

Studies on the Role of Compartmentalized Profiles of Cytokines in the Risk of Hepatocellular Carcinoma

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Results
2.1. Patients
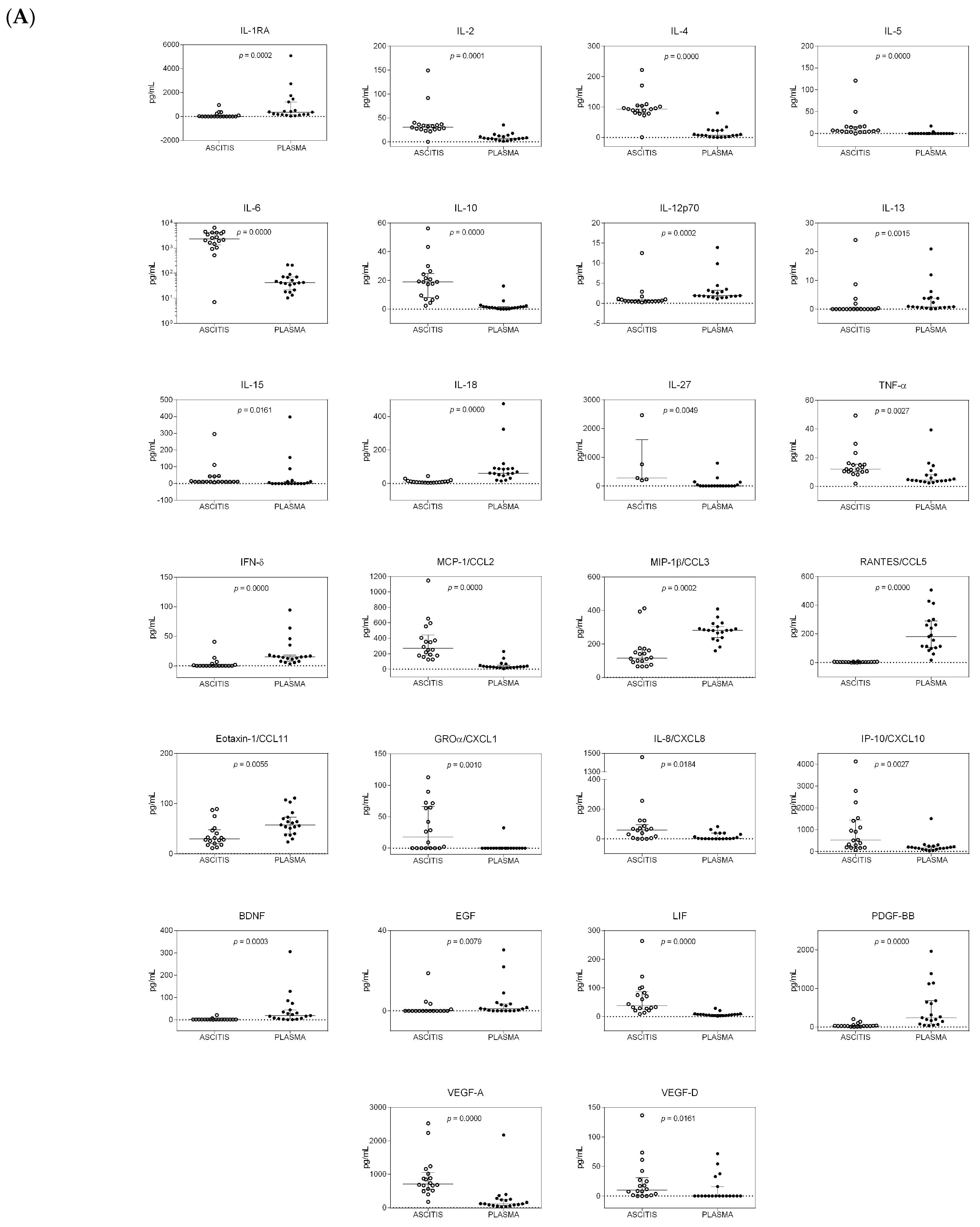
2.2. Trend of Cytokines in the Two Body Compartments
2.3. Trend of Cytokines in the Two Patient Cohorts
2.4. HCC Risk Prediction
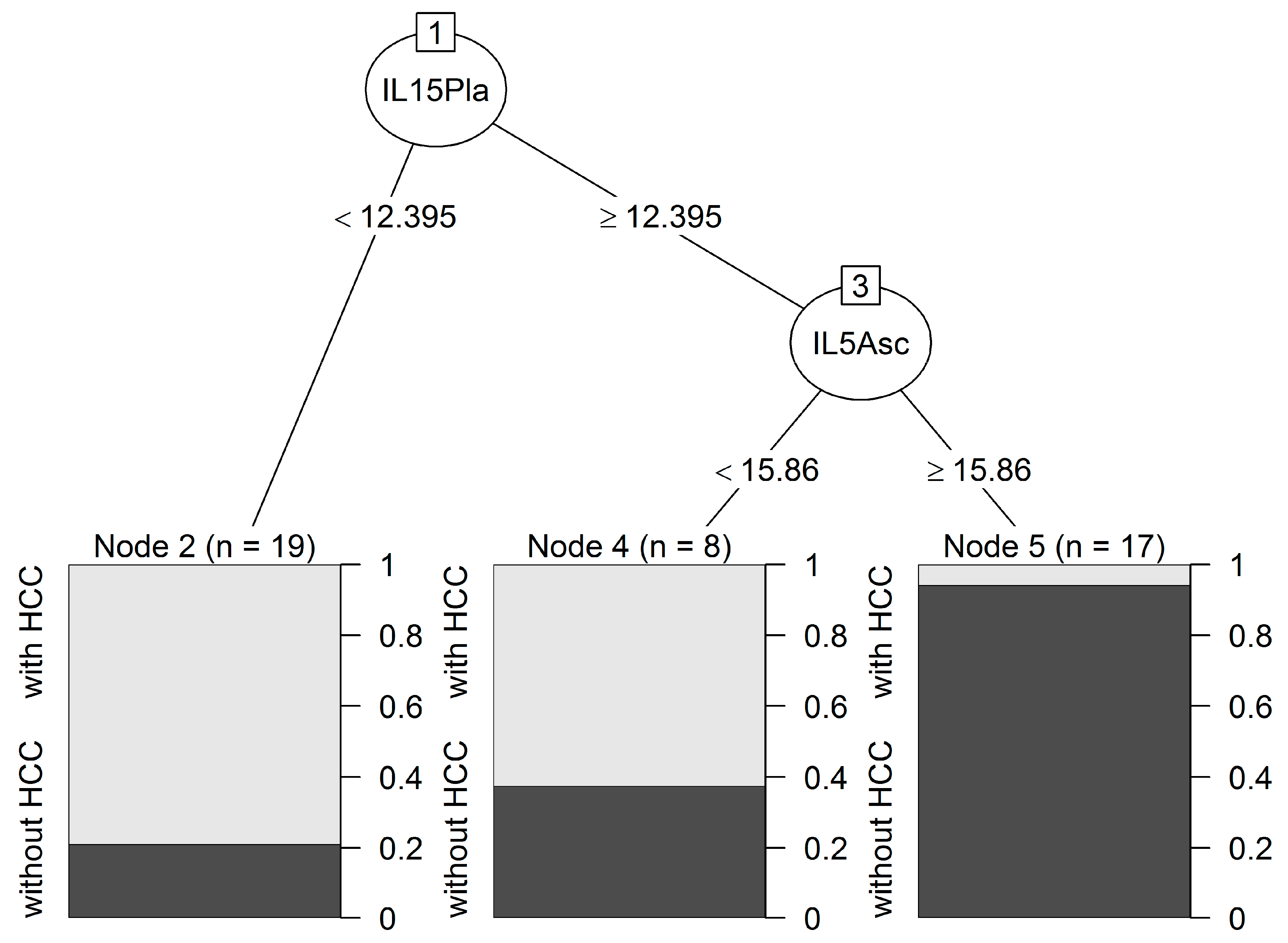
2.5. Classification Tree Predicting HCC
2.6. Trend of Cytokines in the Two Compartments in Subjects with or without HBV/HCV Infection
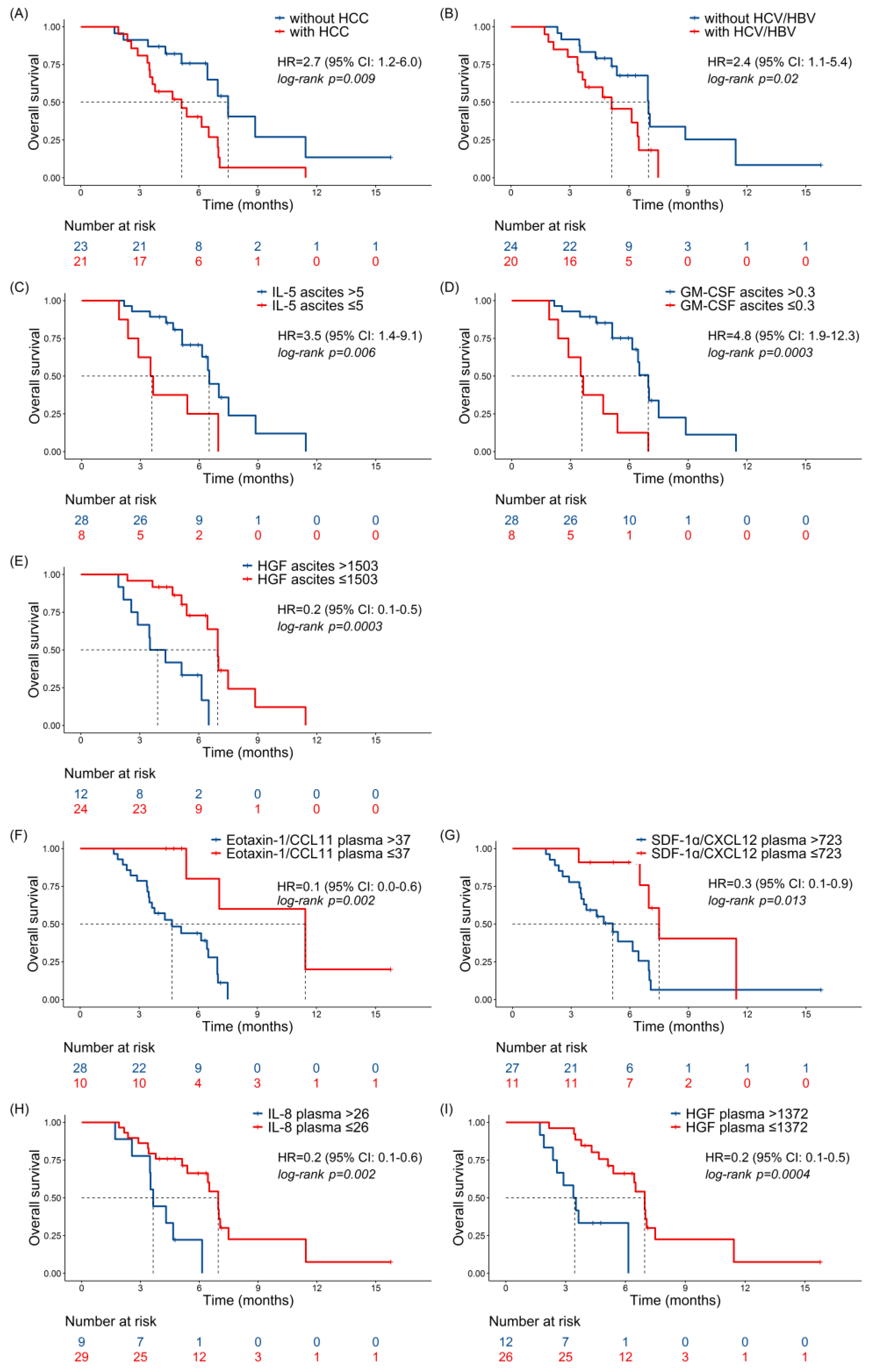
2.7. Univariate Analyses for OS
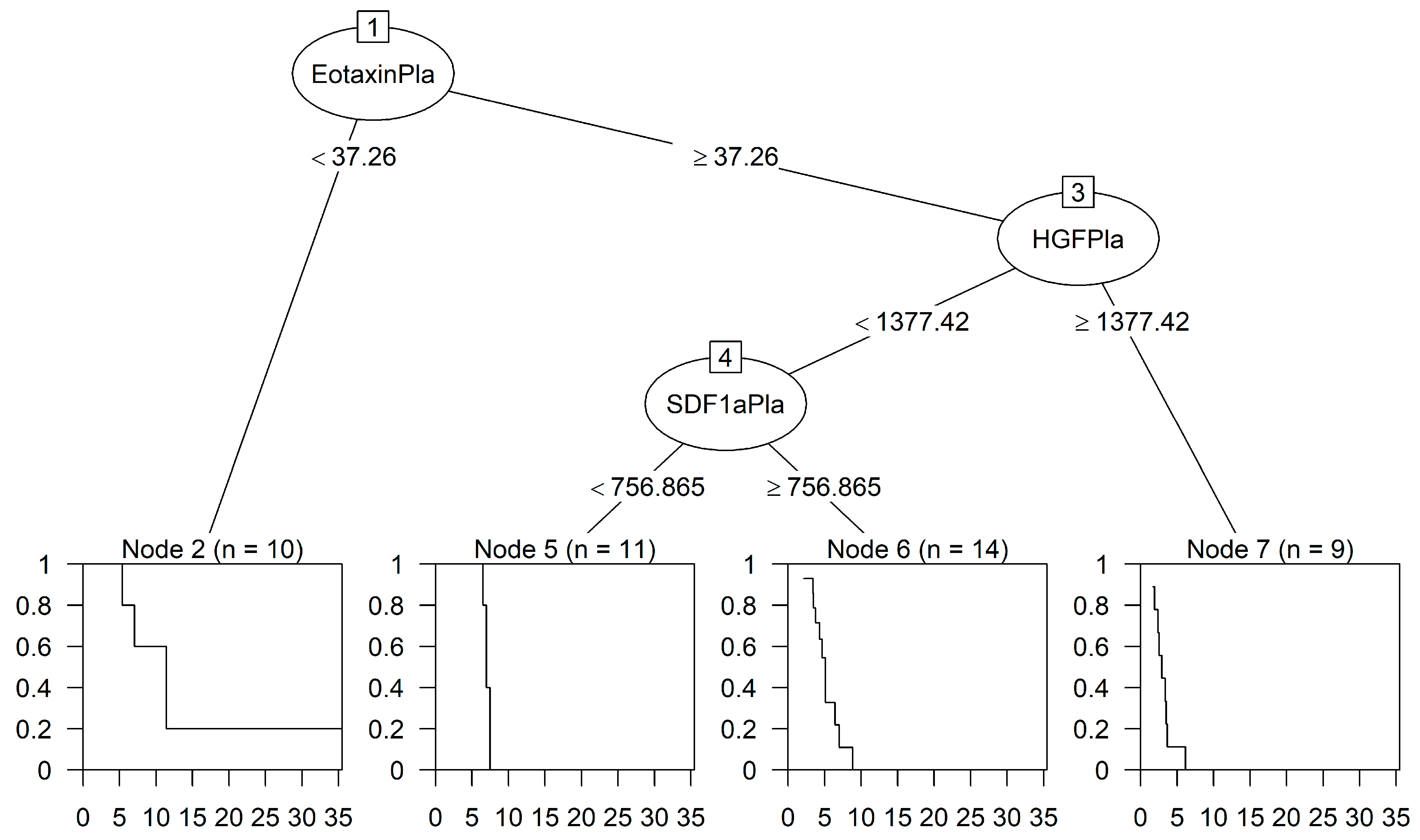
2.8. Classification Tree Predicting OS
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Quantitative Analysis of Cytokines, Chemokines, and Growth Factors
4.3. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk Factors and Prevention of Hepatocellular Carcinoma in the Era of Precision Medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control 2017, 24, 107327481772924. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Epidemiology of Viral Hepatitis and Hepatocellular Carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef] [PubMed]
- Nishitsuji, H.; Funami, K.; Shimizu, Y.; Ujino, S.; Sugiyama, K.; Seya, T.; Takaku, H.; Shimotohno, K. Hepatitis C Virus Infection Induces Inflammatory Cytokines and Chemokines Mediated by the Cross Talk between Hepatocytes and Stellate Cells. J. Virol. 2013, 87, 8169–8178. [Google Scholar] [CrossRef]
- Goossens, N. Molecular Prognostic Prediction in Liver Cirrhosis. World J. Gastroenterol. 2015, 21, 10262–10273. [Google Scholar] [CrossRef]
- Trivanović, D.; Krstić, J.; Djordjević, I.O.; Mojsilović, S.; Santibanez, J.F.; Bugarski, D.; Jauković, A. The Roles of Mesenchymal Stromal/Stem Cells in Tumor Microenvironment Associated with Inflammation. Mediat. Inflamm. 2016, 2016, 7314016. [Google Scholar] [CrossRef]
- Trivanović, D.; Krstić, J.; Mojsilović, S.; Djordjević, I.O.; Ilić, V. Mesenchymal Stem Cells from Different Tissues: Immune Status and Activity. J. Immunol. Infect. Dis. 2016, 3, 102. [Google Scholar] [CrossRef]
- Yu, L.X.; Ling, Y.; Wang, H.Y. Role of Nonresolving Inflammation in Hepatocellular Carcinoma Development and Progression. npj Precis. Oncol. 2018, 2, 6. [Google Scholar] [CrossRef]
- Mack, C.L. Serum Cytokines as Biomarkers of Disease and Clues to Pathogenesis. Hepatology 2007, 46, 6–8. [Google Scholar] [CrossRef]
- Kotyza, J. Chemokines in Tumor Proximal Fluids. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2017, 161, 41–49. [Google Scholar] [CrossRef]
- Jørgensen, H.; Hill, A.S.; Beste, M.T.; Kumar, M.P.; Chiswick, E.; Fedorcsak, P.; Isaacson, K.B.; Lauffenburger, D.A.; Griffith, L.G.; Qvigstad, E. Peritoneal Fluid Cytokines Related to Endometriosis in Patients Evaluated for Infertility. Fertil. Steril. 2017, 107, 1191–1199.e2. [Google Scholar] [CrossRef] [PubMed]
