

In-Vitro Biofilm Removal Efficacy Using Water Jet in Combination with Cold Plasma Technology on Dental Titanium Implants

 , , , ,
, , , , 
Abstract
1. Introduction

2. Results
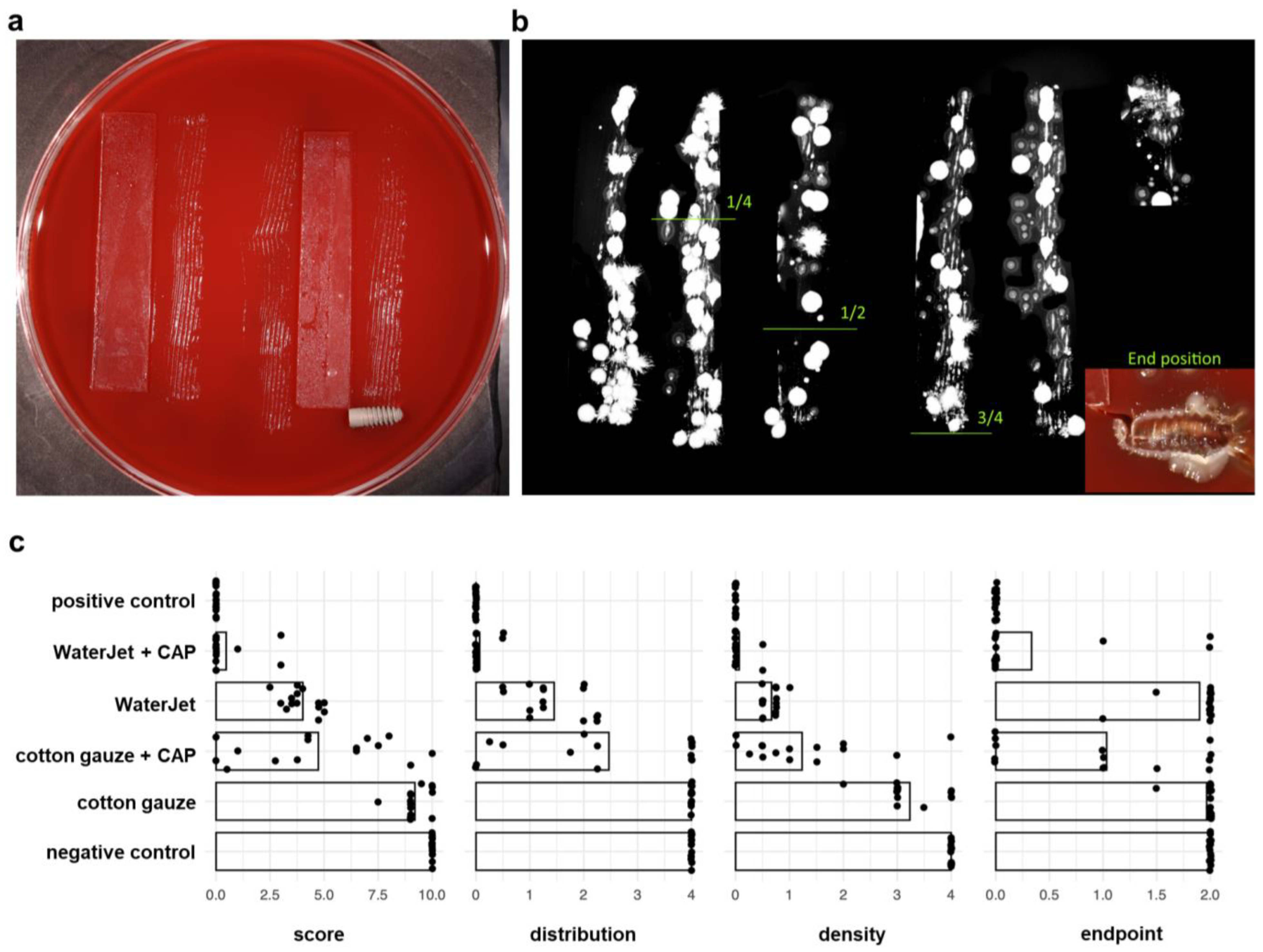
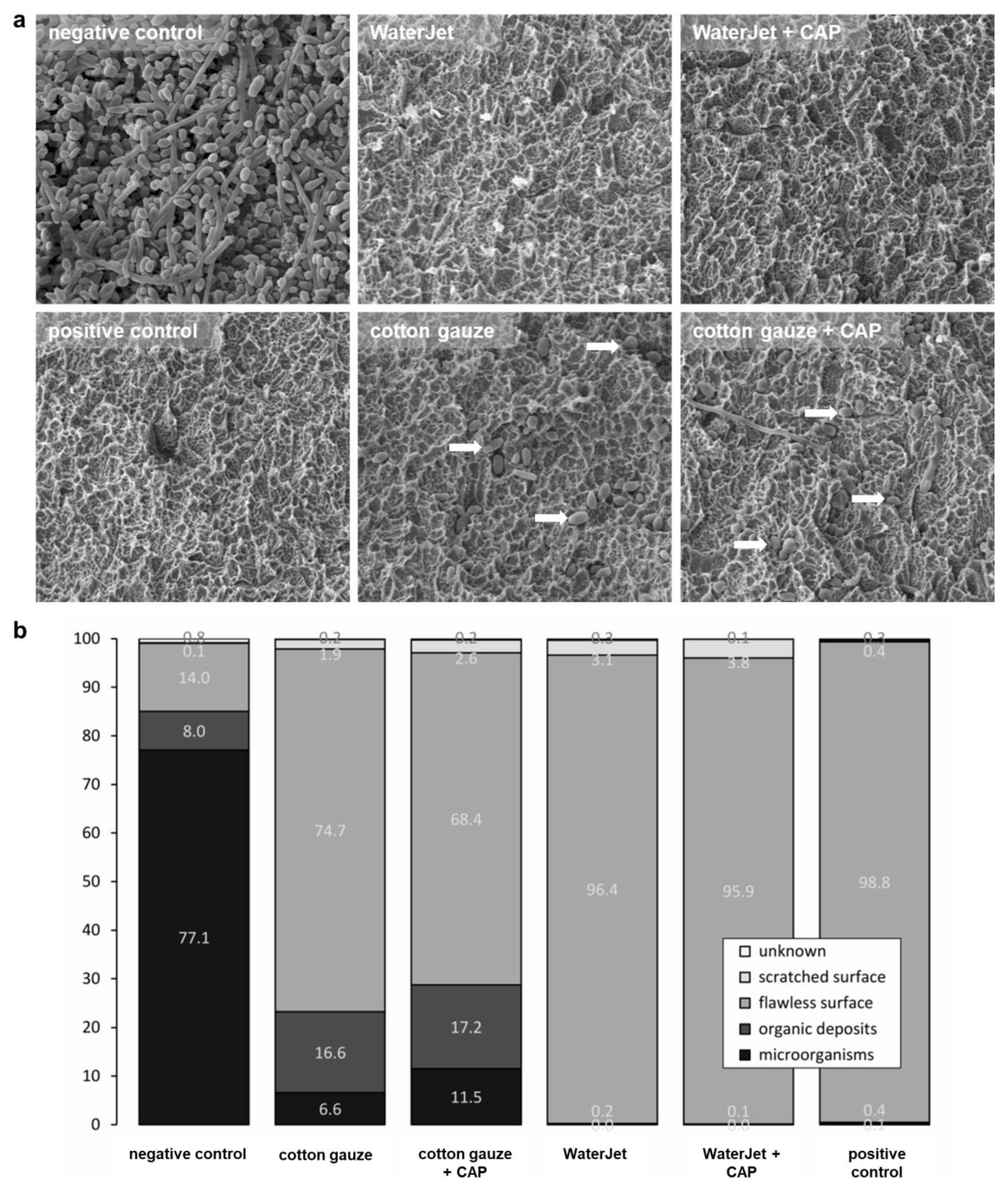
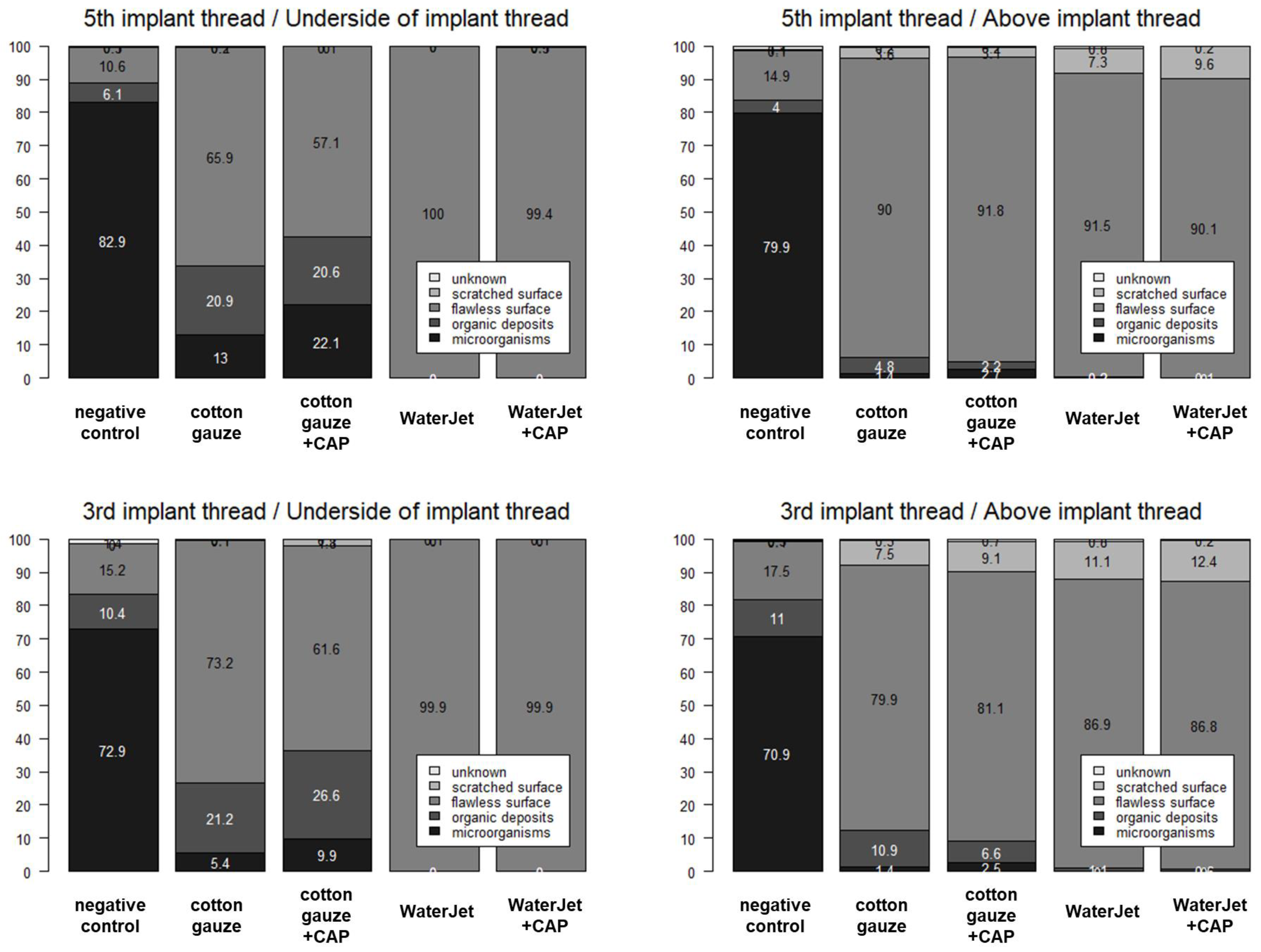
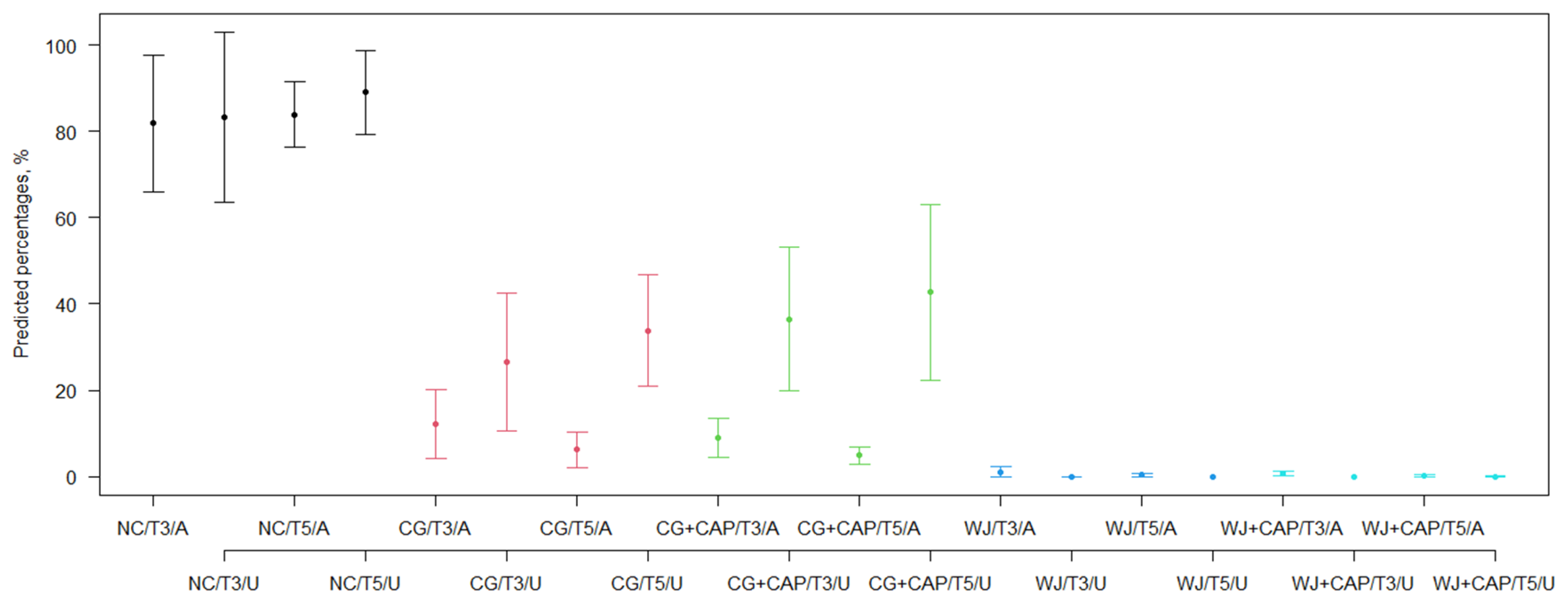
2.1. Combined Treatment of Dental Water Jet and CAP Provides the Best Decontamination Efficacy
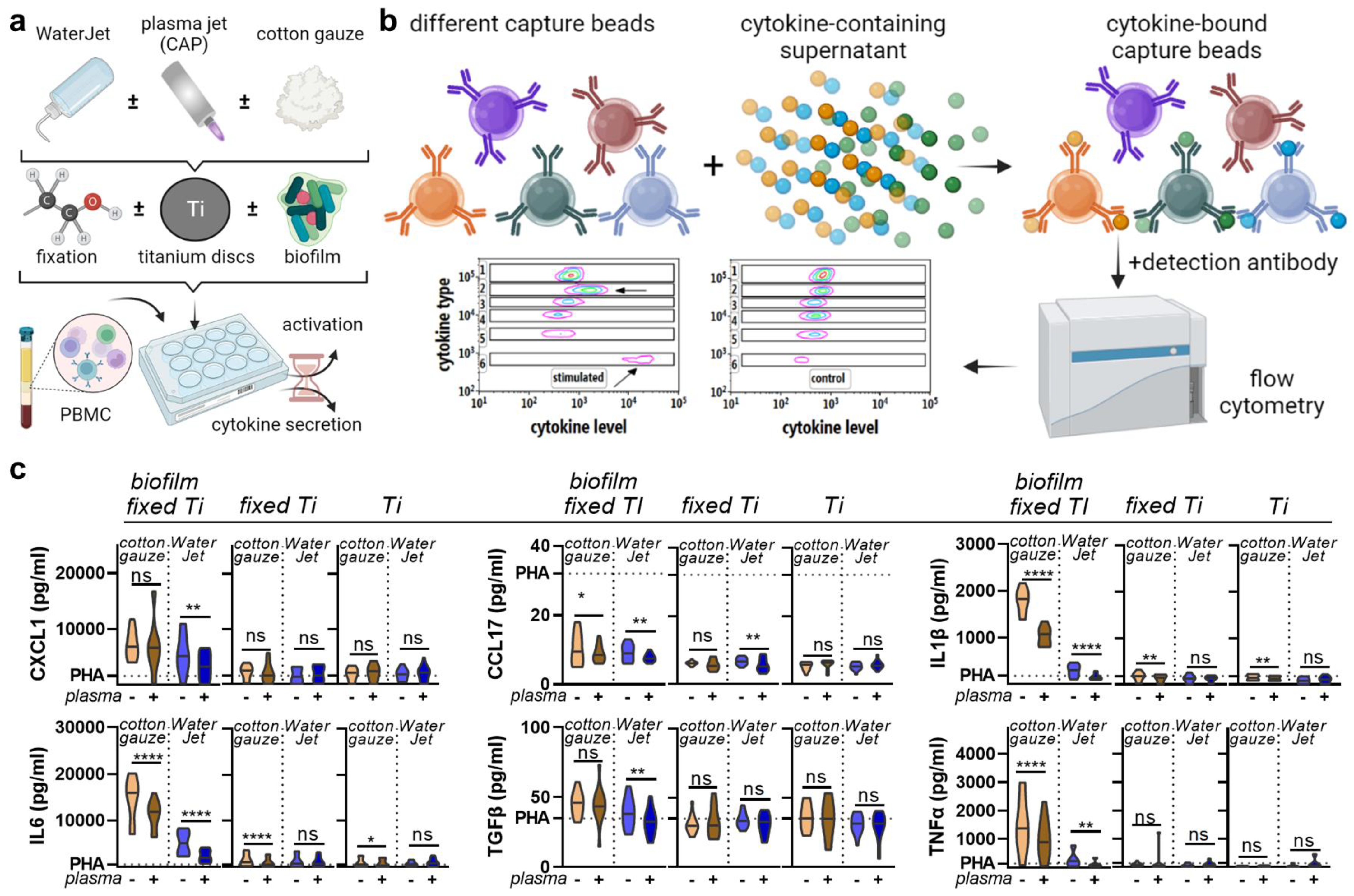
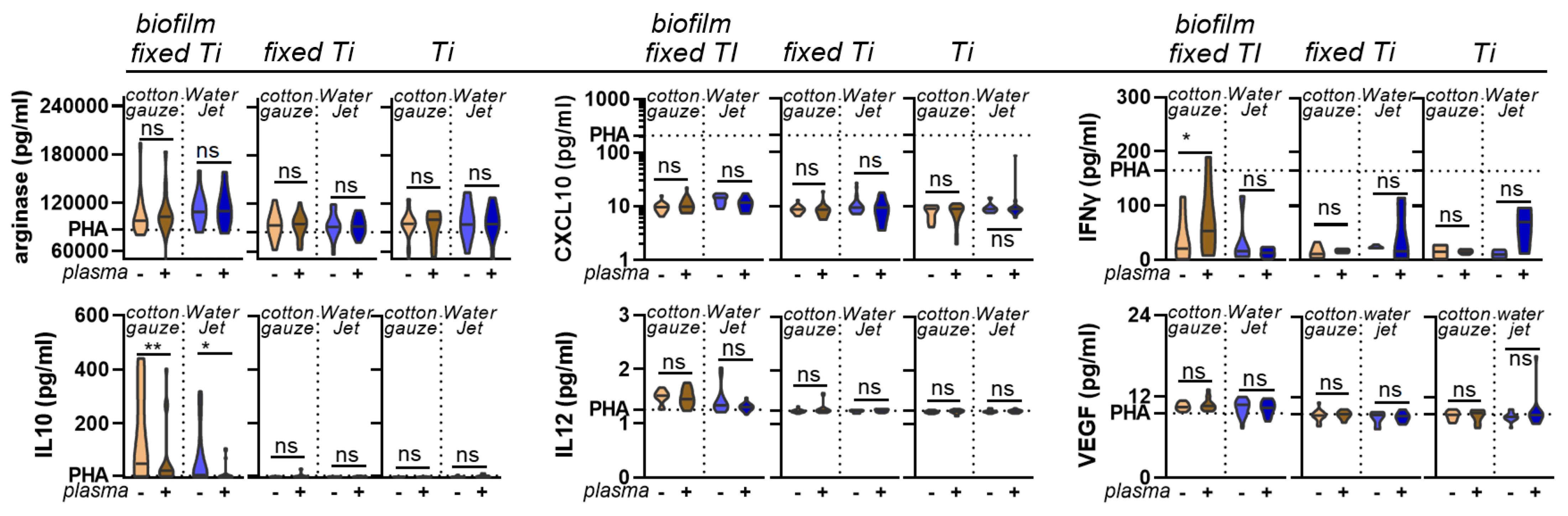
2.2. Combined Treatment of Dental WaterJet and CAP Reduced Chemokine and Cytokine Release
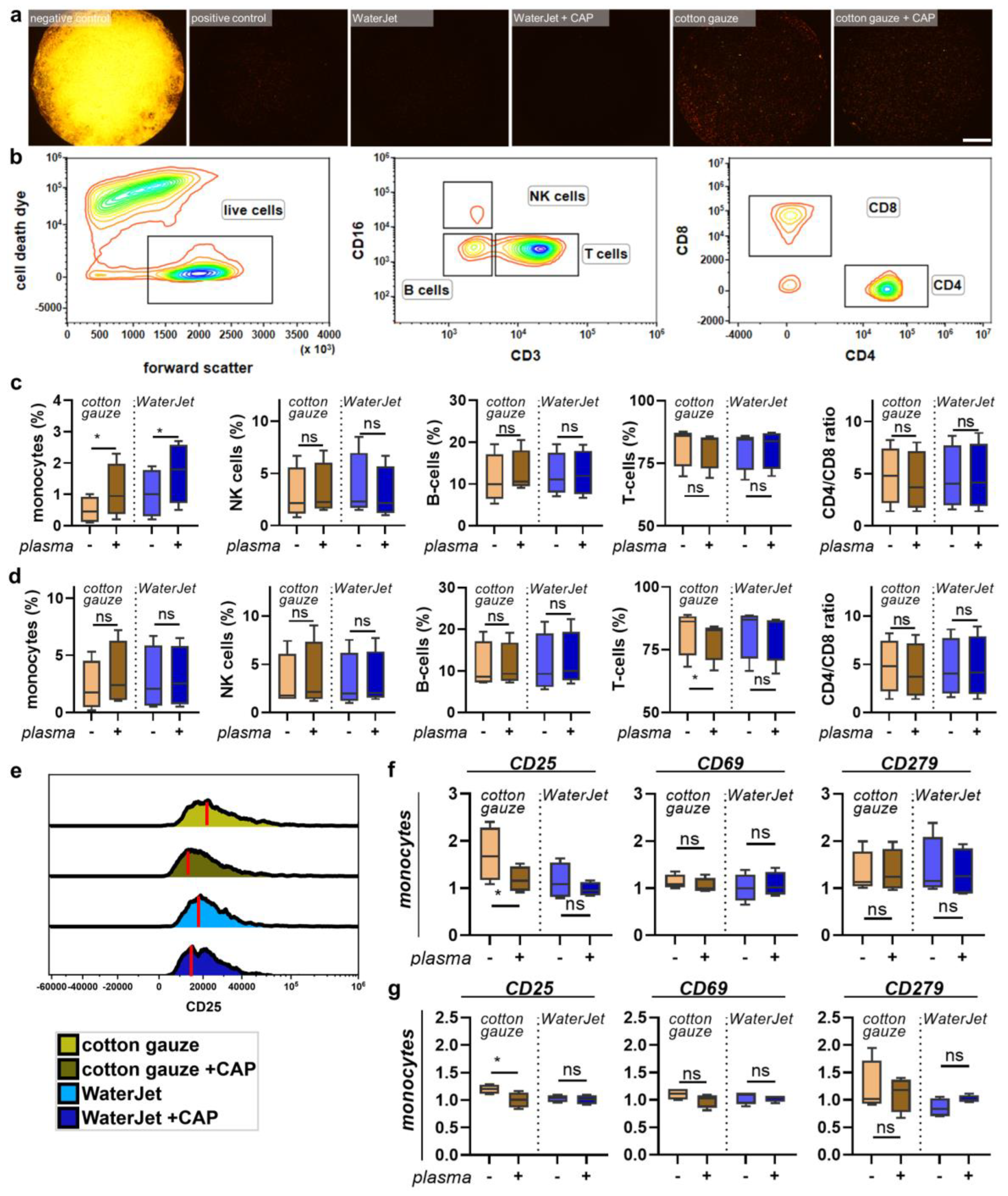
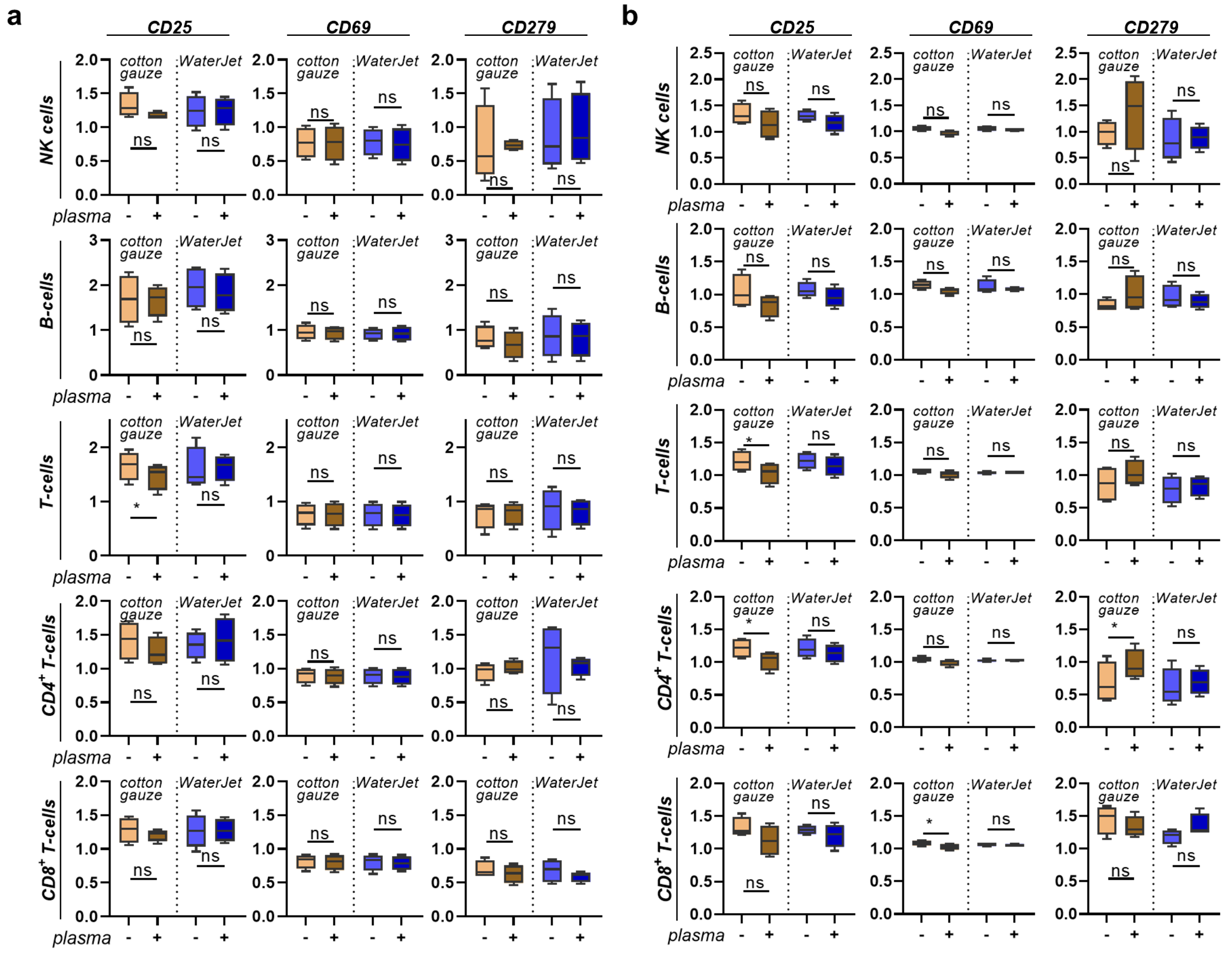
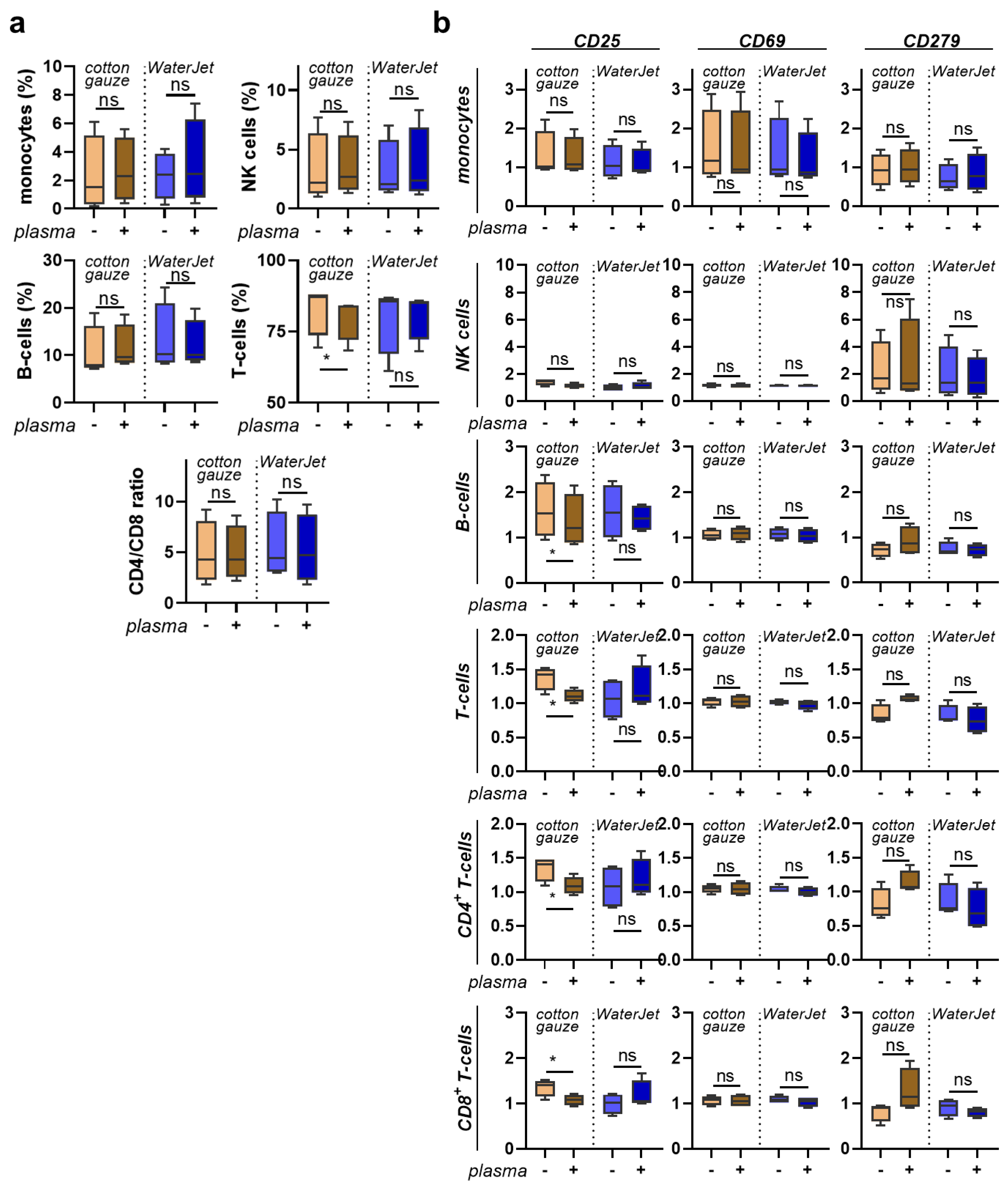
2.3. Combined Treatment with WaterJet and CAP did Not Promote Cellular Inflammation
3. Discussion
4. Material and Methods
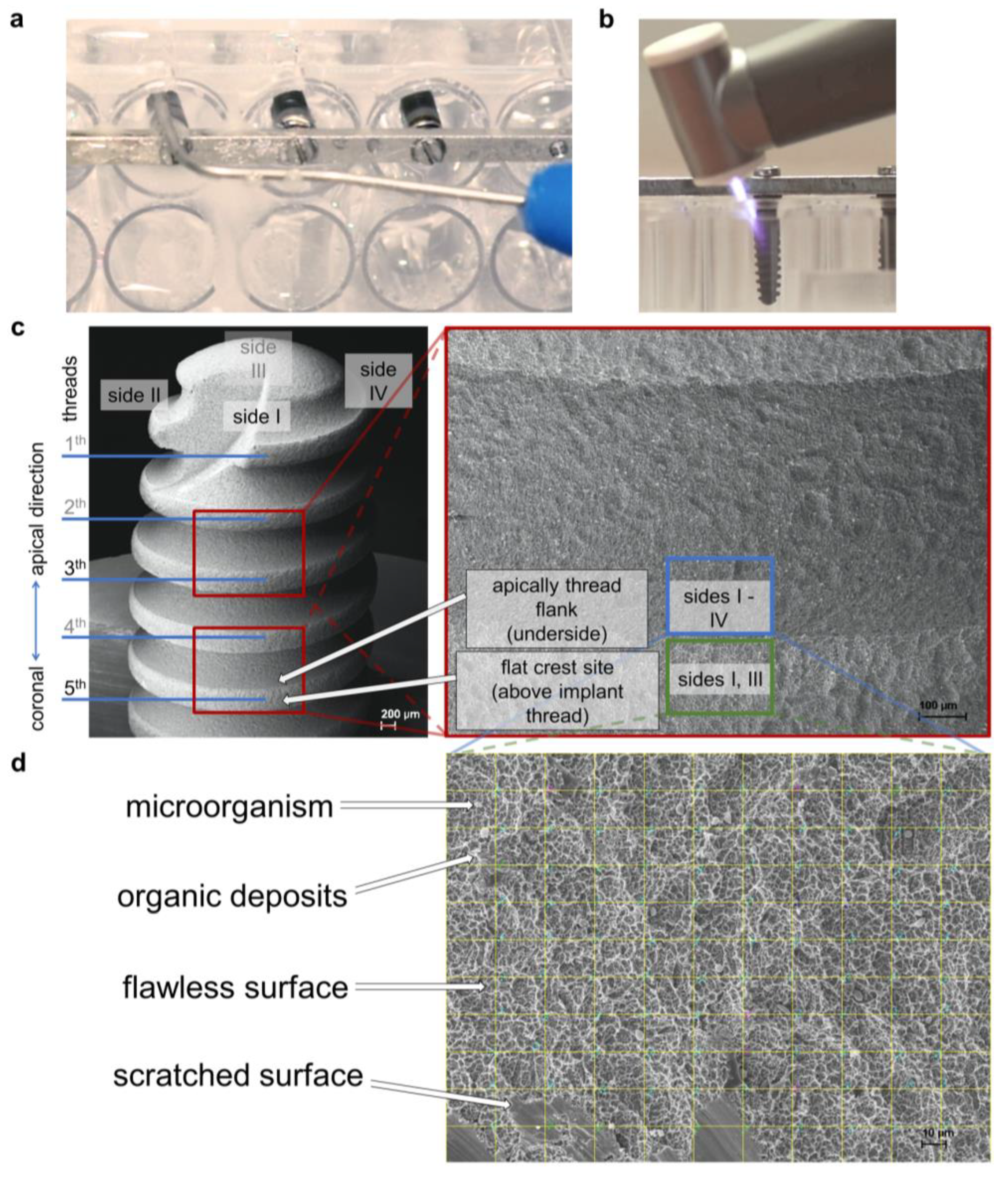
4.1. Treatment Setup, Dental Implants, and Titanium Discs
4.2. Biofilms Cultivation
4.3. Physico-Chemical Treatment with Cold Atmospheric Pressure Plasma (CAP)
4.4. Analysis of Implant Biofilm Removal by Scanning Electron Microscopy
4.5. Analysis of Implant Decontamination by the Roll-Out-on-Agar-Method
4.6. Inflammatory Profiling
4.7. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Score | Distribution | Density | End Position |
|---|---|---|---|---|
| negative control (untreated biofilm) | 10/10 (10; 10) b | 4/4 (4; 4) b | 4/4 (4; 4) b | 2/2 (2; 2) b |
| [10–10] | [4–4] | [4–4] | [2–2] | |
| cotton gauze | 9.2/9 (9; 10) a,b,c | 4/4 (4; 4) b,c | 3.2/3 (3; 4) a,b,c | 2/2 (2; 2) b,c |
| [7.5–10] | [4–4] | [2–4] | [1.5–2] | |
| cotton gauze + CAP | 4.7/4.3 (1; 7.5) a,b,c | 2.5/2.3 (0.5; 4) a,b,c | 1.2/1 (0.5; 2) a,b,c | 1/1 (0; 2) a,b,c |
| [0–10] | [0–4] | [0–4] | [0–2] | |
| WaterJet | 4.0/3.8 (3.5; 4.8) a,b,d | 1.5/1.3 (1; 2) a,b,d | 0.7/0.8 (0.5; 0.8) a,b,d | 2/2 (2; 2) b,d |
| [2.5–5] | [0.5–2.3] | [0.5–1] | [1–2] | |
| WaterJet + CAP | 0.5/0 (0; 0) a,d | 0.1/0 (0; 0) a,d | 0.1/0 (0; 0) a,d | 0.3/0 (0; 0) a,d |
| [0–3] | [0–0.5] | [0–0.5] | [0–2] | |
| positive control (sterile, untreated) | 0/0 (0; 0) a | 0/0 (0; 0) a | 0/0 (0; 0) a | 0/0 (0; 0) a |
| [0–0] | [0–0] | [0–0] | [0–0] |
| Comparison | Score | Distribution | Density | End Position |
|---|---|---|---|---|
| negative control vs. cotton gauze | −0.81 (−1.34; −0.29) | −0.01 (−0.19; 0.17) | −0.76 (−1.08; −0.43) | −0.04 (−0.17; 0.09) |
| negative control vs. cotton gauze + CAP | −5.31 (−7.04; −3.59) | −1.58 (−2.43; −0.73) | −2.76 (−3.35; −2.17) | −0.97 (−1.41; −0.54) |
| negative control vs. WaterJet | −6.00 (−6.60; −5.39) | −2.56 (−2.95; −2.18) | −3.33 (−3.47; −3.18) | −0.11 (−0.31; 0.10) |
| negative control vs. WaterJet + CAP | −9.55 (−10.22; −8.88) | −3.95 (−4.16; −3.73) | −3.93 (−4.10; −3.75) | −1.67 (−2.06; −1.29) |
| cotton gauze vs. cotton gauze + CAP | −4.50 (−6.24; −2.76) | −1.57 (−2.40; −0.73) | −2.00 (−2.65; −1.35) | −0.93 (−1.37; −0.50) |
| cotton gauze vs. WaterJet | −5.18 (−5.90; −4.47) | −2.55 (−2.93; −2.17) | −2.57 (−2.90; −2.23) | −0.07 (−0.28; 0.15) |
| cotton gauze vs. WaterJet + CAP | −8.73 (−9.52; −7.95) | −3.93 (−4.14; −3.73) | −3.17 (−3.51; −2.82) | −1.63 (−2.03; −1.23) |
| cotton gauze + CAP vs. WaterJet | −0.68 (−2.45; 1.08) | −0.98 (−1.89; −0.08) | −0.57 (−1.15; 0.02) | 0.86 (0.40; 1.32) |
| cotton gauze + CAP vs. WaterJet + CAP | −4.23 (−6.03; −2.44) | −2.37 (−3.21; −1.52) | −1.17 (−1.75; −0.58) | −0.70 (−1.27; −0.14) |
| WaterJet vs. WaterJet + CAP | −3.55 (−4.39; −2.71) | −1.38 (−1.78; −0.99) | −0.60 (−0.78; −0.42) | −1.57 (−1.99; −1.14) |
| Treatment | n | Microorganisms | Organic Deposits | Flawless Surface | Scratched Surface | Unknown |
|---|---|---|---|---|---|---|
| total | ||||||
| negative control | 108 | 88.5 (66.5; 99.8) [1–100] | 0 (0; 7.3) [0–78] | 0 (0; 18.8) [0–100] | 0 (0; 0) [0–2.5] | 0 (0; 0.5) [0–19] |
| cotton gauze | 108 | 3 (1; 7.8) [0–96] | 3.3 (0; 25.3) [0–91] | 85 (62; 94) [0–100] | 0 (0; 0.5) [0–50] | 0 (0; 0) [0–4] |
| cotton gauze + CAP | 108 | 4.8 (1.5; 11.5) [0–100] | 5.5 (0; 30.3 [0–93] | 76.8 (44.8; 94.8) [0–99.5] | 0 (0; 0) [0–63] | 0 (0; 0) [0–5.5] |
| WaterJet | 108 | 0 (0; 0) [0–3] | 0 (0; 0) [0–12] | 100 (94.3; 100) [67–100] | 0 (0; 4) [0–33] | 0 (0; 0) [0–8] |
| WaterJet + CAP | 108 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–3.5] | 100 (92.3; 100) [67–100] | 0 (0; 7.5) [0–33] | 0 (0; 0) [0–4] |
| positive control | 84 | 0 (0; 0) [0–2.5] | 0 (0; 0) [0–13] | 100 (99; 100) [76.5–100] | 0 (0; 0) [0–6] | 0 (0; 0) [0–15.5] |
