
HLA Class I Expression Is Associated with DNA Damage and Immune Cell Infiltration into Dysplastic and Neoplastic Lesions in Ulcerative Colitis


 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
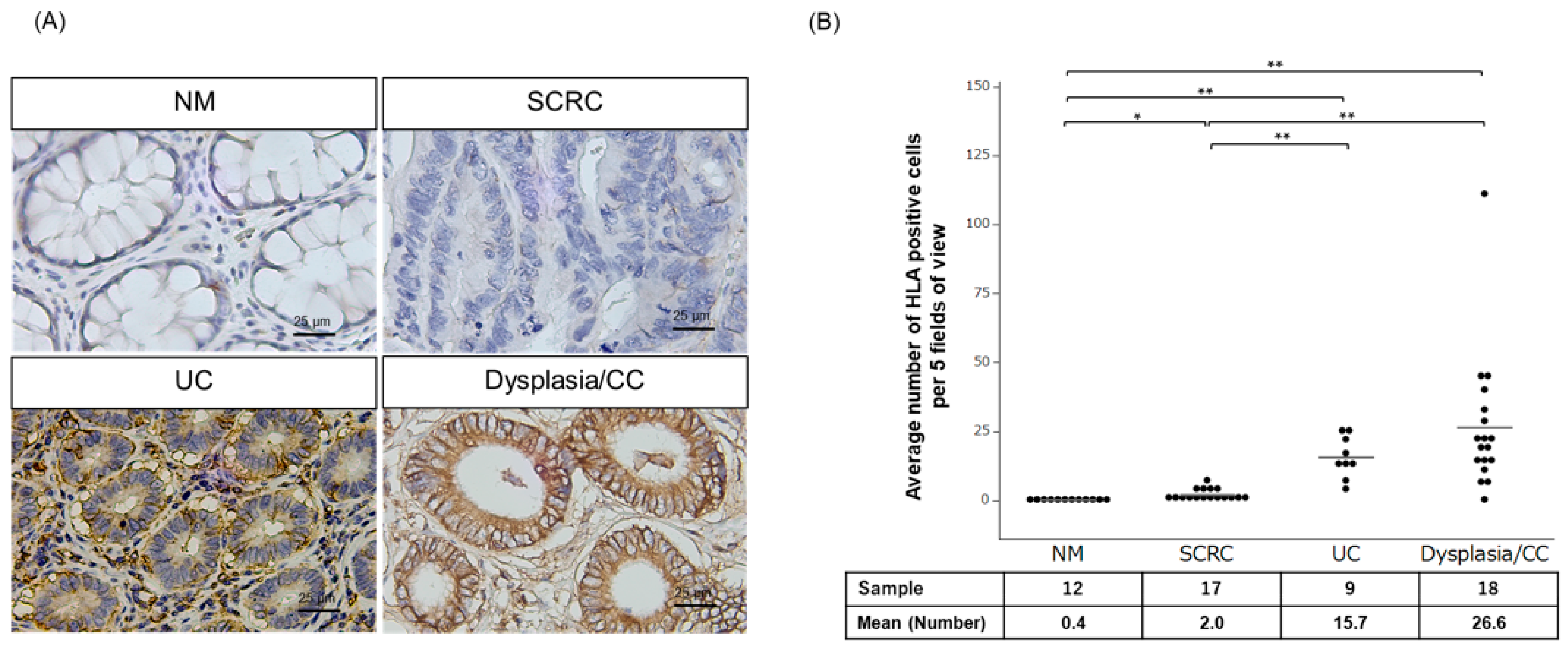
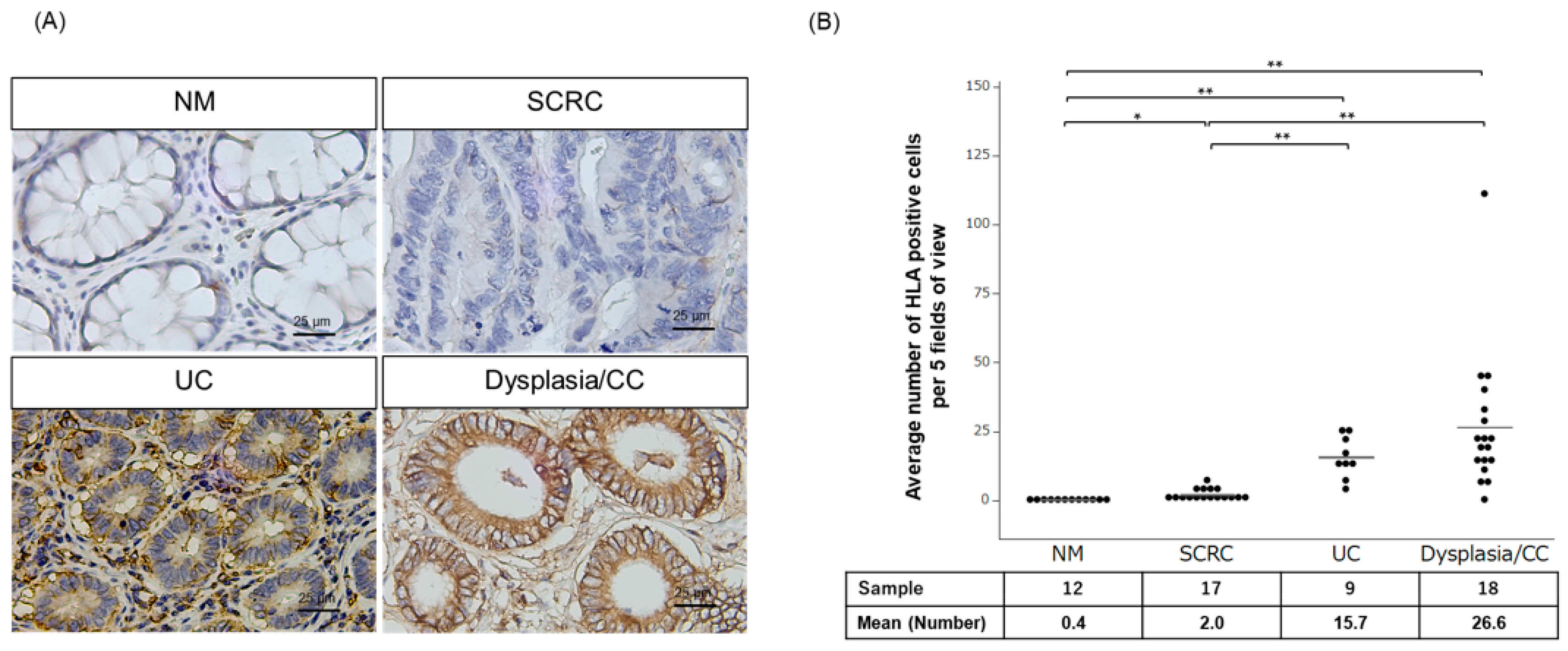
2.1. Evaluation of Membrane HLA-I Expressing Epithelial Cells in Tissues of Patients with SCRC and Dysplasia/Colitic Cancer
2.2. Relationship between HLA-I Expression, DNA Damage, and PD-L1 Expression in SCRC and Dysplasia/CC
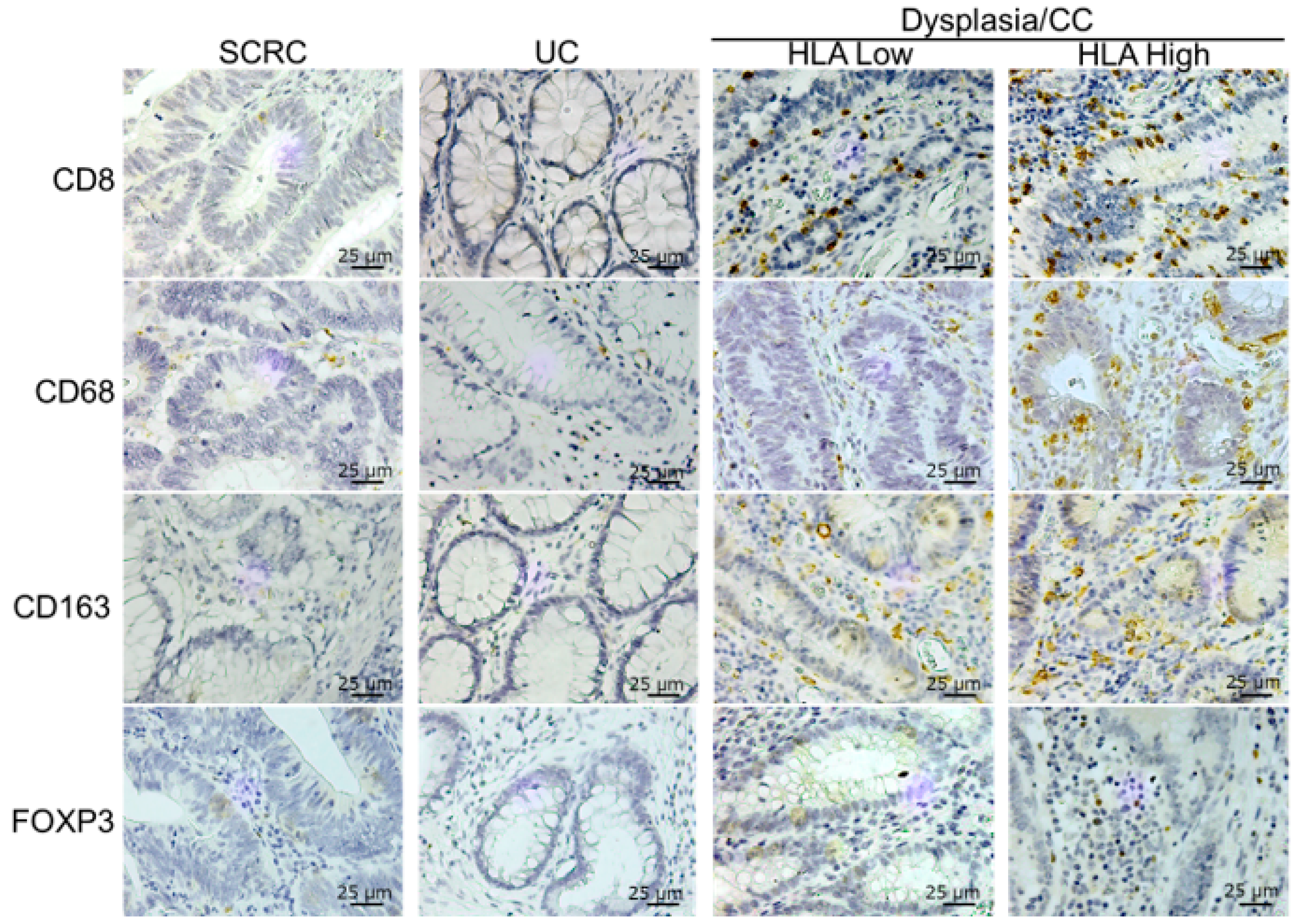
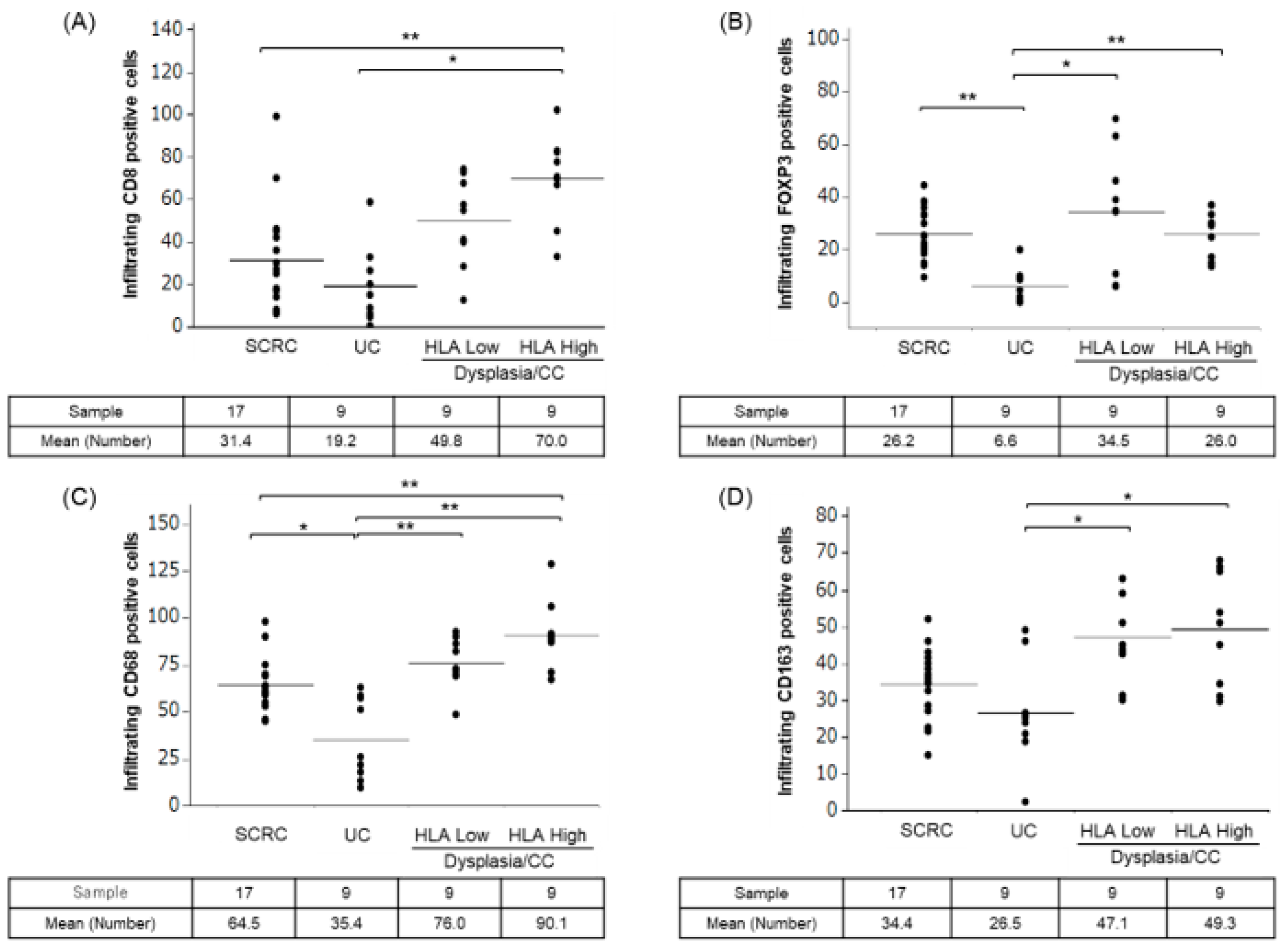
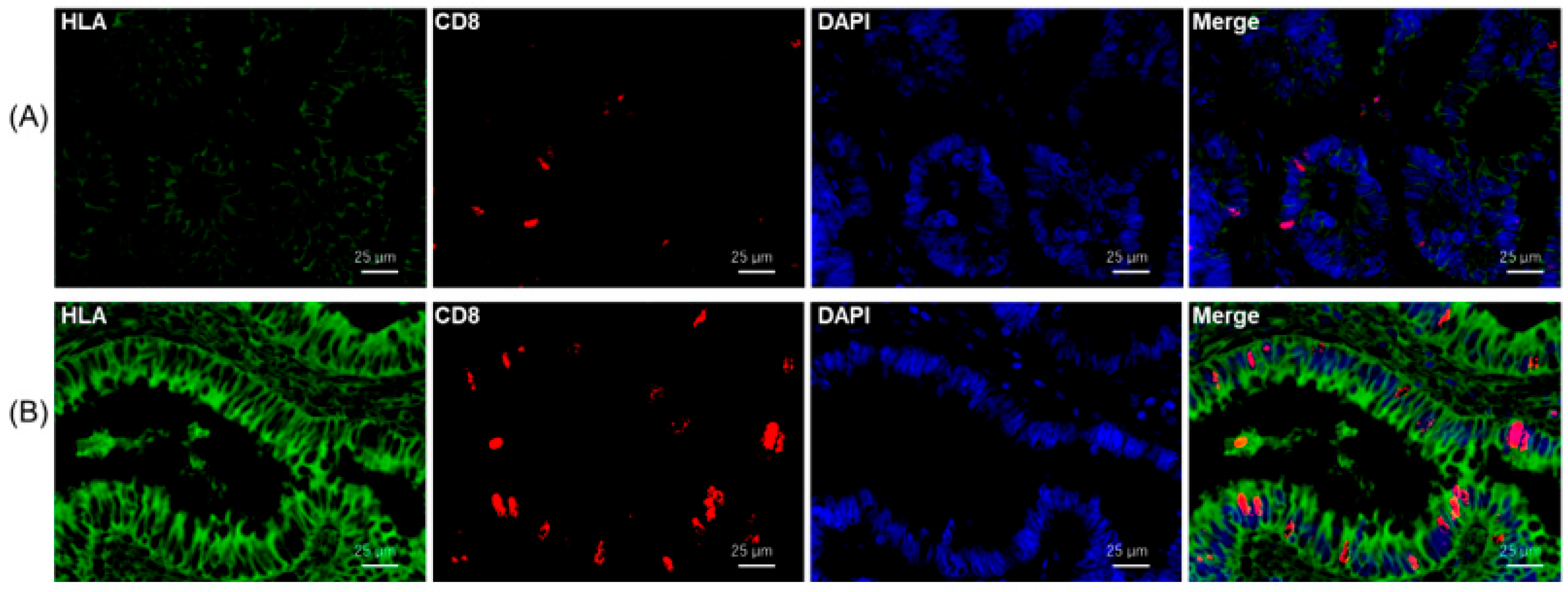
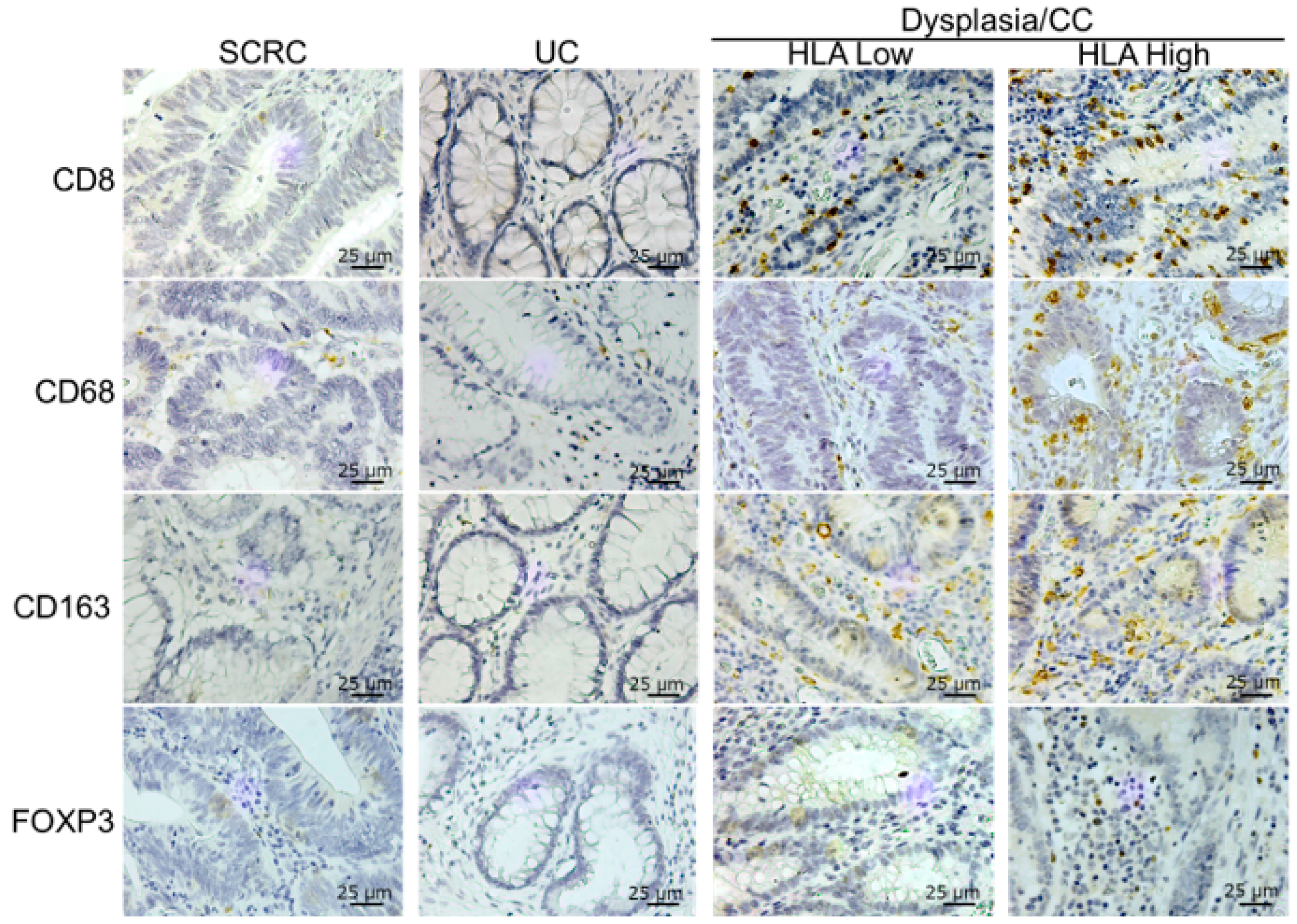
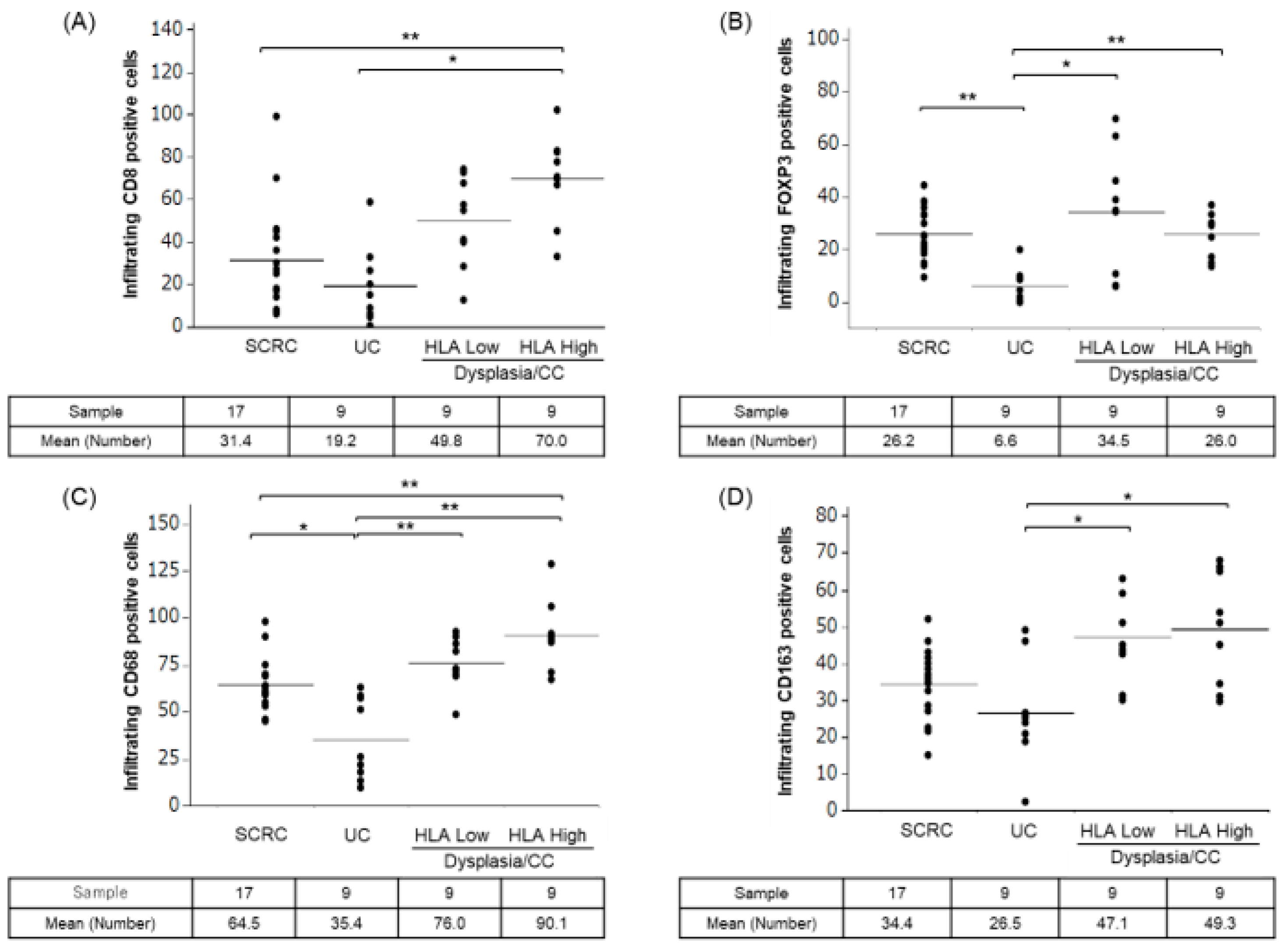
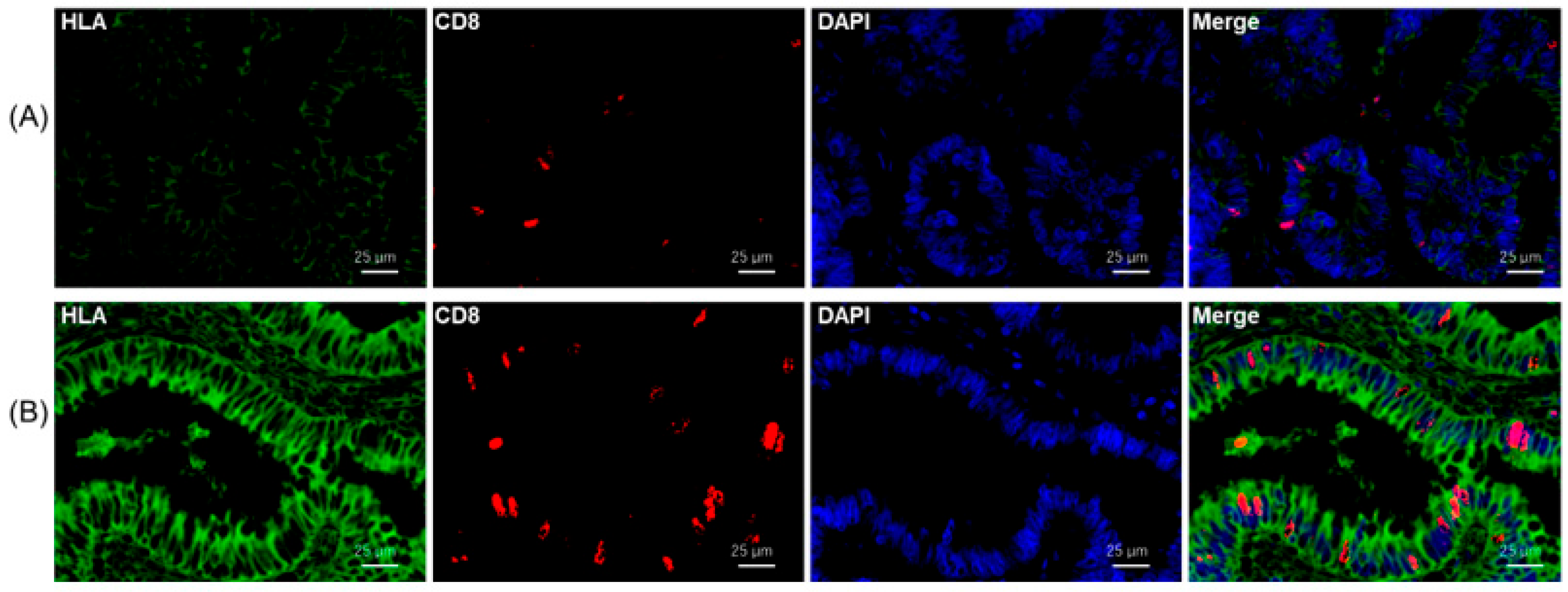
2.3. Immune Cell Infiltration in Tissues of SCRC, UC, and Dysplasia/CC with Low and High HLA-I
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. Immunohistochemical Staining
4.3. Immunohistochemical Evaluation
4.4. Multicolor Immunofluorescence Staining for HLA-I and CD8
4.5. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baron, J.A. Aspirin and NSAIDs for the prevention of colorectal cancer. Recent Results Cancer Res. 2009, 181, 223–229. [Google Scholar] [CrossRef]
- Rothwell, P.M. Aspirin in prevention of sporadic colorectal cancer: Current clinical evidence and overall balance of risks and benefits. Recent Results Cancer Res. 2013, 191, 121–142. [Google Scholar] [CrossRef]
- Kmietowicz, Z. Study finds that aspirin improves survival after colon cancer diagnosis. BMJ 2014, 348, g2476. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, G.; Pallone, F.; Stolfi, C. The dual role of inflammation in colon carcinogenesis. Int. J. Mol. Sci. 2012, 13, 11071–11084. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, R.; Ikeuchi, H.; Horio, Y.; Minagawa, T.; Kusunoki, K.; Uchino, M. Have advances in medical therapy for ulcerative colitis impacted surgical treatment? Ann. Gastroenterol. Surg. 2023, 7, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Marshall, S.E.; Jewell, D. Genetics of inflammatory bowel disease: The role of the HLA complex. World J. Gastroenterol. 2006, 12, 3628–3635. [Google Scholar] [CrossRef] [PubMed]
