
Research Progress of DcR3 in the Diagnosis and Treatment of Sepsis


Abstract
:1. Introduction
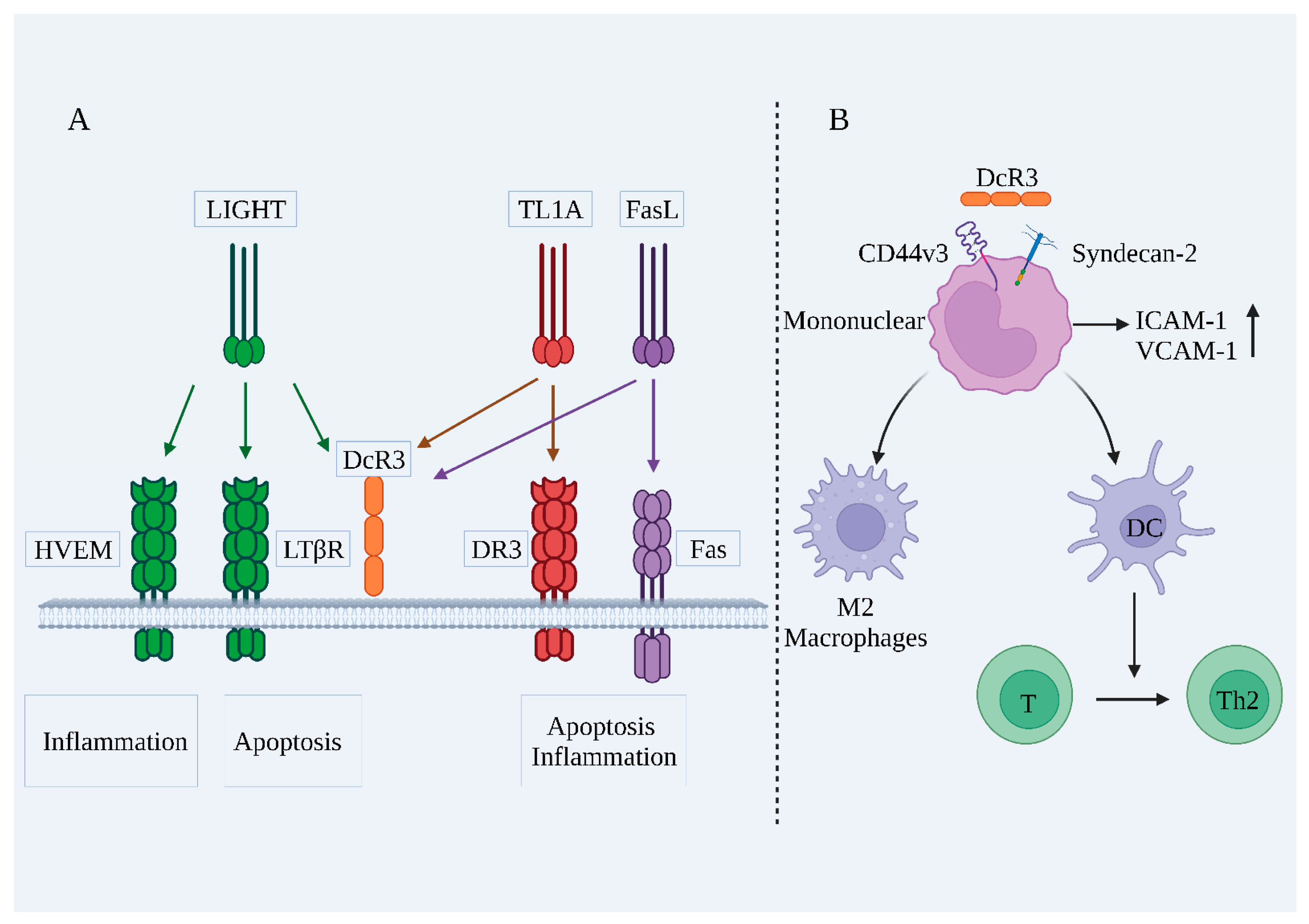
2. DcR3
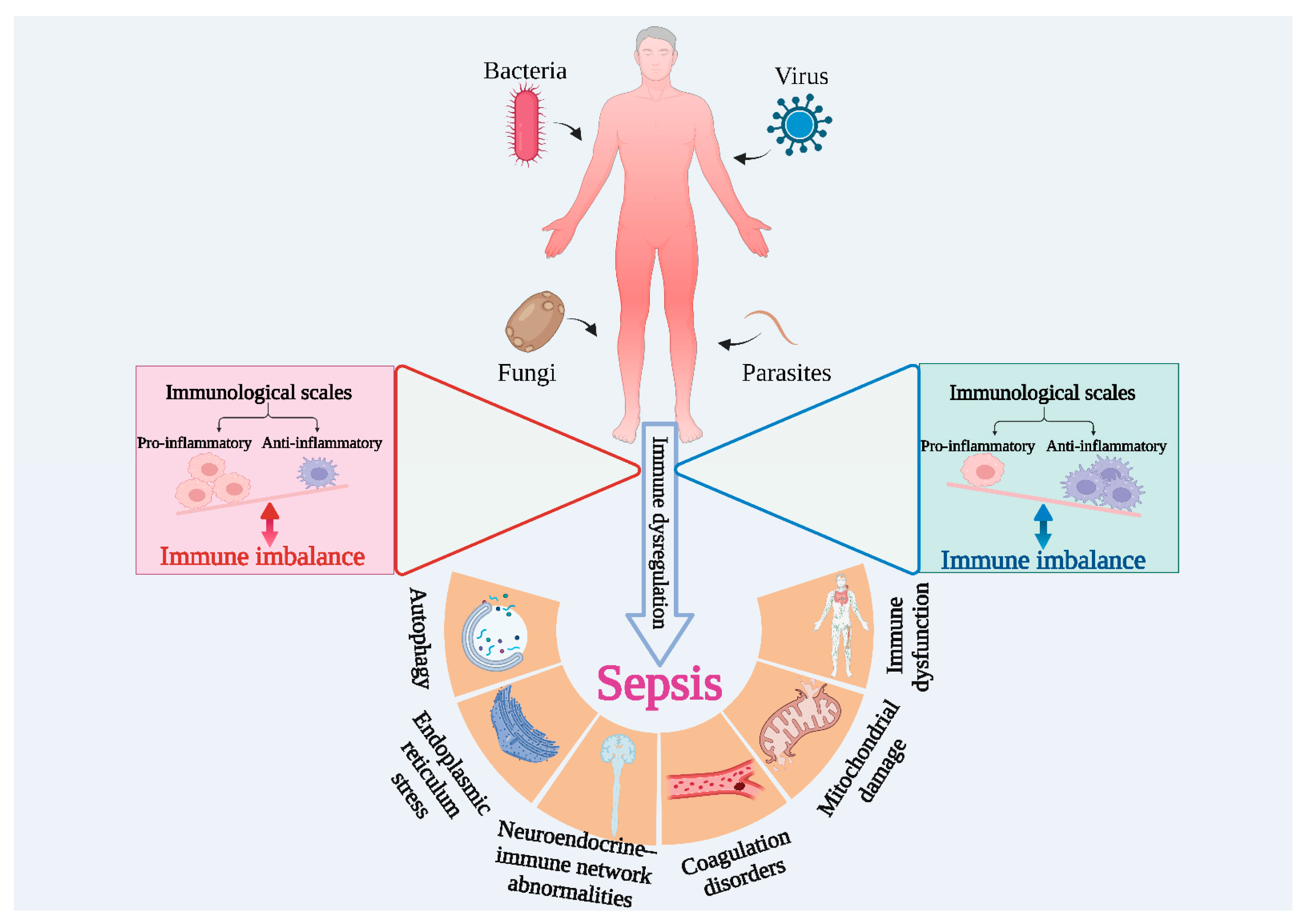
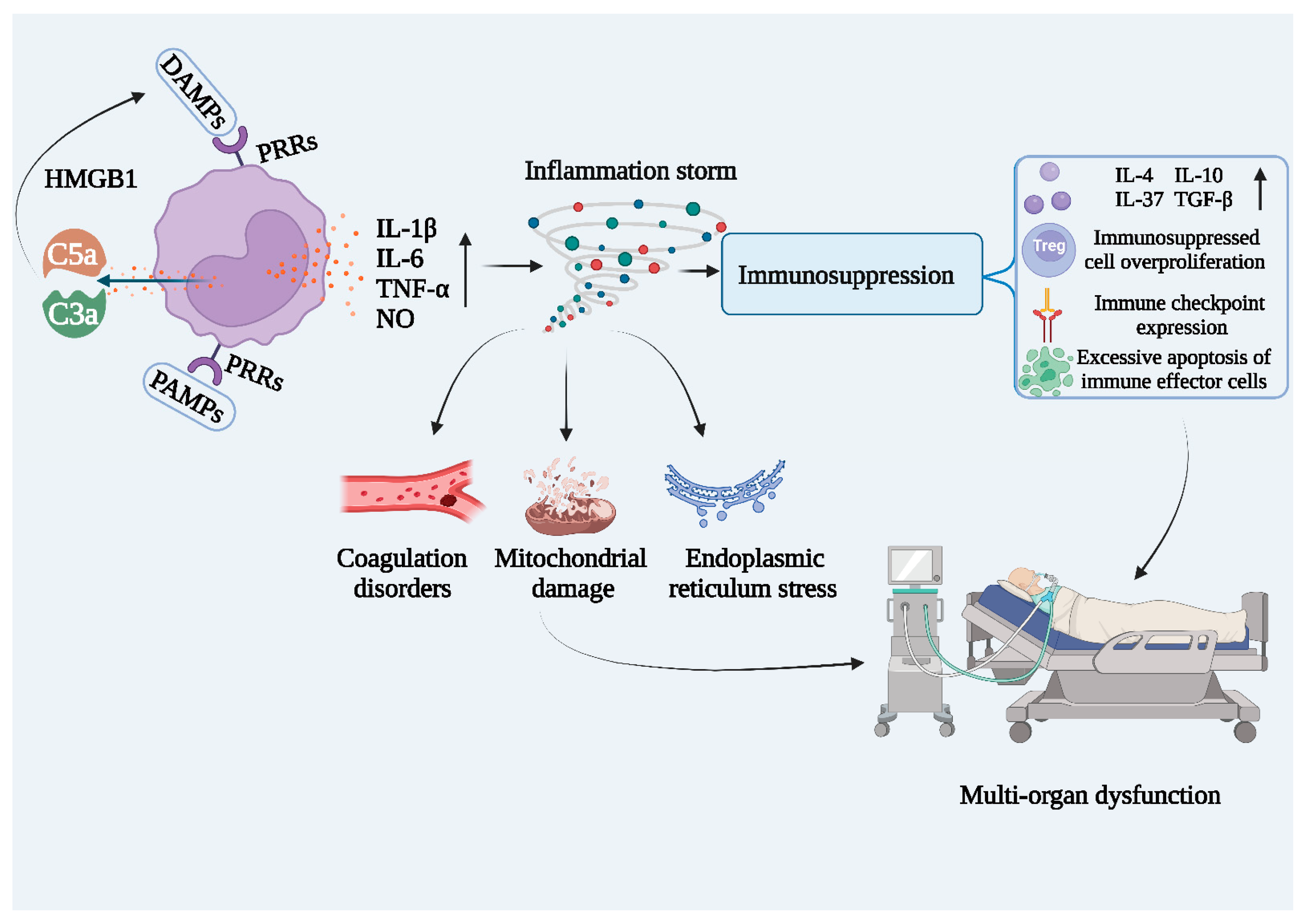
3. Sepsis
4. DcR3 as a Biomarker for Sepsis
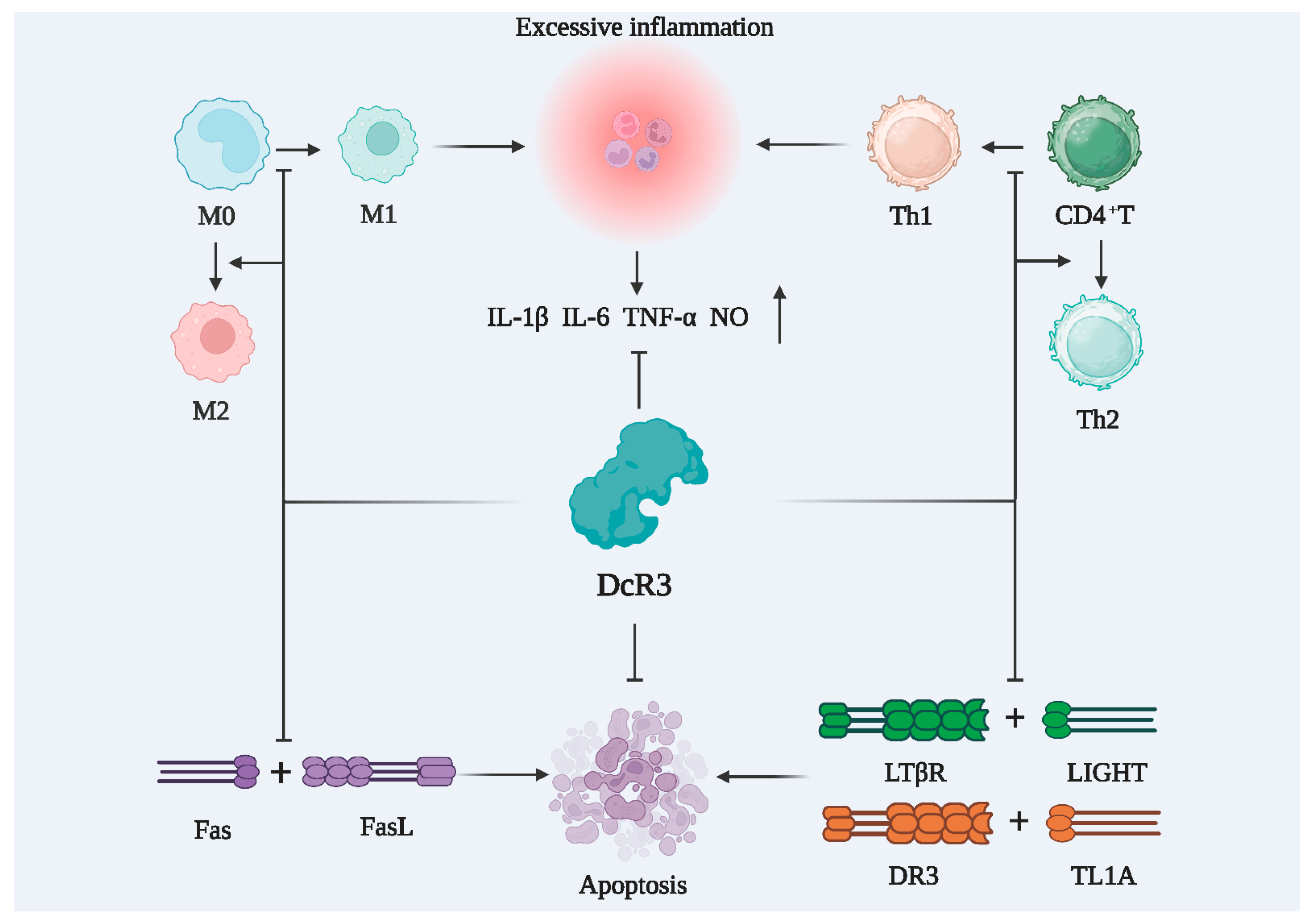
5. DcR3 as a Drug for Sepsis Treatment
6. Summary and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Doustkami, H.; Avesta, L.; Babapour, B.; Boskabady, M.H.; Nikoukhesal, A.; Aslani, M.R. Correlation of Serum Decoy Receptor 3 and Interleukin-6 with Severity of Coronary Artery Diseases in Male Acute Myocardial Infarction Patients. Acta Biomed. 2021, 92, e2021285. [Google Scholar] [CrossRef]
- Peng, Y.J.; Peng, C.T.; Lin, Y.H.; Lin, G.J.; Huang, S.H.; Chen, S.J.; Sytwu, H.K.; Cheng, C.P. Decoy Receptor 3 Promotes Preosteoclast Cell Death via Reactive Oxygen Species-Induced Fas Ligand Expression and the IL-1α/IL-1 Receptor Antagonist Pathway. Mediat. Inflamm. 2020, 2020, 1237281. [Google Scholar] [CrossRef]
- Kerget, F.; Kerget, B.; Laloglu, E. Evaluation of the Role of Serum DcR3 Levels in the Early Clinical Prognosis of Patients with Crimean-Congo Hemorrhagic Fever. Clin. Biochem. 2023, 118, 110574. [Google Scholar] [CrossRef]
- Cecconi, M.; Evans, L.; Levy, M.; Rhodes, A. Sepsis and Septic Shock. Lancet 2018, 392, 75–87. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Tidswell, R.; Singer, M. Sepsi-Thoughtful Management for the Non-expert. Clin. Med. 2018, 18, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Mulita, F.; Liolis, E.; Akinosoglou, K.; Tchabashvili, L.; Maroulis, I.; Kaplanis, C.; Vailas, M.; Panos, G. Postoperative sepsis after colorectal surgery: A prospective single-center observational study and review of the literature. Prz. Gastroenterol. 2022, 17, 47–51. [Google Scholar] [CrossRef]
- Gao, L.; Yang, B.; Zhang, H.; Ou, Q.; Lin, Y.; Zhang, M.; Zhang, Z.; Kim, S.; Wu, B.; Wang, Z.; et al. DcR3, a New Biomarker for Sepsis, Correlates with Infection Severity and Procalcitonin. Oncotarget 2018, 9, 10934–10944. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Hou, Y.; Lou, X.; Chen, H. Decoy Receptor 3 Improves Survival in Experimental Sepsis by Suppressing the Inflammatory Response and Lymphocyte Apoptosis. PLoS ONE 2015, 10, e0131680. [Google Scholar] [CrossRef]
- Weng, S.C.; Tarng, D.C. Role of Prognostic Biomarker Decoy Receptor 3 and Immunomodulation in Kidney Diseases. J. Chin. Med. Assoc. 2019, 82, 680–684. [Google Scholar] [CrossRef]
- Lagou, S.; Grapsa, D.; Syrigos, N.; Bamias, G. The Role of Decoy Receptor DcR3 in Gastrointestinal Malignancy. Cancer Diagn. Progn. 2022, 2, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Pitti, R.M.; Marsters, S.A.; Lawrence, D.A.; Roy, M.; Kischkel, F.C.; Dowd, P.; Huang, A.; Donahue, C.J.; Sherwood, S.W.; Baldwin, D.T.; et al. Genomic Amplification of a Decoy Receptor for Fas Ligand in Lung and Colon Cancer. Nature 1998, 396, 699–703. [Google Scholar] [CrossRef]
- Ge, H.; Liang, C.; Ren, S.; Yue, C.; Wu, J. Prognostic Value of DcR3 in Solid Tumors: A Meta-analysis. Clin. Chim. Acta 2018, 481, 126–131. [Google Scholar] [CrossRef]