| 5th implant thread | ||||||
| negative control | 54 | 88.5 (69.5; 100) [8.5–100] | 0 (0; 5.5) [0–42] | 0.3 (0; 21.5) [0–90] | 0 (0; 0) [0–2.5] | 0 (0; 0.5) [0–9] |
| cotton gauze | 54 | 3.3 (1; 10) [0–96] | 3.8 (0; 23) [0–91] | 86.8 (61; 93.5) [0–100] | 0 (0; 0.5) [0–33] | 0 (0; 0) [0–2] |
| cotton gauze + CAP | 54 | 4.3 (1; 15) [0–100] | 3 (0; 26) [0–93] | 82.3 (43; 96) [0–99.5] | 0 (0; 0) [0–25] | 0 (0; 0) [0–2] |
| WaterJet | 54 | 0 (0; 0) [0–3] | 0 (0; 0) [0–2] | 100 (97.5; 100) [67–100] | 0 (0; 1.5) [0–33] | 0 (0; 0) [0–7] |
| WaterJet + CAP | 54 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–2] | 100 (92.5; 100) [82–100] | 0 (0; 7) [0–18] | 0 (0; 0) [0–2] |
| positive control | 42 | 0 (0; 0) [0–2.5] | 0 (0; 0) [0–13] | 100 (99.5; 100) [86–100] | 0 (0; 0) [0–1] | 0 (0; 0) [0–1] |
| 3rd implant thread | ||||||
| negative control | 54 | 88.5 (55; 99) [0–100] | 0 (0; 11) [0–78] | 0 (0; 6.5) [0–100] | 0 (0; 0) [0–1] | 0 (0; 1) [0–19] |
| cotton gauze | 54 | 3 (1; 5.5) [0–16] | 3 (0; 28) [0–85] | 84.5 (63; 94) [12–98.5] | 0 (0; 0.5) [0–50] | 0 (0; 0) [0–4] |
| cotton gauze + CAP | 54 | 5 (2; 9) [0–87.5] | 10.8 (0; 38) [0–90] | 73.5 (45; 94) [0–99] | 0 (0; 0.5) [0–63] | 0 (0; 0) [0–5.5] |
| WaterJet | 54 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–12] | 100 (93; 100) [73–100] | 0 (0; 5) [0–27] | 0 (0; 0) [0–8] |
| WaterJet + CAP | 54 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–3.5] | 100 (92; 100) [67–100] | 0 (0; 8) [0–33] | 0 (0; 0) [0–4] |
| positive control | 42 | 0 (0; 0) [0–1.5] | 0 (0; 0) [0–2.5] | 100 (99; 100) [76.5–100] | 0 (0; 0) [0–6] | 0 (0; 0) [0–15.5] |
| above implant thread (thread top land) | ||||||
| negative control | 36 | 88.5 (62; 99.3) [0–100] | 1.5 (0; 7.3) [0–78] | 0.5 (0; 25) [0–100] | 0 (0; 0) [0–1] | 0 (0; 1) [0–9] |
| cotton gauze | 36 | 1 (0; 2) [0–7.5] | 2 (0; 6.3) [0–45] | 91.3 (77; 97.3) [47–100] | 0.5 (0; 7.5) [0–50] | 0 (0; 0) [0–4] |
| cotton gauze + CAP | 36 | 1 (0; 4) [0–14.5] | 1 (0; 6.3) [0–24] | 91.8 (76.8; 96) [44–99.5] | 0.3 (0; 7) [0–43] | 0 (0; 0.5) [0–5.5] |
| WaterJet | 36 | 0 (0; 0) [0–3] | 0 (0; 0.3) [0–12] | 92 (85; 94.3) [67–100] | 7.5 (4; 12.5) [0–33] | 0 (0; 0.5) 0–8] |
| WaterJet + CAP | 36 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–3.5] | 88.3 (85.5; 92.5) [67–99] | 11.3 (6.5; 14.5) [1–33] | 0 (0; 0) [0–4] |
| positive control | 28 | 0 (0; 0) [0–1.5] | 0.3 (0; 1.3) [0–13] | 99 (95.8; 100) [76.5–100] | 0 (0; 1) [0–6] | 0 (0; 0.3) [0–15.5] |
| underside of implant thread (bottom thread flank) | ||||||
| negative control | 72 | 88.5 (70; 100) [1–100] | 0 (0; 7.5) [0–58] | 0 (0; 13.3) [0–99] | 0 (0; 0) [0–2.5] | 0 (0; 0.5) [0–19] |
| cotton gauze | 72 | 5.3 (2.3; 10) [0–96] | 11.8 (0; 35.8) [0–91] | 82 (48; 93) [0–98.5] | 0 (0; 0) [0–1.5] | 0 (0; 0) [0–1.5] |
| cotton gauze + CAP | 72 | 7.3 (3.5; 14.3) [0.5–100] | 17.5 (0; 41.3) [0–93] | 63.8 (38.8; 93.8) [0–99.5] | 0 (0; 0) [0–63] | 0 (0; 0) [0–2] |
| WaterJet | 72 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–0] | 100 (100; 100) [99–100] | 0 (0; 0) [0–0] | 0 (0; 0) [0–1] |
| WaterJet + CAP | 72 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–0] | 100 (100; 100) [89–100] | 0 (0; 0) [0–11] | 0 (0; 0) [0–1] |
| positive control | 56 | 0 (0; 0) [0–2.5] | 0 (0; 0) [0–0.5] | 100 (100; 100) [97.5–100] | 0 (0; 0) [0–1] | 0 (0; 0) [0–0.5] |
| Treatment | n | Microorganisms | Organic Deposits | Flawless Surface | Scratched Surface | Unknown |
|---|---|---|---|---|---|---|
| 5th implant thread/underside of implant thread (thread flank) | ||||||
| negative control | 36 | 90.5 (77; 100) [8.5–100] | 0 (0; 6.3) [0–42] | 0 (0; 15.5) [0–90] | 0 (0; 0) [0–2.5] | 0 (0; 0) [0–5] |
| cotton gauze | 36 | 6.8 (2.8; 13) [0–96] | 14 (0; 35.8) [0–91] | 77.5 (47; 91.3) [0–98] | 0 (0; 0) [0–1] | 0 (0; 0) [0–1] |
| cotton gauze + CAP | 36 | 9.5 (3.3; 27.3) [0.5–100] | 13 (0; 33.8) [0–93] | 67.5 (28.3; 90.5) [0–99.5] | 0 (0; 0) [0–1] | 0 (0; 0) [0–2] |
| WaterJet | 36 | 0 (0; 0) [0–0] | 0 (0; 0) [0–0] | 100 (100; 100) [99–100] | 0 (0; 0) [0–0] | 0 (0; 0) [0–1] |
| WaterJet + CAP | 36 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–0] | 100 (100; 100) [89–100] | 0 (0; 0) [0–11] | 0 (0; 0) [0–1] |
| positive control | 28 | 0 (0; 0) [0–2.5] | 0 (0; 0) [0–0.5] | 100 (100; 100) [97.5–100] | 0 (0; 0) [0–1] | 0 (0; 0) [0–0.5] |
| 5th implant thread/above implant thread (thread top land) | ||||||
| negative control | 18 | 84 (62.5; 99) [44.5–100] | 0.5 (0; 4) [0–26.5] | 9.5 (0; 27) [0–42] | 0 (0; 0) [0–1] | 0 (0; 1) [0–9] |
