
Non-Invasive Assessment of Skin Surface Proteins of Psoriasis Vulgaris Patients in Response to Biological Therapy

 ,
,
Abstract
:1. Introduction
2. Results
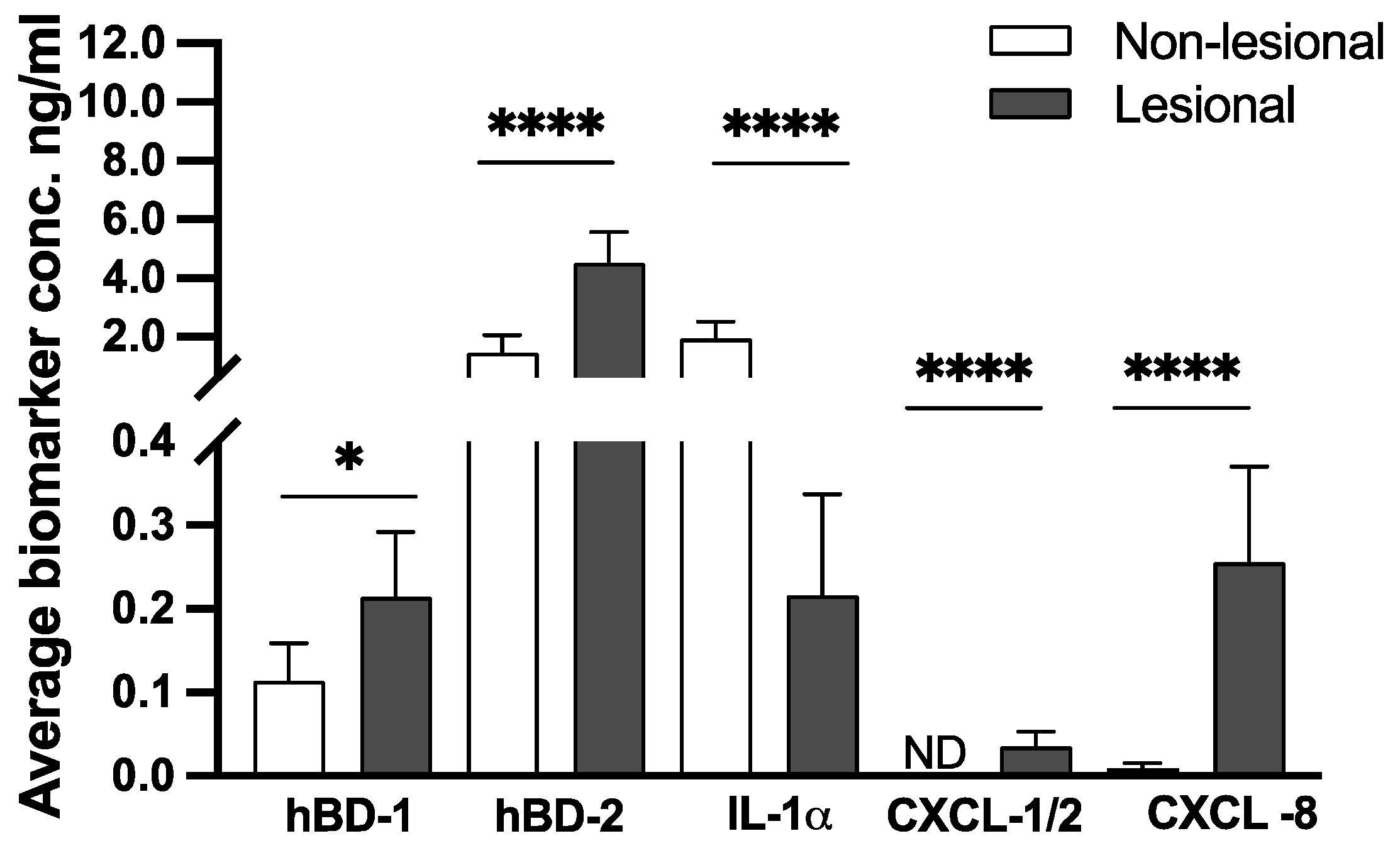
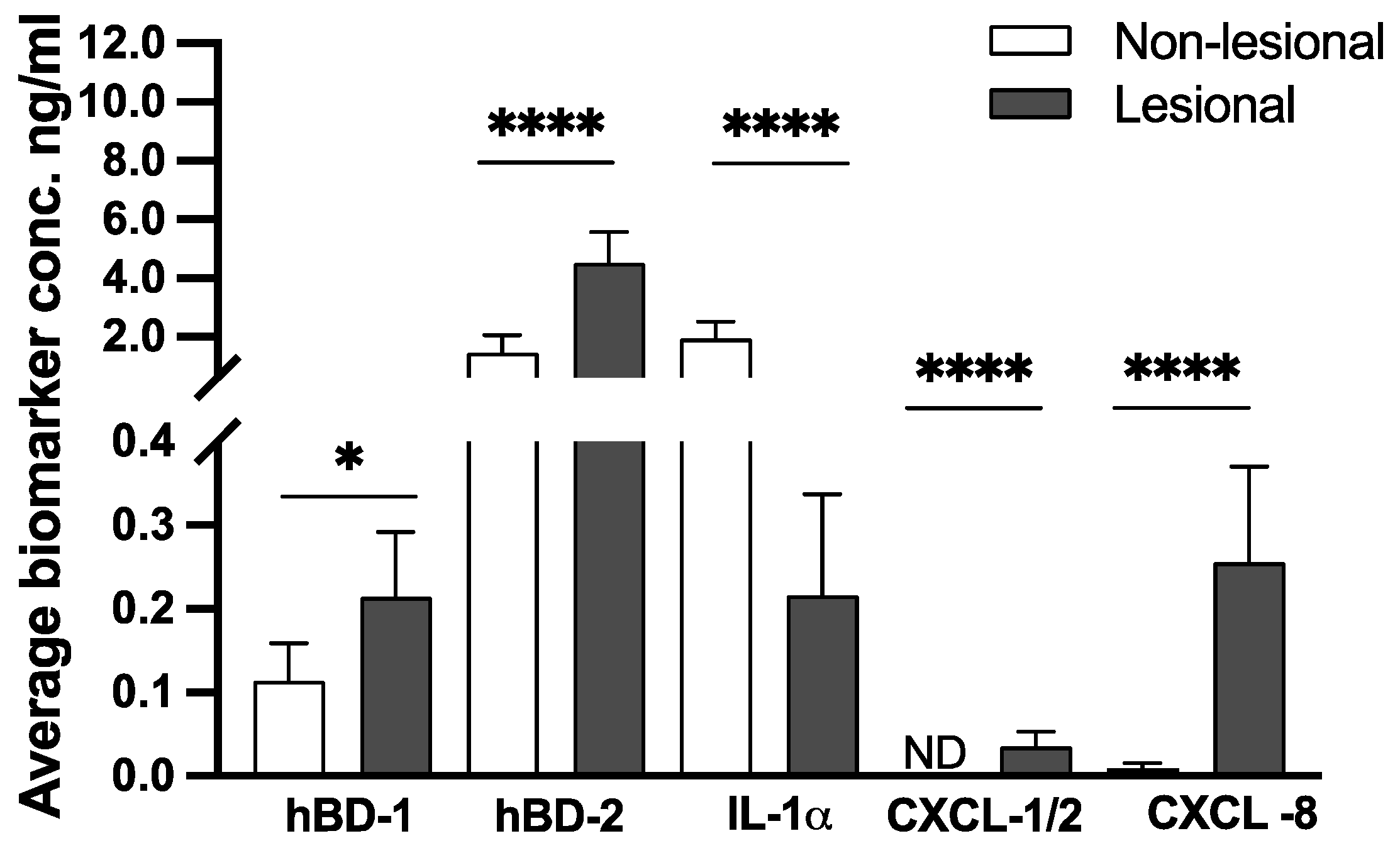
2.1. Human Beta-Defensins and Inflammatory