
Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides



Abstract
1. Introduction
2. Results
2.1. Evaluation Metrics
2.2. Quantitave Analysis
3. Materials and Methods
3.1. The Datasets
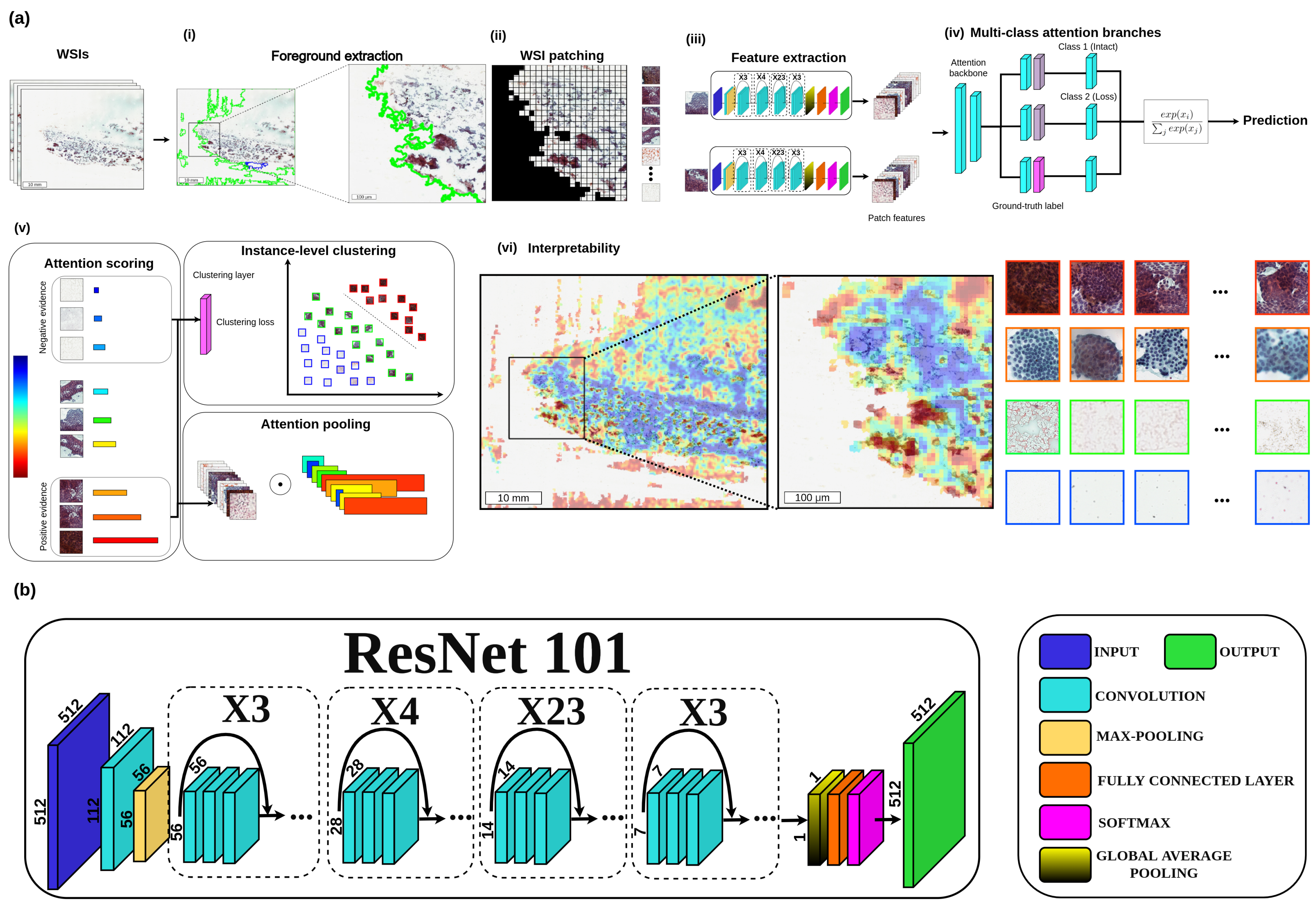
3.2. Methods
3.3. Proposed CLAM-Based Method
3.4. Implementation Details
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, H.; Chen, D.; He, J.; He, Y.; Liu, L.; Zhou, D. Trend of Sudden Unexpected Death in Epilepsy Incidence Rate in Rural West China. Front. Neurol. 2021, 12, 735201. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.; Junit, S.; Ng, K.; Jayapalan, J.; Karikalan, B.; Hashim, O. Papillary thyroid cancer: Genetic alterations and molecular biomarker investigations. Int. J. Med. Sci. 2019, 16, 450. [Google Scholar] [CrossRef] [PubMed]
- Fugazzola, L.; Elisei, R.; Fuhrer, D.; Jarzab, B.; Leboulleux, S.; Newbold, K.; Smit, J. 2019 European Thyroid Association guidelines for the treatment and follow-up of advanced radioiodine-refractory thyroid cancer. Eur. Thyroid J. 2019, 8, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Laha, D.; Nilubol, N.; Boufraqech, M. New therapies for advanced thyroid cancer. Front. Endocrinol. 2020, 11, 82. [Google Scholar] [CrossRef] [PubMed]
- Rodon, J.; Soria, J.; Berger, R.; Miller, W.; Rubin, E.; Kugel, A.; Tsimberidou, A.; Saintigny, P.; Ackerstein, A.; Braña, I.; et al. Genomic and transcriptomic profiling expands precision cancer medicine: The WINTHER trial. Nat. Med. 2019, 25, 751–758. [Google Scholar] [CrossRef]
- Nikiforova, M.; Tseng, G.; Steward, D.; Diorio, D.; Nikiforov, Y. MicroRNA expression profiling of thyroid tumors: Biological significance and diagnostic utility. J. Clin. Endocrinol. Metab. 2008, 93, 1600–1608. [Google Scholar] [CrossRef]
- Li, D.; Zhang, Y.; Xu, H.; Zhang, X. The role of BRAF in the pathogenesis of thyroid carcinoma. Front. Biosci.-Landmark 2015, 20, 1068–1078. [Google Scholar]
- Brose, M.; Cabanillas, M.; Cohen, E.; Wirth, L.; Riehl, T.; Yue, H.; Sherman, S.; Sherman, E. Vemurafenib in patients with BRAFV600E-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: A non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1272–1282. [Google Scholar] [CrossRef]
- Dunn, L.; Sherman, E.; Baxi, S.; Tchekmedyian, V.; Grewal, R.; Larson, S.; Pentlow, K.; Haque, S.; Tuttle, R.; Sabra, M.; et al. Vemurafenib redifferentiation of BRAF mutant, RAI-refractory thyroid cancers. J. Clin. Endocrinol. Metab. 2019, 104, 1417–1428. [Google Scholar] [CrossRef]
- Rothenberg, S.; McFadden, D.; Palmer, E.; Daniels, G.; Wirth, L. Redifferentiation of Iodine-Refractory BRAF V600E-Mutant Metastatic Papillary Thyroid Cancer with Dabraf-enib. Clin. Cancer Res. 2015, 21, 1028–1035. [Google Scholar] [CrossRef]
- Hornick, J. Replacing Molecular Genetic Testing with Immunohisto-chemistry Using Antibodies That Recognize the Protein Products of Gene Rearrange-ments:“Next-Generation” Immunohistochemistry. Am. J. Surg. Pathol. 2021, 45, 584–586. [Google Scholar] [CrossRef]
