
Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery

 , ,
, ,  , and
, and
Abstract
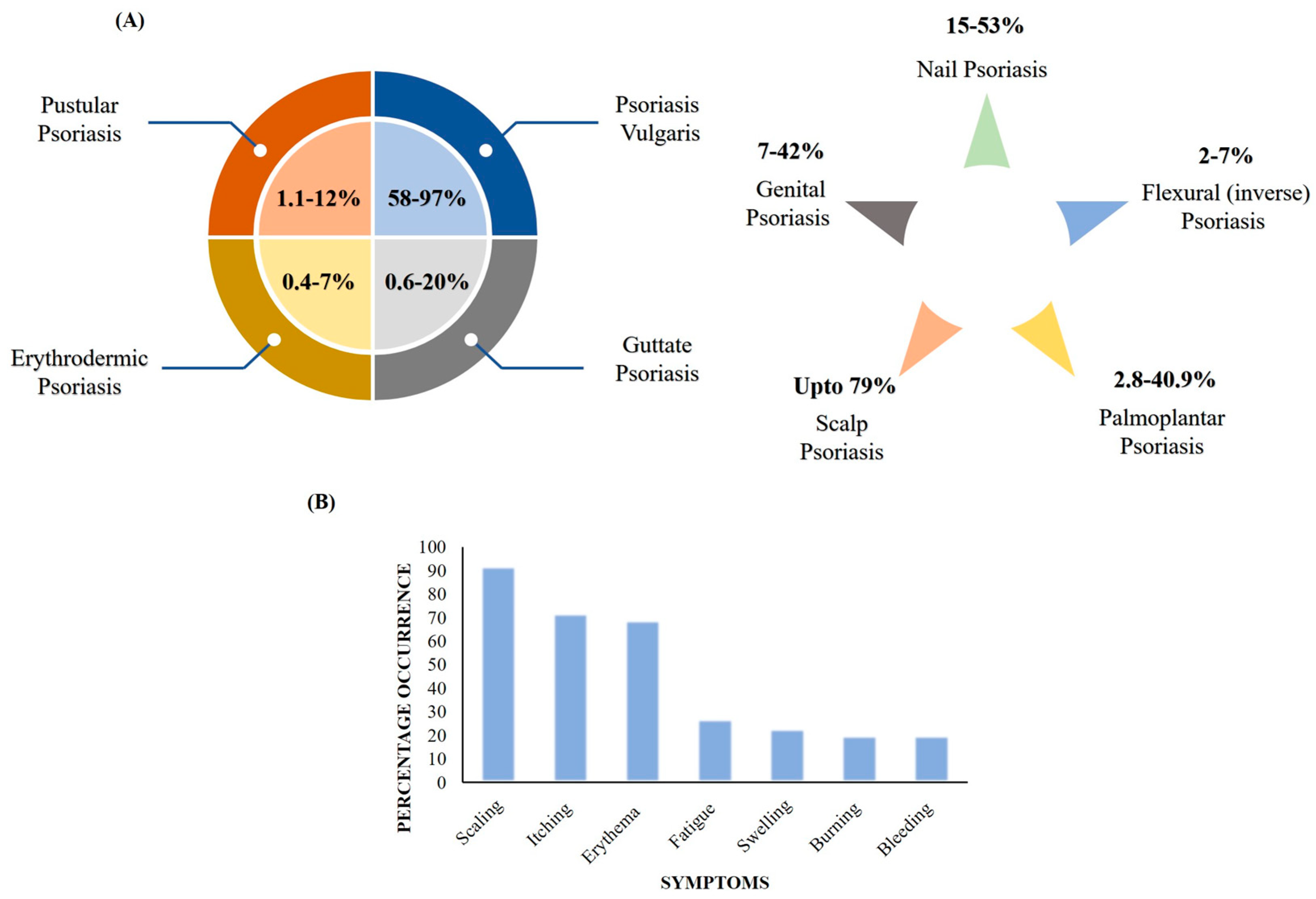
:1. Introduction
- Keratinocyte hyperproliferation leads to an enhanced buildup of keratin as a thick coat (scaly plaques) in the stratum corneum (SC);
- Dilation and proliferation of dermal blood vessels;
2. Present Treatment Options and Limitations
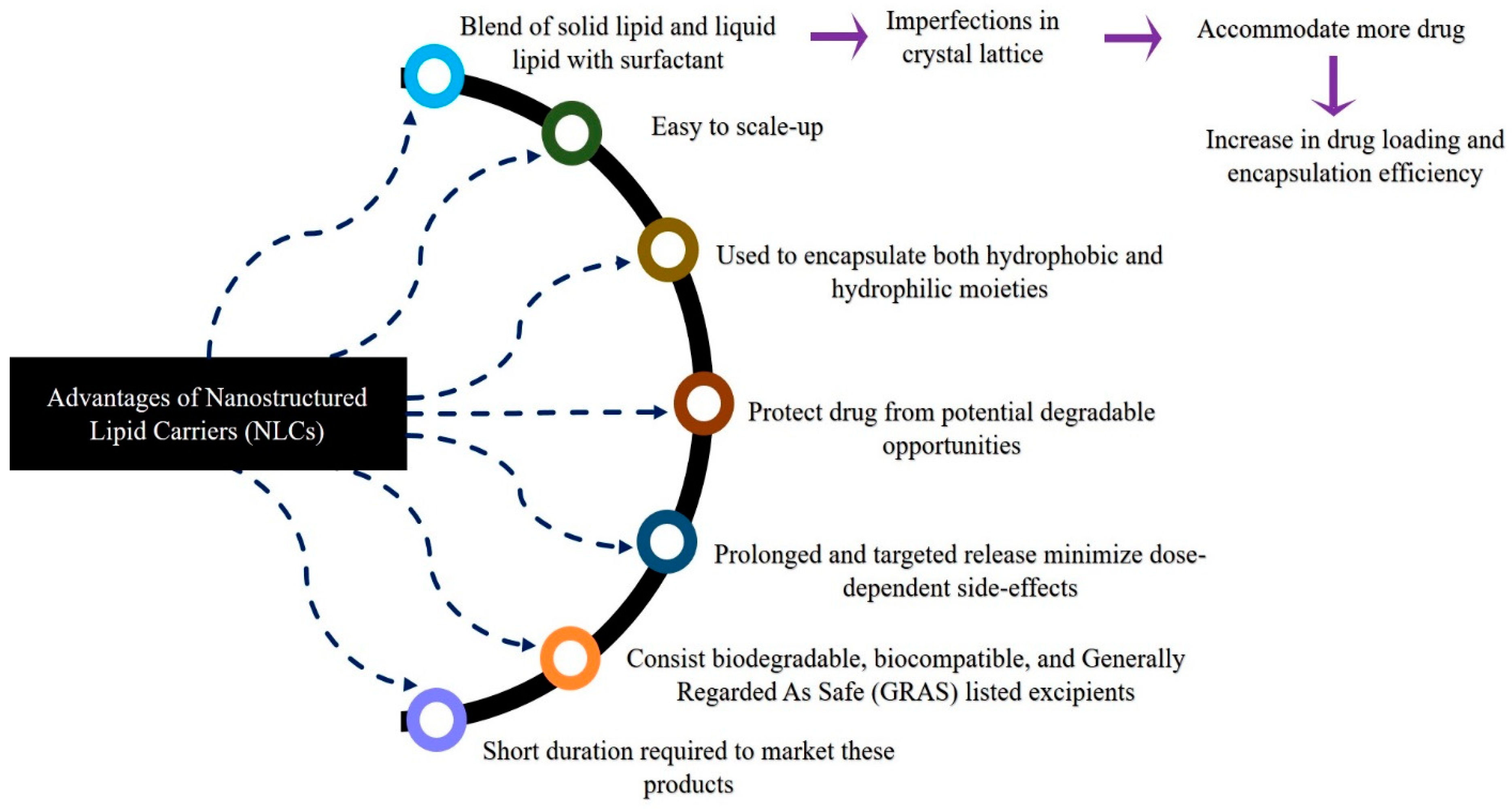
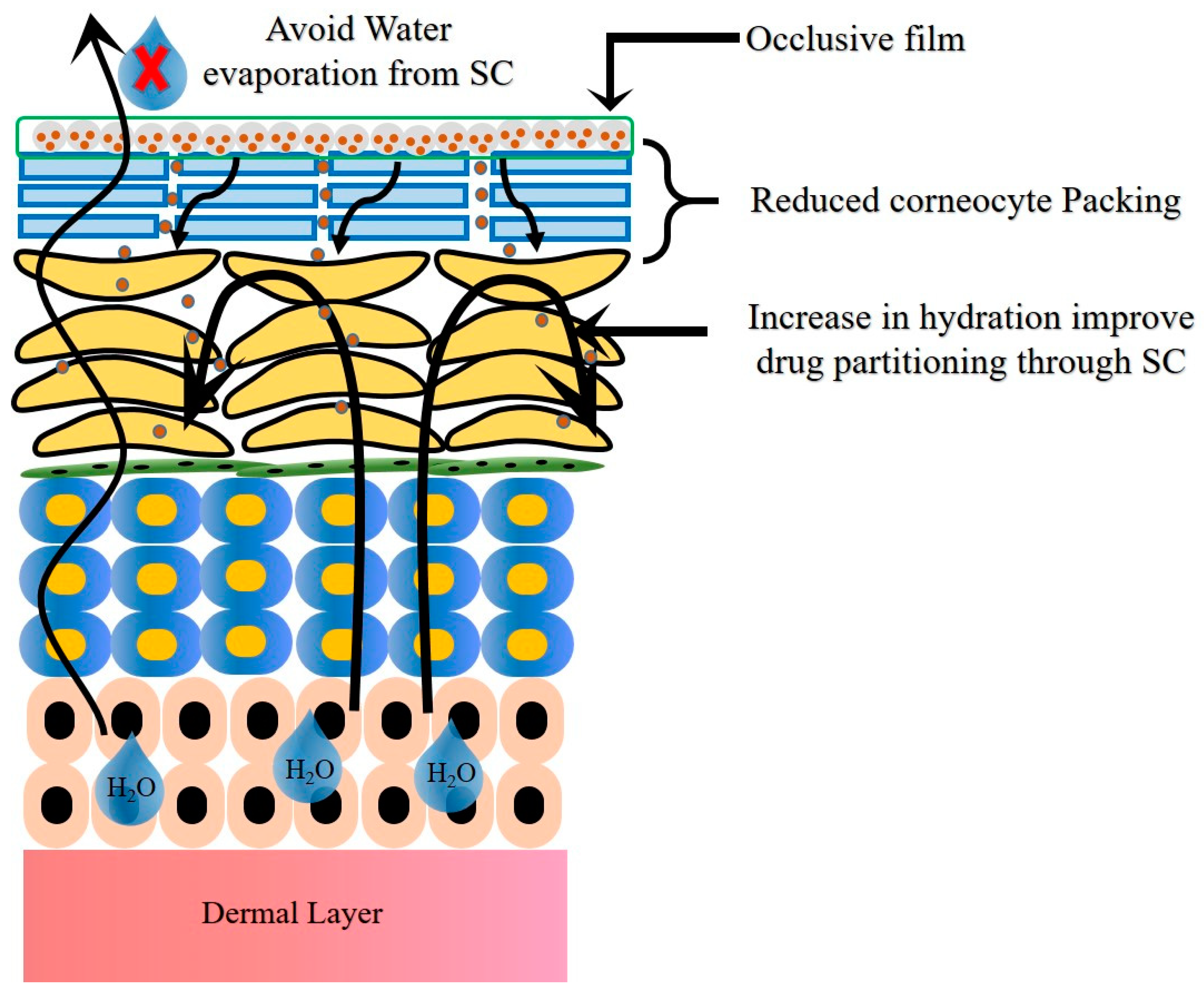
3. Nanostructured Lipid Carriers (NLCs): Advantages, Rationale, and Mode of Permeation for Treating Psoriasis
4. Selection of Excipients in Fabrication of SLNs and NLCs and Their Roles
5. Detailed Account of NLCs for Treating Psoriasis
5.1. Comparative Assessment Studies of NLCs with Other Nano-Lipoidal Carriers
5.2. Dual Drug-Loaded NLCs for Psoriasis Treatment
5.3. Single Drug-Loaded NLCs for Psoriasis Treatment
5.3.1. Acitretin
5.3.2. Methotrexate (MTX)
5.3.3. Fluocinolone Acetonide (FA)
5.3.4. Curcumin
5.3.5. Apremilast (APM)
5.3.6. Pentoxifylline (PTX)
5.3.7. Fucoxanthin (FUCO)
5.3.8. Dithranol (DTN)
5.3.9. Mometasone Furoate (MF)
5.4. Patent Information
6. Regulatory Aspects
7. Summary
8. Future Prospective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Report on Psoriasis 2016. Available online: https://apps.who.int/iris/handle/10665/204417 (accessed on 20 January 2023).