| cotton gauze | 18 | 1 (0; 2) [0–7.5] | 1 (0; 4.5) [0–36.5] | 92.3 (91; 98.5) [61–100] | 0.3 (0; 2) [0–33] | 0 (0; 0) [0–2] |
| cotton gauze + CAP | 18 | 1 (0; 4) [0–14.5] | 0.8 (0; 3.5) [0–10.5] | 95 (88; 98) [71–99.5] | 0 (0; 1) [0–25] | 0 (0; 0.5) [0–2] |
| WaterJet | 18 | 0 (0; 0) [0–3] | 0 (0; 0) [0–2] | 92.8 (92; 97.5) [67–100] | 5.5 (1.5; 8) [0–33] | 0 (0; 1) [0–7] |
| WaterJet + CAP | 18 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–2] | 90 (87; 94) [82–99] | 9.8 (5; 13) [1–18] | 0 (0; 0) [0–2] |
| positive control | 14 | 0 (0; 0) [0–0.5] | 0.3 (0; 1) [0–13] | 99.5 (99; 100) [86–100] | 0 (0; 0) [0–1] | 0 (0; 0) [0–1] |
| 3rd implant thread/underside of implant thread (bottom thread flank) | ||||||
| negative control | 36 | 88.5 (57.5; 98.8) [1–100] | 0 (0; 13) [0–58] | 0 (0; 6) [0–99] | 0 (0; 0) [0–1] | 0 (0; 1) [0–19] |
| cotton gauze | 36 | 4.5 (2; 8) [0–16] | 3.5 (0; 40) [0–85] | 85.5 (50; 94.3) [12–98.5] | 0 (0; 0) [0–1.5] | 0 (0; 0) [0–1.5] |
| cotton gauze + CAP | 36 | 6 (4.3; 11.3) [1.5–87.5] | 30.3 (0; 46.5) [0–90] | 57.5 (42; 94.5) [0–98.5] | 0 (0; 0) [0–63] | 0 (0; 0) [0–1.5] |
| WaterJet | 36 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–0] | 100 (100; 100) [99–100] | 0 (0; 0) [0–0] | 0 (0; 0) [0–1] |
| WaterJet + CAP | 36 | 0 (0; 0) [0–0] | 0 (0; 0) [0–0] | 100 (100; 100) [99–100] | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–1] |
| positive control | 28 | 0 (0; 0) [0–1] | 0 (0; 0) [0–0.5] | 100 (100; 100) [99–100] | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–0.5] |
| 3rd implant thread/above implant thread (thread top land) | ||||||
| negative control | 18 | 88.5 (52; 100) 0–100 | 4 (0; 11) [0–78] | 0 (0; 6.5) [0–100] | 0 (0; 0) [0–1] | 0 (0; 1) [0–3] |
| cotton gauze | 18 | 1 (0; 2) 0–5.5 | 2.8 (1; 19) [0–45] | 83.5 (72; 94) [47–98.5] | 1.5 (0; 13.5) [0–50] | 0 (0; 0) [0–4] |
| cotton gauze + CAP | 18 | 0.5 (0; 4) 0–12 | 3.8 (0; 10) [0–24] | 85.5 (73; 94) [44–99] | 0.8 (0; 11) [0–43] | 0 (0; 1) [0–5.5] |
| WaterJet | 18 | 0 (0; 0) [0–0] | 0 (0; 1) [0–12] | 89.5 (79; 93) [73–97] | 9.3 (5; 15) [0–27] | 0 (0; 0) [0–8] |
| WaterJet + CAP | 18 | 0 (0; 0) [0–0.5] | 0 (0; 0) [0–3.5] | 87.8 (85; 92) [67–96] | 12 (8; 15) [4–33] | 0 (0; 0) [0–4] |
| positive control | 14 | 0 (0; 0.5) [0–1.5] | 0.5 (0; 1.5) [0–2.5] | 97.3 (94.5; 99) [76.5–100] | 0.8 (0; 4.5) [0–6] | 0 (0; 1) [0–15.5] |
| B (95% CI) | OR (95% CI) | p-Value | p-Value (Global Test) | |
|---|---|---|---|---|
| treatment (reference: negative control) | 0.00 (ref.) | 1.00 (ref.) | - | <0.0001 |
| cotton gauze | −3.473 (−4.770; −2.177) | 0.031 (0.008; 0.113) | 0.000 | |
| cotton gauze + CAP | −3.811 (−5.007; −2.615) | 0.022 (0.007; 0.073) | 0.000 | |
| WaterJet | −6.021 (−7.559; −4.483) | 0.002 (0.001; 0.011) | 0.000 | |
| WaterJet+ CAP | −6.599 (−7.948; −5.249) | 0.001 (0.0004; 0.005) | 0.000 | |
| implant thread (ref. 3rd implant thread) | ||||
| 5th implant thread | 0.141 (−0.790; 1.072) | 1.151 (0.454; 2.921) | 0.767 | |
| side of implant thread (Ref. above implant thread) | ||||
| underside of implant thread | 0.099 (−1.077; 1.275) | 1.105 (0.341; 3.580) | 0.868 | |
| interaction Treatment X implant thread | 0.4431 | |||
| cotton gauze X 5th implant thread | −0.883 (−2.296; 0.530) | 0.414 (0.101; 1.699) | 0.221 | |
| cotton gauze + CAP X 5th implant thread | −0.806 (−1.937; 0.326) | 0.447 (0.144; 1.385) | 0.163 | |
| WaterJet X 5th implant thread | −1.172 (−2.990; 0.645) | 0.310 (0.050; 1.907) | 0.206 | |
| WaterJet + CAP X 5th implant thread | −1.628 (−3.671; 0.416) | 0.196 (0.025; 1.516) | 0.119 | |
| interaction treatment X side of implant thread | <0.0001 | |||
| cotton gauze X underside of implant thread | 0.850 (−0.515; 2.216) | 2.341 (0.597; 9.172) | 0.222 | |
| cotton gauze + CAP X underside of implant thread | 1.649 (0.272; 3.026) | 5.203 (1.313; 20.624) | 0.019 | |
| WaterJet X underside of implant thread | −4.468 (−7.036; −1.900) | 0.011 (0.001; 0.150) | 0.001 | |
| WaterJet + CAP X underside of implant thread | −12.699 (−14.284; −11.114) | 3.05 × 10−6 (6.3 × 10−7; 0.00001) | 0.000 | |
| interaction implant thread X side of implant thread | ||||
| 5th implant thread X underside of implant thread | 0.345 (−1.215; 1.905) | 1.412 (0.297; 6.717) | 0.665 | |
| interaction treatment X implant thread X side of implant thread | <0.0001 | |||
| cotton gauze X 5th implant thread X underside of implant thread | 0.743 (−1.057; 2.544) | 2.103 (0.347; 12.734) | 0.418 | |
| cotton gauze + CAP X 5th implant thread X underside of implant thread | 0.580 (−1.167; 2.328) | 1.787 (0.311; 10.255) | 0.515 | |
