
Simultaneous Assessment of mTORC1, JAK/STAT, and NLRP3 Inflammasome Activation Pathways in Patients with Sarcoidosis

 , ,
, ,
Abstract
1. Introduction
2. Results
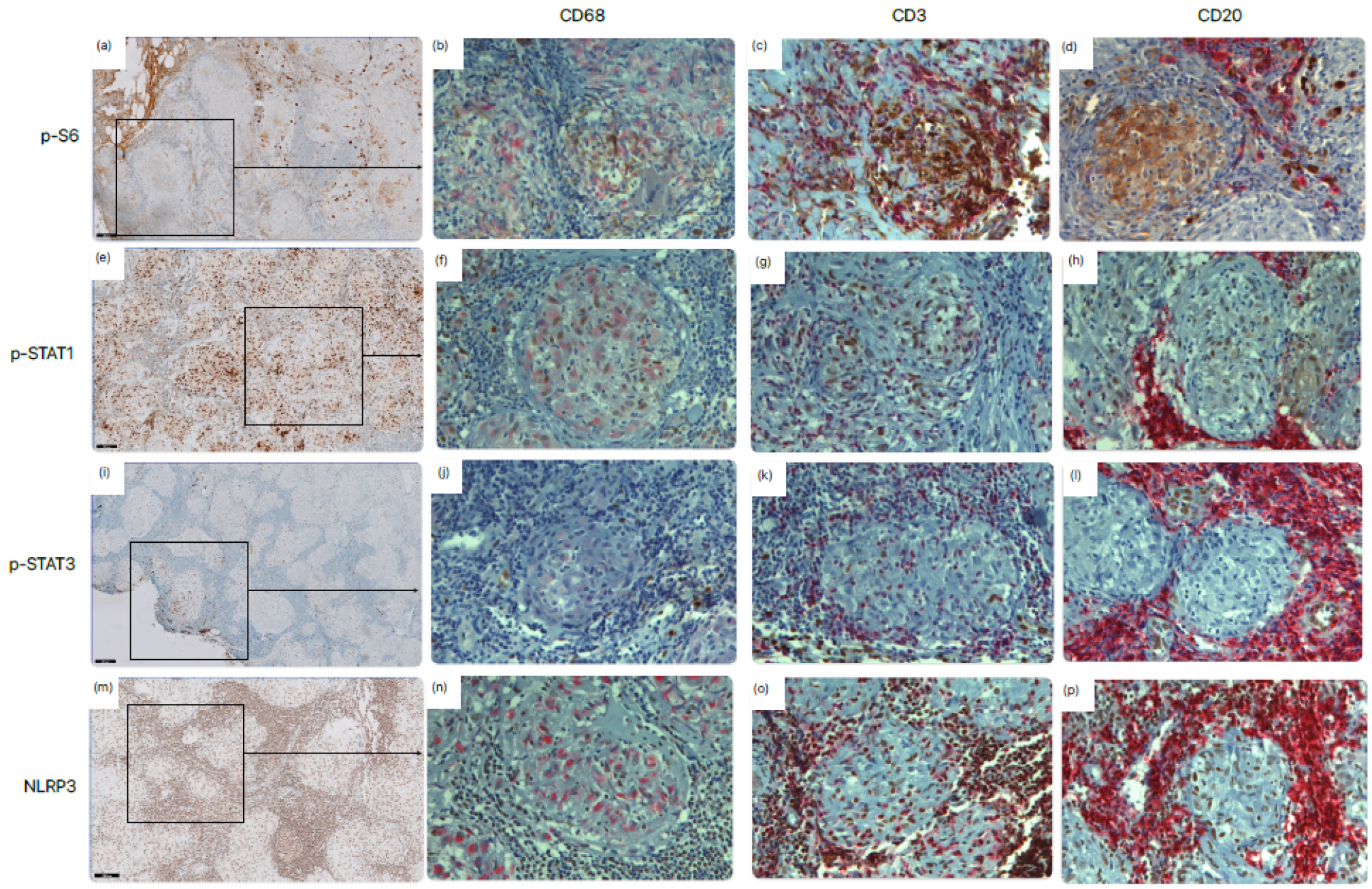
2.1. Expression in Granulomatous Tissue
2.1.1. Immunohistochemical Scoring
2.1.2. Co-Occurrence of Signaling Pathways
2.2. Potential Biomarker for Progressive Disease
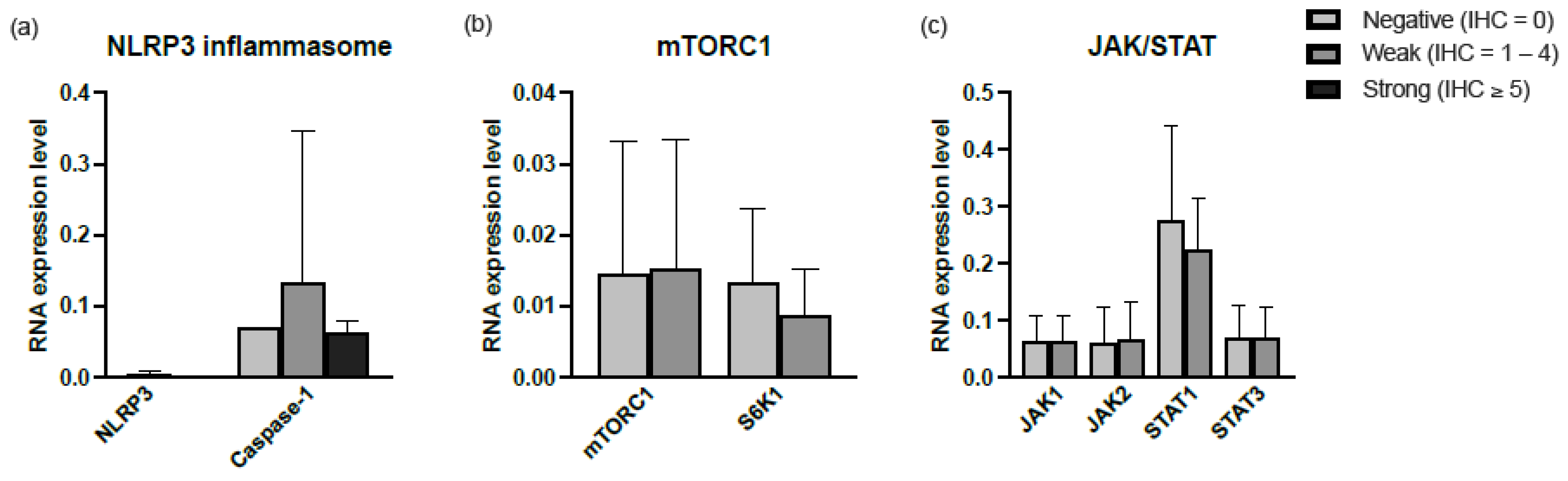
2.3. Activity of Signaling Pathways in Broncho Alveolar Lavage Fluid (BALF)
Correlation of Expression in BALF and Tissue
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. Immunohistochemistry
4.3. Evaluation of Immunohistochemistry
4.4. Clinical Characteristics
4.5. RNA Isolation and Quantitative Real-Time PCR (qPCR)
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costabel, U.; Hunninghake, G.W. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association for Sarcoidosis and Other Granulomatous Disorders. Eur. Respir. J. 1999, 14, 735–737. [Google Scholar] [CrossRef]
- Broos, C.E.; Koth, L.L.; Van Nimwegen, M.; In’T Veen, J.C.C.M.; Paulissen, S.M.J.; Van Hamburg, J.P.; Annema, J.T.; Heller-Baan, R.; Kleinjan, A.; Hoogsteden, H.C.; et al. Increased T-helper 17.1 cells in sarcoidosis mediastinal lymph nodes. Eur. Respir. J. 2018, 51, 1701124. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Casanova, N.; Pouladi, N.; Wang, T.; Lussier, Y.; Knox, K.S.; Garcia, J.G.N.N. Identification of Jak-STAT signaling involvement in sarcoidosis severity via a novel microRNA-regulated peripheral blood mononuclear cell gene signature. Sci. Rep. 2017, 7, 4237. [Google Scholar] [CrossRef] [PubMed]
- Gerke, A.K. Treatment of Sarcoidosis: A Multidisciplinary Approach. Front. Immunol. 2020, 11, 545413. [Google Scholar] [CrossRef] [PubMed]
- Riteau, N.; Bernaudin, J.F. In addition to mTOR and JAK/STAT, NLRP3 inflammasome is another key pathway activated in sarcoidosis. Eur. Respir. J. 2020, 55, 2000149. [Google Scholar] [CrossRef]
