
The Role of Genetics in the Development and Pharmacotherapy of Depression and Its Impact on Drug Discovery




Abstract
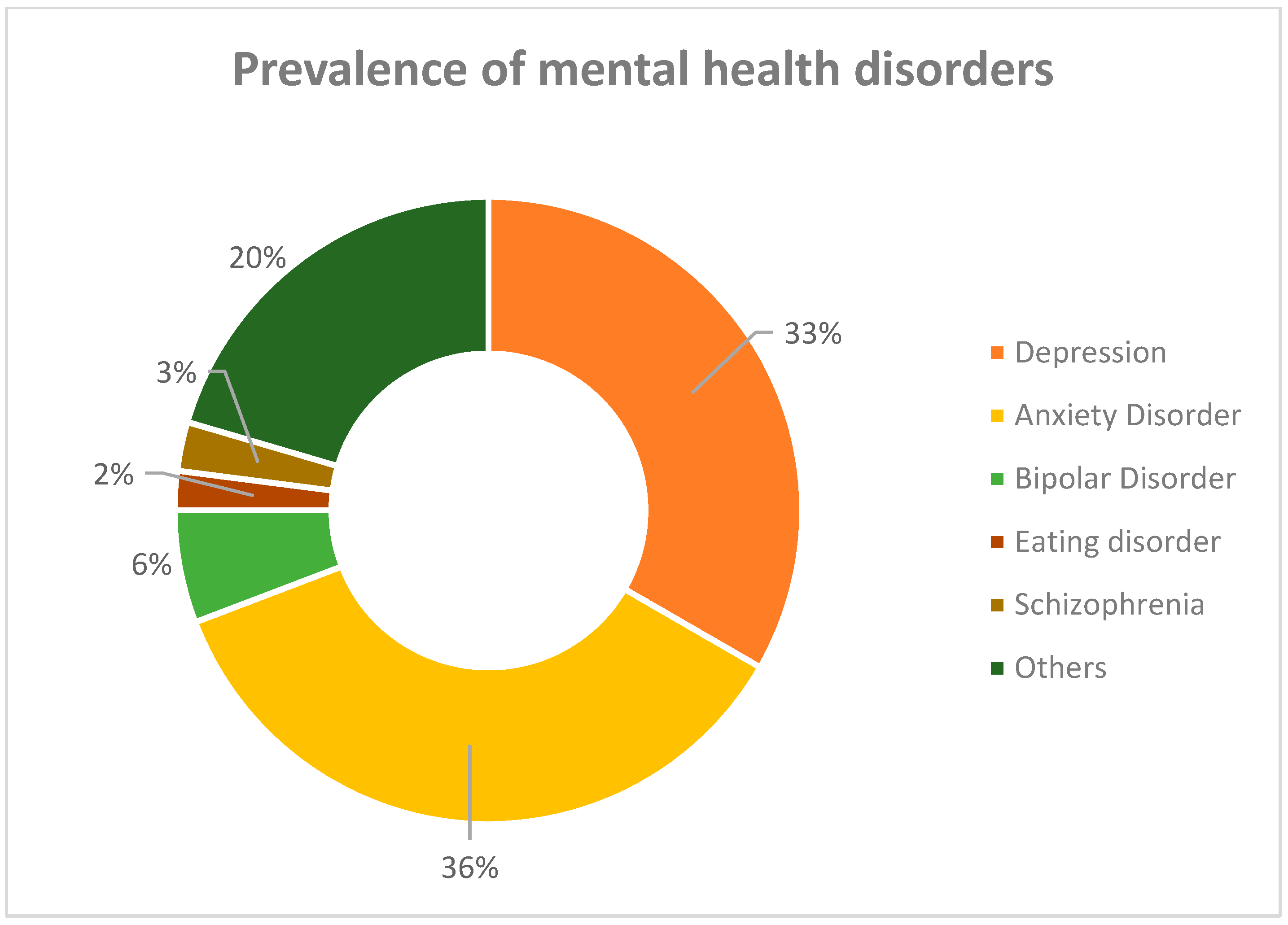
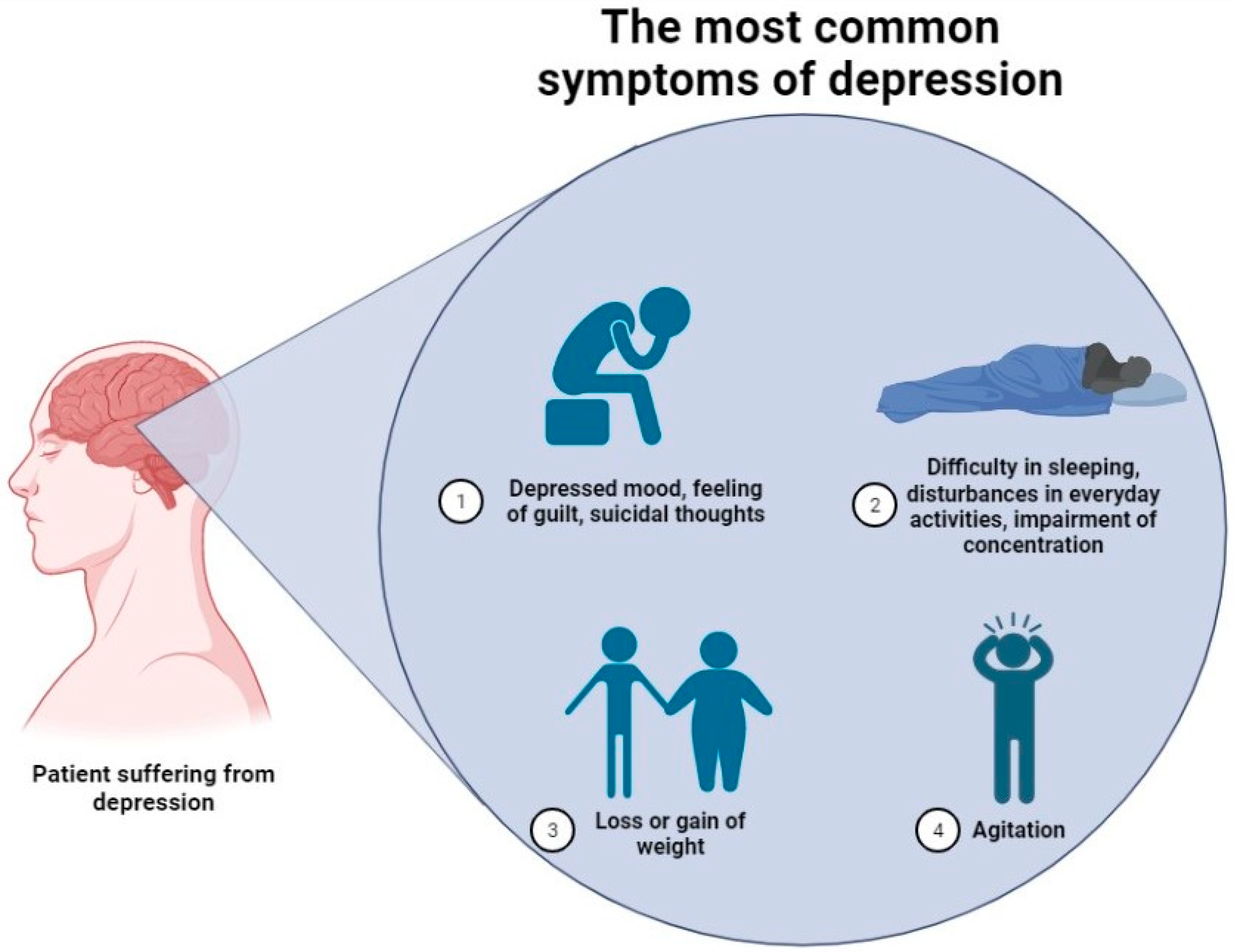
1. Introduction
2. Hereditary Picture of Depression
3. Studies on the Contribution of Certain Genes
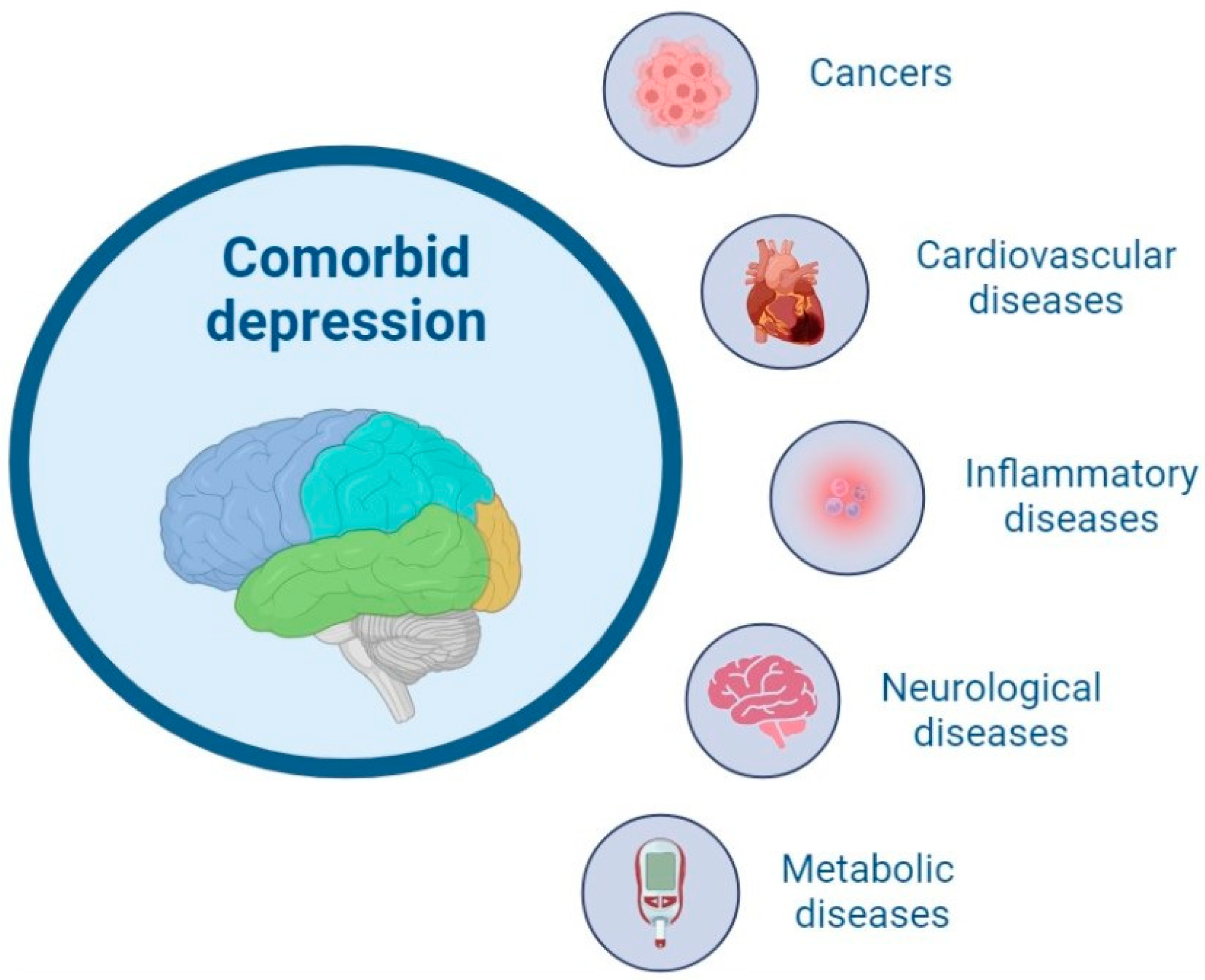
4. Genes Linking Depression with Other Disorders?
5. Approaches Promising for Treatment-Resistant Patients
- Augmentative or adjunctive therapy (using a second medication, which in most cases does not belong to the antidepressant category, e.g., including a lithium-containing agent as an addition to the standard tricyclic antidepressant pharmacotherapy);
- Optimizing, combining, or switching classes of administered antidepressant medication;
- Psychotherapy in addition to some somatic or pharmacological treatments;
- Different forms of brain stimulation therapy were proven to be successful as an alternative therapeutical strategy [64].
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dattani, S.; Ritchie, H.; Roser, M. Mental Health. Our World in Data 2021. Available online: https://ourworldindata.org/mental-health (accessed on 23 January 2023).
- Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief, 2 March 2022. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 15 November 2022).
- Shadrina, M.; Bondarenko, E.A.; Slominsky, P.A. Genetics Factors in Major Depression Disease. Front. Psychiatry 2018, 9, 334. [Google Scholar] [CrossRef]
- Elliott, M. Gender Differences in Causes of Depression. Women Health 2001, 33, 183–198. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Shreck, E.; Batchelder, A. Hamilton Rating Scale for Depression (HAM-D). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 887–888. ISBN 978-1-4419-1005-9. [Google Scholar]
- Adapted from “Brain with Circular Callout (Layout)”; “Risk Factors for Stroke”, by BioRender.com (2023). Available online: https://app.biorender.com/biorender-templates (accessed on 23 January 2023).
- Kendall, K.M.; Assche, E.V.; Andlauer, T.F.M.; Choi, K.W.; Luykx, J.J.; Schulte, E.C.; Lu, Y. The Genetic Basis of Major Depression. Psychol. Med. 2021, 51, 2217–2230. [Google Scholar] [CrossRef]
- Definition of Hereditary Syndrome-NCI Dictionary of Cancer Terms-NCI. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/hereditary-syndrome (accessed on 18 November 2022).
- Pettersson, E.; Lichtenstein, P.; Larsson, H.; Song, J.; Agrawal, A.; Børglum, A.D.; Bulik, C.M.; Daly, M.J.; Davis, L.K.; Demontis, D.; et al. Genetic Influences on Eight Psychiatric Disorders Based on Family Data of 4 408 646 Full and Half-Siblings, and Genetic Data of 333 748 Cases and Controls. Psychol. Med. 2019, 49, 1166–1173. [Google Scholar] [CrossRef]
- Turner, J.R. Family Studies (Genetics). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 773–774. ISBN 978-1-4419-1005-9. [Google Scholar]
- Joseph, J. Behavioral Genetics. In Encyclopedia of Critical Psychology; Teo, T., Ed.; Springer: New York, NY, USA, 2014; pp. 151–156. ISBN 978-1-4614-5583-7. [Google Scholar]
