
The Liver in Heart Failure: From Biomarkers to Clinical Risk
 , ,
, , 

Abstract
:1. Introduction
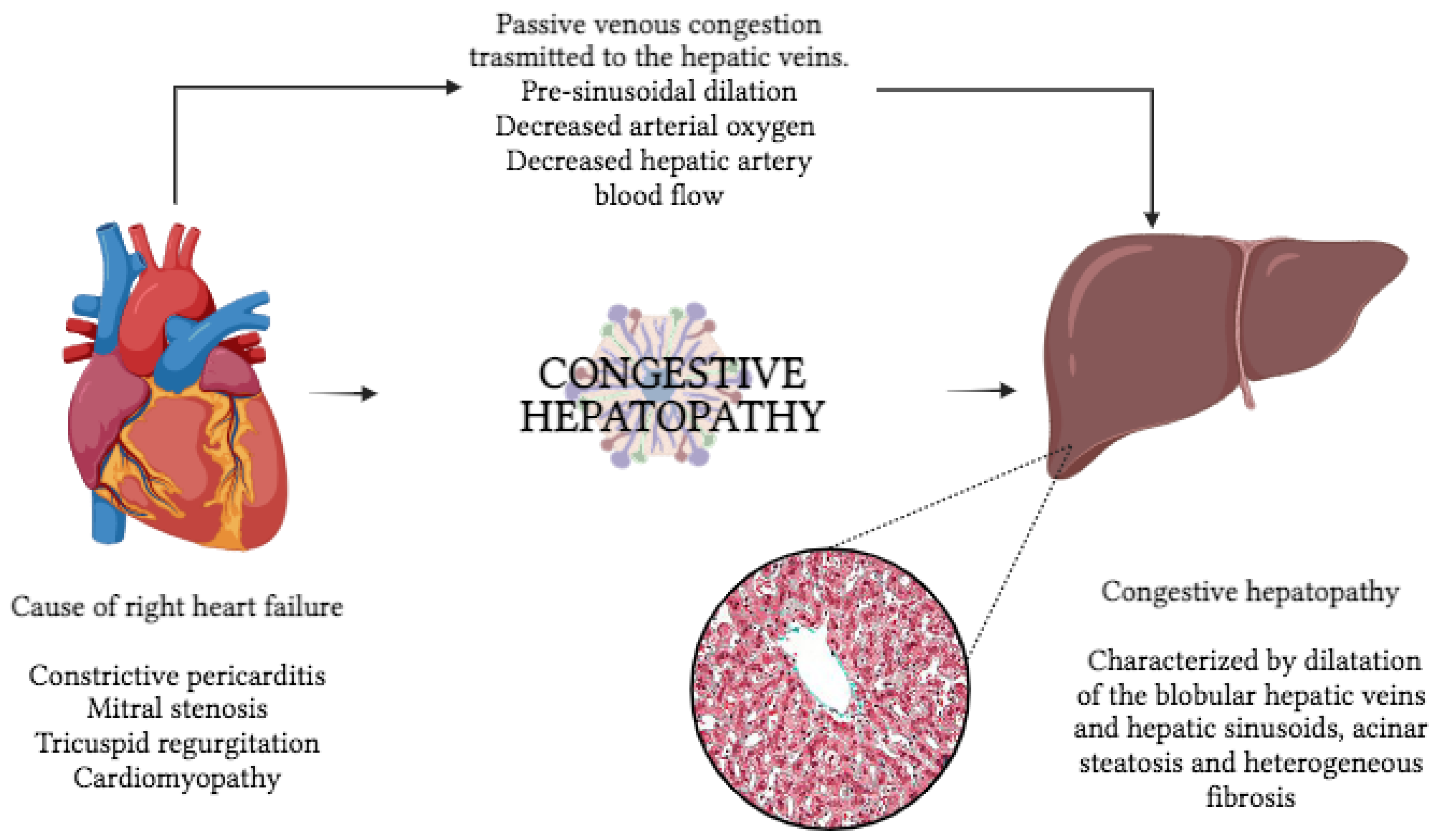
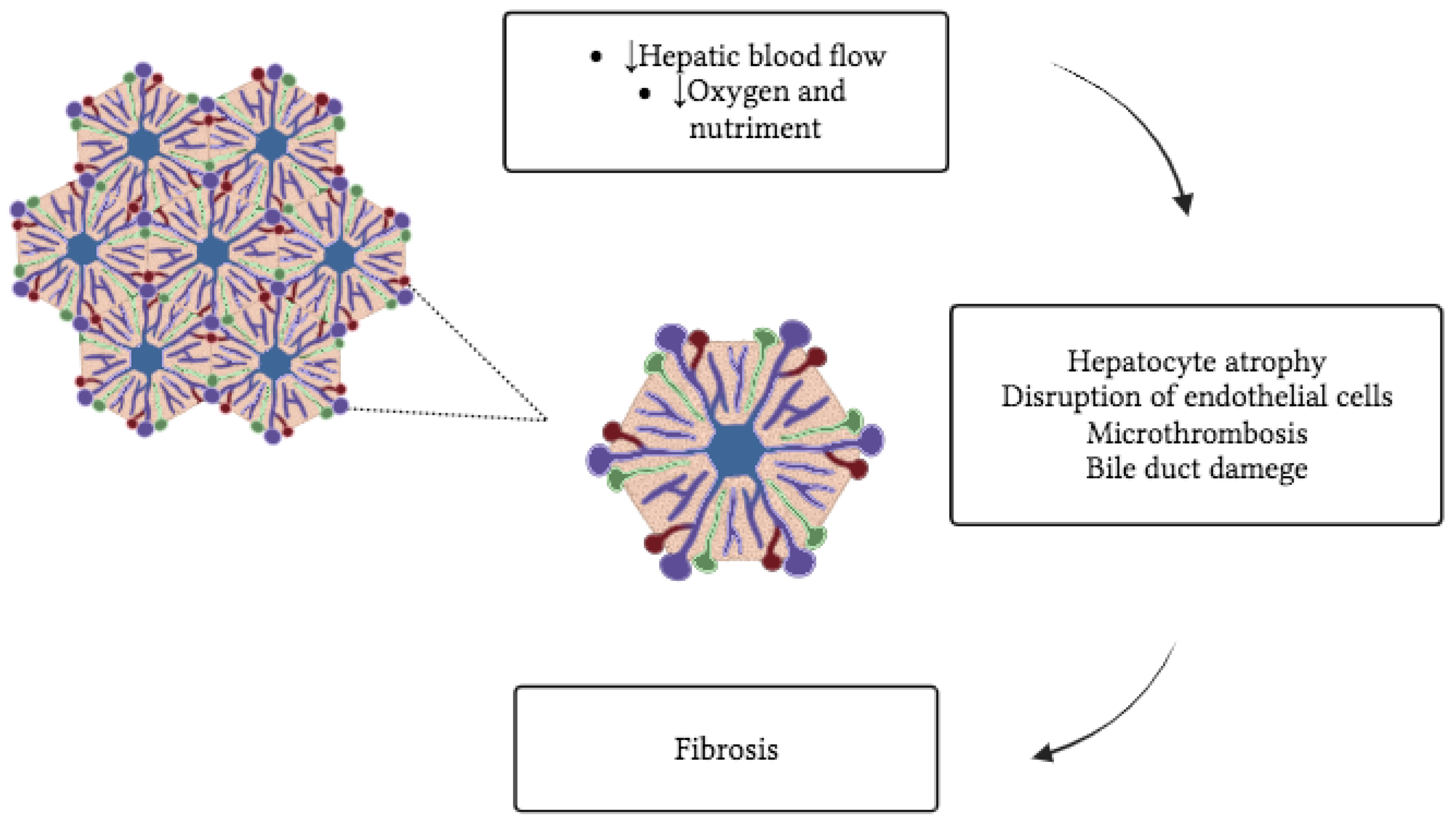
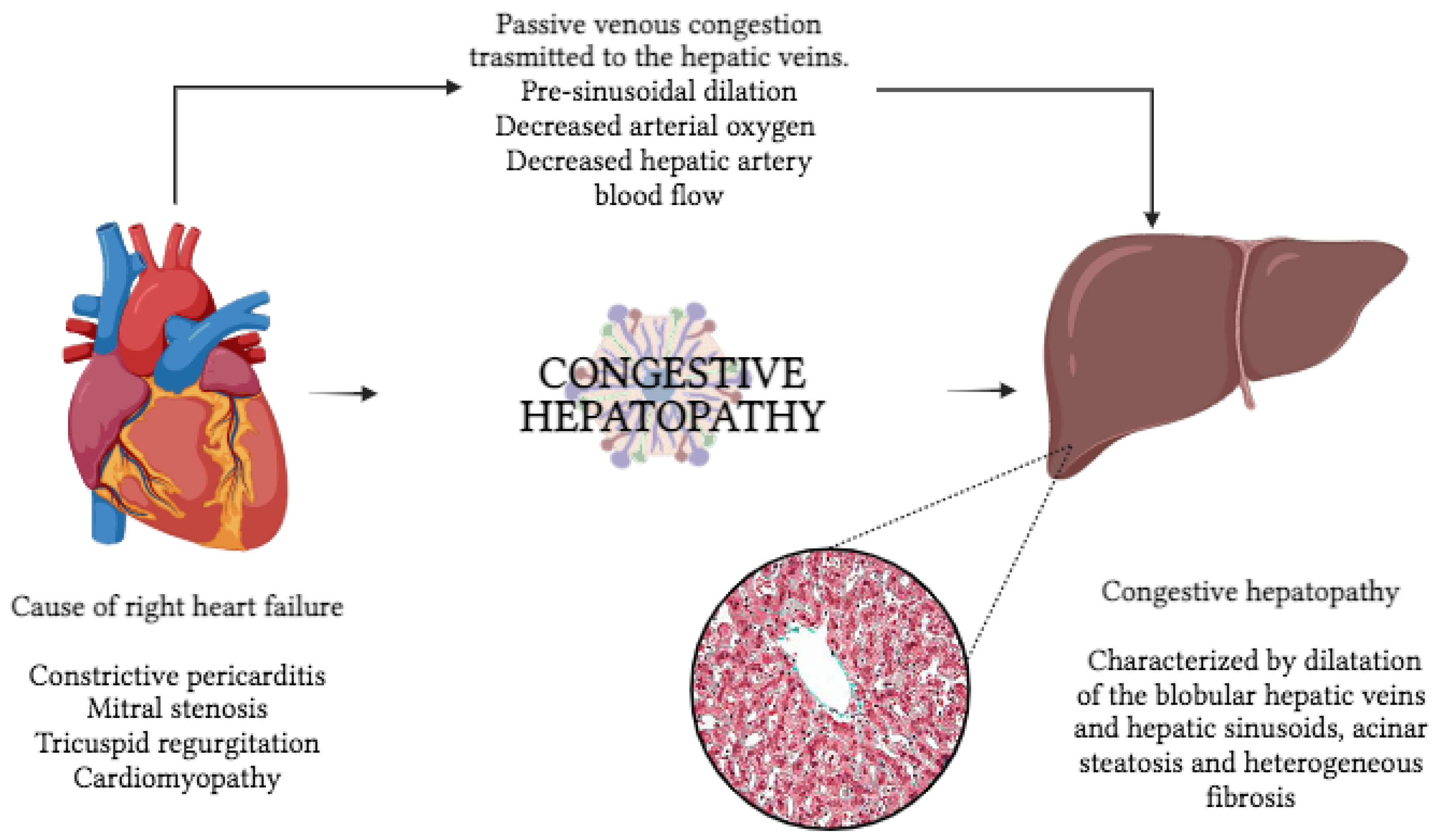
2. Liver in Heart Failure
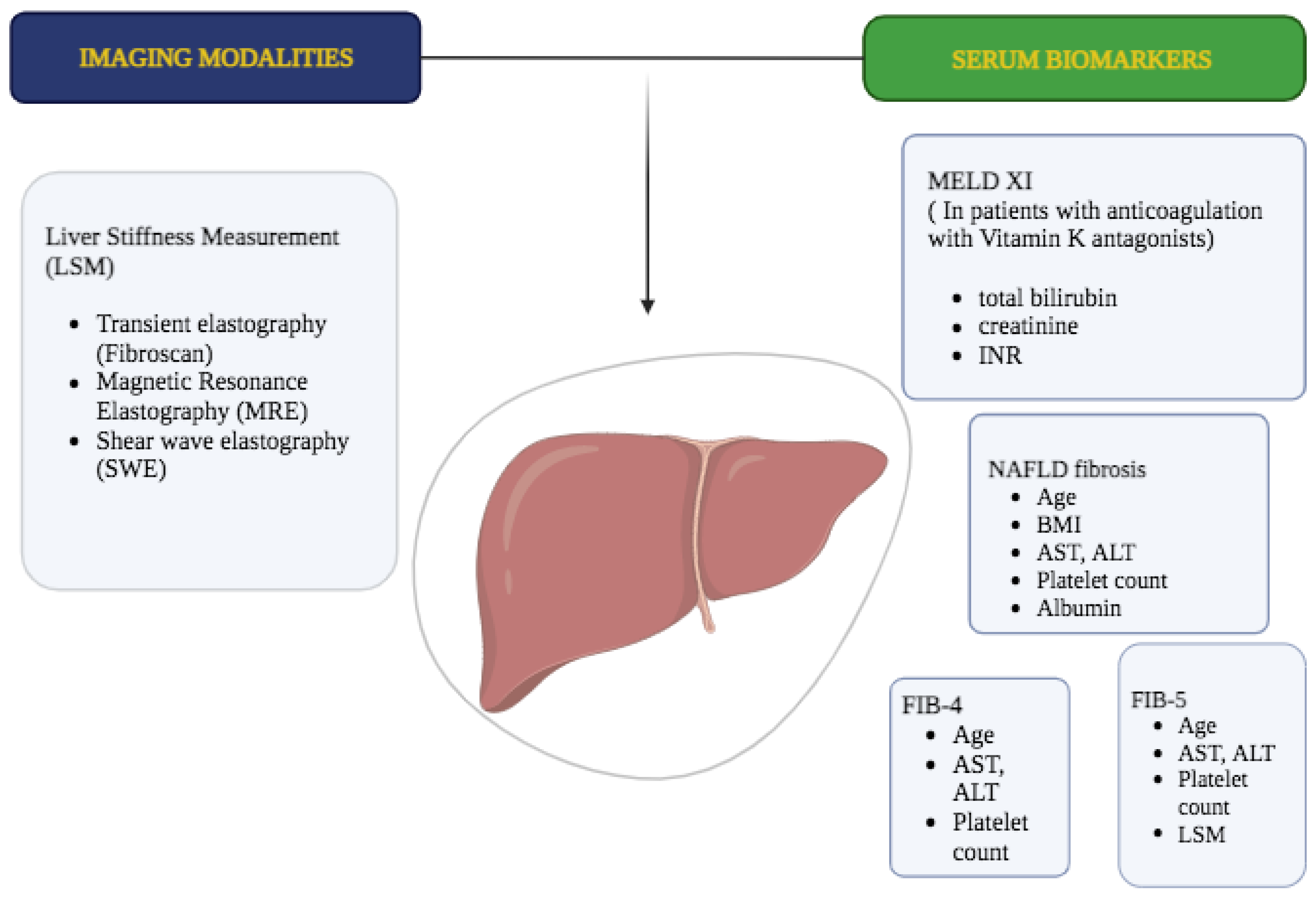
3. Liver Biomarkers as Diagnostic and Prognostic Tools in Heart Diseases
4. Correlation between Non-Invasive Measurement of CVP and LSM
5. Elastography Can Demonstrate Decongestion in Patients with Heart Failure
6. Correlation between LSM and Adverse Outcomes in HF Patients
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e578. [Google Scholar] [CrossRef] [PubMed]
- Gorter, T.M.; van Veldhuisen, D.J.; Bauersachs, J.; Borlaug, B.A.; Celutkiene, J.; Coats, A.J.; Crespo-Leiro, M.G.; Guazzi, M.; Harjola, V.-P.; Heymans, S.; et al. Right heart dysfunction and failure in heart failure with preserved ejection fraction: Mechanisms and management. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Garriz, I.; Olalla-Gómez, C.O.-G.; Garrote, C.; López-Benito, M.L.-B.; Martín, J.M.; Alonso, D.; Rodríguez, M.A.R. Contribution of right ventricular dysfunction to heart failure mortality: A meta-analysis. Rev. Cardiovasc. Med. 2012, 13, e62. [Google Scholar] [CrossRef] [PubMed]
- Gorter, T.M.; Hoendermis, E.S.; Van Veldhuisen, D.J.; Voors, A.A.; Lam, C.S.P.; Geelhoed, B.; Willems, T.P.; Van Melle, J.P. Right ventricular dysfunction in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Eur. J. Heart Fail. 2016, 18, 1472. [Google Scholar] [CrossRef]
- Giallourakis, C.C.; Rosenberg, P.M.; Friedman, L.S. The liver in heart failure. Clin. Liver Dis. 2002, 6, 947. [Google Scholar] [CrossRef]
- Hilscher, M.; Sanchez, W. Congestive hepatopathy. Clin. Liver Dis. 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Xanthopoulos, A.; Starling, R.C.; Kitai, T.; Triposkiadis, F. Heart Failure and Liver Disease: Cardiohepatic Interactions. JACC Heart Fail. 2019, 7, 87. [Google Scholar] [CrossRef]
- Sherlock, S. The liver in heart failure; relation of anatomical, functional, and circulatory changes. Br. Heart J. 1951, 13, 273. [Google Scholar] [CrossRef]
- Safran, A.P.; Schaffner, F. Chronic passive congestion of the liver in man. Electron microscopic study of cell atrophy and intralobular fibrosis. Am. J. Pathol. 1967, 50, 447. [Google Scholar] [PubMed]
- Lemmer, A.; VanWagner, L.B.; Ganger, D. Assessment of Advanced Liver Fibrosis and the Risk for Hepatic Decompensation in Patients with Congestive Hepatopathy. Hepatology 2018, 68, 1633–1641. [Google Scholar] [CrossRef]
- Moussavian, S.N.; Dincsoy, H.P.; Goodman, S.; Helm, R.A.; Bozian, R.C. Severe hyperbilirubinemia and coma in chronic congestive heart failure. Dig. Dis. Sci. 1982, 27, 175. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.A.; Kaplan, M.M. Left-sided heart failure presenting as hepatitis. Gastroenterology 1978, 74, 583. [Google Scholar] [CrossRef] [PubMed]
