
Bone Marrow-Derived Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects of the Knee in Animal Models: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Results
2.1. Study Characteristics
2.2. Histological Scores
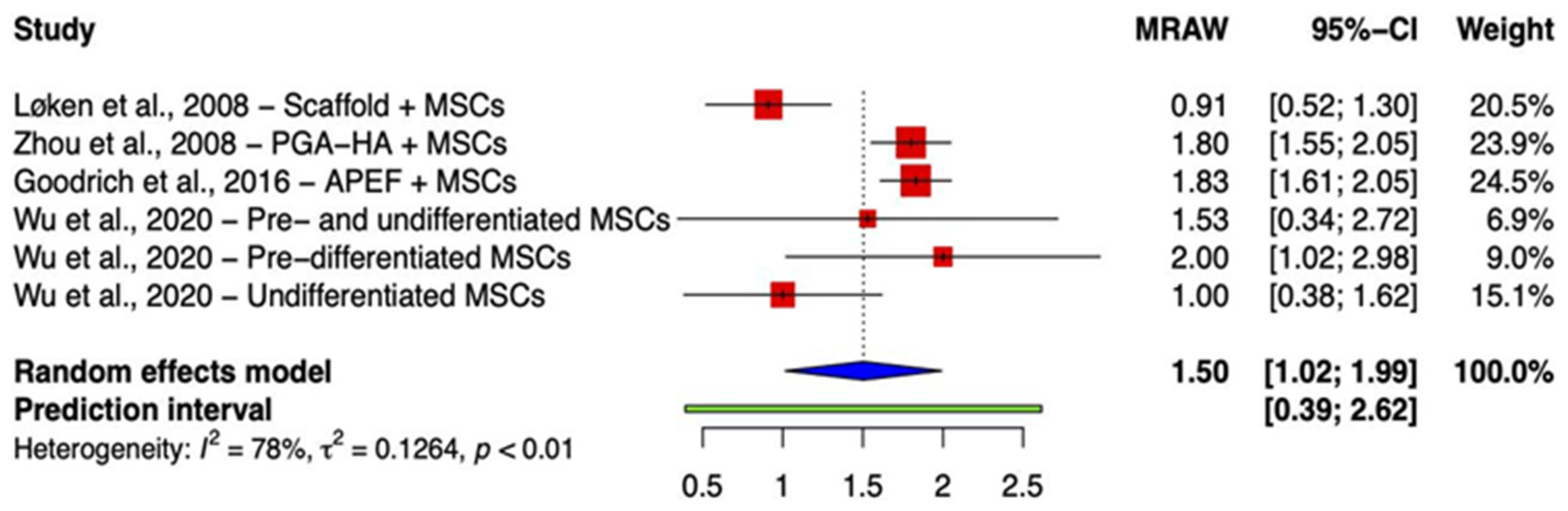
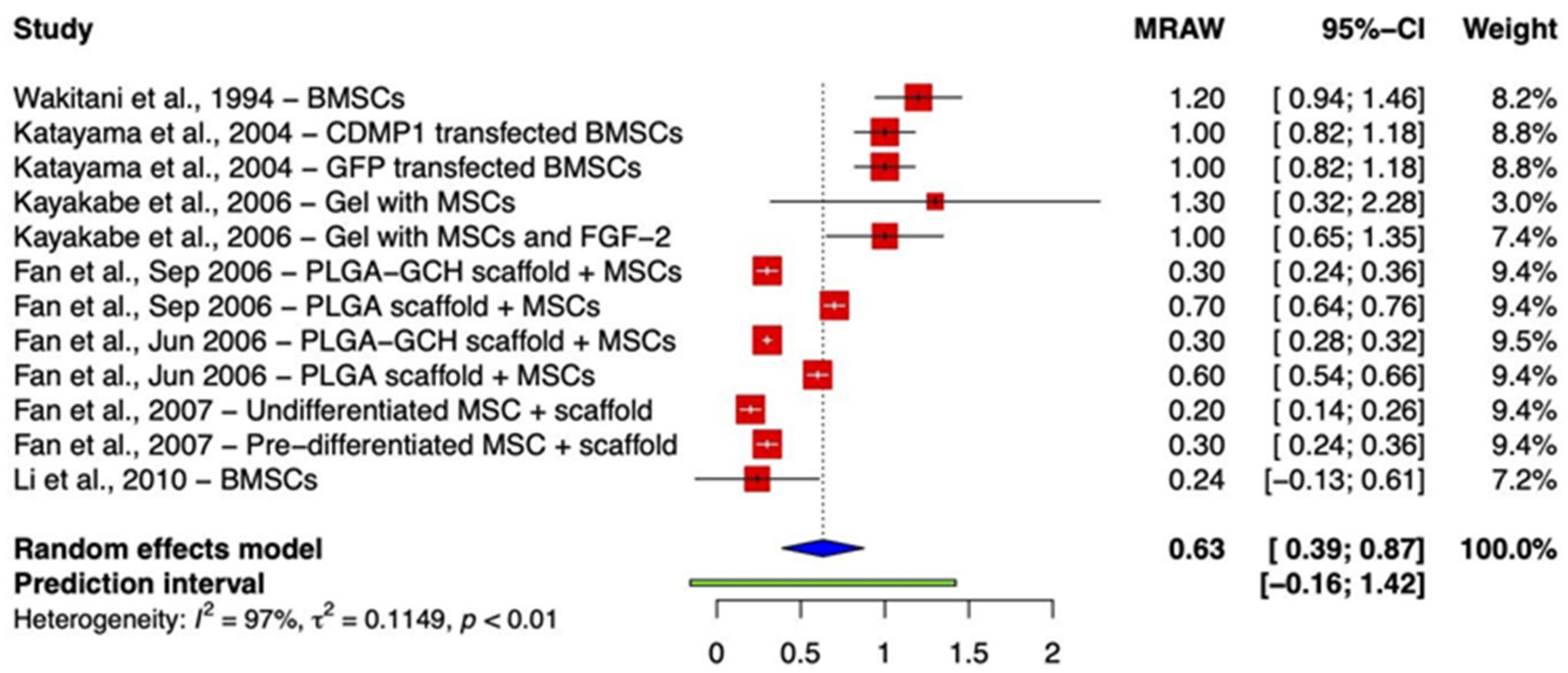
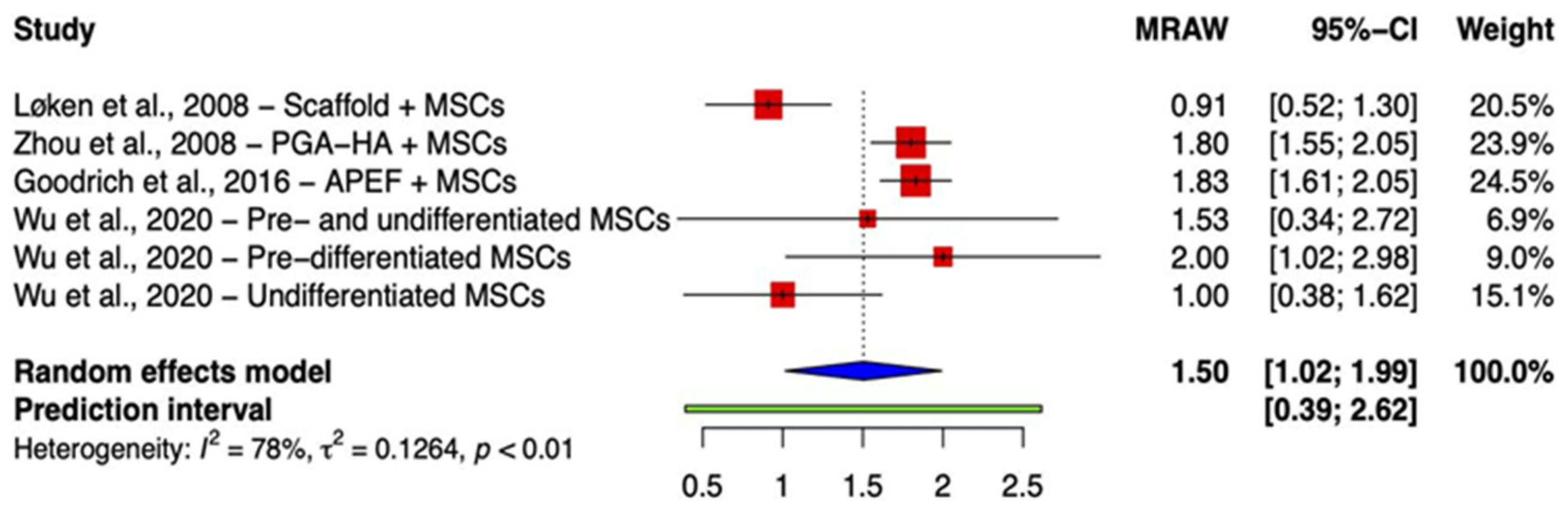
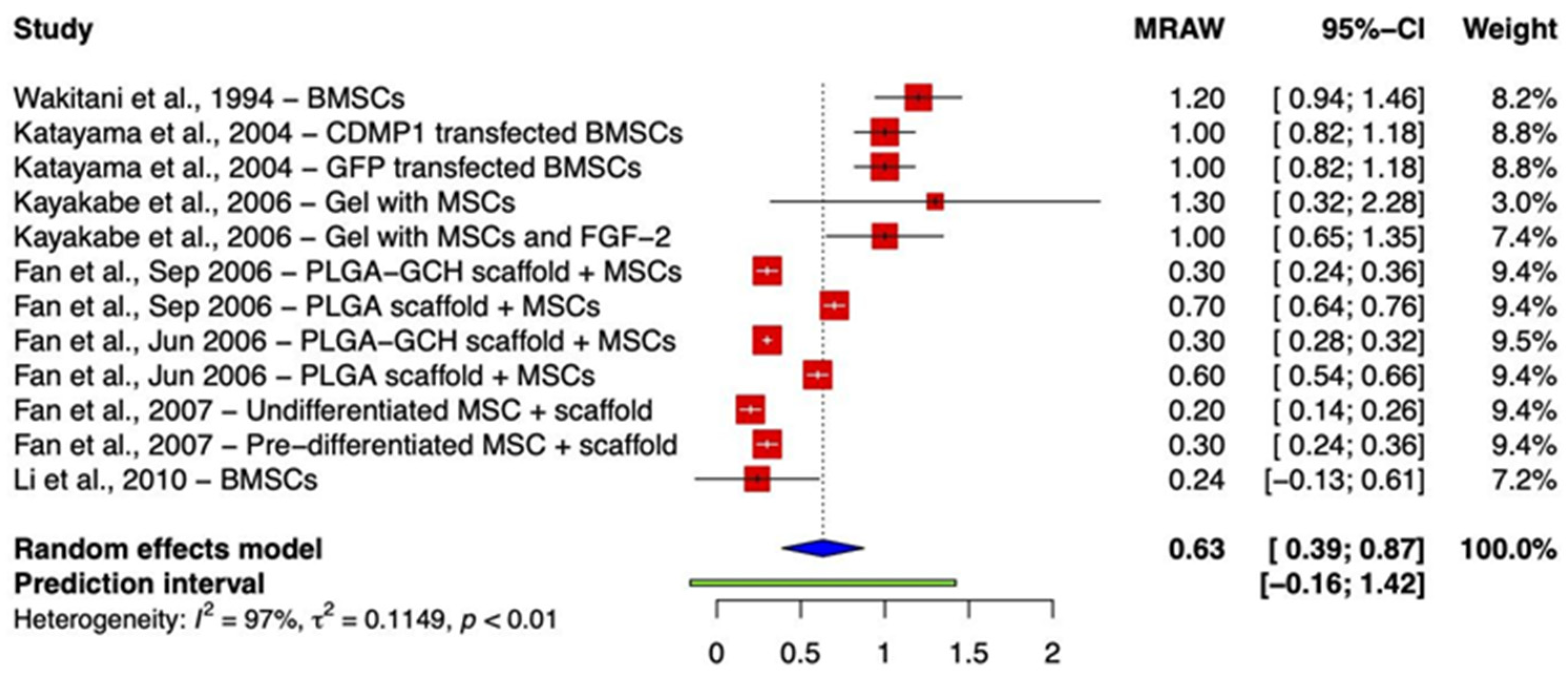
2.2.1. Integration of Repair Tissue
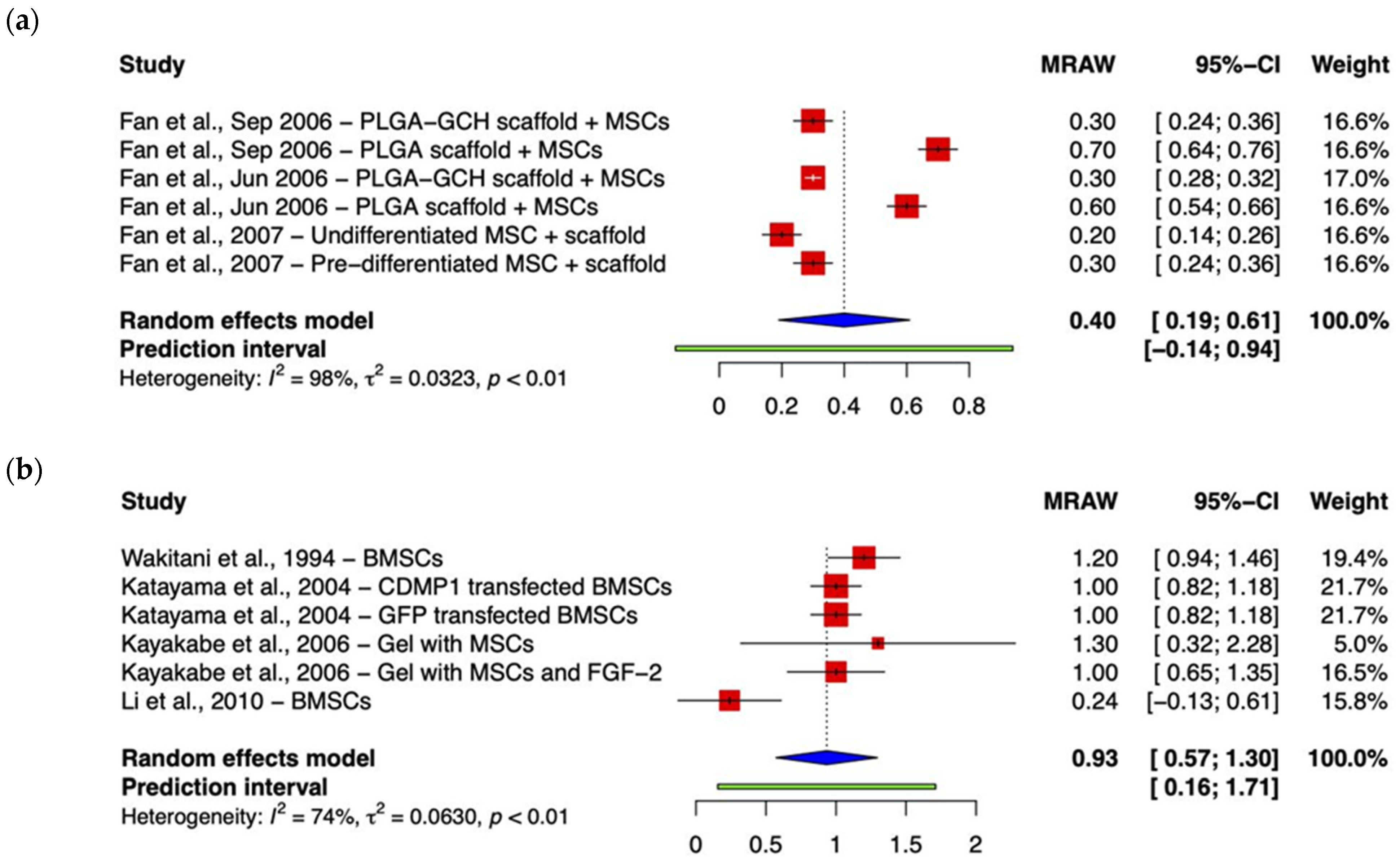
2.2.2. Other Histology Scores
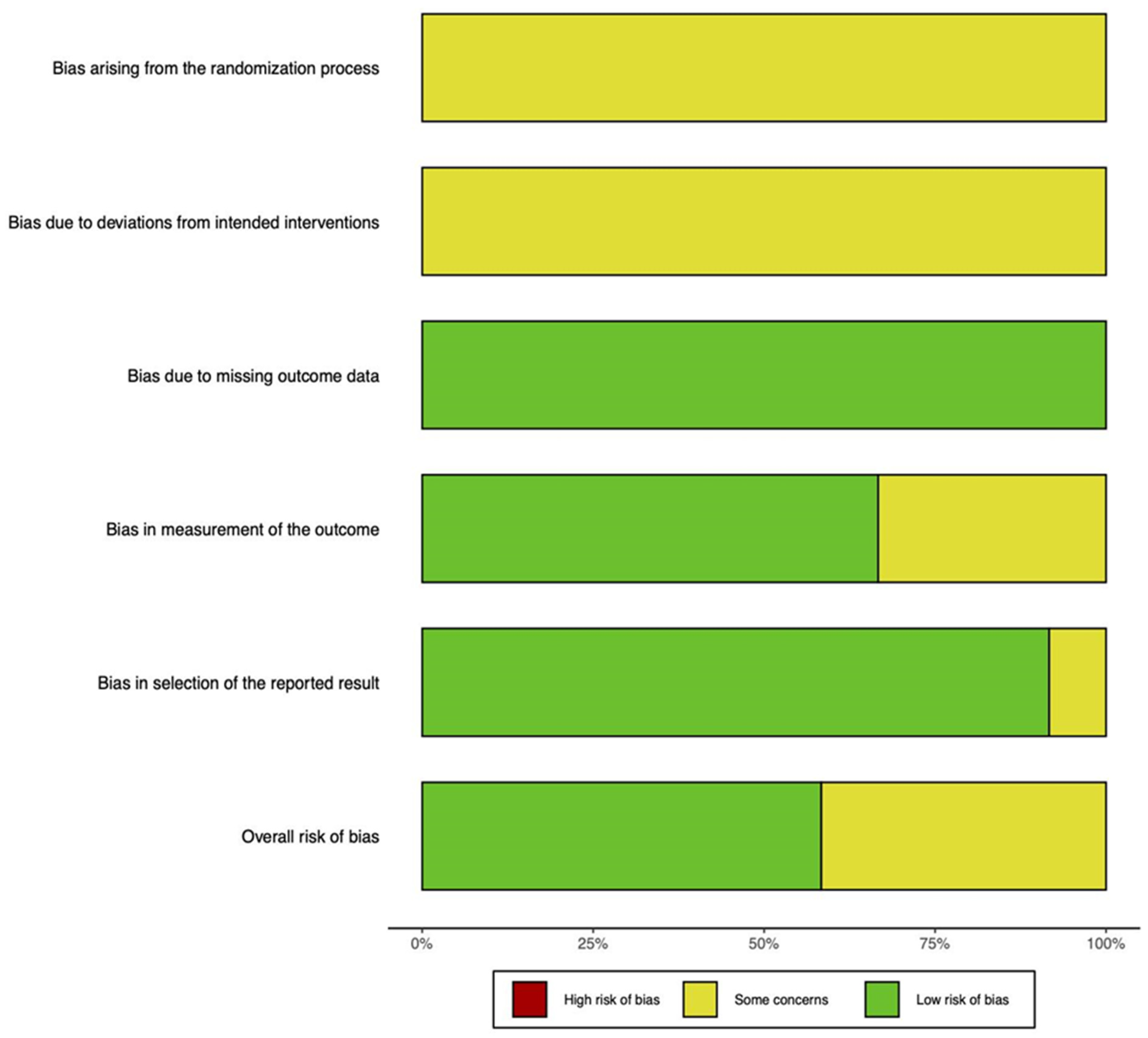
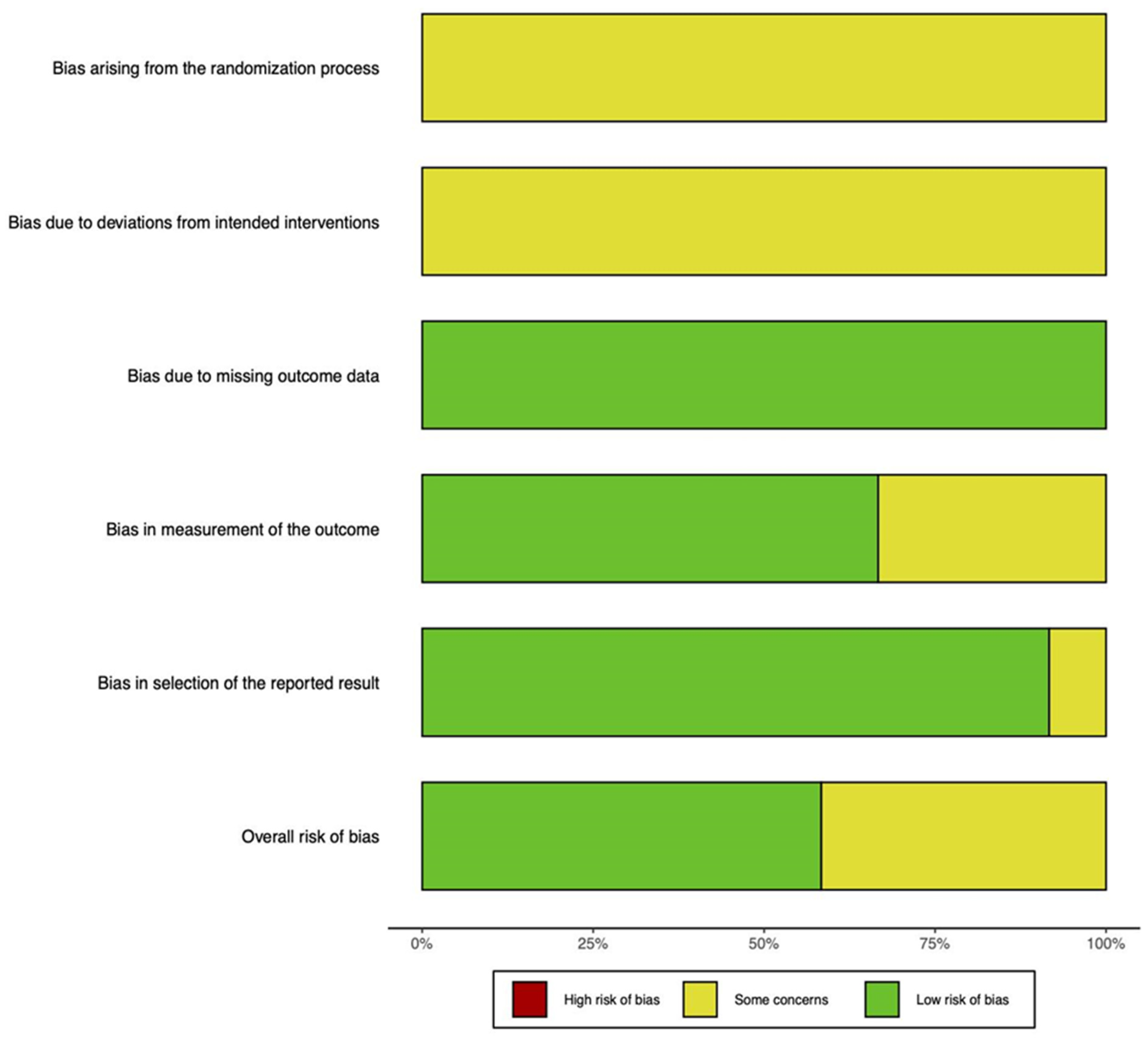
2.3. Risk of Bias Assessment
3. Discussion
3.1. Study Heterogeneity
3.1.1. MSC Source
3.1.2. Implant Composition
3.2. Translation to Clinical Practice
4. Materials and Methods
4.1. Search Algorithm
4.2. Inclusion and Exclusion Criteria
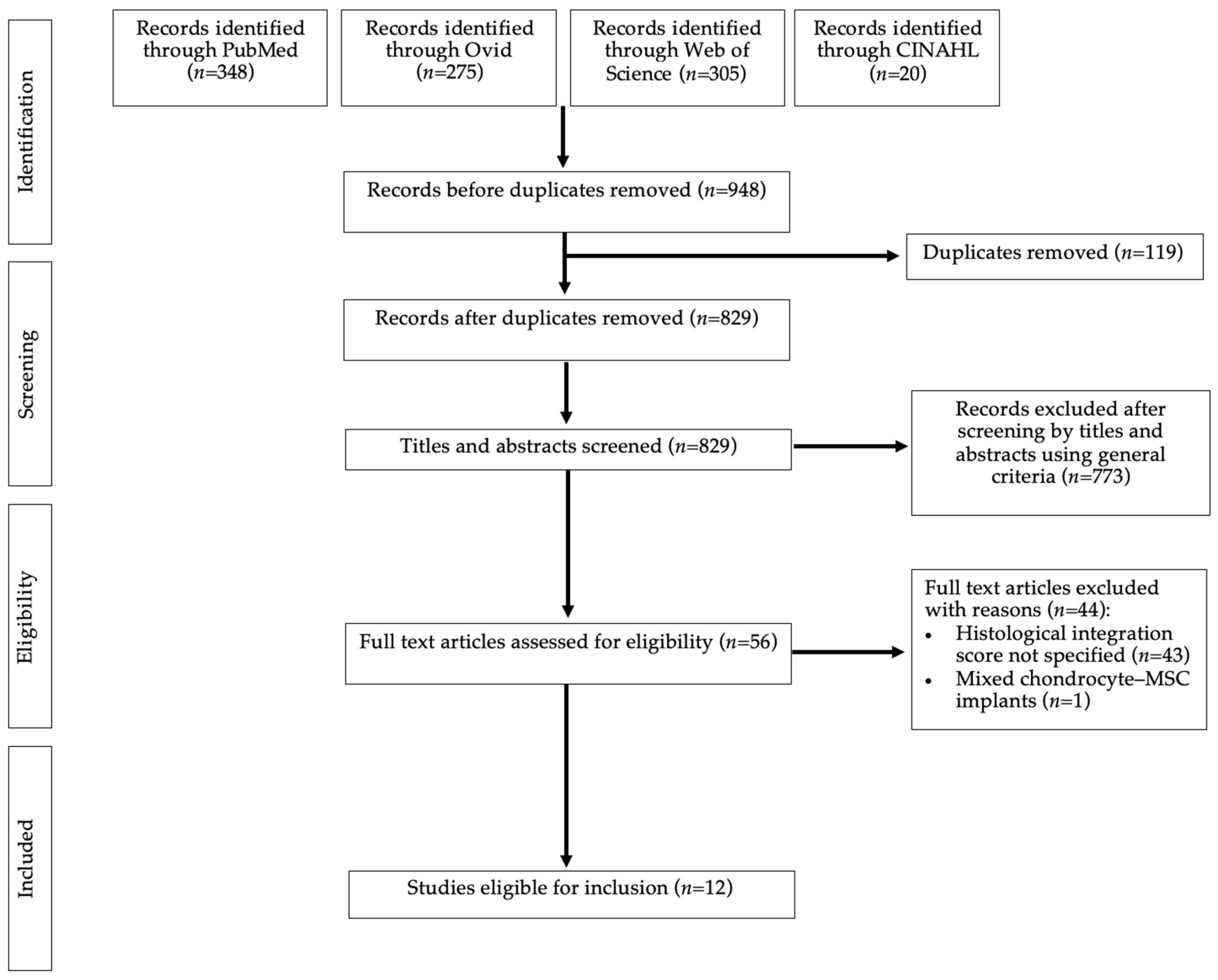
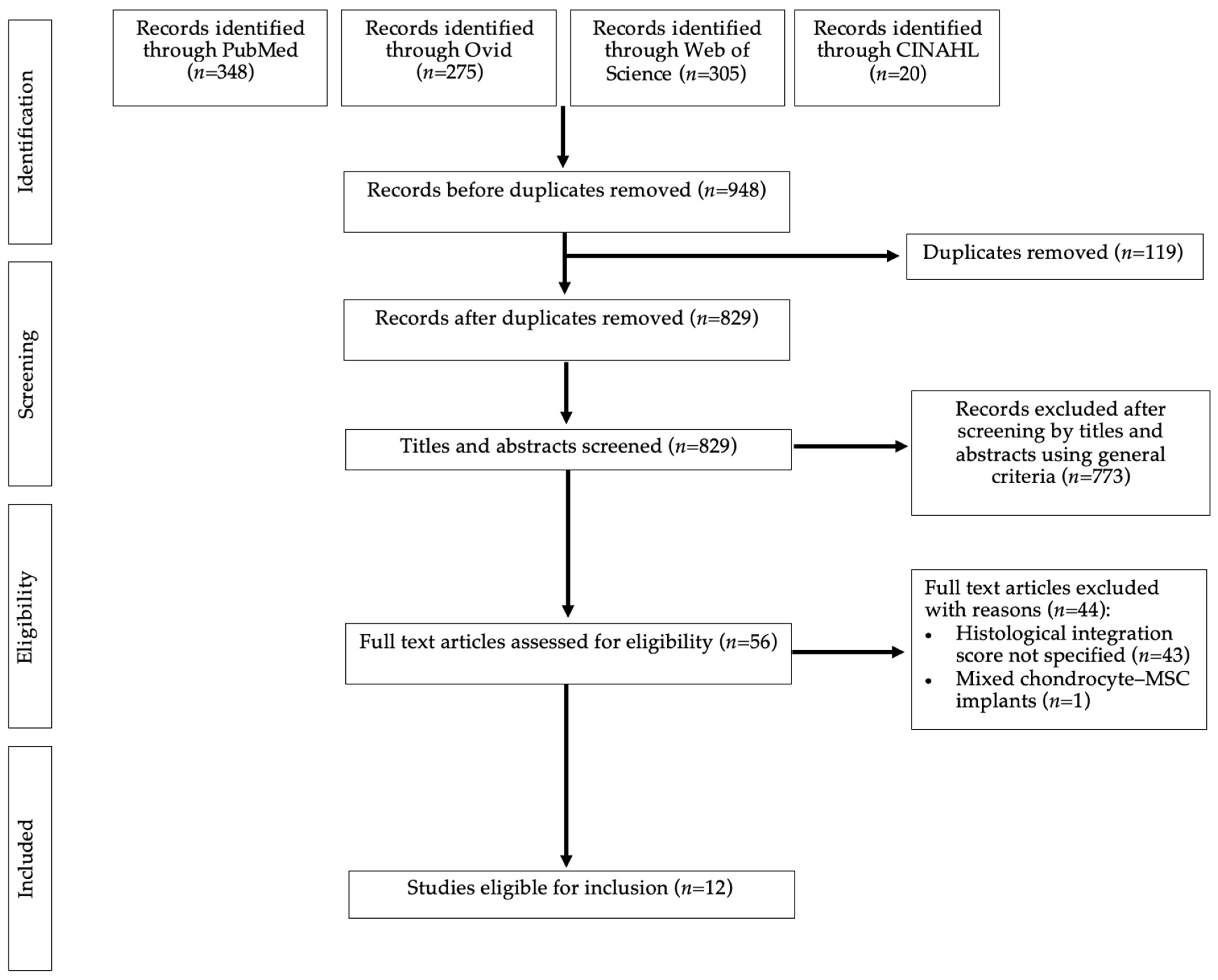
4.3. Search Results
4.4. Data Extraction
- Study characteristics and demographics including study design, animal type, cohort size, cartilage defect location, defect size, and time of sacrifice.
- Type of intervention including source of BMSC and scaffold composition.
- The cluster of differentiation (CD) molecule profile of cells.
- Primary outcome measures regarding integration of the implant and native cartilage, assessed by histological scoring systems.
- Secondary outcomes including total histological scores, data regarding the cartilage morphology, and qualitative descriptions of macro- and microscopic cartilage characteristics.
4.5. Data Analysis
4.6. Assessing Risk of Bias
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Madry, H.; Kon, E.; Condello, V.; Peretti, G.M.; Steinwachs, M.; Seil, R.; Berruto, M.; Engebretsen, L.; Filardo, G.; Angele, P. Early osteoarthritis of the knee. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ding, C.; Wluka, A.E.; Davis, S.; Ebeling, P.R.; Jones, G.; Cicuttini, F.M. Factors affecting progression of knee cartilage defects in normal subjects over 2 years. Rheumatology 2006, 45, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Epanomeritakis, I.E.; Lee, E.; Lu, V.; Khan, W. The Use of Autologous Chondrocyte and Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects in Human Knee Joints—A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 4065. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, L.E.; Culliford, D.; Monk, A.P.; Glyn-Jones, S.; Prieto-Alhambra, D.; Judge, A.; Cooper, C.; Carr, A.J.; Arden, N.K.; Beard, D.J.; et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: A population-based cohort study. Lancet 2017, 389, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Smith, J.; Miller, L.E.; Block, J.E. Clinical and economic burden of revision knee arthroplasty. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2012, 5, 89–94. [Google Scholar] [CrossRef]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L., Jr. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35 (Suppl. S6), S79–S85. [Google Scholar] [CrossRef]
- Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and tissue engineering techniques for articular cartilage. Nat. Rev. Rheumatol. 2015, 11, 21–34. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. Available online: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/maci-autologous-cultured-chondrocytes-porcine-collagen-membrane (accessed on 28 November 2022).
- National Institute for Health and Care Excellence. Available online: https://www.nice.org.uk/guidance/ta477 (accessed on 28 November 2022).
- Oldershaw, R.A. Cell sources for the regeneration of articular cartilage: The past, the horizon and the future. Int. J. Exp. Pathol. 2012, 93, 389–400. [Google Scholar] [CrossRef]
- Le, H.; Xu, W.; Zhuang, X.; Chang, F.; Wang, Y.; Ding, J. Mesenchymal stem cells for cartilage regeneration. J. Tissue Eng. 2020, 11, 2041731420943839. [Google Scholar] [CrossRef]
- De Bari, C.; Roelofs, A.J. Stem cell-based therapeutic strategies for cartilage defects and osteoarthritis. Curr. Opin. Pharmacol 2018, 40, 74–80. [Google Scholar] [CrossRef]
- Goldberg, A.; Mitchell, K.; Soans, J.; Kim, L.; Zaidi, R. The use of mesenchymal stem cells for cartilage repair and regeneration: A systematic review. J. Orthop. Surg. Res. 2017, 12, 39. [Google Scholar] [CrossRef]