- Wu, N.L.; Huang, D.Y.; Hsieh, S.L.; Dai, Y.S.; Lin, W.W. Decoy Receptor 3 Is Involved in Epidermal Keratinocyte Commitment to Terminal Differentiation via EGFR and PKC Activation. Exp. Mol. Med. 2022, 54, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Ge, H.; Liang, C.; Li, Z.; An, D.; Ren, S.; Yue, C.; Wu, J. DcR3 Induces Proliferation, Migration, Invasion, and EMT in Gastric Cancer Cells via the PI3K/AKT/GSK-3β/β-catenin Signaling Pathway. Onco Targets Ther. 2018, 11, 4177–4187. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Chen, X.; Yang, J.; Yao, J.; Yin, N.; Zhang, Z.; Li, D.; Zhu, D.; Zhou, J. DcR3 Promotes Proliferation and Invasion of Pancreatic Cancer via a DcR3/STAT1/IRF1 Feedback Loop. Am. J. Cancer Res. 2019, 9, 2618–2633. [Google Scholar] [PubMed]
- Min, D.; Wu, B.; Chen, L.; Chen, R.; Wang, J.; Zhang, H.; Chen, J.; Kim, S.; Zhang, L.; Xia, Z.; et al. Level of Decoy Receptor 3 for Monitoring Clinical Progression of Severe Burn Patients. J. Burn. Care Res. 2021, 42, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Soliman, M.H.; Ebaid, A.M. Association of Tumor Necrosis Like Factor 1 A (TL1A) and Its Decoy Receptor (DcR3) with the Disease Activity and Autoantibody Production in Rheumatoid Arthritis Patients. Egypt. J. Immunol. 2019, 26, 43–54. [Google Scholar] [PubMed]
- Ghobadi, H.; Hosseini, N.; Aslani, M.R. Correlations Between Serum Decoy Receptor 3 and Airflow Limitation and Quality of Life in Male Patients with Stable Stage and Acute Exacerbation of COPD. Lung 2020, 198, 515–523. [Google Scholar] [CrossRef]
- Liang, D.Y.; Sha, S.; Yi, Q.; Shi, J.; Chen, Y.; Hou, Y.; Chang, Q. Hepatitis B X Protein Upregulates Decoy Receptor 3 Expression via the PI3K/NF-κB Pathway. Cell. Signal. 2019, 62, 109346. [Google Scholar] [CrossRef]
- Zhong, M.; Qiu, X.; Liu, Y.; Yang, Y.; Gu, L.; Wang, C.; Chen, H.; Liu, Z.; Miao, J.; Zhuang, G. TIPE Regulates DcR3 Expression and Function by Activating the PI3K/AKT Signaling Pathway in CRC. Front. Oncol. 2020, 10, 623048. [Google Scholar] [CrossRef]
- Hou, Y.; Liang, D.; Liu, Y.; Chen, H.; Lou, X. Up-Regulation of DcR3 in Microbial Toxins-Stimulated HUVECs Involves NF-κB Signalling. BMC Biochem. 2018, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, R.; Chen, W.; Lai, L.; Li, Z. Decoy Receptor-3 Regulates Inflammation and Apoptosis via PI3K/AKT Signaling Pathway in Coronary Heart Disease. Exp. Ther. Med. 2019, 17, 2614–2622. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, X.; Li, D.; Cui, L.; Li, X.; Ye, X.; Wan, X. DcR3 Promotes Hepatoma Cell Migration by Downregulating E-Cadherin Expression. Oncol. Rep. 2017, 38, 377–383. [Google Scholar] [CrossRef]
- Fukuda, K.; Miura, Y.; Maeda, T.; Hayashi, S.; Kuroda, R. Decoy Receptor 3 Down-Regulates Centrosomal Protein 70 kDa Specifically in Rheumatoid Synovial Fibroblasts. Mod. Rheumatol. 2018, 28, 287–292. [Google Scholar] [CrossRef]
- Jin, Z.; Liu, S.; Zhan, Q.; Shao, X.; Ma, J.; Pan, L. Decoy Receptor 3 Alleviates Hepatic Fibrosis Through Suppressing Inflammation Activated by NF-κB Signaling Pathway. Adv. Clin. Exp. Med. 2018, 27, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Hou, H.T.; Chen, H.X.; Wang, Z.Q.; He, G.W. Increased Circulating Levels of Tumor Necrosis Factor-like Cytokine 1A and Decoy Receptor 3 Correlate with SYNTAX Score in Patients Undergoing Coronary Surgery. J. Int. Med. Res. 2018, 46, 5167–5175. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.L.; Lin, W.W. Decoy Receptor 3: An Endogenous Immunomodulator in Cancer Growth and Inflammatory Reactions. J. Biomed. Sci. 2017, 24, 39. [Google Scholar] [CrossRef]