- Singarayer, R.; Mete, O.; Perrier, L.; Thabane, L.; Asa, S.; Van Uum, S.; Ezzat, S.; Goldstein, D.; Sawka, A. A systematic review and meta-analysis of the diagnostic performance of BRAF V600E immunohistochemistry in thyroid histopathology. Endocr. Pathol. 2019, 30, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Choden, S.; Keelawat, S.; Jung, C.; Bychkov, A. VE1 immunohistochemistry improves the limit of genotyping for detecting BRAF V600E mutation in papillary thyroid cancer. Cancers 2020, 12, 596. [Google Scholar] [CrossRef] [PubMed]
- Choden, S.; Keelawat, S.; Jung, C.; Bychkov, A. An affordable immuno-histochemical approach to estimate the prevalence of BRAFV600E in large cohort studies—Establishing the baseline rate of BRAF mutation in an institutional series of papillary thyroid carcinoma from Thailand. Gland Surg. 2020, 9, 1867. [Google Scholar] [CrossRef] [PubMed]
- Fadda, G.; Rossi, E. Liquid-based cytology in fine-needle aspiration biopsies of the thyroid gland. Acta Cytol. 2011, 55, 389–400. [Google Scholar] [CrossRef]
- Feldkamp, J.; Führer, D.; Luster, M.; Musholt, T.; Spitzweg, C.; Schott, M. Fine needle aspiration in the investigation of thyroid nodules: Indications, procedures and interpretation. Dtsch. Aerzteblatt Int. 2016, 113, 353. [Google Scholar]
- Baum, J.; Soong, L.; Scognamiglio, T.; Margolskee, E.; Hoda, R.; Rao, R. Cytological diagnosis of papillary thyroid carcinoma with tall cells on ThinPrep liquid-based cytology. Diagn. Cytopathol. 2019, 47, 541–546. [Google Scholar] [CrossRef]
- Choi, J.; Shim, H.; Song, J.; Chae, S.; Lee, Y.; Kim, J.; Kim, S. Image analysis of peripheral compression artefacts of ThinPrep® liquid-based cytology preparations. Cytopathology 2013, 24, 99–104. [Google Scholar] [CrossRef]
- Wei, Y.; Lu, Y.; Li, C. Clinical Application of Ultrasound-Guided Thyroid Fine Needle Aspiration Biopsy and Thinprep Cytology Test in Diagnosis of Thyroid Disease. Asian Pac. J. Cancer Prev. APJCP 2016, 17, 4689. [Google Scholar]
- Jiang, Y.; Yang, M.; Wang, S.; Li, X.; Sun, Y. Emerging role of deep learning-based artificial intelligence in tumor pathology. Cancer Commun. 2020, 40, 154–166. [Google Scholar] [CrossRef]
- Kuenzi, B.; Park, J.; Fong, S.; Sanchez, K.; Lee, J.; Kreisberg, J.; Ma, J.; Ideker, T. Predicting drug response and synergy using a deep learning model of human cancer cells. Cancer Cell 2020, 38, 672–684. [Google Scholar] [CrossRef]
- Tolkach, Y.; Dohmgörgen, T.; Toma, M.; Kristiansen, G. High-accuracy prostate cancer pathology using deep learning. Nat. Mach. Intell. 2020, 2, 411–418. [Google Scholar] [CrossRef]
- Campanella, G.; Hanna, M.; Geneslaw, L.; Miraflor, A.; Werneck Krauss Silva, V.; Busam, K.; Brogi, E.; Reuter, V.; Klimstra, D.; Fuchs, T. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat. Med. 2019, 25, 1301–1309. [Google Scholar] [CrossRef]