- Qi, Y.; Du, Y.; Li, W.; Dai, X.; Zhao, T.; Yan, W. Cartilage repair using mesenchymal stem cell (MSC) sheet and MSCs-loaded bilayer PLGA scaffold in a rabbit model. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Fujie, H.; Nansai, R.; Ando, W.; Shimomura, K.; Moriguchi, Y.; Hart, D.A.; Nakamura, N. Zone-specific integrated cartilage repair using a scaffold-free tissue engineered construct derived from allogenic synovial mesenchymal stem cells: Biomechanical and histological assessments. J. Biomech. 2015, 48, 4101–4108. [Google Scholar] [CrossRef] [PubMed]
- Araki, S.; Imai, S.; Ishigaki, H.; Mimura, T.; Nishizawa, K.; Ueba, H.; Kumagai, K.; Kubo, M.; Mori, K.; Ogasawara, K.; et al. Improved quality of cartilage repair by bone marrow mesenchymal stem cells for treatment of an osteochondral defect in a cynomolgus macaque model. Acta Orthop. 2015, 86, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Kim, S.J.; Kim, S.A.; Ju, G.I. Past, present, and future of cartilage restoration: From localized defect to arthritis. Knee Surg. Relat. Res. 2022, 34, 1. [Google Scholar] [CrossRef]
- Freemont, A.J.; Hoyland, J. Lineage plasticity and cell biology of fibrocartilage and hyaline cartilage: Its significance in cartilage repair and replacement. Eur. J. Radiol. 2006, 57, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, N.; Laverty, S.; Kraus, V.B.; Aigner, T. Basic methods in histopathology of joint tissues. Osteoarthritis Cartilage 2010, 18 (Suppl. S3), S113–S116. [Google Scholar] [CrossRef]
- Crema, M.D.; Roemer, F.W.; Marra, M.D.; Burstein, D.; Gold, G.E.; Eckstein, F.; Baum, T.; Mosher, T.; Carrino, J.A.; Guermazi, A. Articular cartilage in the knee: Current mr imaging techniques and applications in clinical practice and research. Radiographics 2011, 31, 37–61. [Google Scholar] [CrossRef]
- Wakitani, S.; Goto, T.; Pineda, S.J.; Young, R.G.; Mansour, J.M.; Caplan, A.I.; Goldberg, V.M. Mesenchymal cell-based repair of large, full-thickness defects of articular cartilage. J. Bone Jt. Surg Am. Am. Vol. 1994, 76, 579–592. [Google Scholar] [CrossRef]
- Løken, S.; Jakobsen, R.B.; Arøen, A.; Heir, S.; Shahdadfar, A.; Brinchmann, J.E.; Engebretsen, L.; Reinholt, F.P. Bone marrow mesenchymal stem cells in a hyaluronan scaffold for treatment of an osteochondral defect in a rabbit model. Knee Surg. Sport. Traumatol. Arthrosc. 2008, 16, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Katayama, R.; Wakitani, S.; Tsumaki, N.; Morita, Y.; Matsushita, I.; Gejo, R.; Kimura, T. Repair of articular cartilage defects in rabbits using CDMP1 gene-transfected autologous mesenchymal cells derived from bone marrow. Rheumatology 2004, 43, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Kayakabe, M.; Tsutsumi, S.; Watanabe, H.; Kato, Y.; Takagishi, K. Transplantation of autologous rabbit BM-derived mesenchymal stromal cells embedded in hyaluronic acid gel sponge into osteochondral defects of the knee. Cytotherapy 2006, 8, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Hu, Y.; Zhang, C.; Li, X.; Lv, R.; Qin, L.; Zhu, R. Cartilage regeneration using mesenchymal stem cells and a PLGA-gelatin/chondroitin/hyaluronate hybrid scaffold. Biomaterials 2006, 27, 4573–4580. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Hu, Y.; Qin, L.; Li, X.; Wu, H.; Lv, R. Porous gelatin-chondroitin-hyaluronate tri-copolymer scaffold containing microspheres loaded with TGF-beta1 induces differentiation of mesenchymal stem cells in vivo for enhancing cartilage repair. J. Biomed. Mater. Res. A 2006, 77, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Liu, H.; Zhu, R.; Li, X.; Cui, Y.; Hu, Y.; Yan, Y. Comparison of chondral defects repair with in vitro and in vivo differentiated mesenchymal stem cells. Cell Transplant. 2007, 16, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.Z.; Leung, V.Y.; Dong, Q.R.; Cheung, K.M.; Chan, D.; Lu, W.W. Mesenchymal stem cell-based repair of articular cartilage with polyglycolic acid-hydroxyapatite biphasic scaffold. Int. J. Artificial. Organs 2008, 31, 480–489. [Google Scholar] [CrossRef]
- Li, Q.; Tang, J.; Wang, R.; Bei, C.; Xin, L.; Zeng, Y.; Tang, X. Comparing the chondrogenic potential in vivo of autogeneic mesenchymal stem cells derived from different tissues. Artif. Cells Blood Substit. Immob. Biotechnol. 2011, 39, 31–38. [Google Scholar] [CrossRef]