- Logan, R.G.; Mowry, F.M.; Judge, R.D. Cardiac failure simulating viral hepatitis. Three cases with serum transaminase levels above 1000. Ann. Intern. Med. 1962, 56, 784. [Google Scholar] [CrossRef] [PubMed]
- Sheer, T.A.; Joo, E.; Runyon, B.A. Usefulness of serum N-terminal-ProBNP in distinguishing ascites due to cirrhosis from ascites due to heart failure. J. Clin. Gastroenterol. 2010, 44, e23. [Google Scholar] [CrossRef]
- Farias, A.Q.; Silvestre, O.M.; Garcia-Tsao, G.; da Costa Seguro, L.F.B.; de Campos Mazo, D.F.; Bacal, F.; Andrade, J.L.; Gonçalves, L.L.; Strunz, C.; Ramos, D.S.; et al. Serum B-type natriuretic peptide in the initial workup of patients with new onset ascites: A diagnostic accuracy study. Hepatology 2014, 59, 1043. [Google Scholar] [CrossRef] [PubMed]
- Wells, M.L.; Fenstad, E.R.; Poterucha, J.T.; Hough, D.M.; Young, P.M.; Araoz, P.A.; Ehman, R.L.; Venkatesh, S.K. Imaging Findings of Congestive Hepatopathy. Radiographics 2016, 36, 1024. [Google Scholar] [CrossRef]
- Ferraioli, G.; Barr, R.G. Ultrasound liver elastography beyond liver fibrosis assessment. World J. Gastroenterol. 2020, 26, 3413. [Google Scholar] [CrossRef]
- Dogan, Y.; Soylu, A.; Kilickesmez, O.; Demirtas, T.; Kilickesmez, K.O.; Dogan, S.N.; Eren, G.; Sevindir, I.; Yasar, N.; Poturoglu, S.; et al. The value of hepatic diffusion-weighted MR imaging in demonstrating hepatic congestion secondary to pulmonary hypertension. Cardiovasc. Ultrasound 2010, 8, 28. [Google Scholar] [CrossRef]
- Nakashima, M.; Nakamura, K.; Nishihara, T.; Ichikawa, K.; Nakayama, R.; Takaya, Y.; Toh, N.; Akagi, S.; Miyoshi, T.; Akagi, T.; et al. Association between Cardiovascular Disease and Liver Disease, from a Clinically Pragmatic Perspective as a Cardiologist. Nutrients 2023, 15, 748. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Björnsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated with Long-term Outcomes of Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef]
- Khalifa, A.; Rockey, D.C. The utility of liver biopsy in 2020. Curr. Opin. Gastroenterol. 2020, 36, 184–191. [Google Scholar] [CrossRef]
- Panel, C.P.; Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M.; European Association for the Study of the Liver; et al. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Coco, B.; Oliveri, F.; Maina, A.M.; Ciccorossi, P.; Sacco, R.; Colombatto, P.; Bonino, F.; Brunetto, M.R. Transient elastography: A new surrogate marker of liver fibrosis influenced by major changes of transaminases. J. Viral Hepat. 2007, 14, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Sagir, A.; Erhardt, A.; Schmitt, M.; Häussinger, D. Transient elastography is unreliable for detection of cirrhosis in patients with acute liver damage. Hepatology 2008, 47, 592–595. [Google Scholar] [CrossRef]
- Miele, L.; Zocco, M.A.; Pizzolante, F.; De Matthaeis, N.; Ainora, M.E.; Liguori, A.; Gasbarrini, A.; Grieco, A.; Rapaccini, G. Use of imaging techniques for non-invasive assessment in the diagnosis and staging of non-alcoholic fatty liver disease. Metabolism 2020, 112, 154355. [Google Scholar] [CrossRef] [PubMed]
