

Endometrial Angiogenesis of Abnormal Uterine Bleeding and Infertility in Patients with Uterine Fibroids—A Systematic Review

 ,
,
Abstract

1. Introduction
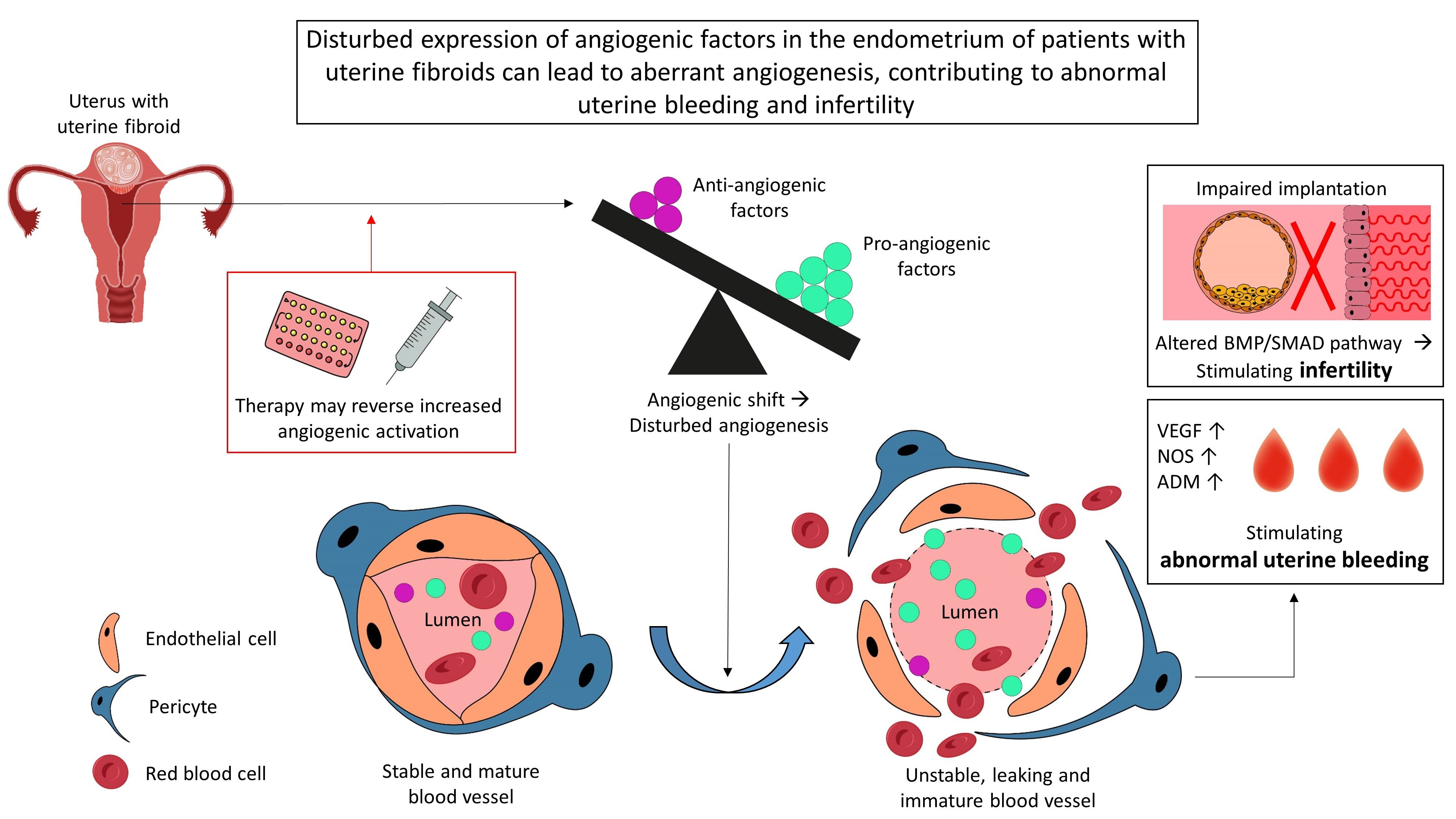
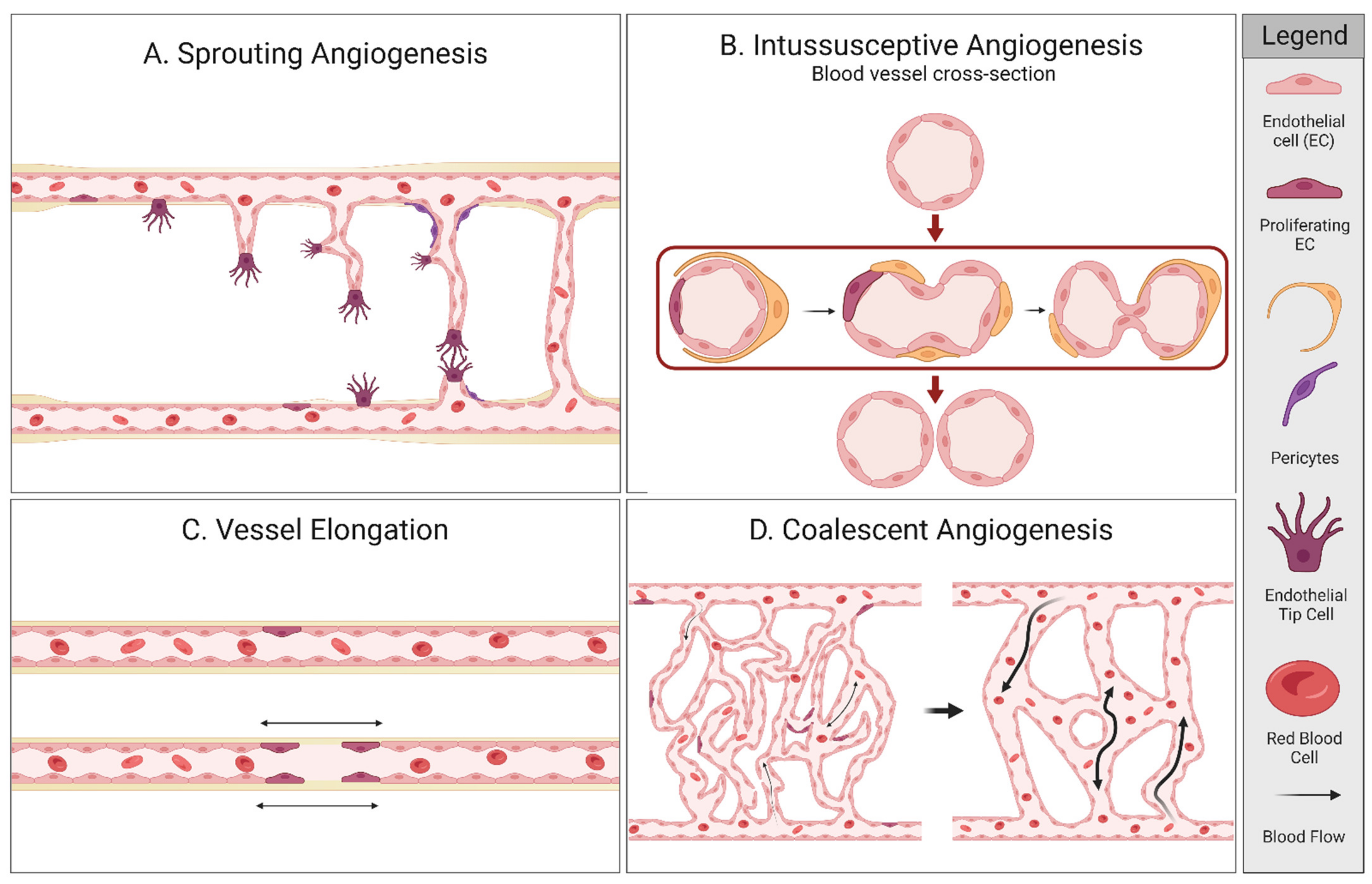
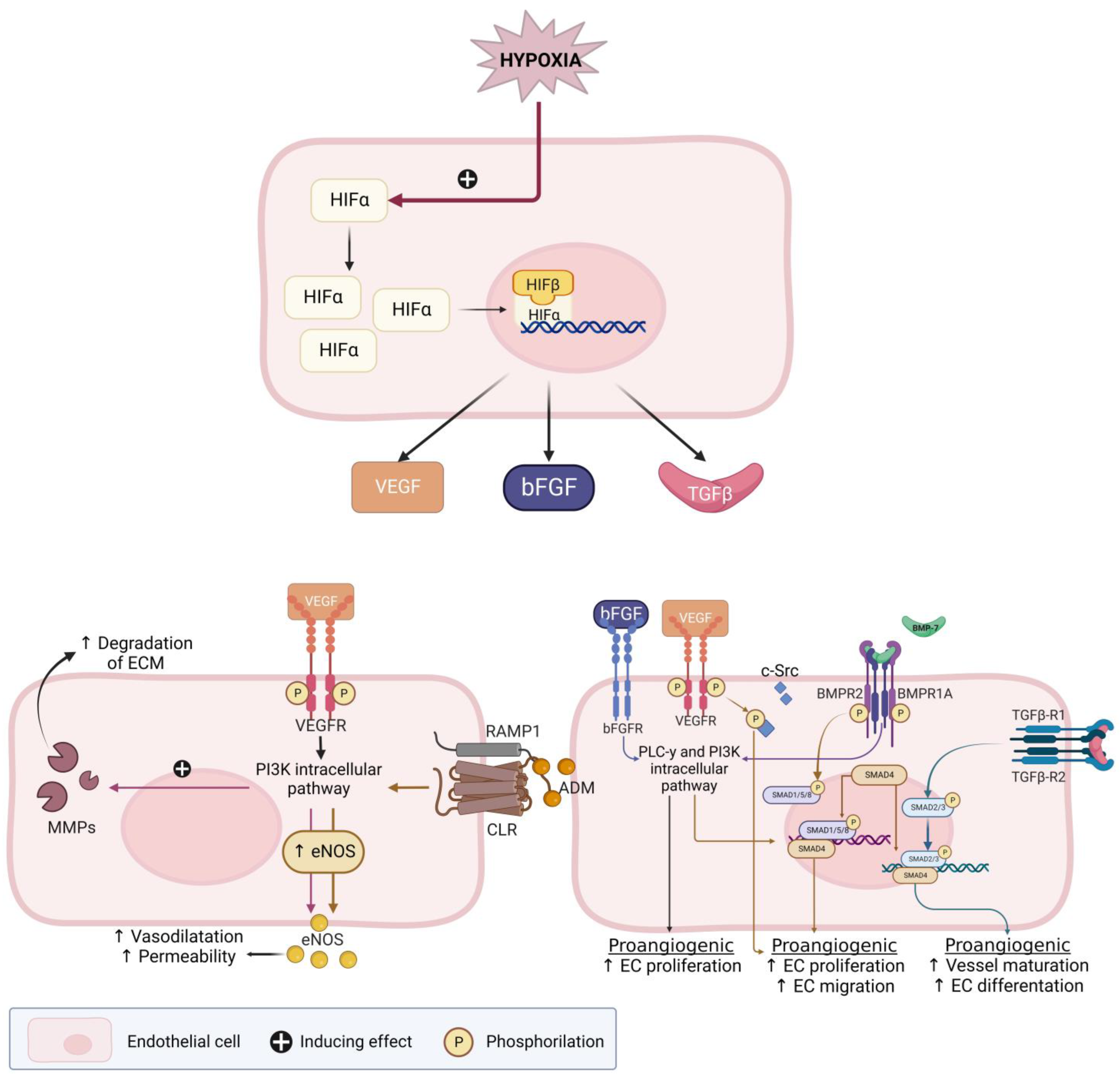
Angiogenesis
2. Materials and Methods
2.1. Protocol Registration
2.2. Data Source and Search Strategy
2.3. Eligibility Criteria and Study Selection
2.4. Data Extraction and Quality Assessment
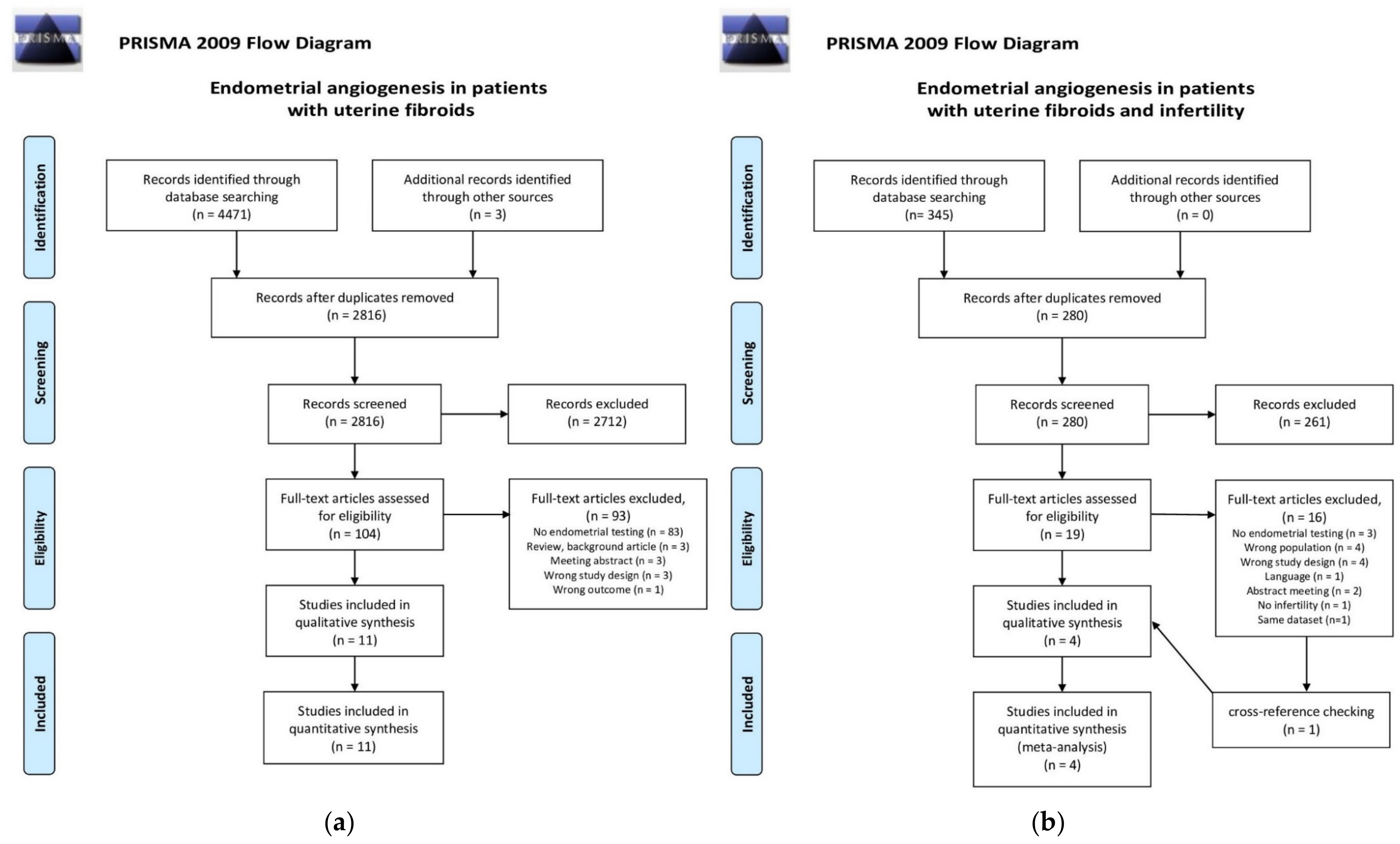
2.5. Study Selection
3. Results
3.1. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Uterine Fibroids (UF), Divided in Four Study Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study, Year | Study Type | Total N | Study Group | Control Group | Matching a | Menstrual Cycle Phase b | Methods c | AUB Classification | |
| 1. Uterine Fibroids | UF | No UF | |||||||
| Bereza et al. 2014 [45] | Retrospective case-control | 22 | 15 | 7 | No | 7 phases | CCT | NA | |
| Hague et al. 2000 [38] | Case-control | 91 | 52 | 39 | Yes | 3 phases | IHC | Subjective complaint of HMB in control group | |
| Governini et al. 2021 [46] | Case-control | 36 | 18 (FIGO type 3) | 18 | Yes | 1 phase (proliferative) | IF; RT-PCR; WB | NA | |
| 2. AUB and UF | UF and AUB | No UF/AUB | |||||||
| Anania et al. 1997 [39] | Case-control | 28 | 14 | 14 | Yes | 3 phases | IHC; RT-PCR; WB | Subjective complaint of HMB | |
| Makhija et al. 2008 [34] | Case-control | 118 | UF: 55 | 63 | No | 5 phases | IHC | Not described | |
| Oh et al. 2013 [35] | Case-control | 32 | UF: 24 Sympt.: 17 Asympt.: 7 | 8 | Yes | 2 phases | IHC | Not described | |
| Zhang et al. 2010 [40] | Case-control | 90 | UF: 60 Sympt.: 29 Asympt.: 31 | 30 | Yes | 2 phases | IHC | Subjective complaint of AUB | |
| 3. Patients with uterine fibroids with and without pharmaceutical therapy | |||||||||
| Study, year | Study type | Total N | Study group with therapy | Control group | Matching a | AUB at start of study (N) d | Methods c | AUB classification | Exogenic hormone e (length of use) |
| Maia et al. 2008 [36] | Retrospective cohort | 118 | 40 | 78 | NA | Study: AUB (9), no MBL(31) Control: HMB + UF | IHC | Not described (indication: hysterectomy) | Continuous Gestinol (1–24 months) |
| Khan et al. 2010a [42] | Prospective case-control | 56 | 20 | 36 | No | Study: HMB Control: HMB | IHC, ELISA | Subjective complaint of AUB | GnRHa (3–6 months) |
| Khan et al. 2010b [41] | Prospective case-control | 56 | 20 | 36 | No | Study: HMB Control: HMB | IHC, BrdU-assay | Subjective complaint of AUB | GnRHa (3–6 months) |
| Kolanska et al. 2019 [37] | Retrospective case-control | 45 | 14 | 27 | No | Not described | IHC | Not described (indication: hysterectomy) | UPA (3 months) |
| 4. Patients with uterine fibroids and infertility | |||||||||
| Study, year | Study type | Total N | Study group | Control group | Matching a | Methods c | Patient sample selection f | ||
| Doherty et al. 2015 [47] | Experimental in vitro study | 14 | 10 | 4 | No | ESCs + FCM exposure; RT-PCR | UF: LCM cultured from patients after myomectomy or hysterectomy. C: ES from fertile controls (no hormonal contraception or uterine pathology) | ||
| Kozachenko et al. 2020 [48] | Prospective case-control | 20 | 10 | 10 | No | IHC | UF: IVF or ICSI indication, ES before and after surgery C: IVF or ICSI indication because of tuboperitoneal infertility factor without endometrial or myometrial pathology | ||