- Thappa, D.; Munisamy, M. Research on psoriasis in India: Where do we stand? Indian J. Med. Res 2017, 146, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M. Nanostructured Lipid Carriers: A New Approach for Psoriasis Dermal Therapy. Master’s Thesis, University of Porto, Porto, Portugal, 2015; pp. 1–115. [Google Scholar]
- Ghate, V.; Kodoth, A.; Shah, A.; Vishalakshi, B.; Lewis, S. Colloidal nanostructured lipid carriers of pentoxifylline produced by microwave irradiation ameliorates imiquimod-induced psoriasis in mice. Colloids Surf. B Biointerfaces 2019, 181, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Rapalli, V.; Kaul, V.; Waghule, T.; Gorantla, S.; Sharma, S.; Roy, A.; Dubey, S.; Singhvi, G. Curcumin loaded nanostructured lipid carriers for enhanced skin retained topical delivery: Optimization, scale-up, in-vitro characterization and assessment of ex-vivo skin deposition. Eur. J. Pharm. Sci. 2020, 152, 105438. [Google Scholar] [CrossRef]
- Mahajan, R.; Handa, S. Pathophysiology of psoriasis. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 1–9. [Google Scholar]
- Hugh, J.; Weinberg, J. Update on the pathophysiology of psoriasis. Cutis 2018, 102, 6–12. [Google Scholar]
- Yamanaka, K.; Yamamoto, O.; Honda, T. Pathophysiology of psoriasis: A review. J. Dermatol. 2021, 48, 722–731. [Google Scholar] [CrossRef]