- Dhall, D.; Kim, S.A.; Mc Phaul, C.; Kransdorf, E.P.; Kobashigawa, J.A.; Sundaram, V.; Mirocha, J.; Guindi, M. Heterogeneity of Fibrosis in Liver Biopsies of Patients with Heart Failure Undergoing Heart Transplant Evaluation. Am. J. Surg. Pathol. 2018, 42, 1617. [Google Scholar] [CrossRef] [PubMed]
- Bosch, D.E.; Koro, K.; Richards, E.; Hoch, B.L.; Jalikis, F.; Koch, L.K.; Swanson, P.E.; Truong, C.D.; Liou, I.; Yu, L.; et al. Validation of a Congestive Hepatic Fibrosis Scoring System. Am. J. Surg. Pathol. 2019, 43, 766. [Google Scholar] [CrossRef]
- Ophir, J.; Cespedes, I.; Ponnekanti, H.; Yazdi, Y.; Li, X. Elastography: A quantitative method for imaging the elasticity of biological tissues. Ultrason. Imaging 1991, 13, 111. [Google Scholar] [CrossRef]
- Forman, D.E.; Maurer, M.S.; Boyd, C.; Brindis, R.; Salive, M.E.; Horne, F.M.; Bell, S.P.; Fulmer, T.; Reuben, D.B.; Zieman, S.; et al. Multimorbidity in Older Adults with Cardiovascular Disease. J. Am. Coll. Cardiol. 2018, 71, 2149–2161. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Song, M. New Insights into the Pathogenesis of Metabolic-Associated Fatty Liver Disease (MAFLD): Gut-Liver-Heart Crosstalk. Nutrients 2023, 15, 3970. [Google Scholar] [CrossRef]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Heart Fail. Rev. 2022, 27, 625–643. [Google Scholar] [CrossRef] [PubMed]
- Aspromonte, N.; Gulizia, M.M.; Clerico, A.; Di Tano, G.; Emdin, M.; Feola, M.; Iacoviello, M.; Latini, R.; Mortara, A.; Valle, R.; et al. ANMCO/ELAS/SIBioC Consensus Document: Biomarkers in heart failure. Eur. Heart J. Suppl. 2017, 19 (Suppl. D), D102–D112. [Google Scholar] [CrossRef] [PubMed]
- Takae, M.; Fujisue, K.; Yamamoto, E.; Egashira, K.; Komorita, T.; Oike, F.; Nishihara, T.; Yamamoto, M.; Hirakawa, K.; Tabata, N.; et al. Prognostic significance of liver stiffness assessed by fibrosis-4 index in patients with heart failure. ESC Heart Fail. 2021, 8, 3809–3821. [Google Scholar] [CrossRef] [PubMed]
- Maeda, D.; Kanzaki, Y.; Sakane, K.; Tsuda, K.; Akamatsu, K.; Hourai, R.; Okuno, T.; Tokura, D.; Nakayama, S.; Hasegawa, H.; et al. Prognostic value of the liver fibrosis marker fibrosis-5 index in patients with acute heart failure. ESC Heart Fail. 2022, 9, 1380–1387. [Google Scholar] [CrossRef]
- Shirakabe, A.; Okazaki, H.; Matsushita, M.; Shibata, Y.; Shigihara, S.; Nishigoori, S.; Sawatani, T.; Sasamoto, N.; Kiuchi, K.; Atsukawa, M.; et al. Type III procollagen peptide level can indicate liver dysfunction associated with volume overload in acute heart failure. ESC Heart Fail. 2022, 9, 1832–1843. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Yoshihisa, A.; Takiguchi, M.; Shimizu, T.; Nakamura, Y.; Yamauchi, H.; Iwaya, S.; Owada, T.; Miyata, M.; Sato, T.; et al. Liver dysfunction assessed by model for end-stage liver disease excluding INR (MELD-XI) scoring system predicts adverse prognosis in heart failure. PLoS ONE 2014, 9, e100618. [Google Scholar] [CrossRef] [PubMed]