- Malarkannan, S. Molecular Mechanisms of FASL-Mediated ‘Reverse-Signaling’. Mol. Immunol. 2020, 127, 31–37. [Google Scholar] [CrossRef]
- Huang, P.; Wang, C.H.; Zhuo, L.Y.; Xia, X.S.; Yang, S.; Zhang, J.W.; Fan, H.Z.; Wu, J.J.; Yu, R.; Yue, M.; et al. Polymorphisms rs763110 in FASL Is Linked to Hepatitis C Virus Infection Among High-Risk Populations. Br. J. Biomed. Sci. 2020, 77, 112–117. [Google Scholar] [CrossRef]
- Yuan, Y.; Zhang, Y.; Zhao, S.; Chen, J.; Yang, J.; Wang, T.; Zou, H.; Wang, Y.; Gu, J.; Liu, X.; et al. Cadmium-Induced Apoptosis in Neuronal Cells Is Mediated by Fas/FASL-Mediated Mitochondrial Apoptotic Signaling Pathway. Sci. Rep. 2018, 8, 8837. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Kocab, A.J.; Zacks, D.N.; Marshak-Rothstein, A.; Gregory-Ksander, M. A Small Peptide Antagonist of the Fas Receptor Inhibits Neuroinflammation and Prevents Axon Degeneration and Retinal Ganglion Cell Death in an Inducible Mouse Model of Glaucoma. J. Neuroinflamm. 2019, 16, 184. [Google Scholar] [CrossRef] [PubMed]
- Abudukeyoumu, A.; Lai, Z.Z.; Lu, J.J.; Zhang, X.; Hou, D.Y.; Dong, J.; Wu, J.N.; Li, M.Q.; Xie, F. A LIGHT-HVEM/LTβR Axis Contributes to the Fibrosis of Intrauterine Adhesion. J. Reprod. Immunol. 2022, 153, 103693. [Google Scholar] [CrossRef] [PubMed]
- del Rio, M.L.; Fernandez-Renedo, C.; Chaloin, O.; Scheu, S.; Pfeffer, K.; Shintani, Y.; Perez-Simon, J.A.; Schneider, P.; Rodriguez-Barbosa, J.I. Immunotherapeutic Targeting of LIGHT/LTβR/HVEM Pathway Fully Recapitulates the Reduced Cytotoxic Phenotype of LIGHT-Deficient T Cells. mAbs 2016, 8, 478–490. [Google Scholar] [CrossRef]
- Perlin, D.S.; Zafir-Lavie, I.; Roadcap, L.; Raines, S.; Ware, C.F.; Neil, G.A. Levels of the TNF-Related Cytokine LIGHT Increase in Hospitalized COVID-19 Patients with Cytokine Release Syndrome and ARDS. mSphere 2020, 5, 10–128. [Google Scholar] [CrossRef] [PubMed]
- Valatas, V.; Kolios, G.; Bamias, G. TL1A (TNFSF15) and DR3 (TNFRSF25): A Co-stimulatory System of Cytokines with Diverse Functions in Gut Mucosal Immunity. Front. Immunol. 2019, 10, 583. [Google Scholar] [CrossRef]
- Safaya, S.; Alfarhan, M.; Sulaiman, A.; Alsulaiman, A.; Al-Ali, A. TNFSF/TNFRSF Cytokine Gene Expression in Sickle Cell Anemia: Up-Regulated TNF-Like Cytokine 1A (TL1A) and Its Decoy Receptor (DcR3) in Peripheral Blood Mononuclear Cells and Plasma. Cytokine 2019, 123, 154744. [Google Scholar] [CrossRef]
- Xu, W.D.; Li, R.; Huang, A.F. Role of TL1A in Inflammatory Autoimmune Diseases: A Comprehensive Review. Front. Immunol. 2022, 13, 891328. [Google Scholar] [CrossRef]
- Yeh, C.C.; Yang, M.J.; Lussier, E.C.; Tsai, H.W.; Lo, P.F.; Hsieh, S.L.; Wang, P.H. Low Plasma Levels of Decoy Receptor 3 (DcR3) in the Third Trimester of Pregnancy with Preeclampsia. Taiwan. J. Obstet. Gynecol. 2019, 58, 349–353. [Google Scholar] [CrossRef]
- Kumanishi, S.; Yamanegi, K.; Nishiura, H.; Fujihara, Y.; Kobayashi, K.; Nakasho, K.; Futani, H.; Yoshiya, S. Epigenetic Modulators Hydralazine and Sodium Valproate Act Synergistically in VEGI-Mediated Anti-angiogenesis and VEGF Interference in Human Osteosarcoma and Vascular Endothelial Cells. Int. J. Oncol. 2019, 55, 167–178. [Google Scholar] [CrossRef]