| Novin et al. 2018 [49] | Prospective case-control | 20 | 10 | 10 | No | IHC | UF: infertile patients, which after myomectomy reported a successful pregnancy. C: at least one natural labour, no hormonal contraception or uterine pathology and a normal menstrual cycle | ||
| Sinclair et al. 2011 [50] | Prospective case-control and in vitro study | 24 | 12 | 12 | No | ESC culture; RT-PCR; IHC; ELISA | UF: Endometrial samples after myomectomy for fertility (8) or hysterectomy (4). C: ES after undergoing laparoscopic (7) or hysteroscopic tubal sterilization (5); without evidence of uterine pathology | ||
3.2. Assessment of Risk of Bias
3.3. Summary of Several Angiogenic Pathways
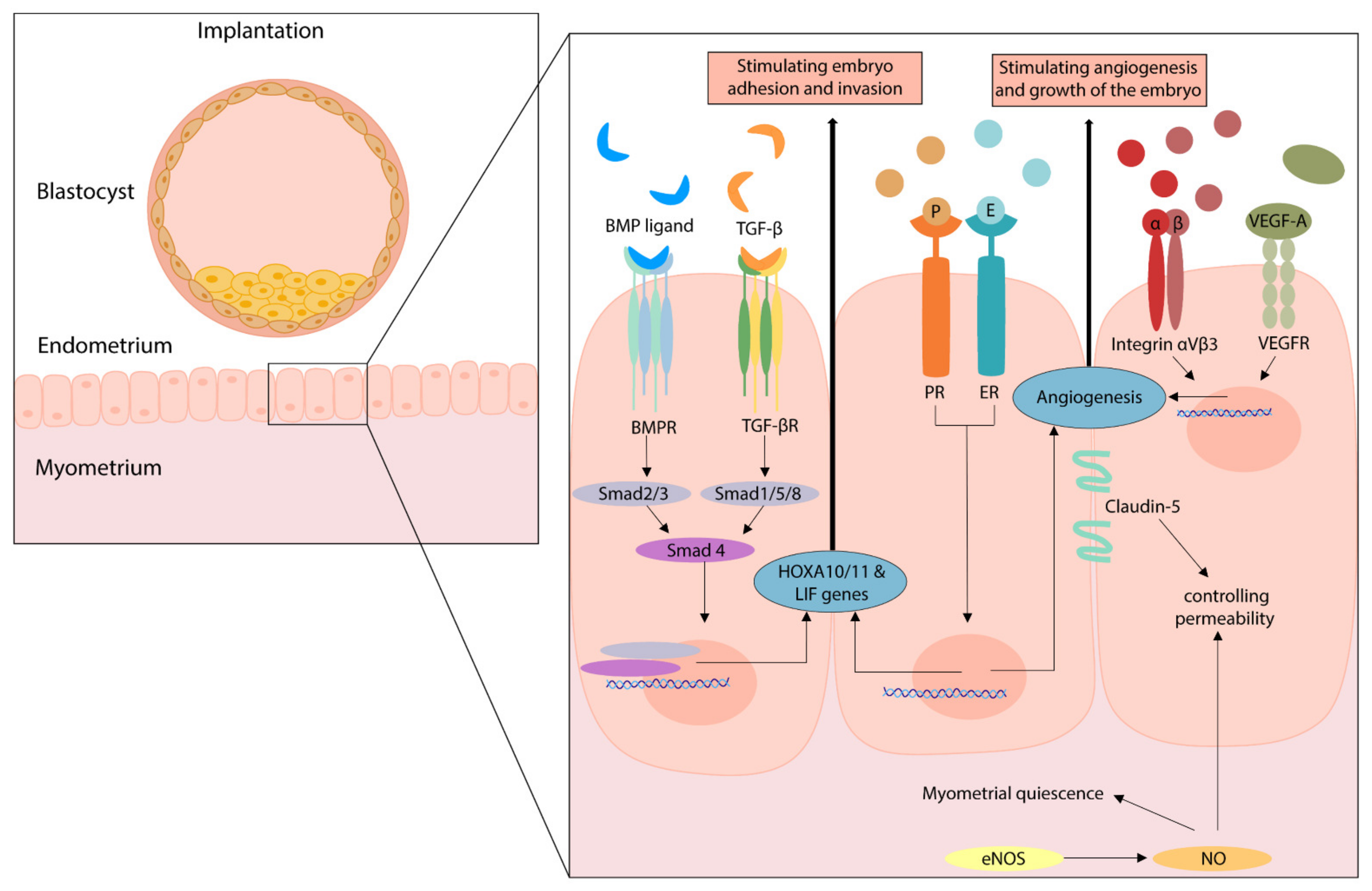
3.4. Summary of Angiogenic Pathways during Implantation
3.5. Results of Individual Studies
3.6. Effects of Pharmaceutical Therapy in Patients with Fibroids
3.7. Angiogenesis in Relation to Fibroids and Infertility
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Selo-Ojeme, D.; Lawal, O.; Shah, J.; Mandal, R.; Pathak, S.; Selo-Ojeme, U.; Samuel, D. The incidence of uterine leiomyoma and other pelvic ultrasonographic findings in 2,034 consecutive women in a north London hospital. J. Obstet. Gynaecol. 2008, 28, 421–423. [Google Scholar] [CrossRef]
- Stewart, E.A.; Laughlin-Tommaso, S.K.; Catherino, W.H.; Lalitkumar, S.; Gupta, D.; Vollenhoven, B. Uterine fibroids. Nat. Rev. Dis. Primers 2016, 2, 16043. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.H. Etiology, symptomatology, and diagnosis of uterine myomas. Fertil. Steril. 2007, 87, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, C.M.; Steiner, C.A. Hysterectomy rates in the United States 1990–1997. Obstet. Gynecol. 2002, 99, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Wright, K.N.; Jonsdottir, G.M.; Jorgensen, S.; Shah, N.; Einarsson, J.I. Costs and outcomes of abdominal, vaginal, laparoscopic and robotic hysterectomies. JSLS 2012, 16, 519–524. [Google Scholar] [CrossRef]
- Munro, M.G.; Critchley, H.O.; Broder, M.S.; Fraser, I.S.; Disorders, F.W.G.o.M. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int. J. Gynaecol. Obstet. 2011, 113, 3–13. [Google Scholar] [CrossRef]
- Munro, M.G.; Critchley, H.O.D.; Fraser, I.S.; Committee, F.M.D. The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int. J. Gynaecol. Obstet. 2018, 143, 393–408. [Google Scholar] [CrossRef]
- National Collaborating Centre for Centre for Women’s and Children’s Health. National Institute for Health and Clinical Excellence: Guidance. In Heavy Menstrual Bleeding; RCOG Press, National Collaborating Centre for Women’s and Children’s Health: London, UK, 2007. [Google Scholar]
- NICE. NICE Guideline: Heavy Menstrual Bleeding: Assessment and Management; NICE: London, UK, 2018. [Google Scholar]
- Navarro, A.; Bariani, M.V.; Yang, Q.; Al-Hendy, A. Understanding the Impact of Uterine Fibroids on Human Endometrium Function. Front. Cell. Dev. Biol. 2021, 9, 633180. [Google Scholar] [CrossRef]
- Cetin, E.; Al-Hendy, A.; Ciebiera, M. Non-hormonal mediators of uterine fibroid growth. Curr. Opin. Obstet. Gynecol. 2020, 32, 361–370. [Google Scholar] [CrossRef]
- Deligdish, L.; Loewenthal, M. Endometrial changes associated with myomata of the uterus. J. Clin. Pathol. 1970, 23, 676–680. [Google Scholar] [CrossRef]
- Buttram, V.C., Jr.; Reiter, R.C. Uterine leiomyomata: Etiology, symptomatology, and management. Fertil. Steril. 1981, 36, 433–445. [Google Scholar] [CrossRef]