- Adamson, C.; Cowan, L.M.; de Boer, R.A.; Diez, M.; Drożdż, J.; Dukát, A.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Ljungman, C.E.; et al. Liver tests and outcomes in heart failure with reduced ejection fraction: Findings from DAPA-HF. Eur. J. Heart Fail. 2022, 24, 1856–1868. [Google Scholar] [CrossRef]
- Yang, J.A.; Kato, T.S.; Shulman, B.P.; Takayama, H.; Farr, M.; Jorde, U.P.; Mancini, D.M.; Naka, Y.; Schulze, P.C. Liver dysfunction as a predictor of outcomes in patients with advanced heart failure requiring ventricular assist device support: Use of the Model of End-stage Liver Disease (MELD) and MELD eXcluding INR (MELD-XI) scoring system. J. Heart Lung Transplant. 2012, 31, 601–610. [Google Scholar] [CrossRef]
- Wu, F.M.; Kogon, B.; Earing, M.G.; Aboulhosn, J.A.; Broberg, C.S.; John, A.S.; Harmon, A.; Sainani, N.I.; Hill, A.J.; Odze, R.D.; et al. Liver health in adults with Fontan circulation: A multicenter cross-sectional study. J. Thorac. Cardiovasc. Surg. 2017, 153, 656–664. [Google Scholar] [CrossRef]
- Louie, C.Y.; Pham, M.X.; Daugherty, T.J.; Kambham, N.; Higgins, J.P. The liver in heart failure: A biopsy and explant series of the histopathologic and laboratory findings with a particular focus on pre-cardiac transplant evaluation. Mod. Pathol. 2015, 28, 932–943. [Google Scholar] [CrossRef]
- Liu, X.; Chen, W.; Shao, W.; Jiang, Y.; Cao, Z.; He, W.; Wu, M.; Chen, Z.; Ma, J.; Chen, Y.; et al. Liver fibrosis scores and atrial fibrillation incidence in heart failure with preserved ejection fraction. ESC Heart Fail. 2022, 9, 3985–3994. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, M.; Chen, T.; Zhou, Y. Correlation Between Liver Stiffness and Diastolic Function, Left Ventricular Hypertrophy, and Right Cardiac Function in Patients with Ejection Fraction Preserved Heart Failure. Front. Cardiovasc. Med. 2021, 8, 748173. [Google Scholar] [CrossRef]
- Zeng, M.; Chen, Y.; Zhao, B. Higher liver stiffness in patients with chronic congestive heart failure: Data from NHANES with liver ultrasound transient elastography. Ann. Palliat. Med. 2021, 10, 6859–6866. [Google Scholar] [CrossRef] [PubMed]
- Yoshitani, T.; Asakawa, N.; Sakakibara, M.; Noguchi, K.; Tokuda, Y.; Kamiya, K.; Iwano, H.; Yamada, S.; Kudou, Y.; Nishida, M.; et al. Value of Virtual Touch Quantification Elastography for Assessing Liver Congestion in Patients with Heart Failure. Circ. J. 2016, 80, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, T.; Sakata, Y.; Ohtani, T.; Mizote, I.; Takeda, Y.; Asano, Y.; Masuda, M.; Minamiguchi, H.; Kanzaki, M.; Ichibori, Y.; et al. Usefulness of transient elastography for noninvasive and reliable estimation of right-sided filling pressure in heart failure. Am. J. Cardiol. 2014, 113, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Nishi, H.; Toda, K.; Miyagawa, S.; Yoshikawa, Y.; Fukushima, S.; Kawamura, M.; Saito, T.; Yoshioka, D.; Daimon, T.; Sawa, Y. Novel method of evaluating liver stiffness using transient elastography to evaluate perioperative status in severe heart failure. Circ. J. 2015, 79, 391–397. [Google Scholar] [CrossRef]
