

Controversies Surrounding Albumin Use in Sepsis: Lessons from Cirrhosis


Abstract
1. Introduction
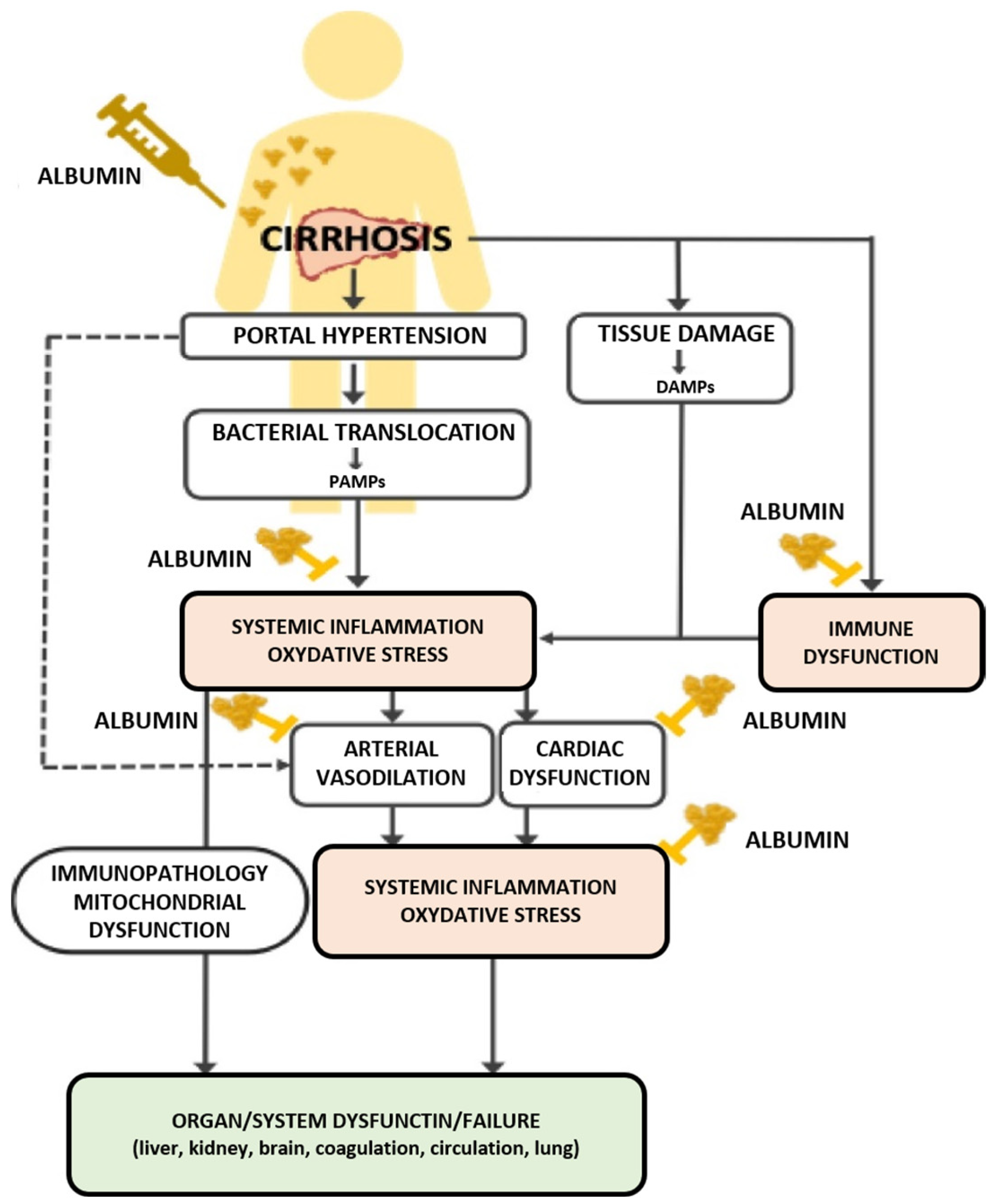
2. Interplay between Liver Function and Gut Microbiota in Sepsis and Cirrhosis
3. Use of Albumin in Cirrhosis
3.1. Effectiveness of Albumin Therapy in Various Cirrhosis Complications
3.2. Circumstances Where Albumin Therapy in Cirrhosis Shows Limited Effectiveness
3.3. Insights from Albumin Therapy in Cirrhosis for Sepsis Management
3.3.1. Inconsistent Effectiveness of Albumin Therapy in Diverse Cirrhosis Scenarios
3.3.2. Organ Dysfunction Conditions Demanding Volume Expansion
3.3.3. Disease Severity and Hypoalbuminemia
3.3.4. Dose and Duration of Albumin Administration
3.3.5. Safety of Albumin Infusion
3.4. Summary of Insights and Implications of Albumin Therapy in Cirrhosis Management
4. Use of Albumin in Sepsis
4.1. Clinical Trials and Evidence
4.1.1. Randomized Controlled Trials of Albumin in Sepsis-Induced Hypotension
4.1.2. Meta-Analyses of Albumin in Sepsis
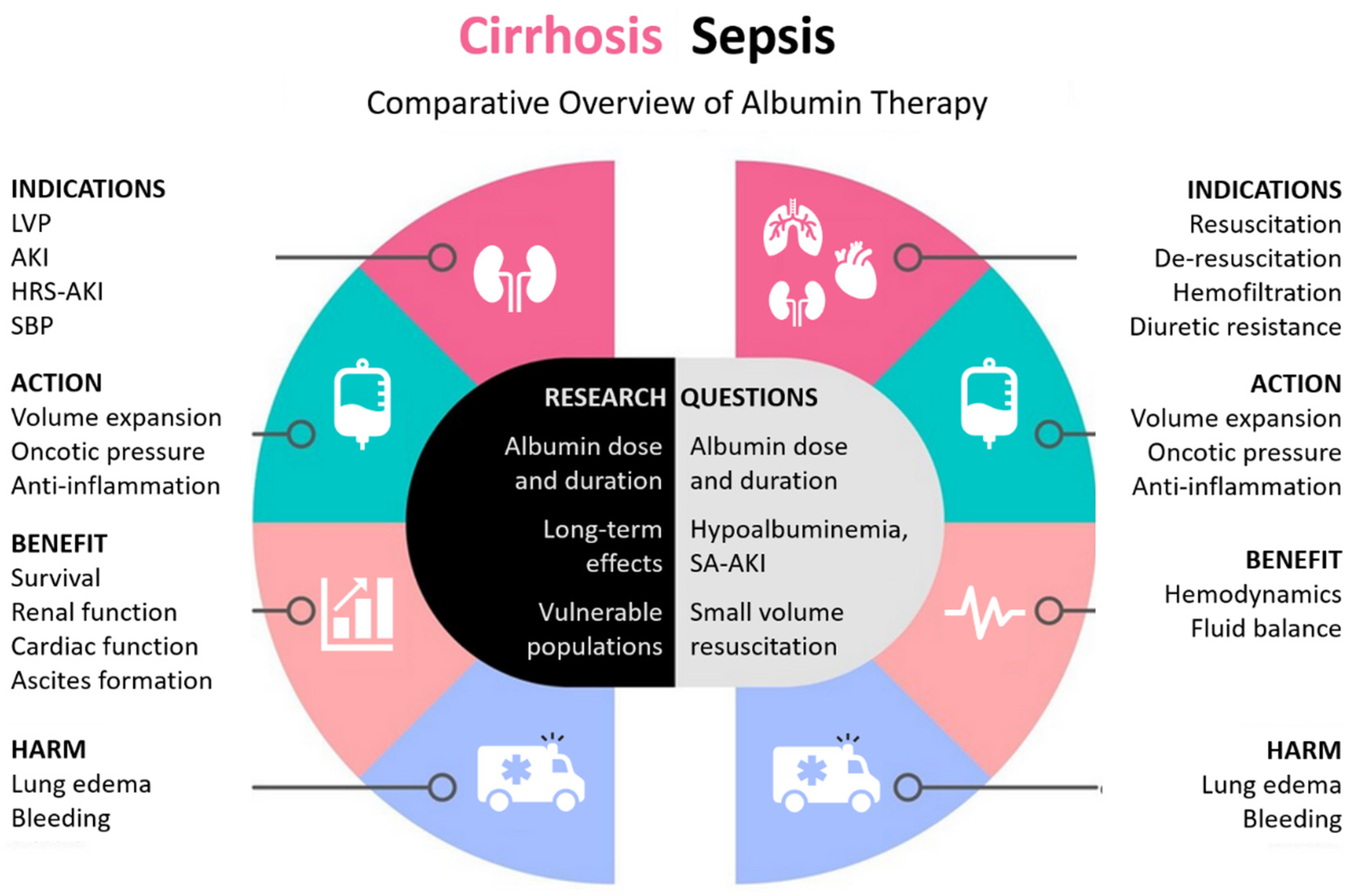
5. Comparative Analysis
5.1. Inconsistent Effectiveness
5.2. Organ Dysfunction and Volume Expansion
5.3. Disease Severity and Hypoalbuminemia
5.4. Dose and Duration of Administration
5.5. Safety
6. Clinical Implications and Future Directions
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peters, T., Jr. All about Albumin: Biochemistry, Genetics, and Medical Applications; Academic Press: Cambridge, MA, USA, 1995; ISBN 0-08-052704-3. [Google Scholar]
- Belinskaia, D.A.; Voronina, P.A.; Shmurak, V.I.; Jenkins, R.O.; Goncharov, N.V. Serum Albumin in Health and Disease: Esterase, Antioxidant, Transporting and Signaling Properties. Int. J. Mol. Sci. 2021, 22, 10318. [Google Scholar] [CrossRef] [PubMed]
- De Simone, G.; di Masi, A.; Ascenzi, P. Serum Albumin: A Multifaced Enzyme. Int. J. Mol. Sci. 2021, 22, 10086. [Google Scholar] [CrossRef] [PubMed]
- Kragh-Hansen, U. Human Serum Albumin: A Multifunctional Protein. In Albumin in Medicine: Pathological and Clinical Applications; Springer: Singapore, 2016; pp. 1–24. [Google Scholar]
- Pompili, E.; Zaccherini, G.; Baldassarre, M.; Iannone, G.; Caraceni, P. Albumin Administration in Internal Medicine: A Journey between Effectiveness and Futility. Eur. J. Intern. Med. 2023, 117, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, C.J. Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years. J. Clin. Med. 2023, 12, 5919. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.; Legrand, M. Epidemiology of Sepsis and Septic Shock. Curr. Opin. Anesthesiol. 2021, 34, 71. [Google Scholar] [CrossRef]
- Bauer, M.; Coldewey, S.M.; Leitner, M.; Löffler, B.; Weis, S.; Wetzker, R. Deterioration of Organ Function As a Hallmark in Sepsis: The Cellular Perspective. Front. Immunol. 2018, 9, 1460. [Google Scholar] [CrossRef]
- Rubio, I.; Osuchowski, M.F.; Shankar-Hari, M.; Skirecki, T.; Winkler, M.S.; Lachmann, G.; La Rosée, P.; Monneret, G.; Venet, F.; Bauer, M.; et al. Current Gaps in Sepsis Immunology: New Opportunities for Translational Research. Lancet Infect. Dis. 2019, 19, e422–e436. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Geng, L.; Tian, X.; Gao, Z.; Mao, A.; Feng, L.; He, C. Different Concentrations of Albumin Versus Crystalloid in Patients with Sepsis and Septic Shock: A Meta-Analysis of Randomized Clinical Trials. J. Intensive Care Med. 2023, 38, 679–689. [Google Scholar] [CrossRef]