- Benhadou, F.; Mintoff, D.; Del Marmol, V. Psoriasis: Keratinocytes or immune cells—which is the trigger? Dermatology 2019, 235, 91–100. [Google Scholar] [CrossRef]
- Griffiths, C.E.M.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J.N.W.N. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef]
- Kim, W.; Jerome, D.; Yeung, J. Diagnosis and management of psoriasis. Can. Fam. Physician. 2017, 63, 278–285. [Google Scholar]
- Rajagopalan, M.; Chatterjee, M.; De, A.; Dogra, S.; Ganguly, S.; Kar, B.; Madnani, N.; Neema, S.; Parasramani, S.; Patel, K.; et al. Systemic management of psoriasis patients in Indian scenario: An expert consensus. Indian Dermatol. Online J. 2021, 12, 674–682. [Google Scholar] [CrossRef]
- Ogawa, E.; Sato, Y.; Minagawa, A.; Okuyama, R. Pathogenesis of psoriasis and development of treatment. J. Dermatol. 2018, 45, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.; Read, C. Pathophysiology, clinical presentation, and treatment of psoriasis: A review. Jama 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Warren, E.; Khanderia, U. Use of retinoids in the treatment of psoriasis. Clin. Pharm. 1989, 8, 344–351. [Google Scholar] [PubMed]
- American Academy of Dermatology Association. Psoriasis Treatment: Coal Tar. Available online: https://www.aad.org/public/diseases/psoriasis/treatment/medications/coal-tar (accessed on 20 January 2023).