- Xie, J.; Han, Z.; Naito, M.; Maeyama, A.; Kim, S.H.; Kim, Y.H.; Matsuda, T. Articular cartilage tissue engineering based on a mechano-active scaffold made of poly(L-lactide-co-epsilon-caprolactone): In vivo performance in adult rabbits. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 94, 80–88. [Google Scholar]
- Goodrich, L.R.; Chen, A.C.; Werpy, N.M.; Williams, A.A.; Kisiday, J.D.; Su, A.W.; Cory, E.; Morley, P.S.; McIlwraith, C.W.; Sah, R.L.; et al. Addition of Mesenchymal Stem Cells to Autologous Platelet-Enhanced Fibrin Scaffolds in Chondral Defects: Does It Enhance Repair? J. Bone Jt. Surg. 2016, 98, 23–34. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, Z.; Denslin, V.; Ren, X.; Lee, C.S.; Yap, F.L.; Lee, E.H. Repair of Osteochondral Defects With Predifferentiated Mesenchymal Stem Cells of Distinct Phenotypic Character Derived From a Nanotopographic Platform. Am. J. Sport. Med. 2020, 48, 1735–1747. [Google Scholar] [CrossRef] [PubMed]
- Trengove, A.; Di Bella, C.; O’Connor, A.J. The challenge of cartilage integration: Understanding a major barrier to chondral repair. Tissue Eng. Part B Rev. 2022, 28, 114–128. [Google Scholar] [CrossRef]
- Cavinatto, L.; Hinckel, B.B.; Tomlinson, R.E.; Gupta, S.; Farr, J.; Bartolozzi, A.R. The role of bone marrow aspirate concentrate for the treatment of focal chondral lesions of the knee: A systematic review and critical analysis of animal and clinical studies. Arthroscopy 2019, 35, 1860–1877. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Berton, A.; Salvatore, G.; Candela, V.; Khan, W.; Longo, U.G.; Denaro, V. Autologous Chondrocyte Implantation and Mesenchymal Stem Cells for the Treatments of Chondral Defects of the Knee—A Systematic Review. Curr. Stem Cell Res. Ther. 2020, 15, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Akgun, I.; Unlu, M.C.; Erdal, O.A.; Ogut, T.; Erturk, M.; Ovali, E.; Kantarci, F.; Caliskan, G.; Akgun, Y. Matrix-induced autologous mesenchymal stem cell implantation versus matrix-induced autologous chondrocyte implantation in the treatment of chondral defects of the knee: A 2-year randomized study. Arch. Orthop. Trauma Surg. 2015, 135, 251–263. [Google Scholar] [CrossRef]
- Zha, K.; Li, X.; Yang, Z.; Tian, G.; Sun, Z.; Sui, X.; Dai, Y.; Liu, S.; Guo, Q. Heterogeneity of mesenchymal stem cells in cartilage regeneration: From characterization to application. NPJ Regen. Med. 2021, 6, 14. [Google Scholar] [CrossRef]
- Badiavas, A.R.; Badiavas, E.V. Potential benefits of allogeneic bone marrow mesenchymal stem cells for wound healing. Expert Opin. Biol. Ther. 2011, 11, 1447–1454. [Google Scholar] [CrossRef]
- Wakitani, S.; Okabe, T.; Horibe, S.; Mitsuoka, T.; Saito, M.; Koyama, T.; Nawata, M.; Tensho, K.; Kato, H.; Uematsu, K.; et al. Safety of autologous bone marrow-derived mesenchymal stem cell transplantation for cartilage repair in 41 patients with 45 joints followed for up to 11 years and 5 months. J. Tissue Eng. Regen. Med. 2011, 5, 146–150. [Google Scholar] [CrossRef]
- Herrmann, M.; Hildebrand, M.; Menzel, U.; Fahy, N.; Alini, M.; Lang, S.; Benneker, L.; Verrier, S.; Stoddart, M.J.; Bara, J.J. Phenotypic Characterization of Bone Marrow Mononuclear Cells and Derived Stromal Cell Populations from Human Iliac Crest, Vertebral Body and Femoral Head. Int. J. Mol. Sci. 2019, 20, 3454. [Google Scholar] [CrossRef]
- Sharifian, Z.; Hashbemibeni, B.; Pourentezari, M.; Valiani, A.; Mardani, M.; Rarani, M.Z.; Pourentezari, H. Comparison of PLGA/Fibrin and PLGA/Hyaluronic Acid Scaffolds for Chondrogenesis of Human Adipose-Derived Stem Cells. Int. J. Med. Lab. 2020, 7, 128–137. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar]
- Tang, C.; Jin, C.; Li, X.; Li, J.; Du, X.; Yan, C.; Lu, S.; Wei, B.; Xu, Y.; Wang, L. Evaluation of an Autologous Bone Mesenchymal Stem Cell-Derived Extracellular Matrix Scaffold in a Rabbit and Minipig Model of Cartilage Repair. Med. Sci. Monit. 2019, 25, 7342–7350. [Google Scholar] [CrossRef] [PubMed]