Chemokines CXCL-1/2 and CXCL-8 Are Highly Expressed on the Surface of Psoriatic Lesions
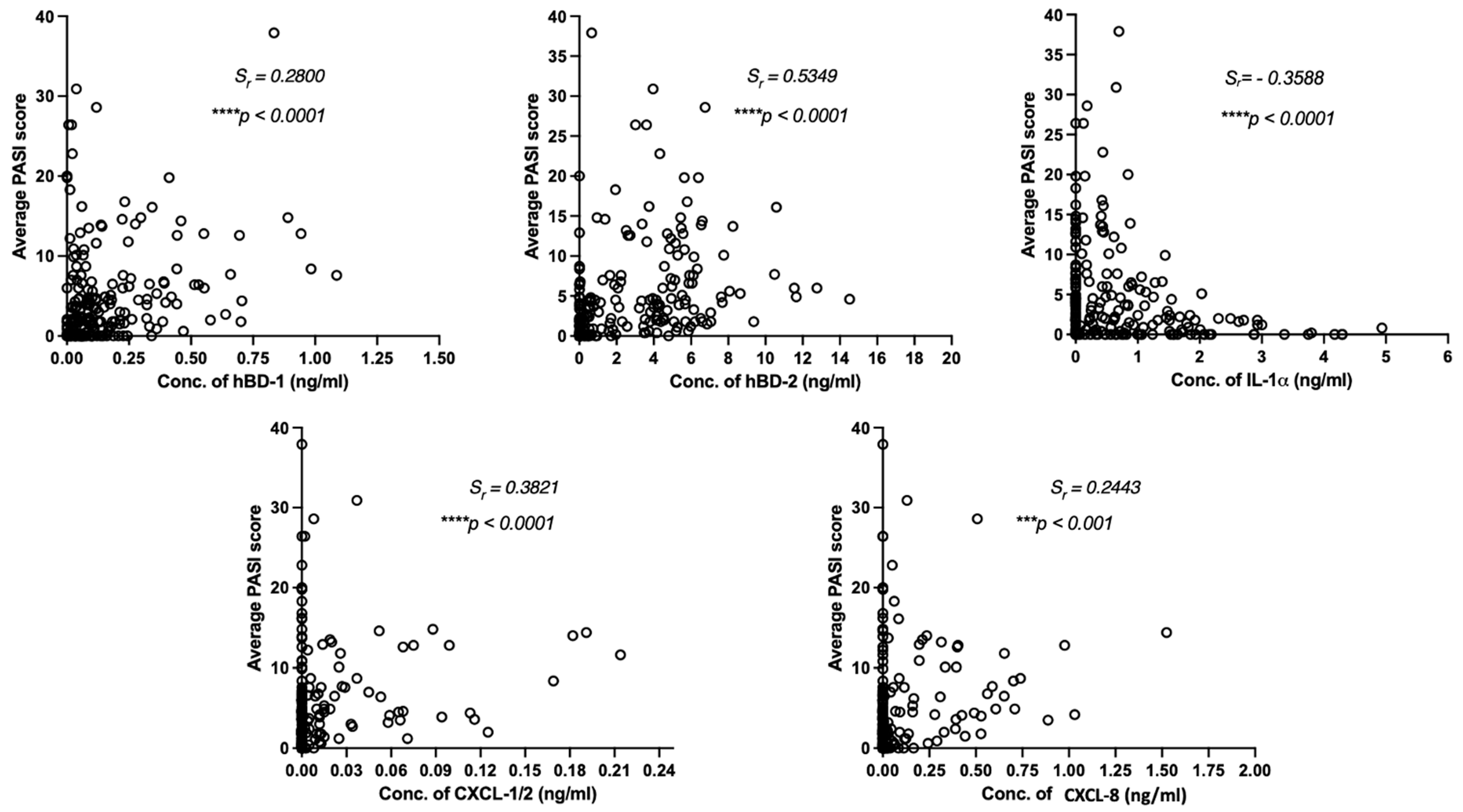
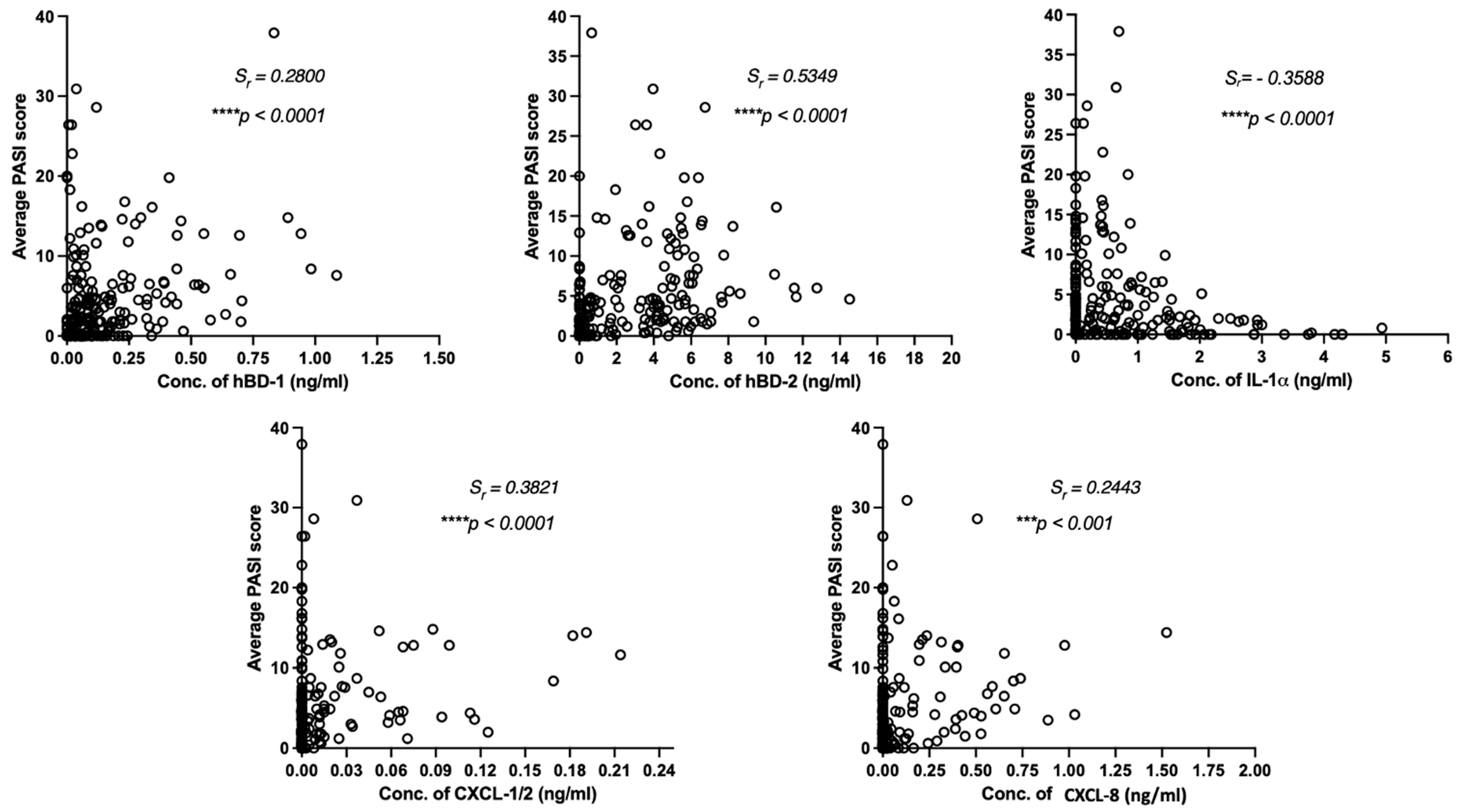
2.2. Psoriasis Area and Severity Index (PASI) and Local Scores of Induration, Desquamation, and Erythema Are Associated