- Kashiyama, N.; Toda, K.; Nakamura, T.; Miyagawa, S.; Nishi, H.; Yoshikawa, Y.; Fukushima, S.; Saito, S.; Yoshioka, D.; Sawa, Y. Evaluation of right ventricular function using liver stiffness in patients with left ventricular assist device. Eur. J. Cardiothorac. Surg. 2017, 51, 715–721. [Google Scholar] [CrossRef]
- Potthoff, A.; Schettler, A.; Attia, D.; Schlue, J.; Schmitto, J.D.; Fegbeutel, C.; Strüber, M.; Haverich, A.; Manns, M.P.; Wedemeyer, H.; et al. Liver stiffness measurements and short-term survival after left ventricular assist device implantation: A pilot study. J. Heart Lung Transplant. 2015, 34, 1586–1594. [Google Scholar] [CrossRef]
- Terashi, E.; Kodama, Y.; Kuraoka, A.; Ishikawa, Y.; Nakamura, M.; Sagawa, K.; Ishikawa, S. Usefulness of Liver Stiffness on Ultrasound Shear-Wave Elastography for the Evaluation of Central Venous Pressure in Children with Heart Diseases. Circ. J. 2019, 83, 1338–1341. [Google Scholar] [CrossRef]
- Jalal, Z.; Iriart, X.; De Lédinghen, V.; Barnetche, T.; Hiriart, J.B.; Vergniol, J.; Foucher, J.; Thambo, J.B. Liver stiffness measurements for evaluation of central venous pressure in congenital heart diseases. Heart 2015, 101, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Millonig, G.; Friedrich, S.; Adolf, S.; Fonouni, H.; Golriz, M.; Mehrabi, A.; Stiefel, P.; Pöschl, G.; Büchler, M.W.; Seitz, H.K.; et al. Liver stiffness is directly influenced by central venous pressure. J. Hepatol. 2010, 52, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Colli, A.; Pozzoni, P.; Berzuini, A.; Gerosa, A.; Canovi, C.; Molteni, E.E.; Barbarini, M.; Bonino, F.; Prati, D. Decompensated chronic heart failure: Increased liver stiffness measured by means of transient elastography. Radiology 2010, 257, 872–878. [Google Scholar] [CrossRef]
- Hopper, I.; Kemp, W.; Porapakkham, P.; Sata, Y.; Condon, E.; Skiba, M.; Farber, L.; Porapakkham, P.; Williams, T.J.; Menahem, S.; et al. Impact of heart failure and changes to volume status on liver stiffness: Non-invasive assessment using transient elastography. Eur. J. Heart Fail. 2012, 14, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Alegre, F.; Herrero, J.I.; Iñarrairaegui, M.; Gavira, J.J.; Pujol, C.; Montero, A.; D’Avola, D.; Prieto, J.; Sangro, B.; Quiroga, J. Increased liver stiffness values in patients with heart failure. Acta Gastroenterol. Belg. 2013, 76, 246–250. [Google Scholar]
- Soloveva, A.; Kobalava, Z.; Fudim, M.; Ambrosy, A.P.; Villevalde, S.; Bayarsaikhan, M.; Garmash, I.; Naumenko, M. Relationship of Liver Stiffness with Congestion in Patients Presenting with Acute Decompensated Heart Failure. J. Card. Fail. 2019, 25, 176–187. [Google Scholar] [CrossRef]
