between 48–72 h post wound and are integral for dermal matrix repair. Fibroblasts produce structural proteins including elastin, matrix metalloproteinases (MMPs) and collagen family members. MMPs degrade the fibrin plug which was formed during hemostasis and facilitate fibroblast movement. Collagen is present 48–72 h post wounding and is at peak secretion between 5 and 7 days []. Remodeling of the wound takes weeks to years. Wound contraction begins around 5 days post wounding as fibroblasts change into myofibroblasts which are predominantly actin producers. MMPs and MMP inhibitors reorganize type III collagen into a strong network of type I collagen. Collagen reaches 20% of its tensile strength after ~3 weeks and 80% strength in 12 months, during which the skin is fragile and prone to re-wounding [].
1.2. Impaired Wound Healing in Chronic Wounds
Chronic wounds are defined by their failure to progress through the stages of wound healing in a regulated and timely fashion. Wound healing takes between four to six weeks, whereas chronic wounds can take significantly longer or can fail to heal entirely []. This loose definition is largely a result of the heterogeneity in chronic wound etiology. Wounds vary greatly in location, size, and host factors. Chronic wounds broadly affect the adult population and the impact is exacerbated by comorbidities such as diabetes, cardiovascular disease, venous/arterial insufficiency and/or lack of mobility []. Chronic wounds can be further subclassified into arterial and venous ulcers, pressure ulcers and diabetic ulcers.
It is estimated that approximately 2% of the population will experience a chronic wound in their lifetime. This translates to 5.7 million people in the United States and an annual cost of around $20 billion. In addition to this economic burden, chronic wounds precede 85% of all amputations, with diabetic ulcers responsible for 70% of all lower limb amputations. Unfortunately, the 5-year mortality rate following amputation is between 40–70% [], demonstrating the importance of effectively managing these wounds. Chronic wounds tend to be treated as a co-morbidity of other conditions by clinicians from a range of specialties including dermatology, podiatry, and geriatrics. Clinicians often lack specialized training in the diagnosis and treatment of wounds as it is not a defined specialty, leading to variations in treatment and wound management.
Chronic wounds generally stagnate between the inflammatory and proliferation stages, failing to reduce inflammation and rebuild the tissue architecture (Figure 1B). Often there is an increase in acute inflammatory cells such as macrophages and neutrophils, as well as cytokines including Interleukin-1β (IL-1β) and TNF-α and an absence of cellular growth and keratinocyte migration over the wound []. In addition, oxidative stress is known to impair the healing process. Reactive oxygen species (ROS)-mediated transcription can lead to sustained pro-inflammatory cytokine secretion and induction of MMPs specifically MMP-1, -3, -7 and -9. Within chronic wounds it is known that MMPs have higher protease activity which contributes to the degradation of the extracellular matrix (ECM), thus preventing healing. Excessive ROS can degrade the extracellular matrix and impair dermal fibroblast and keratinocyte function both directly and indirectly through the activation of proteolysis [,]. While low levels of ROS are required for intracellular signaling and defense against pathogens and can increase the rate of wound healing, higher concentrations can prevent keratinocyte migration impeding healing [].
One of the major impediments to wound healing is infection, which contributes to wound chronicity. Bacteria colonize the wound and irreversibly bind to the wound surface, forming complex communities of bacteria known as biofilms. These chronic, infected wounds are significantly harder to treat owing to their thick extracellular matrix and high prevalence of antimicrobial resistance. In addition, biofilms are hard to remove through physical methods such as sharps debridement [,]. Biofilms are known to be present in at least 60% of all chronic wounds and there is evidence that they form as early as 10 h post wounding []. It is thus unsurprising that many research efforts focus on antimicrobial therapies including therapeutic release hydrogels and novel methods of debridement.
2. Current Therapeutics for Wound Healing
The care of chronic wounds has seen major advancements over the years, particularly with improved surgical wound bed preparation [,,] and better wound dressings []. Wound dressings incorporating novel biomaterials [], altering fluid balance [] and modifying the pH of the wound environment [,,] have greatly improved outcomes for chronic wound patients. Importantly, chronic wounds are often a result of underlying pathology, and advances in the treatment of diabetes [,] and venous insufficiency [] are some of the best ways to reduce the burden of chronic wounds. Here, we examine the progress made in developing therapeutics designed to improve the healing of chronic wounds and their proposed mechanisms of action (Figure 2).
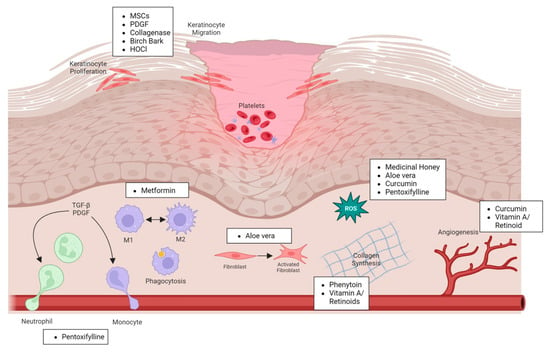
Figure 2.
Cell types affected by different pro-healing treatments.
2.1. Natural Products
2.1.1. Antibiotics
Antibiotics are a front-line therapeutic within wound care and, while their primary use is to eradicate microbial infection, there are several studies that have shown that they may have some pro-healing efficacy. Primarily, antibiotics kill or prevent the growth of the micro-organisms that cause infection and prevent it from spreading and worsening its effects []. Through the removal of micro-organisms, it is thought that antibiotics indirectly enable wound healing to occur more quickly []. While there is little evidence in the literature of antibiotics directly affecting wound healing, several studies have shown the positive impacts of antibiotics on healing time. Hwang et al. found that a gentamicin-loaded hydrogel wound dressing significantly increased wound healing in a non-infectious murine wound model compared to vehicle control dressing and untreated control wounds []. Further, Lin et al. showed a separate gentamicin hydrogel resulted in an increase in wound healing within a rat wound model []. Interestingly, Li et al. showed that a ciprofloxacin-releasing wound dressing significantly increased wound healing when compared to vehicle control in a murine wound model, the group also showed that in response to ciprofloxacin, CD34 expression was increased resulting in a vascular endothelial cell proliferation and migration to the wound area where they participate in the regeneration of blood capillaries and promote healing [].
2.1.2. Silver
Silver dressings are widely used within wound care, and silver is known to be antimicrobial, clearing bacterial contamination and thus enabling wound healing to occur more easily. There is extensive evidence of silver’s utility in infected open wounds [,,,]. However, despite the antimicrobial efficacy of silver, it is also toxic to fibroblasts when present in high concentrations and thus can lead to impaired wound healing. Silver sulfadiazine (SSD) is a topical cream/ointment used within wound care, but interestingly it has been shown to lead to slower epithelialization in multiple randomized control trials []. It is hypothesized that the heavy metal poisoning induced by SSD, which gives rise to its favorable antimicrobial properties, can also have a toxic effect on keratinocytes causing the observed, slowed reepithelization []. Further, systemic toxicity of silver can occur through absorption of silver through the skin and manifests as irreversible grey skin discoloration and loss of night vision. Luckily, this is rare, with only 16 recorded cases in the U.S., as serum silver is rapidly excreted in urine and feces []. Localized silver toxicity occurs more commonly owing to the cytotoxicity of silver ions against keratinocytes and fibroblasts. Toussaint et al. showed that Mepilex Ag had a slower healing time in a non-infected porcine burn model than antibiotic ointment []. Furthermore, Innes et al. [] showed that in skin graft donor sites the silver-containing surgical dressing Acticoat® was found to significantly delay epithelialization when compared to an occlusive dressing []. While silver has utility within infected wound care once a wound is clean silver-free dressings should be used owing to their detrimental effects on epithelization []. It should be noted that the impact of silver on wound healing varies on mode of delivery, release rate, concentration, and exposure. For example, it has been shown that nanocrystalline silver is the most potent delivery system and resulted in the greatest acceleration in wound re-epithelialization and multiple studies have shown that silver nanoparticles (AgNPs) have been shown to increase wound healing [,,].