- Oike, N.; Kawashima, H.; Ogose, A.; Hatano, H.; Ariizumi, T.; Yamagishi, T.; Murayama, Y.; Umezu, H.; Imai, C.; Hayashi, M.; et al. Human leukocyte antigen I is significantly downregulated in patients with myxoid liposarcomas. Cancer Immunol. Immunother. 2021, 70, 3489–3499. [Google Scholar] [CrossRef]
- Ogose, A.; Kawashima, H.; Hotta, T.; Ariizumi, T.; Yamagishi, T.; Oike, N.; Sasaki, T.; Hatano, H.; Umezu, H.; Endo, N. Frequent expression of human leukocyte antigen class I and the status of intratumoral immune cells in alveolar soft part sarcoma. Oncol. Lett. 2017, 13, 2169–2176. [Google Scholar] [CrossRef]
- Asahi, Y.; Hatanaka, K.C.; Hatanaka, Y.; Kamiyama, T.; Orimo, T.; Shimada, S.; Nagatsu, A.; Sakamoto, Y.; Kamachi, H.; Kobayashi, N.; et al. Prognostic impact of CD8+ T cell distribution and its association with the HLA class I expression in intrahepatic cholangiocarcinoma. Surg. Today 2020, 50, 931–940. [Google Scholar] [CrossRef]
- Sato, H.; Suzuki, Y.; Ide, M.; Katoh, T.; Noda, S.E.; Ando, K.; Oike, T.; Yoshimoto, Y.; Okonogi, N.; Mimura, K.; et al. HLA class I expression and its alteration by preoperative hyperthermo-chemoradiotherapy in patients with rectal cancer. PLoS ONE 2014, 9, e108122. [Google Scholar] [CrossRef]
- Möller, P.; Koretz, K.; Schlag, P.; Momburg, F. Frequency of abnormal expression of HLA-A,B,C and HLA-DR molecules, invariant chain, and LFA-3 (CD58) in colorectal carcinoma and its impact on tumor recurrence. Int. J. Cancer Suppl. 1991, 6, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, T.; Collado, A.; Fernandez, M.A.; Ferron, A.; Sancho, J.; Ruiz-Cabello, F.; Garrido, F. High frequency of altered HLA class I phenotypes in invasive colorectal carcinomas. Tissue Antigens 1998, 52, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Lampen, M.H.; van Hall, T. Strategies to counteract MHC-I defects in tumors. Curr. Opin. Immunol. 2011, 23, 293–298. [Google Scholar] [CrossRef]
- Ugurel, S.; Spassova, I.; Wohlfarth, J.; Drusio, C.; Cherouny, A.; Melior, A.; Sucker, A.; Zimmer, L.; Ritter, C.; Schadendorf, D.; et al. MHC class-I downregulation in PD-1/PD-L1 inhibitor refractory Merkel cell carcinoma and its potential reversal by histone deacetylase inhibition: A case series. Cancer Immunol. Immunother. 