
Influence of Pre-Analytic Conditions on Quantity of Lymphocytes


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
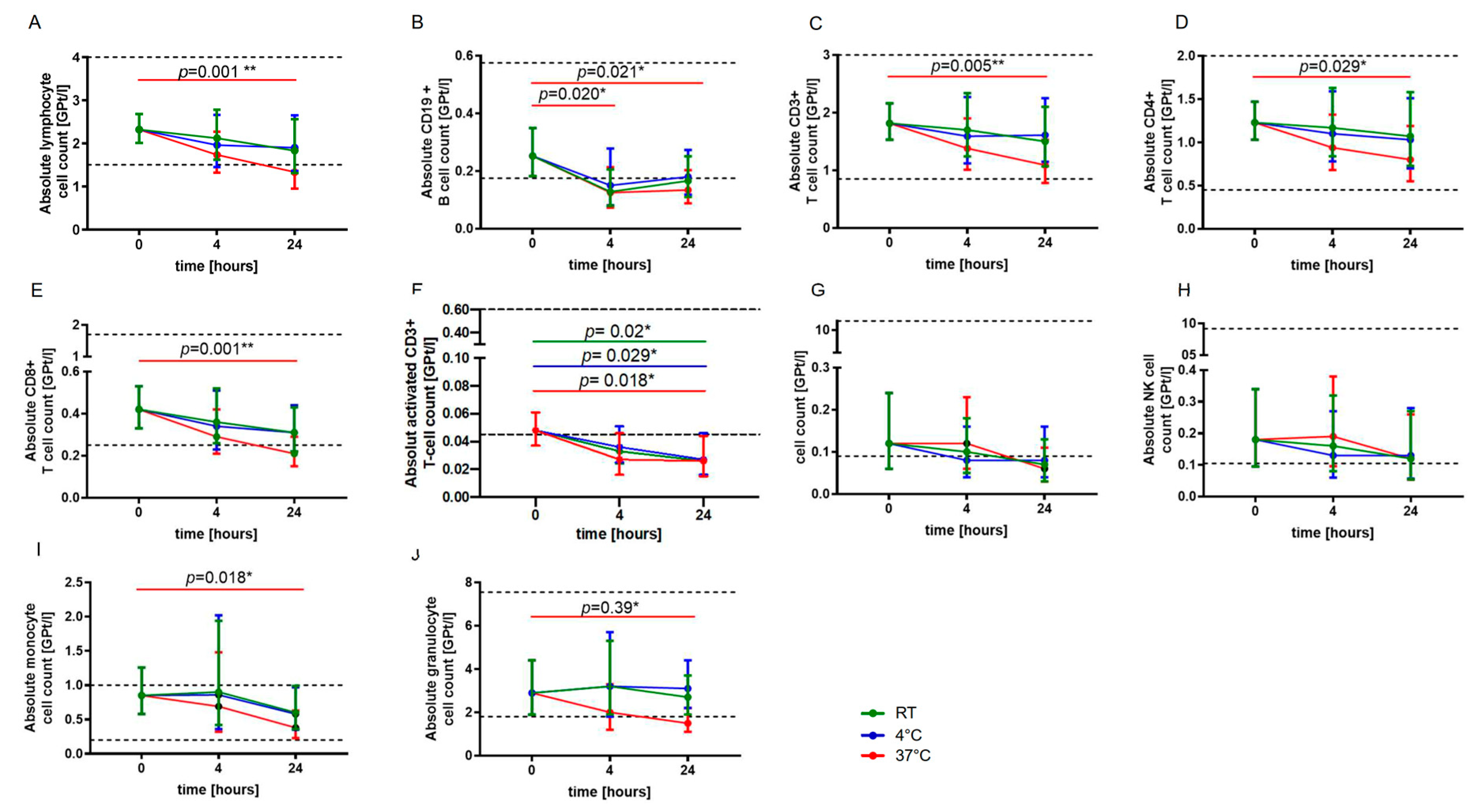
2.1. Storage Temperature and Duration
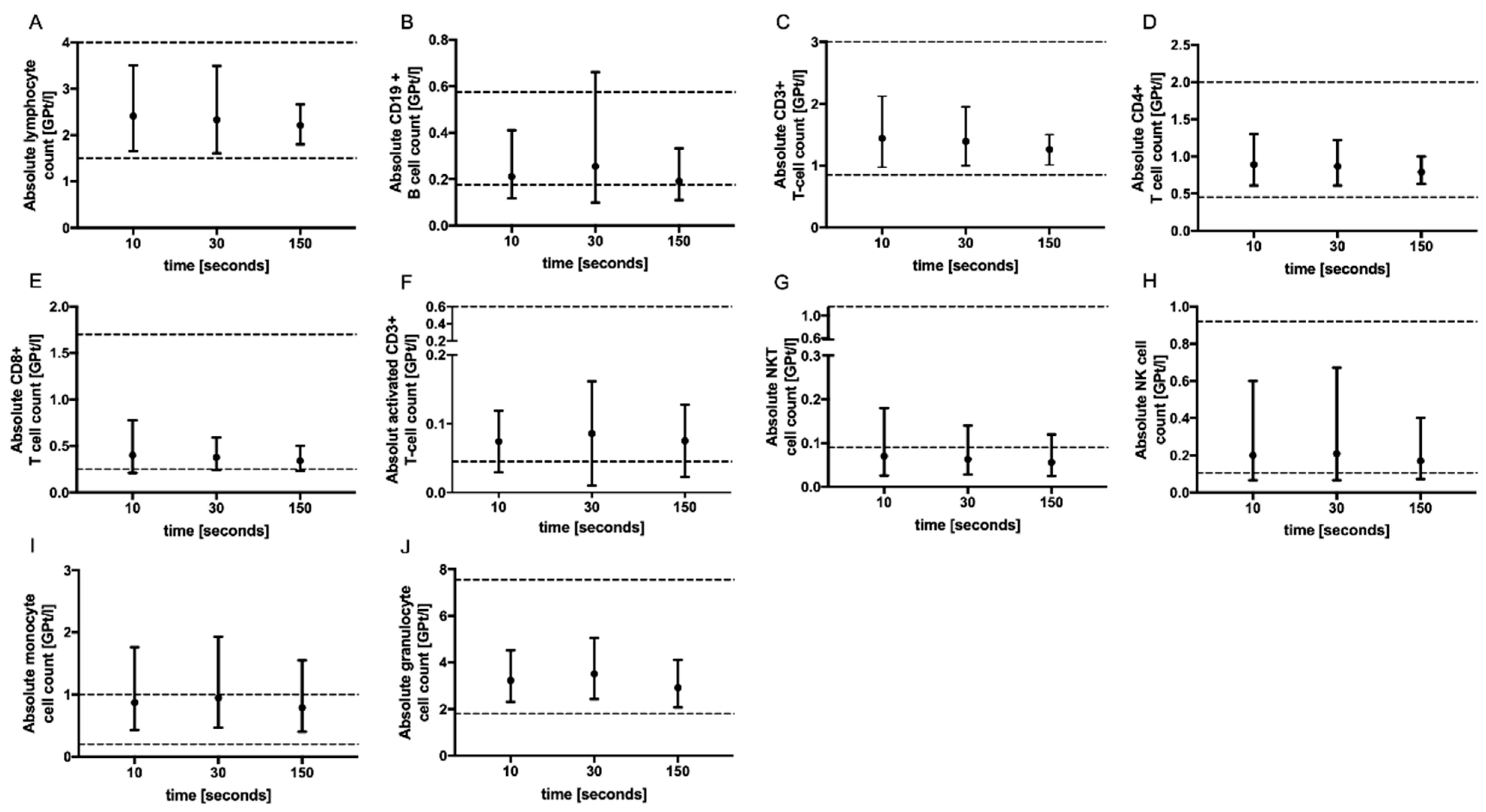
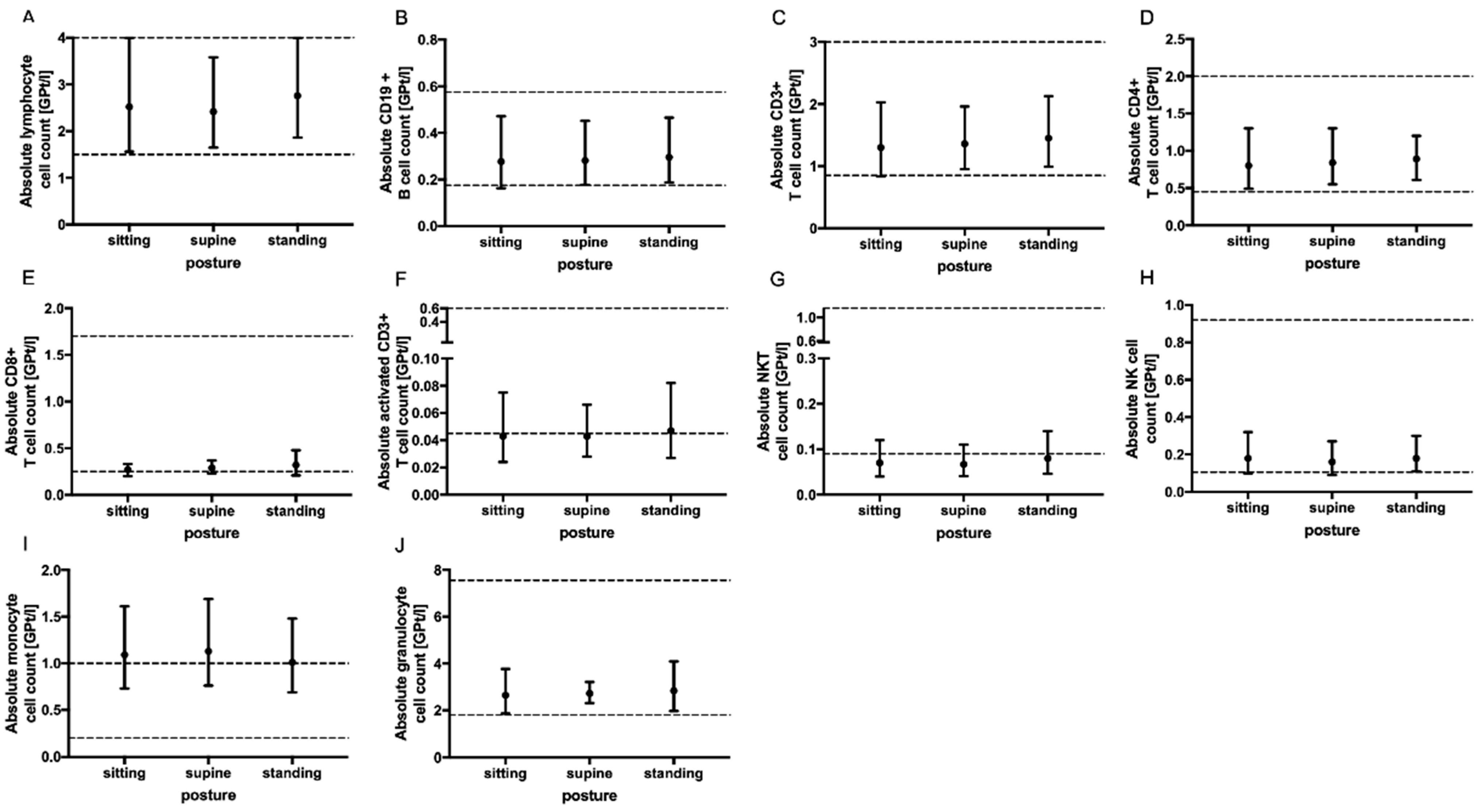
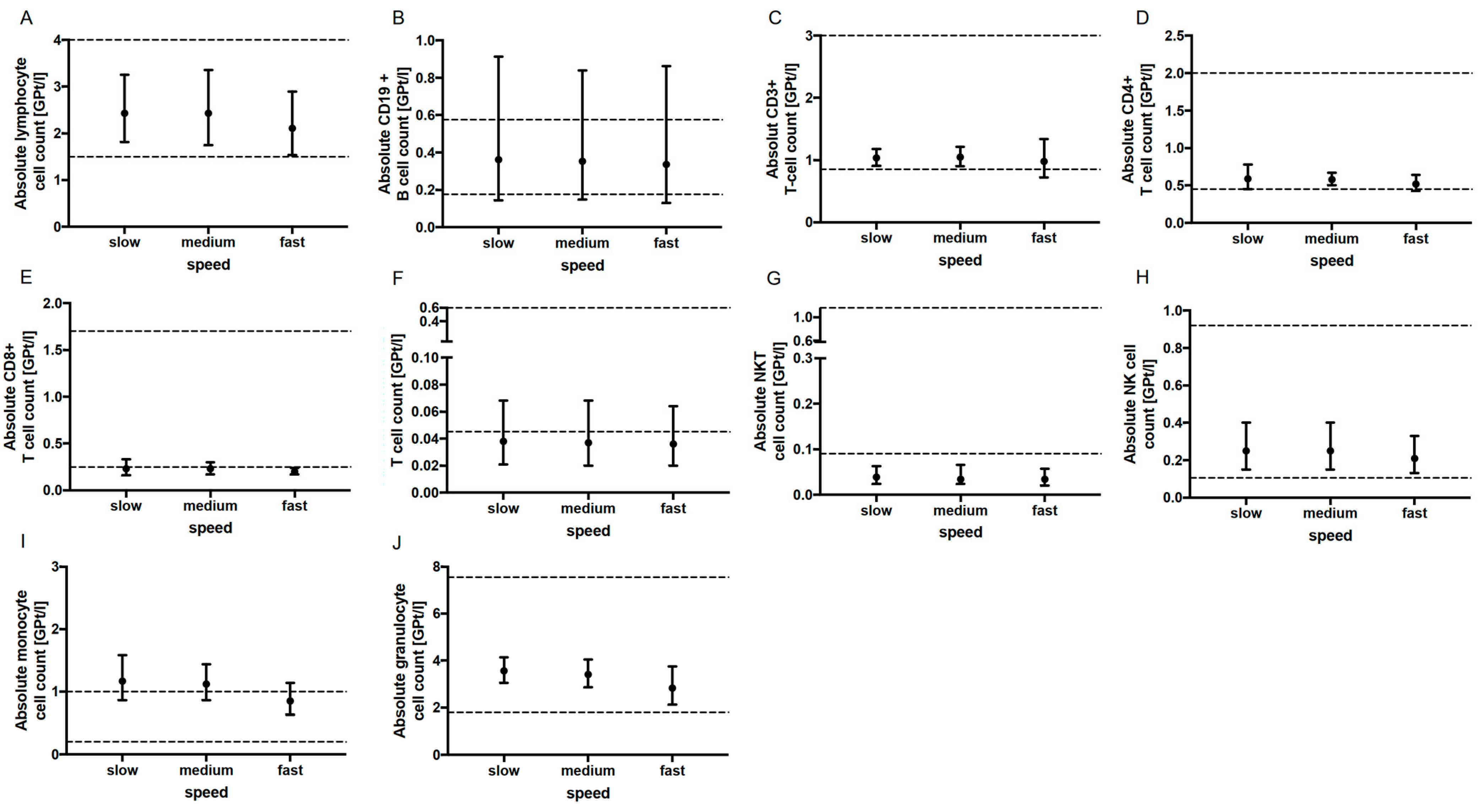
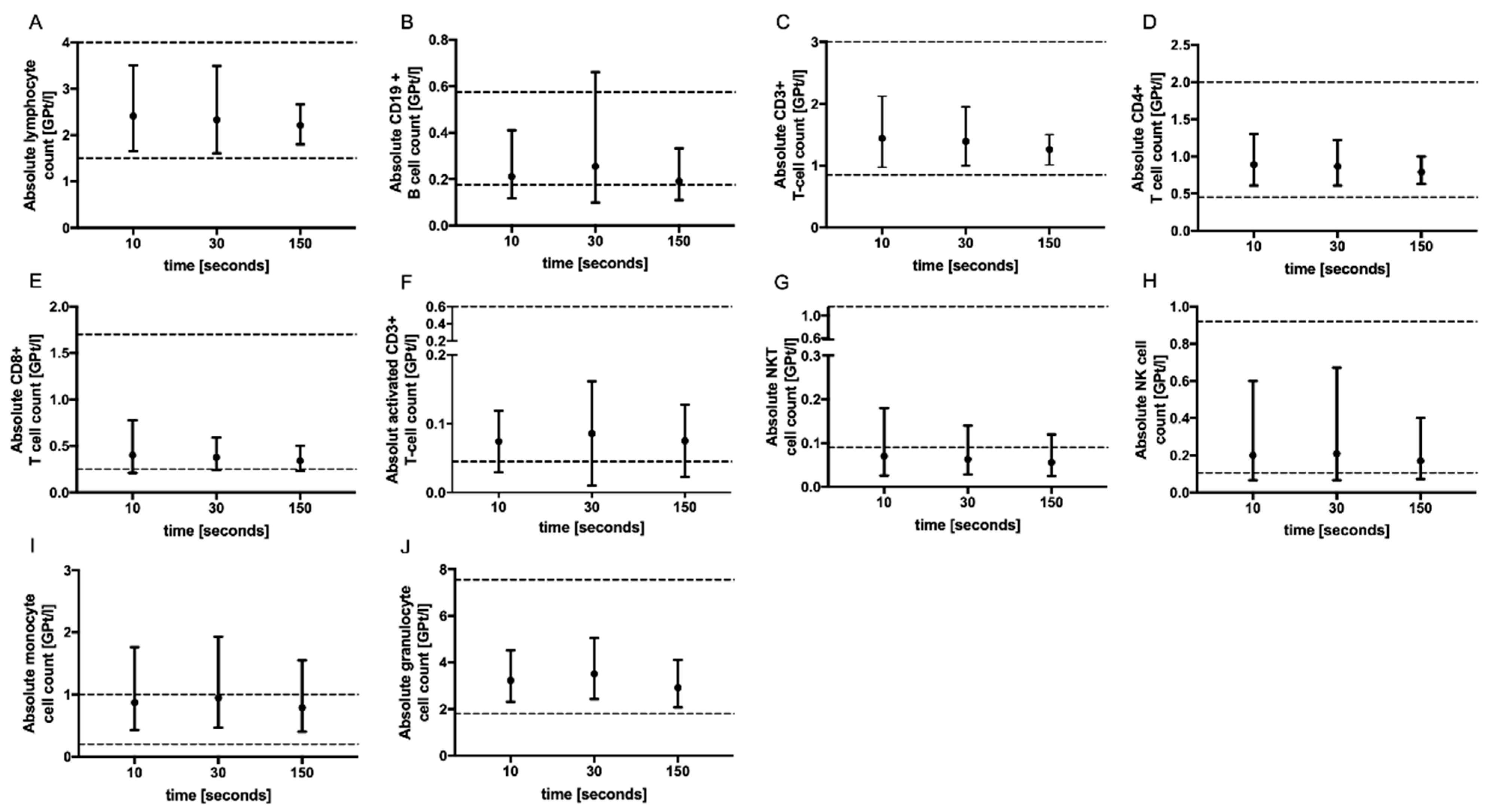
2.2. Tourniquet Application, Body Posture and Aspiration Speed
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Sample Collection
4.3. Ethic Approval
4.4. Immune Cell Phenotyping Using Fluorescence Activated Cell Sorting (FACS)
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J. MSCOI Study Group; European Multiple Sclerosis Platform New Insights into the Burden and Costs of Multiple Sclerosis in Europe. Mult. Scler. 2017, 23, 1123–1136. [Google Scholar] [CrossRef]
- Lassmann, H. Mechanisms of White Matter Damage in Multiple Sclerosis. Glia 2014, 62, 1816–1830. [Google Scholar] [CrossRef]
