
Comparative Analysis of Morphological and Functional Effects of 225Ac- and 177Lu-PSMA Radioligand Therapies (RLTs) on Salivary Glands
 ,
,  ,
,
Abstract
:1. Introduction
2. Results
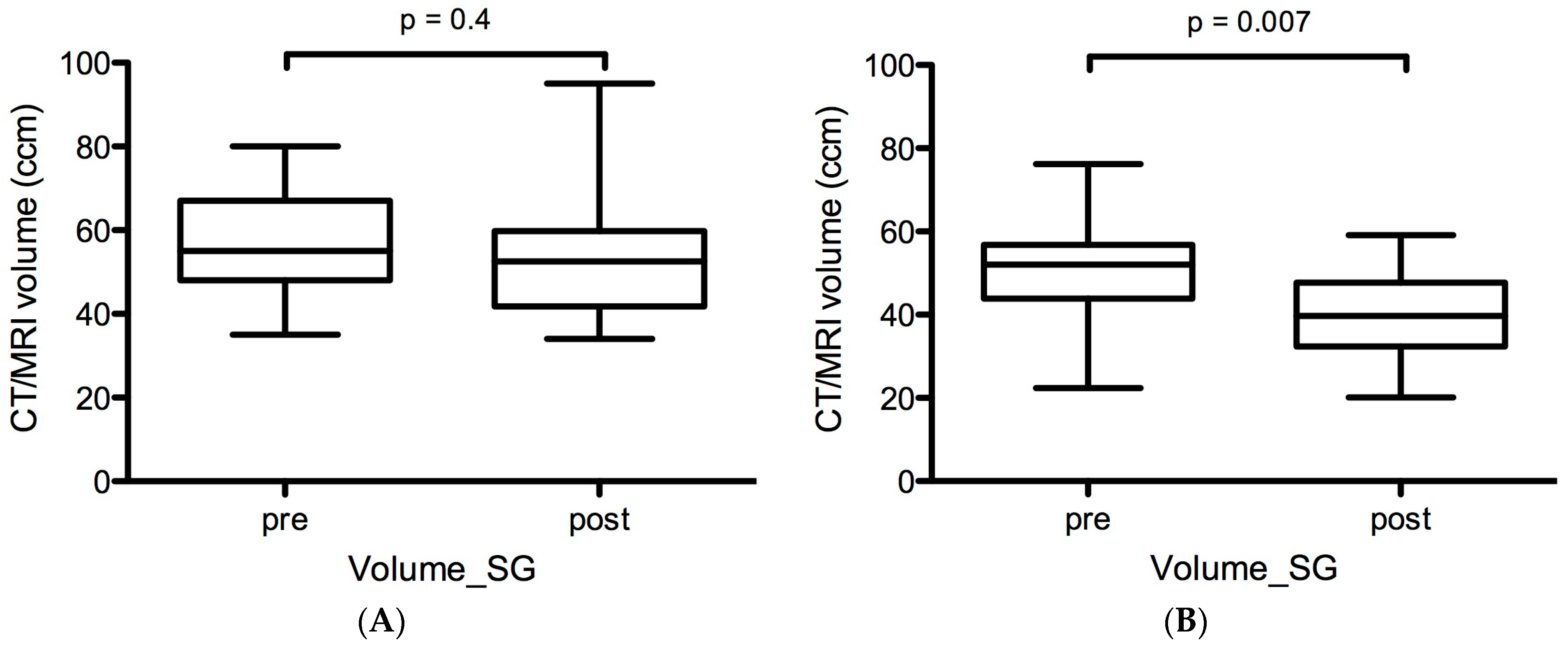
2.1. Volumetric Changes in Salivary Glands before and after LuPSMA and AcPSMA RLTs