- Zou, Y.; Ma, K.; Xiong, J.B.; Xi, C.H.; Deng, X.J. Comparison of the Effects of Albumin and Crystalloid on Mortality among Patients with Septic Shock: Systematic Review with Meta-Analysis and Trial Sequential Analysis. Sao Paulo Med. J. 2018, 136, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.; Perna, B.; Cesaro, A.E.; Maritati, M.; Spampinato, M.D.; Contini, C.; De Giorgio, R. 2023 Update on Sepsis and Septic Shock in Adult Patients: Management in the Emergency Department. J. Clin. Med. 2023, 12, 3188. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence Intravenous Fluid Therapy in Adults in Hospital. Available online: https://www.nice.org.uk/guidance/cg174/chapter/Recommendations#resuscitation-2 (accessed on 4 November 2023).
- Bai, Z.; Méndez-Sánchez, N.; Romeiro, F.G.; Mancuso, A.; Philips, C.A.; Tacke, F.; Basaranoglu, M.; Primignani, M.; Ibrahim, M.; Wong, Y.J.; et al. Use of Albumin Infusion for Cirrhosis-Related Complications: An International Position Statement. JHEP Rep. 2023, 5, 100785. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.D.; Martin, R.H.; Palesch, Y.Y.; Moy, C.S.; Tamariz, D.; Ryckborst, K.J.; Jones, E.B.; Weisman, D.; Pettigrew, C.; Ginsberg, M.D. Albumin Administration in Acute Ischemic Stroke: Safety Analysis of the ALIAS Part 2 Multicenter Trial. PLoS ONE 2015, 10, e0131390. [Google Scholar] [CrossRef] [PubMed]
- Arfaras-Melainis, A.; Polyzogopoulou, E.; Triposkiadis, F.; Xanthopoulos, A.; Ikonomidis, I.; Mebazaa, A.; Parissis, J. Heart Failure and Sepsis: Practical Recommendations for the Optimal Management. Heart Fail. Rev. 2020, 25, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Talvasto, A.; Ilmakunnas, M.; Raivio, P.; Vlasov, H.; Hiippala, S.; Suojaranta, R.; Wilkman, E.; Petäjä, L.; Helve, O.; Juvonen, T.; et al. Albumin Infusion and Blood Loss after Cardiac Surgery. Ann. Thorac. Surg. 2023, 116, 392–399. [Google Scholar] [CrossRef] [PubMed]
- China, L.; Freemantle, N.; Forrest, E.; Kallis, Y.; Ryder, S.D.; Wright, G.; Portal, A.J.; Salles, N.B.; Gilroy, D.W.; O’Brien, A. A Randomized Trial of Albumin Infusions in Hospitalized Patients with Cirrhosis. N. Engl. J. Med. 2021, 384, 808–817. [Google Scholar] [CrossRef]
- Tilg, H.; Adolph, T.E.; Trauner, M. Gut-Liver Axis: Pathophysiological Concepts and Clinical Implications. Cell Metab. 2022, 34, 1700–1718. [Google Scholar] [CrossRef]
- Beyer, D.; Hoff, J.; Sommerfeld, O.; Zipprich, A.; Gaßler, N.; Press, A.T. The Liver in Sepsis: Molecular Mechanism of Liver Failure and Their Potential for Clinical Translation. Mol. Med. 2022, 28, 84. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, H.; Hashimoto, K.; Yuan, S.; Zhang, J. The Gut-Liver Axis in Sepsis: Interaction Mechanisms and Therapeutic Potential. Crit. Care 2022, 26, 213. [Google Scholar] [CrossRef]
- Alexander, J.W.; Ogle, C.K.; Stinnett, J.D.; Macmillan, B.G. A Sequential, Prospective Analysis of Immunologic Abnormalities and Infection Following Severe Thermal Injury. Ann. Surg. 1978, 188, 809–816. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, R.; Murdoch, J.; Kuehn, R.; Marshall, J.C. The Effect of Albumin or Crystalloid Resuscitation on Bacterial Translocation and Endotoxin Absorption Following Experimental Burn Injury. J. Surg. Res. 1992, 52, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Durand, F.; Kellum, J.A.; Nadim, M.K. Fluid Resuscitation in Patients with Cirrhosis and Sepsis: A Multidisciplinary Perspective. J. Hepatol. 