- Quail, D.F.; Joyce, J.A. Microenvironmental Regulation of Tumor Progression and Metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef] [PubMed]
- Zekri, A.R.N.; Deeb, S.E.; Bahnassy, A.A.; Badr, A.M.; Abdellateif, M.S.; Esmat, G.; Salama, H.; Mohanad, M.; El-Dien, A.E.; Rabah, S.; et al. Role of Relevant Immune-Modulators and Cytokines in Hepatocellular Carcinoma and Premalignant Hepatic Lesions. World J. Gastroenterol. 2018, 24, 1228–1238. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-Associated Immune Dysfunction: Distinctive Features and Clinical Relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Angeli, P.; Moreau, R.; Jalan, R.; Clària, J.; Trebicka, J.; Fernández, J.; Gustot, T.; Caraceni, P.; Bernardi, M. The Systemic Inflammation Hypothesis: Towards a New Paradigm of Acute Decompensation and Multiorgan Failure in Cirrhosis. J. Hepatol. 2021, 74, 670–685. [Google Scholar] [CrossRef]
- Chen, H.J.; Hu, M.H.; Xu, F.G.; Xu, H.J.; She, J.J.; Xia, H.P. Understanding the inflammation-cancer transformation in the development of primary liver cancer. Hepatoma Res. 2018, 4, 29. [Google Scholar] [CrossRef]
- Jayant, K.; Habib, N.; Huang, K.W.; Warwick, J.; Arasaradnam, R. Recent Advances: The Imbalance of Immune Cells and Cytokines in the Pathogenesis of Hepatocellular Carcinoma. Diagnostics 2020, 10, 338. [Google Scholar] [CrossRef]
- Rasid, O.; Ciulean, I.S.; Fitting, C.; Doyen, N.; Cavaillon, J.M. Local Microenvironment Controls the Compartmentalization of NK Cell Responses during Systemic Inflammation in Mice. J. Immunol. 2016, 197, 2444–2454. [Google Scholar] [CrossRef]
- Alvarez-Silva, C.; Schierwagen, R.; Pohlmann, A.; Magdaleno, F.; Uschner, F.E.; Ryan, P.; Vehreschild, M.J.G.T.; Claria, J.; Latz, E.; Lelouvier, B.; et al. Compartmentalization of Immune Response and Microbial Translocation in Decompensated Cirrhosis. Front. Immunol. 2019, 10, 69. [Google Scholar] [CrossRef]
- Cavaillon, J.M.; Annane, D. Compartmentalization of the Inflammatory Response in Sepsis and SIRS. J. Endotoxin Res. 2006, 12, 151–170. [Google Scholar] [CrossRef]
- Rabinovich, G.A.; Gabrilovich, D.; Sotomayor, E.M. Immunosuppressive Strategies That Are Mediated by Tumor Cells. Annu. Rev. Immunol. 2007, 25, 267–296. [Google Scholar] [CrossRef] [PubMed]
- Zou, W. Immunosuppressive Networks in the Tumour Environment and Their Therapeutic Relevance. Nat. Rev. Cancer 2005, 5, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Fiore, P.F.; Di Matteo, S.; Tumino, N.; Mariotti, F.R.; Pietra, G.; Ottonello, S.; Negrini, S.; Bottazzi, B.; Moretta, L.; Mortier, E.; et al. Interleukin-15 and Cancer: Some Solved and Many Unsolved Questions. J. Immunother. Cancer 2020, 8, e001428. [Google Scholar] [CrossRef] [PubMed]
- Zaynagetdinov, R.; Sherrill, T.P.; Gleaves, L.A.; McLoed, A.G.; Saxon, J.A.; Habermann, A.C.; Connelly, L.; Dulek, D.; Peebles, R.S.; Fingleton, B.; et al. Interleukin-5 Facilitates Lung Metastasis by Modulating the Immune Microenvironment. Cancer Res. 2015, 75, 1624–1634. [Google Scholar] [CrossRef] [PubMed]
