

Metabolomics of Cerebrospinal Fluid Amino and Fatty Acids in Early Stages of Multiple Sclerosis


Abstract
:1. Introduction
2. Results
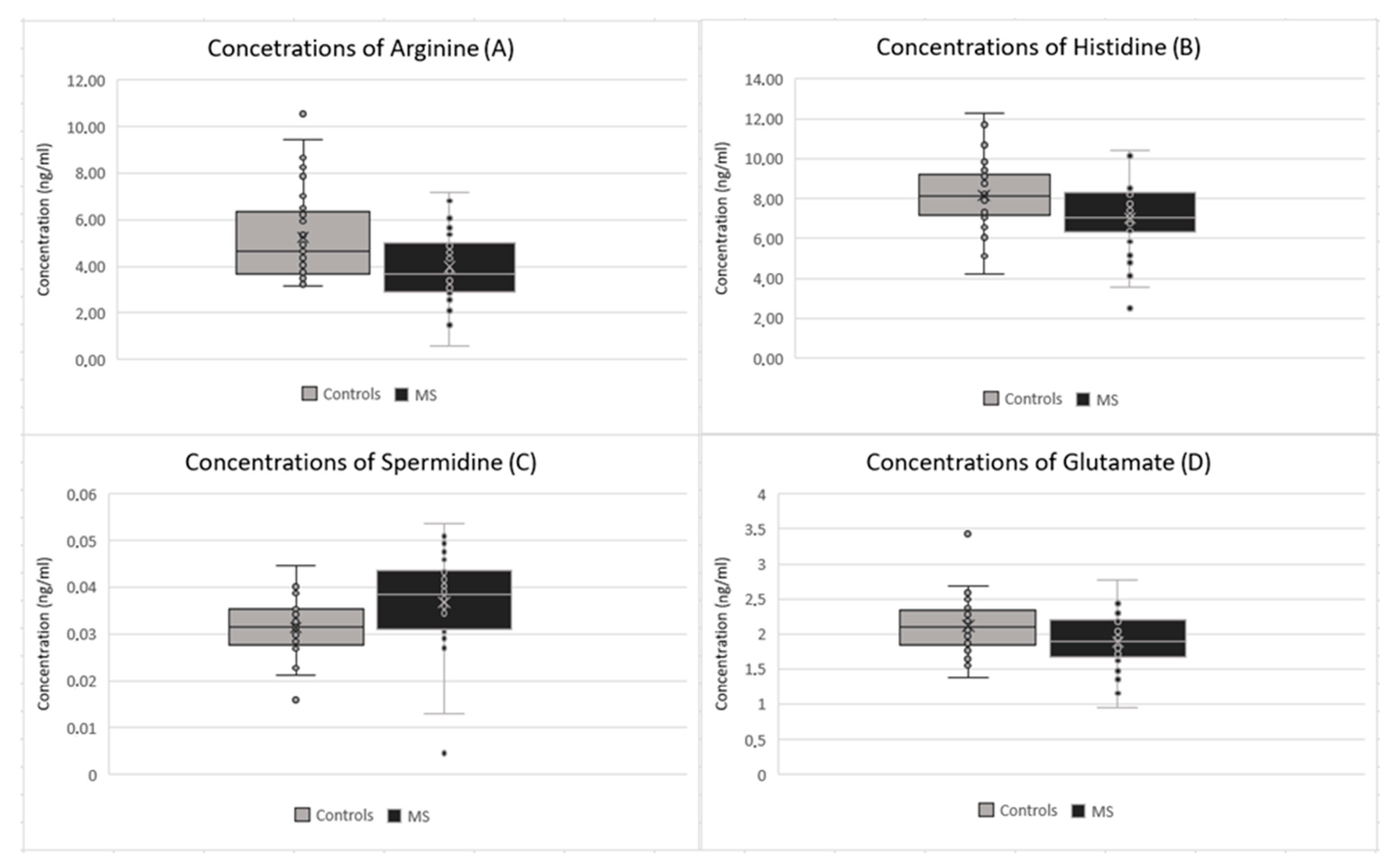
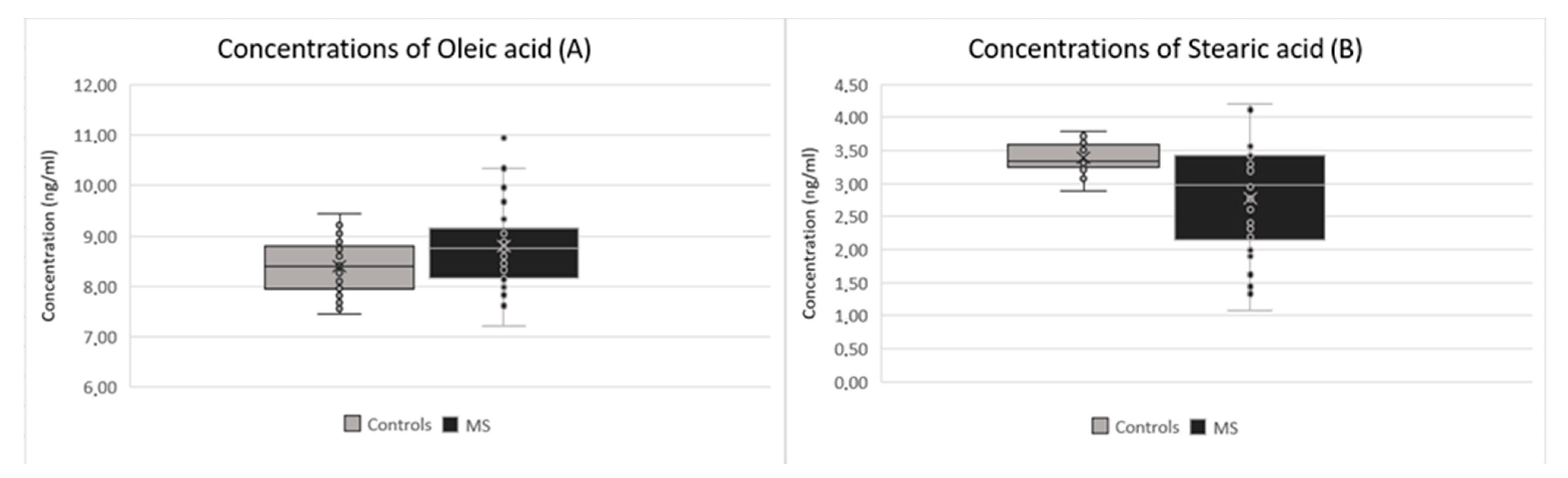
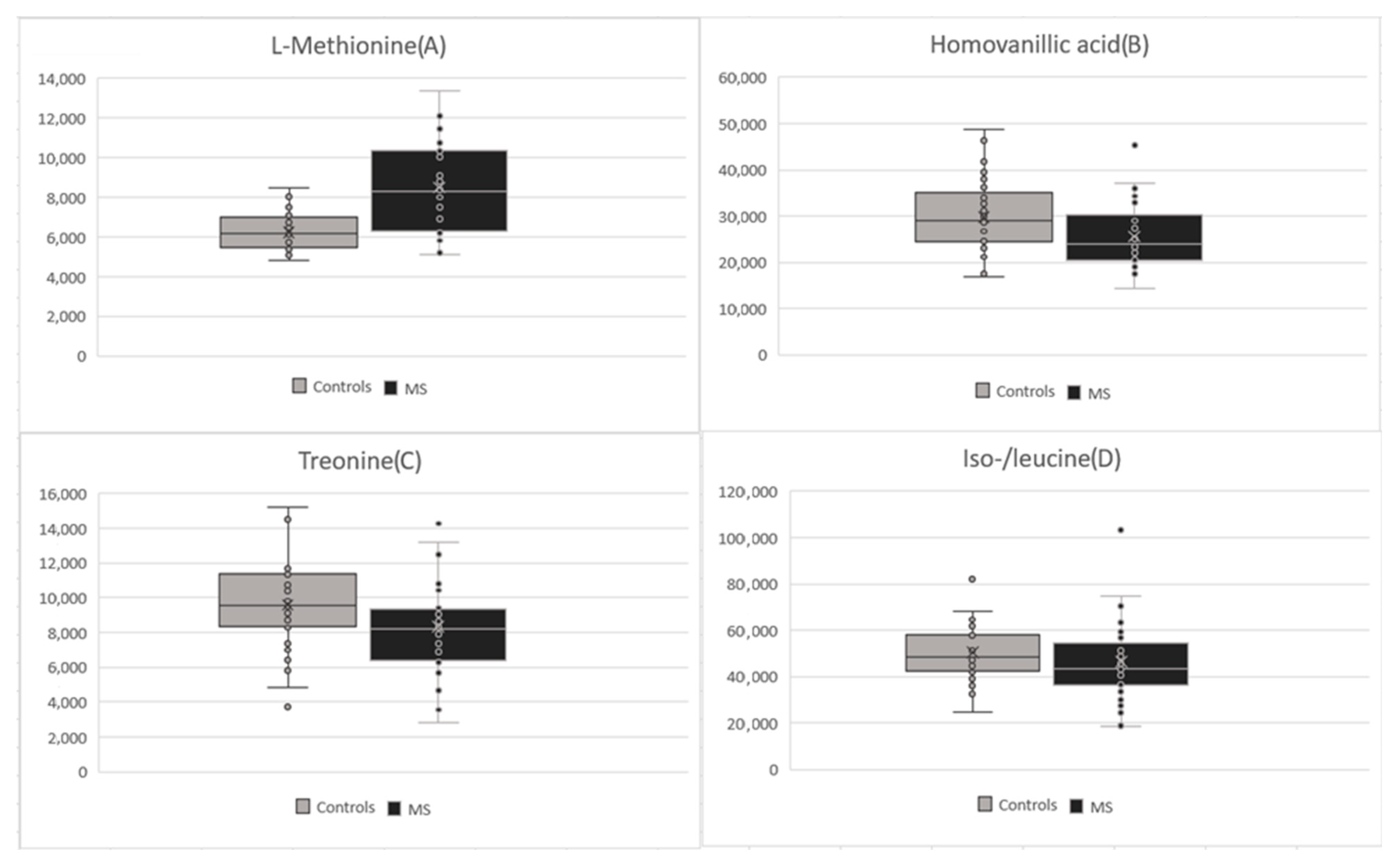
2.1. Metabolomic Analyses
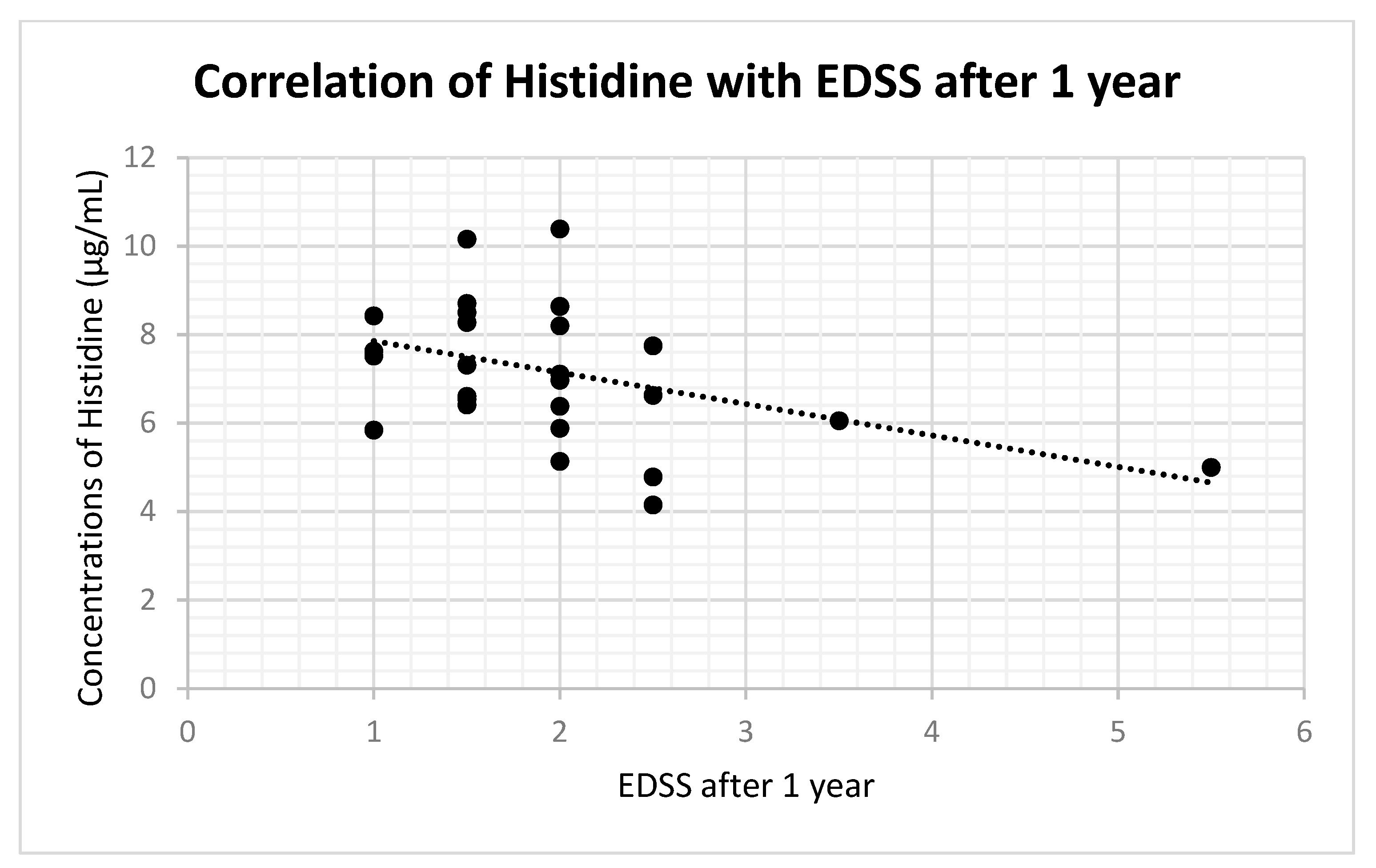
2.2. Correlation of Metabolomics Results with EDSS Values
2.3. Correlation of Metabolomic Results with Onset of Clinical Symptoms to CSF Collection
3. Discussion
4. Methods
4.1. Recruitment of Patients
4.2. Sample Collection and Preparation
4.3. High-Performance Liquid Chromatography Tandem Mass Spectrometry (HPLC-MS/MS) Analysis
4.4. Data Processing
4.5. Extraction of Clinical Data
4.6. Statistical Analyses
5. Conclusions
6. Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schweitzer, F.; Laurent, S.; Fink, G.R.; Barnett, M.H.; Reddel, S.; Hartung, H.-P.; Warnke, C. Age and the risks of high-efficacy disease modifying drugs in multiple sclerosis. Curr. Opin. Neurol. 2019, 32, 305–312. [Google Scholar] [CrossRef]
- Van Wijmeersch, B.; Hartung, H.-P.; Vermersch, P.; Pugliatti, M.; Pozzilli, C.; Grigoriadis, N.; Alkhawajah, M.; Airas, L.; Linker, R.; Oreja-Guevara, C. Using personalized prognosis in the treatment of relapsing multiple sclerosis: A practical guide. Front. Immunol. 2022, 13, 991291. [Google Scholar] [CrossRef]
- Hegen, H.; Walde, J.; Berek, K.; Arrambide, G.; Gnanapavan, S.; Kaplan, B.; Khalil, M.; Saadeh, R.; Teunissen, C.; Tumani, H.; et al. Cerebrospinal fluid kappa free light chains for the diagnosis of multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. J. 2023, 29, 169–181. [Google Scholar] [CrossRef]
- Patti, G.J.; Yanes, O.; Siuzdak, G. Innovation: Metabolomics: The apogee of the omics trilogy. Nat. Rev. Mol. Cell Biol. 2012, 13, 263–269. [Google Scholar] [CrossRef]
- Rabinowitz, J.D.; Purdy, J.G.; Vastag, L.; Shenk, T.; Koyuncu, E. Metabolomics in drug target discovery. Cold Spring Harb. Symp. Quant. Biol. 2011, 76, 235–246. [Google Scholar] [CrossRef]
- Reinke, S.N.; Broadhurst, D.I.; Sykes, B.D.; Baker, G.B.; Catz, I.; Warren, K.; Power, C. Metabolomic profiling in multiple sclerosis: Insights into biomarkers and pathogenesis. Mult. Scler. J. 2014, 20, 1396–1400. [Google Scholar] [CrossRef]
- Park, S.J.; Jeong, I.H.; Kong, B.S.; Lee, J.-E.; Kim, K.H.; Lee, D.Y.; Kim, H.J. Disease Type- and Status-Specific Alteration of CSF Metabolome Coordinated with Clinical Parameters in Inflammatory Demyelinating Diseases of CNS. PLoS ONE 2016, 11, e0166277. [Google Scholar] [CrossRef]