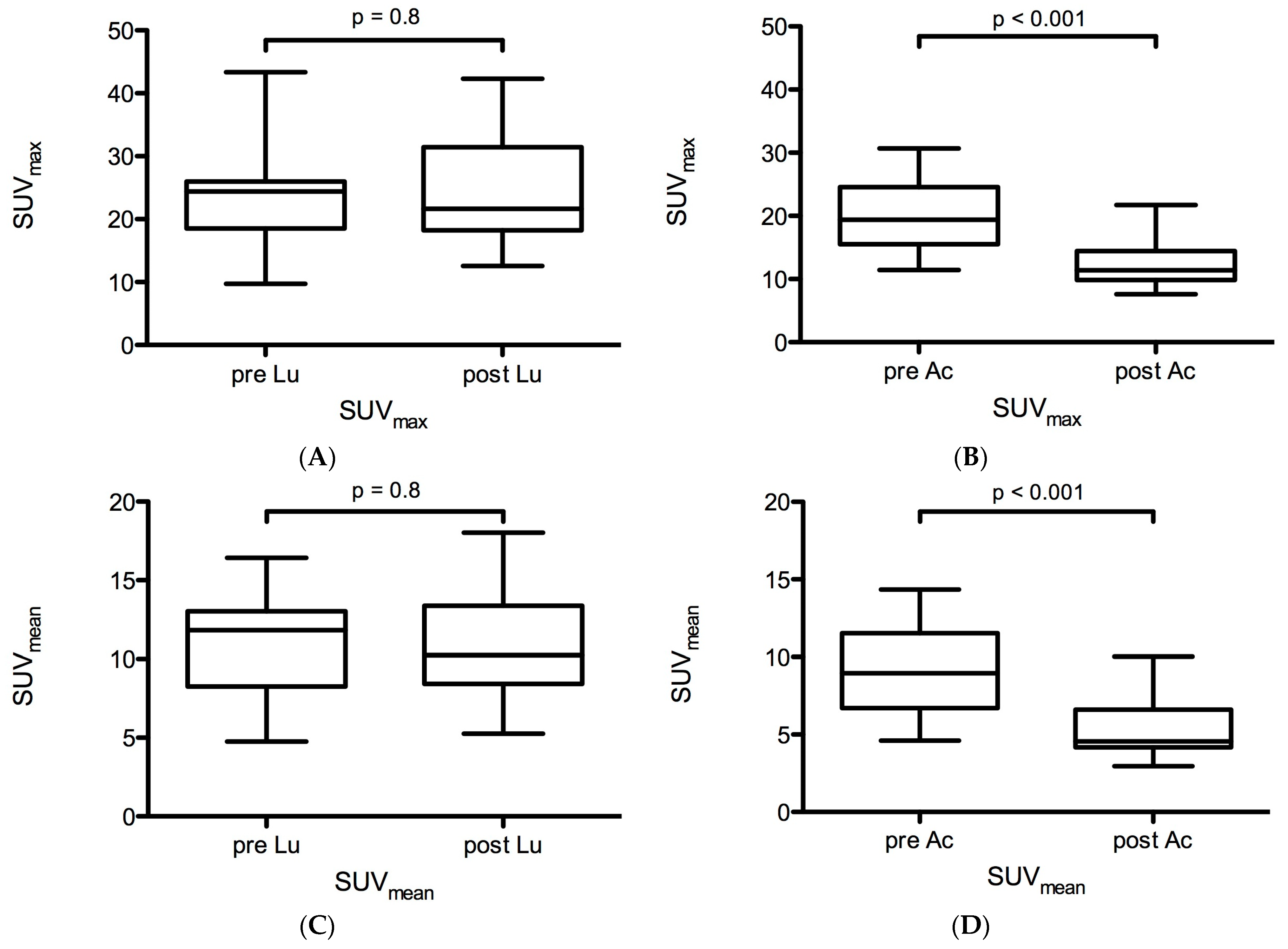
2.2. Functional Changes in PSMA-Ligand Uptake before and after LuPSMA and AcPSMA RLTs
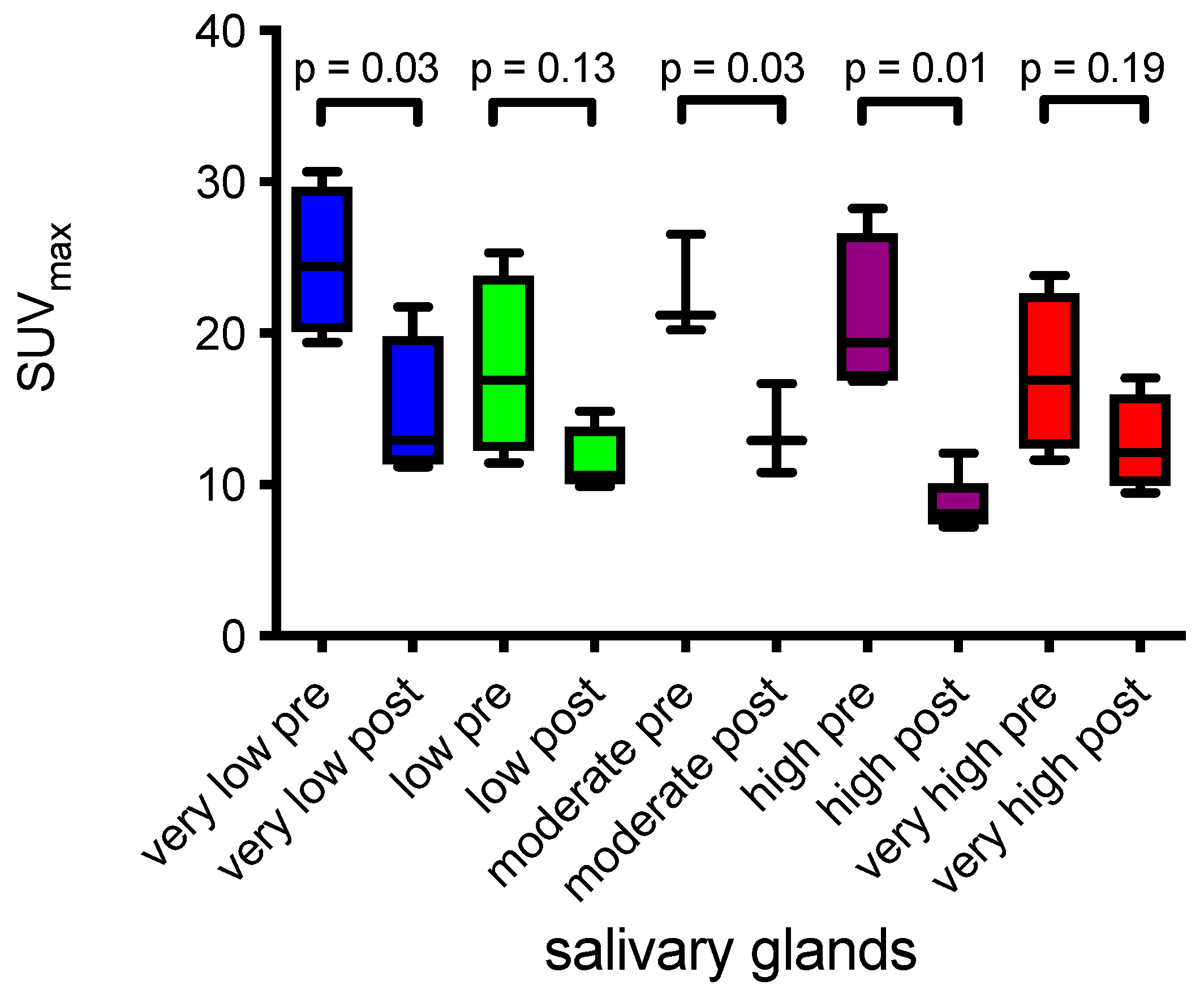
2.3. Salivary Glands and Tumor Burden
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. PSMA-Ligand PET Imaging