- Easom, N.J.W.; Stegmann, K.A.; Swadling, L.; Pallett, L.J.; Burton, A.R.; Odera, D.; Schmidt, N.; Huang, W.C.; Fusai, G.; Davidson, B.; et al. IL-15 Overcomes Hepatocellular Carcinoma-Induced NK Cell Dysfunction. Front. Immunol. 2018, 9, 1009. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Sun, H.; Xiao, W.; Zhang, C.; Tian, Z. Natural Killer Cell Dysfunction in Hepatocellular Carcinoma and NK Cell-Based Immunotherapy. Acta Pharmacol. Sin. 2015, 36, 1191–1199. [Google Scholar] [CrossRef]
- Arici, A.; Matalliotakis, I.; Goumenou, A.; Koumantakis, G.; Vassiliadis, S.; Selam, B.; Mahutte, N.G. Increased Levels of Interleukin-15 in the Peritoneal Fluid of Women with Endometriosis: Inverse Correlation with Stage and Depth of Invasion. Hum. Reprod. 2003, 18, 429–432. [Google Scholar] [CrossRef]
- Cepero-Donates, Y.; Rakotoarivelo, V.; Mayhue, M.; Ma, A.; Chen, Y.G.; Ramanathan, S. Homeostasis of IL-15 Dependent Lymphocyte Subsets in the Liver. Cytokine 2016, 82, 95–101. [Google Scholar] [CrossRef]
- Berger, A.; Colpitts, S.J.; Seabrook, M.S.S.; Furlonger, C.L.; Bendix, M.B.; Moreau, J.M.; McKillop, W.M.; Medin, J.A.; Paige, C.J. Interleukin-15 in Cancer Immunotherapy: IL-15 Receptor Complex versus Soluble IL-15 in a Cancer Cell-Delivered Murine Leukemia Model. J. Immunother. Cancer 2019, 7, 355. [Google Scholar] [CrossRef]
- Wang, W.; Jin, J.; Dai, F.; Long, Z.; Liu, X.; Cai, H.; Zhou, Y.; Chen, Z.; Huang, H. Interleukin-15 Suppresses Gastric Cancer Liver Metastases by Enhancing Natural Killer Cell Activity in a Murine Model. Oncol. Lett. 2018, 16, 4839–4846. [Google Scholar] [CrossRef]
- Do-Thi, V.A.; Lee, H.; Jeong, H.J.; Lee, J.O.; Kim, Y.S. Protective and Therapeutic Effects of an IL-15:IL-15Rα-Secreting Cell-Based Cancer Vaccine Using a Baculovirus System. Cancers 2021, 13, 4039. [Google Scholar] [CrossRef]
- Waldmann, T.A.; Dubois, S.; Miljkovic, M.D.; Conlon, K.C. IL-15 in the Combination Immunotherapy of Cancer. Front. Immunol. 2020, 11, 868. [Google Scholar] [CrossRef] [PubMed]
- Takatsu, K. Interleukin-5 and IL-5 Receptor in Health and Diseases. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2011, 87, 463–485. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.Q.; Cai, D.; Gong, J.P.; Lai, X. Innate Immune Cells and Their Interaction with T Cells in Hepatocellular Carcinoma. Oncol. Lett. 2020, 21, 57. [Google Scholar] [CrossRef]
- Eftimie, R.; Bramson, J.L.; Earn, D.J.D. Modeling Anti-Tumor Th1 and Th2 Immunity in the Rejection of Melanoma. J. Theor. Biol. 2010, 265, 467–480. [Google Scholar] [CrossRef]
- Blomberg, O.S.; Spagnuolo, L.; Garner, H.; Voorwerk, L.; Isaeva, O.I.; Van Dyk, E.; Bakker, N.; Chalabi, M.; Klaver, C.; Duijst, M.; et al. IL-5-Producing CD4+ T Cells and Eosinophils Cooperate to Enhance Response to Immune Checkpoint Blockade in Breast Cancer. Cancer Cell 2023, 41, 106–123.e10. [Google Scholar] [CrossRef]