- Kasakin, M.F.; Rogachev, A.D.; Predtechenskaya, E.V.; Zaigraev, V.J.; Koval, V.V.; Pokrovsky, A.G. Targeted metabolomics approach for identification of relapsing-remitting multiple sclerosis markers and evaluation of diagnostic models. Medchemcomm 2019, 10, 1803–1809. [Google Scholar] [CrossRef]
- Sylvestre, D.A.; Slupsky, C.M.; Aviv, R.I.; Swardfager, W.; Taha, A.Y. Untargeted metabolomic analysis of plasma from relapsing-remitting multiple sclerosis patients reveals changes in metabolites associated with structural changes in brain. Brain Res. 2019, 1732, 146589. [Google Scholar] [CrossRef]
- Nogueras, L.; Gonzalo, H.; Jové, M.; Sol, J.; Gil-Sanchez, A.; Hervás, J.V.; Valcheva, P.; Gonzalez-Mingot, C.; Solana, M.J.; Peralta, S.; et al. Lipid profile of cerebrospinal fluid in multiple sclerosis patients: A potential tool for diagnosis. Sci. Rep. 2019, 9, 11313. [Google Scholar] [CrossRef]
- Murgia, F.; Lorefice, L.; Poddighe, S.; Fenu, G.; Secci, M.A.; Marrosu, M.G.; Cocco, E.; Atzori, L. Multi-Platform Characterization of Cerebrospinal Fluid and Serum Metabolome of Patients Affected by Relapsing-Remitting and Primary Progressive Multiple Sclerosis. J. Clin. Med. 2020, 9, 863. [Google Scholar] [CrossRef]
- Carlsson, H.; Abujrais, S.; Herman, S.; Khoonsari, P.E.; Åkerfeldt, T.; Svenningsson, A.; Burman, J.; Kultima, K. Targeted metabolomics of CSF in healthy individuals and patients with secondary progressive multiple sclerosis using high-resolution mass spectrometry. Metabolomics 2020, 16, 26. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Smith, M.D.; Kim, S.; Sotirchos, E.S.; Kornberg, M.D.; Douglas, M.; Nourbakhsh, B.; Graves, J.; Rattan, R.; Poisson, L.; et al. Multi-omic evaluation of metabolic alterations in multiple sclerosis identifies shifts in aromatic amino acid metabolism. Cell Rep. Med. 2021, 2, 100424. [Google Scholar] [CrossRef]
- Yan, J.; Kuzhiumparambil, U.; Bandodkar, S.; Dale, R.C.; Fu, S. Cerebrospinal fluid metabolomics: Detection of neuroinflammation in human central nervous system disease. Clin. Transl. Immunol. 2021, 10, e1318. [Google Scholar] [CrossRef]
- Signoriello, E.; Iardino, P.; Casertano, S.; De Lucia, D.; Pucciarelli, A.; Puoti, G.; Chiosi, E.; Lus, G. 12-months prospective Pentraxin-3 and metabolomic evaluation in multiple sclerosis patients treated with glatiramer acetate. J. Neuroimmunol. 2020, 348, 577385. [Google Scholar] [CrossRef]