- Lee, P.C.; Yang, L.Y.; Wang, Y.W.; Huang, S.F.; Lee, K.C.; Hsieh, Y.C.; Yang, Y.Y.; Hsieh, S.L.; Hou, M.C.; Lin, H.C.; et al. Mechanisms of the Prevention and Inhibition of the Progression and Development of Non-alcoholic Steatohepatitis by Genetic and Pharmacological Decoy Receptor 3 Supplementation. Hepatol. Res. 2017, 47, 1260–1271. [Google Scholar] [CrossRef] [PubMed]
- Li, T.H.; Liu, C.W.; Lee, P.C.; Huang, C.C.; Lee, K.C.; Hsieh, Y.C.; Yang, Y.Y.; Hsieh, S.L.; Lin, H.C.; Tsai, C.Y. Decoy Receptor 3 Analogous Supplement Protects Steatotic Rat Liver from Ischemia-reperfusion Injury. J. Chin. Med. Assoc. 2017, 80, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Kan, H.T.; Liu, C.Y.; Yu, W.K.; Lee, S.S.; Wang, J.H.; Hsieh, S.L. Serum Decoy Receptor 3 is a Biomarker for Disease Severity in Nonatopic Asthma Patients. J. Formos. Med. Assoc. 2017, 116, 49–56. [Google Scholar] [CrossRef]
- Yan, Y.; Song, D.; Liu, L.; Meng, X.; Qi, C.; Wang, J. The Relationship of Plasma Decoy Receptor 3 and Coronary Collateral Circulation in Patients with Coronary Artery Disease. Life Sci. 2017, 15, 84–88. [Google Scholar] [CrossRef]
- Lin, S.; Wu, B.; Lin, Y.; Wang, M.; Zhu, Y.; Jiang, J.; Zhang, L.; Lin, J. Expression and Clinical Significance of Decoy Receptor 3 in Acute-on-Chronic Liver Failure. Biomed. Res. Int. 2019, 18, 9145736. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.C.; Wen, M.C.; Hsieh, S.L.; Chen, N.J.; Tarng, D.C. Decoy Receptor 3 Suppresses T-Cell Priming and Promotes Apoptosis of Effector T-Cells in Acute Cell-Mediated Rejection: The Role of Reverse Signaling. Front. Immunol. 2022, 13, 879648. [Google Scholar] [CrossRef]
- Liu, Y.L.; Chen, W.T.; Lin, Y.Y.; Lu, P.H.; Hsieh, S.L.; Cheng, I.H. Amelioration of Amyloid-β-Induced Deficits by DcR3 in an Alzheimer’s Disease Model. Mol. Neurodegener. 2017, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Termini, C.M.; Pang, A.; Li, M.; Fang, T.; Chang, V.Y.; Chute, J.P. Syndecan-2 Enriches for Hematopoietic Stem Cells and Regulates Stem Cell Repopulating Capacity. Blood 2022, 139, 188–204. [Google Scholar] [CrossRef]
- Connor, J.P.; Felder, M.; Kapur, A.; Onujiogu, N. DcR3 Binds to Ovarian Cancer via Heparan Sulfate Proteoglycans and Modulates Tumor Cells Response to Platinum with Corresponding Alteration in the Expression of BRCA1. BMC Cancer 2012, 12, 176. [Google Scholar] [CrossRef]
- Pan, Y.G.; Huang, M.T.; Sekar, P.; Huang, D.Y.; Lin, W.W.; Hsieh, S.L. Decoy Receptor 3 Inhibits Monosodium Urate-Induced NLRP3 Inflammasome Activation via Reduction of Reactive Oxygen Species Production and Lysosomal Rupture. Front. Immunol. 2021, 3, 638676. [Google Scholar] [CrossRef]
- Liang, C.; Xu, Y.; Li, G.; Zhao, T.; Xia, F.; Li, G.; Zhang, D.; Wu, J. Downregulation of DcR3 Sensitizes Hepatocellular Carcinoma Cells to TRAIL-Induced Apoptosis. Onco Targets Ther. 2017, 10, 417–428. [Google Scholar] [CrossRef]
- Bullock, B.; Benham, M.D. Bacterial Sepsis. In StatPearls; StatPearls Publishing LLC: Tampa, FL, USA, 2023. [Google Scholar]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, Regional, and National Sepsis Incidence and Mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Y.; Ning, B.T. Signaling Pathways and Intervention Therapies in Sepsis. Signal Transduct. Target. Ther. 2021, 6, 407. [Google Scholar] [CrossRef] [PubMed]