- Sullivan, P.F.; Neale, M.C.; Kendler, K.S. Genetic Epidemiology of Major Depression: Review and Meta-Analysis. Am. J. Psychiatry 2000, 157, 1552–1562. [Google Scholar] [CrossRef]
- Happonen, M.; Pulkkinen, L.; Kaprio, J.; Van der Meere, J.; Viken, R.J.; Rose, R.J. The Heritability of Depressive Symptoms: Multiple Informants and Multiple Measures. J. Child Psychol. Psychiatry 2002, 43, 471–479. [Google Scholar] [CrossRef]
- Jansson, M.; Gatz, M.; Berg, S.; Johansson, B.; Malmberg, B.; McCLEARN, G.E.; Schalling, M.; Pedersen, N.L. Gender Differences in Heritability of Depressive Symptoms in the Elderly. Psychol. Med. 2004, 34, 471–479. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gatz, M.; Gardner, C.O.; Pedersen, N.L. A Swedish National Twin Study of Lifetime Major Depression. Am. J. Psychiatry 2006, 163, 109–114. [Google Scholar] [CrossRef]
- Fernandez-Pujals, A.M.; Adams, M.J.; Thomson, P.; McKechanie, A.G.; Blackwood, D.H.R.; Smith, B.H.; Dominiczak, A.F.; Morris, A.D.; Matthews, K.; Campbell, A.; et al. Epidemiology and Heritability of Major Depressive Disorder, Stratified by Age of Onset, Sex, and Illness Course in Generation Scotland: Scottish Family Health Study (GS:SFHS). PLoS ONE 2015, 10, e0142197. [Google Scholar] [CrossRef]
- Shively, C.A.; Register, T.C.; Friedman, D.P.; Morgan, T.M.; Thompson, J.; Lanier, T. Social Stress-Associated Depression in Adult Female Cynomolgus Monkeys (Macaca Fascicularis). Biol. Psychol. 2005, 69, 67–84. [Google Scholar] [CrossRef]
- Cheslack-Postava, K.; Keyes, K.M.; Lowe, S.R.; Koenen, K.C. Oral Contraceptive Use and Psychiatric Disorders in a Nationally Representative Sample of Women. Arch. Womens Ment. Health 2015, 18, 103–111. [Google Scholar] [CrossRef]
- Albert, P.R. Why Is Depression More Prevalent in Women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Shi, P.; Yang, A.; Zhao, Q.; Chen, Z.; Ren, X.; Dai, Q. A Hypothesis of Gender Differences in Self-Reporting Symptom of Depression: Implications to Solve Under-Diagnosis and Under-Treatment of Depression in Males. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef]
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Blumberg, S.J. Estimated Prevalence of Autism and Other Developmental Disabilities Following Questionnaire Changes in the 2014 National Health Interview Survey. Natl. Health Stat. Report 2015, 1–20. [Google Scholar]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef]
- Kang, H.-J.; Park, Y.; Yoo, K.-H.; Kim, K.-T.; Kim, E.-S.; Kim, J.-W.; Kim, S.-W.; Shin, I.-S.; Yoon, J.-S.; Kim, J.H.; et al. Sex Differences in the Genetic Architecture of Depression. Sci. Rep. 2020, 10, 9927. [Google Scholar] [CrossRef]
- Beckman, G.; Beckman, L.; Cedergren, B.; Perris, C.; Strandman, E. Serum Protein and Red Cell Enzyme Polymorphisms in Affective Disorders. Hum. Hered. 1978, 28, 41–47. [Google Scholar] [CrossRef]
- Belujon, P.; Grace, A.A. Dopamine System Dysregulation in Major Depressive Disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef]