- Dudley, A.C.; Griffioen, A.W. Targeting pathological angiogenesis: Mechanisms and therapeutic strategies. Angiogenesis 2023, in press. [Google Scholar]
- Yetkin-Arik, B.; Kastelein, A.W.; Klaassen, I.; Jansen, C.; Latul, Y.P.; Vittori, M.; Biri, A.; Kahraman, K.; Griffioen, A.W.; Amant, F.; et al. Angiogenesis in gynecological cancers and the options for anti-angiogenesis therapy. Biochim. Biophys. Acta Rev. Cancer 2021, 1875, 188446. [Google Scholar] [CrossRef]
- Latacz, E.; Caspani, E.; Barnhill, R.; Lugassy, C.; Verhoef, C.; Grunhagen, D.; Van Laere, S.; Fernandez Moro, C.; Gerling, M.; Dirix, M.; et al. Pathological features of vessel co-option versus sprouting angiogenesis. Angiogenesis 2020, 23, 43–54. [Google Scholar] [CrossRef]
- Rogers, P.A.; Gargett, C.E. Endometrial angiogenesis. Angiogenesis 1998, 2, 287–294. [Google Scholar] [CrossRef]
- Nitzsche, B.; Rong, W.W.; Goede, A.; Hoffmann, B.; Scarpa, F.; Kuebler, W.M.; Secomb, T.W.; Pries, A.R. Coalescent angiogenesis-evidence for a novel concept of vascular network maturation. Angiogenesis 2022, 25, 35–45. [Google Scholar] [CrossRef]
- Adair, T.H.; Montani, J.P. Overview of Angiogenesis. In Angiogenesis; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2010. [Google Scholar]
- Gambino, L.S.; Wreford, N.G.; Bertram, J.F.; Dockery, P.; Lederman, F.; Rogers, P.A. Angiogenesis occurs by vessel elongation in proliferative phase human endometrium. Hum. Reprod. 2002, 17, 1199–1206. [Google Scholar] [CrossRef]
- Pezzella, F.; Kerbel, R.S. On coalescent angiogenesis and the remarkable flexibility of blood vessels. Angiogenesis 2022, 25, 1–3. [Google Scholar] [CrossRef]
- Girling, J.E.; Rogers, P.A. Recent advances in endometrial angiogenesis research. Angiogenesis 2005, 8, 89–99. [Google Scholar] [CrossRef]
- Möller, B.; Rasmussen, C.H.; Lindblom, B.; Olovsson, M. Expression of the angiogenic growth factors VEGF, FGF-2, EGF and their receptors in normal human endometrium during the menstrual cycle. Mol. Hum. Reprod. 2001, 7, 65–72. [Google Scholar] [CrossRef]
- Burton, G.J.; Charnock-Jones, D.S.; Jauniaux, E. Regulation of vascular growth and function in the human placenta. Reproduction 2009, 138, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Middelkoop, M.A.; Don, E.E.; Hehenkamp, W.J.K.; Polman, N.J.; Griffioen, A.W.; Huirne, J.A.F. Angiogenesis in abnormal uterine bleeding: A narrative review. Hum. Reprod. Update 2023, dmad004. [Google Scholar] [CrossRef] [PubMed]
- Harmsen, M.J.; Wong, C.F.C.; Mijatovic, V.; Griffioen, A.W.; Groenman, F.; Hehenkamp, W.J.K.; Huirne, J.A.F. Role of angiogenesis in adenomyosis-associated abnormal uterine bleeding and subfertility: A systematic review. Hum. Reprod. Update 2019, 25, 647–671. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, L.; Paludan-Müller, A.S.; Laursen, D.R.; Savović, J.; Boutron, I.; Sterne, J.A.; Higgins, J.P.; Hróbjartsson, A. Evaluation of the Cochrane tool for assessing risk of bias in randomized clinical trials: Overview of published comments and analysis of user practice in Cochrane and non-Cochrane reviews. Syst. Rev. 2016, 5, 80. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Conell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 July 2022).
- World Health Organization. Reproductive Health Indicators—Guidelines for Their Generation, Interpretation and Analysis for Global Monitoring; Press, W., Ed.; World Health Organization: Geneva, Switzerland, 2006; p. 67.