- Bornes, T.D.; Adesida, A.B.; Jomha, N.M. Mesenchymal stem cells in the treatment of traumatic articular cartilage defects: A comprehensive review. Arthritis Res. Ther. 2014, 16, 432. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.L.; Yen, C.C.; Liu, T.T.; Chang, C.H.; Shih, T.T.; Wang, J.H.; Yang, M.C.; Lin, F.H.; Liu, H.C. Safety and Efficacy of Kartigen® in Treating Cartilage Defects: A Randomized, Controlled, Phase I Trial. Polymers 2021, 13, 3029. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Chaurasia, S.; Karnatzikos, G.; Nakamura, N. Matrix-Induced Autologous Chondrocyte Implantation versus Multipotent Stem Cells for the Treatment of Large Patellofemoral Chondral Lesions: A Nonrandomized Prospective Trial. Cartilage 2015, 6, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Karnatzikos, G.; Sankineani, S.R. One-step surgery with multipotent stem cells for the treatment of large full-thickness chondral defects of the knee. Am. J. Sport. Med. 2014, 42, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Scotti, C.; Karnatzikos, G.; Mudhigere, A.; Castro, M.; Peretti, G.M. One-step surgery with multipotent stem cells and Hyaluronan-based scaffold for the treatment of full-thickness chondral defects of the knee in patients older than 45 years. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison 841 study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. Some Methods for Strengthening the Common χ 2 Tests. Biometrics 1954, 10, 417. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk- of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Animal Model | Cohort Size | Defect Location and Size | Scaffold Composition | MSC Source | Cell Density | Differentiation | Interventions | Timing of Sacrifice |
|---|---|---|---|---|---|---|---|---|---|
| Wakitani et al., 1994 [22] | Rabbits | 68 | Medial femoral condyle, 6 mm × 3 mm × 3 mm | Type I collagen gel | Tibial bone marrow or periosteum | 5 × 106 cells per mL | in vivo | Collagen gel + bone marrow-derived MSCs, collagen gel + periosteum-derived MSCs, cell-fee collagen gel, empty defect | 2, 4, 12, and 24 weeks |
| Katayama et al., 2004 [24] | Rabbits | 46 | Patellar groove, 4 mm diameter × 4 mm depth | Type I collagen gel | Tibial bone marrow | 1 × 106 cells per 200 µL of gel | in vivo | Green fluorescent protein gene-transfected bone marrow-derived mesenchymal cells, cartilage-derived morphogenetic protein 1 gene-transfected bone marrow-derived mesenchymal cells, empty control | 2, 4, and 8 weeks |
| Kayakabe et al., 2006 [25] | Rabbits | 54 | Patellar groove, 5 mm diameter × 2–3 mm depth | Hyaluronic acid gel sponge or atelocollagen gel | Ilium bone marrow | 1 × 106 cells per 100 µL of Dulbecco’s Modified Eagle Medium | in vivo | Cell-free hyaluronic gel sponge, sponge with autologous MSC grown without fibroblast growth factor-2 (FGF-2), sponge with autologous MSC grown with FGF-2, atelocollagen + MSC implant, empty control | 4 and 12 weeks |
| Fan et al., 2006 [26] | Rabbits | 45 (90 knees) | Patellar groove, 4 mm diameter, 3 mm depth | Poly-lactic-co-glycolic acid (PLGA) scaffold or hybrid PLGA-gelatin/chondroitin/hyaluronate scaffold (PLGA-GCH) | Tibial bone marrow | 1 × 1011 cells per scaffold | in vitro | PLGA scaffold + MSCs, PLGA-GCH scaffold + MSCs, empty control | 6, 12, and 24 weeks |
| Fan et al., 2006 [27] | Rabbits | 30 | Patellar groove, 4 mm diameter, 3 mm depth | Porous PLGA-GCH | Tibial bone marrow | 1 × 1011 cells per scaffold | in vitro and in vivo | Porous PLGA-GCH scaffold + undifferentiated MSCs, PLGA scaffold + pre-differentiated MSCs, empty control | 6, 12, and 24 weeks |
| Fan et al., 2007 [28] | Rabbits | 30 | Patellar groove, 4 mm diameter, 3 mm depth | PLGA scaffold with transforming growth factor-β1-impregnated microspheres (PLGA-GCH/MS-TGF) | Tibial bone marrow | 1 × 1011 cells per scaffold | in vitro and in vivo | Undifferentiated MSC + PLGA-GCH/MS-TGF scaffold, pre-differentiated MSC + PLGA-GCH/MS-TGF scaffold, empty control | 6, 12, and 24 weeks |
| Løken et al., 2008 [23] | Rabbits | 11 (22 knees) | Medial femoral condyle, 4 mm × 1.5 mm | HYAFF-11® (Fidia Advanced Biopolymers, Abano Terme, Italy) | Iliac crest bone marrow | 107 per cm2 | in vivo | Scaffold + MSC, cell-free scaffold | 24 weeks |
| Zhou et al., 2008 [29] | Rabbits | 30 | Femoral intercondylar fossa, 3.2 mm diameter × 3 mm depth | Polyglycolic-acid-hydroxyapatite (PLGA-HA) | Tibial bone marrow | 4 × 105 per scaffold | in vivo | PLGA-HA + MSCs, cell-free PLGA-HA, empty control | 16 and 32 weeks |