- Anguelova, M.; Benkelfat, C.; Turecki, G. A Systematic Review of Association Studies Investigating Genes Coding for Serotonin Receptors and the Serotonin Transporter: I. Affective Disorders. Mol. Psychiatry 2003, 8, 574–591. [Google Scholar] [CrossRef]
- Jacobs, R.H.; Orr, J.L.; Gowins, J.R.; Forbes, E.E.; Langenecker, S.A. Biomarkers of Intergenerational Risk for Depression: A Review of Mechanisms in Longitudinal High-Risk (LHR) Studies. J. Affect. Disord. 2015, 175, 494–506. [Google Scholar] [CrossRef]
- Hu, X.-Z.; Lipsky, R.H.; Zhu, G.; Akhtar, L.A.; Taubman, J.; Greenberg, B.D.; Xu, K.; Arnold, P.D.; Richter, M.A.; Kennedy, J.L.; et al. Serotonin Transporter Promoter Gain-of-Function Genotypes Are Linked to Obsessive-Compulsive Disorder. Am. J. Hum. Genet. 2006, 78, 815–826. [Google Scholar] [CrossRef]
- Wendland, J.R.; Martin, B.J.; Kruse, M.R.; Lesch, K.-P.; Murphy, D.L. Simultaneous Genotyping of Four Functional Loci of Human SLC6A4, with a Reappraisal of 5-HTTLPR and Rs25531. Mol. Psychiatry 2006, 11, 224–226. [Google Scholar] [CrossRef]
- Wendland, J.R.; Moya, P.R.; Kruse, M.R.; Ren-Patterson, R.F.; Jensen, C.L.; Timpano, K.R.; Murphy, D.L. A Novel, Putative Gain-of-Function Haplotype at SLC6A4 Associates with Obsessive-Compulsive Disorder. Hum Mol. Genet. 2008, 17, 717–723. [Google Scholar] [CrossRef]
- Su, S.; Zhao, J.; Bremner, J.D.; Miller, A.H.; Tang, W.; Bouzyk, M.; Snieder, H.; Novik, O.; Afzal, N.; Goldberg, J.; et al. Serotonin Transporter Gene, Depressive Symptoms, and Interleukin-6. Circ. Cardiovasc. Genet 2009, 2, 614–620. [Google Scholar] [CrossRef]
- Kautzky, A.; James, G.M.; Philippe, C.; Baldinger-Melich, P.; Kraus, C.; Kranz, G.S.; Vanicek, T.; Gryglewski, G.; Hartmann, A.M.; Hahn, A.; et al. Epistasis of HTR1A and BDNF Risk Genes Alters Cortical 5-HT1A Receptor Binding: PET Results Link Genotype to Molecular Phenotype in Depression. Transl. Psychiatry 2019, 9, 5. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, X.; Yu, Y.; Han, Y.; Wei, J.; Collier, D.; Li, T.; Ma, X. The Role of Single Nucleotide Polymorphism of D2 Dopamine Receptor Gene on Major Depressive Disorder and Response to Antidepressant Treatment. Psychiatry Res. 2012, 200, 1047–1050. [Google Scholar] [CrossRef]
- DeRijk, R.H.; Schaaf, M.; de Kloet, E.R. Glucocorticoid Receptor Variants: Clinical Implications. J. Steroid Biochem. Mol. Biol. 2002, 81, 103–122. [Google Scholar] [CrossRef]
- Tafet, G.E.; Nemeroff, C.B. The Links Between Stress and Depression: Psychoneuroendocrinological, Genetic, and Environmental Interactions. J. Neuropsychiatry Clin. Neurosci. 2016, 28, 77–88. [Google Scholar] [CrossRef]
- Appel, K.; Schwahn, C.; Mahler, J.; Schulz, A.; Spitzer, C.; Fenske, K.; Stender, J.; Barnow, S.; John, U.; Teumer, A.; et al. Moderation of Adult Depression by a Polymorphism in the FKBP5 Gene and Childhood Physical Abuse in the General Population. Neuropsychopharmacol. 2011, 36, 1982–1991. [Google Scholar] [CrossRef]
- Bai, S.; Guo, W.; Feng, Y.; Deng, H.; Li, G.; Nie, H.; Guo, G.; Yu, H.; Ma, Y.; Wang, J.; et al. Efficacy and Safety of Anti-Inflammatory Agents for the Treatment of Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. J. Neurol. Neurosurg. Psychiatry 2020, 91, 21–32. [Google Scholar] [CrossRef]