- Lu, M.; Williamson, D.; Chen, T.; Chen, R.; Barbieri, M.; Mahmood, F. Data-efficient and weakly supervised computational pathology on whole-slide images. Nat. Biomed. Eng. 2021, 5, 555–570. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Al Rasheed, M.; Xu, B. Molecular alterations in thyroid carcinoma. Surg. Pathol. Clin. 2019, 12, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.; Alexander, E.; Bible, K.; Doherty, G.; Mandel, S.; Nikiforov, Y.; Pacini, F.; Randolph, G.; Sawka, A.; Schlumberger, M.; et al. 2015 American Thyroid Association man-agement guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, L.; Liu, Y.; Cao, N.; Wang, L.; Xing, C. Clinical significance of immunohistochemistry to detect BRAF V600E mutant protein in thyroid tissues. Medicine 2021, 100, e25566. [Google Scholar] [CrossRef]
- Kim, K.; Suh, K.; Kang, D.; Kang, D. Mutations of the BRAF gene in papillary thyroid carcinoma and in Hashimoto’s thyroiditis. Pathol. Int. 2005, 55, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Akbani, R.; ÁArman Aksoy, B.; Ally, A.; Arachchi, H.; Asa, S.; ÁTodd Auman, J.; Balasundaram, M.; Balu, S.; Baylin, S.; et al. Integrated genomic characterization of papillary thyroid carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef]
- Gao, J.; Aksoy, B.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef]
- Bullock, M.; O’Neill, C.; Chou, A.; Clarkson, A.; Dodds, T.; Toon, C.; Sywak, M.; Sidhu, S.; Delbridge, L.; Robinson, B.; et al. Utilization of a MAB for BRAFV600E detection in papillary thyroid carcinoma. Endocr.-Relat. Cancer 2012, 19, 779–784. [Google Scholar] [CrossRef]
- Cabanillas, M.; Ryder, M.; Jimenez, C. Targeted therapy for advanced thyroid cancer: Kinase inhibitors and beyond. Endocr. Rev. 2019, 40, 1573–1604. [Google Scholar] [CrossRef] [PubMed]
- Hamfjord, J.; Stangeland, A.; Skrede, M.; Tveit, K.; Ikdahl, T.; Kure, E. Wobble-enhanced ARMS method for detection of KRAS and BRAF mutations. Diagn. Mol. Pathol. 2011, 20, 158–165. [Google Scholar] [CrossRef]
- Marchant, J.; Mange, A.; Larrieux, M.; Costes, V.; Solassol, J. Comparative evaluation of the new FDA approved THxID™-BRAF test with high resolution melting and sanger sequencing. BMC Cancer 2014, 14, 519. [Google Scholar] [CrossRef] [PubMed]
- Ihle, M.; Fassunke, J.; König, K.; Grünewald, I.; Schlaak, M.; Kreuzberg, N.; Tietze, L.; Schildhaus, H.; Büttner, R.; Merkelbach-Bruse, S. Comparison of high resolution melting analysis, pyrosequencing, next generation sequencing and immunohistochemistry to conventional Sanger sequencing for the detection of p. V600E and non-p. V600E BRAFmutations. BMC Cancer 2014, 14, 13. [Google Scholar] [CrossRef]
- Pichler, M.; Balic, M.; Stadelmeyer, E.; Ausch, C.; Wild, M.; Guelly, C.; Bauernhofer, T.; Samonigg, H.; Hoefler, G.; Dandachi, N. Evaluation of high-resolution melting analysis as a diagnostic tool to detect the BRAF V600E mutation in colorectal tumors. J. Mol. Diagn. 2009, 11, 140–147. [Google Scholar] [CrossRef]
- Lilleberg, S.; Durocher, J.; Sanders, C.; Walters, K.; Culver, K. High Sensitiv-ity Scanning of Colorectal Tumors and Matched Plasma DNA for Mutations in APC, TP53, K-RAS, and BRAF Genes with a Novel DHPLC Fluorescence Detection Platform. Ann. N. Y. Acad. Sci. 2004, 1022, 250–256. [Google Scholar] [CrossRef]