2.1.3. Medicinal Honey
Honey has been used in medicine throughout history and was first used by the Egyptians in surgical dressings to facilitate wound healing. Within wound care, honey is known to be antimicrobial but it also has additional pro-healing effects []. Medical honey is known to upregulate pro-inflammatory cytokines TNF-α, IL-1β, IL-6 and prostaglandin E2 production, aiding in the inflammatory phase. Honey can also increase MMP-9 and TGF-β, contributing to the proliferative and remodeling phase []. One type of medicinal honey, manuka honey, is widely used in wound care. Manuka honey has a cocktail of enzymes in it, one of which is glucose oxidase, which catalyzes the oxidation of glucose to gluconic acid and H2O2. Gluconic acid results in a reduction in pH and the H2O2 is anti-bacterial. This pH change results in a reduction in protease activity at the wound site and a subsequent increase in oxygen release from hemoglobin resulting in the stimulation of fibroblast and macrophage activity. In addition, the H2O2 stimulates VEGF production. Further, flavonoids are present in honey which are ROS scavengers, neutralizing free radicles and further enhancing healing []. There are several Manuka honey dressings approved by the FDA varying in the proportion of Manuka honey applied to the wound. Robson et al. highlight the success of MedihoneyTM in their clinical setting and describe 90% of their cases of chronic wounds as successfully closed []. Moreover, Biglari et al. demonstrated a significant reduction in healing time with MedihoneyTM in patients with chronic pressure ulcers []. While the utility of medical honey as an antimicrobial in wounds is well understood, further study is required to understand if medical honey is physiologically driving healing as opposed to simply reducing bacterial contamination and enabling improved healing.
2.1.4. Curcumin
Curcumin is a polyphenol derived from the rhizome of Curcuma longa, which is commonly known as turmeric. Curcumin has historically been used within herbal medicine across the globe with applications in wound care and other illnesses owing to its anti-inflammatory, antioxidant, antimicrobial and anti-cancer properties. Curcumin modulates inflammatory, proliferative and remodeling phases of wound healing []. It has been reported to inhibit the production of TNF-α and IL-1 via NF-ĸB signaling, which are key cytokines in mediating inflammation [,]. In addition, curcumin scavenges ROS, mitigating oxidative stress and increasing the production of collagen and hydroxyproline during the proliferative phase of wound healing [,]. Gadekar et al. [] showed that applying transdermal curcumin patches to excisional wounds in rats promoted wound contraction and angiogenesis, resulting in reduced healing time []. This phenomenon was further explored in vitro by Phan et al. who used an H2O2 model of damage on human fibroblasts and keratinocytes to demonstrate successful repair after curcumin administration []. Curcumin also has been shown to play a role in the proliferative stage of healing. Gopinath et al. treated wounded rats with curcumin-loaded chitosan sponges and found that there was a better alignment of granulation tissue compared to a control []. Curcumin is thus able to accelerate the process of wound healing by shortening the inflammatory phase and aiding in proliferation and remodeling. Curcumin’s hydrophobicity results in poor oral absorption, and thus it is more commonly used for topical application [].
2.1.5. Aloe Vera
Aloe vera is derived from the cactus-like plant Aloe barbadensis and has been used throughout history, with its earliest use documented by Egyptians in 4000 B.C. [,]. Aloe vera is used to treat burns and ulcers and has been shown to reduce pain and improve healing time []. Aloe vera is also known to decrease TNF-α and IL-1 [,] and its phenolic compound content promotes ROS scavenging, reducing inflammation [,]. In addition, Aloe vera contains polysaccharides, such as mannose-6-phosphate, which bind and stimulate fibroblast activity and proliferation, which increases collagen production [].
2.1.6. Birch Bark
Betula alba (birch bark) has been used within traditional medicine across the northern hemisphere and was first used in wound care by the Native American Ojibwe tribe, who would wrap their wounds with birch bark to accelerate healing []. Birch bark’s healing properties have since been proven clinically using n-heptane dry extract from the outer bark of the birch; 97% of the extract is pentacyclic triterpenes [] and the triterpene responsible for wound healing is botulin []. Ebeling et al. showed that triterpenes significantly increased wound healing in an ex vivo porcine healing model, demonstrating improved skin barrier and enhanced migration when applied to human keratinocytes, mediated through IL-6 and signal transducer and activator of transcription 3 (STAT3) signaling []. A birch bark gel bark extract (Episalvan®) has found accelerated re-epithelialization in partial thickness skin wounds [] and superficial partial thickness burns [] and has been approved for use in humans by the European Medicines Agency (EMA); however, it is yet to be approved by the United States FDA.
2.2. Human-Derived Factors
2.2.1. Mesenchymal Stem Cells
Mesenchymal stem cells (MSCs) are multipotent stem cells derived from the mesoderm and give rise to osteoblasts, chondrocytes, adipocytes, and reticular stroma. MSCs can be isolated from a variety of sources, such as bone marrow, umbilical cord tissue, the placenta, and adipose tissue []. The fundamental biological mechanism of mesenchymal stem cell-induced wound healing is thought to be due to their ability to secrete pro-regenerative cytokines []. MSCs modulate the immune response, through the secretion of interferon gamma (IFN-λ) and TNF-α, leading to an increase in the secretion of IL-10 and IL-4 produced by various immune cells including but not limited to macrophages, dendritic cells (DCs), and lymphocytes [,]. In addition, MSCs promote the formation of new vessels and extracellular matrix and mediate cell proliferation and differentiation through the secretion of VEGF, keratinocyte growth factor, MMP-9, and EGF [].
There have been several trials using MSCs to treat chronic, diabetic wounds. Hashemi et al. seeded an acellular amniotic membrane with Wharton’s jelly mesenchymal stem cells and reported a reduction in wound size and time needed to heal []. Vojtaššák et al. applied a biodegradable collagen membrane (Coladerm) in combination with autologous MSCs from the patient’s bone marrow to the patient’s diabetic foot ulcer on days 0, 7 and 17, relative to when treatment began. By day 29, closing and healing of the wound was achieved []. Multiple clinical trials are ongoing, including Cell2Cure’s study “STEMFOOT” (Trial no: NCT05595681) which is an “off-the-shelf” adipose tissue-derived mesenchymal stem cell product [].
Major drawbacks of MSC therapy include the “standardization” of manufacturing and quality control owing to the variation in cellular proliferation and differentiation capacity between donors. In addition, there is variation observed between subpopulations of MSCs from a single source owing to RNA production variation []. Further complicating this is the issue of which site to obtain MSCs, as bone marrow-derived MSCs are commonly used in cutaneous wound healing whereas adipose-derived and umbilical cord-derived cells have been used in diabetic ulcer trials [,].
2.2.2. Macrophages
Macrophage modulation has been explored as a potential therapeutic option. Goren et al. systemically administered neutralizing monoclonal antibodies anti-TNF-α and anti-F4/80 into diabetic wound models and reported the antibodies effectively targeted and killed pro-inflammatory wound macrophages resulting in accelerated healing []. Danon et al. administered macrophages obtained from the blood of young healthy donors and stimulated by hypo-osmotic shock, intradermally near pressure ulcer site in elderly patients which resulted in an increased rate of healing []. This was further confirmed by Zuloff-Shani et al. with intradermal injection of macrophages increasing healing in both pressure and diabetic ulcers [].
2.2.3. Collagenase
Collagenase belongs to the metalloproteinase family and plays an important role in the metabolism of collagen in mammalian tissues. Skin consists of between 70–80% collagen; thus, unsurprisingly, the action of collagenase is immensely important. Collagenases are the only enzymes that can specifically cleave native collagen. In healthy wounds, endogenous collagenase breaks down necrotic tissue to enable healing to occur. However, often in non-healing wounds the underlying disease etiology such as diabetes or age may cause impaired collagenase activity, resulting in a buildup of necrotic tissue preventing healing from occurring []. Collagenase can therefore be used as a debridement agent, as it can break down necrotic and/or fibrotic tissues within sites of tissue damage without damaging healthy tissue, creating a more congruent wound bed for healing. Interestingly, collagenase has also been shown to increase proliferation, angiogenesis and migration within wounds [].
Collagenase Santyl® ointment (Smith & Nephew) is a preparation of enzymes including collagenase and non-specific proteases produced by Clostridium histolyticum fermentation and is approved by the FDA for clinical use []. Tallis et al. showed that collagenase ointment significantly improved the wound bed appearance and enhanced the rate of healing []. Riley et al. showed in vitro that collagenase indeed does promote keratinocyte proliferation and keratinocyte migration. Further, in vivo findings showed that collagenase increased the rate of re-epithelization and increased wound closure rate in the mini-pig wound model [].