- Linke, M.; Pham, H.T.T.; Katholnig, K.; Schnöller, T.; Miller, A.; Demel, F.; Schütz, B.; Rosner, M.; Kovacic, B.; Sukhbaatar, N.; et al. Chronic signaling via the metabolic checkpoint kinase mTORC1 induces macrophage granuloma formation and marks sarcoidosis progression. Nat. Immunol. 2017, 18, 293–302. [Google Scholar] [CrossRef]
- Kraaijvanger, R.; Seldenrijk, K.; Beijer, E.; Damen, J.; Wilson, J.L.; Weichhart, T.; Grutters, J.C.; Veltkamp, M. Activation of downstream mTORC1 target ribosomal protein S6 kinase (S6K) can be found in a subgroup of Dutch patients with granulomatous pulmonary disease. Cells 2021, 10, 3545. [Google Scholar] [CrossRef]
- Gupta, N.; Bleesing, J.H.; McCormack, F.X. Successful response to treatment with sirolimus in pulmonary sarcoidosis. Am. J. Respir. Crit. Care Med. 2020, 202, E119–E120. [Google Scholar] [CrossRef]
- Damsky, W.; Thakral, D.; Emeagwali, N.; Galan, A.; King, B. Tofacitinib treatment and molecular analysis of cutaneous sarcoidosis. N. Engl. J. Med. 2018, 379, 2540–2546. [Google Scholar] [CrossRef]
- Zhou, E.R.; Arce, S. Key players and biomarkers of the adaptive immune system in the pathogenesis of sarcoidosis. Int. J. Mol. Sci. 2020, 21, 7398. [Google Scholar] [CrossRef]
- Damsky, W.; Wang, A.; Kim, D.J.; Young, B.D.; Singh, K.; Murphy, M.J.; Daccache, J.; Clark, A.; Ayasun, R.; Ryu, C.; et al. Inhibition of type 1 immunity with tofacitinib is associated with marked improvement in longstanding sarcoidosis. Nat. Commun. 2022, 13, 3140. [Google Scholar] [CrossRef] [PubMed]
- Kerkemeyer, K.L.; Meah, N.; Sinclair, R.D. Tofacitinib for cutaneous and pulmonary sarcoidosis: A case series. J. Am. Acad. Dermatol. 2021, 84, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.A.; Le, B.; Stevens, J.; Desmarais, J.; Seifer, D.; Ogle, K.; Choi, D.; Harrington, C.A.; Jackson, P.; Rosenbaum, J.T. Tofacitinib as a Steroid-Sparing Therapy in Pulmonary Sarcoidosis, an Open-Label Prospective Proof-of-Concept Study. Lung 2021, 199, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Huppertz, C.; Jäger, B.; Wieczorek, G.; Engelhard, P.; Oliver, S.J.; Bauernfeind, F.G.; Littlewood-Evans, A.; Welte, T.; Hornung, V.; Prasse, A. The NLRP3 inflammasome pathway is activated in sarcoidosis and involved in granuloma formation. Eur. Respir. J. 2020, 55, 1900119. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Costabel, U.; Dai, H. The Role of Diverse Immune Cells in Sarcoidosis. Front. Immunol. 2021, 12, 788502. [Google Scholar] [CrossRef]