- Khosravi, P.; Kazemi, E.; Imielinski, M.; Elemento, O.; Hajirasouliha, I. Deep convolutional neural networks enable discrimination of heterogeneous digital pathology images. EBioMedicine 2018, 27, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kohlberger, T.; Norouzi, M.; Dahl, G.; Smith, J.; Mohtashamian, A.; Olson, N.; Peng, L.; Hipp, J.; Stumpe, M. Artificial intelligence–based breast cancer nodal metastasis detection: Insights into the black box for pathologists. Arch. Pathol. Lab. Med. 2019, 143, 859–868. [Google Scholar] [CrossRef]
- Li, S.; Jiang, H.; Pang, W. Joint multiple fully connected convolutional neural network with extreme learning machine for hepatocellular carcinoma nuclei grading. Comput. Biol. Med. 2017, 84, 156–167. [Google Scholar] [CrossRef]
- Coudray, N.; Ocampo, P.; Sakellaropoulos, T.; Narula, N.; Snuderl, M.; Fenyö, D.; Moreira, A.; Razavian, N.; Tsirigos, A. Classification and mutation prediction from non–small cell lung cancer histopathology images using deep learning. Nat. Med. 2018, 24, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Anand, D.; Yashashwi, K.; Kumar, N.; Rane, S.; Gann, P.; Sethi, A. Weakly supervised learning on unannotated H&E-stained slides predicts BRAF mutation in thyroid cancer with high accuracy. J. Pathol. 2021, 255, 232–242. [Google Scholar]
- Aboulafia, A. Biopsy. Instr. Course Lect. 1999, 48, 587–590. [Google Scholar] [PubMed]
- Bezabih, M. Cytological diagnosis of soft tissue tumours. Cytopathology 2001, 12, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Fleshman, R.; Mayerson, J.; Wakely, P., Jr. Fine-needle aspiration biopsy of high-grade sarcoma: A report of 107 cases. Cancer Cytopathol. Interdiscip. Int. J. Am. Cancer Soc. 2007, 111, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Kilpatrick, S.; Silverman, J. Fine needle aspiration biopsy of soft tissue sarcomas: Utility and diagnostic challenges. Adv. Anat. Pathol. 2004, 11, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Akerman, M.; Killander, D.; Rydholm, A.; Rooser, B. Aspiration of musculoskeletal tumors for cytodiagnosis and DNA analysis. Acta Orthop. Scand. 1987, 58, 523–528. [Google Scholar] [CrossRef]
- Amin, M.; Luqman, M.; Jamal, S.; Mamoon, N.; Anwar, M. Fine needle aspiration biopsy of soft tissue tumours. J. Coll. Physicians Surg. JCPSP 2003, 13, 625–628. [Google Scholar] [PubMed]
- Barth, R.; Merino, M.; Solomon, D.; Yang, J.; Baker, A. A prospective study of the value of core needle biopsy and fine needle aspiration in the diagnosis of soft tissue masses. Surgery 1992, 112, 536–543. [Google Scholar] [PubMed]
- Costa, M.; Campman, S.; Davis, R.; Howell, L. Fine-needle aspiration cytology of sarcoma: Retrospective review of diagnostic utility and specificity. Diagn. Cytopathol. 1996, 15, 23–32. [Google Scholar] [CrossRef]