| Li et al., 2010 [30] | Rabbits | 54 (108 knees) | Femoral trochlear, 4 mm diameter × 3 mm depth | Demineralized bone | Femoral metaphysis, tibial periosteum, knee synovium, adipose perinephric fat, anterior tibial muscle | NA | in vivo | Bone marrow-derived MSCs, periosteum-derived MSCs, synovium-derived MSCs, adipose-derived MSCs, muscle-derived MSCs, empty control | 4, 8, and 12 weeks |
| Xie et al., 2010 [31] | Rabbits | 18 (36 knees) | Medial femoral condyle, 4.5 mm diameter × 5 mm depth | poly(L-lactide-co-ε-caprolactone) (PLCL) | Tibial bone marrow | NA | in vivo | PLCL + MSCs, cell-free PLCL, empty control | 3 and 6 months |
| Goodrich et al., 2016 [32] | Horses | 12 (24 joints) | Stifle Joint, 15 mm diameter, full thickness | Autologous platelet-enhanced fibrin (AFEP) | Ilium bone marrow | 106 per mL | in vivo | APEP + MSCs, cell-free APEP | 3 and 12 months |
| Wu et al., 2020 [33] | Rabbits | 24 | Trochlear groove, 4.5 mm diameter × 2 mm depth | Nanoimprinted polymeric films with polycaprolactone | Iliac crest | NA | in vitro and in vivo | Mixed pre- and undifferentiated MSCs, bilayered pre-differentiated MSCs, undifferentiated MSCs, empty control | 7 months |
| Author | Scoring | Intervention | Number of Subjects | Total Score | Integration | Cell Morphology | Matrix Staining | p |
|---|---|---|---|---|---|---|---|---|
| Wakitani et al., 1994 [22] | Wakitani scale (lower is better): 0 = both edges integrated, 1 = one edge integrated, 2 = neither edge integrated | Collagen gel + bone marrow derived-MSCs | 7 (2 weeks); 8 (4 weeks); 9 (12 weeks); 7 (24 weeks) | 9.8 (2 weeks); 5.6 (4 weeks); 7.9 (12); 8.4 (24 weeks) | 1.6 (2 weeks); 1.1 (4 weeks); 1.2 (24 weeks) | 2.6 (2 weeks); 1.3 (4 weeks); 1.9 (12 weeks); 1.9 (24 weeks) | 2.2 (2 weeks); 1.3 (4 weeks); 1.7 (12 weeks); 1.7 (24 weeks) | Not assessed |
| Collagen gel + periosteum-derived MSCs | 6 (2 weeks); 17 (4 weeks); 8 (12 weeks); 6 (24 weeks) | 9.3 (2 weeks); 6.0 (4 weeks); 8.1 (12 weeks); 8.4 (24 weeks) | 1.5 (2 weeks); 1.2 (4 weeks); 1.5 (12 weeks); 1.2 (24 weeks) | 2.5 (2 weeks); 1.4 (4 weeks); 1.7 (12 weeks); 2.0 (24 weeks) | 2.0 (2 weeks); 1.3 (4 weeks); 1.6 (12 weeks); 1.6 (24 weeks) | |||
| Cell-free collagen gel | 11 (2 weeks); 19 (4 weeks); 12 (12 weeks); 7 (24 weeks) | 11.6 (2 weeks); 6.9 (4 weeks); 8.7 (12 weeks); 8.9 (24 weeks) | 1.9 (2 weeks); 0.9 (4 weeks); 1.6 (12 weeks); 1.2 (24 weeks) | 2.9 (2 weeks); 1.7 (4 weeks); 1.8 (12 weeks); 2.2 (24 weeks) | 2.2 (2 weeks); 1.6 (4 weeks); 1.7 (12 weeks); 2.0 (24 weeks) | |||
| Empty control | 5 (2 weeks); 7 (4 weeks); 4 (12 weeks); 3 (24 weeks) | 11.8 (2 weeks); 9.0 (4 weeks); 9.2 (12 weeks); 9.5 (24 weeks) | 1.9 (2 weeks); 1.8 (4 weeks); 1.3 (12 weeks); 1.4 (24 weeks) | 3.2 (2 weeks); 1.9 (4 weeks); 2.2 (12 weeks); 2.4 (24 weeks) | 2.2 (2 weeks); 1.8 (4 weeks); 1.8 (12 weeks); 1.9 (24 weeks) | |||
| Katayama et al., 2004 [24] | Modified Wakitani scale (lower is better): 0 = both edges integrated, 1 = integrated at one edge, 2 = no integration | Cartilage-derived morphogenetic protein 1 gene-transfected bone marrow-derived mesenchymal cells | 10 (2 weeks); 10 (4 weeks); 10 (8 weeks) | 11.5 (2 weeks); 7.4 (4 weeks); 7.8 (8 weeks) | 1.2 (2 weeks); 0.7 (4 weeks); 1.0 (8 weeks) | Cell morphology and staining composite score: 6.2 (2 weeks); 4.4 (4 weeks); 4.6 (8 weeks) | Total: p < 0.05 between CDMP group and empty control at 2 weeks; p < 0.05 between CDMP group and the other groups at 8 weeks | |
| Green fluorescent protein gene-transfected bone marrow-derived mesenchymal cells | 10 (2 weeks); 10 (4 weeks); 10 (8 weeks) | 13.4 (2 weeks); 10.7 (4 weeks); 12.7 (8 weeks) | 1.4 (2 weeks); 0.9 (4 weeks); 1.0 (8 weeks) | 7.0 (2 weeks); 6.2 (4 weeks); 6.8 (8 weeks) | ||||
| Empty control | 2 (2 weeks); 7 (4 weeks); 7 (8 weeks) | 18.5 (2 weeks); 12.7 (4 weeks); 13.6 (8 weeks) | 2.0 (2 weeks); 1.6 (4 weeks); 1.0 (8 weeks) | 8.0 (2 weeks); 6.6 (4 weeks); 7.4 (8 weeks) | ||||