4.3. Image Analysis
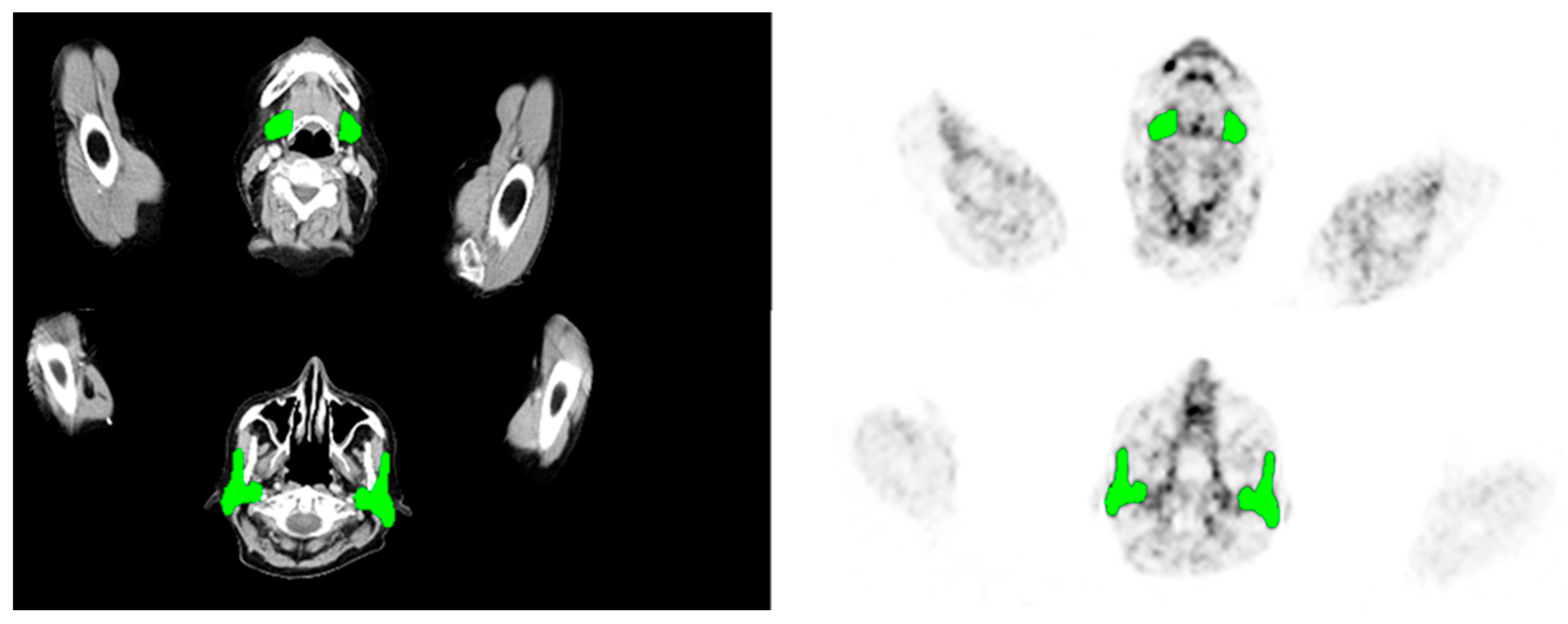
- Volume-SG was determined in the simultaneously acquired anatomical data (CT or MRI) of the SG. Delineation of the submandibular and parotid glands was measured of each gland separately and on the basis of all available slices (Figure 5).