with the Levels of Biomarkers Detected on Psoriatic Lesions
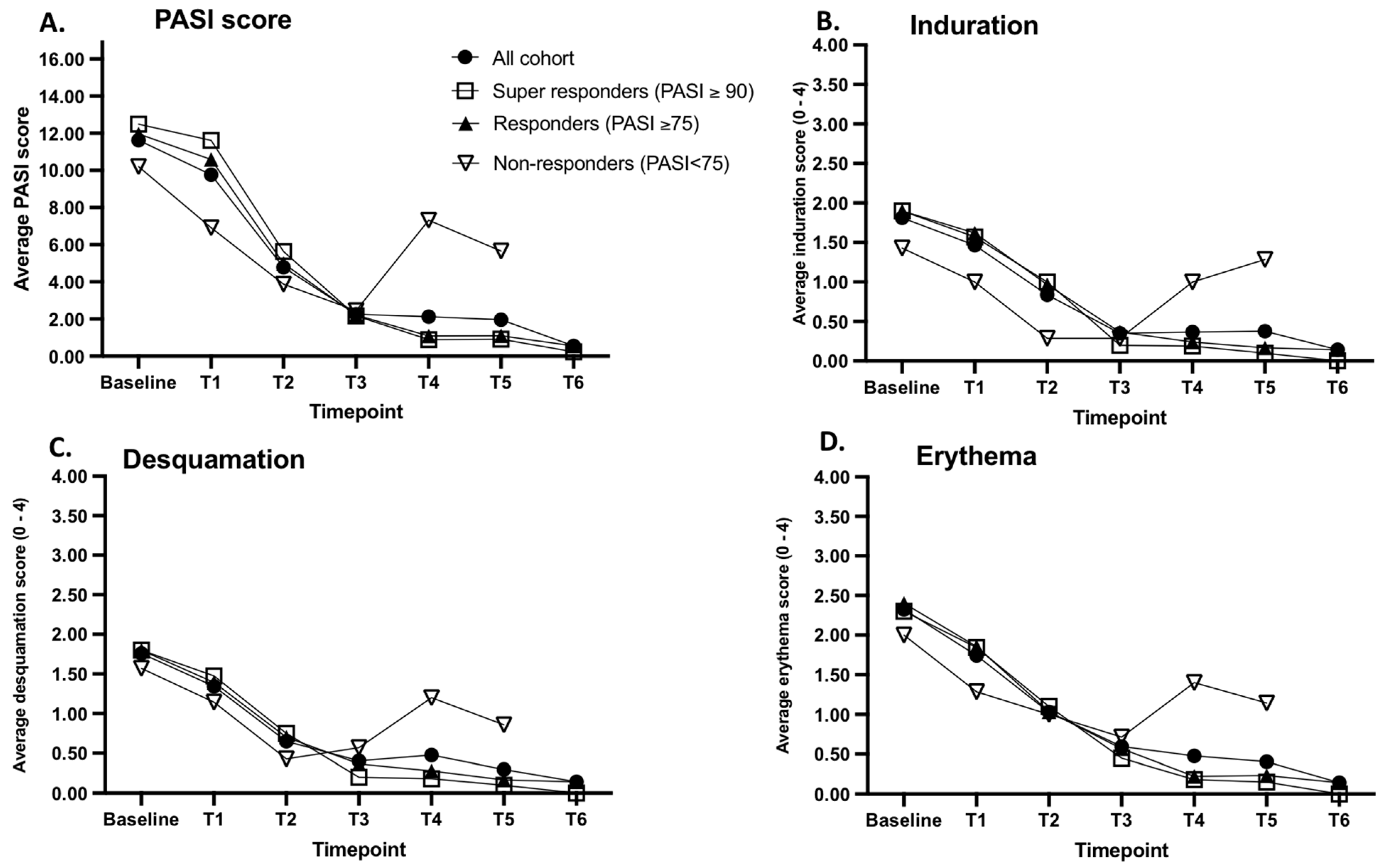
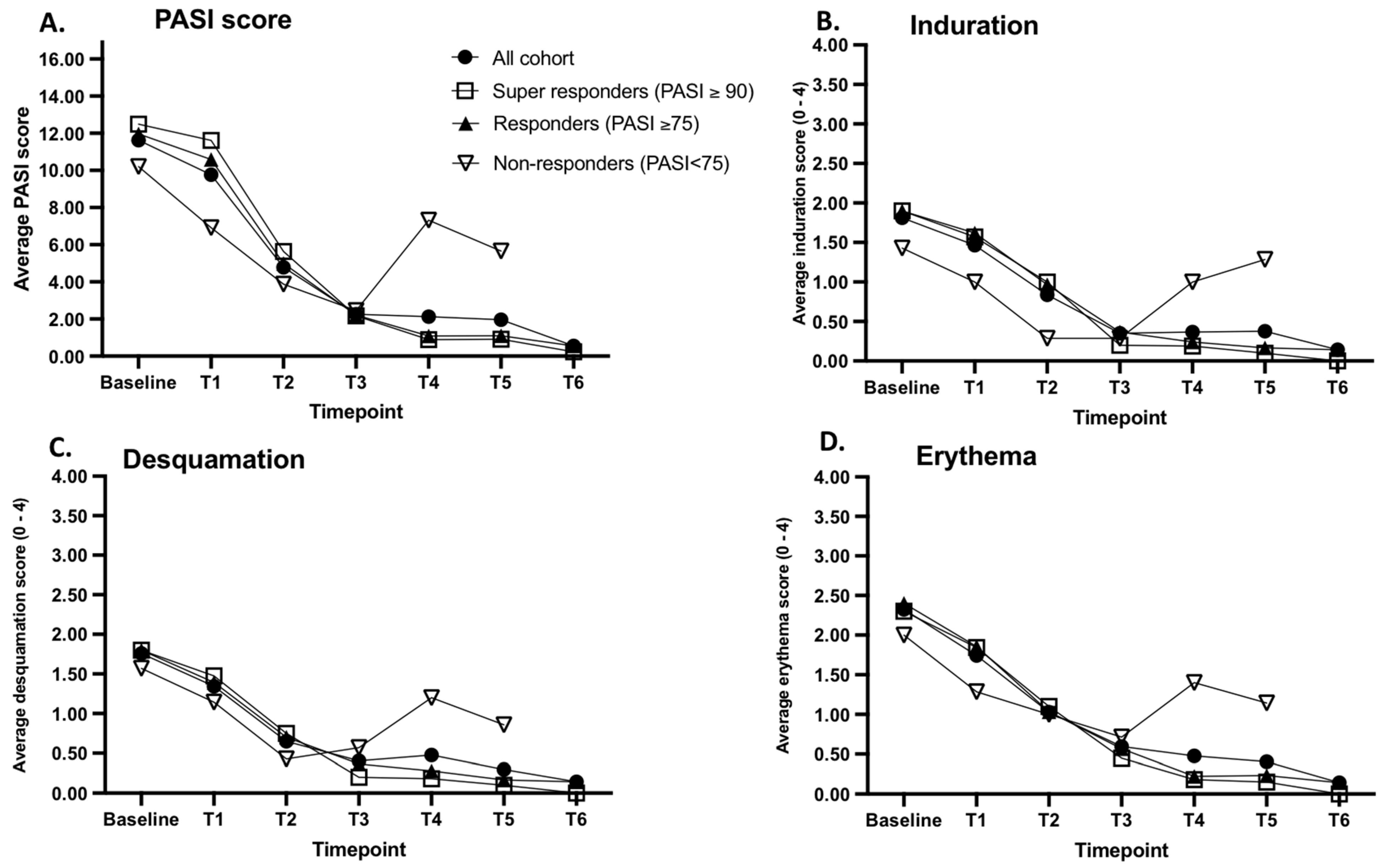
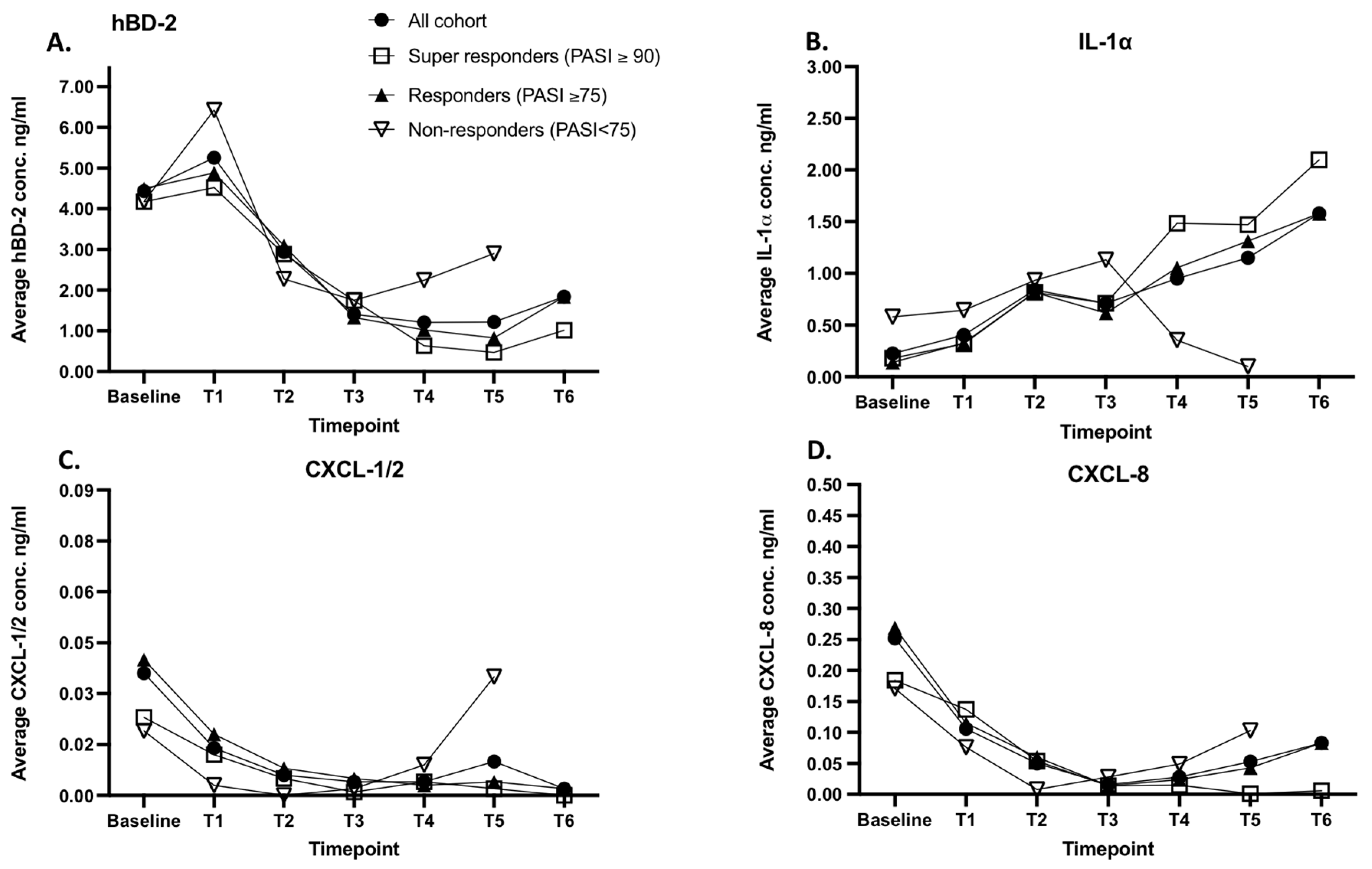
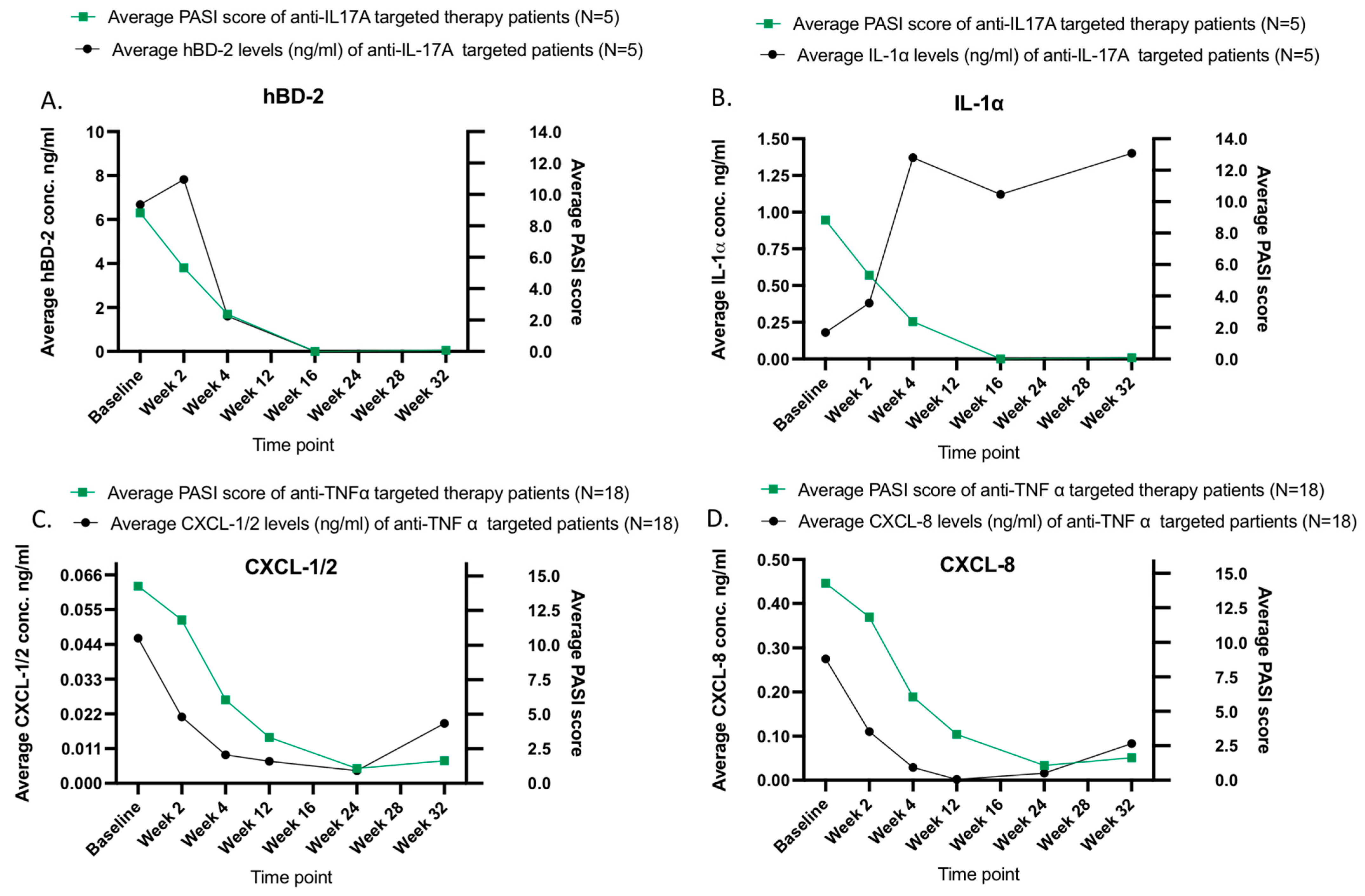
2.3. The Efficacy of Biological Therapy Is Reflected in the