- Sakamoto, T.; Ito, S.; Endo, A.; Yoshitomi, H.; Tanabe, K. Combinational Elastography. Int. Heart J. 2022, 63, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Pekoz, B.C.; Koc, M.; Kucukosmanoglu, M.; Koc, A.S.; Koca, H.; Dönmez, Y.; Sumbul, H.E. Evaluation of Liver Stiffness after Atrial Septal Defect Closure. Ultrasound Q. 2022, 38, 165–169. [Google Scholar] [CrossRef]
- Küçükosmanoğlu, M.; Koç, A.S.; Sümbül, H.E.; Koca, H.; Çakır Pekoz, B.; Koç, M. Liver stiffness value obtained by point shear-wave elastography is significantly related with atrial septal defect size. Diagn. Interv. Radiol. 2020, 26, 284–291. [Google Scholar] [CrossRef]
- Saito, Y.; Kato, M.; Nagashima, K.; Monno, K.; Aizawa, Y.; Okumura, Y.; Matsumoto, N.; Moriyama, M.; Hirayama, A. Prognostic Relevance of Liver Stiffness Assessed by Transient Elastography in Patients with Acute Decompensated Heart Failure. Circ. J. 2018, 82, 1822–1829. [Google Scholar] [CrossRef]
- Omote, K.; Nagai, T.; Asakawa, N.; Kamiya, K.; Tokuda, Y.; Aikawa, T.; Fukushima, A.; Noguchi, K.; Kato, Y.; Komoriyama, H.; et al. Impact of admission liver stiffness on long-term clinical outcomes in patients with acute decompensated heart failure. Heart Vessel. 2019, 34, 984–991. [Google Scholar] [CrossRef]
- Taniguchi, T.; Ohtani, T.; Kioka, H.; Tsukamoto, Y.; Onishi, T.; Nakamoto, K.; Katsimichas, T.; Sengoku, K.; Chimura, M.; Hashimoto, H.; et al. Liver Stiffness Reflecting Right-Sided Filling Pressure Can Predict Adverse Outcomes in Patients With Heart Failure. JACC Cardiovasc. Imaging 2019, 12, 955–964. [Google Scholar] [CrossRef]
- Wang, Q.; Song, Y.; Wu, Q.; Dong, Q.; Yang, S. Liver stiffness for predicting adverse cardiac events in chinese patients with heart failure: A two-year prospective study. BMC Cardiovasc. Disord. 2022, 22, 51. [Google Scholar] [CrossRef]
- Saito, Y.; Matsumoto, N.; Aizawa, Y.; Fukamachi, D.; Kitano, D.; Toyama, K.; Fujito, H.; Sezai, A.; Okumura, Y. Prognostic Value of Liver Stiffness Measured by Two-Dimensional Elastography in Acute Decompensated Heart Failure with Preserved Ejection Fraction. Int. Heart J. 2021, 62, 821–828. [Google Scholar] [CrossRef]
- Panchani, N.; Schulz, P.; Van Zyl, J.; Felius, J.; Baxter, R.; Yoon, E.T.; Baldawi, H.; Bindra, A.; Asrani, S.K. Liver stiffness and prediction of cardiac outcomes in patients with acute decompensated heart failure. Clin. Transplant. 2022, 36, e14545. [Google Scholar] [CrossRef]
- De Ávila, D.X.; de Andrade, T.G.; Mocarzel, L.O.; Gismondi, R.A.; Cabrita, C.M.; Mesquita, E.T.; Villacorta, H. Liver stiffness as measured by transient elastography is a predictor of outcomes in patients with chronic heart failure with reduced, mid-range, and recovered left-ventricular ejection fraction. Am. Heart J. Plus 2021, 11, 100048. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Studies | Biomarker | Study Population | N | Cut-Off for Biomarker Group | Composite Endpoints | N° of Events | Mean FU Time (Days) | Independent Risk Factor (s) for Event |