- PSMA-SGU was quantified before the first and after the first two cycles of LuPSMA (cohort A) treatment and before and after the first cycle of AcPSMA (cohort B). SG was defined as the parotid and the submandibular glands. PSMA-SGU was determined using the in-house developed software qPSMA (with a threshold SUV of 4).
- SUVmean and SUVmax was determined using Syngo.Via (Siemens Healthineers, Erlangen, Germany). For SUVmean, a 3D VOI using an isocontour of 20% of the SUVmax was used.
- PSMA-TV was measured using qPSMA [47]. Bone lesions and soft tissue lesions were separately segmented, and obtained results were summed up. The PSMA-ligand uptake in normal organs was neglected before the quantification of whole-body tumor burden.
4.4. Statistical Analysis
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schafers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; Morgenstern, A. Targeted alpha-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Swimmer-Plot Analysis Suggests Efficacy Regarding Duration of Tumor Control. J. Nucl. Med. 2018, 59, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-Targeted alpha-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [PubMed]
- Zacherl, M.J.; Gildehaus, F.J.; Mittlmeier, L.; Boning, G.; Gosewisch, A.; Wenter, V.; Unterrainer, M.; Schmidt-Hegemann, N.; Belka, C.; Kretschmer, A.; et al. First Clinical Results for PSMA-Targeted alpha-Therapy Using 225Ac-PSMA-I&T in Advanced-mCRPC Patients. J. Nucl. Med. 2021, 62, 669–674. [Google Scholar]
- Feuerecker, B.; Tauber, R.; Knorr, K.; Heck, M.; Beheshti, A.; Seidl, C.; Bruchertseifer, F.; Pickhard, A.; Gafita, A.; Kratochwil, C.; et al. Activity and Adverse Events of Actinium-225-PSMA-617 in Advanced Metastatic Castration-resistant Prostate Cancer After Failure of Lutetium-177-PSMA. Eur. Urol. 2020, 79, 343–350. [Google Scholar] [CrossRef]
- Hey, J.; Setz, J.; Gerlach, R.; Janich, M.; Hildebrandt, G.; Vordermark, D.; Gernhardt, C.R.; Kuhnt, T. Parotid gland-recovery after radiotherapy in the head and neck region--36 months follow-up of a prospective clinical study. Radiat. Oncol. 2011, 6, 125. [Google Scholar] [CrossRef]
- Dijkema, T.; Raaijmakers, C.P.; Ten Haken, R.K.; Roesink, J.M.; Braam, P.M.; Houweling, A.C.; Moerland, M.A.; Eisbruch, A.; Terhaard, C.H. Parotid gland function after radiotherapy: The combined michigan and utrecht experience. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 449–453. [Google Scholar] [CrossRef]
- Fard-Esfahani, A.; Emami-Ardekani, A.; Fallahi, B.; Fard-Esfahani, P.; Beiki, D.; Hassanzadeh-Rad, A.; Eftekhari, M. Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma. Nucl. Med. Commun. 2014, 35, 808–817. [Google Scholar] [CrossRef]
- Itonaga, T.; Tokuuye, K.; Mikami, R.; Shimizu, A.; Sato, H.; Yoshimura, M.; Tsukahara, K.; Saito, K. Mathematical evaluation of post-radiotherapy salivary gland function using salivary gland scintigraphy. Br. J. Radiol. 2022, 95, 20210718. [Google Scholar] [CrossRef]
- Allweiss, P.; Braunstein, G.D.; Katz, A.; Waxman, A. Sialadenitis following I-131 therapy for thyroid carcinoma: Concise communication. J. Nucl. Med. 1984, 25, 755–758. [Google Scholar] [PubMed]