2019, 68, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; Aptsiauri, N.; Ruiz-Cabello, F.; Garrido, F. HLA class I loss in colorectal cancer: Implications for immune escape and immunotherapy. Cell. Mol. Immunol. 2021, 18, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Uchihara, Y.; Permata, T.B.M.; Sato, H.; Kawabata-Iwakawa, R.; Katada, S.; Gu, W.; Kakoti, S.; Yamauchi, M.; Kato, R.; Gondhowiardjo, S.; et al. DNA damage promotes HLA class I presentation by stimulating a pioneer round of translation-associated antigen production. Mol. Cell 2022, 82, 2557–2570.e2557. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Niimi, A.; Yasuhara, T.; Permata, T.B.M.; Hagiwara, Y.; Isono, M.; Nuryadi, E.; Sekine, R.; Oike, T.; Kakoti, S.; et al. DNA double-strand break repair pathway regulates PD-L1 expression in cancer cells. Nat. Commun. 2017, 8, 1751. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, N.; Yokobori, T.; Osone, K.; Katayama, C.; Suga, K.; Komine, C.; Shibasaki, Y.; Shiraishi, T.; Okada, T.; Kato, R.; et al. PD-L1 upregulation is associated with activation of the DNA double-strand break repair pathway in patients with colitic cancer. Sci. Rep. 2021, 11, 13077. [Google Scholar] [CrossRef]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Osone, K.; Yokobori, T.; Katayama, C.; Takahashi, R.; Kato, R.; Tatsuski, H.; Takada, T.; Yajima, R.; Motegi, Y.; Ogawa, H.; et al. STMN1 accumulation is associated with dysplastic and neoplastic lesions in patients with ulcerative colitis. Oncol. Lett. 2019, 18, 4712–4718. [Google Scholar] [CrossRef]
- Ashton, J.J.; Latham, K.; Beattie, R.M.; Ennis, S. Review article: The genetics of the human leucocyte antigen region in inflammatory bowel disease. Aliment Pharmacol. Ther. 2019, 50, 885–900. [Google Scholar] [CrossRef] [PubMed]
- Bouma, G.; Oudkerk Pool, M.; Crusius, J.B.; Schreuder, G.M.; Hellemans, H.P.; Meijer, B.U.; Kostense, P.J.; Giphart, M.J.; Meuwissen, S.G.; Peña, A.S. Evidence for genetic heterogeneity in inflammatory bowel disease (IBD); HLA genes in the predisposition to suffer from ulcerative colitis (UC) and Crohn’s disease (CD). Clin. Exp. Immunol. 