- Jacenik, D.; Karagiannidis, I.; Beswick, E.J. Th2 Cells Inhibit Growth of Colon and Pancreas Cancers by Promoting Anti-Tumorigenic Responses from Macrophages and Eosinophils. Br. J. Cancer 2023, 128, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Ikutani, M.; Yanagibashi, T.; Ogasawara, M.; Tsuneyama, K.; Yamamoto, S.; Hattori, Y.; Kouro, T.; Itakura, A.; Nagai, Y.; Takaki, S.; et al. Identification of Innate IL-5–Producing Cells and Their Role in Lung Eosinophil Regulation and Antitumor Immunity. J. Immunol. 2012, 188, 703–713. [Google Scholar] [CrossRef]
- Walker, C.; Checkel, J.; Cammisuli, S.; Leibson, P.J.; Gleich, G.J. IL-5 Production by NK Cells Contributes to Eosinophil Infiltration in a Mouse Model of Allergic Inflammation. J. Immunol. 1998, 161, 1962–1969. [Google Scholar] [CrossRef] [PubMed]
- Linch, S.N.; Danielson, E.T.; Kelly, A.M.; Tamakawa, R.A.; Lee, J.J.; Gold, J.A. Interleukin 5 Is Protective during Sepsis in an Eosinophil-Independent Manner. Am. J. Respir. Crit. Care Med. 2012, 186, 246–254. [Google Scholar] [CrossRef]
- Hayashi, T.; Yamashita, T.; Terashima, T.; Suda, T.; Okada, H.; Asahina, Y.; Hayashi, T.; Hara, Y.; Nio, K.; Sunagozaka, H.; et al. Serum Cytokine Profiles Predict Survival Benefits in Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib: A Retrospective Cohort Study. BMC Cancer 2017, 17, 870. [Google Scholar] [CrossRef]
- Liu, P.; Gao, Y.; Huan, J.; Ge, X.; Tang, Y.; Shen, W.; Tian, Y.; Shen, W.; Zou, S.; Zhou, J.; et al. Upregulation of PAX2 Promotes the Metastasis of Esophageal Cancer through Interleukin-5. Cell. Physiol. Biochem. 2015, 35, 740–754. [Google Scholar] [CrossRef]
- Jammal, M.P.; Martins-Filho, A.; Silveira, T.P.; Murta, E.F.C.; Nomelini, R.S. Cytokines and Prognostic Factors in Epithelial Ovarian Cancer. Clin. Med. Insights Oncol. 2016, 10, 71–76. [Google Scholar] [CrossRef]
- Liu, Y.; Hu, J.; Luo, N.; Zhao, J.; Liu, S.; Ma, T.; Yao, Y. The Essential Involvement of the Omentum in the Peritoneal Defensive Mechanisms During Intra-Abdominal Sepsis. Front. Immunol. 2021, 12, 631609. [Google Scholar] [CrossRef] [PubMed]
- Fagan, K.J.; Rogers, G.B.; Melino, M.; Arthur, D.M.; Costello, M.E.; Morrison, M.; Powell, E.E.; Irvine, K.M. Ascites Bacterial Burden and Immune Cell Profile Are Associated with Poor Clinical Outcomes in the Absence of Overt Infection. PLoS ONE 2015, 10, e0120642. [Google Scholar] [CrossRef] [PubMed]
- Lutz, P.; Jeffery, H.C.; Jones, N.; Birtwistle, J.; Kramer, B.; Nattermann, J.; Spengler, U.; Strassburg, C.P.; Adams, D.H.; Oo, Y.H. NK Cells in Ascites From Liver Disease Patients Display a Particular Phenotype and Take Part in Antibacterial Immune Response. Front. Immunol. 2019, 10, 1838. [Google Scholar] [CrossRef] [PubMed]