- Wang, K.; Pearlstein, K.A.; Moon, D.H.; Mahbooba, Z.M.; Deal, A.M.; Wang, Y.; Sutton, S.R.; Motley, B.B.; Judy, G.D.; Holmes, J.A.; et al. Assessment of Risk of Xerostomia After Whole-Brain Radiation Therapy and Association With Parotid Dose. JAMA Oncol. 2019, 5, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Badam, R.K.; Suram, J.; Babu, D.B.; Waghray, S.; Marshal, R.; Bontha, S.C.; Lavanya, R.; Kanth, S. Assessment of Salivary Gland Function Using Salivary Scintigraphy in Pre and Post Radioactive Iodine Therapy in Diagnosed Thyroid Carcinoma Patients. J. Clin. Diagn. Res. 2016, 10, ZC60. [Google Scholar] [CrossRef]
- Bohuslavizki, K.H.; Brenner, W.; Lassmann, S.; Tinnemeyer, S.; Tonshoff, G.; Sippel, C.; Wolf, H.; Clausen, M.; Henze, E. Quantitative salivary gland scintigraphy in the diagnosis of parenchymal damage after treatment with radioiodine. Nucl. Med. Commun. 1996, 17, 681–686. [Google Scholar] [CrossRef]
- Malpani, B.L.; Samuel, A.M.; Jaiswar, R.K. Salivary gland scintigraphy after radioiodine therapy. Nucl. Med. Commun. 1998, 19, 183–184. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Kim, J.M.; Choi, M.E.; Kim, S.K.; Kim, Y.M.; Choi, J.S. Does Salivary Function Decrease in Proportion to Radioiodine Dose? Laryngoscope 2020, 130, 2173–2178. [Google Scholar] [CrossRef]
- Langbein, T.; Kulkarni, H.R.; Schuchardt, C.; Mueller, D.; Volk, G.F.; Baum, R.P. Salivary Gland Toxicity of PSMA-Targeted Radioligand Therapy with 177Lu-PSMA and Combined 225Ac- and 177Lu-Labeled PSMA Ligands (TANDEM-PRLT) in Advanced Prostate Cancer: A Single-Center Systematic Investigation. Diagnostics 2022, 12, 1926. [Google Scholar] [CrossRef]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Tripathi, M.; Seth, A.; Bal, C. Efficacy and safety of 225Ac-PSMA-617 targeted alpha therapy in metastatic castration-resistant Prostate Cancer patients. Theranostics 2020, 10, 9364–9377. [Google Scholar] [CrossRef]
- Konings, A.W.; Coppes, R.P.; Vissink, A. On the mechanism of salivary gland radiosensitivity. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1187–1194. [Google Scholar] [CrossRef]
- Nomayr, A.; Lell, M.; Sweeney, R.; Bautz, W.; Lukas, P. MRI appearance of radiation-induced changes of normal cervical tissues. Eur. Radiol. 2001, 11, 1807–1817. [Google Scholar] [CrossRef]
- Barker, J.L., Jr.; Garden, A.S.; Ang, K.K.; O′Daniel, J.C.; Wang, H.; Court, L.E.; Morrison, W.H.; Rosenthal, D.I.; Chao, K.S.; Tucker, S.L.; et al. Quantification of volumetric and geometric changes occurring during fractionated radiotherapy for head-and-neck cancer using an integrated CT/linear accelerator system. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 960–970. [Google Scholar] [CrossRef]
- Wu, V.W.; Ying, M.T.; Kwong, D.L. Evaluation of radiation-induced changes to parotid glands following conventional radiotherapy in patients with nasopharygneal carcinoma. Br. J. Radiol. 2011, 84, 843–849. [Google Scholar] [CrossRef]
- Belli, M.L.; Sarnelli, A.; Mezzenga, E.; Cesarini, F.; Caroli, P.; Di Iorio, V.; Strigari, L.; Cremonesi, M.; Romeo, A.; Nicolini, S.; et al. Targeted Alpha Therapy in mCRPC (Metastatic Castration-Resistant Prostate Cancer) Patients: Predictive Dosimetry and Toxicity Modeling of 225Ac-PSMA (Prostate-Specific Membrane Antigen). Front. Oncol. 2020, 10, 531660. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Giesel, F.L.; Stefanova, M.; Benesova, M.; Bronzel, M.; Afshar-Oromieh, A.; Mier, W.; Eder, M.; Kopka, K.; Haberkorn, U. PSMA-Targeted Radionuclide Therapy of Metastatic Castration-Resistant Prostate Cancer with 177Lu-Labeled PSMA-617. J. Nucl. Med. 2016, 57, 1170–1176. [Google Scholar] [CrossRef] [PubMed]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P.; et al. Dosimetry of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes. J. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef]
