
Multi-Level Biomarkers for Early Diagnosis of Ischaemic Stroke: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
2.6. Bioinformatic Analysis
3. Results
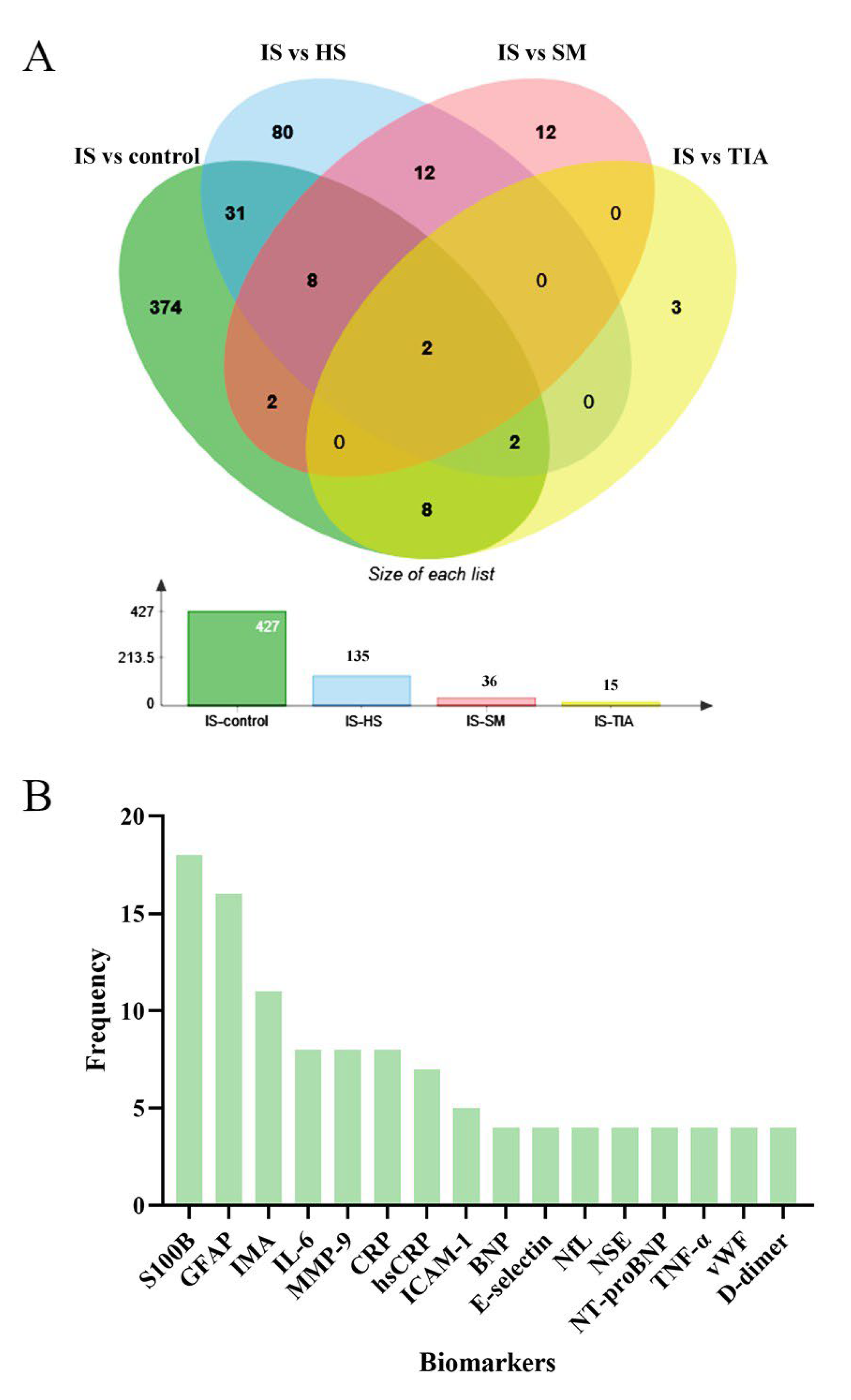
3.1. Qualitative Synthesis
3.2. Quality Assessment
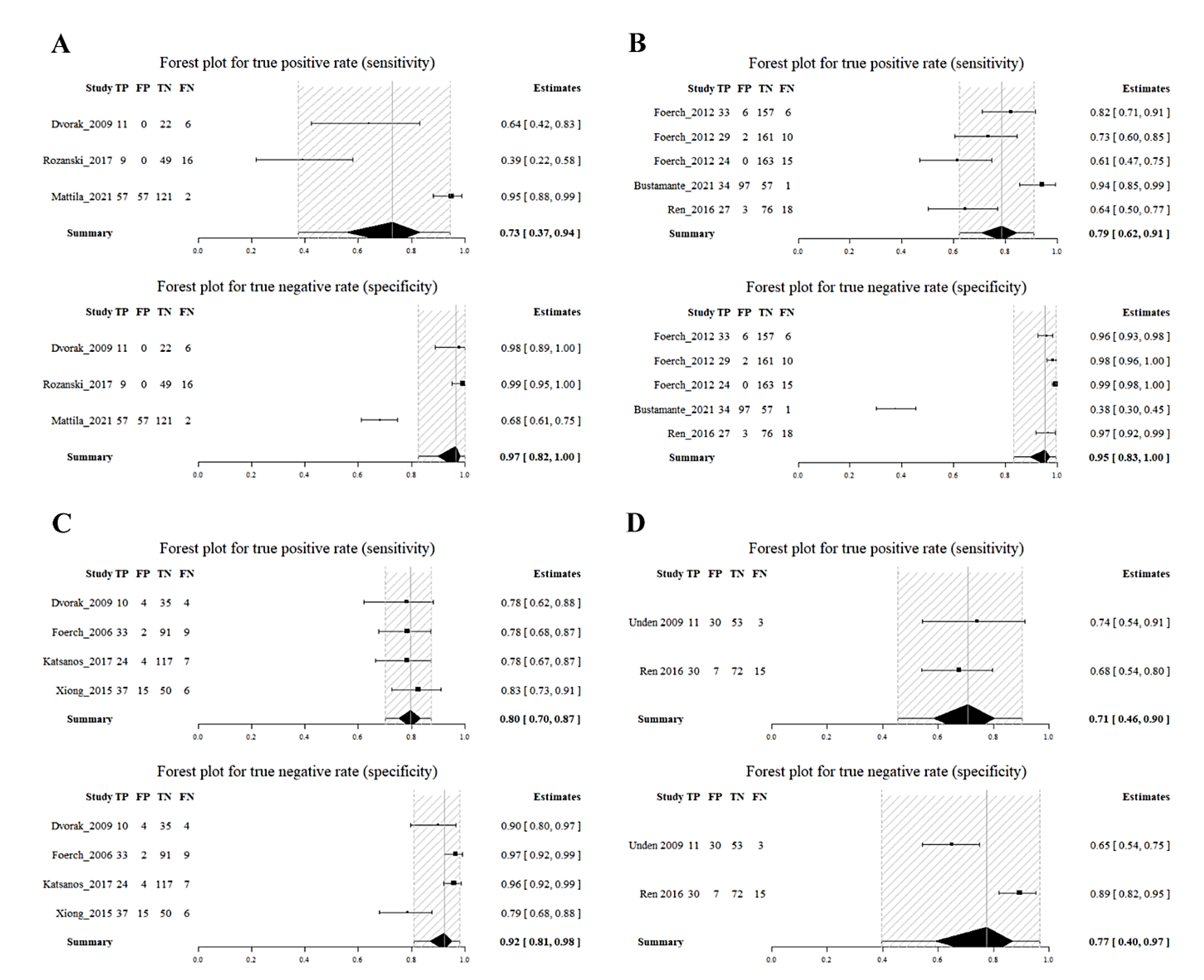
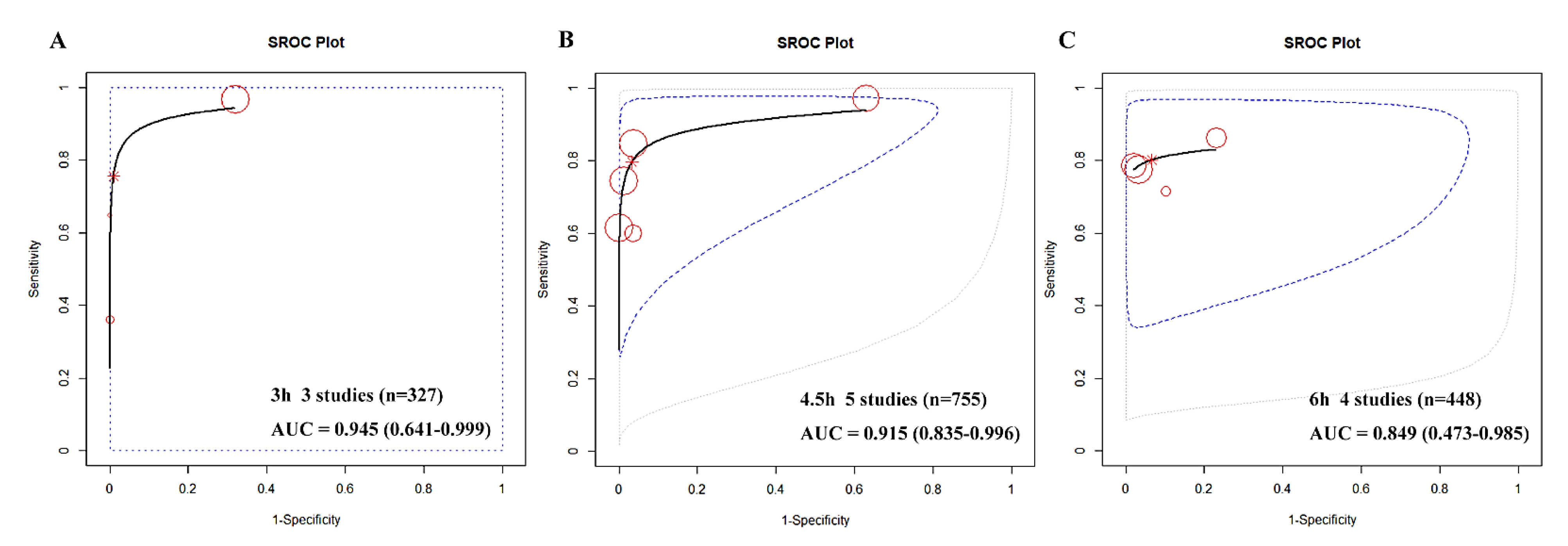
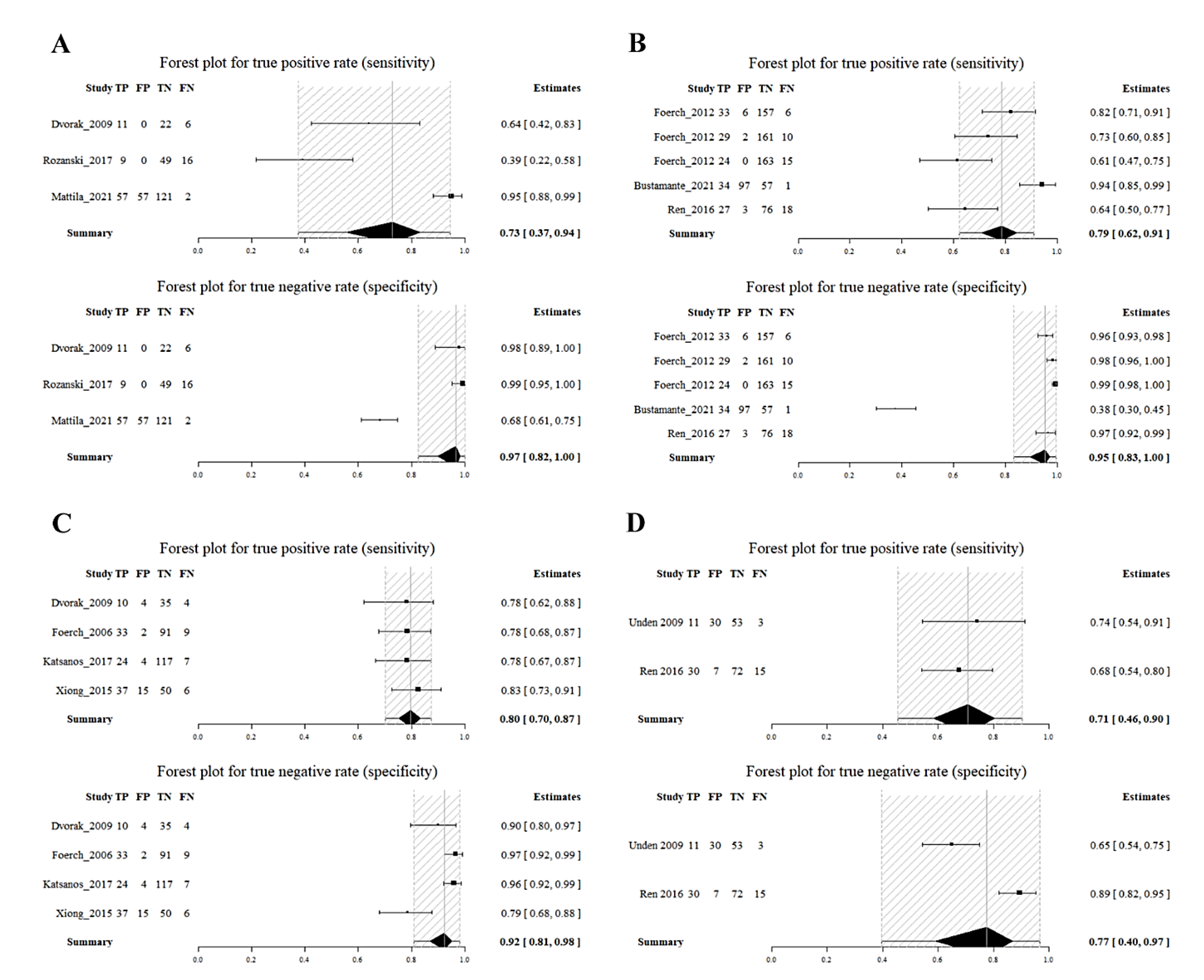
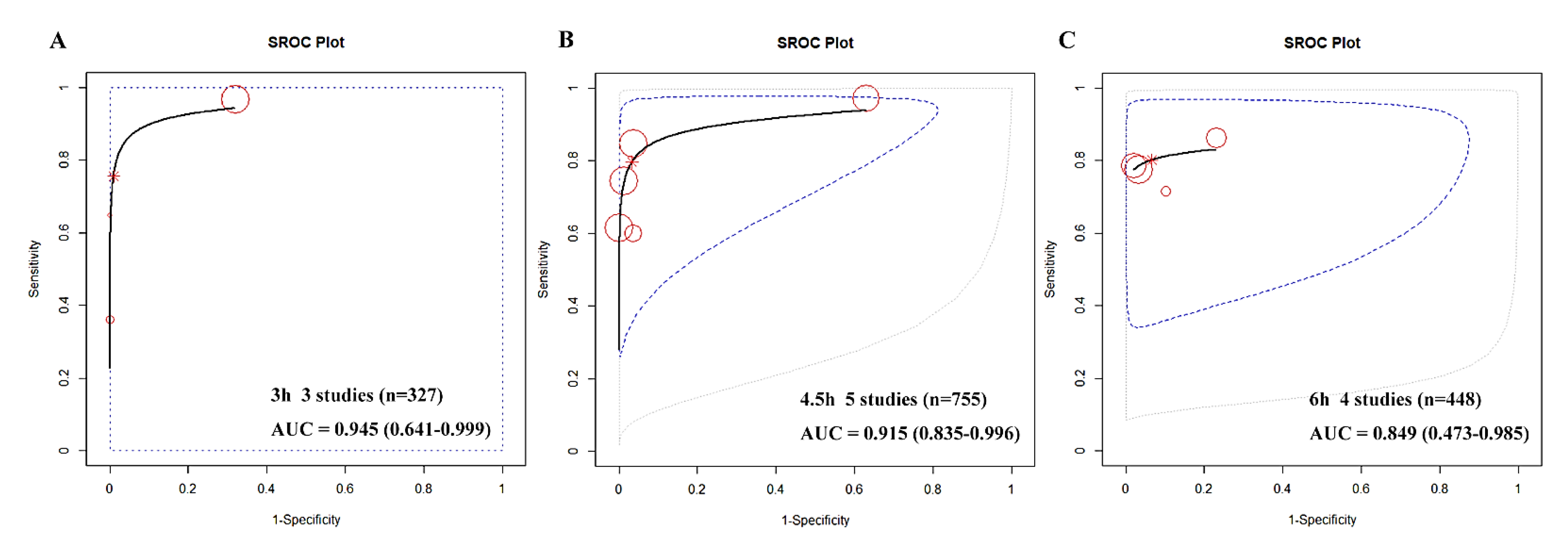
3.3. Quantitative Analysis and Meta-Analysis
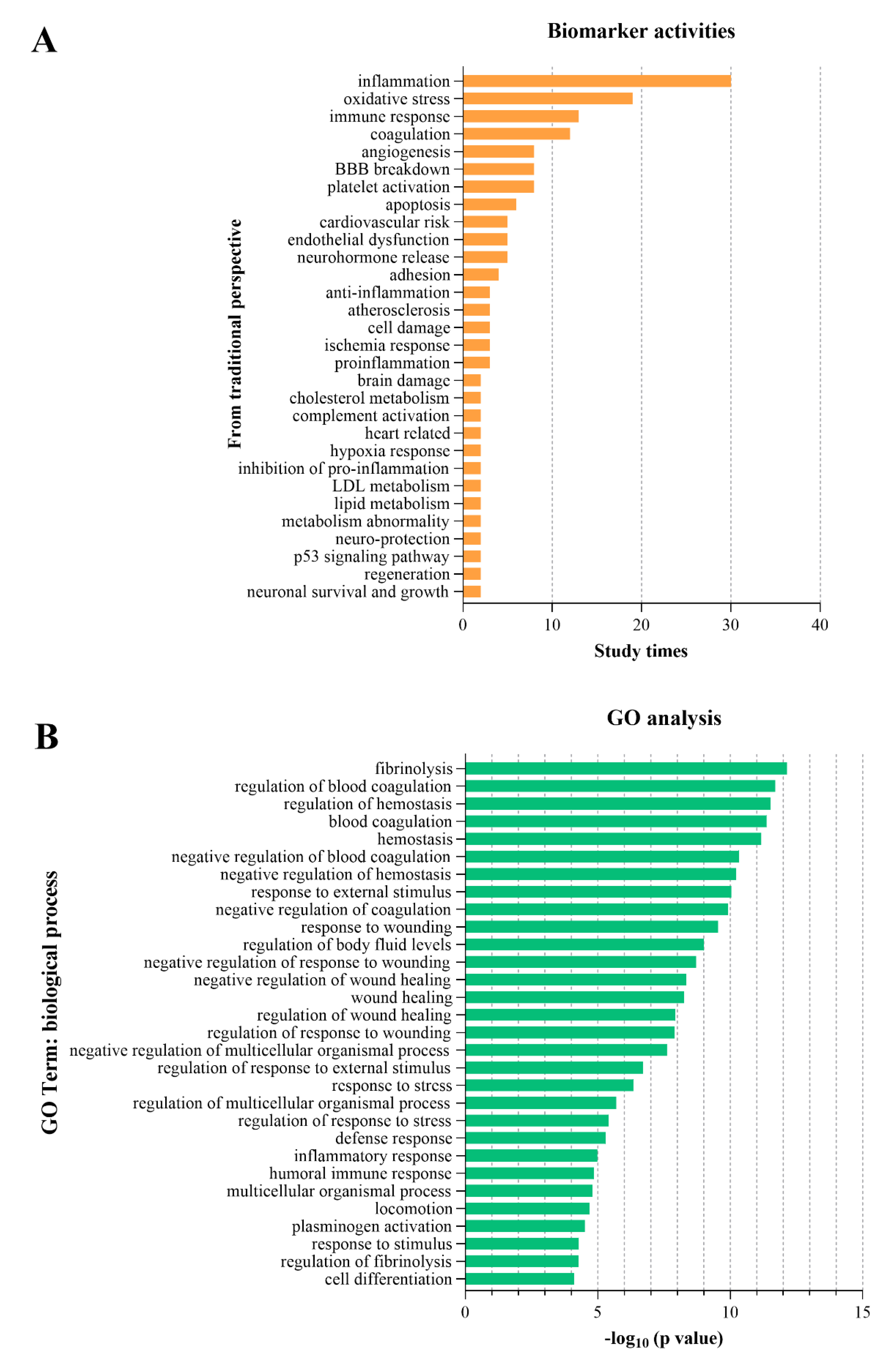
3.4. Biological Processes and GO Analysis
4. Discussion
4.1. The Shortlist of Biomarkers with Optimal Diagnostic Performance
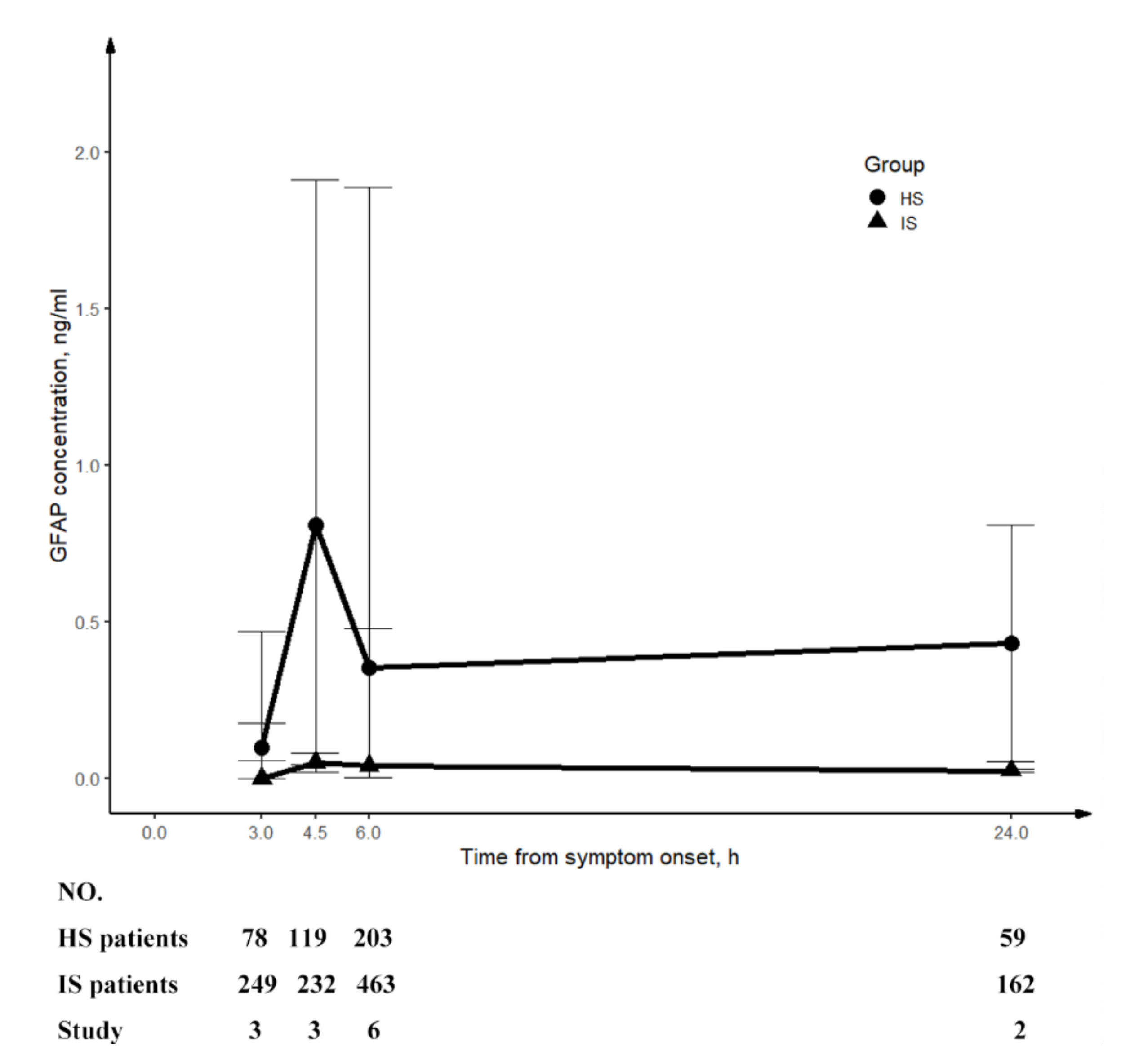
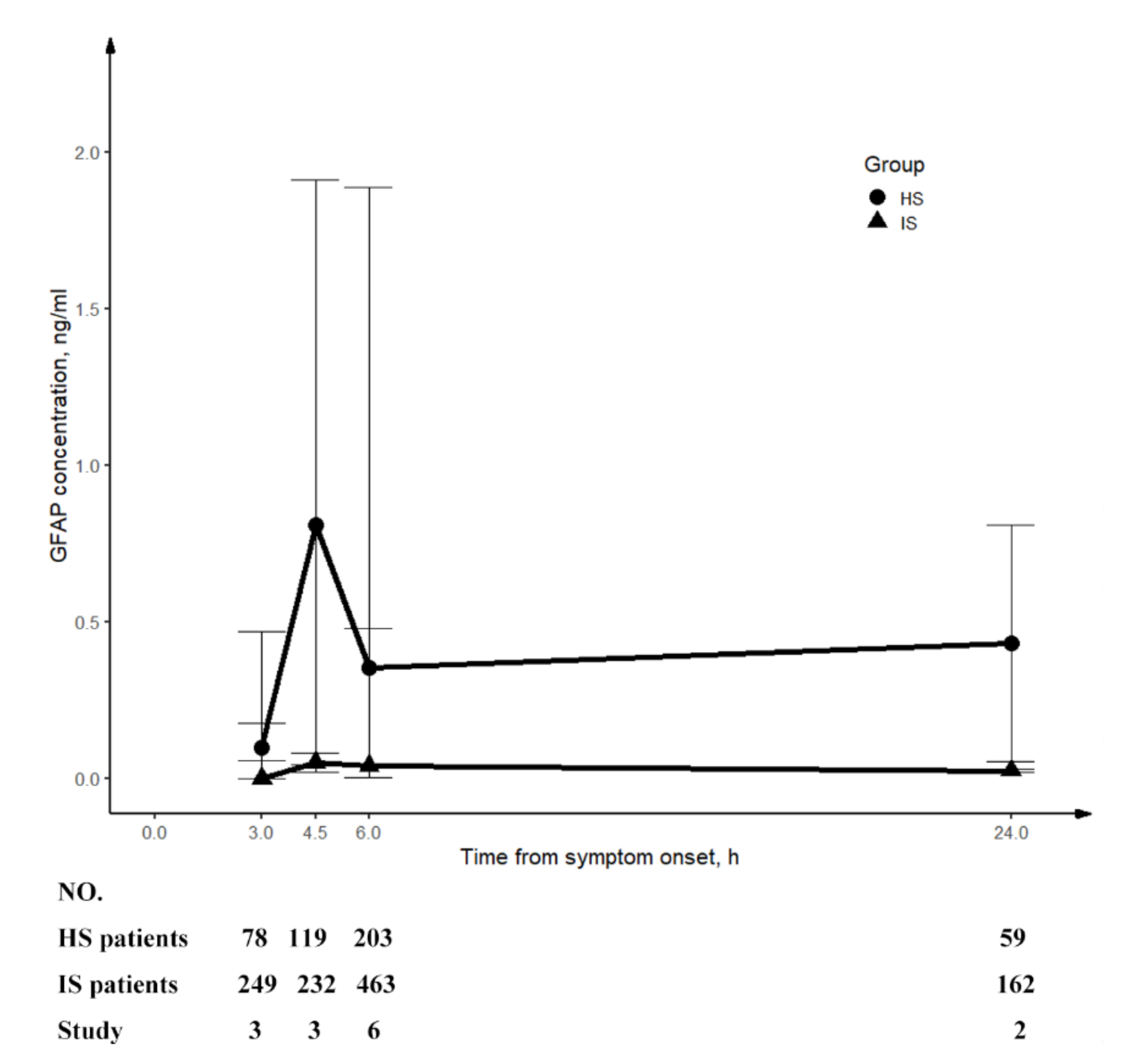
4.2. The Synthesis of GFAP
4.3. High-Throughput Omics Studies
4.4. Pivotal Biological Processes
4.5. Compare with Previous Related Studies
4.6. The Current Status and Recommendations for Future Research
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Campbell, B.C.V.; De Silva, D.A.; Macleod, M.R.; Coutts, S.B.; Schwamm, L.H.; Davis, S.M.; Donnan, G.A. Ischaemic stroke. Nat. Rev. Dis. Primers 2019, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.B.D.S. Global, regional, and national burden of stroke, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef] [PubMed]
- Tong, E.; Hou, Q.; Fiebach, J.B.; Wintermark, M. The role of imaging in acute ischemic stroke. Neurosurg. Focus. 2014, 36, E3. [Google Scholar] [CrossRef] [PubMed]
- Asci Erkocyigit, B.; Ozufuklar, O.; Yardim, A.; Guler Celik, E.; Timur, S. Biomarker Detection in Early Diagnosis of Cancer: Recent Achievements in Point-of-Care Devices Based on Paper Microfluidics. Biosensors 2023, 13, 387. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Yang, L.; Han, M.; Xu, H.; Ding, W.; Dong, X. CRISPR-cas technology: A key approach for SARS-CoV-2 detection. Front. Bioeng. Biotechnol. 2023, 11, 1158672. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Pu, X.; Jun, P.; Zhu, X.; Zhu, D.; Chen, M. Rapid and quantitative detection of C-reactive protein using quantum dots and immunochromatographic test strips. Int. J. Nanomed. 2014, 9, 5619–5626. [Google Scholar] [CrossRef]
- Park, H.D. Current Status of Clinical Application of Point-of-Care Testing. Arch. Pathol. Lab. Med. 2021, 145, 168–175. [Google Scholar] [CrossRef]