- Irvine, K.M.; Ratnasekera, I.; Powell, E.E.; Hume, D.A. Causes and Consequences of Innate Immune Dysfunction in Cirrhosis. Front. Immunol. 2019, 10, 293. [Google Scholar] [CrossRef]
- Dougan, M.; Dranoff, G.; Dougan, S.K. GM-CSF, IL-3, and IL-5 Family of Cytokines: Regulators of Inflammation. Immunity 2019, 50, 796–811. [Google Scholar] [CrossRef] [PubMed]
- Hercus, T.R.; Kan, W.L.T.; Broughton, S.E.; Tvorogov, D.; Ramshaw, H.S.; Sandow, J.J.; Nero, T.L.; Dhagat, U.; Thompson, E.J.; Shing, K.S.C.T.; et al. Role of the β Common (Βc) Family of Cytokines in Health and Disease. Cold Spring Harb. Perspect. Biol. 2018, 10, a028514. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.K.; Brickner, H.; Panwar, B.; Ramírez-Suástegui, C.; Herrera-de La Mata, S.; Liu, N.; Diaz, D.; Alexander, L.E.C.; Ay, F.; Vijayanand, P.; et al. Human Eosinophils Express a Distinct Gene Expression Program in Response to IL-3 Compared with Common β-Chain Cytokines IL-5 and GM-CSF. J. Immunol. 2019, 203, 329–337. [Google Scholar] [CrossRef]
- Guthridge, M.A.; Stomski, F.C.; Thomas, D.; Woodcock, J.M.; Bagley, C.J.; Berndt, M.C.; Lopez, A.F. Mechanism of Activation of the GM-CSF, IL-3, and IL-5 Family of Receptors. Stem Cells 1998, 16, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Charrier, E.; Vernet, R.; Schwenter, F.; Luy, P.; Donda, A.; Mach, N. A Functional GM-CSF Receptor on Dendritic Cells Is Required for Efficient Protective Anti-Tumor Immunity. Immuno 2021, 1, 240–252. [Google Scholar] [CrossRef]
- Ruffolo, L.I.; Jackson, K.M.; Kuhlers, P.C.; Dale, B.S.; Figueroa Guilliani, N.M.; Ullman, N.A.; Burchard, P.R.; Qin, S.S.; Juviler, P.G.; Keilson, J.M.; et al. GM-CSF Drives Myelopoiesis, Recruitment and Polarisation of Tumour-Associated Macrophages in Cholangiocarcinoma and Systemic Blockade Facilitates Antitumour Immunity. Gut 2022, 71, 1386–1398. [Google Scholar] [CrossRef]
- Zarei, S.; Schwenter, F.; Luy, P.; Aurrand-Lions, M.; Morel, P.; Kopf, M.; Dranoff, G.; Mach, N. Role of GM-CSF Signaling in Cell-Based Tumor Immunization. Blood 2009, 113, 6658–6668. [Google Scholar] [CrossRef] [PubMed]
- McCully, M.L.; Madrenas, J. Dendritic Cells as Arbiters of Peritoneal Immune Responses. Perit. Dial. Int. 2006, 26, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Lanfrancone, L.; Boraschi, D.; Ghiara, P.; Falini, B.; Grignani, F.; Peri, G.; Mantovani, A.; Pelicci, P.G. Human Peritoneal Mesothelial Cells Produce Many Cytokines (Granulocyte Colony-Stimulating Factor [CSF], Granulocyte-Monocyte-CSF, Macrophage-CSF, Interleukin-1 [IL-1], and IL-6) and Are Activated and Stimulated to Grow by IL-1. Blood 1992, 80, 2835–2842. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, K. Diverse Properties of the Mesothelial Cells in Health and Disease. Pleura Peritoneum 2016, 1, 79–89. [Google Scholar] [CrossRef]