| WaterJet X 5th implant thread X underside of implant thread | −8.122 (−11.021; −5.222) | 0.0003 (0.00002; 0.005) | 0.000 | |
| WaterJet + CAP X 5th implant thread X underside of implant thread | 10.645 (7.387; 13.902) | 41962.5 (1615.4; 1090027) | 0.000 | |
| intercept | 1.507 (0.444; 2.570) | 4.513 (1.559; 13.061) | 0.005 |
References
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Effectiveness of Implant Therapy Analyzed in a Swedish Population Prevalence of Peri-implantitis. J. Dent. Res. 2016, 95, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Lang, N.P. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontol. 2000 2010, 53, 167–181. [Google Scholar] [CrossRef]
- Rosen, P.; Clem, D.; Cochran, D.; Bradley, S.F.; Renvert, S.; Wang, H.-L. Peri-implant mucositis and peri-implantitis: A current understanding of their diagnoses and clinical implications. J. Periodontol. 2013, 84, 436–443. [Google Scholar] [CrossRef]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Treatment of pathologic peri-implant pockets. Periodontol. 2000 2018, 76, 180–190. [Google Scholar] [CrossRef]
- Meyle, J. Mechanical, chemical and laser treatments of the implant surface in the presence of marginal bone loss around implants. Eur. J. Oral Implant. 2012, 5, 71–81. [Google Scholar]
- Sahrmann, P.; Ronay, V.; Hofer, D.; Attin, T.; Jung, R.E.; Schmidlin, P.R. In vitro cleaning potential of three different implant debridement methods. Clin. Oral Implant. Res. 2015, 26, 314–319. [Google Scholar] [CrossRef]
- Baima, G.; Citterio, F.; Romandini, M.; Romano, F.; Mariani, G.M.; Buduneli, N.; Aimetti, M. Surface decontamination protocols for surgical treatment of peri-implantitis: A systematic review with meta-analysis. Clin. Oral Implant. Res. 2022, 33, 1069–1086. [Google Scholar] [CrossRef]
- Luengo, F.; Sanz-Esporrín, J.; Noguerol, F.; Sanz-Martín, I.; Sanz-Sánchez, I.; Sanz, M. In vitro effect of different implant decontamination methods in three intraosseous defect configurations. Clin. Oral Implant. Res. 2022, 33, 1087–1097. [Google Scholar] [CrossRef]
- Puisys, A.; Schlee, M.; Linkevicius, T.; Petrakakis, P.; Tjaden, A. Photo-activated implants: A triple-blinded, split-mouth, randomized controlled clinical trial on the resistance to removal torque at various healing intervals. Clin. Oral Investig. 2020, 24, 1789–1799. [Google Scholar] [CrossRef]
- Rupp, F.; Gittens, R.A.; Scheideler, L.; Marmur, A.; Boyan, B.D.; Schwartz, Z.; Geis-Gerstorfer, J. A review on the wettability of dental implant surfaces I: Theoretical and experimental aspects. ACTA Biomater. 2014, 10, 2894–2906. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Wieland, M.; Schwartz, Z.; Zhao, G.; Rupp, F.; Geis-Gerstorfer, J.; Schedle, A.; Broggini, N.; Bornstein, M.M.; Buser, D.; et al. Potential of chemically modified hydrophilic surface characteristics to support tissue integration of titanium dental implants. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 88B, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implant. Res. 2011, 22, 349–356. [Google Scholar] [CrossRef]
- John, G.; Becker, J.; Schwarz, F. Rotating titanium brush for plaque removal from rough titanium surfaces--an in vitro study. Clin. Oral Implant. Res. 2014, 25, 838–842. [Google Scholar] [CrossRef]
- Kotsakis, G.A.; Lan, C.; Barbosa, J.; Lill, K.; Chen, R.; Rudney, J.; Aparicio, C. Antimicrobial Agents Used in the Treatment of Peri-Implantitis Alter the Physicochemistry and Cytocompatibility of Titanium Surfaces. J. Periodontol. 2016, 87, 809–819. [Google Scholar] [CrossRef]
- Charalampakis, G.; Ramberg, P.; Dahlén, G.; Berglundh, T.; Abrahamsson, I. Effect of cleansing of biofilm formed on titanium discs. Clin. Oral Implant. Res. 2015, 26, 931–936. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennstrom, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Hallström, H.; Persson, G.R.; Lindgren, S.; Renvert, S. Open flap debridement of peri-implantitis with or without adjunctive systemic antibiotics: A randomized clinical trial. J. Clin. Periodontol. 2017, 44, 1285–1293. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennstrom, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef]
- de Waal, Y.C.M.; Raghoebar, G.M.; Huddleston Slater, J.J.R.; Meijer, H.J.A.; Winkel, E.G.; van Winkelhoff, A.J. Implant decontamination during surgical peri-implantitis treatment: A randomized, double-blind, placebo-controlled trial. J. Clin. Periodontol. 2013, 40, 186–195. [Google Scholar] [CrossRef]
