


Monocytes in the Characterization of Pain in Palliative Patients with Severe Dementia—A Pilot Study

 , , , , , , and
, , , , , , and
Abstract
1. Introduction and Objectives
2. Results
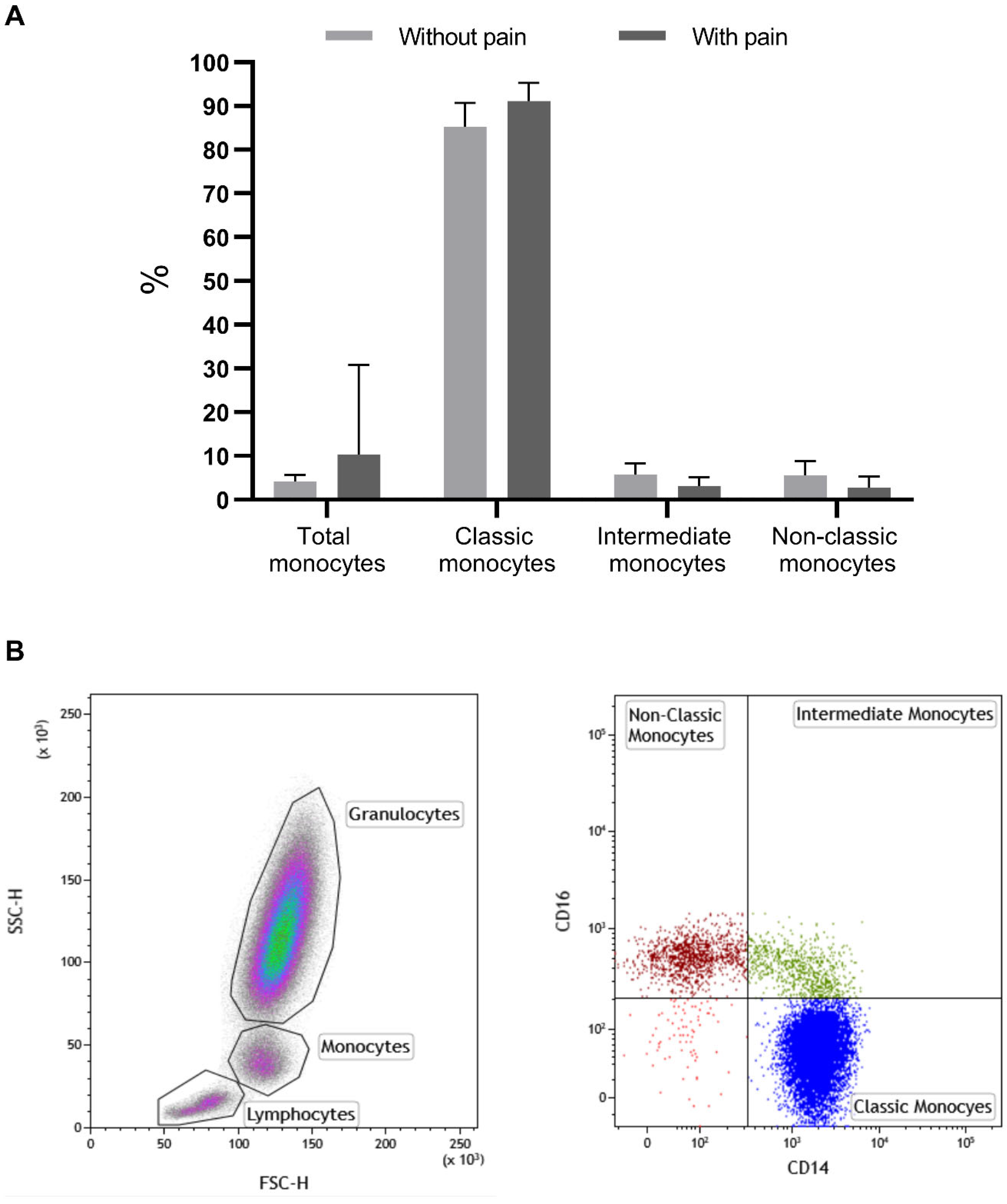
2.1. Monocyte Characterization in Patients with and without Chronic Pain
2.2. Monocytes and Gender
2.3. Type of Pain and Monocyte Biomarkers
2.4. Analgesic Drugs and Monocyte Biomarkers
2.5. Monocyte Characterization and Dementia
2.6. Monocyte Characterization and Opioids and Other Analgesics Used to Control Pain in These Patients
3. Material and Methods
3.1. Evaluation of Monocytes Subsets by Flow Cytometry
3.2. Evaluation of Monocyte Subsets and Membrane Proteins Using Flow Cytometry
3.3. Statistical Analysis
3.4. Inclusion Criteria
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orr, P.M.; Shank, B.C.; Black, A.C. The Role of Pain Classification Systems in Pain Management. Crit. Care Nurs. Clin. North Am. 2017, 29, 407–418. [Google Scholar] [CrossRef]
- World Health Organization. WHO’s Pain Relief Ladder; World Health Organization: Geneva, Switzerland, 2009.