- Gonzalo, H.; Brieva, L.; Tatzber, F.; Jové, M.; Cacabelos, D.; Cassanyé, A.; Lanau-Angulo, L.; Boada, J.; Serrano, J.C.E.; González, C.; et al. Lipidome analysis in multiple sclerosis reveals protein lipoxidative damage as a potential pathogenic mechanism. J. Neurochem. 2012, 123, 622–634. [Google Scholar] [CrossRef]
- de Oliveira, E.M.L.; Montani, D.A.; Oliveira-Silva, D.; Rodrigues-Oliveira, A.F.; Matas, S.L.d.A.; Fernandes, G.B.P.; da Silva, I.D.C.G.; Turco, E.G.L. Multiple sclerosis has a distinct lipid signature in plasma and cerebrospinal fluid. Arq. Neuro-Psiquiatr. 2019, 77, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Viant, M.R.; Ball, A.K.; Burdon, M.A.; Walker, E.A.; Stewart, P.M.; Rauz, S.; Young, S.P. NMR-based metabolomic analysis of cerebrospinal fluid and serum in neurological diseases—A diagnostic tool? NMR Biomed. 2010, 23, 123–132. [Google Scholar] [CrossRef]
- Pieragostino, D.; D’Alessandro, M.; di Ioia, M.; Rossi, C.; Zucchelli, M.; Urbani, A.; Di Ilio, C.; Lugaresi, A.; Sacchetta, P.; Del Boccio, P. An integrated metabolomics approach for the research of new cerebrospinal fluid biomarkers of multiple sclerosis. Mol. Biosyst. 2015, 11, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Sarchielli, P.; Greco, L.; Floridi, A.; Floridi, A.; Gallai, V. Excitatory amino acids and multiple sclerosis: Evidence from cerebrospinal fluid. Arch. Neurol. 2003, 60, 1082–1088. [Google Scholar] [CrossRef]
- Poddighe, S.; Murgia, F.; Lorefice, L.; Liggi, S.; Cocco, E.; Marrosu, M.G.; Atzori, L. Metabolomic analysis identifies altered metabolic pathways in Multiple Sclerosis. Int. J. Biochem. Cell Biol. 2017, 93, 148–155. [Google Scholar] [CrossRef]
- Srinivasan, R.; Sailasuta, N.; Hurd, R.; Nelson, S.; Pelletier, D. Evidence of elevated glutamate in multiple sclerosis using magnetic resonance spectroscopy at 3 T. Brain 2005, 128, 1016–1025. [Google Scholar] [CrossRef]
- Cocco, E.; Murgia, F.; Lorefice, L.; Barberini, L.; Poddighe, S.; Frau, J.; Fenu, G.; Coghe, G.; Murru, M.R.; Murru, R.; et al. (1)H-NMR analysis provides a metabolomic profile of patients with multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2015, 3, e185. [Google Scholar] [CrossRef]