2023, 79, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Moreau, R.; Jalan, R. Acute-on-Chronic Liver Failure. N. Engl. J. Med. 2020, 382, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Claudel, S.E.; Jaganathan, J.; Patel, A.; Tapper, E.B.; Verma, A. Review Article: Practical Considerations for Fluid Resuscitation in Cirrhosis. Aliment. Pharmacol. Ther. 2023, 57, 1066–1082. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.N.; Moraes, A.G.d.; Simonetto, D.A. Cirrhosis Management in the Intensive Care Unit. Semin. Liver Dis. 2023, 43, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martinez, R.; Caraceni, P.; Bernardi, M.; Gines, P.; Arroyo, V.; Jalan, R. Albumin: Pathophysiologic Basis of Its Role in the Treatment of Cirrhosis and Its Complications. Hepatology 2013, 58, 1836–1846. [Google Scholar] [CrossRef]
- Caraceni, P.; Abraldes, J.G.; Ginès, P.; Newsome, P.N.; Sarin, S.K. The Search for Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing to Drug Discovery. J. Hepatol. 2021, 75, S118–S134. [Google Scholar] [CrossRef]
- Bernardi, M.; Angeli, P.; Claria, J.; Moreau, R.; Gines, P.; Jalan, R.; Caraceni, P.; Fernandez, J.; Gerbes, A.L.; O’Brien, A.J.; et al. Albumin in Decompensated Cirrhosis: New Concepts and Perspectives. Gut 2020, 69, 1127–1138. [Google Scholar] [CrossRef]
- Zheng, X.; Bai, Z.; Wang, T.; Romeiro, F.G.; Mancuso, A.; Philips, C.A.; Wong, Y.J.; Nery, F.G.; Qi, X. Human Albumin Infusion for the Management of Liver Cirrhosis and Its Complications: An Overview of Major Findings from Meta-Analyses. Adv. Ther. 2023, 40, 1494–1529. [Google Scholar] [CrossRef]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-Term Albumin Administration in Decompensated Cirrhosis (ANSWER): An Open-Label Randomised Trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef] [PubMed]
- Solà, E.; Solé, C.; Simón-Talero, M.; Martín-Llahí, M.; Castellote, J.; Garcia-Martínez, R.; Moreira, R.; Torrens, M.; Márquez, F.; Fabrellas, N.; et al. Midodrine and Albumin for Prevention of Complications in Patients with Cirrhosis Awaiting Liver Transplantation. A Randomized Placebo-Controlled Trial. J. Hepatol. 2018, 69, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Tsukamoto, M.M.; Mathur, A.K.; Ghomri, Y.M.; Hou, L.A.; Sheibani, S.; Runyon, B.A. Delayed Paracentesis Is Associated with Increased In-Hospital Mortality in Patients with Spontaneous Bacterial Peritonitis. Off. J. Am. Coll. Gastroenterol. ACG 2014, 109, 1436. [Google Scholar] [CrossRef] [PubMed]
- Rimola, A.; García-Tsao, G.; Navasa, M.; Piddock, L.J.V.; Planas, R.; Bernard, B.; Inadomi, J.M. Diagnosis, Treatment and Prophylaxis of Spontaneous Bacterial Peritonitis: A Consensus Document. J. Hepatol. 2000, 32, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Sort, P.; Navasa, M.; Arroyo, V.; Aldeguer, X.; Planas, R.; Ruiz-del-Arbol, L.; Castells, L.; Vargas, V.; Soriano, G.; Guevara, M.; et al. Effect of Intravenous Albumin on Renal Impairment and Mortality in Patients with Cirrhosis and Spontaneous Bacterial Peritonitis. N. Engl. J. Med. 1999, 341, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Allegretti, A.S.; Subramanian, R.M.; Francoz, C.; Olson, J.C.; Cárdenas, A. Respiratory Events with Terlipressin and Albumin in Hepatorenal Syndrome: A Review and Clinical Guidance. Liver Int. 2022, 42, 2124–2130. [Google Scholar] [CrossRef]