- Kingren, M.S.; Starr, M.E.; Saito, H. Divergent Sepsis Pathophysiology in Older Adults. Antioxid. Redox Signal. 2021, 35, 1358–1375. [Google Scholar] [CrossRef]
- Huang, M.; Cai, S.; Su, J. The Pathogenesis of Sepsis and Potential Therapeutic Targets. Int. J. Mol. Sci. 2019, 20, 5376. [Google Scholar] [CrossRef]
- Wang, P.; Feng, Z.; Sang, X.; Chen, W.; Zhang, X.; Xiao, J.; Chen, Y.; Chen, Q.; Yang, M.; Su, J. Kombucha Ameliorates LPS-Induced Sepsis in a Mouse Model. Food Funct. 2021, 12, 10263–10280. [Google Scholar] [CrossRef]
- Reinhart, K.; Daniels, R.; Kissoon, N.; Machado, F.R.; Schachter, R.D.; Finfer, S. Recognizing Sepsis as a Global Health Priority-A WHO Resolution. N. Engl. J. Med. 2017, 377, 414–417. [Google Scholar] [CrossRef]
- Salomão, R.; Ferreira, B.L.; Salomão, M.C.; Santos, S.S.; Azevedo, L.C.P.; Brunialti, M.K.C. Sepsis: Evolving Concepts and Challenges. Braz. J. Med. Biol. Res. 2019, 52, e8595. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.; Legrand, M. Epidemiology of Sepsis and Septic Shock. Curr. Opin. Anaesthesiol. 2021, 34, 71–76. [Google Scholar] [CrossRef]
- Hecker, A.; Reichert, M.; Reuß, C.J.; Schmoch, T.; Riedel, J.G.; Schneck, E.; Padberg, W.; Weigand, M.A.; Hecker, M. Intra-abdominal Sepsis: New Definitions and Current Clinical Standards. Langenbecks Arch. Surg. 2019, 404, 257–271. [Google Scholar] [CrossRef]
- Thompson, K.; Venkatesh, B.; Finfer, S. Sepsis and Septic Shock: Current Approaches to Management. Intern. Med. J. 2019, 49, 160–170. [Google Scholar] [CrossRef]
- Cavaillon, J.M.; Singer, M.; Skirecki, T. Sepsis Therapies: Learning from 30 Years of Failure of Translational Research to Propose New Leads. EMBO Mol. Med. 2020, 12, e10128. [Google Scholar] [CrossRef]
- Su, J.; Guo, K.; Huang, M.; Liu, Y.; Zhang, J.; Sun, L.; Li, D.; Pang, K.L.; Wang, G.; Chen, L.; et al. Fucoxanthin, a Marine Xanthophyll Isolated from Conticribra weissflogii ND-8: Preventive Anti-Inflammatory Effect in a Mouse Model of Sepsis. Front. Pharmacol. 2019, 10, 906. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Valenzuela-Sánchez, F.; Ruiz-Rodriguez, M.; Moyano, S. Sepsis: A Review of Advances in Management. Adv. Ther. 2017, 34, 2393–2411. [Google Scholar] [CrossRef] [PubMed]
- Nedeva, C.; Menassa, J.; Puthalakath, H. Sepsis: Inflammation Is a Necessary Evil. Front. Cell Dev. Biol. 2019, 7, 108. [Google Scholar] [CrossRef]
- Tang, D.; Wang, H.; Billiar, T.R.; Kroemer, G.; Kang, R. Emerging Mechanisms of Immunocoagulation in Sepsis and Septic Shock. Trends Immunol. 2021, 42, 508–522. [Google Scholar] [CrossRef]
- Liu, D.; Huang, S.Y.; Sun, J.H.; Zhang, H.C.; Cai, Q.L.; Gao, C.; Li, L.; Cao, J.; Xu, F.; Zhou, Y.; et al. Sepsis-Induced Immunosuppression: Mechanisms, Diagnosis and Current Treatment Options. Mil. Med. Res. 2022, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Minasyan, H. Sepsis: Mechanisms of Bacterial Injury to the Patient. Scand. J. Trauma. Resusc. Emerg. Med. 2019, 27, 19. [Google Scholar] [CrossRef]
- Watkins, R.R.; Bonomo, R.A.; Rello, J. Managing Sepsis in the Era of Precision Medicine: Challenges and Opportunities. Expert Rev. Anti-Infect. Ther. 2022, 20, 871–880. [Google Scholar] [CrossRef]