- Coal tar and Dithranol. Meyler’s Side Effects of Drugs, The International Encyclopedia of Adverse Drug Reactions and Interactions, 16th ed.; Aronson, J.K., Ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 487–489. [Google Scholar]
- Pradhan, M.; Singh, D.; Murthy, S.; Singh, M. Design, characterization and skin permeating potential of Fluocinolone acetonide loaded nanostructured lipid carriers for topical treatment of psoriasis. Steroids 2015, 101, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Petkar, K.; Sawant, K. Development, evaluation and clinical studies of Acitretin loaded nanostructured lipid carriers for topical treatment of psoriasis. Int. J. Pharm. 2010, 401, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Mahajan, U.; Mahajan, H.; Ojha, S. Methotrexate-loaded nanostructured lipid carrier gel alleviates imiquimod-induced psoriasis by moderating inflammation: Formulation, optimization, characterization, in-vitro and in-vivo studies. Int. J. Nanomed. 2020, 15, 4763–4778. [Google Scholar] [CrossRef]
- Rahman, M.; Akhter, S.; Ahmad, J.; Ahmad, M.; Beg, S.; Ahmad, F. Nanomedicine-based drug targeting for psoriasis: Potentials and emerging trends in nanoscale pharmacotherapy. Expert Opin. Drug Deliv. 2015, 12, 635–652. [Google Scholar] [CrossRef]
- Puglia, C.; Bonina, F. Lipid nanoparticles as novel delivery systems for cosmetics and dermal pharmaceuticals. Expert. Opin. Drug Deliv. 2012, 9, 429–441. [Google Scholar] [CrossRef]
- Nordin, U.; Ahmad, N.; Salim, N.; Yusof, N. Lipid-based nanoparticles for psoriasis treatment: A review on conventional treatments, recent works, and future prospects. RSC Adv. 2021, 11, 29080–29101. [Google Scholar] [CrossRef]
- Muller, R.; Radtke, M.; Wissing, S. Nanostructured lipid matrices for improved microencapsulation of drugs. Int. J. Pharm. 2002, 242, 121–128. [Google Scholar] [CrossRef]
- Chauhan, I.; Yasir, M.; Verma, M.; Singh, A. Nanostructured lipid carriers: A groundbreaking approach for transdermal drug delivery. Adv. Pharm. Bull. 2020, 10, 150–165. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.; Zimmer, A.; Pardeike, J. Solid lipid nanoparticles (SLN) and nanostructured lipid carriers (NLC) for pulmonary application: A review of the state of the art. Eur. J. Pharm. Biopharm. 2014, 86, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Patil, T.; Deshpande, A. Nanostructured lipid carriers-based drug delivery for treating various lung diseases: A state-of-the-art review. Int. J. Pharm. 2018, 547, 209–225. [Google Scholar] [CrossRef]
- Patil, T.; Deshpande, A.; Deshpande, S.; Shende, P. Targeting pulmonary tuberculosis using nanocarrier-based dry powder inhalation: Current status and futuristic need. J. Drug Target 2019, 27, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, U.; Gupta, M.; Vyas, S. Capsaicin delivery into the skin with lipidic nanoparticles for the treatment of psoriasis. Artif. Cells Nanomed. Biotechnol. 2015, 43, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.; Katiyar, S.; Kushwah, V.; Jain, S. Solid lipid nanoparticles and nanostructured lipid carrier-based nanotherapeutics in treatment of psoriasis: A comparative study. Expert. Opin. Drug Deliv. 2017, 14, 165–177. [Google Scholar] [CrossRef]
- Pinto, M.; Moura, C.; Nunes, C.; Segundo, M.; Lima, S.; Reis, S. A new topical formulation for psoriasis: Development of methotrexate-loaded nanostructured lipid carriers. Int. J. Pharm. 2014, 477, 519–526. [Google Scholar] [CrossRef]
- Borgia, S.; Regehly, M.; Sivaramakrishnan, R.; Mehnert, W.; Korting, H.; Danker, K.; Röder, B.; Kramer, K.; Schäfer-Korting, M. Lipid nanoparticles for skin penetration enhancement—Correlation to drug localization within the particle matrix as determined by fluorescence and parelectric spectroscopy. J. Control. Release 2005, 110, 151–163. [Google Scholar] [CrossRef]
- Kilfoyle, B.; Sheihet, L.; Zhang, Z.; Laohoo, M.; Kohn, J.; Michniak-Kohn, B. Development of paclitaxel-TyroSpheres for topical skin treatment. J. Control. Release 2012, 63, 18–24. [Google Scholar] [CrossRef]
- Lin, Y.; Huang, Z.; Zhuo, R.; Fang, J. Combination of calcipotriol and methotrexate in nanostructured lipid carriers for topical delivery. Int. J. Nanomed. 2010, 5, 117–128. [Google Scholar]