| Kayakabe et al., 2006 [25] | Modified Wakitani scale (lower is better): 0 = both edges integrated, 1 = integrated at one edge, 2 = no integration | Cell-free hyaluronic gel sponge alone | 6 (4 weeks); 3 (12 weeks) | 9.2 ± 2.5 (4 weeks); 6.3 ± 1.2 (12 weeks) | 1.3 ± 0.5 (4 weeks); 1.7 ± 0.6 (12 weeks) | 2.0 ± 0.0 (4 weeks); 1.3 ± 0.6 (12 weeks) | 1.3 ± 0.6 (4 weeks); 1.0 ± 0.0 (12 weeks) | Total: p < 0.05 between HS/MSC/ FGF and empty control at 12 weeks |
| Hyaluronic acid gel sponge loaded with autologous MSC grown without FGF-2 | 3 (4 weeks); 4 (12 weeks) | 7.7 ± 0.6 (4 weeks); 5.8 ± 1.5 (12 weeks) | 2.0 ± 0.0 (4 weeks); 1.3 ± 1.0 (12 weeks) | 2.3 ± 0.8 (4 weeks); 1.5 ± 0.6 (12 weeks) | 2.0 ± 0.6 (4 weeks); 1.3 ± 0.5 (12 weeks) | |||
| Hyaluronic gel sponge loaded with autologous MSC grown with FGF-2 | 9 (4 weeks); 8 (12 weeks) | 8.7 ± 3.1 (4 weeks); 4.0 ± 1.4 (12 weeks) | 1.0 ± 1.0 (4 weeks); 1.0 ± 0.5 (12 weeks) | 2.7 ± 0.6 (4 weeks); 2.8 ± 0.5 (12 weeks) | 2.7 ± 0.6 (4 weeks); 0.5 ± 0.8 (12 weeks) | |||
| Atelocollagen loaded with autologous MSC grown with FGF-2 | NA | 7.8 ± 3.0 (4 weeks); 5.0 ± 2.0 (12 weeks) | NA | NA | NA | |||
| Empty control | 3 (4 weeks); 4 (12 weeks) | 9.7 ± 2.5 (4 weeks); 8.5 ± 1.3 (12 weeks) | 1.3 ± 0.6 (4 weeks); 1.0 ± 0.0 (12 weeks) | 2.4 ± 1.3 (4 weeks); 2.8 ± 0.5 (12 weeks) | 2.2 ± 1.0 (4 weeks); 2.0 ± 0.0 (12 weeks) | |||
| Fan et al., 2006 [26] | Modified Wakitani scale (lower is better): 0 = both edges integrated, 1 = integrated at one edge, 2 = no integration | PLGA-GCH scaffold + MSCs | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 7.7 ± 0.2 (6 weeks); 4.7 ± 0.2 (12 weeks); 3.7 ± 0.1 (24 weeks) | 1.0 ± 0.2 (6 weeks); 0.4 ± 0.1 (12 weeks); 0.3 ± 0.1 (24 weeks) | 4.5 ± 0.4 (6 weeks); 2.9 ± 0.3 (12 weeks); 2.2 ± 0.1 (24 weeks) | Integration: p < 0.05 for PLGA-GCH/MSC group compared with control at 12 and 24 weeks Total: p < 0.05 for PLGA-GCH/MSC group compared with control at 6, 12 and 24 weeks; p < 0.05 for PLGA-GCH/MSC group compared with PLGA/ MSC group at 12 and 24 weeks Cell morphology and matrix staining: p < 0.05 for PLGA-GCH/MSC group compared with control at 12 and 24 weeks; p < 0.05 for PLGA-GCH/MSC group compared with PLGA/ MSC group at 24 weeks | |
| PLGA scaffold + MSCs | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 8.3 ± 0.4 (6 weeks); 7.5 ± 0.3 (12 weeks); 8.2 ± 0.3 (24 weeks) | 1.0 ± 0.2 (6 weeks); 0.8 ± 0.1 (12 weeks); 0.7 ± 0.1 (24 weeks) | 4.9 ± 0.6 (6 weeks); 4.2 ± 0.3 (12 weeks); 4.7 ± 0.3 (24 weeks) | ||||
| Empty control | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 17.3 ± 0.4 (6 weeks); 17.5 ± 0.3(12 weeks); 17.1 ± 0.5 (24 weeks) | 2.2 ± 0.3 (6 weeks); 1.9 ± 0.1 (12 weeks); 1.6 ± 0.1 (24 weeks) | 6.3 ± 0.8 (6 weeks); 7.5 ± 0.3(12 weeks); 7.6 ± 0.6 (24 weeks) | ||||
| Fan et al., 2006 [27] | Modified Wakitani scale (lower is better): 0 = both edges integrated, 1 = integrated at one edge, 2 = no integration | Porous PLGA-GCH scaffold + undifferentiated MSCs | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 7.9 ± 0.4 (6 weeks); 4.7 (12 weeks); 3.7 ± 0.2 (24 weeks) | 1.0 ± 0.2 (6 weeks); 0.5 ± 0.1 (12 weeks); 0.3 ± 0.04 (24 weeks) | 4.7 ± 0.5 (6 weeks); 3.0 ± 0.4 (12 weeks); 2.2 ± 0.1 (24 weeks) | Integration: p < 0.05 for in vivo repair group compared with control at 24 weeks Total: p < 0.05 compared with control at 6, 12 and 24 weeks and with the in vitro differentiated MSCs repair group at 12 and 24 weeks. | |
| PLGA scaffold + pre- differentiated MSCs | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 8.4 ± 0.4 (6 weeks); 7.4 ± 0.3 (12 weeks); 8.1 + 0.3 (24 weeks) | 1.0 ± 0.3 (6 week); 0.8 ± 0.1 (12 weeks); 0.6 ± 0.1 (24 weeks) | 5.0 ± 0.6 (6 weeks); 4.0 ± 0.7 (12 weeks); 4.7 ± 0.3 (24 weeks) | ||||
| Empty control | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 17.2 ± 0.7 (6 weeks); 17.5 ± 0.4 (12 weeks); 16.9 ± 0.5 (24 weeks) | 2.0 ± 0.3 (6 weeks); 1.8 ± 0.1 (12 weeks); 1.5 ± 0.1 (24 weeks) | 6.5 ± 0.8 (6 weeks); 7.4 ± 0.3 (12 weeks); 7.6 ± 0.5 (24 weeks) | ||||
| Fan et al., 2007 [28] | Modified Wakitani scale (lower is better): 0 = both edges integrated, 1 = integrated at one edge, 2 = no integration | Undifferentiated MSC + PLGA-GCH/MS-TGF scaffold | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 7.2 + 0.2 (6 weeks); 4.2 ± 0.2 (12 weeks); 2.8 ± 0.1 (24 weeks) | 0.9 ± 0.2 (6 weeks); 0.3 ± 0.1 (12 weeks); 0.2 ± 0.1 (24 weeks) | 0.9 ± 0.2 (6 weeks); 0.3 ± 0.1 (12 weeks); 0.2 ± 0.1 (24 weeks) | Integration: p < 0.05 for in vivo differentiated group compared to control at 12 and 24 weeks. Morphology and Matrix Staining: p < 0.05 compared to control at 12 and 24 weeks, and compared to in vitro group at 24 weeks. Total: p < 0.05 compared to control at 6, 12, and 24 weeks, and compared to in vitro group at 12 and 24 weeks. | |