|---|---|---|---|---|---|---|---|---|
| Takae et al. [34] | FIB-4 | HF | 704 | >2.67 (on admission) | Total CV events | |||
| HFrEF | 83 | 19 | 695 | |||||
| HFmrEF | 117 | 26 | 632 | |||||
| HFpEF | 504 | 237 | 1159 | FIB-4 | ||||
| Maeda et al. [35] | FIB-5 | HF | 906 | <−8.20 (on discharge) | Cardiac death; readmission for HF | 320 | 152 | FIB-5 |
| Shirakabe et al. [36] | P3P | AHF admitted in ICU | 643 | >1.2 U/mL (on admission) >16.09% | All-cause death; readmission for HF | 229 | 365 | P3P |
| PVS | 307 | PVS | ||||||
| Abe et al. [37] | MELD-XI | Decompensated HF | 562 | >10 | Cardiac death; all-cause death | 62 | 471 | age |
| reduced HF | ||||||||
| 42 | MELD-XI | |||||||
| Adamson et al. [38] | Bilirubin | HFrEF | 4720 | >1.0 mg/dL | CV death, worsening of HF, or all-cause death | 885 | 720 | bilirubin |
| ALP | 4729 | >120 IU/L | ||||||
| ALT | 4714 | >35 IU/L | ||||||
| AST | 4681 | >35 IU/L | ||||||
| Yang et al. [39] | MELD-XI | VAD | 255 | >17 | CV death | 48 | 365 | MELD-XI |
| Studies | Modality | Study Population | N | LSM | Measured CVP | Correlation (r) | p Value |
|---|---|---|---|---|---|---|---|
| Taniguchi et al. [46] | FibroScan | Decompensated HF | 31 | 8.5 (5.3–12.0) kPa | 9.0 (5.0–12.0) mm Hg | 0.95 | <0.001 |
| Nishi et al. [47] | FibroScan | LVAD recipients | 30 | 13.3 ± 13 kPa | 8.8 ± 6.9 mm Hg | 0.515 | <0.01 |
| Kashiyama et al. [48] | FibroScan | LVAD recipients | 55 | 12.7 ± 13.1 kPa | 7.4 ± 5.0 mm Hg | 0.52 | <0.01 |
| Potthoff et al. [49] | ARFI | LVAD recipients | 28 | 2.50 ± 0.92 m/s | 14.0 ± 6.0 mm Hg | 0.793 | 0.001 |
| Yoshitani et al. [45] | ARFI | Decompensated HF | 38 | 2.03 ± 0.91 m/s | 11.8 ± 5.4 mm Hg | 0.636 | 0.014 |
| Terashi et al. [50] | Ultrasound SWE | Children with congenital heart diseases | 79 | / | 5.7 ± 3.5 mm Hg | 0.776 | <0.001 |
| Jalal et al. [51] | FibroScan | Children/adults with congenital heart diseases | 96 (60/36) | 5 (2.8–47.2) m/s [4.6 (3–21)/6.1 (2.8–47.2)] m/s | 6 (3–20) mm Hg [6 (3–15)/7 (3/20)] mm Hg | 0.75 (0.68/0.84) | <0.0001 |
| Studies | Modality | Intervention | N | LSM before | LSM after | p Value |
|---|---|---|---|---|---|---|
| Millonig et al. [52] | FibroScan | Diuresis | 10 | 40.7 (6.1–51.3) kPa | 17.8 (3.3–33.2 kPa) | 0.004 |
| Colli et al. [53] | FibroScan | Diuresis | 27 | 8.80 (5.92–11.90) kPa | 7.20 (5.2–11.30) kPa | 0.003 |
| Hopper et al. [54] | FibroScan | Diuresis | 8 | 11.2 (6.7–14.3) kPa | 9.5 (7.3–21.6) kPa | >0.09 |
| Alegre et al. [55] | FibroScan | Diuresis | 9 | 14.7 (8.3–18.8) kPa | 8.2 (5.1–11.2) kPa | 0.008 |
| Soloveva et al. [56] | FibroScan | Diuresis | 149 | 12.2 (6.3–23.6) kPa | 8.7 (5.9–14.4) kPa | <0.001 |
| Yoshitani et al. [45] | ARFI | Diuresis | 14 | 2.37 ± 1.09 m/s | 1.27 ± 0.33 m/s | <0.001 |
| Potthoff et al. [49] | ARFI | LVAD placement | 23 | 1.88 (0.92–3.72) m/s | 1.43 (0.93–3.67) m/s | <0.001 |