- de Waal, Y.C.M.; Raghoebar, G.M.; Meijer, H.J.A.; Winkel, E.G.; van Winkelhoff, A.J. Implant decontamination with 2% chlorhexidine during surgical peri-implantitis treatment: A randomized, double-blind, controlled trial. Clin. Oral Implant. Res. 2015, 26, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Hentenaar, D.F.M.; de Waal, Y.C.M.; Strooker, H.; Meijer, H.J.A.; van Winkelhoff, A.-J.; Raghoebar, G.M. Implant decontamination with phosphoric acid during surgical peri-implantitis treatment: A RCT. Int. J. Implant. Dent. 2017, 3, 33. [Google Scholar] [CrossRef]
- Berglundh, T.; Wennström, J.L.; Lindhe, J. Long-term outcome of surgical treatment of peri-implantitis. A 2-11-year retrospective study. Clin. Oral Implant. Res. 2018, 29, 404–410. [Google Scholar] [CrossRef]
- Papadopoulos, C.A.; Vouros, I.; Menexes, G.; Konstantinidis, A. The utilization of a diode laser in the surgical treatment of peri-implantitis. A randomized clinical trial. Clin. Oral Investig. 2015, 19, 1851–1860. [Google Scholar] [CrossRef]
- Schwarz, F.; John, G.; Schmucker, A.; Sahm, N.; Becker, J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: A 7-year follow-up observation. J. Clin. Periodontol. 2017, 44, 337–342. [Google Scholar] [CrossRef]
- Deppe, H.; Horch, H.-H.; Neff, A. Conventional versus CO2 laser-assisted treatment of peri-implant defects with the concomitant use of pure-phase beta-tricalcium phosphate: A 5-year clinical report. Int. J. Oral Maxillofac. Implant. 2007, 22, 79–86. [Google Scholar]
- Máximo, M.B.; de Mendonça, A.C.; Renata Santos, V.; Figueiredo, L.C.; Feres, M.; Duarte, P.M. Short-term clinical and microbiological evaluations of peri-implant diseases before and after mechanical anti-infective therapies. Clin. Oral Implant. Res. 2009, 20, 99–108. [Google Scholar] [CrossRef]
- Bürgers, R.; Witecy, C.; Hahnel, S.; Gosau, M. The effect of various topical peri-implantitis antiseptics on Staphylococcus epidermidis, Candida albicans, and Streptococcus sanguinis. Arch. Oral Biol. 2012, 57, 940–947. [Google Scholar] [CrossRef]
- Alani, A.; Bishop, K. Peri-implantitis. Part 3: Current modes of management. Br. Dent. J. 2014, 217, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Panariello, B.H.; de Araújo Costa, C.A.; Pavarina, A.C.; Santiago, S.L.; Duarte, S. Advances and Challenges in Oral Biofilm Control. Curr. Oral Health Rep. 2017, 4, 29–33. [Google Scholar] [CrossRef]
- Klinge, B.; Klinge, A.; Bertl, K.; Stavropoulos, A. Peri-implant diseases. Eur. J. Oral Sci. 2018, 126 (Suppl. S1), 88–94. [Google Scholar] [CrossRef] [PubMed]
- Matthes, R.; Duske, K.; Kebede, T.G.; Pink, C.; Schlüter, R.; von Woedtke, T.; Weltmann, K.-D.; Kocher, T.; Jablonowski, L. Osteoblast growth, after cleaning of biofilm-covered titanium discs with air-polishing and cold plasma. J. Clin. Periodontol. 2017, 44, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Flemmig, T.F.; Hetzel, M.; Topoll, H.; Gerss, J.; Haeberlein, I.; Petersilka, G. Subgingival debridement efficacy of glycine powder air polishing. J. Periodontol. 2007, 78, 1002–1010. [Google Scholar] [CrossRef]
- Alonso, V.; García-Caballero, L.; Couto, I.; Diniz, M.; Diz, P.; Limeres, J. Subcutaneous emphysema related to air-powder tooth polishing: A report of three cases. Aust. Dent. J. 2017, 62, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-T.; Subu, M.G.; Kwon, T.-G. Emphysema following air-powder abrasive treatment for peri-implantitis. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 12. [Google Scholar] [CrossRef]
- Sato, Y.; Iikubo, M.; Nishioka, T.; Yoda, N.; Kusunoki, T.; Nakagawa, A.; Sasaki, K.; Tominaga, T. The effectiveness of an actuator-driven pulsed water jet for the removal of artificial dental calculus: A preliminary study. BMC Oral Health 2020, 20, 205. [Google Scholar] [CrossRef]
- Keblish, D.J.; DeMaio, M. Early pulsatile lavage for the decontamination of combat wounds: Historical review and point proposal. Mil. Med. 1998, 163, 844–846. [Google Scholar] [CrossRef]
- Yamada, J.; Takiguchi, T.; Saito, A.; Odanaka, H.; Soyama, H.; Yamamoto, M. Removal of Oral Biofilm on an Implant Fixture by a Cavitating Jet. Implant. Dent. 2017, 26, 904–910. [Google Scholar] [CrossRef]
- Vyas, N.; Grewal, M.; Kuehne, S.A.; Sammons, R.L.; Walmsley, A.D. High speed imaging of biofilm removal from a dental implant model using ultrasonic cavitation. Dent. Mater. 2020, 36, 733–743. [Google Scholar] [CrossRef]