| Pre-differentiated MSC + PLGA-GCH/MS-TGF scaffold | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 8.0 ± 0.2 (6 weeks); 4.8 ± 0.2 (12 weeks); 4.0 ± 0.1 (24 weeks) | 1.0 ± 0.2 (6 weeks); 0.5 ± 0.1 (12 weeks); 0.3 ± 0.1 (24 weeks) | 1.0 ± 0.2 (6 weeks); 0.5 ± 0.1 (12 weeks); 0.3 ± 0.1(24 weeks) | ||||
| Empty control | 10 (6 weeks); 10 (12 weeks); 10 (24 weeks) | 17.9 ± 0.4 (6 weeks); 17.7 ± 0.3 (12 weeks); 17.4 ± 0.3 (24 weeks) | 2.3 ± 0.3 (6 weeks); 2.0 ± 0.1 (12 weeks); 1.7 ± 0.1 (24 weeks) | 2.3 ± 0.3 (6 weeks); 2.0 ± 0.1 (12 weeks); 1.7 ± 0.1 (24 weeks) | ||||
| Løken et al., 2008 [23] | Modified O’Driscoll score (higher is better): 0 = not bonded, 1 = bonded at one end, 2 = bonded at both ends | Scaffold + MSCs | 11 | NA | 0.91 (SD = 0.66) | Hyaline cartilage score: 1.45 (SD = 0.47); Necrosis: 1.45 (SD = 0.56); Chondrocyte clustering: 0.86 (SD = 0.51) | NA | Hyaline cartilage: p = 0.06 Necrosis: p = 0.09 Chondrocyte clustering: p = 0.03 for scaffold + MSC vs empty scaffold |
| Empty Scaffold | 11 | NA | 0.50 (SD = 0.63) | Hyaline Cartilage score: 1.05 (SD = 0.47); Necrosis: 1.05 (SD = 0.52); Chondrocyte clustering: 0.36 (SD = 0.39) | NA | |||
| Zhou et al., 2008 [29] | Integration with adjacent cartilage, higher score means better outcome (Both edges integrated = 2; One edge integrated = 1; Neither edge integrated = 0) | PGA-HA + MSCs | 10 (16 weeks); 10 (32 weeks) | 14.2 ± 1.4 (16 weeks); 15.1 ± 1.4 (32 weeks) | 1.7 ± 0.5 (16 weeks); 1.8 ± 0.4 (32 weeks) | 3.5 ± 0.7 (16 weeks); 3.7 ± 0.5 (32 weeks) | 2.3 ± 0.5 (16 weeks); 2.5 ± 0.5 (32 weeks) | Total: p < 0.05 between the MSCs-PGA-HA group and the two control groups |
| Cell-free PGA-HA | 6.8 ± 1.1 (16 weeks); 8.4 ± 1.7 (32 weeks) | 0.9 ± 0.7 (16 weeks); 1.2 ± 0.8 (32 weeks) | 2.1 ± 0.7 (16 weeks); 2.2 ± 0.6 (32 weeks) | 1.4 ± 0.8 (16 weeks); 1.3 ± 0.9 (32 weeks) | ||||
| Empty control | 11 | 6.6 ± 2.5 (16 weeks); 7.4 ± 2.0 (32 weeks) | 0.7 ± 0.8 (16 weeks); 1.0 ± 0.8 (32 weeks) | 1.9 ± 0.7 (16 weeks); 2.0 ± 0.7 (32 weeks) | 1.2 ± 0.6 (16 weeks); 1.0 ± 0.7 (32 weeks) | |||
| Li et al., 2010 [30] | O’Driscoll score (lower is better): 0 = both edges integrated; 1 = one edge integrated; 2 = neither edge integrated | Bone-marrow derived MSCs | 6 (12 weeks) | 4.13 ± 0.83 | 0.25 ± 0.46 | 1.25 ± 0.46 | 0.38 ± 0.52 | Total: p < 0.05 between BMSC group and all others. p < 0.05 between periosteum-, synovium-, adipose- and muscle-derived MSCs to control Integration: p < 0.05 between BMSC group and all others p < 0.05 between periosteum-, synovium- and adipose-derived MSCs and control Cell Morphology and Organization: p < 0.05 between BMSC group and all others p < 0.05 between synovium- and adipose-derived MSCs and control |
| Periosteum-derived MSCs | 6 (12 weeks) | 12.0 ± 1.60 | 1.25 ± 0.46 | 2.50 ± 0.53 | 1.26 ± 0.71 | |||
| Synovium-derived MSCs | 6 (12 weeks) | 11.4 ± 3.08 | 1.20 ± 0.72 | 2.67 ± 0.56 | 1.34 ± 0.42 | |||
| Adipose-derived MSCs | 6 (12 weeks) | 10.98 ± 2.14 | 1.57 ± 0.42 | 2.05 ± 1.45 | 1.56 ± 0.58 | |||
| Muscle-derived MSCs | 6 (12 weeks) | 12.23 ± 4.65 | 1.78 ± 0.80 | 1.98 ± 0.76 | 1.12 ± 0.34 | |||
| Empty control | 6 (12 weeks) | 15.87 ± 0.64 | 2.00 ± 0.00 | 2.75 ± 0.46 | 1.87 ± 0.35 | |||
| Xie et al., 2010 [31] | Two integration scores for lateral and medial integration to adjacent cartilage (Bonded = 2, Partially bonded = 1, Not bonded = 0) | PLCL + MSCs | 4 (3 months); 4 (6 months) | 13.5 ± 2.1 (3 months); 21.7 ± 6 4.5 (6 months) | Medially: 0.4 ± 0.3 (3 months); 1.3 ± 0.3 (6 months); Laterally: 0.5 ± 0.4 (3 months); (6 months) 1.4 ± 0.5 | 4.1 ± 1.4 (3 months); 6.9 ± 2.5 (6 months) | NA | Total: p < 0.05 for PLCL + MSC vs cell-free PLCL and empty control at 3 months; p < 0.05 for MSC group at 6 months vs MSC group at 3 months. Empty control group was significantly worse at 6 months vs 3 months Hyaline cartilage: p < 0.05 for MSC group relative to other two groups at 3 and 6 months |