1997, 109, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Stefanile, R.; Camarca, A.; Giliberti, P.; Cosentini, E.; Marano, C.; Iaquinto, G.; Giardullo, N.; Auricchio, S.; Sette, A.; et al. Gliadin activates HLA class I-restricted CD8+ T cells in celiac disease intestinal mucosa and induces the enterocyte apoptosis. Gastroenterology 2008, 134, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Hazini, A.; Fisher, K.; Seymour, L. Deregulation of HLA-I in cancer and its central importance for immunotherapy. J. Immunother. Cancer 2021, 9, e002899. [Google Scholar] [CrossRef] [PubMed]
- Ullman, T.A.; Itzkowitz, S.H. Intestinal inflammation and cancer. Gastroenterology 2011, 140, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.J.; Arends, M.J.; Churchhouse, A.M.D.; Din, S. Inflammatory Bowel Disease-Associated Colorectal Cancer: Translational Risks from Mechanisms to Medicines. J. Crohns Colitis 2021, 15, 2131–2141. [Google Scholar] [CrossRef] [PubMed]
- Courtney, E.D.; Melville, D.M.; Leicester, R.J. Review article: Chemoprevention of colorectal cancer. Aliment Pharmacol. Ther. 2004, 19, 1–24. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Fowkes, F.G.; Belch, J.F.; Ogawa, H.; Warlow, C.P.; Meade, T.W. Effect of daily aspirin on long-term risk of death due to cancer: Analysis of individual patient data from randomised trials. Lancet 2011, 377, 31–41. [Google Scholar] [CrossRef]
- Qiu, X.; Ma, J.; Wang, K.; Zhang, H. Chemopreventive effects of 5-aminosalicylic acid on inflammatory bowel disease-associated colorectal cancer and dysplasia: A systematic review with meta-analysis. Oncotarget 2017, 8, 1031–1045. [Google Scholar] [CrossRef]
- Chen, Y.; Sun, L.; Li, D.; Yin, X.; Shang, G.; Diao, T.; Shi, L. Aspirin Inhibits Carcinogenesis of Intestinal Mucosal Cells in UC Mice Through Inhibiting IL-6/JAK/STAT3 Signaling Pathway and Modulating Apoptosis and Proliferation. Turk. J. Gastroenterol. 2022, 33, 731–742. [Google Scholar] [CrossRef]
- Ohnishi, S.; Hiramoto, K.; Ma, N.; Kawanishi, S. Chemoprevention by aspirin against inflammation-related colorectal cancer in mice. J. Clin. Biochem. Nutr. 2021, 69, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Köhnke, T.; Gomolka, B.; Bilal, S.; Zhou, X.; Sun, Y.; Rothe, M.; Baumgart, D.C.; Weylandt, K.H. Acetylsalicylic Acid reduces the severity of dextran sodium sulfate-induced colitis and increases the formation of anti-inflammatory lipid mediators. Biomed. Res. Int. 2013, 2013, 748160. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.J.; Bie, C.Q.; Guo, L.L.; Zhong, L.X.; Tang, S.H. Efficacy and safety of vedolizumab in the treatment of patients with inflammatory bowel disease: A systematic review and meta-analysis of randomized controlled trials. Exp. Ther. Med. 2023, 25, 298. [Google Scholar] [CrossRef] [PubMed]
- Besendorf, L.; Müller, T.M.; Geppert, C.I.; Schneider, I.; Mühl, L.; Atreya, I.; Vitali, F.; Atreya, R.; Neurath, M.F.; Zundler, S. Vedolizumab blocks α4β7 integrin-mediated T cell adhesion to MAdCAM-1 in microscopic colitis. Therap. Adv. Gastroenterol. 2022, 15, 17562848221098899. [Google Scholar] [CrossRef] [PubMed]
- Domènech, E.; Gisbert, J.P. Efficacy and safety of vedolizumab in the treatment of ulcerative colitis. Gastroenterol. Hepatol. 2016, 39, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.J.; Danese, S.; et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Burisch, J.; Ben-Horin, S.; Braegger, F.; Fernández-Nistal, A.; Lara, N.; Heinrich, H.S.; Vavricka, S.R. Impact of Vedolizumab on Extraintestinal Manifestations in Inflammatory Bowel Disease: Results From a Descriptive, Retrospective, Real-world Study. Inflamm. Bowel Dis. 2023, izad075. [Google Scholar] [CrossRef]
- Reinisch, W.; Sandborn, W.J.; Danese, S.; Hébuterne, X.; Kłopocka, M.; Tarabar, D.; Vaňásek, T.; Greguš, M.; Hellstern, P.A.; Kim, J.S.; et al. Long-term Safety and Efficacy of the Anti-MAdCAM-1 Monoclonal Antibody Ontamalimab [SHP647] for the Treatment of Ulcerative Colitis: The Open-label Study TURANDOT II. J. Crohns Colitis 2021, 15, 938–949. [Google Scholar] [CrossRef]
- D’Haens, G.R.; Reinisch, W.; Lee, S.D.; Tarabar, D.; Louis, E.; Kłopocka, M.; Klaus, J.; Schreiber, S.; Il Park, D.; Hébuterne, X.; et al. Long-Term Safety and Efficacy of the Anti-Mucosal Addressin Cell Adhesion Molecule-1 Monoclonal Antibody Ontamalimab (SHP647) for the Treatment of Crohn’s Disease: The OPERA II Study. Inflamm. Bowel Dis. 2022, 28, 1034–1044. [Google Scholar] [CrossRef]
- Jung, M.; Rose, M.; Knuechel, R.; Loeffler, C.; Muti, H.; Kather, J.N.; Gaisa, N.T.; on behalf of the German Study Group of Bladder Cancer (DFBK e.V.). Characterisation of tumour-immune phenotypes and PD-L1 positivity in squamous bladder cancer. BMC Cancer 2023, 23, 113. [Google Scholar] [CrossRef]