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Makhija, D.; Mathai, A.M.; Naik, R.; Kumar, S.; Rai, S.; Pai, M.R.; Baliga, P. Morphometric evaluation of endometrial blood vessels. Indian. J. Pathol. Microbiol. 2008, 51, 346–350. [Google Scholar] [CrossRef]
- Oh, N.J.; Ryu, K.Y.; Jung, C.N.; Yi, S.Y.; Kim, S.R. Expression of endothelial nitric oxide synthase in the uterus of patients with leiomyoma or adenomyosis. J. Obstet. Gynaecol. Res. 2013, 39, 536–542. [Google Scholar] [CrossRef]
- Maia, H., Jr.; Casoy, J.; Pimentel, K.; Correia, T.; Athayde, C.; Cruz, T.; Coutinho, E.M. Effect of oral contraceptives on vascular endothelial growth factor, Cox-2 and aromatase expression in the endometrium of uteri affected by myomas and associated pathologies. Contraception 2008, 78, 479–485. [Google Scholar] [CrossRef]
- Kolanska, K.; Varinot, J.; Canlorbe, G.; Bergeron, C.; Mekinian, A.; Capmas, P.; Koskas, M.; Darai, E.; Aractingi, S.; Bendifallah, S.; et al. Absence of predictable long-term molecular effect of ulipristal acetate (UPA) on the endometrium. Reprod. Biomed. Online 2019, 38, 825–834. [Google Scholar] [CrossRef]
- Hague, S.; Zhang, L.; Oehler, M.K.; Manek, S.; MacKenzie, I.Z.; Bicknell, R.; Rees, M.C. Expression of the hypoxically regulated angiogenic factor adrenomedullin correlates with uterine leiomyoma vascular density. Clin. Cancer Res. 2000, 6, 2808–2814. [Google Scholar]
- Anania, C.A.; Stewart, E.A.; Quade, B.J.; Hill, J.A.; Nowak, R.A. Expression of the fibroblast growth factor receptor in women with leiomyomas and abnormal uterine bleeding. Mol. Hum. Reprod. 1997, 3, 685–691. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Zhu, S.J.; Jia, W.J. Expressions and significance of VEGF and MMP-2 in endometrium of patients with sympotomatic uterine leiomyomas. Chin. Journal. Cancer Prev. Treat. 2010, 17, 1942–1945. [Google Scholar]
- Khan, K.N.; Kitajima, M.; Hiraki, K.; Fujishita, A.; Nakashima, M.; Ishimaru, T.; Masuzaki, H. Cell proliferation effect of GnRH agonist on pathological lesions of women with endometriosis, adenomyosis and uterine myoma. Hum. Reprod. 2010, 25, 2878–2890. [Google Scholar] [CrossRef]
- Khan, K.N.; Kitajima, M.; Hiraki, K.; Fujishita, A.; Sekine, I.; Ishimaru, T.; Masuzaki, H. Changes in tissue inflammation, angiogenesis and apoptosis in endometriosis, adenomyosis and uterine myoma after GnRH agonist therapy. Hum. Reprod. 2010, 25, 642–653. [Google Scholar] [CrossRef]
- Noyes, R.W.; Hertig, A.T.; Rock, J. Reprint of: Dating the Endometrial Biopsy. Fertil. Steril. 2019, 112, e93–e115. [Google Scholar] [CrossRef]
- Fox, H.; Buckley, C.H. Endometrium. In Atlas of Gynaecological Pathology, 5th ed.; Gresham, G.A., Ed.; Current Histopathology; Springer: Dordrecht, The Netherlands, 1983; pp. 61–63. [Google Scholar]
- Bereza, T.; Tomaszewski, K.A.; Lis, G.J.; Mizia, E.; Pasternak, A.; Mazur, M.; Mituś, J. ‘Venous lakes’—A corrosion cast scanning electron microscopy study of regular and myomatous human uterine blood vessels. Folia Morphol. 2014, 73, 164–168. [Google Scholar] [CrossRef]
- Governini, L.; Marrocco, C.; Semplici, B.; Pavone, V.; Belmonte, G.; Luisi, S.; Petraglia, F.; Luddi, A.; Piomboni, P. Extracellular matrix remodeling and inflammatory pathway in human endometrium: Insights from uterine leiomyomas. Fertil. Steril. 2021, 116, 1404–1414. [Google Scholar] [CrossRef]