- Baroli, B. Penetration of nanoparticles and nanomaterials in the skin: Fiction or reality? J. Pharm. Sci. 2010, 99, 21–50. [Google Scholar] [CrossRef] [PubMed]
- Souto, E.; Almeida, A.; Müller, R. Lipid nanoparticles (SLN®, NLC®) for cutaneous drug delivery: Structure, protection and skin effects. J. Biomed. Nanotech. 2007, 3, 317–331. [Google Scholar] [CrossRef]
- Raza, K.; Singh, B.; Lohan, S.; Sharma, G.; Negi, P.; Yachha, Y.; Katare, O. Nano-lipoidal carriers of tretinoin with enhanced percutaneous absorption, photostability, biocompatibility and anti-psoriatic activity. Int. J. Pharm. 2013, 456, 65–72. [Google Scholar] [CrossRef]
- Madan, J.; Khobaragade, S.; Dua, K.; Awasthi, R. Formulation, optimization, and in vitro evaluation of nanostructured lipid carriers for topical delivery of Apremilast. Dermatol. Ther. 2020, 33, e13370. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, P.; Kumar, A.; Jain, P.; Patel, J. Carbomer gel bearing methotrexate loaded lipid nanocontainers shows improved topical delivery intended for effective management of psoriasis. Int. J. Biol. Macromol. 2018, 120, 1322–1334. [Google Scholar] [CrossRef]
- Viegas, J.S.R.; Praca, F.G.; Caron, A.L.; Suzuki, I.; Silvestrini, A.V.P.; Medina, W.S.G.; Del Ciampo, J.O.; Kravicz, M.; Bentley, M.V.L.B. Nanostructured lipid carrier co-delivering tacrolimus and TNF-α siRNA as an innovate approach to psoriasis. Drug Deliv. Trans. Res. 2020, 10, 646–660. [Google Scholar] [CrossRef]
- Avasatthi, V.; Pawar, H.; Dora, C.; Bansod, P.; Gill, M.; Suresh, S. A novel nanogel formulation of methotrexate for topical treatment of psoriasis: Optimization, in vitro and in vivo evaluation. Pharm. Dev. Technol. 2016, 21, 554–562. [Google Scholar] [CrossRef]
- Kesharwani, P.; Jain, A.; Srivastava, A.; Keshari, M. Systematic development and characterization of curcumin-loaded nanogel for topical application. Drug Dev. Ind. Pharm. 2020, 46, 1443–1457. [Google Scholar] [CrossRef]
- Sathe, P.; Saka, R.; Kommineni, N.; Raza, K.; Khan, W. Dithranol-loaded nanostructured lipid carrier-based gel ameliorate psoriasis in imiquimod-induced mice psoriatic plaque model. Drug Dev. Ind. Pharm. 2019, 45, 826–838. [Google Scholar] [CrossRef]
- Kang, N.; Kim, M.; Sohn, S.; Kim, K.; Park, J.; Lee, S.; Lee, J.; Kim, D. Curcumin-loaded lipid-hybridized cellulose nanofiber film ameliorates imiquimod-induced psoriasis-like dermatitis in mice. Biomaterials 2018, 182, 245–258. [Google Scholar] [CrossRef]
- Cordenonsi, L.; Faccendini, A.; Catanzaro, M.; Bonferoni, M.; Rossi, S.; Malavasi, L.; Raffin, R.; Schapoval, E.; Lanni, C.; Sandri, G.; et al. The role of chitosan as coating material for nanostructured lipid carriers for skin delivery of fucoxanthin. Int. J. Pharm. 2019, 567, 118487. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Sharma, K.; Bedi, N. Topical nanostructured lipid carrier based hydrogel of mometasone furoate for the treatment of psoriasis. Pharm. Nanotechnol. 2018, 6, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, M.; Sahu, K.; Singh, D.; Singh, M.; Yadav, K. A Method of Preparation of Triamcinolone Acetonide Encapsulated Nanostructured Lipid Carriers for Psoriasis Treatment. AU2021106678, 18 November 2021. [Google Scholar]
- Parmar, M.; Patel, L.; Rathod, L.; Parikh, K. Nanostructured Lipid Carriers Containing Tazarotene and Pharmaceutical Formulations Containing Said Particles. IN201921023616, 18 December 2020. [Google Scholar]
- Kudamala, R.; Suggala, V.; Veeram, J.; Palagati, S. Antipsoriatic Effects of Clobetasol Loaded Nanostructured Lipid Carriers on Imiquimod Induced Psoriasis. IN202141009486, 12 March 2021. [Google Scholar]
- Kudamala, R.; Shaik, C.; Veeram, J.; Medarametla, K.; Anna, B.; Chiruthanur, M.C.G.; Ponnaiah, B.; Ranganatham, V.; Palagati, S. Clobetasol Loaded Solid Lipid Nanoparticles and Nanostructured Lipid Carriers for Topical Treatment of Psoriasis. IN202141046636, 5 November 2021. [Google Scholar]
- Shah, M.; Panigrahi, L.; Patravale, V.; Kakade, P. Topical Composition. IN201921019828, 27 November 2020. [Google Scholar]