- Wang, T.; Luo, Y.; Zhang, Q.; Shen, Y.; Peng, M.; Huang, P.; Zhou, Z.; Wu, X.; Chen, K. COX-2-related tumor immune microenvironment in non-small cell lung cancer: A novel signature to predict hot and cold tumor. J. Thorac. Dis. 2022, 14, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Kijima, T.; Kubo, T.; Nishihara, D.; Nukui, A.; Hirohashi, Y.; Torigoe, T.; Kamai, T. Cancer immunohistogram representing cancer-immunity cycle by immunohistochemistry predicts the efficacy of immune checkpoint inhibitors in urological cancer patients. Sci. Rep. 2022, 12, 10617. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.M.; Castro, A.; Pyke, R.M.; Okamura, R.; Kato, S.; Riviere, P.; Frampton, G.; Sokol, E.; Zhang, X.; Ball, E.D.; et al. MHC-I genotype and tumor mutational burden predict response to immunotherapy. Genome Med. 2020, 12, 45. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Age | Sex | Pathological Diagnosis | MMRD | Location | Differentiation | T Factor | N Factor | M Factor | Stage | Average Number of HLA Positive Cells per 5 Fields of View | HLA | γH2AX | PD-L1 | IRF-1 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case1 | 72 | Female | UC | − | 4.2 | Low | − | + | + | ||||||
| CC | − | S | Poor | 4b | 0 | 0 | IIC | 20 | Low | + | + | + | |||
| Case2 | 62 | Male | UC | − | 22.2 | Low | − | + | + | ||||||
| CC | − | Rb | Well | 2 | 0 | 0 | I | 22.6 | High | + | + | + | |||
| CC | − | D | Well | 1 | 0 | 0 | I | 0.4 | High | + | + | + | |||
| Case3 | 37 | Male | UC | − | 13.6 | Low | − | + | + | ||||||
| Dysplasia | − | A | 111.2 | Low | + | + | + | ||||||||
| Dysplasia | − | A | 6.8 | High | + | + | + | ||||||||
| Dysplasia | − | Ce | 45.4 | High | + | + | + | ||||||||
| CC | − | A | Moderate | 4a | 1a | 0 | IIIB | 40.2 | High | + | + | + | |||
| CC | − | S | Moderate | 2 | 0 | 0 | IIIB | 22.6 | High | + | + | + | |||
| CC | − | Ce | Moderate | 3 | 0 | 0 | IIIB | 33 | High | + | + | + | |||
| Case4 | 38 | Male | UC | − | 12.6 | Low | − | + | + | ||||||
| CC | − | S | Moderate | 4a | 0 | 0 | IIB | 28.9 | High | + | + | + | |||
| Case5 | 51 | Female | UC | − | 24.8 | High | − | − | + | ||||||