- Doherty, L.F.; Taylor, H.S. Leiomyoma-derived transforming growth factor-beta impairs bone morphogenetic protein-2-mediated endometrial receptivity. Fertil. Steril. 2015, 103, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Kozachenko, I.F.; Faizullina, N.M.; Shchegolev, A.I.; Adamyan, L.V. Endometrial receptivity in patients with benign uterine diseases and infertility before and after surgery. Akusherstvo Ginekol./Obstet. Gynecol. 2020, 2020, 147–158. (In Russian) [Google Scholar] [CrossRef]
- Novin, M.G.; Moini, A.; Niknezhad, S.; Najafi, T.; Novin, M.G. Immunohistochemical localization of endothelial nitric oxide synthase in endometrial tissues of women with uterine myomas. Int. J. Women’s Health Reprod. Sci. 2018, 6, 263–268. [Google Scholar] [CrossRef]
- Sinclair, D.C.; Mastroyannis, A.; Taylor, H.S. Leiomyoma simultaneously impair endometrial BMP-2-mediated decidualization and anticoagulant expression through secretion of TGF-beta3. J. Clin. Endocrinol. Metab. 2011, 96, 412–421. [Google Scholar] [CrossRef]
- Hillen, F.; Griffioen, A.W. Tumour vascularization: Sprouting angiogenesis and beyond. Cancer Metastasis Rev. 2007, 26, 489–502. [Google Scholar] [CrossRef]
- Khorram, O.; Garthwaite, M.; Magness, R.R. Endometrial and myometrial expression of nitric oxide synthase isoforms in pre- and postmenopausal women. J. Clin. Endocrinol. Metab. 1999, 84, 2226–2232. [Google Scholar] [CrossRef]
- Wong, H.K.; Cheung, T.T.; Cheung, B.M. Adrenomedullin and cardiovascular diseases. JRSM Cardiovasc. Dis. 2012, 1, 14. [Google Scholar] [CrossRef]
- Griffioen, A.W.; Molema, G. Angiogenesis: Potentials for pharmacologic intervention in the treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol. Rev. 2000, 52, 237–268. [Google Scholar]
- Lai, T.H.; Vlahos, N.; Shih Ie, M.; Zhao, Y. Expression Patterns of VEGF and Flk-1 in Human Endometrium during the Menstrual Cycle. J. Reprod. Infertil. 2015, 16, 3–9. [Google Scholar]
- Kitamura, K.; Kangawa, K.; Kawamoto, M.; Ichiki, Y.; Nakamura, S.; Matsuo, H.; Eto, T. Adrenomedullin: A novel hypotensive peptide isolated from human pheochromocytoma. Biochem. Biophys. Res. Commun. 1993, 192, 553–560. [Google Scholar] [CrossRef]
- Nikitenko, L.L.; MacKenzie, I.Z.; Rees, M.C.; Bicknell, R. Adrenomedullin is an autocrine regulator of endothelial growth in human endometrium. Mol. Hum. Reprod. 2000, 6, 811–819. [Google Scholar] [CrossRef]
- Nikitenko, L.L.; Smith, D.M.; Hague, S.; Wilson, C.R.; Bicknell, R.; Rees, M.C. Adrenomedullin and the microvasculature. Trends Pharmacol. Sci. 2002, 23, 101–103. [Google Scholar] [CrossRef]
- Ha, C.; Stavreus-Evers, A.; Landgren, B.M.; Mints, M.; Rees, M.C. Adrenomedullin and its receptor, calcitonin receptor-like receptor, are aberrantly expressed in women with idiopathic menorrhagia. Mol. Med. Rep. 2009, 2, 7–11. [Google Scholar] [CrossRef]
- Smith, O.P.; Jabbour, H.N.; Critchley, H.O. Cyclooxygenase enzyme expression and E series prostaglandin receptor signalling are enhanced in heavy menstruation. Hum. Reprod. 2007, 22, 1450–1456. [Google Scholar] [CrossRef]
- Richards, E.G.; El-Nashar, S.A.; Schoolmeester, J.K.; Keeney, G.L.; Mariani, A.; Hopkins, M.R.; Dowdy, S.C.; Daftary, G.S.; Famuyide, A.O. Abnormal Uterine Bleeding Is Associated With Increased BMP7 Expression in Human Endometrium. Reprod. Sci. 2017, 24, 671–681. [Google Scholar] [CrossRef]
- Tian, M.; Neil, J.R.; Schiemann, W.P. Transforming growth factor-beta and the hallmarks of cancer. Cell. Signal. 2011, 23, 951–962. [Google Scholar] [CrossRef]