- Park, S.-Y.; Kim, K.-H.; Shin, S.-Y.; Koo, K.-T.; Lee, Y.-M.; Chung, C.-P.; Seol, Y.-J. Decontamination methods using a dental water jet and dental floss for microthreaded implant fixtures in regenerative periimplantitis treatment. Implant. Dent. 2015, 24, 307–316. [Google Scholar] [CrossRef]
- Hihara, H.; Tagaino, R.; Washio, J.; Laosuwan, K.; Wicaksono, D.P.; Izumita, K.; Koide, R.; Takahashi, N.; Sasaki, K. Effectiveness and safety of a new dental plaque removal device utilizing micro mist spray for removing oral biofilm in vitro. BMC Oral Health 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Kotsakis, G.A.; Black, R.; Kum, J.; Berbel, L.; Sadr, A.; Karoussis, I.; Simopoulou, M.; Daubert, D. Effect of implant cleaning on titanium particle dissolution and cytocompatibility. J. Periodontol. 2020, 92, 580–591. [Google Scholar] [CrossRef]
- Medaxis. Available online: https://www.medaxis.ch/de.html (accessed on 3 November 2022).
- Matthes, R.; Koban, I.; Bender, C.; Masur, K.; Kindel, E.; Weltmann, K.-D.; Kocher, T.; Kramer, A.; Hübner, N.-O. Antimicrobial Efficacy of an Atmospheric Pressure Plasma Jet Against Biofilms of Pseudomonas aeruginosa and Staphylococcus epidermidis. Plasma Process. Polym. 2013, 10, 161–166. [Google Scholar] [CrossRef]
- Daeschlein, G.; Napp, M.; von Podewils, S.; Lutze, S.; Emmert, S.; Lange, A.; Klare, I.; Haase, H.; Gümbel, D.; von Woedtke, T.; et al. In Vitro Susceptibility of Multidrug Resistant Skin and Wound Pathogens Against Low Temperature Atmospheric Pressure Plasma Jet (APPJ) and Dielectric Barrier Discharge Plasma (DBD). Plasma Process. Polym. 2014, 11, 175–183. [Google Scholar] [CrossRef]
- Duske, K.; Jablonowski, L.; Koban, I.; Matthes, R.; Holtfreter, B.; Sckell, A.; Nebe, J.B.; von Woedtke, T.; Weltmann, K.D.; Kocher, T. Cold atmospheric plasma in combination with mechanical treatment improves osteoblast growth on biofilm covered titanium discs. Biomaterials 2015, 52, 327–334. [Google Scholar] [CrossRef]
- Mai-Prochnow, A.; Murphy, A.B.; McLean, K.M.; Kong, M.G.; Ostrikov, K.K. Atmospheric pressure plasmas: Infection control and bacterial responses. Int. J. Antimicrob. Agents 2014, 43, 508–517. [Google Scholar] [CrossRef]
- Koban, I.; Holtfreter, B.; Hübner, N.-O.; Matthes, R.; Sietmann, R.; Kindel, E.; Weltmann, K.-D.; Welk, A.; Kramer, A.; Kocher, T. Antimicrobial efficacy of non-thermal plasma in comparison to chlorhexidine against dental biofilms on titanium discs in vitro-proof of principle experiment. J. Clin. Periodontol. 2011, 38, 956–965. [Google Scholar] [CrossRef]
- Schwarz, F.; Ferrari, D.; Popovski, K.; Hartig, B.; Becker, J. Influence of different air-abrasive powders on cell viability at biologically contaminated titanium dental implants surfaces. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 88B, 83–91. [Google Scholar] [CrossRef]
- Duske, K.; Koban, I.; Kindel, E.; Schröder, K.; Nebe, B.; Holtfreter, B.; Jablonowski, L.; Weltmann, K.-D.; Kocher, T. Atmospheric plasma enhances wettability and cell spreading on dental implant metals. J. Clin. Periodontol. 2012, 39, 400–407. [Google Scholar] [CrossRef]
- Coelho, P.G.; Giro, G.; Teixeira, H.S.; Marin, C.; Witek, L.; Thompson, V.P.; Tovar, N.; Silva, N.R.F.A. Argon-based atmospheric pressure plasma enhances early bone response to rough titanium surfaces. J. Biomed. Mater. Res. 2012, 100A, 1901–1906. [Google Scholar] [CrossRef]
- Kawase, T.; Tanaka, T.; Minbu, H.; Kamiya, M.; Oda, M.; Hara, T. An atmospheric-pressure plasma-treated titanium surface potentially supports initial cell adhesion, growth, and differentiation of cultured human prenatal-derived osteoblastic cells. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1289–1296. [Google Scholar] [CrossRef]
- Duske, K.; Wegner, K.; Donnert, M.; Kunert, U.; Podbielski, A.; Kreikemeyer, B.; Gerling, T.; Weltmann, K.-D.; Nebe, B.; Bader, R. Comparative In Vitro Study of Different Atmospheric Pressure Plasma Jets Concerning their Antimicrobial Potential and Cellular Reaction. Plasma Process. Polym. 2015, 12, 1050–1060. [Google Scholar] [CrossRef]
- Rupf, S.; Idlibi, A.N.; Marrawi, F.A.; Hannig, M.; Schubert, A.; von Mueller, L.; Spitzer, W.; Holtmann, H.; Lehmann, A.; Rueppell, A.; et al. Removing Biofilms from Microstructured Titanium Ex Vivo: A Novel Approach Using Atmospheric Plasma Technology. PLoS ONE 2011, 6, e25893. [Google Scholar] [CrossRef]
- Fricke, K.; Koban, I.; Tresp, H.; Jablonowski, L.; Schroder, K.; Kramer, A.; Weltmann, K.-D.; von Woedtke, T.; Kocher, T. Atmospheric pressure plasma: A high-performance tool for the efficient removal of biofilms. PLoS ONE 2012, 7, e42539. [Google Scholar] [CrossRef]