- Arora, V.; Vijayaraghavan, R.; Maiwall, R.; Sahney, A.; Thomas, S.S.; Ali, R.; Jain, P.; Kumar, G.; Sarin, S.K. Paracentesis-Induced Circulatory Dysfunction with Modest-Volume Paracentesis Is Partly Ameliorated by Albumin Infusion in Acute-on-Chronic Liver Failure. Hepatology 2020, 72, 1043–1055. [Google Scholar] [CrossRef]
- Child, C.G.; Turcotte, J.G. Surgery and Portal Hypertension. Major. Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients with Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Lammers, W.J.; Hirschfield, G.M.; Corpechot, C.; Nevens, F.; Lindor, K.D.; Janssen, H.L.A.; Floreani, A.; Ponsioen, C.Y.; Mayo, M.J.; Invernizzi, P.; et al. Development and Validation of a Scoring System to Predict Outcomes of Patients with Primary Biliary Cirrhosis Receiving Ursodeoxycholic Acid Therapy. Gastroenterology 2015, 149, 1804–1812.e4. [Google Scholar] [CrossRef]
- Biggins, S.W.; Angeli, P.; Garcia-Tsao, G.; Ginès, P.; Ling, S.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, Evaluation, and Management of Ascites and Hepatorenal Syndrome. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef] [PubMed]
- Thévenot, T.; Bureau, C.; Oberti, F.; Anty, R.; Louvet, A.; Plessier, A.; Rudler, M.; Heurgué-Berlot, A.; Rosa, I.; Talbodec, N.; et al. Effect of Albumin in Cirrhotic Patients with Infection Other than Spontaneous Bacterial Peritonitis. A Randomized Trial. J. Hepatol. 2015, 62, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Guevara, M.; Terra, C.; Nazar, A.; Sola, E.; Fernandez, J.; Pavesi, M.; Arroyo, V.; Gines, P. Albumin for Bacterial Infections Other than Spontaneous Bacterial Peritonitis in Cirrhosis. A Randomized, Controlled Study. J. Hepatol. 2012, 57, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Claria, J.; Amoros, A.; Aguilar, F.; Castro, M.; Casulleras, M.; Acevedo, J.; Duran-Guell, M.; Nunez, L.; Costa, M.; et al. Effects of Albumin Treatment on Systemic and Portal Hemodynamics and Systemic Inflammation in Patients with Decompensated Cirrhosis. Gastroenterology 2019, 157, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Tufoni, M.; Zaccherini, G.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; et al. On-Treatment Serum Albumin Level Can Guide Long-Term Treatment in Patients with Cirrhosis and Uncomplicated Ascites. J. Hepatol. 2021, 74, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.; Pappas, S.C.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N. Engl. J. Med. 2021, 384, 818–828. [Google Scholar] [CrossRef]
- Edwards, J.D. Management of Septic Shock. BMJ 1993, 306, 1661–1664. [Google Scholar] [CrossRef]
- Dyson, A.; Cone, S.; Singer, M.; Ackland, G.L. Microvascular and Macrovascular Flow Are Uncoupled in Early Polymicrobial Sepsis. Br. J. Anaesth. 2012, 108, 973–978. [Google Scholar] [CrossRef][Green Version]
- Chappell, D.; Bruegger, D.; Potzel, J.; Jacob, M.; Brettner, F.; Vogeser, M.; Conzen, P.; Becker, B.F.; Rehm, M. Hypervolemia Increases Release of Atrial Natriuretic Peptide and Shedding of the Endothelial Glycocalyx. Crit. Care 2014, 18, 538. [Google Scholar] [CrossRef]