- Barnes, J.; Mondelli, V.; Pariante, C.M. Genetic Contributions of Inflammation to Depression. Neuropsychopharmacology 2017, 42, 81–98. [Google Scholar] [CrossRef]
- Ancelin, M.-L.; Farré, A.; Carrière, I.; Ritchie, K.; Chaudieu, I.; Ryan, J. C-Reactive Protein Gene Variants: Independent Association with Late-Life Depression and Circulating Protein Levels. Transl. Psychiatry 2015, 5, e499. [Google Scholar] [CrossRef]
- Giménez-Palomo, A.; Dodd, S.; Anmella, G.; Carvalho, A.F.; Scaini, G.; Quevedo, J.; Pacchiarotti, I.; Vieta, E.; Berk, M. The Role of Mitochondria in Mood Disorders: From Physiology to Pathophysiology and to Treatment. Front. Psychiatry 2021, 12. [Google Scholar]
- Cataldo, A.M.; McPhie, D.L.; Lange, N.T.; Punzell, S.; Elmiligy, S.; Ye, N.Z.; Froimowitz, M.P.; Hassinger, L.C.; Menesale, E.B.; Sargent, L.W.; et al. Abnormalities in Mitochondrial Structure in Cells from Patients with Bipolar Disorder. Am. J. Pathol. 2010, 177, 575–585. [Google Scholar] [CrossRef]
- Hyde, C.L.; Nagle, M.W.; Tian, C.; Chen, X.; Paciga, S.A.; Wendland, J.R.; Tung, J.Y.; Hinds, D.A.; Perlis, R.H.; Winslow, A.R. Identification of 15 Genetic Loci Associated with Risk of Major Depression in Individuals of European Descent. Nat. Genet. 2016, 48, 1031–1036. [Google Scholar] [CrossRef]
- Howard, D.M.; Adams, M.J.; Clarke, T.-K.; Hafferty, J.D.; Gibson, J.; Shirali, M.; Coleman, J.R.I.; Hagenaars, S.P.; Ward, J.; Wigmore, E.M.; et al. Genome-Wide Meta-Analysis of Depression Identifies 102 Independent Variants and Highlights the Importance of the Prefrontal Brain Regions. Nat. Neurosci. 2019, 22, 343–352. [Google Scholar] [CrossRef]
- Howard, D.M.; Adams, M.J.; Shirali, M.; Clarke, T.-K.; Marioni, R.E.; Davies, G.; Coleman, J.R.I.; Alloza, C.; Shen, X.; Barbu, M.C.; et al. Genome-Wide Association Study of Depression Phenotypes in UK Biobank Identifies Variants in Excitatory Synaptic Pathways. Nat. Commun. 2018, 9, 1470. [Google Scholar] [CrossRef]
- Kamran, M.; Bibi, F.; ur. Rehman, A.; Morris, D.W. Major Depressive Disorder: Existing Hypotheses about Pathophysiological Mechanisms and New Genetic Findings. Genes 2022, 13, 646. [Google Scholar] [CrossRef]
- Shirvani-Farsani, Z.; Maloum, Z.; Bagheri-Hosseinabadi, Z.; Vilor-Tejedor, N.; Sadeghi, I. DNA Methylation Signature as a Biomarker of Major Neuropsychiatric Disorders. J. Psychiatr. Res. 2021, 141, 34–49. [Google Scholar] [CrossRef]
- Bohacek, J.; Gapp, K.; Saab, B.J.; Mansuy, I.M. Transgenerational Epigenetic Effects on Brain Functions. Biol. Psychiatry 2013, 73, 313–320. [Google Scholar] [CrossRef]
- Lehotzky, A.; Lau, P.; Tőkési, N.; Muja, N.; Hudson, L.D.; Ovádi, J. Tubulin Polymerization-Promoting Protein (TPPP/P25) Is Critical for Oligodendrocyte Differentiation. Glia 2010, 58, 157–168. [Google Scholar] [CrossRef]
- Vincze, O.; Oláh, J.; Zádori, D.; Klivényi, P.; Vécsei, L.; Ovádi, J. A New Myelin Protein, TPPP/P25, Reduced in Demyelinated Lesions Is Enriched in Cerebrospinal Fluid of Multiple Sclerosis. Biochem. Biophys. Res. Comm. 2011, 409, 137–141. [Google Scholar] [CrossRef]