- Dalén, B.; Meis-Kindblom, J.; Sumathi, V.; Ryd, W.; Kindblom, L. Fine-needle aspiration cytology and core needle biopsy in the preoperative diagnosis of desmoid tumors. Acta Orthop. 2006, 77, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Dey, P.; Mallik, M.; Gupta, S.; Vasishta, R. Role of fine needle aspiration cytology in the diagnosis of soft tissue tumours and tumour-like lesions. Cytopathology 2004, 15, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Klijanienko, J.; Caillaud, J.; Lagacé, R.; Vielh, P. Comparative fine-needle aspiration and pathologic study of malignant fibrous histiocytoma: Cytodiagnostic features of 95 tumors in 71 patients. Diagn. Cytopathol. 2003, 29, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Klijanienko, J.; Caillaud, J.; Lagacé, R. Fine-needle aspiration in liposar-coma: Cytohistologic correlative study including well-differentiated, myxoid, and pleomorphic variants. Diagn. Cytopathol. 2004, 30, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Chowdhury, N. Accuracy, limitations and pitfalls in the diagnosis of soft tissue tumors by fine needle aspiration cytology. Indian J. Pathol. Microbiol. 2007, 50, 42–45. [Google Scholar] [PubMed]
- Layfield, L.; Anders, K.; Glasgow, B.; Mirra, J. Fine-needle aspiration of pri-mary soft-tissue lesions. Arch. Pathol. Lab. Med. 1986, 110, 420–424. [Google Scholar] [PubMed]
- Maitra, A.; Ashfaq, R.; Saboorian, M.; Lindberg, G.; Gokaslan, S. The role of fine-needle aspiration biopsy in the primary diagnosis of mesenchymal lesions: A community hospital–based experience. Cancer Cytopathol. Interdiscip. Int. J. Am. Cancer Soc. 2000, 90, 178–185. [Google Scholar] [CrossRef]
- Miralles, T.; Gosalbez, F.; Menendez, P.; Astudillo, A.; Torre, C.; Buesa, J. Fine needle aspiration cytology of soft-tissue lesions. Acta Cytol. 1986, 30, 671–678. [Google Scholar]
- Oland, J.; Rosen, A.; Reif, R.; Sayfan, J.; Orda, R. Cytodiagnosis of soft tissue tumors. J. Surg. Oncol. 1988, 37, 168–170. [Google Scholar] [CrossRef]
- Palmer, H.; Mukunyadzi, P.; Culbreth, W.; Thomas, J. Subgrouping and grading of soft-tissue sarcomas by fine-needle aspiration cytology: A histopathologic correlation study. Diagn. Cytopathol. 2001, 24, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Sápi, Z.; Antal, I.; Pápai, Z.; Szendröi, M.; Mayer, Á.; Jakab, K.; Pajor, L.; Bodó, M. Diagnosis of soft tissue tumors by fine-needle aspiration with combined cytopathology and an-cillary techniques. Diagn. Cytopathol. 2002, 26, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Wakely, P., Jr.; Kneisl, J. Soft tissue aspiration cytopathology: Diagnostic accuracy and limitations. Cancer Cytopathol. Interdiscip. Int. J. Am. Cancer Soc. 2000, 90, 292–298. [Google Scholar] [CrossRef]
- Bhinder, B.; Gilvary, C.; Madhukar, N.; Elemento, O. Artificial intelligence in cancer research and precision medicine. Cancer Discov. 2021, 11, 900–915. [Google Scholar] [CrossRef] [PubMed]
- Kather, J.; Pearson, A.; Halama, N.; Jäger, D.; Krause, J.; Loosen, S.; Marx, A.; Boor, P.; Tacke, F.; Neumann, U.; et al. Deep learning can predict microsatellite instability directly from histology in gastrointestinal cancer. Nat. Med. 2019, 25, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Skrede, O.; De Raedt, S.; Kleppe, A.; Hveem, T.; Liestøl, K.; Maddison, J.; Askautrud, H.; Pradhan, M.; Nesheim, J.; Albregtsen, F.; et al. Deep learning for prediction of colorectal cancer outcome: A discovery and validation study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Chao, T.; Khalil, M.; Lee, Y.; Hong, D.; Wu, J.; Wang, C. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers 2021, 13, 3891. [Google Scholar] [CrossRef]