Clinical Scores and the Levels of Skin Surface Proteins Detected on Psoriatic Lesions
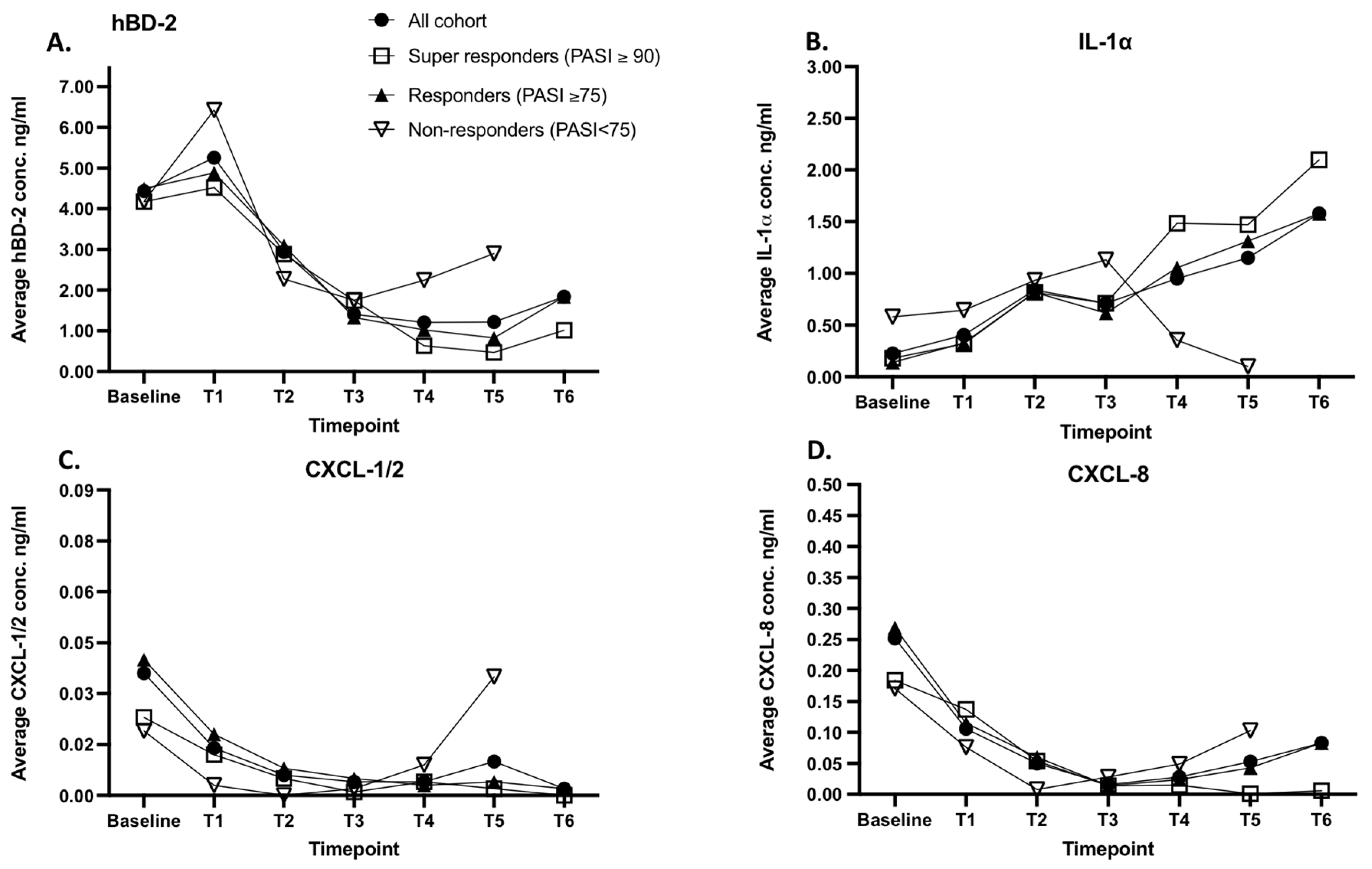
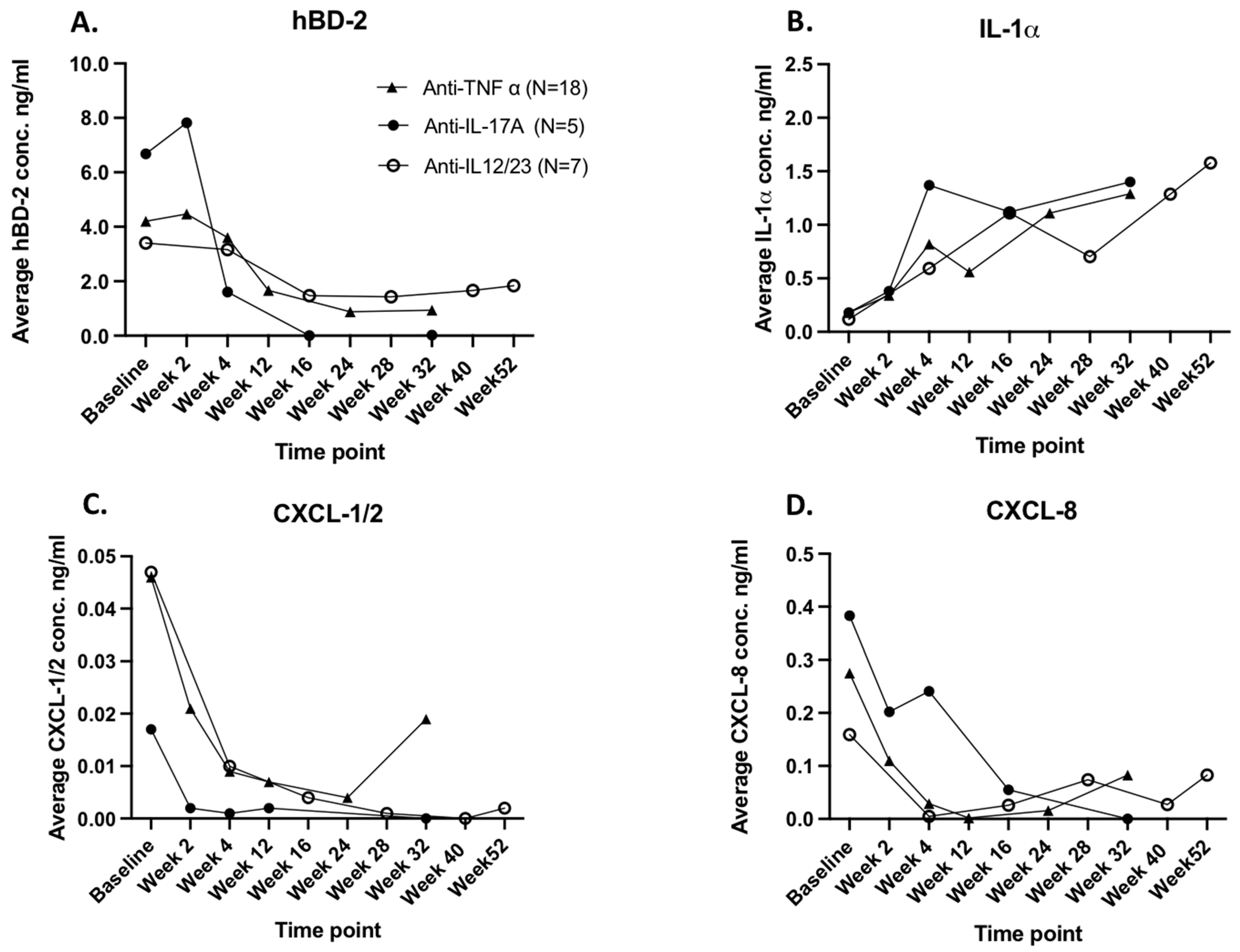
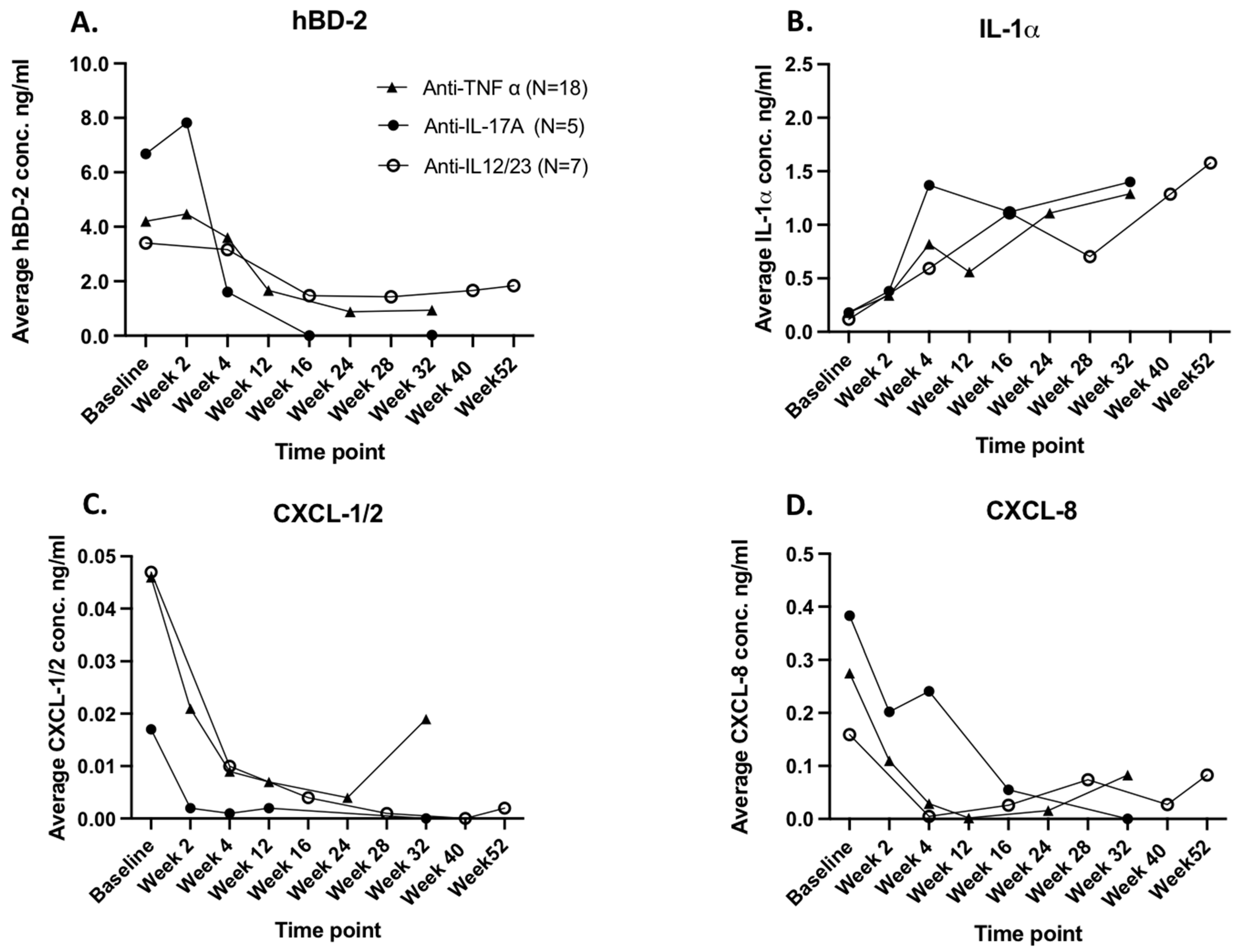
2.4. The Biomarker Response Kinetics to Biological Therapy Is Influenced by Applied Therapeutics
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Transdermal Analysis Patch Measurements and Skin Disease Severity Scores
4.3. Biological Therapy
- Anti-TNF-α-targeted therapy (infliximab (N = 8), and adalimumab (N = 15); Baseline (T0), Week 2 (T1), Week 4 (T2), Week 12 (T3), Week 24 (T4), Week 32 (T5);
- Anti-17A-targeted therapy (secukinumab): Baseline (T0), Week 2 (T1), Week 4 (T2), Week 16 (T3), Week 32 (T5);
- Anti-IL-12/23-targeted therapy (ustekinumab): Baseline (T0), Week 4 (T2), Week 16 (T3), Week 28 (T4), Week 40 (T5), Week 52 (T6).