- Cao, H.; Wang, J.; Baranova, A.; Zhang, F. Classifying Major Mental Disorders Genetically. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 112, 110410. [Google Scholar] [CrossRef]
- Mulugeta, A.; Zhou, A.; King, C.; Hyppönen, E. Association between Major Depressive Disorder and Multiple Disease Outcomes: A Phenome-Wide Mendelian Randomisation Study in the UK Biobank. Mol. Psychiatry 2020, 25, 1469–1476. [Google Scholar] [CrossRef]
- Rogers, D.; Pies, R. General Medical Drugs Associated with Depression. Psychiatry 2008, 5, 28–41. [Google Scholar]
- Gold, S.M.; Köhler-Forsberg, O.; Moss-Morris, R.; Mehnert, A.; Miranda, J.J.; Bullinger, M.; Steptoe, A.; Whooley, M.A.; Otte, C. Comorbid Depression in Medical Diseases. Nat. Rev. Dis. Primers 2020, 6, 69. [Google Scholar] [CrossRef]
- Cosci, F.; Fava, G.A. When Anxiety and Depression Coexist: The Role of Differential Diagnosis Using Clinimetric Criteria. Psychother. Psychosom. 2021, 90, 308–317. [Google Scholar] [CrossRef]
- McTeague, L.M.; Rosenberg, B.M.; Lopez, J.W.; Carreon, D.M.; Huemer, J.; Jiang, Y.; Chick, C.F.; Eickhoff, S.B.; Etkin, A. Identification of Common Neural Circuit Disruptions in Emotional Processing Across Psychiatric Disorders. Am. J. Psychiatry 2020, 177, 411–421. [Google Scholar] [CrossRef]
- Kalin, N.H. The Critical Relationship between Anxiety and Depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef]
- Siddiqi, S.H.; Taylor, S.F.; Cooke, D.; Pascual-Leone, A.; George, M.S.; Fox, M.D. Distinct Symptom-Specific Treatment Targets for Circuit-Based Neuromodulation. Am. J. Psychiatry 2020, 177, 435–446. [Google Scholar] [CrossRef]
- Zhou, C.; Kong, D.; Zhu, X.; Wu, W.; Xue, R.; Li, G.; Xu, Y.; Liu, S.; Tian, H.; Zhuo, C. Rethinking Schizophrenia and Depression Comorbidity as One Psychiatric Disorder Entity: Evidence from Mouse Model. Front. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Rothschild, A.J. Challenges in the Treatment of Major Depressive Disorder with Psychotic Features. Schizophr. Bull. 2013, 39, 787–796. [Google Scholar] [CrossRef]
- Kang, H.-J.; Kim, S.-Y.; Bae, K.-Y.; Kim, S.-W.; Shin, I.-S.; Yoon, J.-S.; Kim, J.-M. Comorbidity of Depression with Physical Disorders: Research and Clinical Implications. Chonnam Med. J. 2015, 51, 8–18. [Google Scholar] [CrossRef]
- Whooley, M.A.; Wong, J.M. Depression and Cardiovascular Disorders. Ann. Rev. Clin. Psychol. 2013, 9, 327–354. [Google Scholar] [CrossRef]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and Cardiovascular Disease: A Clinical Review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef]
- Jukic, M.; Milosavljević, F.; Molden, E.; Ingelman-Sundberg, M. Pharmacogenomics in Treatment of Depression and Psychosis: An Update. Trends Pharmacol. Sci. 2022, 43, 1055–1069. [Google Scholar] [CrossRef]