- Yan, C.; Zhenhai, Z.; Zhou, L.; Qingqing, W. Tripterine Nanostructure Lipid Carrier and Preparation Method and Application Thereof. CN102225205B, 13 March 2013. [Google Scholar]
- Sachdeva, M.; Patlolla, R. Novel Nanoparticle Formulations for Skin Delivery. US20120195957A1, 6 May 2014. [Google Scholar]
- Foulkes, R.; Man, E.; Thind, J.; Yeung, S.; Joy, A.; Hoskins, C. The regulation of nanomaterials and nanomedicines for clinical application: Current and future perspectives. Biomater. Sci. 2020, 8, 4653–4664. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Evaluation of Nanopharmaceuticals in India; Department of Biotechnology, Government of India: New Delhi, India, 2019; pp. 1–36. Available online: https://dbtindia.gov.in/sites/default/files/uploadfiles/Guidelines_For_Evaluation_of_Nanopharmaceuticals_in_India_24.10.19.pdf (accessed on 20 January 2023).
- Javed, S.; Mangla, B.; Almoshari, Y.; Sultan, M.H.; Ahsan, W. Nanostructured Lipid carrier system: A compendium of their formulation development approaches, optimization strategies by quality by design, and recent applications in drug delivery. Nanotechnol. Rev. 2022, 11, 1744–1777. [Google Scholar] [CrossRef]
- Muller, R.H.; Shegokar, R.; Keck, C.M. 20 years of lipid nanoparticles (SLN&NLC): Present state of development&industrial applications. Curr. Drug Discov. Technol. 2011, 8, 207–227. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Type of Therapy | Drug Candidates | Adverse Effects of Current Therapy |
|---|---|---|---|
| 1. | Topical therapy (ointments, creams, lotions, gels, or foams applied to the skin | Vitamin D3 analogues (e.g., calcitriol, calcipotriol) | Cutaneous irritation, itching, burning, dryness of skin |
| Corticosteroids, e.g., betamethasone dipropionate, hydrocortisone, clobetasol propionate, triamcinolone acetonide, mometasone furoate, Fluocinolone acetonide, etc. | Dermal atrophy, acne-like skin, decreased pigmentation, allergic contact dermatitis, and their long-term use suppresses the body’s immune system | ||
| Anthralin/dithranol | Irritating, burning, staining, and necrosis | ||
| Retinoids, e.g., tazarotine, acetratin, etretinate | Cheilitis, alopecia, desquamation, drying of mucous membranes, pruritus, etc. | ||
| Calcineurin inhibitors, e.g., tacrolimus, pimecrolimus | Burning, pruritus, and erythema | ||
| Tar | Irritation, rash, or acne-like skin, skin burning, and makes skin more subtle to ultraviolet (UV) light | ||
| Diathranol | Skin irritation, pruritus, erythema, dry skin, eczema rash, etc. | ||
| Keratolytic agents, e.g., omega-3 fatty acids, cod liver oil, salicylic acid, etc. | Skin irritation, burning, peeling, etc. | ||
| 2. | Phototherapy | UV-B therapy Psoralen plus UV-A therapy (PUVA) | Photo aging, sunburn, and erythema |
| 3. | Systemic therapies (tablets or injections/infusion) | Methotrexate | Nausea, malaise, elevated transaminases, bone marrow suppression, gastrointestinal ulcers, pneumonitis, etc. |
| Cyclosporin | Kidney failure, hypertension, gingival hyperplasia, headache, hypertrichosis | ||
| Acitretin | Hyperlipidemia, liver toxicity, teratogenicity, mucocutaneous lesions, etc. | ||
| Biologic agents, e.g., infliximab, etanercept, adalimumab, secukinumab, etc. | Candidiasis observed with secukinumab in initial stages of therapy; infusion reactions common with infliximab | ||
| Oral small molecules, e.g., apremilast | Diarrhea, augmented gastrocolic reflex, depression, weight loss, upper respiratory tract infection (URTI), nasopharyngitis, etc. |
| Sr. No. | Categories of Excipients | In Vitro/Ex Vivo Studies | In Vivo Studies | Ref. | ||||
|---|---|---|---|---|---|---|---|---|
| Solid Lipids | Liquid Lipids | Surfactants/Co-Surfactants (Emulsifier) | Other Excipients | Organic Solvents | ||||
| 1. | Palmitic acid | Oleic acid | Surfactant mixture (smix) of Tween 20®®: Span 60®®: n-butanol in a ratio 3.5:1.0:0.5 | - | - | NLCs exhibited initial sustained release phase for the first 10 h and subsequent steady state release of Acitretin. | Clinical study depicted significant reduction in erythema, followed by marked reduction in scaling, indicating moderate to excellent improvement in the disease symptoms. | [4] |