| CC | + | Ra | Well | Tis | 0 | 0 | 0 | 45 | High | + | + | + | |||
| Case6 | 42 | Female | UC | − | 6.6 | Low | − | + | + | ||||||
| Dysplasia | − | S | 15 | Low | + | + | + | ||||||||
| CC | − | S | Well | 2 | 0 | 0 | I | 18.6 | Low | + | + | + | |||
| Case7 | 55 | Male | UC | − | 17.2 | Low | − | + | + | ||||||
| Dysplasia | − | S | 6.8 | Low | + | + | + | ||||||||
| CC | − | S | Well | 4a | 2a | M1b | IVB | 15.2 | Low | + | + | + | |||
| Case8 | 51 | Male | UC | − | 26 | Low | − | − | + | ||||||
| CC | − | D | Well | Tis | 0 | 0 | 0 | 22.3 | High | + | + | + | |||
| CC | − | D | Well | Tis | 0 | 0 | 0 | 11.2 | High | + | + | + | |||
| Case9 | 38 | Male | UC | − | 14 | Low | − | + | + | ||||||
| CC | + | Rb | Well | T1b | 0 | 0 | I | 13.8 | Low | + | + | + |
| Case Number | Age | Sex | Pathological Diagnosis | MMRD | Location | Differentiation | T Factor | N Factor | M Factor | Stage | Average Number of HLA Positive Cells per 5 Fields of View | HLA | γH2AX | PD-L1 | IRF-1 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case1 | 72 | Female | UC | − | 4.2 | Low | − | + | + | ||||||
| CC | − | S | Poor | 4b | 0 | 0 | IIC | 20 | Low | + | + | + | |||
| Case2 | 62 | Male | UC | − | 22.2 | Low | − | + | + | ||||||
| CC | − | Rb | Well | 2 | 0 | 0 | I | 22.6 | High | + | + | + | |||
| CC | − | D | Well | 1 | 0 | 0 | I | 0.4 | High | + | + | + | |||
| Case3 | 37 | Male | UC | − | 13.6 | Low | − | + | + | ||||||
| Dysplasia | − | A | 111.2 | Low | + | + | + | ||||||||
| Dysplasia | − | A | 6.8 | High | + | + | + | ||||||||
| Dysplasia | − | Ce | 45.4 | High | + | + | + | ||||||||
| CC | − | A | Moderate | 4a | 1a | 0 | IIIB | 40.2 | High | + | + | + | |||
| CC | − | S | Moderate | 2 | 0 | 0 | IIIB | 22.6 | High | + | + | + | |||
| CC | − | Ce | Moderate | 3 | 0 | 0 | IIIB | 33 | High | + | + | + | |||
| Case4 | 38 | Male | UC | − | 12.6 | Low | − | + | + | ||||||
| CC | − | S | Moderate | 4a | 0 | 0 | IIB | 28.9 | High | + | + | + | |||
| Case5 | 51 | Female | UC | − | 24.8 | High | − | − | + | ||||||
| CC | + | Ra | Well | Tis | 0 | 0 | 0 | 45 | High | + | + | + | |||
| Case6 | 42 | Female | UC | − | 6.6 | Low | − | + | + | ||||||
| Dysplasia | − | S | 15 | Low | + | + | + | ||||||||