- Voineskos, D.; Daskalakis, Z.J.; Blumberger, D.M. Management of Treatment-Resistant Depression: Challenges and Strategies. Neuropsychiatr. Dis. Treat. 2020, 16, 221–234. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Suganuma, A.; Ostinelli, E.G.; Andersson, G.; Beevers, C.G.; Shumake, J.; Berger, T.; Boele, F.W.; Buntrock, C.; Carlbring, P.; et al. Dismantling, Optimising, and Personalising Internet Cognitive Behavioural Therapy for Depression: A Systematic Review and Component Network Meta-Analysis Using Individual Participant Data. Lancet Psychiatry 2021, 8, 500–511. [Google Scholar] [CrossRef]
- Cacabelos, R.; Torrellas, C.; López-Muñoz, F. Pharmacogenomics of Antidepressant Drugs. In Melatonin, Neuroprotective Agents and Antidepressant Therapy; López-Muñoz, F., Srinivasan, V., de Berardis, D., Álamo, C., Kato, T.A., Eds.; Springer: New Delhi, India, 2016; pp. 545–609. ISBN 978-81-322-2803-5. [Google Scholar]
- Milosavljevic, F.; Bukvic, N.; Pavlovic, Z.; Miljevic, C.; Pešic, V.; Molden, E.; Ingelman-Sundberg, M.; Leucht, S.; Jukic, M.M. Association of CYP2C19 and CYP2D6 Poor and Intermediate Metabolizer Status with Antidepressant and Antipsychotic Exposure: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2021, 78, 270–280. [Google Scholar] [CrossRef]
- Greden, J.F.; Parikh, S.V.; Rothschild, A.J.; Thase, M.E.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; Forester, B.P.; Mondimore, F.M.; Shelton, R.C.; et al. Impact of Pharmacogenomics on Clinical Outcomes in Major Depressive Disorder in the GUIDED Trial: A Large, Patient- and Rater-Blinded, Randomized, Controlled Study. J. Psychiatr. Res. 2019, 111, 59–67. [Google Scholar] [CrossRef]
- Perlis, R.H.; Dowd, D.; Fava, M.; Lencz, T.; Krause, D.S. Randomized, Controlled, Participant- and Rater-Blind Trial of Pharmacogenomic Test-Guided Treatment versus Treatment as Usual for Major Depressive Disorder. Depress. Anxiety 2020, 37, 834–841. [Google Scholar] [CrossRef]
- Oslin, D.W.; Lynch, K.G.; Shih, M.-C.; Ingram, E.P.; Wray, L.O.; Chapman, S.R.; Kranzler, H.R.; Gelernter, J.; Pyne, J.M.; Stone, A.; et al. Effect of Pharmacogenomic Testing for Drug-Gene Interactions on Medication Selection and Remission of Symptoms in Major Depressive Disorder: The PRIME Care Randomized Clinical Trial. JAMA 2022, 328, 151–161. [Google Scholar] [CrossRef]
- Porcelli, S.; Fabbri, C.; Serretti, A. Meta-Analysis of Serotonin Transporter Gene Promoter Polymorphism (5-HTTLPR) Association with Antidepressant Efficacy. Eur. Neuropsychopharmacol. 2012, 22, 239–258. [Google Scholar] [CrossRef]
- Chung, W.-H.; Hung, S.-I.; Hong, H.-S.; Hsih, M.-S.; Yang, L.-C.; Ho, H.-C.; Wu, J.-Y.; Chen, Y.-T. A Marker for Stevens–Johnson Syndrome. Nature 2004, 428, 486. [Google Scholar] [CrossRef]
- Viikki, M.; Huuhka, K.; Leinonen, E.; Illi, A.; Setälä-Soikkeli, E.; Huuhka, M.; Mononen, N.; Lehtimäki, T.; Kampman, O. Interaction between Two HTR2A Polymorphisms and Gender Is Associated with Treatment Response in MDD. Neurosci. Lett. 2011, 501, 20–24. [Google Scholar] [CrossRef]
- McMahon, F.J.; Buervenich, S.; Charney, D.; Lipsky, R.; Rush, A.J.; Wilson, A.F.; Sorant, A.J.M.; Papanicolaou, G.J.; Laje, G.; Fava, M.; et al. Variation in the Gene Encoding the Serotonin 2A Receptor Is Associated with Outcome of Antidepressant Treatment. Am. J. Hum. Genet. 2006, 78, 804–814. [Google Scholar] [CrossRef]