| 2. | Glyceryl distearate (Precirol®® ATO 5) | Oleoyl polyoxyl-6 glycerides (Labrafil M1944 CS) | Poloxamers and polysorbate 80 | - | - | Curcumin-NLCs demonstrated 48 h in vitro release with 3.24-fold improved permeation and skin retention. | - | [5] |
| 3. | Compritol®® 888 ATO | Medium chain triglyceride (MCT) (Miglyol®® 812) | Polysorbate 80 | - | Methanol and acetone (1:1, v/v): for dissolving lipids and drug | Fluocinolone acetonide NCLs showed prolonged drug release with significant amount of drug in epidermal and dermal layer of skin. | - | [18] |
| 4. | Compritol 888 | Capmul®® MCM | - | - | Acidified isopropyl alcohol (IPA): to dissolve lipids | Methotrexate release with sustained and steady release over a period of 30 h | Methotrexate NLC gel exhibited significant anti-psoriasis activity as compared to the control and plain methotrexate gel formulation. | [20] |
| 5. | Compritol 888 ATO | Oleic acid | L- α egg phosphatidylcholine | - | Acetone and ethanol(1:1): to dissolve drug | Capsaicin NLCs showed better drug penetration than SLNs with higher amount of drug retention. | Capsaicin NLCs showed 8.7-fold higher accumulation of drug in viable skin. | [29] |
| 6. | Glyceryl monostearate | Castor oil (Cremophor RH40) | Sorbitan monolaurate (Span 20) PEG-40 Hydrogenated | Carbopol®® 934P NF polyacrylic acid-based gelling agent: for better hydration and retention of gel | - | HaCaT cell line study revealed higher uptake and efficacy due to decreased cell viability for NLC. | The anti-psoriatic effect increased significantly as compared to drug-loaded SLN and marketed formulations. | [30] |
| 7. | Combinations of hard fat, polyoxyethylene, (25) cetyl stearyl ether, and glyceryl ricinoleate (stabilized) (Witepsol®® S51); | Oleic acid | Polysorbate 60 and polysorbate 80 | - | - | Methotrexate was released from the NLCs in vitro in a fast release pattern, reaching 70% in 2 h. Increased skin permeation on methotrexate compared with the free drug. | - | [31] |
| 8. | Glyceryl palmitostearate (Precirol) Palmitinic acid monoglycerides (Myverol™ 18–04 K) | Squalene | Polyoxyethylene-polyoxypropylene block copolymer (pluronic F-68) | - | Chloroform: methanol (2:1 v/v): for dissolving lipid | In vitro permeation study suggests calcipotriol NLCs easily penetrated into the stratum corneum. Skin permeation of methotrexate NLCs was enhanced 2.4 to 4.4 times versus control. | Confocal laser scanning microscopy (CLSM) showed good topical delivery of calcipotriol and methotrexate. | [34] |
| 9. | Glyceryl dibehenate (Compritol®® 888 ATO) | Isopropyl myristate | Tween 80 | Butylated hydroxytoluene (BHT): preservative | Ethanol: to dissolve tretinoin drug and BHT | Tretinoin NLCs provided significantly higher skin retention and permeation when compared to other products such as liposomes, ethosomes, SLNs, etc. | The mouse tail model demonstrated improved tretinoin NLC efficacy. NLCs demonstrated comparable and improved orthokeratosis compared to other drug products. | [37] |
| 10. | Compritol®® 888 ATO | Oleic acid | Polysorbate (Tween) 80 or 60 or 20 | Carbomers (Carbopol®® 974P NF, Carbopol®® 980, Carbopol®® 940): for preparation of NLC-gel | Transcutol P: as a penetration enhancer | Apremilast NLCs showed sustained release over a period of 9 h. Apremilast NLC-based hydrogel showed 60.1% skin deposition. | - | [38] |
| 11. | Glyceryl monostearate | Oleic acid | - | Carbomer 934: as geling agent | Acetone and ethanol (1:1 v/v): for dissolving lipids with/without drug | Methotrexate-loaded NLC hydrogel showed prolonged release over period of 24 h. | - | [39] |
| 12. | Glycerol distearate | Oleic acid | Poloxamer 407 | Polyethylenimine (PEI): a transfection agent for siRNA | - | Tacrolimus NLCs showed sustained release over a period of 24 h with zero-order release kinetics. | NLCs prevented the appearance of inflammation and psoriatic plaque with significant inhibition of TNF-α. | [40] |
| 13. | Precirol®® ATO 5 | Triglycerides of caprylic acid and capric acid (Captex®® 300); | Poloxamer 407 | Mannitol: cryo protectant in freeze drying | - | Methotrexate NLCs exhibited sustained release over a period of 48 h. | Imiquimod-induced psoriasis model depicted normal skin structure with very mild keratosis. | [41] |