- Goyder, C.; Tan, P.S.; Verbakel, J.; Ananthakumar, T.; Lee, J.J.; Hayward, G.; Turner, P.J.; Van Den Bruel, A. Impact of point-of-care panel tests in ambulatory care: A systematic review and meta-analysis. BMJ Open 2020, 10, e032132. [Google Scholar] [CrossRef]
- Cooke, J.; Butler, C.; Hopstaken, R.; Dryden, M.S.; McNulty, C.; Hurding, S.; Moore, M.; Livermore, D.M. Narrative review of primary care point-of-care testing (POCT) and antibacterial use in respiratory tract infection (RTI). BMJ Open Respir. Res. 2015, 2, e000086. [Google Scholar] [CrossRef]
- Ramos-Fernandez, M.; Bellolio, M.F.; Stead, L.G. Matrix metalloproteinase-9 as a marker for acute ischemic stroke: A systematic review. J. Stroke Cerebrovasc. Dis. 2011, 20, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Montaner, J.; Ramiro, L.; Arora, R.; Talwar, P.; Nath, M.; Kumar, A.; Kumar, P.; Pandit, A.K.; Mohania, D.; et al. Blood biomarkers for the diagnosis and differentiation of stroke: A systematic review and meta-analysis. Int. J. Stroke 2020, 15, 704–721. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Wang, Q.; Zhu, R.; Yang, J. Circulating Non-coding RNAs as Potential Biomarkers for Ischemic Stroke: A Systematic Review. J. Mol. Neurosci. 2022, 72, 1572–1585. [Google Scholar] [CrossRef] [PubMed]
- Ke, C.; Pan, C.W.; Zhang, Y.; Zhu, X.; Zhang, Y. Metabolomics facilitates the discovery of metabolic biomarkers and pathways for ischemic stroke: A systematic review. Metabolomics 2019, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Baez, S.C.; Garcia Del Barco, D.; Hardy-Sosa, A.; Guillen Nieto, G.; Bringas-Vega, M.L.; Llibre-Guerra, J.J.; Valdes-Sosa, P. Scalable Bio Marker Combinations for Early Stroke Diagnosis: A Systematic Review. Front. Neurol. 2021, 12, 638693. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.; Ramiro, L.; Simats, A.; Tiedt, S.; Makris, K.; Jickling, G.C.; Debette, S.; Sanchez, J.C.; Bustamante, A. Multilevel omics for the discovery of biomarkers and therapeutic targets for stroke. Nat. Rev. Neurol. 2020, 16, 247–264. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; the PRISMA-DTA Group; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2 a revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Guo, J.; Riebler, A. meta4diag: Bayesian Bivariate Meta-Analysis of Diagnostic Test Studies for Routine Practice. arXiv 2018, arXiv:1512.06220. [Google Scholar] [CrossRef]