- Podlecka-Piętowska, A.; Kacka, A.; Zakrzewska-Pniewska, B.; Nojszewska, M.; Zieminska, E.; Chalimoniuk, M.; Toczylowska, B. Altered Cerebrospinal Fluid Concentrations of Hydrophobic and Hydrophilic Compounds in Early Stages of Multiple Sclerosis-Metabolic Profile Analyses. J. Mol. Neurosci. 2019, 69, 94–105. [Google Scholar] [CrossRef]
- Murgia, F.; Lorefice, L.; Noto, A.; Spada, M.; Frau, J.; Fenu, G.; Coghe, G.; Gagliano, A.; Atzori, L.; Cocco, E. Metabolomic Changes in Patients Affected by Multiple Sclerosis and Treated with Fingolimod. Metabolites 2023, 13, 428. [Google Scholar] [CrossRef] [PubMed]
- Židó, M.; Kačer, D.; Valeš, K.; Svobodová, Z.; Zimová, D.; Štětkárová, I. Metabolomics of Cerebrospinal Fluid in Multiple Sclerosis Compared with Healthy Controls: A Pilot Study. Front. Neurol. 2022, 13, 874121. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Teunissen, C.; Menge, T.; Altintas, A.; Álvarez-Cermeño, J.C.; Bertolotto, A.; Berven, F.S.; Brundin, L.; Comabella, M.; Degn, M.; Deisenhammer, F.; et al. Consensus definitions and application guidelines for control groups in cerebrospinal fluid biomarker studies in multiple sclerosis. Mult. Scler. J. 2013, 19, 1802–1809. [Google Scholar] [CrossRef]
- Tapiero, H.; Mathé, G.; Couvreur, P.; Tew, K.D.I. Arginine. Biomed. Pharmacother. 2002, 56, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, H.; Zheng, Y.M.; Heber-Katz, E.; Fraser, N.; Rorke, L.; Fu, Z.F.; Hanlon, C.; Dietzschold, B. In vivo expression of inducible nitric oxide synthase in experimentally induced neurologic diseases. Proc. Natl. Acad. Sci. USA 1993, 90, 3024–3027. [Google Scholar] [CrossRef]
- Smith, K.J.; Lassmann, H. The role of nitric oxide in multiple sclerosis. Lancet Neurol. 2002, 1, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, V.; Scapagnini, G.; Ravagna, A.; Bella, R.; Foresti, R.; Bates, T.E.; Stella, A.-M.G.; Pennisi, G. Nitric oxide synthase is present in the cerebrospinal fluid of patients with active multiple sclerosis and is associated with increases in cerebrospinal fluid protein nitrotyrosine and S-nitrosothiols and with changes in glutathione levels. J. Neurosci. Res. 2002, 70, 580–587. [Google Scholar] [CrossRef]
- Cantoni, C.; Cignarella, F.; Ghezzi, L.; Mikesell, B.; Bollman, B.; Berrien-Elliott, M.M.; Ireland, A.R.; Fehniger, T.A.; Wu, G.F.; Piccio, L. Mir-223 regulates the number and function of myeloid-derived suppressor cells in multiple sclerosis and experimental autoimmune encephalomyelitis. Acta Neuropathol. 2017, 133, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Haas, H.L.; Sergeeva, O.A.; Selbach, O. Histamine in the nervous system. Physiol. Rev. 2008, 88, 1183–1241. [Google Scholar] [CrossRef] [PubMed]