- Kabasakal, L.; AbuQbeitah, M.; Aygun, A.; Yeyin, N.; Ocak, M.; Demirci, E.; Toklu, T. Pre-therapeutic dosimetry of normal organs and tissues of 177Lu-PSMA-617 prostate-specific membrane antigen (PSMA) inhibitor in patients with castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1976–1983. [Google Scholar] [CrossRef] [PubMed]
- Feuerecker, B.; Chantadisai, M.; Allmann, A.; Tauber, R.; Allmann, J.; Steinhelfer, L.; Rauscher, I.; Wurzer, A.; Wester, H.J.; Weber, W.A.; et al. Pretherapeutic Comparative Dosimetry of 177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T in Patients with Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2022, 63, 833–839. [Google Scholar] [PubMed]
- Derlin, T.; Widjaja, L.; Werner, R.A.; Bengel, F.M. 177Lu-PSMA for Extended Treatment of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2023, 64, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Taieb, D.; Foletti, J.M.; Bardies, M.; Rocchi, P.; Hicks, R.J.; Haberkorn, U. PSMA-Targeted Radionuclide Therapy and Salivary Gland Toxicity: Why Does It Matter? J. Nucl. Med. 2018, 59, 747–748. [Google Scholar] [CrossRef]
- Navazesh, M.; Christensen, C.; Brightman, V. Clinical criteria for the diagnosis of salivary gland hypofunction. J. Dent. Res. 1992, 71, 1363–1369. [Google Scholar] [CrossRef]
- Gaertner, F.C.; Halabi, K.; Ahmadzadehfar, H.; Kurpig, S.; Eppard, E.; Kotsikopoulos, C.; Liakos, N.; Bundschuh, R.A.; Strunk, H.; Essler, M. Uptake of PSMA-ligands in normal tissues is dependent on tumor load in patients with prostate cancer. Oncotarget 2017, 8, 55094–55103. [Google Scholar] [CrossRef] [PubMed]
- Gafita, A.; Wang, H.; Robertson, A.; Armstrong, W.R.; Zaum, R.; Weber, M.; Yagubbayli, F.; Kratochwil, C.; Grogan, T.R.; Nguyen, K.; et al. Tumor sink effect in 68Ga-PSMA-11 PET: Myth or Reality? J. Nucl. Med. 2021, 63, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Lapa, C.; Yin, Y.; Javadi, M.S.; Buck, A.K.; Higuchi, T.; Pienta, K.J.; Pomper, M.G.; et al. Semiquantitative Parameters in PSMA-Targeted PET Imaging with [18F]DCFPyL: Impact of Tumor Burden on Normal Organ Uptake. Mol. Imaging Biol. 2020, 22, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [177Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Rupp, N.J.; Umbricht, C.A.; Pizzuto, D.A.; Lenggenhager, D.; Topfer, A.; Muller, J.; Muehlematter, U.J.; Ferraro, D.A.; Messerli, M.; Morand, G.B.; et al. First Clinicopathologic Evidence of a Non-PSMA-Related Uptake Mechanism for 68Ga-PSMA-11 in Salivary Glands. J. Nucl. Med. 2019, 60, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Tonnesmann, R.; Meyer, P.T.; Eder, M.; Baranski, A.C. [177Lu]Lu-PSMA-617 Salivary Gland Uptake Characterized by Quantitative In Vitro Autoradiography. Pharmaceuticals 2019, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Filss, C.; Heinzel, A.; Miiller, B.; Vogg, A.T.J.; Langen, K.J.; Mottaghy, F.M. Relevant tumor sink effect in prostate cancer patients receiving 177Lu-PSMA-617 radioligand therapy. Nuklearmedizin 2018, 57, 19–25. [Google Scholar] [CrossRef]
- Tuncel, M.; Telli, T.; Tuncali, M.C.; Karabulut, E. Predictive factors of tumor sink effect: Insights from 177Lu-Prostate-specific membrane antigen therapy. Ann. Nucl. Med. 2021, 35, 529–539. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Haberkorn, U.; Zechmann, C.; Armor, T.; Mier, W.; Spohn, F.; Debus, N.; Holland-Letz, T.; Babich, J.; Kratochwil, C. Repeated PSMA-targeting radioligand therapy of metastatic prostate cancer with 131I-MIP-1095. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 950–959. [Google Scholar] [CrossRef]