- Shin, J.J.; Zurakowski, D. Null Hypotheses, Interval Estimation, and Bayesian Analysis. Otolaryngol. Head. Neck Surg. 2017, 157, 919–920. [Google Scholar] [CrossRef] [PubMed]
- Granholm, A.; Alhazzani, W.; Moller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef]
- Ashburner, M.; Ball, C.A.; Blake, J.A.; Botstein, D.; Butler, H.; Cherry, J.M.; Davis, A.P.; Dolinski, K.; Dwight, S.S.; Eppig, J.T.; et al. Gene ontology: Tool for the unification of biology. The Gene Ontology Consortium. Nat. Genet. 2000, 25, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Gene Ontology, C.; Aleksander, S.A.; Balhoff, J.; Carbon, S.; Cherry, J.M.; Drabkin, H.J.; Ebert, D.; Feuermann, M.; Gaudet, P.; Harris, N.L.; et al. The Gene Ontology knowledgebase in 2023. Genetics 2023, 224, iyad031. [Google Scholar] [CrossRef]
- Raudvere, U.; Kolberg, L.; Kuzmin, I.; Arak, T.; Adler, P.; Peterson, H.; Vilo, J. g:Profiler: A web server for functional enrichment analysis and conversions of gene lists (2019 update). Nucleic Acids Res. 2019, 47, W191–W198. [Google Scholar] [CrossRef] [PubMed]
- Dambinova, S.A.; Khounteev, G.A.; Izykenova, G.A.; Zavolokov, I.G.; Ilyukhina, A.Y.; Skoromets, A.A. Blood test detecting autoantibodies to N-methyl-D-aspartate neuroreceptors for evaluation of patients with transient ischemic attack and stroke. Clin. Chem. 2003, 49, 1752–1762. [Google Scholar] [CrossRef] [PubMed]
- Algin, A.; Erdogan, M.O.; Aydin, I.; Poyraz, M.K.; Sirik, M. Clinical usefulness of brain-derived neurotrophic factor and visinin-like protein-1 in early diagnostic tests for acute stroke. Am. J. Emerg. Med. 2019, 37, 2051–2054. [Google Scholar] [CrossRef]
- Ahn, J.H.; Choi, S.C.; Lee, W.G.; Jung, Y.S. The usefulness of albumin-adjusted ischemia-modified albumin index as early detecting marker for ischemic stroke. Neurol. Sci. 2011, 32, 133–138. [Google Scholar] [CrossRef]
- Dambinova, S.A.; Bettermann, K.; Glynn, T.; Tews, M.; Olson, D.; Weissman, J.D.; Sowell, R.L. Diagnostic potential of the NMDA receptor peptide assay for acute ischemic stroke. PLoS ONE 2012, 7, e42362. [Google Scholar] [CrossRef]