- Perner, A.; Cecconi, M.; Cronhjort, M.; Darmon, M.; Jakob, S.M.; Pettila, V.; van der Horst, I.C.C. Expert Statement for the Management of Hypovolemia in Sepsis. Intensive Care Med. 2018, 44, 791–798. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Via, L.; Dezio, V.; Amelio, P.; Genoese, G.; Franchi, F.; Messina, A.; Robba, C.; Noto, A. Inferior vena cava distensibility from subcostal and trans- hepatic imaging using both M-mode or artificial intelligence: A prospective study on mechanically ventilated patients. Intensive Care Med. Exp. 2023, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro, N.I.; Douglas, I.S.; Brower, R.G.; Brown, S.M.; Exline, M.C.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Hayden, D.; et al. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N. Engl. J. Med. 2023, 388, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Radecki, R.P.; Spiegel, R. Usual Care, Unusual Care, and the Lessons from CLOVERS: April 2023 Annals of Emergency Medicine Journal Club. Ann. Emerg. Med. 2023, 81, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Andrews, B.; Semler, M.W.; Muchemwa, L.; Kelly, P.; Lakhi, S.; Heimburger, D.C.; Mabula, C.; Bwalya, M.; Bernard, G.R. Effect of an Early Resuscitation Protocol on In-Hospital Mortality Among Adults with Sepsis and Hypotension: A Randomized Clinical Trial. JAMA 2017, 318, 1233–1240. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Phases of Fluid Management and the Roles of Human Albumin Solution in Perioperative and Critically Ill Patients. Curr. Med. Res. Opin. 2020, 36, 1961–1973. [Google Scholar] [CrossRef]
- Bakker, J.; Kattan, E.; Annane, D.; Castro, R.; Cecconi, M.; De Backer, D.; Dubin, A.; Evans, L.; Gong, M.N.; Hamzaoui, O.; et al. Current Practice and Evolving Concepts in Septic Shock Resuscitation. Intensive Care Med. 2022, 48, 148–163. [Google Scholar] [CrossRef]
- Perez Nieto, O.R.; Wong, A.; Lopez Fermin, J.; Zamarron Lopez, E.I.; Meade Aguilar, J.A.; Deloya Tomas, E.; Carrion Moya, J.D.; Castillo Gutierrez, G.; Olvera Ramos, M.G.; García Montes, X.; et al. Aiming for Zero Fluid Accumulation: First, Do No Harm. Anaesthesiol. Intensive Ther. 2021, 53, 162–178. [Google Scholar] [CrossRef]
- Joannidis, M.; Wiedermann, C.J.; Ostermann, M. Ten Myths about Albumin. Intensive Care Med. 2022, 48, 602–605. [Google Scholar] [CrossRef]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R.; Safe Study Investigators. A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [CrossRef]
- Safe Study Investigators; Finfer, S.; McEvoy, S.; Bellomo, R.; McArthur, C.; Myburgh, J.; Norton, R. Impact of Albumin Compared to Saline on Organ Function and Mortality of Patients with Severe Sepsis. Intensive Care Med. 2011, 37, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, J.; Mira, J.P. Efficacy and Tolerance of Hyperoncotic Albumin Administration in Septic Shock Patients: The EARSS Study. Intensive Care Med. 2011, 37, S115. [Google Scholar]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin Replacement in Patients with Severe Sepsis or Septic Shock. N. Engl. J. Med. 2014, 370, 1412–1421. [Google Scholar] [CrossRef] [PubMed]
- Vasques, F.; Duscio, E.; Romitti, F.; Pasticci, I.; Caironi, P.; Meessen, J.; Latini, R.; Cressoni, M.; Camporota, L.; Pesenti, A.; et al. Septic Shock-3 vs 2: An Analysis of the ALBIOS Study. Crit. Care 2018, 22, 237. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.L.; de Almeida, J.P.; de Oliveira, G.Q.; Rizk, S.I.; Fukushima, J.T.; Nakamura, R.E.; Mourão, M.M.; Galas, F.R.B.G.; Abdala, E.; Pinheiro Freire, M.; et al. Lactated Ringer’s Versus 4% Albumin on Lactated Ringer’s in Early Sepsis Therapy in Cancer Patients: A Pilot Single-Center Randomized Trial. Crit. Care Med. 2019, 47, e798–e805. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A.; Maiwall, R.; Sharma, M.K.; Jindal, A.; Choudhury, A.K.; Kumar, G.; Bhardwaj, A.; Mitra, L.G.; Agarwal, P.M.; Sarin, S.K. Comparison of 5% Human Albumin and Normal Saline for Fluid Resuscitation in Sepsis Induced Hypotension among Patients with Cirrhosis (FRISC Study): A Randomized Controlled Trial. Hepatol. Int. 2021, 15, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Maiwall, R.; Kumar, A.; Pasupuleti, S.S.R.; Hidam, A.K.; Tevethia, H.; Kumar, G.; Sahney, A.; Mitra, L.G.; Sarin, S.K. A Randomized-Controlled Trial Comparing 20% Albumin to Plasmalyte in Patients with Cirrhosis and Sepsis-Induced Hypotension [ALPS Trial]. J. Hepatol. 2022, 77, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, C.J.; Joannidis, M. Albumin Replacement in Severe Sepsis or Septic Shock. N. Engl. J. Med. 2014, 371, 83. [Google Scholar] [CrossRef]
- Delaney, A.P.; Dan, A.; McCaffrey, J.; Finfer, S. The Role of Albumin as a Resuscitation Fluid for Patients with Sepsis: A Systematic Review and Meta-Analysis. Crit. Care Med. 2011, 39, 386–391. [Google Scholar] [CrossRef]
- Haase, N.; Perner, A.; Hennings, L.I.; Siegemund, M.; Lauridsen, B.; Wetterslev, M.; Wetterslev, J. Hydroxyethyl Starch 130/0.38-0.45 versus Crystalloid or Albumin in Patients with Sepsis: Systematic Review with Meta-Analysis and Trial Sequential Analysis. BMJ 2013, 346, f839. [Google Scholar] [CrossRef]
- Lewis, S.R.; Pritchard, M.W.; Evans, D.J.; Butler, A.R.; Alderson, P.; Smith, A.F.; Roberts, I. Colloids versus Crystalloids for Fluid Resuscitation in Critically Ill People. Cochrane Database Syst. Rev. 2018, 8, CD000567. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.S.; Bassett, P. Crystalloids vs. Colloids for Fluid Resuscitation in the Intensive Care Unit: A Systematic Review and Meta-Analysis. J. Crit. Care 2019, 50, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Alhazzani, W.; Gibson, A.; Ribic, C.M.; Sindi, A.; Heels-Ansdell, D.; Thabane, L.; Fox-Robichaud, A.; Mbuagbaw, L.; Szczeklik, W.; et al. Fluid Type and the Use of Renal Replacement Therapy in Sepsis: A Systematic Review and Network Meta-Analysis. Intensive Care Med. 2015, 41, 1561–1571. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Laffan, M.A.; Waheed, U.; Brett, S.J. Randomised Trials of Human Albumin for Adults with Sepsis: Systematic Review and Meta-Analysis with Trial Sequential Analysis of All-Cause Mortality. BMJ 2014, 349, g4561. [Google Scholar] [CrossRef] [PubMed]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis—Pathophysiology and Therapeutic Concepts. Front. Med. 2021, 8, 628302. [Google Scholar] [CrossRef]
- Doyle, J.F.; Forni, L.G. Update on Sepsis-Associated Acute Kidney Injury: Emerging Targeted Therapies. Biol. Targets Ther. 2016, 10, 149–156. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wiedermann, C.J. Hypoalbuminemia and the Risk of Acute Kidney Injury in Sepsis. Crit. Care Med. 2019, 47, e377–e378. [Google Scholar] [CrossRef]
- Zarbock, A.; Nadim, M.K.; Pickkers, P.; Gomez, H.; Bell, S.; Joannidis, M.; Kashani, K.; Koyner, J.L.; Pannu, N.; Meersch, M.; et al. Sepsis-Associated Acute Kidney Injury: Consensus Report of the 28th Acute Disease Quality Initiative Workgroup. Nat. Rev. Nephrol. 2023, 19, 401–417. [Google Scholar] [CrossRef]