- Jadidi-Niaragh, F.; Mirshafiey, A. Histamine and histamine receptors in pathogenesis and treatment of multiple sclerosis. Neuropharmacology 2010, 59, 180–189. [Google Scholar] [CrossRef]
- Musio, S.; Gallo, B.; Scabeni, S.; Lapilla, M.; Poliani, P.L.; Matarese, G.; Ohtsu, H.; Galli, S.J.; Mantegazza, R.; Steinman, L.; et al. A key regulatory role for histamine in experimental autoimmune encephalomyelitis: Disease exacerbation in histidine decarboxylase-deficient mice. J. Immunol. 2006, 176, 17–26. [Google Scholar] [CrossRef]
- Loy, B.D.; O’Connor, P.J. The effect of histamine on changes in mental energy and fatigue after a single bout of exercise. Physiol. Behav. 2016, 153, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Loy, B.D.; Fling, B.W.; Sage, K.M.; Spain, R.I.; Horak, F.B. Serum Histidine is Lower in Fatigued Women with Multiple Sclerosis. Fatigue 2019, 7, 69–80. [Google Scholar] [CrossRef]
- Tuomisto, L.; Kilpeläinen, H.; Riekkinen, P. Histamine and histamine-N-methyltransferase in the CSF of patients with multiple sclerosis. Agents Actions 1983, 13, 255–257. [Google Scholar] [CrossRef]
- Kallweit, U.; Aritake, K.; Bassetti, C.L.; Blumenthal, S.; Hayaishi, O.; Linnebank, M.; Baumann, C.R.; Urade, Y. Elevated CSF histamine levels in multiple sclerosis patients. Fluids Barriers CNS 2013, 10, 19. [Google Scholar] [CrossRef]
- Igarashi, K.; Kashiwagi, K. Modulation of cellular function by polyamines. Int. J. Biochem. Cell Biol. 2010, 42, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Zheng, C.; Cao, J.; Cao, G.; Shou, P.; Lin, L.; Velletri, T.; Jiang, M.; Chen, Q.; Han, Y.; et al. Spermidine alleviates experimental autoimmune encephalomyelitis through inducing inhibitory macrophages. Cell Death Differ. 2016, 23, 1850–1861. [Google Scholar] [CrossRef] [PubMed]
- Morselli, E.; Mariño, G.; Bennetzen, M.V.; Eisenberg, T.; Megalou, E.; Schroeder, S.; Cabrera, S.; Bénit, P.; Rustin, P.; Criollo, A.; et al. Spermidine and resveratrol induce autophagy by distinct pathways converging on the acetylproteome. J. Cell Biol. 2011, 192, 615–629. [Google Scholar] [CrossRef]