| Sakamoto et al. [57] | Shear wave elastography | Diuresis | 51 | 2.01 ± 0.61 m/s | 1.62 ± 0.49 m/s | 0.026 |
| Pekoz et al. [58] | FibroScan | Atrial Septal Defect Closure | 66 | / | / | / |
| Studies | Modality | Study Population | N | Cut-off for High LSM Group | Composite Endpoints | Number of Events | Mean FU Time (Days) | Independent Risk Factor (s) for Event |
|---|---|---|---|---|---|---|---|---|
| Saito et al. [60] | FibroScan | ADHF | 105 | >8.8 kPa (on admission) | Death from CVD; readmission for HF | 42 | 153 | LSM |
| Omote et al. [61] | pSWE/ARFI | ADHF | 70 | >1.50 m/s (on admission) | All-cause death; worsening HF | 26 | 272 | SBP LSM |
| Taniguchi et al. [62] | FibroScan | HF | 171 | >6.9 kPa (on discharge) | Cardiac death; readmission for HF | 41 | 203 | LSM |
| Soloveva et al. [56] | FibroScan | ADHF | 149 | >13 kPa (on admission) >5 kPa (on discharge) | All-cause death, heart transplant, or readmission for HF | 71 | 289 | LSM at discharge |
| Qian Wang et al. [63] | FibroScan | HF | 53 | >6.9 kPa (on discharge) | Death or readmission for HF | 24 | 730 | LSM TAPSE |
| Saito et al. [64] | US 2D-SWE | ADHFpEF | 80 | >10.2 kPa (on discharge) | All-cause death; readmission for HF | 25 | 212 | LSM |
| Zhang et al. [43] | FibroScan | Decompensated HFpEF | 150 | >8.30 kPa (on admission) | MACE (CV death, malignant arrhythmia, AMI, stroke, and rehospitalization for HF) | 26 | 197 | LSM AF NYHA class NT-proBNP |
| Panchani et al. [65] | US 2D-SWE | ADHF | 49 | >39.8 kPa (on admission) | LVAD, HT, death, and rehospitalization | 21 | 365 | LSM |
| de Ávila et al. [66] | FibroScan | Ambulatory HF (HFpEF, HFmrEF, HFrEF) | 85 | >5.9 kPa | CV death or HF hospitalization | 20 HF hospitalizations 3 deaths | 219 ± 86 days | LSM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aspromonte, N.; Fumarulo, I.; Petrucci, L.; Biferali, B.; Liguori, A.; Gasbarrini, A.; Massetti, M.; Miele, L. The Liver in Heart Failure: From Biomarkers to Clinical Risk. Int. J. Mol. Sci. 2023, 24, 15665. https://doi.org/10.3390/ijms242115665
Aspromonte N, Fumarulo I, Petrucci L, Biferali B, Liguori A, Gasbarrini A, Massetti M, Miele L. The Liver in Heart Failure: From Biomarkers to Clinical Risk. International Journal of Molecular Sciences. 2023; 24(21):15665. https://doi.org/10.3390/ijms242115665
Chicago/Turabian StyleAspromonte, Nadia, Isabella Fumarulo, Lucrezia Petrucci, Bianca Biferali, Antonio Liguori, Antonio Gasbarrini, Massimo Massetti, and Luca Miele. 2023. "The Liver in Heart Failure: From Biomarkers to Clinical Risk" International Journal of Molecular Sciences 24, no. 21: 15665. https://doi.org/10.3390/ijms242115665
APA StyleAspromonte, N., Fumarulo, I., Petrucci, L., Biferali, B., Liguori, A., Gasbarrini, A., Massetti, M., & Miele, L. (2023). The Liver in Heart Failure: From Biomarkers to Clinical Risk. International Journal of Molecular Sciences, 24(21), 15665. https://doi.org/10.3390/ijms242115665