- Park, K.Y.; Ay, I.; Avery, R.; Caceres, J.A.; Siket, M.S.; Pontes-Neto, O.M.; Zheng, H.; Rost, N.S.; Furie, K.L.; Sorensen, A.G.; et al. New biomarker for acute ischaemic stroke: Plasma glycogen phosphorylase isoenzyme BB. J. Neurol. Neurosurg. Psychiatry 2018, 89, 404–409. [Google Scholar] [CrossRef] [PubMed]
- AlGawwam, G.; Shake, M.E. Evaluation of glycogen phosphorylase bb (GPBB) level in serum as marker in diagnosis of acute ischemic stroke. Indian J. Forensic Med. Toxicol. 2021, 15, 1603–1608. [Google Scholar]
- Sharma, R.; Gowda, H.; Chavan, S.; Advani, J.; Kelkar, D.; Kumar, G.S.; Bhattacharjee, M.; Chaerkady, R.; Prasad, T.S.; Pandey, A.; et al. Proteomic Signature of Endothelial Dysfunction Identified in the Serum of Acute Ischemic Stroke Patients by the iTRAQ-Based LC-MS Approach. J. Proteome Res. 2015, 14, 2466–2479. [Google Scholar] [CrossRef] [PubMed]
- Stejskal, D.; Sporova, L.; Svestak, M.; Karpisek, M. Determination of serum visinin like protein-1 and its potential for the diagnosis of brain injury due to the stroke: A pilot study. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc Czech Repub. 2011, 155, 263–268. [Google Scholar] [CrossRef]
- Laterza, O.F.; Modur, V.R.; Crimmins, D.L.; Olander, J.V.; Landt, Y.; Lee, J.M.; Ladenson, J.H. Identification of novel brain biomarkers. Clin. Chem. 2006, 52, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.B.; Li, T.B.; Zhang, Z.; Ren, K.D.; Zheng, Z.F.; Peng, J.; Luo, X.J. The Diagnostic Value of Circulating Brain-specific MicroRNAs for Ischemic Stroke. Intern. Med. 2016, 55, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Qi, L. miR-124 Is Downregulated in Serum of Acute Cerebral Infarct Patients and Shows Diagnostic and Prognostic Value. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211035446. [Google Scholar] [CrossRef]
- Ji, Q.; Ji, Y.; Peng, J.; Zhou, X.; Chen, X.; Zhao, H.; Xu, T.; Chen, L.; Xu, Y. Increased Brain-Specific MiR-9 and MiR-124 in the Serum Exosomes of Acute Ischemic Stroke Patients. PLoS ONE 2016, 11, e0163645. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, J.; Han, R.; Liu, H.; Sun, D.; Liu, X. Downregulation of serum brain specific microRNA is associated with inflammation and infarct volume in acute ischemic stroke. J. Clin. Neurosci. 2015, 22, 291–295. [Google Scholar] [CrossRef]