- Michel, L.; Touil, H.; Pikor, N.B.; Gommerman, J.L.; Prat, A.; Bar-Or, A. B Cells in the Multiple Sclerosis Central Nervous System: Trafficking and Contribution to CNS-Compartmentalized Inflammation. Front. Immunol. 2015, 6, 636. [Google Scholar] [CrossRef]
- Mishra, M.K.; Yong, V.W. Myeloid Cells—Targets of Medication in Multiple Sclerosis. Nat. Rev. Neurol. 2016, 12, 539–551. [Google Scholar] [CrossRef]
- Metz, I.; Weigand, S.D.; Popescu, B.F.G.; Frischer, J.M.; Parisi, J.E.; Guo, Y.; Lassmann, H.; Brück, W.; Lucchinetti, C.F. Pathologic Heterogeneity Persists in Early Active Multiple Sclerosis Lesions. Ann. Neurol. 2014, 75, 728–738. [Google Scholar] [CrossRef]
- Brück, W.; Gold, R.; Lund, B.T.; Oreja-Guevara, C.; Prat, A.; Spencer, C.M.; Steinman, L.; Tintore, M.; Vollmer, T.L.; Weber, M.S.; et al. Therapeutic decisions in multiple sclerosis: Moving beyond efficacy. JAMA Neurol. 2013, 70, 1315–1324. [Google Scholar] [CrossRef]
- Ziemssen, T.; Akgün, K.; Brück, W. Molecular biomarkers in multiple sclerosis. J. Neuroinflammation 2019, 16, 272. [Google Scholar] [CrossRef]