- Yadav, P.; Yadav, S.K. Progress in Diagnosis and Treatment of Neonatal Sepsis: A Review Article. JNMA J. Nepal Med. Assoc. 2022, 60, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Borges Sá, M.; Belda, S.; Bou, G.; Del Pozo, J.L.; Estrada, O.; Ferrer, R.; González Del Castillo, J.; Julián-Jiménez, A.; Martín-Loeches, I.; et al. Current Aspects in Sepsis Approach. Turning Things Around. Rev. Esp. Quimioter. 2018, 31, 298–315. [Google Scholar] [PubMed]
- Mulita, F.; Verras, G.-I.; Bouchagier, K.; Dafnomili, V.-D.; Perdikaris, I.; Perdikaris, P.; Samaras, A.; Antzoulas, A.; Iliopoulos, F.; Akinosoglou, K.; et al. Butyrylcholinesterase levels as a predictive factor of septic complications development in the postoperative period of colorectal patients: Univariate analysis and predictive modeling. Eur. J. Surg. Oncol. 2023, 49, e15. [Google Scholar] [CrossRef]
- Bahloul, M.; Baccouch, N.; Chtara, K.; Turki, M.; Turki, O.; Hamida, C.B.; Chelly, H.; Ayedi, F.; Chaari, A.; Bouaziz, M. Value of Serum Cholinesterase Activity in the Diagnosis of Septic Shock Due to Bacterial Infections. J. Intensive. Care. Med. 2017, 32, 346–352. [Google Scholar] [CrossRef]
- Velissaris, D.; Zareifopoulos, N.; Karamouzos, V.; Karanikolas, E.; Pierrakos, C.; Koniari, I.; Karanikolas, M. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus 2021, 13, e15019. [Google Scholar] [CrossRef]
- Önal, U.; Valenzuela-Sánchez, F.; Vandana, K.E.; Rello, J. Mid-Regional Pro-Adrenomedullin (MR-proADM) as a Biomarker for Sepsis and Septic Shock: Narrative Review. Healthcare 2018, 6, 110. [Google Scholar] [CrossRef]
- Pierrakos, C.; Velissaris, D.; Bisdorff, M.; Marshall, J.C.; Vincent, J.L. Biomarkers of Sepsis: Time for a Reappraisal. Crit. Care 2020, 24, 287. [Google Scholar] [CrossRef]
- Nagalingam, K. Understanding Sepsis. Br. J. Nurs. 2018, 27, 1168–1170. [Google Scholar] [CrossRef]
- Gotur, D.B. Sepsis in a Panorama: What the Cardiovascular Physician Should Know. Methodist Debakey CardioVasc J. 2018, 14, 89–100. [Google Scholar] [CrossRef]
- Gauer, R.; Forbes, D.; Boyer, N. Sepsis: Diagnosis and Management. Am. Fam. Physician 2020, 101, 409–418. [Google Scholar]
- Srzić, I.; Nesek Adam, V.; Tunjić Pejak, D. Sepsis Definition: What’s New in the Treatment Guidelines. Acta Clin. Croat. 2022, 61 (Suppl. S1), 67–72. [Google Scholar] [CrossRef] [PubMed]
- Brink, A.; Alsma, J.; Verdonschot, R.J.C.G.; Rood, P.P.M.; Zietse, R.; Lingsma, H.F.; Schuit, S.C.E. Predicting Mortality in Patients with Suspected Sepsis at the Emergency Department; A Retrospective Cohort Study Comparing qSOFA, SIRS and National Early Warning Score. PLoS ONE 2019, 14, e0211133. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; He, C.; He, W.; Jiang, T. Lactate-Enhanced-qSOFA (LqSOFA) Score Is Superior to the Other Four Rapid Scoring Tools in Predicting in-Hospital Mortality Rate of the Sepsis Patients. Ann. Transl. Med. 2020, 8, 1013. [Google Scholar] [CrossRef]
- Godinjak, A.; Iglica, A.; Rama, A.; Tančica, I.; Jusufović, S.; Ajanović, A.; Kukuljac, A. Predictive Value of SAPS II and Apache II Scoring Systems for Patient Outcome in a Medical Intensive Care Unit. Acta Med. Acad. 2016, 45, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Boomer, L.A.; Feliz, A. Sepsis Management and the Pediatric Surgeon. Semin. Pediatr. Surg. 2019, 28, 67–72. [Google Scholar] [CrossRef]