- Stojanovic, I.R.; Kostic, M.; Ljubisavljevic, S. The role of glutamate and its receptors in multiple sclerosis. J. Neural. Transm 2014, 121, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Hinzman, J.M.; Thomas, T.C.; Burmeister, J.J.; Quintero, J.E.; Huettl, P.; Pomerleau, F.; Gerhardt, G.A.; Lifshitz, J.; Carlson, S.W.; Yan, H.; et al. Diffuse brain injury elevates tonic glutamate levels and potassium-evoked glutamate release in discrete brain regions at two days post-injury: An enzyme-based microelectrode array study. J. Neurotrauma 2010, 27, 889–899. [Google Scholar] [CrossRef]
- Skripuletz, T.; Manzel, A.; Gropengießer, K.; Schäfer, N.; Gudi, V.; Singh, V.; Salinas Tejedor, L.; Jörg, S.; Hammer, A.; Voss, E.; et al. Pivotal role of choline metabolites in remyelination. Brain 2015, 138, 398–413. [Google Scholar] [CrossRef]
- Ye, L.; Sun, Y.; Jiang, Z.; Wang, G. L-Serine, an Endogenous Amino Acid, Is a Potential Neuroprotective Agent for Neurological Disease and Injury. Front. Mol. Neurosci. 2021, 14, 726665. [Google Scholar] [CrossRef]
- Lau, L.; Huganir, R.L. Role of Tyrosine Phosphorylation in the Nervous System. In Basic Neurochemistry: Molecular, Cellular and Medical Aspects, 6th ed.; Siegel, G.J., Agranoff, B.W., Albers, R.W., Fisher, S.K., Uhler, M.D., Eds.; Lippincott-Raven: Philadelphia, PA, USA, 1999. Available online: https://www.ncbi.nlm.nih.gov/books/NBK28147/ (accessed on 7 June 2023).
- Andersen, S.; Briggs, F.; Winnike, J.; Natanzon, Y.; Maichle, S.; Knagge, K.; Newby, L.; Gregory, S. Metabolome-based signature of disease pathology in MS. Mult. Scler. Relat. Disord. 2019, 31, 12–21. [Google Scholar] [CrossRef]
- Morell, P.; Quarles, R.H. The myelin sheath. In Basic Neurochemistry: Molecular, Cellular and Medical Aspects, 6th ed.; Lippincott-Raven: Philadelphia, PA, USA, 1999. [Google Scholar]
- Mathieu, P.A.; Gubiani, M.F.A.; Rodríguez, D.; Pinto, L.I.G.; Calcagno, M.D.L.; Adamo, A.M. Demyelination-remyelination in the Central Nervous System: Ligand-dependent Participation of the Notch Signaling Pathway. Toxicol. Sci. 2019, 171, 172–192. [Google Scholar] [CrossRef]
- Deisenhammer, F.; Zetterberg, H.; Fitzner, B.; Zettl, U.K. The Cerebrospinal Fluid in Multiple Sclerosis. Front. Immunol. 2019, 10, 726. [Google Scholar] [CrossRef]
- Levi, I.; Gurevich, M.; Perlman, G.; Magalashvili, D.; Menascu, S.; Bar, N.; Godneva, A.; Zahavi, L.; Chermon, D.; Kosower, N.; et al. Potential role of indolelactate and butyrate in multiple sclerosis revealed by integrated microbiome-metabolome analysis. Cell Rep. Med. 2021, 2, 100246. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 20 August 2023).