- Wu, B.; Sodji, Q.H.; Oyelere, A.K. Inflammation, Fibrosis and Cancer: Mechanisms, Therapeutic Options and Challenges. Cancers 2022, 14, 552. [Google Scholar] [CrossRef]
- Li, X.; Jiang, M.; Chen, X.; Sun, W. Etanercept alleviates psoriasis by reducing the Th17/Treg ratio and promoting M2 polarization of macrophages. Immun. Inflamm. Dis. 2022, 10, e734. [Google Scholar] [CrossRef]
- Xia, T.; Zhang, M.; Lei, W.; Yang, R.; Fu, S.; Fan, Z.; Yang, Y.; Zhang, T. Advances in the role of STAT3 in macrophage polarization. Front. Immunol. 2023, 14, 1160719. [Google Scholar] [CrossRef]
- Artlett, C.M.; Sassi-Gaha, S.; Rieger, J.L.; Boesteanu, A.C.; Feghali-Bostwick, C.A.; Katsikis, P.D. The Inflammasome Activating Caspase 1 Mediates Fibrosis and Myofibroblast Differentiation in Systemic Sclerosis. ARTHRITIS Rheum. 2011, 63, 3563–3574. [Google Scholar] [CrossRef]
- Lasithiotaki, I.; Giannarakis, I.; Tsitoura, E.; Samara, K.D.; Margaritopoulos, G.A.; Choulaki, C.; Vasarmidi, E.; Tzanakis, N.; Voloudaki, A.; Sidiropoulos, P.; et al. NLRP3 inflammasome expression in idiopathic pulmonary fibrosis and rheumatoid lung. Eur. Respir. J. 2016, 47, 910–918. [Google Scholar] [CrossRef]
- Prasse, A.; Artysh, N.; Culver, D.A.; Young, P.R.; Jäger, B. High MTOR Activity in Bronchoalveolar Lavage Cells From Patients with Sarcoidosis. Am. J. Respir. Crit. Care Med. 2023, 207, A4815. Available online: www.atsjournals.org (accessed on 11 July 2023).
- Roux, P.P.; Shahbazian, D.; Vu, H.; Holz, M.K.; Cohen, M.S.; Taunton, J.; Sonenberg, N.; Blenis, J. RAS/ERK Signaling Promotes Site-specific Ribosomal Protein S6 Phosphorylation via RSK and Stimulates Cap-dependent Translation. J. Biol. Chem. 2011, 18, 1492–1501. [Google Scholar]