- Wiedermann, C.J.; Wiedermann, W.; Joannidis, M. Hypoalbuminemia and Acute Kidney Injury: A Meta-Analysis of Observational Clinical Studies. Intensive Care Med. 2010, 36, 1657–1665. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Moderator Effect of Hypoalbuminemia in Volume Resuscitation and Plasma Expansion with Intravenous Albumin Solution. Int. J. Mol. Sci. 2022, 23, 14175. [Google Scholar] [CrossRef]
- Yoon, S.H.; Choi, B.; Eun, S.; Bae, G.E.; Koo, C.M.; Kim, M.K. Using the Lactate-to-Albumin Ratio to Predict Mortality in Patients with Sepsis or Septic Shock: A Systematic Review and Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-M.; Jo, Y.H.; Lee, J.H.; Hwang, J.E.; Park, I.; Baek, S.; Jeong, H.; Um, Y.W.; Kim, H.E. Associations of the Serum Albumin Concentration and Sequential Organ Failure Assessment Score at Discharge with 1-Year Mortality in Sepsis Survivors: A Retrospective Cohort Study. Shock Inj. Inflamm. Sepsis Lab. Clin. Approaches 2023, 59, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martinez, R.; Andreola, F.; Mehta, G.; Poulton, K.; Oria, M.; Jover, M.; Soeda, J.; Macnaughtan, J.; Chiara, F.D.; Habtesion, A.; et al. Immunomodulatory and Antioxidant Function of Albumin Stabilises the Endothelium and Improves Survival in a Rodent Model of Chronic Liver Failure. J. Hepatol. 2015, 62, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Safe Study Investigators; Finfer, S.; Bellomo, R.; McEvoy, S.; Lo, S.K.; Myburgh, J.; Neal, B.; Norton, R. Effect of Baseline Serum Albumin Concentration on Outcome of Resuscitation with Albumin or Saline in Patients in Intensive Care Units: Analysis of Data from the Saline versus Albumin Fluid Evaluation (SAFE) Study. BMJ 2006, 333, 1044. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M. Effective Albumin—A Novel Paradigm in the Management of Decompensated Liver Cirrhosis. J. Transl. Intern. Med. 2023, 11, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Maimone, S.; Tripodi, V.F.; Mazzeo, A.T. Response to: A Randomized-Controlled Trial Comparing 20% Albumin to Plasmalyte in Patients with Cirrhosis and Sepsis-Induced Hypotension [ALPS Trial]. J. Hepatol. 2022, 77, 1731–1732. [Google Scholar] [CrossRef]
- Jonsson, A.B.; Rygård, S.L.; Hildebrandt, T.; Perner, A.; Møller, M.H.; Russell, L. Thrombocytopenia in Intensive Care Unit Patients: A Scoping Review. Acta Anaesthesiol. Scand. 2021, 65, 2–14. [Google Scholar] [CrossRef]
- Pathirana, S.; Wong, G.; Williams, P.; Yang, K.; Kershaw, G.; Dunkley, S.; Kam, P.C.A. The Effects of Haemodilution with Albumin on Coagulation in Vitro as Assessed by Rotational Thromboelastometry. Anaesth. Intensive Care 2015, 43, 187–192. [Google Scholar] [CrossRef]
- Pesonen, E.; Vlasov, H.; Suojaranta, R.; Hiippala, S.; Schramko, A.; Wilkman, E.; Eränen, T.; Arvonen, K.; Mazanikov, M.; Salminen, U.-S.; et al. Effect of 4% Albumin Solution vs. Ringer Acetate on Major Adverse Events in Patients Undergoing Cardiac Surgery with Ccrdiopulmonary Bypass: A Randomized Clinical Trial. JAMA 2022, 328, 251–258. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Lessons | Key Insights |
|---|---|
| Inconsistent Effectiveness | Varies by cirrhosis scenario |
| Less pronounced in LVP, non-SBP infections, and overt HE | |
| Short-term use aligns with colloid properties of albumin | |
| Organ Dysfunction and Volume Expansion | Highly effective in decompensated cirrhosis requiring volume expansion |