2.2.4. Placental-Derived Products
Tissue derived from the placenta contains a variety of growth factors (PDGF-BB, TGFα, bFGF and EGF), cytokines (IL-4, IL-6, IL-8 and IL-10) and ECM components [], which have been shown to contribute to wound healing. This can include dehydrated human amnion/chorion membrane (dHACM) products such as EPIFIX (MiMedx) and a dehydrated human umbilical cord (DHUC) such as EPICORD (MiMedx). In vitro studies have shown that dHACM can increase fibroblast migration and induce MSC migration. This MSC migration was also seen in a murine wound model which was treated with dHCAM []. As these grafts contain a complex mixture of components with biological activity, the key factors mediating these effects are not clear. However, there is ample clinical evidence for a positive effect on wound healing in patients [,] and this treatment is recommended by The International Working Group on the Diabetic Foot [].
2.2.5. Autologous Leucocyte/Platelet/Fibrin Patch
It has been recognized that during the initial phases of wound healing, platelets and leucocytes are recruited to the wound site and release growth factors such as PDGF []. While treatment with individual growth factors has not been reported to be beneficial, better success has been found in developing products that contain living platelets and leucocytes as opposed to just individual growth factors. In these systems, platelets and leucocytes are harvested from patients and placed in a fibrin membrane for use on the patient’s wound. Encouragingly, products such as the 3C PATCH® (Reapplix) have shown good efficacy in diabetic foot ulcers [,,], and this treatment has also been recommended by The International Working Group on the Diabetic Foot [].
2.3. Pharmaceutical Drugs
2.3.1. PDGF (Becapletmin)
Multiple growth factors have been identified as being critical in wound healing, including PDGF, EGF, FGF and TGF. However, only PDGF has been shown to augment wound healing in vivo []. PDGF is predominantly synthesized by platelets and is a dimer of A and/or B chains held together by disulfide bonds. There are three known isomers of PDGF that have been isolated from human platelets, AA, BB and AB, the most potent of which is BB. PDGF can bind to cells via two cell surface receptors: α-PDGF and β-PDGF. α-PDGF is a non-specific receptor while β-PDGF specifically binds PDGF-BB. β-PDGF is the most common receptor found in humans; as such, only PDGF-BB has been explored as a therapeutic [].
Becaplermin is a homodimeric protein produced from DNA technology whereby the gene for the B chain PDGF is inserted into Saccharomyces cerevisiae. Becaplermin’s biological activity is like endogenous PDGF-BB specifically in its ability to promote chemotactic recruitment and proliferation of cells involved in wound repair. Becaplermin has been used extensively in the management of diabetic foot ulceration [] and is currently licensed as Regranex® (Smith and Nephew) []. Extensive animal and human studies have been carried out to demonstrate the efficacy of Becaplermin. Pierce et al. applied PDGF to incision wounds in rats and found that it both accelerated wound healing and improved the breaking strength of the wound []. The in vitro evidence of PDGF’s direct effect on keratinocytes is lacking however, it has been shown to increase the rate of epithelization in vivo. It is thus hypothesized that PDGF indirectly affects reepithelization through the recruitment of macrophages and fibroblasts []. Controversially, upon the original FDA approval of Regranex® in 2008, it had a black box warning owing to an increased rate of mortality from secondary malignancy []. However, in 2018, the black box warning was removed after multiple studies including one by Ziyadeh et al., and showed that there was no increased incidence of cancer or cancer mortality associated with Regranex® gel use [].
2.3.2. Phenytoin
Phenytoin (diphenylhydantoin) is a medication that was FDA approved in 1939 to treat convulsive disorders, such as epilepsy and seizures. However, according to the National Health Services (NHS), inflamed gums, specifically the development of fibrous overgrowth of gingiva and mild skin thickening, were common side effects of the use of phenytoin []. This stimulatory effect of phenytoin on connective tissues suggested its potential for use within wound care. Phenytoin has been shown to promote wound healing in dental extraction sockets [] and corneal wounds []. Using a rat burn skin wound model, Sayar et al. showed administration of phenytoin increased healing through the development of vascularized, granulation tissue and increased collagen synthesis through re-epithelization []. Carneiro et al. conducted a clinical trial where acute burns were treated with topical phenytoin powder improved healing outcomes relative to Silverex, a cream containing SSD, commonly used for burn treatment []. Further, Inchingolo et al. investigated the use of topical phenytoin on bedsores by administering phenytoin-soaked patches at 12-h intervals. The patients treated with the phenytoin patches healed significantly quicker than those treated with water solution-soaked patches []. The exact mechanism of phenytoin in wound healing is unknown; however, studies suggest phenytoin promotes collagen deposition, decreases wound exudate and bacteria contamination [,] and may promote fibroblast proliferation [].
2.3.3. Vitamin A/Retinoids
Vitamin A is an essential fat-soluble dietary vitamin that is known to play a key role in epidermal maintenance by promoting desquamation and maturation through decreased production of keratin, keratohyalin granules and desmosomes. Within wound healing, vitamin A is known to contribute through the stimulation of angiogenesis, epithelization, and collagen synthesis. The pro-healing efficacy of vitamin A can rescue the antagonistic effect of steroids upon healing. However, their mechanism of healing is unknown. Vitamin A’s clinical use within wound care is hindered by its secondary effects. Systemic side effects include neurological and psychiatric effects and cutaneous effects include coarse hair, dry skin and widespread alopecia [,].
Owing to these side effects, retinoids were developed to combine the therapeutic effects of vitamin A with fewer adverse events. Retinoids are synthetic and natural derivatives of vitamin A. They bind to nuclear receptors on keratinocytes and regulate gene expression. First-generation retinoids, isotretinoin, all-trans-retinoic acid (tretinoin) and 9-cis-retinoic acid are nonaromatic compounds with modification on the polar end group and polyene side chain of vitamin A [,]. Originally an acne vulgaris therapeutic, retinoids have proven useful in preoperative facial rejuvenation and wound management [,,]. Second-generation retinoids are monoaromatic formed by replacing the cyclic end of vitamin A with a modified ring. The most used is acitretin, which is used to treat psoriasis and other conditions which involve abnormal keratinization. Third-generation retinoids are polyaromatic compounds formed by cyclization of polyene side chains. Tazarotene is used for psoriasis and adapalene is used for acne vulgaris [].
The evidence for the use of topical retinoids for use on wounds is conflicting. Tretinoin’s capacity to improve wound healing is thought to be due to its ability to reduce the production of procollagen in fibroblasts. This has been shown to be advantageous in hypertrophic scars and keloids. However, abnormal healing has also been reported through increased collagen degradation. Tom et al. showed a significant increase in diabetic ulcer healing in tretinoin-treated patients compared to placebo []. These findings were further supported by Paquette et al. in patients with chronic leg ulcers from venous disease or rheumatoid arthritis. With a short 10-minute application of 0.05% retinoic acid solution, within 7 days granulation tissue started to appear []. However, several studies have shown conflicting evidence against the utility of retinoids in wound healing. Watcher and Wheeland found that tretinoin resulted in significant retardation of reepithelization []. Overall, the evidence for good outcomes with retinoic acid in wounds with unfavorable baseline conditions is positive [].
2.3.4. Hypochlorous Acid
The immune system produces a range of ROS to protect from invading pathogens. During neutrophil activation, respiratory bursts generate H2O2 and activated granule enzyme myeloperoxidase converts H2O2 to hypochlorous acid (HOCl) in the presence of Cl− and H+. HOCl causes cell death by oxidation of sulfhydryl enzymes and amino acids, ring chlorination of amino acids, loss of intracellular contents, decreased uptake of nutrients, inhibition of protein synthesis, decreased oxygen uptake, breaks DNA and depressed DNA synthesis [,]. As such, HOCl is a known antimicrobial capable of clearing bacterial, viral, and fungal contamination from the wound. Using an in vitro wound migration model, Sakarya et al. found that applying an HOCl solution, as an antimicrobial agent, in a dose-dependent manner increased keratinocyte and fibroblast migration []. Da Costa et al. showed that HOCl was effective in significantly increasing wound closure in a murine cutaneous wound model. They also showed that HOCl increased vascularization, increased neutrophil activity in the early phase of wounding and increased collagen []. Further work done by Dharap et al. showed success in the clinic where patients’ ulcers were dressed with Oxum, a super oxidized solution containing HOCl, reduced ulcer size and inflammation [].