- Assadian, O.; Ousey, K.J.; Daeschlein, G.; Kramer, A.; Parker, C.; Tanner, J.; Leaper, D.J. Effects and safety of atmospheric low-temperature plasma on bacterial reduction in chronic wounds and wound size reduction: A systematic review and meta-analysis. Int. Wound J. 2019, 16, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Evert, K.; Kocher, T.; Schindler, A.; Müller, M.; Müller, K.; Pink, C.; Holtfreter, B.; Schmidt, A.; Dombrowski, F.; Schubert, A.; et al. Repeated exposure of the oral mucosa over 12 months with cold plasma is not carcinogenic in mice. Sci. Rep. 2021, 11, 20672. [Google Scholar] [CrossRef] [PubMed]
- Almohandes, A.; Carcuac, O.; Abrahamsson, I.; Lund, H.; Berglundh, T. Re-osseointegration following reconstructive surgical therapy of experimental peri-implantitis. A pre-clinical in vivo study. Clin. Oral Implant. Res. 2019, 30, 447–456. [Google Scholar] [CrossRef]
- Bekeschus, S.; Meyer, D.; Arlt, K.; von Woedtke, T.; Miebach, L.; Freund, E.; Clemen, R. Argon Plasma Exposure Augments Costimulatory Ligands and Cytokine Release in Human Monocyte-Derived Dendritic Cells. IJMS 2021, 22, 3790. [Google Scholar] [CrossRef]
- Matthes, R.; Jablonowski, L.; Pitchika, V.; Holtfreter, B.; Eberhard, C.; Seifert, L.; Gerling, T.; Vilardell Scholten, L.; Schlüter, R.; Kocher, T. Efficiency of biofilm removal by combination of water jet and cold plasma: An in-vitro study. BMC Oral Health 2022, 22, 157. [Google Scholar] [CrossRef] [PubMed]
- Ichioka, Y.; Derks, J.; Dahlén, G.; Berglundh, T.; Larsson, L. Mechanical removal of biofilm on titanium discs: An in vitro study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 1044–1055. [Google Scholar] [CrossRef]
- Doria, A.C.; Sorge, C.D.; Santos, T.B.; Brandão, J.; Gonçalves, P.A.; Maciel, H.S.; Khouri, S.; Pessoa, R.S. Application of post-discharge region of atmospheric pressure argon and air plasma jet in the contamination control of Candida albicans biofilms. Res. Biomed. Eng. 2015, 31, 358–362. [Google Scholar] [CrossRef]
- Koch, M.; Göltz, M.; Xiangjun, M.; Karl, M.; Rosiwal, S.; Burkovski, A. Electrochemical Disinfection of Dental Implants Experimentally Contaminated with Microorganisms as a Model for Periimplantitis. J. Clin. Med. 2020, 9, 475. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, T.; Shrestha, A.; Kishen, A. Inflammatory potential of monospecies biofilm matrix components. Int. Endod. J. 2019, 52, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Peyyala, R.; Kirakodu, S.S.; Novak, K.F.; Ebersole, J.L. Oral microbial biofilm stimulation of epithelial cell responses. Cytokine 2012, 58, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Bekeschus, S.; Seebauer, C.; Wende, K.; Schmidt, A. Physical plasma and leukocytes-immune or reactive? Biol. Chem. 2018, 400, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Bekeschus, S.; Kramer, A.; Schmidt, A. Gas Plasma-Augmented Wound Healing in Animal Models and Veterinary Medicine. Molecules 2021, 26, 5682. [Google Scholar] [CrossRef]
- Freund, E.; Moritz, J.; Stope, M.; Seebauer, C.; Schmidt, A.; Bekeschus, S. Plasma-Derived Reactive Species Shape a Differentiation Profile in Human Monocytes. Appl. Sci. 2019, 9, 2530. [Google Scholar] [CrossRef]
- Fischer, M.; Schoon, J.; Freund, E.; Miebach, L.; Weltmann, K.-D.; Bekeschus, S.; Wassilew, G.I. Biocompatible Gas Plasma Treatment Affects Secretion Profiles but Not Osteogenic Differentiation in Patient-Derived Mesenchymal Stromal Cells. IJMS 2022, 23, 2038. [Google Scholar] [CrossRef]
- Chen, R.; Curran, J.; Pu, F.; Zhuola, Z.; Bayon, Y.; Hunt, J.A. In Vitro Response of Human Peripheral Blood Mononuclear Cells (PBMC) to Collagen Films Treated with Cold Plasma. Polymers 2017, 9, 254. [Google Scholar] [CrossRef]
- Bekeschus, S.; Miebach, L.; Pommerening, J.; Clemen, R.; Witzke, K. Biological Risk Assessment of Three Dental Composite Materials following Gas Plasma Exposure. Molecules 2022, 27, 4519. [Google Scholar] [CrossRef]
- Shintani, H.; Shimizu, N.; Imanishi, Y.; Sekiya, T.; Tamazawa, K.; Taniguchi, A.; Kido, N. Inactivation of microorganisms and endotoxins by low temperature nitrogen gas plasma exposure. Biocontrol. Sci. 2007, 12, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Bekeschus, S.; Rödder, K.; Schmidt, A.; Stope, M.B.; von Woedtke, T.; Miller, V.; Fridman, A.; Weltmann, K.-D.; Masur, K.; Metelmann, H.-R.; et al. Cold physical plasma selects for specific T helper cell subsets with distinct cells surface markers in a caspase-dependent and NF-κB-independent manner. Plasma. Process. Polym. 2016, 13, 1144–1150. [Google Scholar] [CrossRef]