| Beneficial for SBP and HRS-AKI, reducing renal failure and mortality | |
| Disease Severity and Hypoalbuminemia | Serum albumin levels inform prognostic scoring |
| Disease severity influences albumin dose needs | |
| Short-term use mainly effective in SBP or HRS-AKI | |
| Dose and Duration of Administration | Higher doses/longer durations improve outcomes |
| Reduced mortality and inflammation with long-term use | |
| Safety | Requires careful dosing to prevent complications |
| Risks include pulmonary edema and bleeding in vulnerable patients |
| Study | Year | Patient Population | Intervention | Control | Dose and Duration of Albumin | Primary Endpoint | Outcomes |
|---|---|---|---|---|---|---|---|
| SAFE [63,64] | 2004 | Critically ill | 4% Albumin | 0.9% Saline | All fluid resuscitation in ICU until death, discharge, or for up to 28 days; volumes reducing over time (2247 mL on days 1 to 4) | Mortality, Organ Failure, ICU Stay | Similar outcomes at 28 days; post hoc reduced 28-day mortality and reduced vasopressor use in sepsis subgroup |
| EARSS [65] | 2011 | Septic shock | 20% Albumin | 0.9% Saline | 100 mL every 8 h for 3 days | 28-Day Survival | No significant mortality difference |
| ALBIOS [66,67] | 2014 | Severe sepsis or septic shock | 20% Albumin | Crystalloids | Administered 300 mL after randomization, from day 1 until day 28 or ICU discharge titration of albumin serum levels to 3 g/dL | 90-Day Survival | Improved MAP and reduced heart rate; shorter time to cessation of vasopressor or inotropic agents; no difference in new organ failures; no difference in mortality; post hoc reduced 90-day mortality in septic shock subgroup |
| RASP [68] | 2019 | Septic cancer patients in ICU | 4% Albumin | Lactated Ringer’s | Mean volume of 2402 mL during initial 6 h | Mortality at day 7 and day 28 | No significant improvement in mortality rates |
| FRISC [69] | 2021 | Cirrhotic patients with sepsis-induced hypotension | 5% Albumin | 0.9% Saline | Administered 250 mL over 15–30 min followed by 50 mL/h for 3 h | Hypotension reversal at 1 and 3 h, survival at one week | Higher rate of hypotension reversal, sustained reductions in heart rate and hyperlactatemia, higher proportion of surviving patients at one week |
| ALPS [70] | 2022 | Cirrhotic patients with sepsis-induced hypotension | 20% Albumin | Plasmalyte | Administered 0.5–1.0 g/kg over a period of 3 h | MAP > 65 mmHg at 3 h | Albumin more effective, faster decline in lactate, reduced need for dialysis, longer time to dialysis initiation, similar 28-day mortality, associated with pulmonary complications |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiedermann, C.J. Controversies Surrounding Albumin Use in Sepsis: Lessons from Cirrhosis. Int. J. Mol. Sci. 2023, 24, 17606. https://doi.org/10.3390/ijms242417606
Wiedermann CJ. Controversies Surrounding Albumin Use in Sepsis: Lessons from Cirrhosis. International Journal of Molecular Sciences. 2023; 24(24):17606. https://doi.org/10.3390/ijms242417606
Chicago/Turabian StyleWiedermann, Christian J. 2023. "Controversies Surrounding Albumin Use in Sepsis: Lessons from Cirrhosis" International Journal of Molecular Sciences 24, no. 24: 17606. https://doi.org/10.3390/ijms242417606
APA StyleWiedermann, C. J. (2023). Controversies Surrounding Albumin Use in Sepsis: Lessons from Cirrhosis. International Journal of Molecular Sciences, 24(24), 17606. https://doi.org/10.3390/ijms242417606