2.3.5. Pentoxifylline
Pentoxifylline (PTX) is a dimethylxanthine derivative that increases cyclic adenosine monophosphate (cAMP) levels in the smooth muscle of blood vessels resulting in improved blood flow and oxygenation of ischemic tissues. It is also known to increase red and white cell filterability and platelet aggregation, fibrinogen levels and decrease whole blood viscosity []. This antithrombotic effect of PTX is linked to its induction of prostacyclin synthesis and inhibition of phosphodiesterase E enzyme. Prostacyclin is a potent vasodilator and platelet aggregation inhibitor. Further, PTX has been shown to inhibit the synthesis of inflammatory mediators, decrease cytokine release, suppress leukocyte function and reduce oxidative stress []. Velaei et al. used PTX as a treatment in a pressure wound-induced model on rats and reported accelerated wound healing through undefined mechanisms []. A study by Lim et al. tested PTX on a burn wound model, where relative to their small sample size, they did find a benefit compared to the placebo []. While the experimental data were mixed, Rawlins et al. showed in a clinical study that PTX was able to significantly improve perioral burns and improve scarring outcomes owing to PTX’s ability to inhibit fibroblast proliferation resulting in a decrease in type I and III collagens and glycosaminoglycans and increase collagenase activity []. Overall, further investigation is needed to define the success of PTX in wound care and the mechanisms by which it acts.
2.3.6. Metformin
Metformin is an oral diabetic medication that helps lower blood sugar levels in type 2 diabetic patients. Interestingly, metformin treatment improved wound healing in aged rats, increasing both vascularization of the wound bed and proliferation of keratinocytes through activation of AMP-activated protein kinase (AMPK) []. Metformin has also been shown to boost M2 macrophage polarization through the induction of AMPK and mTOR and accelerate wound healing []. Further, Han et al. showed that metformin accelerated wound healing in the murine diabetic wound model []. While metformin is a promising therapeutic in diabetic patients due to its ability to treat the potential underlying pathology, further research is needed to assess its direct effects on wound healing.
3. Conclusions and Future Perspectives
The wound environment is a complex and changing environment, which creates unique challenges in the development of new and effective therapeutics. For example, treatments that promote an immune response may help prevent biofilm formation but could impede the transition from the inflammatory phase to the proliferative phase. Spatial differences also can complicate treatment approaches, particularly in keratinocytes, which need to migrate at the wound edges, but proliferate further away from the wound []. It is therefore essential to develop therapeutic strategies which allow for precise spatial and temporal drug release. An ideal delivery system would enable maximum therapeutic benefit by protecting the therapeutic payload from proteolysis, localizing bioavailability, and limiting systemic uptake and distribution to enable release maintenance at a physiologically relevant dose and duration. There is a range of biomaterials that can act as delivery vehicles including hydrogels, scaffolds and particles []. Hydrogels are the favored method of drug delivery in wound care owing to their multifaceted functionality. They provide a physical barrier between the wound and the external environment, preventing further pathogenic contamination, they are semi-permeable, allowing vapor transmission and oxygen and carbon dioxide exchange, and can be made of polymers that have intrinsic antimicrobial and pro-healing properties themselves such as chitosan. Importantly, the physical properties of hydrogels can be tuned to release the therapeutic at the optimal rate and concentration or in response to an environmental or physiological change, such as using H2O2 to trigger therapeutic release [] or wound pH [] to maximize efficacy [].
Traditional therapeutics, such as aloe vera, have been used for centuries to treat wounds, and several natural products, including manuka honey and birch bark extract, are now sold commercially as a wound therapy. While progress has been made in the development of targeted therapeutics, the mechanisms of action of many of these treatments remain ill-defined. Contributing to the difficulty in developing new treatments is the fact that the underlying mechanisms regulating normal wound healing are still being elucidated (Table 1). This knowledge gap has made it difficult to pinpoint exactly what is dysfunctional in chronic wounds and how to correct these defects to normalize the wound environment. Compounding this problem, patients with chronic wounds often have underlying pathologies, like diabetes, which further impairs the healing process and creates an altered wound environment. Despite these challenges, recent technological advances in single-cell multi-omics and spatial profiling have vastly expanded our ability to interrogate the wound microenvironment and the dynamic interplay between cell populations during the wound healing process. These studies will undoubtedly lead to new, mechanism-driven treatments with the potential to attack root causes of dysfunctional wound closure and vastly improve patient outcomes. In summary, there are multiple therapeutic options available that stimulate wound healing to some extent, but there are substantial unmet needs highlighting the necessity for more effective treatments to improve the quality of life for individuals battling chronic wounds.

Table 1.
Overview of the different categories of pro-healing drugs covered in the review, the drug name, effect on healing and commercial name.
Author Contributions
Conceptualization, B.L.P. and M.R.R.; writing—original draft preparation, B.L.P.; writing—review and editing, K.A.C. and M.R.R.; visualization, B.L.P.; funding acquisition, M.R.R. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded in part by a Fund to Sustain Research Excellence award from the Brigham Research Institute. K.A.C. is funded by a training grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (T32AR007098).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We wish to thank Maria Padilla for her helpful suggestions and comments.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Morton, L.M.; Phillips, T.J. Wound healing and treating wounds: Differential diagnosis and evaluation of chronic wounds. J. Am. Acad. Dermatol. 2016, 74, 589–605. [Google Scholar] [CrossRef] [PubMed]
- Enyedi, B.; Kala, S.; Nikolich-Zugich, T.; Niethammer, P. Tissue damage detection by osmotic surveillance. Nat. Cell Biol. 2013, 15, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Niethammer, P.; Grabher, C.; Look, A.T.; Mitchison, T.J. A tissue-scale gradient of hydrogen peroxide mediates rapid wound detection in zebrafish. Nature 2009, 459, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Mills, C.D. M1 and M2 Macrophages: Oracles of Health and Disease. Crit. Rev. Immunol. 2012, 32, 463–488. [Google Scholar] [CrossRef]
- Martinez, F.O.; Gordon, S. The M1 and M2 paradigm of macrophage activation: Time for reassessment. F1000Prime Rep. 2014, 6, 13. [Google Scholar] [CrossRef]
- Haensel, D.; Dai, X. Epithelial-to-mesenchymal transition in cutaneous wound healing: Where we are and where we are heading. Dev. Dyn. 2018, 247, 473–480. [Google Scholar] [CrossRef]