- Mutsaers, S.E.; Pixley, F.J.; Prêle, C.M.; Hoyne, G.F. Mesothelial Cells Regulate Immune Responses in Health and Disease: Role for Immunotherapy in Malignant Mesothelioma. Curr. Opin. Immunol. 2020, 64, 88–109. [Google Scholar] [CrossRef]
- Lachaud, C.C.; Rodriguez-Campins, B.; Hmadcha, A.; Soria, B. Use of Mesothelial Cells and Biological Matrices for Tissue Engineering of Simple Epithelium Surrogates. Front. Bioeng. Biotechnol. 2015, 3, 117. [Google Scholar] [CrossRef]
- Shidham, V.B. The Panorama of Different Faces of Mesothelial Cells. CytoJournal 2021, 18, 31. [Google Scholar] [CrossRef]
- Tacke, F.; Trautwein, C.; Yagmur, E.; Hellerbrand, C.; Wiest, R.; Brenner, D.A.; Schnabl, B. Up-Regulated Eotaxin Plasma Levels in Chronic Liver Disease Patients Indicate Hepatic Inflammation, Advanced Fibrosis and Adverse Clinical Course. J. Gastroenterol. Hepatol. 2007, 22, 1256–1264. [Google Scholar] [CrossRef]
- Koç, Ü.; Çetinkaya, E.; Bostanci, E.B.; Kemık, A.S.; Tez, M.; Gömceli, İ.; Akoğlu, M. Diagnostic Significance of Serum Eotaxin-1 Level in Gastric Cancer Patients. Dis. Markers 2013, 35, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Levina, V.; Nolen, B.M.; Marrangoni, A.M.; Cheng, P.; Marks, J.R.; Szczepanski, M.J.; Szajnik, M.E.; Gorelik, E.; Lokshin, A.E. Role of Eotaxin-1 Signaling in Ovarian Cancer. Clin. Cancer Res. 2009, 15, 2647–2656. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Kong, M.; Dong, W.; Dong, C.; Miao, X.; Guo, Y.; Liu, X.; Miao, S.; Li, L.; Chen, T.; et al. Trans-Activation of Eotaxin-1 by Brg1 Contributes to Liver Regeneration. Cell Death Dis. 2022, 13, 495. [Google Scholar] [CrossRef]
- Karabulut, S.; Tas, F.; Akyüz, F.; Ormeci, A.C.; Serilmez, M.; Soydinç, H.O.; Vatansever, S.; Yasasever, V. Clinical Significance of Serum Hepatocyte Growth Factor (HGF) Levels in Hepatocellular Carcinoma. Tumor Biol. 2014, 35, 2327–2333. [Google Scholar] [CrossRef] [PubMed]
- Peng, F.; Liang, C.; Chang, W.; Sun, Q.; Xie, J.; Qiu, H.; Yang, Y. Prognostic Significance of Plasma Hepatocyte Growth Factor in Sepsis. J. Intensive Care Med. 2022, 37, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Jia, C.C.; Wang, T.T.; Liu, W.; Fu, B.S.; Hua, X.; Wang, G.Y.; Li, T.J.; Li, X.; Wu, X.Y.; Tai, Y.; et al. Cancer-Associated Fibroblasts from Hepatocellular Carcinoma Promote Malignant Cell Proliferation by HGF Secretion. PLoS ONE 2013, 8, e63243. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.S.; Grassberger, C.; Yeap, B.Y.; Jiang, W.; Wo, J.Y.; Goyal, L.; Clark, J.W.; Crane, C.H.; Koay, E.J.; Dima, S.; et al. Pretreatment Plasma HGF as Potential Biomarker for Susceptibility to Radiation-Induced Liver Dysfunction after Radiotherapy. npj Precis. Oncol. 2018, 2, 22. [Google Scholar] [CrossRef]
- Cuneo, K.C.; Devasia, T.; Sun, Y.; Schipper, M.J.; Karnak, D.; Davis, M.A.; Owen, D.; Feng, M.; El Naqa, I.; Bazzi, L.; et al. Serum Levels of Hepatocyte Growth Factor and CD40 Ligand Predict Radiation-Induced Liver Injury. Transl. Oncol. 2019, 12, 889–894. [Google Scholar] [CrossRef]