- Pende, M.; Um, S.H.; Mieulet, V.; Sticker, M.; Goss, V.L.; Mestan, J.; Mueller, M.; Fumagalli, S.; Kozma, S.C.; Thomas, G. S6K1 −/−/S6K2 −/− Mice Exhibit Perinatal Lethality and Rapamycin-Sensitive 5′-Terminal Oligopyrimidine mRNA Translation and Reveal a Mitogen-Activated Protein Kinase-Dependent S6 Kinase Pathway. Mol. Cell Biol. 2004, 24, 3112–3124. [Google Scholar] [CrossRef] [PubMed]
- Canto, E.; Isobe, N.; Didonna, A.; Hauser, S.L.; Oksenberg, J.R.; Baranzini, S.; Bevan, C.; Bove, R.; Crabtree-Hartman, E.; Gelfand, J.M.; et al. Aberrant STAT phosphorylation signaling in peripheral blood mononuclear cells from multiple sclerosis patients. J. Neuroinflammation 2018, 15, 72. [Google Scholar] [CrossRef]
- Beijer, E.; Seldenrijk, K.; Meek, B.; Damen, J.; Quanjel, M.J.R.; Grutters, J.C.; Veltkamp, M. Detection of C. acnes in granulomas of patients with either hypersensitivity pneumonitis or vasculitis reveals that its presence is not unique for sarcoidosis. ERJ Open Res. 2021, 7, 00930–02020. [Google Scholar] [CrossRef]
- Gulhati, P.; Cai, Q.; Li, J.; Liu, J.; Rychahou, P.G.; Qiu, S.; Lee, E.Y.; Silva, S.R.; Bowen, K.A.; Gao, T.; et al. Targeted inhibition of mammalian target of rapamycin signaling inhibits tumorigenesis of colorectal cancer. Clin. Cancer Res. 2009, 15, 7207–7216. [Google Scholar] [CrossRef]
- Baughman, R.P.; Nagai, S.; Balter, M.; Costabel, U.; Drent, M.; Du Bois, R.; Grutters, J.C.; Judson, M.A.; Lambin, I.; Lower, E.E.; et al. Defining the clinical outcome status (COS) in sarcoidosis: Results of WASOG Task Force. Sarcoidosis Vasc. Diffus. Lung Dis. 2011, 28, 56–64. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2-ΔΔCT method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Treeck, O.; Wackwitz, B.; Haus, U.; Ortmann, O. Effects of a combined treatment with mTOR inhibitor RAD001 and tamoxifen in vitro on growth and apoptosis of human cancer cells. Gynecol. Oncol. 2006, 102, 292–299. [Google Scholar] [CrossRef]
- Berman, A.Y.; Manna, S.; Schwartz, N.S.; Katz, Y.E.; Sun, Y.; Behrmann, C.A.; Yu, J.J.; Plas, D.R.; Alayev, A.; Holz, M.K. ERRα regulates the growth of triple-negative breast cancer cells via S6K1-dependent mechanism. Signal Transduct. Target. Ther. 2017, 2, 17035. [Google Scholar] [CrossRef]