- Zhao, X.; Yu, Y.; Xu, W.; Dong, L.; Wang, Y.; Gao, B.; Li, G.; Zhang, W. Apolipoprotein A1-Unique Peptide as a Diagnostic Biomarker for Acute Ischemic Stroke. Int. J. Mol. Sci. 2016, 17, 458. [Google Scholar] [CrossRef]
- Ewida, H.A.; Zayed, R.K.; Darwish, H.A.; Shaheen, A.A. Circulating lncRNAs HIF1A-AS2 and LINLK-A: Role and Relation to Hypoxia-Inducible Factor-1alpha in Cerebral Stroke Patients. Mol. Neurobiol. 2021, 58, 4564–4574. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, G.C.; Chantler, P.D.; Barr, T.L. Stroke-associated pattern of gene expression previously identified by machine-learning is diagnostically robust in an independent patient population. Genom. Data 2017, 14, 47–52. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, G.C.; Petrone, A.B.; Treadway, M.B.; Tennant, C.S.; Lucke-Wold, N.; Chantler, P.D.; Barr, T.L. Machine-learning approach identifies a pattern of gene expression in peripheral blood that can accurately detect ischaemic stroke. NPJ Genom. Med. 2016, 1, 16038. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.A.; Kirchick, H.J.; Dahlen, J.R.; Anderberg, J.M.; McPherson, P.H.; Nakamura, K.K.; Laskowitz, D.T.; Valkirs, G.E.; Buechler, K.F. Early Biomarkers of Stroke. Clin. Chem. 2003, 49, 1733–1739. [Google Scholar] [CrossRef] [PubMed]
- Stanca, D.M.; Marginean, I.C.; Soritau, O.; Dragos, C.; Marginean, M.; Muresanu, D.F.; Vester, J.C.; Rafila, A. GFAP and antibodies against NMDA receptor subunit NR2 as biomarkers for acute cerebrovascular diseases. J. Cell Mol. Med. 2015, 19, 2253–2261. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, G.C.; Stafford, P.; Walsh, K.B.; Adeoye, O.; Barr, T.L. High-Throughput Profiling of Circulating Antibody Signatures for Stroke Diagnosis Using Small Volumes of Whole Blood. Neurotherapeutics 2019, 16, 868–877. [Google Scholar] [CrossRef] [PubMed]
- Llombart, V.; Garcia-Berrocoso, T.; Bustamante, A.; Giralt, D.; Rodriguez-Luna, D.; Muchada, M.; Penalba, A.; Boada, C.; Hernandez-Guillamon, M.; Montaner, J. Plasmatic retinol-binding protein 4 and glial fibrillary acidic protein as biomarkers to differentiate ischemic stroke and intracerebral hemorrhage. J. Neurochem. 2016, 136, 416–424. [Google Scholar] [CrossRef]