- Wang, C.; Chang, C.; Khalil, M.; Lin, Y.; Liou, Y.; Hsu, P.; Lee, Y.; Wang, C.; Chao, T. Histopathological whole slide image dataset for classification of treatment effectiveness to ovarian cancer. Sci. Data 2022, 9, 1–5. [Google Scholar] [CrossRef]
- Wang, C.; Chang, C.; Lee, Y.; Lin, Y.; Lo, S.; Hsu, P.; Liou, Y.; Wang, C.; Chao, T. Weakly supervised deep learning for prediction of treatment effectiveness on ovarian cancer from his-topathology images. Comput. Med Imaging Graph. 2022, 99, 102093. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lee, Y.; Chang, C.; Lin, Y.; Liou, Y.; Hsu, P.; Chang, C.; Sai, A.; Wang, C.; Chao, T. A Weakly Supervised Deep Learning Method for Guiding Ovarian Cancer Treatment and Identifying an Effective Biomarker. Cancers 2022, 14, 1651. [Google Scholar] [CrossRef]
- Nikiforov, Y.; Nikiforova, M. Molecular genetics and diagnosis of thy-roid cancer. Nat. Rev. Endocrinol. 2011, 7, 569–580. [Google Scholar] [CrossRef]
- Tran, K.; Kondrashova, O.; Bradley, A.; Williams, E.; Pearson, J.; Waddell, N. Deep learning in cancer diagnosis, prognosis and treatment selection. Genome Med. 2021, 13, 1–17. [Google Scholar] [CrossRef]
- Ilse, M.; Tomczak, J.; Welling, M. Attention-based deep multiple instance learning. In Proceedings of the International Conference on Machine Learning, Stockholm, Sweden, 10–15 July 2018; pp. 2127–2136. [Google Scholar]


{kind=link}
| Methods | Accuracy | Precision | Sensitivity | Specificity | Mean SS (Sens., Spec.) |
|---|---|---|---|---|---|
| NASNetLarge [22] | 0.82 | 0.82 | 1.00 | 0.00 | 0.50 |
| MIL with Resnet34 + RNN [23] | 0.77 | 0.83 | 0.90 | 0.14 | 0.52 |
| CLAM with Resnet50 [24] | 0.82 | 0.86 | 0.94 | 0.29 | 0.62 |
| Modified CLAM with Resnet101 | 0.87 | 0.94 | 0.91 | 0.71 | 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-W.; Muzakky, H.; Lee, Y.-C.; Lin, Y.-J.; Chao, T.-K. Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides. Int. J. Mol. Sci. 2023, 24, 2521. https://doi.org/10.3390/ijms24032521
Wang C-W, Muzakky H, Lee Y-C, Lin Y-J, Chao T-K. Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides. International Journal of Molecular Sciences. 2023; 24(3):2521. https://doi.org/10.3390/ijms24032521
Chicago/Turabian StyleWang, Ching-Wei, Hikam Muzakky, Yu-Ching Lee, Yi-Jia Lin, and Tai-Kuang Chao. 2023. "Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides" International Journal of Molecular Sciences 24, no. 3: 2521. https://doi.org/10.3390/ijms24032521
APA StyleWang, C.-W., Muzakky, H., Lee, Y.-C., Lin, Y.-J., & Chao, T.-K. (2023). Annotation-Free Deep Learning-Based Prediction of Thyroid Molecular Cancer Biomarker BRAF (V600E) from Cytological Slides. International Journal of Molecular Sciences, 24(3), 2521. https://doi.org/10.3390/ijms24032521