- Lee, K.-Y.; Lee, Y.-L.; Chiang, M.-H.; Wang, H.-Y.; Chen, C.-Y.; Lin, C.-H.; Chen, Y.-C.; Fan, C.-K.; Cheng, P.-C. Schistosoma egg antigens suppress LPS-induced inflammation in human IMR-90 cells by modulation of JAK/STAT1 signaling. Immunol. Infect. 2021, 54, 501–513. [Google Scholar] [CrossRef]
- Najafi, S.; Saadat, P.; Beladi Moghadam, N.; Manoucherinia, A.; Aghazadeh, Z.; Vali Mohammadi, A.; Noorbakhsh, S.M.; Movahedi, M.; Nikouei Moghaddam, M.R.; Pashaiefar, H.; et al. The Effects of Mannuronic Acid on IL-1β, IL-17A, STAT1, and STAT3 Gene Expressions and TLR2 and TLR4 Molecules in Multiple Sclerosis. J. Clin. Pharmacol. 2022, 62, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Ganji, P.N.; Park, W.; Wen, J.; Mahaseth, H.; Landry, J.; Farris, A.B.; Willingham, F.; Sullivan, P.S.; Proia, D.A.; El-Hariry, I.; et al. Antiangiogenic effects of ganetespib in colorectal cancer mediated through inhibition of HIF-1α and STAT-3. Angiogenesis 2013, 16, 903–917. [Google Scholar] [CrossRef]
- Shi, X.; Xie, W.L.; Kong, W.W.; Chen, D.; Qu, P. Expression of the NLRP3 Inflammasome in Carotid Atherosclerosis. J. Stroke Cerebrovasc. Dis. 2015, 24, 2455–2466. [Google Scholar] [CrossRef] [PubMed]
- Ran, S.; Liu, B.; Gu, S.; Sun, Z.; Liang, J. Analysis of the expression of NLRP3 and AIM2 in periapical lesions with apical periodontitis and microbial analysis outside the apical segment of teeth. Arch. Oral. Biol. 2017, 78, 39–47. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IHC Score | p-S6 n (%) | p-STAT1 | p-STAT3 | NLRP3 |
|---|---|---|---|---|
| 0 | 29 (49.2) | 30 (50.0) | 44 (73.3) | 9 (15.0) |
| 1 | 13 (22.0) | 13 (21.7) | 9 (15.0) | 4 (6.7) |
| 2 | 7 (11.9) | 5 (8.3) | 5 (8.3) | 4 (6.7) |
| 3 | 6 (10.2) | 2 (3.3) | 0 (0.0) | 6 (10.0) |
| 4 | 4 (6.8) | 3 (5.0) | 2 (3.3) | 5 (8.3) |
| 5 | 0 (0) | 3 (5.0) | 0 (0.0) | 2 (3.3) |
| 6 | 0 (0) | 1 (1.7) | 0 (0.0) | 14 (23.3) |
| 7 | 0 (0) | 3 (5.0) | 0 (0.0) | 16 (26.7) |