- Luger, S.; Witsch, J.; Dietz, A.; Hamann, G.F.; Minnerup, J.; Schneider, H.; Sitzer, M.; Wartenberg, K.E.; Niessner, M.; Foerch, C.; et al. Glial Fibrillary Acidic Protein Serum Levels Distinguish between Intracerebral Hemorrhage and Cerebral Ischemia in the Early Phase of Stroke. Clin. Chem. 2017, 63, 377–385. [Google Scholar] [CrossRef]
- Abdelhak, A.; Foschi, M.; Abu-Rumeileh, S.; Yue, J.K.; D’Anna, L.; Huss, A.; Oeckl, P.; Ludolph, A.C.; Kuhle, J.; Petzold, A.; et al. Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat. Rev. Neurol. 2022, 18, 158–172. [Google Scholar] [CrossRef]
- Jaeger, H.S.; Tranberg, D.; Larsen, K.; Valentin, J.B.; Blauenfeldt, R.A.; Luger, S.; Bache, K.G.; Gude, M.F. Diagnostic performance of Glial Fibrillary Acidic Protein and Prehospital Stroke Scale for identification of stroke and stroke subtypes in an unselected patient cohort with symptom onset < 4.5 h. Scand. J. Trauma. Resusc. Emerg. Med. 2023, 31, 1. [Google Scholar] [CrossRef]
- Tiedt, S.; Brandmaier, S.; Kollmeier, H.; Duering, M.; Artati, A.; Adamski, J.; Klein, M.; Liebig, T.; Holdt, L.M.; Teupser, D.; et al. Circulating Metabolites Differentiate Acute Ischemic Stroke from Stroke Mimics. Ann. Neurol. 2020, 88, 736–746. [Google Scholar] [CrossRef] [PubMed]
- Simats, A.; Ramiro, L.; Garcia-Berrocoso, T.; Brianso, F.; Gonzalo, R.; Martin, L.; Sabe, A.; Gill, N.; Penalba, A.; Colome, N.; et al. A Mouse Brain-based Multi-omics Integrative Approach Reveals Potential Blood Biomarkers for Ischemic Stroke. Mol. Cell Proteom. 2020, 19, 1921–1936. [Google Scholar] [CrossRef]
- Wang, T.X.; Shao, W.; Huang, Z.; Tang, H.X.; Zhang, J.; Ding, Z.M.; Huang, K. MOGONET integrates multi-omics data using graph convolutional networks allowing patient classification and biomarker identification. Nat. Commun. 2021, 12, 3445. [Google Scholar] [CrossRef] [PubMed]
- Dirnagl, U.; Iadecola, C.; Moskowitz, M.A. Pathobiology of ischaemic stroke: An integrated view. Trends Neurosci. 1999, 22, 391–397. [Google Scholar] [CrossRef]
- Perry, L.A.; Lucarelli, T.; Penny-Dimri, J.C.; McInnes, M.D.; Mondello, S.; Bustamante, A.; Montaner, J.; Foerch, C.; Kwan, P.; Davis, S.; et al. Glial fibrillary acidic protein for the early diagnosis of intracerebral hemorrhage: Systematic review and meta-analysis of diagnostic test accuracy. Int. J. Stroke 2019, 14, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Misra, S.; Yadav, A.K.; Sagar, R.; Verma, B.; Grover, A.; Prasad, K. Role