- Fischer, S.; Proschmann, U.; Akgün, K.; Ziemssen, T. Lymphocyte counts and multiple sclerosis therapeutics: Between mechanisms of action and treatment-limiting side effects. Cells 2021, 10, 3177. [Google Scholar] [CrossRef]
- Voigt, I.; Inojosa, H.; Dillenseger, A.; Haase, R.; Akgün, K.; Ziemssen, T. Digital twins for multiple sclerosis. Front. Immunol. 2021, 12, 669811. [Google Scholar] [CrossRef]
- Cellerino, M.; Ivaldi, F.; Pardini, M.; Rotta, G.; Vila, G.; Bäcker-Koduah, P.; Berge, T.; Laroni, A.; Lapucci, C.; Novi, G.; et al. Impact of treatment on cellular immunophenotype in MS: A cross-sectional study. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e693. [Google Scholar] [CrossRef]
- Cornes, M.; van Dongen-Lases, E.; Grankvist, K.; Ibarz, M.; Kristensen, G.; Lippi, G.; Nybo, M.; Simundic, A.-M. Order of blood draw: Opinion paper by the european federation for clinical chemistry and laboratory medicine (EFLM) Working Group for the Preanalytical Phase (WG-PRE). Clin. Chem. Lab. Med. 2017, 55, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Lima-Oliveira, G.; Guidi, G.C.; Salvagno, G.L.; Danese, E.; Montagnana, M.; Lippi, G. Patient posture for blood collection by venipuncture: Recall for standardization after 28 years. Rev. Bras. Hematol. Hemoter. 