- Luddi, A.; Marrocco, C.; Governini, L.; Semplici, B.; Pavone, V.; Capaldo, A.; Tosti, C.; Greco, S.; Luisi, S.; Ciarmela, P.; et al. Increased expression of neurogenic factors in uterine fibroids. Hum. Reprod. 2019, 34, 2153–2162. [Google Scholar] [CrossRef]
- Buxton, I.L. Regulation of uterine function: A biochemical conundrum in the regulation of smooth muscle relaxation. Mol. Pharmacol. 2004, 65, 1051–1059. [Google Scholar] [CrossRef]
- Ota, H.; Igarashi, S.; Hatazawa, J.; Tanaka, T. Endothelial nitric oxide synthase in the endometrium during the menstrual cycle in patients with endometriosis and adenomyosis. Fertil. Steril. 1998, 69, 303–308. [Google Scholar] [CrossRef]
- Najafi, T.; Novin, M.G.; Ghazi, R.; Khorram, O. Altered endometrial expression of endothelial nitric oxide synthase in women with unexplained recurrent miscarriage and infertility. Reprod. Biomed. Online 2012, 25, 408–414. [Google Scholar] [CrossRef]
- Avraamides, C.J.; Garmy-Susini, B.; Varner, J.A. Integrins in angiogenesis and lymphangiogenesis. Nat. Rev. Cancer 2008, 8, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Hodivala-Dilke, K. αvβ3 integrin and angiogenesis: A moody integrin in a changing environment. Curr. Opin. Cell. Biol. 2008, 20, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.Y.; Jeong, J.W.; Wang, J.; Ma, L.; Martin, J.F.; Tsai, S.Y.; Lydon, J.P.; DeMayo, F.J. Bmp2 is critical for the murine uterine decidual response. Mol. Cell. Biol. 2007, 27, 5468–5478. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.K. Regulation of angiogenesis in the endometrium. Trends Endocrinol. Metab. 2001, 12, 147–151. [Google Scholar] [CrossRef]
- Godoy Morales, H.S.G.H.; Paz Martinez, A.d.J.P.A.; Mamani Cancino, A.D.M.A.; Lozano Sánchez, J.M.L.J.; Romo Aguirre, C.R.C.; Montaño, L.F.M.L. Claudin 5 as a marker of endometrial receptivity in patients with previous implantation failure. Fertil. Steril. 2013, 100, S393. [Google Scholar] [CrossRef]
- Hlatky, L.; Hahnfeldt, P.; Folkman, J. Clinical Application of Antiangiogenic Therapy: Microvessel Density, What It Does and Doesn’t Tell Us. JNCI J. Natl. Cancer Inst. 2002, 94, 883–893. [Google Scholar] [CrossRef]
- Jabbour, H.N.; Kelly, R.W.; Fraser, H.M.; Critchley, H.O. Endocrine regulation of menstruation. Endocr. Rev. 2006, 27, 17–46. [Google Scholar] [CrossRef]
- Donoghue, J.F.; McGavigan, C.J.; Lederman, F.L.; Cann, L.M.; Fu, L.; Dimitriadis, E.; Girling, J.E.; Rogers, P.A. Dilated thin-walled blood and lymphatic vessels in human endometrium: A potential role for VEGF-D in progestin-induced break-through bleeding. PLoS ONE 2012, 7, e30916. [Google Scholar] [CrossRef]
- Ravet, S.; Munaut, C.; Blacher, S.; Brichant, G.; Labied, S.; Beliard, A.; Chabbert-Buffet, N.; Bouchard, P.; Foidart, J.M.; Pintiaux, A. Persistence of an intact endometrial matrix and vessels structure in women exposed to VA-2914, a selective progesterone receptor modulator. J. Clin. Endocrinol. Metab. 2008, 93, 4525–4531. [Google Scholar] [CrossRef][Green Version]
- Frijlingh, M.; De Milliano, I.; Hehenkamp, W.J.K.; Huirne, J.A.F. Differences in fibroid vascularity after three months of pre-treatment with leuprolide acetate or ulipristal acetate: A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 186–192. [Google Scholar] [CrossRef]
- Horne, A.W.; Critchley, H.O. The effect of uterine fibroids on embryo implantation. Semin. Reprod. Med. 2007, 25, 483–489. [Google Scholar] [CrossRef]