| Cell-free PLCL | 4 (3 months); 4 (6 months) | 9.2 ± 2.6 (3 months); 12.3 ± 2.4 (6 months) | Medially: 0.3 ± 0.1 (3 months); 1.1 ± 0.2 (6 months); Laterally: 0.2 ± 0.2 (3 months); (6 months) 1.3 ± 0.6 | 1.0 ± 0.8 (3 months); 1.2 ± 0.4 (6 months) | NA | |||
| Empty control | 4 (3 months); 4 (6 months) | 11.6 ± 3.1 (3 months); 5.9 ± 3.2 (6 months) | Medially: 0.8 ± 0.3 (3 months); 0.6 ± 0.5 (6 months); Laterally: 0.7 ± 0.1 (3 months); 0.2 ± 0.2 (6 months) | 2.1 ± 1.1 (3 months); 0.9 ± 0.2 (6 months) | NA | |||
| Goodrich et al., 2016 [32] | Bonding to adjacent cartilage, (higher is better): Bonded at both ends of the graft = 2, Bonded at 1 end or partially at both ends = 1, Not bonded = 0 | APEF + MSCs | 12 (12 months) | NA | 1.83 ± 0.39 | Cellular morphology = 1.42 ± 0.79; Chondrocyte Clustering = 1.25 ± 0.62 | Safranin-O staining = 1.33 ± 0.49 | None significant |
| Cell-free APEF | 12 (12 months) | NA | 2.0 ± 0.0 | Cellular morphology = 1.25 ± 0.75; Chondrocyte Clustering = 1.25 ± 0.75 | Safranin-O staining = 0.83 ± 0.71 | |||
| Wu et al., 2020 [33] | Modified O’Driscoll score, higher score means better outcome (Bonded at both ends of graft = 2, Bonded at one end = 1, Not bonded = 0) | Mixed pre- and undifferentiated MSCs | 4 (7 months) | NA | 1.53 ± 1.21 | NA | NA | Integration: bilayered differentiated and mixed-phenotype groups significantly better compared to control (p < 0.05); bilayered differentiated group showed significant increase vs undifferentiated group |
| Bilayered pre-differentiated MSCs | 4 (7 months) | NA | 2.0 ± 1.0 | NA | NA | |||
| Undifferentiated MSCs | 4 (7 months) | NA | 1.0 ± 0.63 | NA | NA | |||
| Empty control | 4 (7 months) | NA | 0.5 ± 0.63 | NA | NA | |||
| Domain | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Animal subjects with surgically-created focal chondral defects of the knee joint. | Studies involving human or cadaveric subjects. Studies involving animals with diffuse osteoarthritis models. Ex vivo, in vitro, or in silico studies. |
| Intervention | Studies using implants consisting of autologous or allogeneic mesenchymal stem cells seeded into an organic scaffold or gel which were surgically introduced into a focal chondral defect. | Studies involving cell-free therapy, cell therapy without open surgical implantation, cells which are not bone marrow-derived, or other cell types such as chondrocytes, except as comparators. Studies using xenogeneic stem cells. |
| Comparison | Studies comparing the use of scaffolds/gel implants to cell-free scaffolds/gels, cell therapy without implantation, or empty controls. | None. |
| Outcome | Studies which quantitatively report the quality of integration of the regenerated and native cartilage, assessed histologically. | Studies reporting outcomes of joints other than the knee. Studies without a quantitative scoring system. Studies not involving a histological assessment. Studies which do not specify integration scores. |
| Study Type | English articles with full text available. Sample size greater than 10 animals. | Case reports, case series with fewer than 10 subjects, review articles. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Epanomeritakis, I.E.; Lu, V.; Khan, W. Bone Marrow-Derived Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects of the Knee in Animal Models: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 3227. https://doi.org/10.3390/ijms24043227
Lee E, Epanomeritakis IE, Lu V, Khan W. Bone Marrow-Derived Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects of the Knee in Animal Models: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(4):3227. https://doi.org/10.3390/ijms24043227
Chicago/Turabian StyleLee, Ernest, Ilias Ektor Epanomeritakis, Victor Lu, and Wasim Khan. 2023. "Bone Marrow-Derived Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects of the Knee in Animal Models: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 4: 3227. https://doi.org/10.3390/ijms24043227
APA StyleLee, E., Epanomeritakis, I. E., Lu, V., & Khan, W. (2023). Bone Marrow-Derived Mesenchymal Stem Cell Implants for the Treatment of Focal Chondral Defects of the Knee in Animal Models: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 24(4), 3227. https://doi.org/10.3390/ijms24043227