2017, 39, 127–132. [Google Scholar] [CrossRef]
- Diks, A.M.; Bonroy, C.; Teodosio, C.; Groenland, R.J.; de Mooij, B.; de Maertelaere, E.; Neirynck, J.; Philippé, J.; Orfao, A.; van Dongen, J.; et al. Impact of blood storage and sample handling on quality of high dimensional flow cytometric data in multicenter clinical research. J. Immunol. Methods 2019, 475, 112616. [Google Scholar] [CrossRef]
- Klotz, L.; Berthele, A.; Brück, W.; Chan, A.; Flachenecker, P.; Gold, R.; Haghikia, A.; Hellwig, K.; Hemmer, B.; Hohlfeld, R.; et al. Monitoring von Blutparametern unter verlaufsmodifizierender MS-Therapie. Nervenarzt 2016, 87, 645–659. [Google Scholar] [CrossRef]
- Datta, P. Resolving discordant samples in clinical laboratory practice. MLO Med. Lab. Obs. 2004, 36, 28–31. [Google Scholar] [PubMed]
- Wiendl, H.; Kieseier, B. Multiple Sclerosis: Reprogramming the Immune Repertoire with Alemtuzumab in MS. Nat. Rev. Neurol. 2013, 9, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Plebani, M.; Carraro, P. Mistakes in a stat laboratory: Types and frequency. Clin. Chem. 1997, 43, 1348–1351. [Google Scholar] [CrossRef]
- Bergman, M.; Bessler, H.; Salman, H.; Djaldetti, M. Relationship between Temperature and Apoptosis of Human Peripheral Blood Mononuclear Cells. Int. J. Hematol. 2003, 77, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-W.; Jang, Y.-Y.; Shin, M.-G.; Shin, J.-H.; Suh, S.-P.; Ryang, D.-W.; Yoon, M.; Lee, J.-J.; Kim, S.-K.; Cho, D. Overnight Storage of Blood in ACD Tubes at 4 °C Increases NK Cell Fraction in Peripheral Blood Mononuclear Cells. Ann. Clin. Lab. Sci. 2013, 43, 267–273. [Google Scholar]
- Kelman, G.R.; Nunn, J.F. Nomograms for Correction of Blood Po2, Pco2, PH, and Base Excess for Time and Temperature. J. Appl. Physiol. 1966, 21, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.A.; Green, T.A. Selection of Anticoagulants for Lymphocyte Immunophenotyping. J. Immunol. Methods 1993, 165, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Saleem, S.; Mani, V.; A