of glial fibrillary acidic protein as a biomarker in differentiating intracerebral haemorrhage from ischaemic stroke and stroke mimics: A meta-analysis. Biomarkers 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarkers | Study ID | Levels | Sampling Time | Sensitivity | Specificity | AUC | Comparison Groups | Sample Size | Biological Process | |
|---|---|---|---|---|---|---|---|---|---|---|
| Antibody to NR 2A/2B | Dambinova 2003 [27] | Protein | 3 h | 97% | 98% | 0.99 | IS 1 | HC 230 + VC 25 + ICH 18 | 304 | Immune response |
| BDNF | Algin 2019 [28] | Protein | 4 h | 100% | 92% | 0.983 | IS 75 | HC 28 | 103 | Neuronal survival and growth |
| IMA index | Ahn 2011 [29] | Protein | 6 h | 95.8% | 96.4% | 0.99 | IS 28 | SM 24 | 52 | Ischemia response |
| NR2 peptide | Dambinova 2012 [30] | Protein | 12 h | 92.1% | 96.5% | 0.92 | IS 50 | SM 91 + VC 48 + HC 52 | 241 | Brain cell damage |
| GPBB | Park 2018 [31] | Protein | 12 h | 93% | 93% | 0.96 | IS 172 | NSC 133 | 305 | Ischaemia response |
| Algawwam 2021 [32] | Protein | 24 h | N/A | N/A | N/A | IS 40 | HC 40 | 80 | ||
| ADAMTS13 | Sharma 2015 [33] | Proteomics | 24 h | 90% | 98% | 0.96 | IS 50 | HC 35 | 85 | Blood haemostasis and endothelial function regulation |
| S100A7 | Sharma 2015 [33] | Proteomics | 24 h | 97% | 91% | 0.912 | IS 50 | HC 35 | 85 | Blood haemostasis and endothelial function regulation |
| VILIP-1 | Stejskal 2011 [34] | Protein | 3 h | 100% | 100% | 1.0 | IS 16 | HC 17 | 33 | Brain cell damage |
| Laterza 2006 [35] | Protein | 24 h | N/A | N/A | N/A | IS 18 | HC N/A | 18 | ||
| Algin 2019 [28] | Protein | 4 h | No statistical significance | IS 75 | HC 28 | 103 | ||||
| miR-107 | Yang 2016 [36] | Transcript | 24 h | 93.8% | 92.2% | 0.97 | IS 114 | HC58 | 172 | Cerebral ischaemic injury |
| miR-124 | Zhou 2021 [37] | Transcript | 24 h | 91.67% | 93.52% | 0.9527 | IS 108 | HC 108 | 216 | Anti-inflammation |
| Ji 2016 [38] | Transcript | 24 h | N/A | N/A | 0.69 | IS 65 | NSC 66 | 131 | ||
| Liu 2015 [39] | Transcript | 24 h | N/A | N/A | 0.76 | IS 31 | HC 11 | 42 | ||
| APOA1-UP | Zhao 2016 [40] | Protein | 24 h | 90.3% | 97.14% | 0.975 | IS 168 | HC 104 | 272 | Cholesterol metabolism |
| lncRNAs LINK-A | Ewida 2021 [41] | Transcript | 24 h | 92% | 94% | 0.914 | IS 50 | HS 25 | 75 | Angiogenesis |