- Cakmak, H.; Taylor, H.S. Implantation failure: Molecular mechanisms and clinical treatment. Hum. Reprod. Update 2011, 17, 242–253. [Google Scholar] [CrossRef]
- Donaghay, M.; Lessey, B.A. Uterine receptivity: Alterations associated with benign gynecological disease. Semin. Reprod. Med. 2007, 25, 461–475. [Google Scholar] [CrossRef]
- Blumenthal, R.D.; Taylor, A.P.; Goldman, L.; Brown, G.; Goldenberg, D.M. Abnormal expression of the angiopoietins and Tie receptors in menorrhagic endometrium. Fertil. Steril. 2002, 78, 1294–1300. [Google Scholar] [CrossRef]




| A. Sprouting Angiogenesis | B. Intussusceptive Angiogenesis | C. Vessel Elongation | D. Coalescent Angiogenesis | |
|---|---|---|---|---|
| Process | Vessel growth from existing vessels by initiation of tip cells | An initial vessel splits into two daughter vessels | Passive cell growth, whereas a vessel widens and/or extends | Capillary mesh fusion by parallel processes of vessel maturation and regression |
| Stimulant | Hypoxia, growth factors | Growth factors, shear stress | Metabolic signals of surrounding cells | Shear stress |
| Vessel perfusion | Only after completion | Continuous | Continuous | Continuous |
| Growth rate | Slow | Fast | Fast | Fast |
| (Possible) Effect on vascular morphology a | ↑ MVD | ↑ MVD | =/↑ MVD | =/↓ MVD ↑ Vessel diameter b |
| Search I | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Premenopausal patients With fibroids and/or AUB With and without of exogenous hormones | Uterine abnormalities other than fibroid(s). |
| Intervention | In vitro experiment with non-human cells | |
| Outcomes | Angiogenic factors in endometrium Vascular characteristics | Menstrual effluent Serum levels |
| Study design | Randomized Controlled Trial Case control Cohort study | Meta-analysis Case reports Reviews |
| Search II | Inclusion Criteria | Exclusion Criteria |
| Population | Premenopausal patients With fibroids With infertility | Uterine abnormalities other than fibroid(s). |
| Intervention | In vitro experiment with non-human cells | |
| Outcomes | Angiogenic factors in endometrium Vascular characteristics | Menstrual effluent Serum levels |
| Study design | Randomized controlled trial Case control Cohort study | Meta-analysis Case reports Reviews |
| Uterine Fibroids (UF) Compared to Normal Controls | Abnormal Uterine Blood (AUB) Loss and UF Compared to Normal Controls | Studies [Reference Citation Number] | ||
|---|---|---|---|---|
| Angiogenic parameters | Outcomes a | Outcomes a in the proliferative phase | Outcomes a in the secretory phase | |
| ADM | ↑ | Hague et al. 2000 [38] | ||
| aFGF | = | Hague et al. 2000 [38] | ||
| bFGF | = | Hague et al. 2000 [38] | ||
| COX1 | = b | Governini et al. 2021 [46] | ||
| COX2 | = b | Governini et al. 2021 [46] | ||
| eNOS | ↑ | ↑ c | Oh et al. 2013 [35] | |
| FGF-R1 | = | ↑a | Anania et al. 1997 [39] | |
| IL-1β/6/10 | ↓ | Governini et al. 2021 [46] | ||
| STAT3 | = b | Governini et al. 2021 [46] | ||
| VEGF | ↑/= b | ↑ | ↑ d | UF: Hague et al. 2000 [38] Governini et al. 2021 [46] AUB & UF: Zhang et al. 2010 [40] |
| Vascular morphology outcomes a | ||||
| MVD (by H&E) e | = | = | UF: Hague et al. 2000 [38] AUB & UF: Makhija et al. 2008 [34] | |
| Vessel diameter | = | Makhija et al. 2008 [34] | ||
| Venous lakes | ↑ | Bereza et al. 2014 [45] | ||
| Vascular congestion | = | Makhija et al. 2008 [34] | ||
| Angiogenic Parameters a | Studies b [Reference Citation Number] | ||
|---|---|---|---|
| Comparison: patients with AUB and UF with and without continuous Gestinol b,c | |||