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boehncke, W.H. Etiology and pathogenesis of psoriasis. Rheum. Dis. Clin. 2015, 41, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Troxel, A.B.; Lewis, J.D.; Kurd, S.K.; Shin, D.B.; Wang, X.; Strom, B.L. The risk of mortality in patients with psoriasis: Results from a population-based study. Arch. Dermatol. 2007, 143, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Implications for management. J. Am. Acad. Dermatol. 2017, 76, 393–403. [Google Scholar] [CrossRef]
- Schon, M.P.; Boehncke, W.H.; Brocker, E.B. Psoriasis: Clinical manifestations, pathogenesis and therapeutic perspectives. Discov. Med. 2009, 5, 253–258. [Google Scholar]
- Patel, R.V.; Clark, L.N.; Lebwohl, M.; Weinberg, J.M. Treatments for psoriasis and the risk of malignancy. J. Am. Acad. Dermatol. 2009, 60, 1001–1017. [Google Scholar] [CrossRef]
- Kim, I.H.; West, C.E.; Kwatra, S.G.; Feldman, S.R.; O’Neill, J.L. Comparative efficacy of biologics in psoriasis: A review. Am. J. Clin. Dermatol. 2012, 13, 365–374. [Google Scholar] [CrossRef]
- Laws, P.M.; Young, H.S. Current and emerging systemic treatment strategies for psoriasis. Drugs 2012, 72, 1867–1880. [Google Scholar] [CrossRef]
- Rustin, M.H.A. Long-term safety of biologics in the treatment of moderate-to-severe plaque psoriasis: Review of current data. Br. J. Dermatol. 2012, 167, 3–11. [Google Scholar] [CrossRef]
- Kamata, M.; Tada, Y. Efficacy and safety of biologics for psoriasis and psoriatic arthritis and their impact on comorbidities: A literature review. Int. J. Mol. Sci. 2020, 21, 1690. [Google Scholar] [CrossRef]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef]
- Clinical Review Report. Clinical Review Report: Ixekizumab (Taltz); APPENDIX 6, Validity of Outcome Measures; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2017; Available online: https://www.ncbi.nlm.nih.gov/books/NBK533695/ (accessed on 9 October 2023).
- Jansen, P.A.; Rodijk-Olthuis, D.; Hollox, E.J.; Kamsteeg, M.; Tjabringa, G.S.; de Jongh, G.J.; van Vlijmen-Willems, I.M.J.J.; Bergboer, J.G.M.; van Rossum, M.M.; de Jong, E.M.G.J.; et al. β-Defensin-2 protein is a serum biomarker for disease activity in psoriasis and reaches biologically relevant concentrations in lesional skin. PLoS ONE 2009, 4, e4725. [Google Scholar] [CrossRef]
- Baliwag, J.; Barnes, D.H.; Johnston, A. Cytokines in psoriasis. Cytokine 2015, 73, 342–350. [Google Scholar] [CrossRef]
- Méhul, B.; Laffet, G.; Séraïdaris, A.; Russo, L.; Fogel, P.; Carlavan, I.; Voegel, J.J. Noninvasive proteome analysis of psoriatic stratum corneum reflects pathophysiological pathways and is useful for drug profiling. Br. J. Dermatol. 2017, 177, 470–488. [Google Scholar] [CrossRef] [PubMed]
- Chularojanamontri, L.; Charoenpipatsin, N.; Silpa-Archa, N.; Wongpraparut, C.; Thongboonkerd, V. Proteomics in psoriasis. Int. J. Mol. Sci. 2019, 20, 1141. [Google Scholar] [CrossRef] [PubMed]
- Orro, K.; Smirnova, O.; Arshavskaja, J.; Salk, K.; Meikas, A.; Pihelgas, S.; Spee, P. Development of TAP, a non-invasive test for qualitative and quantitative measurements of biomarkers from the skin surface. Biomark. Res. 2014, 2, 20. [Google Scholar] [CrossRef] [PubMed]
- Falcone, D.; Spee, P.; Salk, K.; Peppelman, M.; Van De Kerkhof, P.C.M.; Van Erp, P.E.J. Measurement of skin surface biomakers by transdermal analyses patch following different in vivo models of irritation: A pilot study. Skin Res. Technol. 2017, 23, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Schaap, M.J.; Bruins, F.M.; He, X.; Orro, K.; Peppelman, M.; van Erp, P.E.; Seyger, M. Skin surface protein detection by transdermal analysis patches in pediatric psoriasis. Skin Pharmacol. Physiol. 2021, 34, 271–280. [Google Scholar] [CrossRef]
- Schaap, M.J.; Bruins, F.M.; van den Brink, N.J.; Orro, K.; Groenewoud, H.M.; de Jong, E.M.; Seyger, M.M. Challenges in noninvasive skin biomarker measurements in daily practice: A longitudinal study on skin surface protein detection by the transdermal analysis patch in pediatric psoriasis. Skin Pharmacol. Physiol. 2022, 35, 319–327. [Google Scholar] [CrossRef]
- Orro, K.; Salk, K.; Abram, K.; Arshavskaja, J.; Meikas, A.; Karelson, M.; Spee, P. Assessment of soluble skin surface protein levels for monitoring psoriasis vulgaris in adult psoriasis patients using non-invasive transdermal analysis patch: A pilot study. Front. Med. 2023, 10, 1072160. [Google Scholar] [CrossRef] [PubMed]
- Carlin, C.S.; Feldman, S.R.; Krueger, J.G.; Menter, A.; Krueger, G.G. A 50% reduction in the Psoriasis Area and Severity Index (PASI 50) is a clinically significant endpoint in the assessment of psoriasis. J. Am. Acad. Dermatol. 2004, 50, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Daugaard, C.; Iversen, L.; Hjuler, K.F. Comorbidity in adult psoriasis: Considerations for the clinician. Psoriasis Targets Ther. 2022, 12, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Iznardo, H.; Puig, L. IL-1 family cytokines in inflammatory dermatoses: Pathogenetic role and potential therapeutic implications. Int. J. Mol. Sci. 2022, 23, 9479. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.; Zhang, M.F.; Liao, P.Y.; Wang, T.T.; Li, S.J.; Fan, Y.M.; Zhu, K.J. Lack of association between CARD10/CARMA3 tag SNPs and psoriasis vulgaris in the southern Chinese population. Genet. Mol. Res. 2017, 16, gmr16019025. [Google Scholar] [CrossRef]