- Harbo, H.F.; Gold, R.; Tintoré, M. Sex and gender issues in multiple sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237–248. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metabolites | Mean (±SD) MS (μg/mL) | Mean (±SD) C (μg/mL) | p-Value |
|---|---|---|---|
| Arginine | 3.9708 (±1.4863) | 5.2351 (±1.9583) | 0.0037 |
| Histidine | 7.0202 (±1.6554) | 8.1648 (±1.7159) | 0.0058 |
| Spermidine | 0.0367 (±0.01111) | 0.0313 (±0.0059) | 0.0124 |
| Glutamate | 1.8883 (±0.3890) | 2.1190 (±0.3840) | 0.0145 |
| Choline | 1.0436 (±0.2841) | 1.2276 (±0.3691) | 0.0233 |
| Tyrosine | 1.1032 (±0.2936) | 1.2527 (±0.2786) | 0.0313 |
| Serine | 2.2714 (±0.7321) | 2.5920 (±0.6051) | 0.0473 |
| Linoleic acid | 3.1304 (±0.277) | 3.3933 (±0.228) | 0.001 |
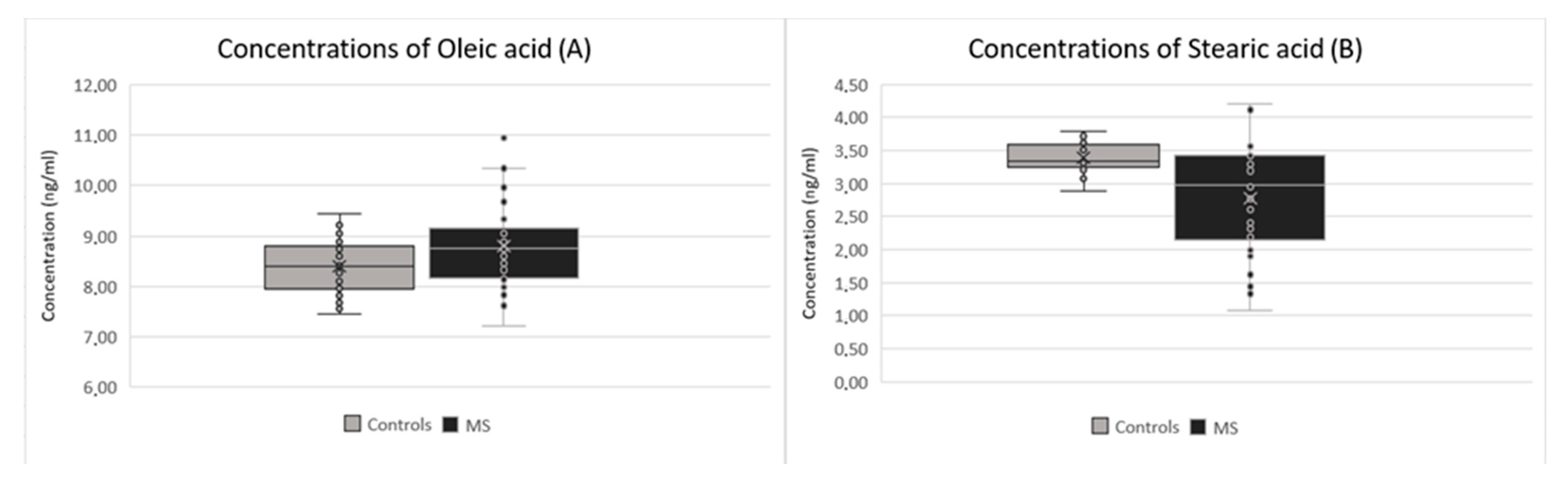
| Oleic acid | 8.797 (±0.824) | 8.393 (±0.523) | 0.015 |
| Stearic acid | 2.7739 (±0.825) | 3.1582 (±0.623) | 0.029 |
| Metabolites | Mean (±SD) MS | Mean (±SD) C | p-Value |
|---|---|---|---|
| Methionine | 8504.86 (±2293.06) | 6256.73 (±896.85) | <0.001 |
| Homovanillic acid | 25,611.18 (±6850.19) | 29,774.24 (±8085.84) | 0.024 |
| Threonine | 8363.92 (±2797.24) | 9587.38 (±2447.98) | 0.053 |
| Uridine | 54,333.68 (±37,916.23) | 73,550.91 (±46,254.03) | 0.063 |
| Oxoglutaric acid | 3671.48 (±585.98) | 3466.02 (±400.76) | 0.086 |
| Serotonin | 72,399.12 (±103,619.34) | 36,146.67 (±70,506.17) | 0.086 |
| Biotin | 18,633.25 (±10,638.00) | 23,614.50 (±14,333.83) | 0.106 |
| Palmitoleic acid | 16,785.92 (±2676.63) | 15,807.12 (±2426.12) | 0.111 |
| Dopamine | 7914.79 (±2566.33) | 8832.67 (±2475.26) | 0.130 |
| Adipic acid | 93,639.30 (±19,305.67 | 98,516.06 (±10,593.10) | 0.185 |
| Creatine | 414,855.54 (±100,129.74) | 444,733.33 (±98,329.90) | 0.210 |
| Tryptophane | 75,840.66 (±12,870.37) | 71,938.48 (±13,716.55) | 0.223 |
| Iso-/leucine | 46,331.37 (±16,522.71) | 50,641.21 (±12,977.94) | 0.223 |
| Adenine | 208,212.43 (±44,745.61) | 219,853.18 (±36,331.27) | 0.231 |
| Alanine | 9162.12 (±2287.16) | 9821.76 (±2585.61) | 0.262 |
| Uric acid | 18,416.67 (±11,654.81) | 16,896.35 (±8212.53) | 0.523 |