- Zhao, M.; Song, B.; Pu, J.; Wada, T.; Reid, B.; Tai, G.; Wang, F.; Guo, A.; Walczysko, P.; Gu, Y.; et al. Electrical signals control wound healing through phosphatidylinositol-3-OH kinase-gamma and PTEN. Nature 2006, 442, 457–460. [Google Scholar] [CrossRef]
- Liu, Y.; Cox, S.R.; Morita, T.; Kourembanas, S. Hypoxia Regulates Vascular Endothelial Growth Factor Gene Expression in Endothelial Cells. Circ. Res. 1995, 77, 638–643. [Google Scholar] [CrossRef]
- Cucina, A.; Borrelli, V.; Randone, B.; Coluccia, P.; Sapienza, P.; Cavallaro, A. Vascular endothelial growth factor increases the migration and proliferation of smooth muscle cells through the mediation of growth factors released by endothelial cells. J. Surg. Res. 2003, 109, 16–23. [Google Scholar] [CrossRef]
- Gilmore, M.A. Phases of wound healing. Dimens. Oncol. Nurs. J. Div. Nurs. 1991, 5, 32–34. [Google Scholar]
- Frykberg, R.G.; Banks, J. Challenges in the Treatment of Chronic Wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V.; Isseroff, R.R.; Soulika, A.M.; Romanelli, M.; Margolis, D.; Kapp, S.; Granick, M.; Harding, K. Chronic wounds. Nat. Rev. Dis. Primers 2022, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Järbrink, K.; Ni, G.; Sönnergren, H.; Schmidtchen, A.; Pang, C.; Bajpai, R.; Car, J. The humanistic and economic burden of chronic wounds: A protocol for a systematic review. Syst. Rev. 2017, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Dunnill, C.; Patton, T.; Brennan, J.; Barrett, J.; Dryden, M.; Cooke, J.; Leaper, D.; Georgopoulos, N.T. Reactive oxygen species (ROS) and wound healing: The functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 2017, 14, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Moseley, R.; Stewart, J.E.; Stephens, P.; Waddington, R.J.; Thomas, D.W. Extracellular matrix metabolites as potential biomarkers of disease activity in wound fluid: Lessons learned from other inflammatory diseases? Br. J. Dermatol. 2004, 150, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, M.; Werner, S. Oxidative stress in normal and impaired wound repair. Pharmacol. Res. 2008, 58, 165–171. [Google Scholar] [CrossRef] [PubMed]
- James, G.A.; Swogger, E.; Wolcott, R.; Pulcini, E.; Secor, P.; Sestrich, J.; Costerton, J.W.; Stewart, P.S. Biofilms in chronic wounds. Wound Repair. Regen. 2008, 16, 37–44. [Google Scholar] [CrossRef]
- Percival, S.L.; McCarty, S.M.; Lipsky, B. Biofilms and wounds: An overview of the evidence. Adv. Wound Care 2015, 4, 373–381. [Google Scholar] [CrossRef]
- Patenall, B.L.; Ridgley, J.D.; Jenkins, A.T.A.; Young, A.E. Evidence of bacterial biofilms within acute wounds: A systematic review. J. Wound Care 2023, 32, 273–278. [Google Scholar] [CrossRef]
- Schultz, G.S.; Sibbald, R.G.; Falanga, V.; Ayello, E.A.; Dowsett, C.; Harding, K.; Romanelli, M.; Stacey, M.C.; Teot, L.; Vanscheidt, W. Wound bed preparation: A systematic approach to wound management. Wound Repair Regen. 2003, 11 (Suppl. 1), S1–S28. [Google Scholar] [CrossRef]
- Schaper, N.C.; van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Fitridge, R.; Game, F.; Monteiro-Soares, M.; Senneville, E.; Board, I.E. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab. Res. Rev. 2023, e3657. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Nomkhondorj, O.; An, C.Y.; Choi, Y.C.; Cho, J. Management of diabetic foot ulcers: A narrative review. J. Yeungnam Med. Sci. 2023, 40, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Jia, Y.; Fu, L.; Guo, K.; Xie, S. The emerging progress on wound dressings and their application in clinic wound management. Heliyon 2023, 9, e22520. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.; Leal, E.C.; Carvalho, E.; Silva, E.A. Innovative Functional Biomaterials as Therapeutic Wound Dressings for Chronic Diabetic Foot Ulcers. Int. J. Mol. Sci. 2023, 24, 9900. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, V.; Astrelina, T.; Malivanova, T.; Samoilov, A. Modern Wound Dressings: Hydrogel Dressings. Biomedicines 2021, 9, 1235. [Google Scholar] [CrossRef]
- Haverkampf, S.; Heider, J.; Weiss, K.T.; Haubner, F.; Ettl, T.; Schreml, J.; Hedtrich, S.; von Susskind-Schwendi, M.; Berneburg, M.; Karrer, S.; et al. NHE1 expression at wound margins increases time-dependently during physiological healing. Exp. Dermatol. 2017, 26, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Schreml, S.; Meier, R.J.; Kirschbaum, M.; Kong, S.C.; Gehmert, S.; Felthaus, O.; Kuchler, S.; Sharpe, J.R.; Woltje, K.; Weiss, K.T.; et al. Luminescent dual sensors reveal extracellular pH-gradients and hypoxia on chronic wounds that disrupt epidermal repair. Theranostics 2014, 4, 721–735. [Google Scholar] [CrossRef]
- Schreml, S.; Meier, R.J.; Wolfbeis, O.S.; Landthaler, M.; Szeimies, R.M.; Babilas, P. 2D luminescence imaging of pH in vivo. Proc. Natl. Acad. Sci. USA 2011, 108, 2432–2437. [Google Scholar] [CrossRef]
- von Scholten, B.J.; Kreiner, F.F.; Gough, S.C.L.; von Herrath, M. Current and future therapies for type 1 diabetes. Diabetologia 2021, 64, 1037–1048. [Google Scholar] [CrossRef]
- Tahrani, A.A.; Barnett, A.H.; Bailey, C.J. Pharmacology and therapeutic implications of current drugs for type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2016, 12, 566–592. [Google Scholar] [CrossRef]
- Stanek, A.; Mosti, G.; Nematillaevich, T.S.; Valesky, E.M.; Planinsek Rucigaj, T.; Boucelma, M.; Marakomichelakis, G.; Liew, A.; Fazeli, B.; Catalano, M.; et al. No More Venous Ulcers-What More Can We Do? J Clin Med 2023, 12, 6153. [Google Scholar] [CrossRef] [PubMed]
- Altoe, L.S.; Alves, R.S.; Sarandy, M.M.; Morais-Santos, M.; Novaes, R.D.; Goncalves, R.V. Does antibiotic use accelerate or retard cutaneous repair? A systematic review in animal models. PLoS ONE 2019, 14, e0223511. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.; Dumville, J.C.; Mohapatra, D.P.; Owens, G.L.; Crosbie, E.J. Antibiotics and antiseptics for surgical wounds healing by secondary intention. Cochrane Database Syst. Rev. 2016, 3, CD011712. [Google Scholar] [CrossRef] [PubMed]
- Hwang, M.R.; Kim, J.O.; Lee, J.H.; Kim, Y.I.; Kim, J.H.; Chang, S.W.; Jin, S.G.; Kim, J.A.; Lyoo, W.S.; Han, S.S.; et al. Gentamicin-loaded wound dressing with polyvinyl alcohol/dextran hydrogel: Gel characterization and in vivo healing evaluation. AAPS PharmSciTech 2010, 11, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-H.; Lin, J.-H.; Peng, S.-F.; Yeh, C.-L.; Chen, W.-C.; Chang, T.-L.; Liu, M.-J.; Lai, C.-H. Multifunctional gentamicin supplementation of poly(γ-glutamic acid)-based hydrogels for wound dressing application. J. Appl. Polym. Sci. 2011, 120, 1057–1068. [Google Scholar] [CrossRef]
- Li, H.; Williams, G.R.; Wu, J.; Lv, Y.; Sun, X.; Wu, H.; Zhu, L.M. Thermosensitive nanofibers loaded with ciprofloxacin as antibacterial wound dressing materials. Int. J. Pharm. 2017, 517, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Sim, W.; Barnard, R.T.; Blaskovich, M.A.T.; Ziora, Z.M. Antimicrobial Silver in Medicinal and Consumer Applications: A Patent Review of the Past Decade (2007–2017). Antibiotics 2018, 7, 93. [Google Scholar] [CrossRef]
- Leaper, D. Appropriate use of silver dressings in wounds: International consensus document. Int. Wound J. 2012, 9, 461–464. [Google Scholar] [CrossRef]
- Warriner, R.; Burrell, R. Infection and the chronic wound: A focus on silver. Adv. Ski. Wound Care 2005, 18 (Suppl. S1), 2–12. [Google Scholar] [CrossRef]