| ANTXR2 + STK3 + PDK4 + CD163 + MAL + GRAP + ID3 + KIF1B + PLXDC2 + CTSZ | O’Connell 2017 [42] | Gene | 5 h, 24 h | 95.7% | 95.7% | 0.997 | IS 23 | VC 23 | 46 | Immune response |
| O’Connell 2017 [42] | Gene | 3 h | 91.3% | 95.7% | 0.991 | IS 23 | VC 23 | 46 | ||
| O’Connell 2016 [43] | Genomics | 5.3 h | 97.4% | 100% | N/A | IS 39 | NAC 24 | 63 | ||
| O’Connell 2016 [43] | Genomics | 4.6 h | 92.3% | 100% | N/A | IS 39 | NAC 24 | 63 | ||
| O’Connell 2016 [43] | Genomics | 4.6 h | 97.4% | 90% | N/A | IS 39 | SM 20 | 59 | ||
| S100B + BNGF + vWF + MMP9 + MCP-1 | Reynolds 2003 [44] | Protein | 3 h | 98.1% | 91.7% | N/A | IS 82 | HS 103 + HC 214 + TBI 38 | 437 | Brain cell damage, neuronal survive, coagulation, inflammation |
| Reynolds 2003 [44] | Protein | 6 h | 98.1% | 93.1% | N/A | IS 82 | HS 103 + HC 214 + TBI 38 | 437 | ||
| GFAP+ antibody against NR2 | Stanca 2015 [45] | Protein | 12 h | 94% | 91% | N/A | IS 49 | HS 23 | 72 | Brain cell damage, immune response |
| 17-peptide-panel | O’Connell 2019 [46] | Proteomics | 12 h | 93.3% | 90% | 0.95 | IS 19 | HS 17 | 36 | Immune response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Q.; Zhao, L.; Chan, C.L.; Zhang, Y.; Tong, S.W.; Zhang, X.; Ho, J.W.K.; Jiao, Y.; Rainer, T.H. Multi-Level Biomarkers for Early Diagnosis of Ischaemic Stroke: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 13821. https://doi.org/10.3390/ijms241813821
Li Q, Zhao L, Chan CL, Zhang Y, Tong SW, Zhang X, Ho JWK, Jiao Y, Rainer TH. Multi-Level Biomarkers for Early Diagnosis of Ischaemic Stroke: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(18):13821. https://doi.org/10.3390/ijms241813821
Chicago/Turabian StyleLi, Qianyun, Lingyun Zhao, Ching Long Chan, Yilin Zhang, See Wai Tong, Xiaodan Zhang, Joshua Wing Kei Ho, Yaqing Jiao, and Timothy Hudson Rainer. 2023. "Multi-Level Biomarkers for Early Diagnosis of Ischaemic Stroke: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 18: 13821. https://doi.org/10.3390/ijms241813821
APA StyleLi, Q., Zhao, L., Chan, C. L., Zhang, Y., Tong, S. W., Zhang, X., Ho, J. W. K., Jiao, Y., & Rainer, T. H. (2023). Multi-Level Biomarkers for Early Diagnosis of Ischaemic Stroke: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 24(18), 13821. https://doi.org/10.3390/ijms241813821