| 14. | Precirol®® ATO 5 | Glyceryl monocaprylate (Capmul®® MCM C-8 EP) | Tween 80®® | Triethanolamine: to maintain the pH of NLC-nano gel | Methanol: to dissolve curcumin drug | Curcumin NLCs depicted sustained release over the period of 24 h (in vivo) and prolonged permeation for 24 h (ex vivo). | - | [42] |
| 15. | Precirol®® ATO 5 | Propylene glycol dicaprolate (Labrafac™ PG) | Tween 20®® | Methylcellulose: thickening/suspending agent in preparation of NLC-nanogel | Chloroform: to dissolve drug and antioxidants | Dithranol NLCs exhibited sustained release of dithranol over 24 h. | Imiquimo-induced psoriatic plaque model suggests reduction in psoriatic symptoms in mice. | [43] |
| 16. | Butyrospermum parkii (Shea) butter (Jarplex™ SB35) | - | - | Acetone: to dissolve lipids and drug | In contrast to normal skin, psoriatic skin depicted higher levels of curcumin deposition in the epidermis. | Alleviation of psoriatic skin symptoms in imiquimo-induced mice | [44] | |
| 17. | Bacuri butter | Tucuma oil | Sorbitan monooleate (Span 80®®) and polysorbate 80 Chitosan: to coat NLCs for enhancing bio adhesion and improving biopharmaceutical properties | - | - | NLCs depicted improved cellular uptake, cell viability, and fibrolast uptake of fucoxanthin. | - | [45] |
| 18. | Stearic acid | - | Tween 80®® and Transcutol P (2:1 ratio) | - | - | Permeation study revealed prolonged release of mometasone furoate with Higuchi release kinetics. | Treatment with the prepared NLC formulation completely eliminated the parakeratosis in the imiquimo-induced mouse model. | [46] |
| Sr. No. | Title of Patent | Name of Inventors | Patent Grant No./Application No. | Summary of Invention |
|---|---|---|---|---|
| 1. | A Method of Preparation of Triamcinolone Acetonide-Encapsulated Nanostructured Lipid Carriers For Psoriasis Treatment | Pradhan, M; Sahu, K.K.; Singh, D.; Singh, M.R.; Yadav, K. | AU2021106678 |
|
| 2. | Nanostructured Lipid Carriers Containing Tazarotene and Pharmaceutical Formulations Containing Said Particles | Parmar, M.; Patel, L.D.; Rathod, L.; Parikh, K. | IN201921023616 |
|
| 3. | Antipsoriatic Effects of Clobetasol-Loaded Nanostructured Lipid Carriers on Imiquimod-Induced Psoriasis | Kudamala, R.R.; Suggala, V. S.; Veeram, J. R.; Palagati, S. | IN202141009486 |
|
| 4. | Clobetasol-Loaded Solid Lipid Nanoparticles and Nanostructured Lipid Carriers for Topical Treatment of Psoriasis | Kudamala, R.R.; Shaik, C. B.; Veeram, J.R.; Medarametla, K. B.; Anna, B.; Challa M.C.; Chiruthanur, G.; Ponnaiah, B.R.K.; Ranganatham, V.P.; Palagati, S. | IN202141046636 |
|
| 5. | Topical Composition | Shah, M.; Panigrahi, L.; Patravale, V.; Kakade, P. | IN201921019828 |
|
| 6. | Tripterine Nanostructure Lipid Carrier and Preparation Method and Application Thereof | Yan, C.; Zhenhai, Z.; Zhou, Lei; Qingqing, Wu. | CN102225205B |
|
| 7. | Novel Nanoparticle Formulations for Skin Delivery | Sachdeva, M.S.; Patlolla, R. | US20120195957A1 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patil, T.S.; Gujarathi, N.A.; Aher, A.A.; Pachpande, H.E.; Sharma, C.; Ojha, S.; Goyal, S.N.; Agrawal, Y.O. Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery. Int. J. Mol. Sci. 2023, 24, 2978. https://doi.org/10.3390/ijms24032978
Patil TS, Gujarathi NA, Aher AA, Pachpande HE, Sharma C, Ojha S, Goyal SN, Agrawal YO. Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery. International Journal of Molecular Sciences. 2023; 24(3):2978. https://doi.org/10.3390/ijms24032978
Chicago/Turabian StylePatil, Tulshidas S., Nayan A. Gujarathi, Abhijeet A. Aher, Hemal E. Pachpande, Charu Sharma, Shreesh Ojha, Sameer N. Goyal, and Yogeeta O. Agrawal. 2023. "Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery" International Journal of Molecular Sciences 24, no. 3: 2978. https://doi.org/10.3390/ijms24032978
APA StylePatil, T. S., Gujarathi, N. A., Aher, A. A., Pachpande, H. E., Sharma, C., Ojha, S., Goyal, S. N., & Agrawal, Y. O. (2023). Recent Advancements in Topical Anti-Psoriatic Nanostructured Lipid Carrier-Based Drug Delivery. International Journal of Molecular Sciences, 24(3), 2978. https://doi.org/10.3390/ijms24032978