- Storm-Versloot, M.N.; Vos, C.G.; Ubbink, D.T.; Vermeulen, H. Topical silver for preventing wound infection. Cochrane Database Syst. Rev. 2010, 3, Cd006478. [Google Scholar] [CrossRef]
- Khansa, I.; Schoenbrunner, A.R.; Kraft, C.T.; Janis, J.E. Silver in Wound Care-Friend or Foe?: A Comprehensive Review. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2390. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.J.; Hollyoak, M.A.; Moaveni, Z.; Brown, T.L.H.; Herndon, D.N.; Heggers, J.P. Retardation of wound healing by silver sulfadiazine is reversed by Aloe vera and nystatin. Burns 2003, 29, 834–836. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Konkel, K.; McCulley, L.; Diak, I.-L. Cases of Argyria Associated With Colloidal Silver Use. Ann. Pharmacother. 2019, 53, 867–870. [Google Scholar] [CrossRef]
- Toussaint, J.; Chung, W.T.; Osman, N.; McClain, S.A.; Raut, V.; Singer, A.J. Topical Antibiotic Ointment Versus Silver-containing Foam Dressing for Second-degree Burns in Swine. Acad. Emerg. Med. 2015, 22, 927–933. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Innes, M.E.; Umraw, N.; Fish, J.S.; Gomez, M.; Cartotto, R.C. The use of silver coated dressings on donor site wounds: A prospective, controlled matched pair study. Burns 2001, 27, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lee, P.Y.; Ho, C.M.; Lui, V.C.; Chen, Y.; Che, C.M.; Tam, P.K.; Wong, K.K. Silver nanoparticles mediate differential responses in keratinocytes and fibroblasts during skin wound healing. ChemMedChem 2010, 5, 468–475. [Google Scholar] [CrossRef]
- Oryan, A.; Alemzadeh, E.; Tashkhourian, J.; Nami Ana, S.F. Topical delivery of chitosan-capped silver nanoparticles speeds up healing in burn wounds: A preclinical study. Carbohydr. Polym. 2018, 200, 82–92. [Google Scholar] [CrossRef]
- Stojkovska, J.; Djurdjevic, Z.; Jancic, I.; Bufan, B.; Milenkovic, M.; Jankovic, R.; Miskovic-Stankovic, V.; Obradovic, B. Comparative in vivo evaluation of novel formulations based on alginate and silver nanoparticles for wound treatments. J. Biomater. Appl. 2018, 32, 1197–1211. [Google Scholar] [CrossRef]
- Lee, D.S.; Sinno, S.; Khachemoune, A. Honey and Wound Healing. Am. J. Clin. Dermatol. 2011, 12, 181–190. [Google Scholar] [CrossRef]
- Hadagali, M.D.; Chua, L.S. The anti-inflammatory and wound healing properties of honey. Eur. Food Res. Technol. 2014, 239, 1003–1014. [Google Scholar] [CrossRef]
- Tashkandi, H. Honey in wound healing: An updated review. Open Life Sci. 2021, 16, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Robson, V.; Dodd, S.; Thomas, S. Standardized antibacterial honey (Medihoney™) with standard therapy in wound care: Randomized clinical trial. J. Adv. Nurs. 2009, 65, 565–575. [Google Scholar] [CrossRef]
- Biglari, B.; vd Linden, P.H.; Simon, A.; Aytac, S.; Gerner, H.J.; Moghaddam, A. Use of Medihoney as a non-surgical therapy for chronic pressure ulcers in patients with spinal cord injury. Spinal Cord. 2012, 50, 165–169. [Google Scholar] [CrossRef]
- Akbik, D.; Ghadiri, M.; Chrzanowski, W.; Rohanizadeh, R. Curcumin as a wound healing agent. Life Sci. 2014, 116, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.L.; Li, Y.; Wen, Y.; Chen, Y.F.; Na, L.X.; Li, S.T.; Sun, C.H. Curcumin, a potential inhibitor of up-regulation of TNF-alpha and IL-6 induced by palmitate in 3T3-L1 adipocytes through NF-kappaB and JNK pathway. Biomed. Environ. Sci. 2009, 22, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Gupta, S.C.; Sung, B. Curcumin: An orally bioavailable blocker of TNF and other pro-inflammatory biomarkers. Br. J. Pharmacol. 2013, 169, 1672–1692. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, D.; Ahmed, M.R.; Gomathi, K.; Chitra, K.; Sehgal, P.K.; Jayakumar, R. Dermal wound healing processes with curcumin incorporated collagen films. Biomaterials 2004, 25, 1911–1917. [Google Scholar] [CrossRef]
- Gadekar, R.; Saurabh, M.K.; Thakur, G.S.; Saurabh, A. Study of formulation, characterisation and wound healing potential of transdermal patches of curcumin. Asian J Pharm Clin Res 2012, 5, 225–230. [Google Scholar]
- Phan, T.-T.; See, P.; Lee, S.-T.; Chan, S.-Y. Protective effects of curcumin against oxidative damage on skin cells in vitro: Its implication for wound healing. J. Trauma Acute Care Surg. 2001, 51, 927–931. [Google Scholar] [CrossRef]
- Sung, C.K. The history of Aloe. In New Perspectives on Aloe; Park, Y.I., Lee, S.K., Eds.; Springer: Boston, MA, USA, 2006; pp. 7–17. [Google Scholar]
- Lee, S.K. Overview of Aloe study. In New Perspectives on Aloe; Park, Y.I., Lee, S.K., Eds.; Springer: Boston, MA, USA, 2006; pp. 1–5. [Google Scholar]
- Eshghi, F.; Hosseinimehr, S.J.; Rahmani, N.; Khademloo, M.; Norozi, M.S.; Hojati, O. Effects of Aloe vera cream on posthemorrhoidectomy pain and wound healing: Results of a randomized, blind, placebo-control study. J. Altern. Complement. Med. 2010, 16, 647–650. [Google Scholar] [CrossRef]
- Liang, J.; Cui, L.; Li, J.; Guan, S.; Zhang, K.; Li, J. Aloe vera: A medicinal plant used in skin wound healing. Tissue Eng. Part B Rev. 2021, 27, 455–474. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.H.; Donato, J.; Hartman, G.M.; Haas, R.C. Anti-inflammatory and wound healing activity of a growth substance in Aloe vera. J. Am. Podiatr. Med. Assoc. 1994, 84, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.-C.; Kim, S.Y.; Kim, Y.T.; Kim, E.-A.; Lee, S.-H.; Ko, S.-C.; Wijesinghe, W.A.J.P.; Samarakoon, K.W.; Kim, Y.-S.; Cho, J.H.; et al. In vitro and in vivo antioxidant activities of polysaccharide purified from aloe vera (Aloe barbadensis) gel. Carbohydr. Polym. 2014, 99, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Ozsoy, N.; Candoken, E.; Akev, N. Implications for Degenerative Disorders: Antioxidative Activity, Total Phenols, Flavonoids, Ascorbic Acid, β-Carotene and β-Tocopherol inAloe vera. Oxid. Med. Cell. Longev. 2009, 2, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Erichsen-Brown, C. Medicinal and Other Uses of North American Plants: A Historical Survey with Special Reference to the Eastern Indian Tribes; Courier Corporation: Chelmsford, MA, USA, 2013. [Google Scholar]
- Scheffler, A. The Wound Healing Properties of Betulin from Birch Bark from Bench to Bedside. Planta Med. 2019, 85, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Emrich, S.; Schuster, A.; Schnabel, T.; Oostingh, G.J. Antimicrobial Activity and Wound-Healing Capacity of Birch, Beech and Larch Bark Extracts. Molecules 2022, 27, 2817. [Google Scholar] [CrossRef]
- Ebeling, S.; Naumann, K.; Pollok, S.; Wardecki, T.; Vidal-y-Sy, S.; Nascimento, J.M.; Boerries, M.; Schmidt, G.; Brandner, J.M.; Merfort, I. From a Traditional Medicinal Plant to a Rational Drug: Understanding the Clinically Proven Wound Healing Efficacy of Birch Bark Extract. PLoS ONE 2014, 9, e86147. [Google Scholar] [CrossRef]
- Barret, J.P.; Podmelle, F.; Lipový, B.; Rennekampff, H.O.; Schumann, H.; Schwieger-Briel, A.; Zahn, T.R.; Metelmann, H.R. Accelerated re-epithelialization of partial-thickness skin wounds by a topical betulin gel: Results of a randomized phase III clinical trials program. Burns 2017, 43, 1284–1294. [Google Scholar] [CrossRef]
- Frew, Q.; Rennekampff, H.-O.; Dziewulski, P.; Moiemen, N.; Zahn, T.; Hartmann, B. Betulin wound gel accelerated healing of superficial partial thickness burns: Results of a randomized, intra-individually controlled, phase III trial with 12-months follow-up. Burns 2019, 45, 876–890. [Google Scholar] [CrossRef]