| Cystine | 13,257.83 (±969.36) | 13,426.36 (±1277.90) | 0.539 |
| Aspartate | 5438.97 (±918.10) | 5558.92 (±726.05) | 0.541 |
| Palmitic acid | 53,262.32 (±20,906.23) | 54,647.30 (±8844.53) | 0.712 |
| Myristic acid | 4917.08 (±2478.17) | 5009.62 (±1479.14) | 0.847 |
| Metabolites | r EDSS 0 | p-v EDSS 0 | r EDSS 1 | p-v EDSS 1 | r EDSS 2 | p-v EDSS 2 |
|---|---|---|---|---|---|---|
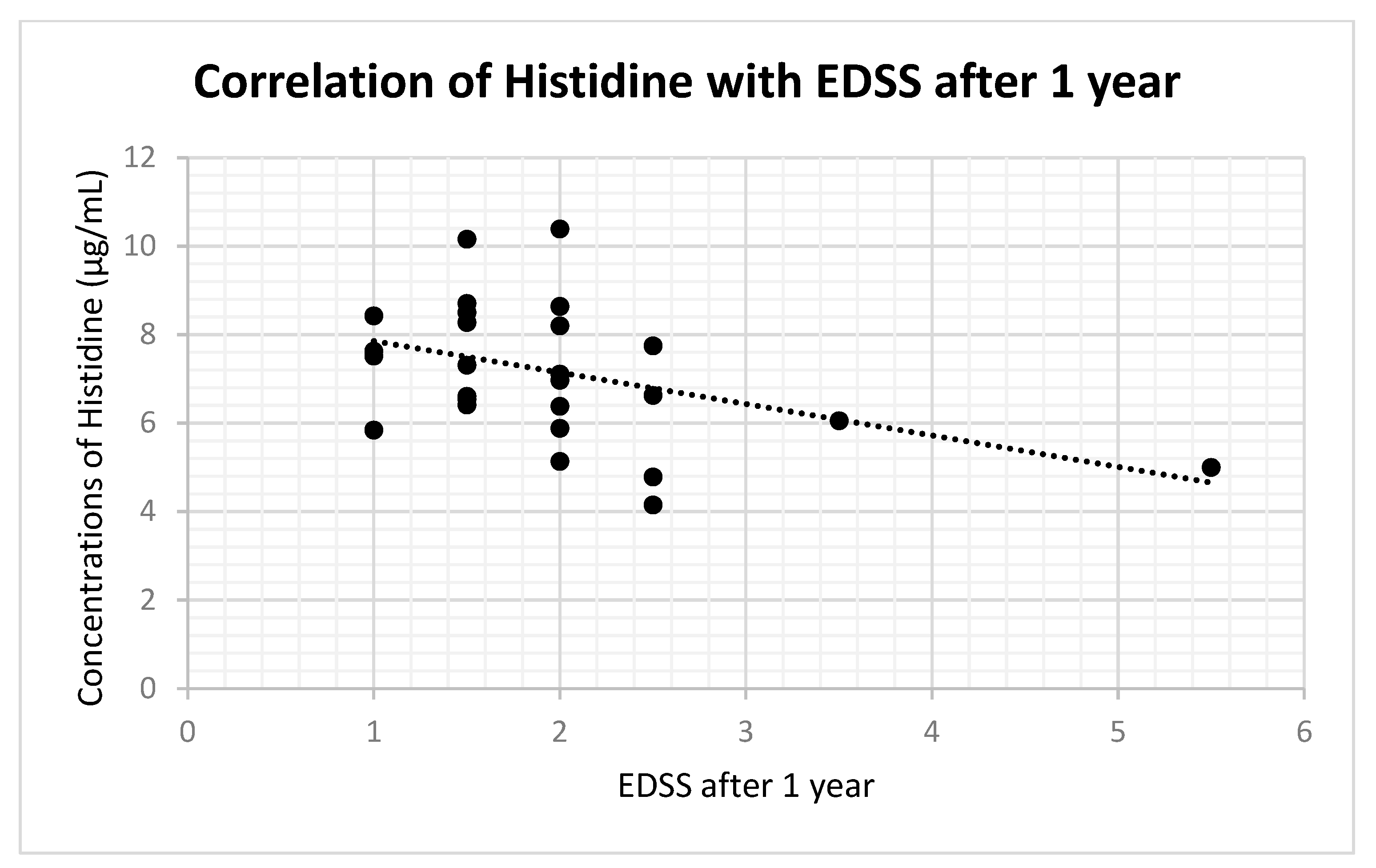
| Histidine | 0.043 | 0.744 | −0.415 | 0.031 | −0.437 | 0.048 |
| Arginine | −0.003 | 0.577 | −0.104 | 0.604 | −0.023 | 0.920 |
| Spermidine | −0.163 | 0.329 | −0.324 | 0.087 | 0.005 | 0.982 |
| Glutamate | −0.212 | 0.202 | −0.066 | 0.736 | 0.099 | 0.670 |
| Choline | −0.161 | 0.168 | −0.288 | 0.130 | 0.080 | 0.729 |
| Tyrosine | −0.177 | 0.288 | −0.125 | 0.519 | 0.034 | 0.883 |
| Serine | −0.150 | 0.375 | −0.066 | 0.733 | 0.042 | 0.857 |
| Oleic a. | −0.056 | 0.740 | −0.202 | 0.292 | −0.036 | 0.877 |
| Stearic a. | −0.202 | 0.224 | −0.051 | 0.792 | 0.369 | 0.100 |
| Linoleic a. | −0.016 | 0.925 | 0.057 | 0.771 | 0.091 | 0.695 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Židó, M.; Kačer, D.; Valeš, K.; Zimová, D.; Štětkářová, I. Metabolomics of Cerebrospinal Fluid Amino and Fatty Acids in Early Stages of Multiple Sclerosis. Int. J. Mol. Sci. 2023, 24, 16271. https://doi.org/10.3390/ijms242216271
Židó M, Kačer D, Valeš K, Zimová D, Štětkářová I. Metabolomics of Cerebrospinal Fluid Amino and Fatty Acids in Early Stages of Multiple Sclerosis. International Journal of Molecular Sciences. 2023; 24(22):16271. https://doi.org/10.3390/ijms242216271
Chicago/Turabian StyleŽidó, Michal, David Kačer, Karel Valeš, Denisa Zimová, and Ivana Štětkářová. 2023. "Metabolomics of Cerebrospinal Fluid Amino and Fatty Acids in Early Stages of Multiple Sclerosis" International Journal of Molecular Sciences 24, no. 22: 16271. https://doi.org/10.3390/ijms242216271
APA StyleŽidó, M., Kačer, D., Valeš, K., Zimová, D., & Štětkářová, I. (2023). Metabolomics of Cerebrospinal Fluid Amino and Fatty Acids in Early Stages of Multiple Sclerosis. International Journal of Molecular Sciences, 24(22), 16271. https://doi.org/10.3390/ijms242216271