- Andre, K.; Kampman, O.; Setälä-Soikkeli, E.; Viikki, M.; Poutanen, O.; Nuolivirta, T.; Mononen, N.; Lehtimäki, T.; Leinonen, E.; Illi, A. Temperament Profiles, 5-HT2A Genotype, and Response to Treatment with SSRIs in Major Depression. J. Neural Transm. 2010, 117, 1431–1434. [Google Scholar] [CrossRef]
- Gong, L.; Whirl-Carrillo, M.; Klein, T.E. PharmGKB, an Integrated Resource of Pharmacogenomic Knowledge. Curr. Protoc. 2021, 1, e226. [Google Scholar] [CrossRef]
- Firouzabadi, D.; Firouzabadi, N.; Kalani, K.; Zomorrodian, K.; Tehrani, E.S. Response to Sertraline Is Influenced by GNβ3 Gene G-350A Variant in Patients with Major Depressive Disorder. Eur. J. Clin. Pharmacol. 2019, 75, 189–194. [Google Scholar] [CrossRef]
- Bahramali, E.; Firouzabadi, N.; Yavarian, I.; Shayesteh, M.R.H.; Erfani, N.; Shoushtari, A.A.; Asadpour, R. Influence of ACE Gene on Differential Response to Sertraline versus Fluoxetine in Patients with Major Depression: A Randomized Controlled Trial. Eur. J. Clin. Pharmacol. 2016, 72, 1059–1064. [Google Scholar] [CrossRef]
- Kim, H.; Lim, S.-W.; Kim, S.; Kim, J.-W.; Chang, Y.H.; Carroll, B.J.; Kim, D.K. Monoamine Transporter Gene Polymorphisms and Antidepressant Response in Koreans with Late-Life Depression. JAMA 2006, 296, 1609–1618. [Google Scholar] [CrossRef]
- Elias, E.; Zhang, A.Y.; Manners, M.T. Novel Pharmacological Approaches to the Treatment of Depression. Life 2022, 12, 196. [Google Scholar] [CrossRef]
- Henter, I.D.; de Sousa, R.T.; Gold, P.W.; Brunoni, A.R.; Zarate, C.A.; Machado-Vieira, R. Mood Therapeutics: Novel Pharmacological Approaches for Treating Depression. Expert Rev. Clin. Pharmacol. 2017, 10, 153–166. [Google Scholar] [CrossRef]
- Lutz, P.-E.; Kieffer, B.L. Opioid Receptors: Distinct Roles in Mood Disorders. Trends Neurosci. 2013, 36, 195–206. [Google Scholar] [CrossRef]
- Wagstaff, A.J.; Ormrod, D.; Spencer, C.M. Tianeptine. Mol. Diag. Ther. 2001, 15, 231–259. [Google Scholar] [CrossRef]
- Haj-Mirzaian, A.; Nikbakhsh, R.; Ramezanzadeh, K.; Rezaee, M.; Amini-Khoei, H.; Haj-Mirzaian, A.; Ghesmati, M.; Afshari, K.; Haddadi, N.-S.; Dehpour, A.R. Involvement of Opioid System in Behavioral Despair Induced by Social Isolation Stress in Mice. Biomed. Pharmacother. 2019, 109, 938–944. [Google Scholar] [CrossRef]
- Van’t Veer, A.; Carlezon, W.A. Role of Kappa-Opioid Receptors in Stress and Anxiety-Related Behavior. Psychopharmacology 2013, 229, 435–452. [Google Scholar] [CrossRef]
- Morgan, M.M.; Christie, M.J. Analysis of Opioid Efficacy, Tolerance, Addiction and Dependence from Cell Culture to Human. Br. J. Pharmacol. 2011, 164, 1322–1334. [Google Scholar] [CrossRef]
- Lei, T.; Dong, D.; Song, M.; Sun, Y.; Liu, X.; Zhao, H. Rislenemdaz Treatment in the Lateral Habenula Improves Despair-like Behavior in Mice. Neuropsychopharmacology 2020, 45, 1717–1724. [Google Scholar] [CrossRef]