- Zechmann, C.M.; Afshar-Oromieh, A.; Armor, T.; Stubbs, J.B.; Mier, W.; Hadaschik, B.; Joyal, J.; Kopka, K.; Debus, J.; Babich, J.W.; et al. Radiation dosimetry and first therapy results with a 124I/131I-labeled small molecule (MIP-1095) targeting PSMA for prostate cancer therapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1280–1292. [Google Scholar] [CrossRef]
- Mahajan, S.; Grewal, R.K.; Friedman, K.P.; Schoder, H.; Pandit-Taskar, N. Assessment of salivary gland function after 177Lu-PSMA radioligand therapy: Current concepts in imaging and management. Transl. Oncol. 2022, 21, 101445. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, T.; Zisser, L.; Kretschmer-Chott, E.; Weber, M.; Grubmuller, B.; Kramer, G.; Shariat, S.F.; Mitterhauser, M.; Schmitl, S.; Vraka, C.; et al. Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer. Curr. Oncol. 2021, 28, 3692–3704. [Google Scholar] [CrossRef]
- Rahbar, K.; Bode, A.; Weckesser, M.; Avramovic, N.; Claesener, M.; Stegger, L.; Bogemann, M. Radioligand Therapy With 177Lu-PSMA-617 as A Novel Therapeutic Option in Patients With Metastatic Castration Resistant Prostate Cancer. Clin. Nucl. Med. 2016, 41, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Baum, R.P.; Kulkarni, H.R.; Schuchardt, C.; Singh, A.; Wirtz, M.; Wiessalla, S.; Schottelius, M.; Mueller, D.; Klette, I.; Wester, H.J. 177Lu-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy of Metastatic Castration-Resistant Prostate Cancer: Safety and Efficacy. J. Nucl. Med. 2016, 57, 1006–1013. [Google Scholar] [CrossRef]
- Van Kalmthout, L.; Braat, A.; Lam, M.; van Leeuwaarde, R.; Krijger, G.; Ververs, T.; Mehra, N.; Bins, A.; Hunting, J.; de Keizer, B. First Experience With 177Lu-PSMA-617 Therapy for Advanced Prostate Cancer in the Netherlands. Clin. Nucl. Med. 2019, 44, 446–451. [Google Scholar] [CrossRef]
- Gafita, A.; Bieth, M.; Kronke, M.; Tetteh, G.; Navarro, F.; Wang, H.; Gunther, E.; Menze, B.; Weber, W.A.; Eiber, M. qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT. J. Nucl. Med. 2019, 60, 1277–1283. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Body Tumor Volume Prior to AcPSMA | Very Low | Low | Moderate | High | Very High | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| pre | post | pre | post | pre | post | pre | post | pre | post | ||
| AcPSMA RLT | |||||||||||
| Whole body | PSMA-TV (mL) | 602 ± 354 | 431 ± 296 | 1393 ± 217 | 1456 ± 391 | 1848 ± 156 | 2370 ± 1076 | 3378 ± 288 | 3216 ± 693 | 4869 ± 342 | 4296 ± 1252 |
| Salivary glands | SUVmean | 11.7 ± 2.4 | 6.7 ± 2.4 * | 8.1 ± 3.3 | 4.9 ± 1.1 | 11.1 ± 1.8 | 5.7 ± 1.6 ** | 9.1 ± 2.9 | 4.5 ± 2.3 *** | 7.8 ± 2.7 | 5.3 ± 1.7 |
| SUVmax | 24.8 ± 4.9 | 14.7 ± 4.8 * | 17.7 ± 6.1 | 11.5 ± 2.3 | 22.7 ± 3.4 | 13.5 ± 2.9 ** | 20.9 ± 5.4 | 8.6 ± 1.9 # | 17.3 ± 5.3 | 12.7 ± 3.2 | |
| LuPSMA RLT | |||||||||||
| Salivary glands | SUVmean | 14.9 ± 2.9 | 13.5 ± 2.6 | 11.3 ± 2.2 | 11.2 + 5.3 | 9.0 ± 2.8 | 11.9 ± 1.9 * | 10.2 ± 2.6 | 8.8 ± 1.4 | 11.3 ± 2.8 | 10.3 ± 3.1 |
| SUVmax | 33.6 ± 9.8 | 33.4 ± 14.3 | 23.9 ± 4.0 | 23.7 ± 10.3 | 18.6 ± 4.1 | 25.4 ± 5.9 ** | 21.5 ± 5.3 | 18.8 ± 2.9 | 24.5 ± 5.6 | 26.1 ± 12.1 | |
| No. | Number (Agents) of Previous mCRPC Lines Prior to 225Ac-RLT | Number (Agents) of Previous mCRPC Lines Prior to 225Ac-RLT | Number of LuPSMA Cycles | Activity LuPSMA RLT (GBq)/Cycle | ECOG Score | Metastases | Activity of First AcPSMA RLT (MBq) |