- Villarino, A.V.; Kanno, Y.; O’Shea, J.J. Mechanisms and consequences of Jak–STAT signaling in the immune system. Nat. Immunol. 2017, 18, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Palomino, D.C.T.; Marti, L.C. Chemokines and immunity. Einstein 2015, 13, 469–473. [Google Scholar] [CrossRef]
- Zdanowska, N.; Kasprowicz-Furmańczyk, M.; Placek, W.; Owczarczyk-Saczonek, A. The role of chemokines in psoriasis—An overview. Medicina 2021, 57, 754. [Google Scholar] [CrossRef]
- Chieosilapatham, P.; Ogawa, H.; Niyonsaba, F. Current insights into the role of human β-defensins in atopic dermatitis. Clin. Exp. Immunol. 2017, 190, 155–166. [Google Scholar] [CrossRef]
- Tingting Jin, T.; Sun, Z.; Chen, X.; Wang, Y.; Li, R.; Ji, S.; Zhao, Y. Serum human beta-defensin-2 is a possible biomarker for monitoring response to JAK inhibitor in psoriasis patients. Dermatology 2017, 233, 164–169. [Google Scholar]
- Kolbinger, F.; Loesche, C.; Valentin, M.A.; Jiang, X.; Cheng, Y.; Jarvis, P.; Patel, D.D. β-Defensin 2 is a responsive biomarker of IL-17A—Driven skin pathology in patients with psoriasis. J. Allergy Clin. Immunol. 2017, 139, 923–932. [Google Scholar] [CrossRef]
- Hulshof, L.; Hack, D.P.; Hasnoe, Q.C.J.; Dontje, B.; Jakasa, I.; Riethmüller, C.; Middelkamp-Hup, M.A. A minimally invasive tool to study immune response and skin barrier in children with atopic dermatitis. Br. J. Dermatol. 2019, 180, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Tarentini, E.; Odorici, G.; Righi, V.; Paganelli, A.; Giacomelli, L.; Mirisola, V.; Magnoni, C. Integrated metabolomic analysis and cytokine profiling define clusters of immuno-metabolic correlation in new-onset psoriasis. Sci. Rep. 2021, 11, 10472. [Google Scholar] [CrossRef] [PubMed]
- Røpke, M.A.; Mekulova, A.; Pipper, C.; Eisen, M.; Pender, K.; Spee, P.; Kezic, S. Non-invasive assessment of soluble skin surface biomarkers in atopic dermatitis patients—Effect of treatment. Skin Res Technol. 2021, 27, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Boraschi, D.; Tagliabue, A. The interleukin-1 receptor family. In Seminars in Immunology; Academic Press: Cambridge, MA, USA, 2013; Volume 25, pp. 394–407. [Google Scholar]
- Lebwohl, M.; Christophers, E.; Langley, R.; Ortonne, J.P.; Roberts, J.; Griffiths, C.E. An international, randomized, double-blind, placebo-controlled phase 3 trial of intramuscular alefacept in patients with chronic plaque psoriasis. Arch. Dermatol. 2003, 139, 719–727. [Google Scholar] [CrossRef]
- Langley, R.G.; Elewski, B.E.; Lebwohl, M.; Reich, K.; Griffiths, C.E.; Papp, K.; Papavassilis, C. Secukinumab in plaque psoriasis—Results of two phase 3 trials. N. Engl. J. Med. 2014, 371, 326–338. [Google Scholar] [CrossRef]
- Ten Bergen, L.L.; Petrovic, A.; Krogh Aarebrot, A.; Appel, S. The TNF/IL-23/IL-17 axis—Head-to-head trials comparing different biologics in psoriasis treatment. Scand. J. Immunol. 2020, 92, e12946. [Google Scholar] [CrossRef]
- Hong, J.J.; Hadeler, E.K.; Mosca, M.L.; Brownstone, N.D.; Bhutani, T.; Liao, W.J. TNF-alpha inhibitors and ustekinumab for the treatment of psoriasis: Therapeutic utility in the era of IL-17 and IL-23 inhibitors. J. Psoriasis Psoriatic Arthritis 2022, 7, 79–92. [Google Scholar] [CrossRef]
- Nast, A.; Smith, C.; Spuls, P.I.; Avila Valle, G.; Bata-Csörgö, Z.; Bogdanov, I.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; et al. Euroguiderm Guideline for the Systemic Treatment of Psoriasis Vulgaris. February 2022. Available online: https://www.guidelines.edf.one//uploads/attachments/cl27nt7yb001q90jnmykcah83-euroguiderm-pso-gl-feb-2022.pdf (accessed on 9 October 2023).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Induration | Desquamation | Erythema | |||
|---|---|---|---|---|---|---|
| Sr | p | Sr | p | Sr | p | |
| hBD-1 | 0.0004 | p *** = 0.0004 | 0.217 | p ** = 0.0015 | 0.2722 | p **** < 0.0001 |
| hBD-2 | 0.4863 | p **** < 0.0001 | 0.4821 | p **** < 0.0001 | 0.5165 | p **** < 0.0001 |
| IL-1a | −0.4589 | p **** < 0.0001 | −0.4417 | p **** < 0.0001 | −0.4401 | p **** < 0.0001 |
| CXCL-1/2 | 0.4854 | p **** < 0.0001 | 0.3679 | p **** < 0.0001 | 0.4591 | p **** < 0.0001 |
| CXCL-8 | 0.3401 | p **** < 0.0001 | 0.2564 | p *** = 0.0002 | 0.3786 | p **** < 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orro, K.; Salk, K.; Merkulova, A.; Abram, K.; Karelson, M.; Traks, T.; Neuman, T.; Spee, P.; Kingo, K. Non-Invasive Assessment of Skin Surface Proteins of Psoriasis Vulgaris Patients in Response to Biological Therapy. Int. J. Mol. Sci. 2023, 24, 16248. https://doi.org/10.3390/ijms242216248
Orro K, Salk K, Merkulova A, Abram K, Karelson M, Traks T, Neuman T, Spee P, Kingo K. Non-Invasive Assessment of Skin Surface Proteins of Psoriasis Vulgaris Patients in Response to Biological Therapy. International Journal of Molecular Sciences. 2023; 24(22):16248. https://doi.org/10.3390/ijms242216248
Chicago/Turabian StyleOrro, Kadri, Kristiina Salk, Anna Merkulova, Kristi Abram, Maire Karelson, Tanel Traks, Toomas Neuman, Pieter Spee, and Külli Kingo. 2023. "Non-Invasive Assessment of Skin Surface Proteins of Psoriasis Vulgaris Patients in Response to Biological Therapy" International Journal of Molecular Sciences 24, no. 22: 16248. https://doi.org/10.3390/ijms242216248
APA StyleOrro, K., Salk, K., Merkulova, A., Abram, K., Karelson, M., Traks, T., Neuman, T., Spee, P., & Kingo, K. (2023). Non-Invasive Assessment of Skin Surface Proteins of Psoriasis Vulgaris Patients in Response to Biological Therapy. International Journal of Molecular Sciences, 24(22), 16248. https://doi.org/10.3390/ijms242216248