- Guarino, M.; Perna, B.; Cesaro, A.E.; Maritati, M.; Spampinato, M.D.; Contini, C.; De Giorgio, R. 2023 Update on Sepsis and Septic Shock in Adult Patients: Management in the Emergency Department. J. Clin. Med. 2023, 12, 3188. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.H.; Kee, A.C.; Li, A.; Rubulotta, F. Controversies in Sepsis Management-What Is the Way Forward? Ann. Acad. Med. Singap. 2020, 49, 661–668. [Google Scholar] [CrossRef]
- Patel, S.; Puri, N.; Dellinger, R.P. Sepsis Management for the Nephrologist. Clin. J. Am. Soc. Nephrol. 2022, 17, 880–889. [Google Scholar] [CrossRef]
- Einav, S.; Leone, M.; Martin-Loeches, I. Sepsis and Antibiotics: When Should We Deploy a Parachute? Int. J. Antimicrob. Agents 2023, 61, 106732. [Google Scholar] [CrossRef]
- Fallon, E.A.; Chung, C.S.; Heffernan, D.S.; Chen, Y.; De Paepe, M.E.; Ayala, A. Survival and Pulmonary Injury After Neonatal Sepsis: PD1/PDL1’s Contributions to Mouse and Human Immunopathology. Front. Immunol. 2021, 12, 634529. [Google Scholar] [CrossRef]
- Wang, X.H.; Xu, D.Q.; Chen, Y.Y.; Yue, S.J.; Fu, R.J.; Huang, L.; Tang, Y.P. Traditional Chinese Medicine: A Promising Strategy to Regulate Inflammation, Intestinal Disorders and Impaired Immune Function Due to Sepsis. Front. Pharmacol. 2022, 13, 952938. [Google Scholar] [CrossRef]
- Holford, P.; Carr, A.C.; Jovic, T.H.; Ali, S.R.; Whitaker, I.S.; Marik, P.E.; Smith, A.D. Vitamin C-an Adjunctive Therapy for Respiratory Infection, Sepsis and COVID-19. Nutrients 2020, 12, 3760. [Google Scholar] [CrossRef] [PubMed]
- Graber, M.L.; Patel, M.; Claypool, S. Sepsis as a Model for Improving Diagnosis. Diagnosis 2018, 5, 3–10. [Google Scholar] [CrossRef]
- Zhu, H.F.; Liu, Y.P.; Liu, D.L.; Ma, Y.D.; Hu, Z.Y.; Wang, X.Y.; Gu, C.S.; Zhong, Y.; Long, T.; Kan, H.P.; et al. Role of TGFβ3-Smads-Sp1 Axis in DcR3-Mediated Immune Escape of Hepatocellular Carcinoma. Oncogenesis 2019, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Abdelmegeid, A.K.; Gabr, M.A.M.; Basanti, C.W.S. Serum Decoy Receptor 3 (DcR3): A Promising Biomarker for Atopic Asthma in Children. Immunol. Res. 2021, 69, 568–575. [Google Scholar] [CrossRef]
- Thompson, K.; Connor, J. When Cultures Fail: Postmortem Decoy Receptor 3 (DcR3) as a Marker of Antemortem Sepsis. Acad. Forensic Pathol. 2019, 9, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.J.; Lou, X.L.; Chen, H.W.; Zhu, F.T.; Hou, Y.Q. Diagnostic Value of Decoy Receptor 3 Combined with Procalcitonin and Soluble Urokinase-Type Plasminogen Activator Receptor for Sepsis. Cell. Mol. Biol. Lett. 2018, 23, 22. [Google Scholar] [CrossRef]
- Nedeva, C. Inflammation and Cell Death of the Innate and Adaptive Immune System During Sepsis. Biomolecules 2021, 11, 1011. [Google Scholar] [CrossRef]
- Zhu, C.L.; Wang, Y.; Liu, Q.; Li, H.R.; Yu, C.M.; Li, P.; Deng, X.M.; Wang, J.F. Dysregulation of Neutrophil Death in Sepsis. Front. Immunol. 2022, 13, 963955. [Google Scholar] [CrossRef]