|---|---|---|---|---|---|---|---|
| 1 * | 4 (E, A, D, Lu) | 4 | 2 | 8/7.2 | 0 | B, LN | 8 |
| 2 | 8 (D, C, A, C, E, C, Ra, Lu) | 8 | 2 | 5.7/5.7 | 0 | B | 8 |
| 3 | 4 (D, E, A, Lu) | 4 | 8 | 7.4/7.4/7.3/7.3/7.1/7.1/7.1/7.3 | 1 | B, LN | 8 |
| 4 * | 5 (A, E, Lu, D, Cis/Eto) | 5 | 4 | 7.2/7.7/7.2/7.7 | 1 | B, LN | 8 |
| 5 * | 6 (D, A, Lu, C, E, Cis/Eto) | 6 | 2 | 7.6/7.4 | 1 | B, LN, Liver, Lungs | 8 |
| 6 * | 6 (D, Ra, E, C, A, Lu) | 6 | 4 | 6.9/7.3/7.4/7.5 | 2 | B, LN | 10 |
| 7 | 4 (D, Ra, A, Lu) | 4 | 5 | 7.5/7.3/7.5/7.8/7.7 | 1 | B, LN | 8 |
| 8 * | 8 (CureVac, A + CureVac, D, Study, C, Lu, E, A) | 8 | 2 | 7.3/7.5 | 1 | B, LN, Lungs | 8 |
| 9 * | 4 (A, D, Lu, E) | 4 | 6 | 7.2/7.4/7.3/7.4/7.3/6.7 | 1 | B, LN, Peritoneal | 10 |
| 10 * | 3 (A, E, Lu) | 3 | 6 | 7.3/7.6/7.7/7.0/7.5/ 7.4 | 1 | B, LN | 10 |
| 11 | 7 (A, E, D, A, D, C, Lu) | 7 | 6 | 8.3/7.9/8.3/7.9/7.4/7.3 | 1 | B | 8 |
| 12 | 6 (A, E, D, C, Lu, Cis/Eto) | 6 | 2 | 8.3/7.8 | 1 | B, LN | 13 |
| 13 * | 5 (E, D, A, E, Lu) | 5 | 6 | 5.1/7.4/7.3/7.6/7.4/6.7 | 1 | B, LN, Liver, Lung | 11 |
| 14 * | 5 (A, E, D, C, Lu) | 5 | 1 | 7.9 | 1 | B, LN, Liver, Brain | 6 |
| 15 * | 8 (CureVac, A, Ra, Lu, E, D, O, C) | 8 | 6 | 7.3/7.3/7.3/7.6/7.4/ 7.0 | 1 | B, LN | 10 |
| 16 * | 8 (D, C, A, D, E, A, C, Lu) | 8 | 8 | 7.3/7.8/7.2/7.2/7.5/7.5/7.5/7.4 | 0 | B, LN, Lungs | 12 |
| 17 * | 5 (D/C, A, D/C, Carbo, Lu) | 5 | 4 | 7.3/7.6/7.2/7.3 | 1 | LN, B, Peritoneal | 9 |
| 18 | 3 (A, Lu, D) | 3 | 5 | 3.7/3.7/5.5/5.5/4.2 | 1 | B, LN | 10 |
| 19 * | 6 (D, A, E, C, Lu, C) | 6 | 4 | 6.8/7.6/7.3/9.0 | 1 | B, LN, Liver | 14 |
| 20 * | 5 (E, D, A, Lu, C) | 5 | 4 | 8.2/7.5/6.2/7.5 | 1 | B, LN | 8 |
| 21 * | 6 (A, E, D, Lu, Ra, C) | 6 | 4 | 3.3/3.3/3.4/3.5 | 1 | B | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feuerecker, B.; Gafita, A.; Langbein, T.; Tauber, R.; Seidl, C.; Bruchertseifer, F.; Gschwendt, J.E.; Weber, W.A.; D’Alessandria, C.; Morgenstern, A.; et al. Comparative Analysis of Morphological and Functional Effects of 225Ac- and 177Lu-PSMA Radioligand Therapies (RLTs) on Salivary Glands. Int. J. Mol. Sci. 2023, 24, 16845. https://doi.org/10.3390/ijms242316845
Feuerecker B, Gafita A, Langbein T, Tauber R, Seidl C, Bruchertseifer F, Gschwendt JE, Weber WA, D’Alessandria C, Morgenstern A, et al. Comparative Analysis of Morphological and Functional Effects of 225Ac- and 177Lu-PSMA Radioligand Therapies (RLTs) on Salivary Glands. International Journal of Molecular Sciences. 2023; 24(23):16845. https://doi.org/10.3390/ijms242316845
Chicago/Turabian StyleFeuerecker, Benedikt, Andrei Gafita, Thomas Langbein, Robert Tauber, Christof Seidl, Frank Bruchertseifer, Jürgen E. Gschwendt, Wolfgang A. Weber, Calogero D’Alessandria, Alfred Morgenstern, and et al. 2023. "Comparative Analysis of Morphological and Functional Effects of 225Ac- and 177Lu-PSMA Radioligand Therapies (RLTs) on Salivary Glands" International Journal of Molecular Sciences 24, no. 23: 16845. https://doi.org/10.3390/ijms242316845
APA StyleFeuerecker, B., Gafita, A., Langbein, T., Tauber, R., Seidl, C., Bruchertseifer, F., Gschwendt, J. E., Weber, W. A., D’Alessandria, C., Morgenstern, A., & Eiber, M. (2023). Comparative Analysis of Morphological and Functional Effects of 225Ac- and 177Lu-PSMA Radioligand Therapies (RLTs) on Salivary Glands. International Journal of Molecular Sciences, 24(23), 16845. https://doi.org/10.3390/ijms242316845