- Wang, H.; Rao, B.; Lou, J.; Li, J.; Liu, Z.; Li, A.; Cui, G.; Ren, Z.; Yu, Z. The Function of the HGF/c-Met Axis in Hepatocellular Carcinoma. Front. Cell Dev. Biol. 2020, 8, 55. [Google Scholar] [CrossRef]
- Meng, W.; Chen, T. Association between the HGF/c-MET Signaling Pathway and Tumorigenesis, Progression and Prognosis of Hepatocellular Carcinoma. Oncol. Rep. 2021, 46, 191. [Google Scholar] [CrossRef] [PubMed]
- Yepes Barreto, I.D.J.; Múnera Contreras, M.N.; Suárez-Causado, A. Relationship between Hepatocyte Growth Factor (HGF) and Stage of Cirrhosis. Rev. Colomb. Gastroenterol. 2017, 32, 24. [Google Scholar] [CrossRef]
- Gitto, S.B.; Beardsley, J.M.; Nakkina, S.P.; Oyer, J.L.; Cline, K.A.; Litherland, S.A.; Copik, A.J.; Khaled, A.S.; Fanaian, N.; Arnoletti, J.P.; et al. Identification of a Novel IL-5 Signaling Pathway in Chronic Pancreatitis and Crosstalk with Pancreatic Tumor Cells. Cell Commun. Signal. 2020, 18, 95. [Google Scholar] [CrossRef] [PubMed]
- Newaz Khan, K.; Masuzaki, H.; Fujishita, A.; Kitajima, M.; Hiraki, K.; Miura, S.; Sekine, I.; Ishimaru, T. Peritoneal Fluid and Serum Levels of Hepatocyte Growth Factor May Predict the Activity of Endometriosis. Acta Obstet. Gynecol. Scand. 2006, 85, 458–466. [Google Scholar] [CrossRef][Green Version]
- Liepelt, A.; Tacke, F. Stromal Cell-Derived Factor-1 (SDF-1) as a Target in Liver Diseases. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 311, G203–G209. [Google Scholar] [CrossRef]
- Majka, M.; Drukala, J.; Lesko, E.; Wysoczynski, M.; Jenson, A.B.; Ratajczak, M.Z. SDF-1 Alone and in Co-Operation with HGF Regulates Biology of Human Cervical Carcinoma Cells. Folia Histochem. Cytobiol. 2006, 44, 155–164. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| with HCC 1 with Virus | with HCC without Virus | without HCC with Virus | without HCC without Virus | Total | ||
|---|---|---|---|---|---|---|
| Total | N | 10 | 11 | 10 | 13 | 44 |
| Age | Median (Q1, Q3) | 59 (56, 72) | 63 (55, 65) | 63 (53.50, 74) | 66 (54, 69) | 63 (54, 69.5) |
| Gender | Female | 3 (30.0%) | 4 (36.4%) | 5 (50.0%) | 7 (53.8%) | 19 (43.2%) |
| Male | 7 (70.0%) | 7 (63.6%) | 5 (50.0%) | 6 (46.2%) | 25 (56.8%) | |
| HBsAg 2 | Positive | 2 (20.0%) | 0 (0.0%) | 2 (9.5%) | ||
| Negative | 8 (80.0%) | 11 (100.0%) | 19 (90.5%) | |||
| Tumor encapsulation | Yes | 1 (10.0%) | 1 (9.1%) | 2 (9.5%) | ||
| Diameter (cm) | ≤5 | 6 (60.0%) | 7 (63.6%) | 13 (61.9%) | ||
| >5 | 4 (40.0%) | 4 (36.4%) | 8 (38.1%) | |||
| Tumor multiplicity | Multiple | 8 (80.0%) | 9 (81.8%) | 17 (81.0%) | ||
| Solitary | 2 (20.0%) | 2 (18.2%) | 4 (19.0%) | |||
| Histological grade | Poorly differentiated | 5 (50.0%) | 4 (36.4%) | 9 (42.9%) | ||
| Moderately differentiated | 3 (30.0%) | 4 (36.4%) | 7 (33.3%) | |||
| Well differentiated | 2 (20.0%) | 3 (27.3%) | 5 (23.8%) | |||
| Alpha-fetoprotein | Median (Q1, Q3) | 34.9 (8.2, 904.2) | 36.0 (8.4, 183.0) | 36.00 (6.3, 344.0) | ||