| CC | − | S | Well | 2 | 0 | 0 | I | 18.6 | Low | + | + | + | |||
| Case7 | 55 | Male | UC | − | 17.2 | Low | − | + | + | ||||||
| Dysplasia | − | S | 6.8 | Low | + | + | + | ||||||||
| CC | − | S | Well | 4a | 2a | M1b | IVB | 15.2 | Low | + | + | + | |||
| Case8 | 51 | Male | UC | − | 26 | Low | − | − | + | ||||||
| CC | − | D | Well | Tis | 0 | 0 | 0 | 22.3 | High | + | + | + | |||
| CC | − | D | Well | Tis | 0 | 0 | 0 | 11.2 | High | + | + | + | |||
| Case9 | 38 | Male | UC | − | 14 | Low | − | + | + | ||||||
| CC | + | Rb | Well | T1b | 0 | 0 | I | 13.8 | Low | + | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okami, H.; Ozawa, N.; Sohda, M.; Yokobori, T.; Osone, K.; Erkhem-Ochir, B.; Dorjkhorloo, G.; Shiraishi, T.; Okada, T.; Sano, A.; et al. HLA Class I Expression Is Associated with DNA Damage and Immune Cell Infiltration into Dysplastic and Neoplastic Lesions in Ulcerative Colitis. Int. J. Mol. Sci. 2023, 24, 13648. https://doi.org/10.3390/ijms241713648
Okami H, Ozawa N, Sohda M, Yokobori T, Osone K, Erkhem-Ochir B, Dorjkhorloo G, Shiraishi T, Okada T, Sano A, et al. HLA Class I Expression Is Associated with DNA Damage and Immune Cell Infiltration into Dysplastic and Neoplastic Lesions in Ulcerative Colitis. International Journal of Molecular Sciences. 2023; 24(17):13648. https://doi.org/10.3390/ijms241713648
Chicago/Turabian StyleOkami, Haruka, Naoya Ozawa, Makoto Sohda, Takehiko Yokobori, Katsuya Osone, Bilguun Erkhem-Ochir, Gendensuren Dorjkhorloo, Takuya Shiraishi, Takuhisa Okada, Akihiko Sano, and et al. 2023. "HLA Class I Expression Is Associated with DNA Damage and Immune Cell Infiltration into Dysplastic and Neoplastic Lesions in Ulcerative Colitis" International Journal of Molecular Sciences 24, no. 17: 13648. https://doi.org/10.3390/ijms241713648
APA StyleOkami, H., Ozawa, N., Sohda, M., Yokobori, T., Osone, K., Erkhem-Ochir, B., Dorjkhorloo, G., Shiraishi, T., Okada, T., Sano, A., Sakai, M., Miyazaki, T., Ogawa, H., Yao, T., Oike, T., Sato, H., Shirabe, K., Shibata, A., & Saeki, H. (2023). HLA Class I Expression Is Associated with DNA Damage and Immune Cell Infiltration into Dysplastic and Neoplastic Lesions in Ulcerative Colitis. International Journal of Molecular Sciences, 24(17), 13648. https://doi.org/10.3390/ijms241713648