- Becker, M.; Quabius, S.; Kewitz, T.; Hansen, L.; Becker, G.; Kern, M.; Kersten, H.; Harder, S. In vitro proinflammatory gene expression changes in human whole blood after contact with plasma-treated implant surfaces. J. Craniomaxillofac. Surg. 2019, 47, 1255–1261. [Google Scholar] [CrossRef]
- Jeong, W.-S.; Kwon, J.-S.; Choi, E.-H.; Kim, K.-M. The Effects of Non-Thermal Atmospheric Pressure Plasma treated Titanium Surface on Behaviors of Oral Soft Tissue Cells. Sci. Rep. 2018, 8, 15963. [Google Scholar] [CrossRef]
- Spiliopoulou, A.I.; Kolonitsiou, F.; Krevvata, M.I.; Leontsinidis, M.; Wilkinson, T.S.; Mack, D.; Anastassiou, E.D. Bacterial adhesion, intracellular survival and cytokine induction upon stimulation of mononuclear cells with planktonic or biofilm phase Staphylococcus epidermidis. FEMS Microbiol. Lett. 2012, 330, 56–65. [Google Scholar] [CrossRef]
- Keim, D.; Nickles, K.; Dannewitz, B.; Ratka, C.; Eickholz, P.; Petsos, H. In-vitro efficacy of three different implant-surface decontamination methods in three different defect configurations. Clin. Oral Implant. Res. 2019, 30, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Tastepe, C.S.; van Waas, R.; Liu, Y.; Wismeijer, D. Air powder abrasive treatment as an implant surface cleaning method: A literature review. Int. J. Oral Maxillofac. Implant. 2012, 27, 1461–1473. [Google Scholar]
- Sahrmann, P.; Ronay, V.; Sener, B.; Jung, R.E.; Attin, T.; Schmidlin, P.R. Cleaning potential of glycine air-flow application in an in vitro peri-implantitis model. Clin. Oral Implant. Res. 2013, 24, 666–670. [Google Scholar] [CrossRef]
- Gittens, R.A.; Scheideler, L.; Rupp, F.; Hyzy, S.L.; Geis-Gerstorfer, J.; Schwartz, Z.; Boyan, B.D. A review on the wettability of dental implant surfaces II: Biological and clinical aspects. ACTA Biomater. 2014, 10, 2907–2918. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.B.; Silva, N.; Marques, J.F.; Mata, A.; Silva, F.S.; Caramês, J. Biomimetic Implant Surfaces and Their Role in Biological Integration-A Concise Review. Biomimetics 2022, 7, 74. [Google Scholar] [CrossRef]
- Wagner, G.; Eggers, B.; Duddeck, D.; Kramer, F.-J.; Bourauel, C.; Jepsen, S.; Deschner, J.; Nokhbehsaim, M. Influence of cold atmospheric plasma on dental implant materials-an in vitro analysis. Clin. Oral Investig. 2022, 26, 2949–2963. [Google Scholar] [CrossRef] [PubMed]
- Bekeschus, S.; Ressel, V.; Freund, E.; Gelbrich, N.; MUSTEA, A.; Stope, M.B. Gas Plasma-Treated Prostate Cancer Cells Augment Myeloid Cell Activity and Cytotoxicity. Antioxidants 2020, 9, 323. [Google Scholar] [CrossRef] [PubMed]
- Stata Technical Support. Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation: Vienna, Austria, 2022. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Springer International Publishing: Cham, Switzerland, 2016; ISBN 9783319242774. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matthes, R.; Jablonowski, L.; Miebach, L.; Pitchika, V.; Holtfreter, B.; Eberhard, C.; Seifert, L.; Gerling, T.; Schlüter, R.; Kocher, T.; et al. In-Vitro Biofilm Removal Efficacy Using Water Jet in Combination with Cold Plasma Technology on Dental Titanium Implants. Int. J. Mol. Sci. 2023, 24, 1606. https://doi.org/10.3390/ijms24021606
Matthes R, Jablonowski L, Miebach L, Pitchika V, Holtfreter B, Eberhard C, Seifert L, Gerling T, Schlüter R, Kocher T, et al. In-Vitro Biofilm Removal Efficacy Using Water Jet in Combination with Cold Plasma Technology on Dental Titanium Implants. International Journal of Molecular Sciences. 2023; 24(2):1606. https://doi.org/10.3390/ijms24021606
Chicago/Turabian StyleMatthes, Rutger, Lukasz Jablonowski, Lea Miebach, Vinay Pitchika, Birte Holtfreter, Christian Eberhard, Leo Seifert, Torsten Gerling, Rabea Schlüter, Thomas Kocher, and et al. 2023. "In-Vitro Biofilm Removal Efficacy Using Water Jet in Combination with Cold Plasma Technology on Dental Titanium Implants" International Journal of Molecular Sciences 24, no. 2: 1606. https://doi.org/10.3390/ijms24021606
APA StyleMatthes, R., Jablonowski, L., Miebach, L., Pitchika, V., Holtfreter, B., Eberhard, C., Seifert, L., Gerling, T., Schlüter, R., Kocher, T., & Bekeschus, S. (2023). In-Vitro Biofilm Removal Efficacy Using Water Jet in Combination with Cold Plasma Technology on Dental Titanium Implants. International Journal of Molecular Sciences, 24(2), 1606. https://doi.org/10.3390/ijms24021606