| Microvascular invasion | Yes | 5 (50.0%) | 6 (54.5%) | 11 (52.4%) | ||
| AJCC 3 stage | I | 2 (20.0%) | 2 (18.2%) | 4 (19.0%) | ||
| II | 0 (0.0%) | 1 (9.1%) | 1 (4.8%) | |||
| III | 3 (30.0%) | 2 (18.2%) | 5 (23.8%) | |||
| IV | 5 (50.0%) | 6 (54.5%) | 11 (52.4%) | |||
| T 4 | T1 | 2 (20.0%) | 2 (18.2%) | 4 (19.0%) | ||
| T2 | 2 (20.0%) | 2 (18.2%) | 4 (19.0%) | |||
| T3 | 6 (60.0%) | 6 (54.6%) | 12 (27.3%) | |||
| T4 | 0 (0.0%) | 1 (9.1%) | 1 (4.8%) | |||
| N | N0 | 5 (50.0%) | 3 (27.3%) | 8 (38.1%) | ||
| N1 | 4 (40.0%) | 6 (54.5%) | 10 (47.6%) | |||
| NX | 1 (10.0%) | 2 (18.2%) | 3 (14.3%) | |||
| M | M0 | 8 (80.0%) | 9 (81.8%) | 17 (81.0%) | ||
| M1 | 2 (20.0%) | 2 (18.2%) | 4 (19.0%) |
| without HCC | with HCC | Total | p-Value | |
|---|---|---|---|---|
| Total | 23 | 21 | 44 | |
| Ascites | ||||
| IL-13 | 4.12 (0.60, 9.40) | 0.00 (0.00, 0.26) | 0.38 (0.00, 5.75) | 0.041 |
| IL-17A | 15.95 (4.43, 41.40) | 0.00 (0.00, 3.70) | 4.44 (0.00, 20.36) | 0.041 |
| IFN-α | 1.90 (0.60, 5.99) | 0.00 (0.00, 0.86) | 0.69 (0.00, 2.84) | 0.041 |
| IFN-γ | 3.52 (0.47, 14.74) | 0.00 (0.00, 1.56) | 0.90 (0.00, 6.88) | 0.041 |
| Plasma | ||||
| IL-2 | 16.12 (11.21, 42.38) | 7.44 (5.18, 11.65) | 11.54 (6.71, 17.80) | 0.041 |
| IL-5 | 1.41 (0.00, 27.71) | 0.00 (0.00, 0.00) | 0.00 (0.00, 6.94) | 0.041 |
| IL-15 | 39.57 (15.66, 93.03) | 0.00 (0.00, 11.56) | 14.04 (0.00, 50.77) | 0.041 |
| IFN-α | 0.37 (0.04, 1.61) | 0.00 (0.00, 0.03) | 0.04 (0.00, 0.85) | 0.041 |
| GM-CSF | 37.85 (11.30, 78.72) | 2.60 (0.00, 17.70) | 14.37 (0.00, 49.10) | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasolato, S.; Del Bianco, P.; Malacrida, S.; Mattiolo, A.; Gringeri, E.; Angeli, P.; Pontisso, P.; Calabrò, M.L. Studies on the Role of Compartmentalized Profiles of Cytokines in the Risk of Hepatocellular Carcinoma. Int. J. Mol. Sci. 2023, 24, 13432. https://doi.org/10.3390/ijms241713432
Fasolato S, Del Bianco P, Malacrida S, Mattiolo A, Gringeri E, Angeli P, Pontisso P, Calabrò ML. Studies on the Role of Compartmentalized Profiles of Cytokines in the Risk of Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2023; 24(17):13432. https://doi.org/10.3390/ijms241713432
Chicago/Turabian StyleFasolato, Silvano, Paola Del Bianco, Sandro Malacrida, Adriana Mattiolo, Enrico Gringeri, Paolo Angeli, Patrizia Pontisso, and Maria Luisa Calabrò. 2023. "Studies on the Role of Compartmentalized Profiles of Cytokines in the Risk of Hepatocellular Carcinoma" International Journal of Molecular Sciences 24, no. 17: 13432. https://doi.org/10.3390/ijms241713432
APA StyleFasolato, S., Del Bianco, P., Malacrida, S., Mattiolo, A., Gringeri, E., Angeli, P., Pontisso, P., & Calabrò, M. L. (2023). Studies on the Role of Compartmentalized Profiles of Cytokines in the Risk of Hepatocellular Carcinoma. International Journal of Molecular Sciences, 24(17), 13432. https://doi.org/10.3390/ijms241713432