| Gene | Forward | Reverse |
|---|---|---|
| mTORC1 [29] | 5′GGAGGCTGATGGACACAAAT 3′ | 5′CTGTGGTCCCCGTTTTCTTA 3′ |
| S6K1 [30] | 5′CTCTGAGGATGAGCTGGAGG3′ | 5′TTCTCACAATGTTCCATGCC3′ |
| JAK1 * | 5′CACAGGCATGCCGTATCTCT 3′ | 5′CCAGAGCTTGGTGTTCTCGT 3′ |
| JAK2 [31] | 5′GATGGATGCCCAGATGAGAT 3′ | 5′TTGATCCACTCGAAGAGCTAGA 3′ |
| STAT1 [32] | 5′ACCTAACGTGCTGTGCGTAG3′ | 5′GAGACATCCTGCCACCTTGT3′ |
| STAT3 [33] | 5′GCTTCCTGCAAGAGTCGAAT3′ | 5′ATTGGCTTCTCAA GATACCTG3′ |
| NLRP3 [34] | 5′ AAGCCAAGAATCCACAGTGTAAC 3′ | 5′TTGCCTCGCAGGTAAAGGT 3′ |
| Caspase-1 [35] | 5′CCTTAATATGCAAGACTCTCAAGGA3′ | 5′TAAGCTGGGTTGTCCTGCACT3′ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraaijvanger, R.; Ambarus, C.A.; Damen, J.; van der Vis, J.J.; Kazemier, K.M.; Grutters, J.C.; van Moorsel, C.H.M.; Veltkamp, M. Simultaneous Assessment of mTORC1, JAK/STAT, and NLRP3 Inflammasome Activation Pathways in Patients with Sarcoidosis. Int. J. Mol. Sci. 2023, 24, 12792. https://doi.org/10.3390/ijms241612792
Kraaijvanger R, Ambarus CA, Damen J, van der Vis JJ, Kazemier KM, Grutters JC, van Moorsel CHM, Veltkamp M. Simultaneous Assessment of mTORC1, JAK/STAT, and NLRP3 Inflammasome Activation Pathways in Patients with Sarcoidosis. International Journal of Molecular Sciences. 2023; 24(16):12792. https://doi.org/10.3390/ijms241612792
Chicago/Turabian StyleKraaijvanger, Raisa, Carmen A. Ambarus, Jan Damen, Joanne J. van der Vis, Karin M. Kazemier, Jan C. Grutters, Coline H. M. van Moorsel, and Marcel Veltkamp. 2023. "Simultaneous Assessment of mTORC1, JAK/STAT, and NLRP3 Inflammasome Activation Pathways in Patients with Sarcoidosis" International Journal of Molecular Sciences 24, no. 16: 12792. https://doi.org/10.3390/ijms241612792
APA StyleKraaijvanger, R., Ambarus, C. A., Damen, J., van der Vis, J. J., Kazemier, K. M., Grutters, J. C., van Moorsel, C. H. M., & Veltkamp, M. (2023). Simultaneous Assessment of mTORC1, JAK/STAT, and NLRP3 Inflammasome Activation Pathways in Patients with Sarcoidosis. International Journal of Molecular Sciences, 24(16), 12792. https://doi.org/10.3390/ijms241612792