- Liu, W.; Li, Q.; Ye, B.; Cao, H.; Shen, F.; Xu, Z.; Du, W.; Guo, F.; Liu, J.; Li, T.; et al. Repeated Nitrous Oxide Exposure Exerts Antidepressant-Like Effects through Neuronal Nitric Oxide Synthase Activation in the Medial Prefrontal Cortex. Front. Psychiatry 2020, 11, 837. [Google Scholar] [CrossRef]
- Nagele, P.; Duma, A.; Kopec, M.; Gebara, M.A.; Parsoei, A.; Walker, M.; Janski, A.; Panagopoulos, V.N.; Cristancho, P.; Miller, J.P.; et al. Nitrous Oxide for Treatment-Resistant Major Depression: A Proof-of-Concept Trial. Biol. Psychiatry 2015, 78, 10–18. [Google Scholar] [CrossRef]
- Lüscher Dias, T.; Schuch, V.; Beltrão-Braga, P.C.B.; Martins-de-Souza, D.; Brentani, H.P.; Franco, G.R.; Nakaya, H.I. Drug Repositioning for Psychiatric and Neurological Disorders through a Network Medicine Approach. Transl. Psychiatry 2020, 10, 1–10. [Google Scholar] [CrossRef]
- De Giorgi, R.; Cowen, P.J.; Harmer, C.J. Statins in Depression: A Repurposed Medical Treatment Can Provide Novel Insights in Mental Health. Int. Rev. Psychiatry 2022, 1–16. [Google Scholar] [CrossRef]
- Carboni, E.; Carta, A.R.; Carboni, E.; Novelli, A. Repurposing Ketamine in Depression and Related Disorders: Can This Enigmatic Drug Achieve Success? Front. Neurosci. 2021, 15, 657714. [Google Scholar] [CrossRef]
- Das, J. Repurposing of Drugs–The Ketamine Story. J. Med. Chem. 2020, 63, 13514–13525. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Substance Name | Gene (Variant) | Association |
|---|---|---|
| SERTRALINE | GNB3 (rs5441) G- protein subunit beta-3 gene | Patients holding a GG genotype were significantly more likely to respond to sertraline than those with AA or AG genotypes [77]. |
| ACE (rs1799752) Angiotensin I converting enzyme | Patients with depressive disorder holding del/del genotype are associated with an increased response to sertraline [78]. | |
| SLC6A4 (SLC6A4 HTTLPR long—l allele; short—s allele) Solute carrier family 6 member 4 | SLC6A4 HTTLPR short form is associated with an increased response to sertraline in people with major depressive disorder (as compared with l-allele) [79]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zięba, A.; Matosiuk, D.; Kaczor, A.A. The Role of Genetics in the Development and Pharmacotherapy of Depression and Its Impact on Drug Discovery. Int. J. Mol. Sci. 2023, 24, 2946. https://doi.org/10.3390/ijms24032946
Zięba A, Matosiuk D, Kaczor AA. The Role of Genetics in the Development and Pharmacotherapy of Depression and Its Impact on Drug Discovery. International Journal of Molecular Sciences. 2023; 24(3):2946. https://doi.org/10.3390/ijms24032946
Chicago/Turabian StyleZięba, Agata, Dariusz Matosiuk, and Agnieszka A. Kaczor. 2023. "The Role of Genetics in the Development and Pharmacotherapy of Depression and Its Impact on Drug Discovery" International Journal of Molecular Sciences 24, no. 3: 2946. https://doi.org/10.3390/ijms24032946
APA StyleZięba, A., Matosiuk, D., & Kaczor, A. A. (2023). The Role of Genetics in the Development and Pharmacotherapy of Depression and Its Impact on Drug Discovery. International Journal of Molecular Sciences, 24(3), 2946. https://doi.org/10.3390/ijms24032946