- Zhang, W.; Fang, X.; Gao, C.; Song, C.; He, Y.; Zhou, T.; Yang, X.; Shang, Y.; Xu, J. MDSCs in Sepsis-Induced Immunosuppression and Its Potential Therapeutic Targets. Cytokine Growth Factor Rev. 2023, 69, 90–103. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Qu, M.; Li, W.; Wu, D.; Cata, J.P.; Miao, C. Neutrophil, Neutrophil Extracellular Traps and Endothelial Cell Dysfunction in Sepsis. Clin. Transl. Med. 2023, 13, e1170. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Umemura, Y.; Wada, H.; Levy, J.H. Roles of Coagulation Abnormalities and Microthrombosis in Sepsis: Pathophysiology, Diagnosis, and Treatment. Arch. Med. Res. 2021, 52, 788–797. [Google Scholar] [CrossRef]
- Huang, M.T.; Chen, S.T.; Wu, H.Y.; Chen, Y.J.; Chou, T.Y.; Hsieh, S.L. DcR3 Suppresses Influenza Virus-Induced Macrophage Activation and Attenuates Pulmonary Inflammation and Lethality. J. Mol. Med. 2015, 93, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Yao, R.Q.; Ren, C.; Zheng, L.Y.; Xia, Z.F.; Yao, Y.M. Advances in Immune Monitoring Approaches for Sepsis-Induced Immunosuppression. Front. Immunol. 2022, 13, 891024. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liang, G.; Shen, J.; Kong, H.; Wu, D.; Huang, J.; Li, X. Long Non-coding RNAs as Biomarkers and Therapeutic Targets in Sepsis. Front. Immunol. 2021, 12, 722004. [Google Scholar] [CrossRef]
- Chiu, C.W.; Huang, W.H.; Lin, S.J.; Tsai, M.J.; Ma, H.; Hsieh, S.L.; Cheng, H. The Immunomodulator Decoy Receptor 3 Improves Locomotor Functional Recovery After Spinal Cord Injury. J. Neuroinflamm. 2016, 13, 154. [Google Scholar] [CrossRef]
- van der Poll, T.; van de Veerdonk, F.L.; Scicluna, B.P.; Netea, M.G. The Immunopathology of Sepsis and Potential Therapeutic Targets. Nat. Rev. Immunol. 2017, 17, 407–420. [Google Scholar] [CrossRef]
- Liu, A.C.; Patel, K.; Vunikili, R.D.; Johnson, K.W.; Abdu, F.; Belman, S.K.; Glicksberg, B.S.; Tandale, P.; Fontanez, R.; Mathew, O.K.; et al. Sepsis in the Era of Data-Driven Medicine: Personalizing Risks, Diagnoses, Treatments and Prognoses. Brief. Bioinform. 2020, 21, 1182–1195. [Google Scholar] [CrossRef]
- Karampela, I.; Fragkou, P.C. Future Perspectives in the Diagnosis and Treatment of Sepsis and Septic Shock. Medicina 2022, 58, 844. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Function | Markers |
|---|---|
| Acute phase reactive protein | PCT; CRP |
| Cytokines and chemokines | IL-6; IL-10 |
| Cell surface and soluble receptors | HLA-DR; CD64 |
| Vascular endothelium-related | cell adhesion molecules; angiopoietin |
| Coagulation-related | antithrombin III |
| Neurotransmitter-related | butyrylcholinesterase |
| Hormone-related | presepsin; pro-adrenomedullin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, J.; Tong, Z.; Wu, S.; Zhou, F.; Chen, Q. Research Progress of DcR3 in the Diagnosis and Treatment of Sepsis. Int. J. Mol. Sci. 2023, 24, 12916. https://doi.org/10.3390/ijms241612916
Su J, Tong Z, Wu S, Zhou F, Chen Q. Research Progress of DcR3 in the Diagnosis and Treatment of Sepsis. International Journal of Molecular Sciences. 2023; 24(16):12916. https://doi.org/10.3390/ijms241612916
Chicago/Turabian StyleSu, Jingqian, Zhiyong Tong, Shun Wu, Fen Zhou, and Qi Chen. 2023. "Research Progress of DcR3 in the Diagnosis and Treatment of Sepsis" International Journal of Molecular Sciences 24, no. 16: 12916. https://doi.org/10.3390/ijms241612916
APA StyleSu, J., Tong, Z., Wu, S., Zhou, F., & Chen, Q. (2023). Research Progress of DcR3 in the Diagnosis and Treatment of Sepsis. International Journal of Molecular Sciences, 24(16), 12916. https://doi.org/10.3390/ijms241612916