- Clevers, H. What is an adult stem cell? Science 2015, 350, 1319–1320. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Discher, D.E.; Peault, B.M.; Phinney, D.G.; Hare, J.M.; Caplan, A.I. Mesenchymal stem cell perspective: Cell biology to clinical progress. NPJ Regen. Med. 2019, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, M.; O’Garra, A. The regulation of IL-10 production by immune cells. Nat. Rev. Immunol. 2010, 10, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Gadani, S.P.; Cronk, J.C.; Norris, G.T.; Kipnis, J. IL-4 in the brain: A cytokine to remember. J. Immunol. 2012, 189, 4213–4219. [Google Scholar] [CrossRef]
- Guillamat-Prats, R. The Role of MSC in Wound Healing, Scarring and Regeneration. Cells 2021, 10, 1729. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, S.-S.; Mohammadi, A.A.; Kabiri, H.; Hashempoor, M.R.; Mahmoodi, M.; Amini, M.; Mehrabani, D. The healing effect of Wharton’s jelly stem cells seeded on biological scaffold in chronic skin ulcers: A randomized clinical trial. J. Cosmet. Dermatol. 2019, 18, 1961–1967. [Google Scholar] [CrossRef]
- Vojtaššák, J.; Danišovič, L.; Kubeš, M.; Bakoš, D.; Jarabek, L.; Uličná, M.; Blaško, M. Autologous biograft and mesenchymal stem cells in treatment of the diabetic foot. Neuroendocrinol. Lett. 2006, 27, 134–137. [Google Scholar] [PubMed]
- Hansen, S.B.; Højgaard, L.D.; Kastrup, J.; Ekblond, A.; Follin, B.; Juhl, M. Optimizing an immunomodulatory potency assay for Mesenchymal Stromal Cell. Front. Immunol. 2022, 13, 1085312. [Google Scholar] [CrossRef]
- Zhou, T.; Yuan, Z.; Weng, J.; Pei, D.; Du, X.; He, C.; Lai, P. Challenges and advances in clinical applications of mesenchymal stromal cells. J. Hematol. Oncol. 2021, 14, 24. [Google Scholar] [CrossRef]
- Nuschke, A. Activity of mesenchymal stem cells in therapies for chronic skin wound healing. Organogenesis 2014, 10, 29–37. [Google Scholar] [CrossRef]
- Lee, D.E.; Ayoub, N.; Agrawal, D.K. Mesenchymal stem cells and cutaneous wound healing: Novel methods to increase cell delivery and therapeutic efficacy. Stem Cell Res. Ther. 2016, 7, 37. [Google Scholar] [CrossRef]
- Goren, I.; Müller, E.; Schiefelbein, D.; Christen, U.; Pfeilschifter, J.; Mühl, H.; Frank, S. Systemic Anti-TNFα Treatment Restores Diabetes-Impaired Skin Repair in ob/ob Mice by Inactivation of Macrophages. J. Investig. Dermatol. 2007, 127, 2259–2267. [Google Scholar] [CrossRef] [PubMed]
- Danon, D.; Madjar, J.; Edinov, E.; Knyszynski, A.; Brill, S.; Diamantshtein, L.; Shinar, E. Treatment of human ulcers by application of macrophages prepared from a blood unit. Exp. Gerontol. 1997, 32, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Zuloff-Shani, A.; Adunsky, A.; Even-Zahav, A.; Semo, H.; Orenstein, A.; Tamir, J.; Regev, E.; Shinar, E.; Danon, D. Hard to heal pressure ulcers (stage III–IV): Efficacy of injected activated macrophage suspension (AMS) as compared with standard of care (SOC) treatment controlled trial. Arch. Gerontol. Geriatr. 2010, 51, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.; Winter, H. Considerations for the Use of Clostridial Collagenase in Clinical Practice. Clin. Drug Investig. 1998, 15, 245–252. [Google Scholar] [CrossRef]
- Alipour, H.; Raz, A.; Zakeri, S.; Dinparast Djadid, N. Therapeutic applications of collagenase (metalloproteases): A review. Asian Pac. J. Trop. Biomed. 2016, 6, 975–981. [Google Scholar] [CrossRef]
- Sheets, A.R.; Demidova-Rice, T.N.; Shi, L.; Ronfard, V.; Grover, K.V.; Herman, I.M. Identification and Characterization of Novel Matrix-Derived Bioactive Peptides: A Role for Collagenase from Santyl® Ointment in Post-Debridement Wound Healing? PLoS ONE 2016, 11, e0159598. [Google Scholar] [CrossRef]
- Tallis, A.; Motley, T.A.; Wunderlich, R.P.; Dickerson, J.E.; Waycaster, C.; Slade, H.B. Clinical and Economic Assessment of Diabetic Foot Ulcer Debridement with Collagenase: Results of a Randomized Controlled Study. Clin. Ther. 2013, 35, 1805–1820. [Google Scholar] [CrossRef]
- Riley, K.N.; Herman, I.M. Collagenase promotes the cellular responses to injury and wound healing in vivo. J. Burn. Wounds 2005, 4, e8. [Google Scholar]
- Koob, T.J.; Rennert, R.; Zabek, N.; Massee, M.; Lim, J.J.; Temenoff, J.S.; Li, W.W.; Gurtner, G. Biological properties of dehydrated human amnion/chorion composite graft: Implications for chronic wound healing. Int. Wound J. 2013, 10, 493–500. [Google Scholar] [CrossRef]
- Tettelbach, W.; Cazzell, S.; Sigal, F.; Caporusso, J.M.; Agnew, P.S.; Hanft, J.; Dove, C. A multicentre prospective randomised controlled comparative parallel study of dehydrated human umbilical cord (EpiCord) allograft for the treatment of diabetic foot ulcers. Int. Wound J. 2019, 16, 122–130. [Google Scholar] [CrossRef]
- Zelen, C.M. An evaluation of dehydrated human amniotic membrane allografts in patients with DFUs. J. Wound Care 2013, 22, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Londahl, M.; Tarnow, L.; Karlsmark, T.; Lundquist, R.; Nielsen, A.M.; Michelsen, M.; Nilsson, A.; Zakrzewski, M.; Jorgensen, B. Use of an autologous leucocyte and platelet-rich fibrin patch on hard-to-heal DFUs: A pilot study. J. Wound Care 2015, 24, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Game, F.; Jeffcoate, W.; Tarnow, L.; Day, F.; Fitzsimmons, D.; Jacobsen, J. The LeucoPatch(R) system in the management of hard-to-heal diabetic foot ulcers: Study protocol for a randomised controlled trial. Trials 2017, 18, 469. [Google Scholar] [CrossRef] [PubMed]
- Game, F.; Jeffcoate, W.; Tarnow, L.; Jacobsen, J.L.; Whitham, D.J.; Harrison, E.F.; Ellender, S.J.; Fitzsimmons, D.; Londahl, M.; LeucoPatch, I.I.t.t. LeucoPatch system for the management of hard-to-heal diabetic foot ulcers in the UK, Denmark, and Sweden: An observer-masked, randomised controlled trial. Lancet Diabetes Endocrinol. 2018, 6, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Embil, J.M.; Nagai, M.K. Becaplermin: Recombinant platelet derived growth factor, a new treatment for healing diabetic foot ulcers. Expert Opin. Biol. Ther. 2002, 2, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Steed, D.L. Clinical evaluation of recombinant human platelet-derived growth factor for the treatment of lower extremity diabetic ulcers. Diabetic Ulcer Study Group. J. Vasc. Surg. 1995, 21, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Smiell, J.M.; Wieman, T.J.; Steed, D.L.; Perry, B.H.; Sampson, A.R.; Schwab, B.H. Efficacy and safety of becaplermin (recombinant human platelet-derived growth factor-BB) in patients with nonhealing, lower extremity diabetic ulcers: A combined analysis of four randomized studies. Wound Repair Regen. 1999, 7, 335–346. [Google Scholar] [CrossRef]
- Pierce, G.F.; Mustoe, T.A.; Senior, R.M.; Reed, J.; Griffin, G.L.; Thomason, A.; Deuel, T.F. In vivo incisional wound healing augmented by platelet-derived growth factor and recombinant c-sis gene homodimeric proteins. J. Exp. Med. 1988, 167, 974–987. [Google Scholar] [CrossRef]
- LeGrand, E.K. Preclinical promise of becaplermin (rhPDGF-BB) in wound healing. Am. J. Surg. 1998, 176, 48s–54s. [Google Scholar] [CrossRef]
- Winterfield, L.; Vleugels, R.A.; Park, K.K. The Value of the Black Box Warning in Dermatology. J. Drugs Dermatol. 2015, 14, 660–666. [Google Scholar]
- Ziyadeh, N.; Fife, D.; Walker, A.M.; Wilkinson, G.S.; Seeger, J.D. A matched cohort study of the risk of cancer in users of becaplermin. Adv. Ski. Wound Care 2011, 24, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, J.D.; Queiroz-Junior, C.M.; Costa, J.E.; Teixeira, A.L.; Silva, T.A. Phenytoin-induced gingival overgrowth: A review of the molecular, immune, and inflammatory features. ISRN Dent. 2011, 2011, 497850. [Google Scholar] [CrossRef] [PubMed]