| Angiogenic factor | Outcomes d | ||
| VEGF | ↓ | Maia et al. 2008 [36] | |
| Aromatase | ↓ f | Maia et al. 2008 [36] | |
| COX-2 A vs. C b BTB vs. C b BTB vs. no MBL b,e | Proliferative phase | Secretory phase | Maia et al. 2008 [36] Maia et al. 2008 [36] Maia et al. 2008 [36] |
| ↓ | = | ||
| = | ↑ | ||
| ↑ | |||
| Comparison: patients with AUB, UF and GnRHa compared to patients with AUB and without UF and GnRHa b,c | |||
| Vessel | Outcomes d | ||
| MVD (vWF) | ↓ | Khan et al. 2010a [42] | |
| Macrophages infiltration (CD68) | ↓ | Khan et al. 2010a [42] | |
| MCP-1 | ↓ | Khan et al. 2010a [42] | |
| Proliferation (Ki67) | |||
| Endothelial cell | ↓ | Khan et al. 2010b [41] | |
| Epithelial and stromal cell | ↓ | Khan et al. 2010b [41] | |
| Comparison: patients with AUB, UF and UPA compared to patients with NMB and without UF and UPA b,c | |||
| Angiogenic factor | Outcomes d | ||
| VEGFR2 | = | Kolanska et al. 2019 [37] | |
| ER | ↑ | Kolanska et al. 2019 [37] | |
| PR | ↑ | Kolanska et al. 2019 [37] | |
| Proliferation (Ki67) | Proliferative phase | Secretory phase | |
| Epithelial cell | ↓ g | ↑ g | Kolanska et al. 2019 [37] |
| Stromal cell | ↓ g | = g | Kolanska et al. 2019 [37] |
| Angiogenic Arameters a | Outcomes b | Studies [Reference Citation Number] |
|---|---|---|
| BMP-2 | ↓ | Sinclair et al. 2011 [50] |
| BMPR-1A | = ↓ | Doherty et al. 2015 [47] Sinclair et al. 2011 [50] |
| BMPR-1B | ↓ | Doherty et al. 2015, Sinclair et al. 2011 [47,50] |
| BMPR-2 | ↓ | Doherty et al. 2015, Sinclair et al. 2011 [47,50] |
| CLDN-5 | ↓ | Kozachenko et al. 2020 [48] |
| eNOS | ↑ | Novin et al. 2018 [49] |
| Estradiol receptor (ER) | ↓ | Kozachenko et al. 2020 [48] |
| HOXA10 | ↓ = | Doherty et al. 2015 [47] Kozachenko et al. 2020 [48] |
| HOXA11 | ↓ | Kozachenko et al. 2020 [48] |
| Integrin αVβ3 | ↓ | Kozachenko et al. 2020 [48] |
| LIF | ↓ | Doherty et al. 2015, Kozachenko et al. 2020 [47,48] |
| Progesterone receptor (PR) | ↓ | Kozachenko et al. 2020 [48] |
| SPEI (PR/ER) | = | Kozachenko et al. 2020 [48] |
| VEGF-A | ↓ | Kozachenko et al. 2020 [48] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Don, E.E.; Middelkoop, M.-A.; Hehenkamp, W.J.K.; Mijatovic, V.; Griffioen, A.W.; Huirne, J.A.F. Endometrial Angiogenesis of Abnormal Uterine Bleeding and Infertility in Patients with Uterine Fibroids—A Systematic Review. Int. J. Mol. Sci. 2023, 24, 7011. https://doi.org/10.3390/ijms24087011
Don EE, Middelkoop M-A, Hehenkamp WJK, Mijatovic V, Griffioen AW, Huirne JAF. Endometrial Angiogenesis of Abnormal Uterine Bleeding and Infertility in Patients with Uterine Fibroids—A Systematic Review. International Journal of Molecular Sciences. 2023; 24(8):7011. https://doi.org/10.3390/ijms24087011
Chicago/Turabian StyleDon, Emma E., Mei-An Middelkoop, Wouter J. K. Hehenkamp, Velja Mijatovic, Arjan W. Griffioen, and Judith A. F. Huirne. 2023. "Endometrial Angiogenesis of Abnormal Uterine Bleeding and Infertility in Patients with Uterine Fibroids—A Systematic Review" International Journal of Molecular Sciences 24, no. 8: 7011. https://doi.org/10.3390/ijms24087011
APA StyleDon, E. E., Middelkoop, M.-A., Hehenkamp, W. J. K., Mijatovic, V., Griffioen, A. W., & Huirne, J. A. F. (2023). Endometrial Angiogenesis of Abnormal Uterine Bleeding and Infertility in Patients with Uterine Fibroids—A Systematic Review. International Journal of Molecular Sciences, 24(8), 7011. https://doi.org/10.3390/ijms24087011