Chadwick, M.; Creanor, S.; Ayling, R.M. A prospective study of causes of haemolysis during venepuncture: Tourniquet time should be kept to a minimum. Ann. Clin. Biochem. 2009, 46 Pt 3, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Lima-Oliveira, G.; Lippi, G.; Salvagno, G.L.; Montagnana, M.; Scartezini, M.; Guidi, G.C.; Picheth, G. Transillumination: A new tool to eliminate the impact of venous stasis during the procedure for the collection of diagnostic blood specimens for routine haematological testing. Int. J. Lab. Hematol. 2011, 33, 457–462. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Analytic Factor | Age, Years, Mean (SD) | Gender, Female/Male | BMI, Mean (SD) |
|---|---|---|---|
| Storage temperature and time (n = 5) | 25.4 (2.3) | 3/2 | 24.5 (3.4) |
| Tourniquet application time (n = 5) | 23.2 (0.8) | 3/2 | 24.1 (2.9) |
| Body posture (n = 5) | 26.4 (5.4) | 1/4 | 26.6 (2.5) |
| Aspiration speed (n = 5) | 24.6 (2.4) | 3/2 | 22.8 (2.5) 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Proschmann, U.; Shalchi Amirkhiz, P.; Andres, P.; Haase, R.; Inojosa, H.; Ziemssen, T.; Akgün, K. Influence of Pre-Analytic Conditions on Quantity of Lymphocytes. Int. J. Mol. Sci. 2023, 24, 13479. https://doi.org/10.3390/ijms241713479
Proschmann U, Shalchi Amirkhiz P, Andres P, Haase R, Inojosa H, Ziemssen T, Akgün K. Influence of Pre-Analytic Conditions on Quantity of Lymphocytes. International Journal of Molecular Sciences. 2023; 24(17):13479. https://doi.org/10.3390/ijms241713479
Chicago/Turabian StyleProschmann, Undine, Puya Shalchi Amirkhiz, Pauline Andres, Rocco Haase, Hernan Inojosa, Tjalf Ziemssen, and Katja Akgün. 2023. "Influence of Pre-Analytic Conditions on Quantity of Lymphocytes" International Journal of Molecular Sciences 24, no. 17: 13479. https://doi.org/10.3390/ijms241713479
APA StyleProschmann, U., Shalchi Amirkhiz, P., Andres, P., Haase, R., Inojosa, H., Ziemssen, T., & Akgün, K. (2023). Influence of Pre-Analytic Conditions on Quantity of Lymphocytes. International Journal of Molecular Sciences, 24(17), 13479. https://doi.org/10.3390/ijms241713479