- Goebel, R.W. Sodium diphenylhydantoin association with oral healing. J. Oral Surg. 1972, 30, 191–195. [Google Scholar] [PubMed]
- Shafer, W.G.; Beatty, R.K.; Davis, W.B. Effect of dilantin sodium on tensile strength of healing wounds. Proc. Soc. Exp. Biol. Med. 1958, 98, 348–350. [Google Scholar] [CrossRef] [PubMed]
- Sayar, H.; Gergerlioglu, N.; Seringec, N.; Ozturk, P.; Bulbuloglu, E.; Karabay, G. Comparison of efficacy of topical phenytoin with hypericin in second-degree burn wound healing: An experimental study in rats. Med. Sci. Monit. Basic Res. 2014, 20, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, P.; Rwanyuma, L.; Mkony, C. A comparison of topical Phenytoin with Silverex in the treatment of superficial dermal burn wounds. Cent. Afr. J. Med. 2002, 48, 105–108. [Google Scholar] [PubMed]
- Inchingolo, F.; Vermesan, D.; Inchingolo, A.D.; Malcangi, G.; Santacroce, L.; Scacco, S.; Benagiano, V.; Girolamo, F.; Cagiano, R.; Caprio, M.; et al. Bedsores successfully treated with topical phenytoin. Acta Biomed. 2017, 88, 45–48. [Google Scholar] [CrossRef]
- Anstead, G.M.; Hart, L.M.; Sunahara, J.F.; Liter, M.E. Phenytoin in wound healing. Ann. Pharmacother. 1996, 30, 768–775. [Google Scholar] [CrossRef]
- Talas, G.; Brown, R.A.; McGrouther, D.A. Role of phenytoin in wound healing—A wound pharmacology perspective. Biochem. Pharmacol. 1999, 57, 1085–1094. [Google Scholar] [CrossRef]
- Moy, L.S.; Tan, E.M.L.; Holness, R.; Uitto, J. Phenytoin Modulates Connective Tissue Metabolism and Cell Proliferation in Human Skin Fibroblast Cultures. Arch. Dermatol. 1985, 121, 79–83. [Google Scholar] [CrossRef]
- Abdelmalek, M.; Spencer, J. Retinoids and Wound Healing. Dermatol. Surg. 2006, 32, 1219–1230. [Google Scholar] [CrossRef] [PubMed]
- Zasada, M.; Budzisz, E. Retinoids: Active molecules influencing skin structure formation in cosmetic and dermatological treatments. Postep. Dermatol. Alergol. 2019, 36, 392–397. [Google Scholar] [CrossRef]
- Wicke, C.; Halliday, B.; Allen, D.; Roche, N.S.; Scheuenstuhl, H.; Spencer, M.M.; Roberts, A.B.; Hunt, T.K. Effects of Steroids and Retinoids on Wound Healing. Arch. Surg. 2000, 135, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Polcz, M.E.; Barbul, A. The Role of Vitamin A in Wound Healing. Nutr. Clin. Pract. 2019, 34, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Leyden, J.; Stein-Gold, L.; Weiss, J. Why Topical Retinoids Are Mainstay of Therapy for Acne. Dermatol. Ther. 2017, 7, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Vagotis, F.L.; Brundage, S.R. Histologic study of dermabrasion and chemical peel in an animal model after pretreatment with Retin-A. Aesthetic Plast. Surg. 1995, 19, 243–246. [Google Scholar] [CrossRef]
- Orringer, J.S.; Kang, S.; Johnson, T.M.; Karimipour, D.J.; Hamilton, T.; Hammerberg, C.; Voorhees, J.J.; Fisher, G.J. Tretinoin treatment before carbon-dioxide laser resurfacing: A clinical and biochemical analysis. J. Am. Acad. Dermatol. 2004, 51, 940–946. [Google Scholar] [CrossRef]
- Tom, W.L.; Peng, D.H.; Allaei, A.; Hsu, D.; Hata, T.R. The effect of short-contact topical tretinoin therapy for foot ulcers in patients with diabetes. Arch. Dermatol. 2005, 141, 1373–1377. [Google Scholar] [CrossRef]
- Paquette, D.; Badiavas, E.; Falanga, V. Short-contact topical tretinoin therapy to stimulate granulation tissue in chronic wounds. J. Am. Acad. Dermatol. 2001, 45, 382–386. [Google Scholar] [CrossRef]
- Watcher, M.A.; Wheeland, R.G. The role of topical agents in the healing of full-thickness wounds. J. Dermatol. Surg. Oncol. 1989, 15, 1188–1195. [Google Scholar] [CrossRef]
- Sakarya, S.; Gunay, N.; Karakulak, M.; Ozturk, B.; Ertugrul, B. Hypochlorous Acid: An ideal wound care agent with powerful microbicidal, antibiofilm, and wound healing potency. Wounds 2014, 26, 342–350. [Google Scholar] [PubMed]
- Gold, M.H.; Andriessen, A.; Bhatia, A.C.; Bitter, P., Jr.; Chilukuri, S.; Cohen, J.L.; Robb, C.W. Topical stabilized hypochlorous acid: The future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J. Cosmet. Dermatol. 2020, 19, 270–277. [Google Scholar] [CrossRef] [PubMed]
- da Costa, M.C.; Ferreira, B.A.; de Moura, F.B.R.; de Lima, L.G.; Araujo, F.d.A.; Mota, F.C.D. Evaluation of 4% stabilized Sodium Hypochlorite activity in the repair of cutaneous excisional wounds in mice. Injury 2021, 52, 2075–2083. [Google Scholar] [CrossRef]
- Dharap, S.B.; Ghag, G.S.; Kulkarni, K.P.; Venkatesh, V. Efficacy and safety of oxum in treatment of the venous ulcer. J. Indian. Med. Assoc. 2008, 106, 326–328. [Google Scholar] [PubMed]
- Jull, A.B.; Arroll, B.; Parag, V.; Waters, J. Pentoxifylline for treating venous leg ulcers. Cochrane Database Syst. Rev. 2012, 12, Cd001733. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Khalili, H. Potential benefits of pentoxifylline on wound healing. Expert. Rev. Clin. Pharmacol. 2016, 9, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Velaei, K.; Bayat, M.; Torkman, G.; Rezaie, F.; Amini, A.; Noruzian, M.; Tavassol, A.; Bayat, M. Evaluating the effects of pentoxifylline administration on experimental pressure sores in rats by biomechanical examinations. Lab. Anim. Res. 2012, 28, 209–215. [Google Scholar] [CrossRef]
- Lim, T.; Taira, B.; Singer, A.; Lin, F.; McClain, S.; Clark, R. 314: Effect of IV Pentoxifylline on Burn Wound Progression. Ann. Emerg. Med. 2009, 54, S98. [Google Scholar] [CrossRef]
- Rawlins, J.M.; Lam, W.L.; Karoo, R.O.; Naylor, I.L.; Sharpe, D.T. Pentoxifylline inhibits mature burn scar fibroblasts in culture. Burns 2006, 32, 42–45. [Google Scholar] [CrossRef]
- Zhao, P.; Sui, B.-D.; Liu, N.; Lv, Y.-J.; Zheng, C.-X.; Lu, Y.-B.; Huang, W.-T.; Zhou, C.-H.; Chen, J.; Pang, D.-L.; et al. Anti-aging pharmacology in cutaneous wound healing: Effects of metformin, resveratrol, and rapamycin by local application. Aging Cell 2017, 16, 1083–1093. [Google Scholar] [CrossRef]
- Qing, L.; Fu, J.; Wu, P.; Zhou, Z.; Yu, F.; Tang, J. Metformin induces the M2 macrophage polarization to accelerate the wound healing via regulating AMPK/mTOR/NLRP3 inflammasome singling pathway. Am. J. Transl. Res. 2019, 11, 655–668. [Google Scholar] [PubMed]
- Han, X.; Tao, Y.; Deng, Y.; Yu, J.; Sun, Y.; Jiang, G. Metformin accelerates wound healing in type 2 diabetic db/db mice. Mol. Med. Rep. 2017, 16, 8691–8698. [Google Scholar] [CrossRef] [PubMed]
- Aragona, M.; Dekoninck, S.; Rulands, S.; Lenglez, S.; Mascre, G.; Simons, B.D.; Blanpain, C. Defining stem cell dynamics and migration during wound healing in mouse skin epidermis. Nat. Commun. 2017, 8, 14684. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.R.; Wang, Y. Drug delivery systems for wound healing. Curr. Pharm. Biotechnol. 2015, 16, 621–629. [Google Scholar] [CrossRef]
- Gaur, N.; Patenall, B.L.; Ghimire, B.; Thet, N.T.; Gardiner, J.E.; Le Doare, K.E.; Ramage, G.; Short, B.; Heylen, R.A.; Williams, C.; et al. Cold Atmospheric Plasma-Activated Composite Hydrogel for an Enhanced and On-Demand Delivery of Antimicrobials. ACS Appl. Mater. Interfaces 2023, 15, 19989–19996. [Google Scholar] [CrossRef]
- Ninan, N.; Forget, A.; Shastri, V.P.; Voelcker, N.H.; Blencowe, A. Antibacterial and Anti-Inflammatory pH-Responsive Tannic Acid-Carboxylated Agarose Composite Hydrogels for Wound Healing. ACS Appl. Mater. Interfaces 2016, 8, 28511–28521. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).