- Ali, A.; Arif, A.W.; Bhan, C.; Kumar, D.; Malik, M.B.; Sayyed, Z.; Akhtar, K.H.; Ahmad, M.Q. Managing Chronic Pain in the Elderly: An Overview of the Recent Therapeutic Advancements. Cureus 2018, 10, e3293. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.; Moutinho, R.; Dourado, M. Particularidades da Avaliação e Tratamento da dor no Idoso: Contributo para a Validação da Pain Quality Assessment Scale© e Abordagem Terapêutica na População Idosa; Universidade de Coimbra: Coimbra, Portugal, 2017. [Google Scholar]
- World Health Organization. Normative Guidelines on Pain Management; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Dong, X.; Nao, J.; Shi, J.; Zheng, D. Predictive Value of Routine Peripheral Blood Biomarkers in Alzheimer’s Disease. Front. Aging Neurosci. 2019, 11, 332. [Google Scholar] [CrossRef]
- Varesi, A.; Carrara, A.; Pires, V.G.; Floris, V.; Pierella, E.; Savioli, G.; Prasad, S.; Esposito, C.; Ricevuti, G.; Chirumbolo, S.; et al. Blood-Based Biomarkers for Alzheimer’s Disease Diagnosis and Progression: An Overview. Cells 2022, 11, 1367. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.; Alves, R.; Jorge, J.; Gonçalves, A.C.; Sarmento-Ribeiro, A.B.; Teixeira-Veríssimo, M.; Dourado, M.; Andrade, J.P. Platelet Membrane Proteins as Pain Biomarkers in Patients with Severe Dementia. Biomedicines 2023, 11, 380. [Google Scholar] [CrossRef] [PubMed]
- Charach, G.; Rogowski, O.; Karniel, E.; Charach, L.; Grosskopf, I.; Novikov, I. Monocytes may be favorable biomarker and predictor of long-term outcome in patients with chronic heart failure. Medicine 2019, 98, e17108. [Google Scholar] [CrossRef]
- Marimuthu, R.; Francis, H.; Dervish, S.; Li, S.C.H.; Medbury, H.; Williams, H. Characterization of Human Monocyte Subsets by Whole Blood Flow Cytometry Analysis. J. Vis. Exp. 2018, 140, 57941. [Google Scholar] [CrossRef]
- Kapellos, T.S.; Bonaguro, L.; Gemünd, I.; Reusch, N.; Saglam, A.; Hinkley, E.R.; Schultze, J.L. Human Monocyte Subsets and Phenotypes in Major Chronic Inflammatory Diseases. Front. Immunol. 2019, 10, 2035. [Google Scholar] [CrossRef]
- Oggero, S.; Cecconello, C.; Silva, R.; Zeboudj, L.; Sideris-Lampretsas, G.; Perretti, M.; Malcangio, M. Dorsal root ganglia CX3CR1 expressing monocytes/macrophages contribute to arthritis pain. Brain Behav. Immun. 2022, 106, 289–306. [Google Scholar] [CrossRef]
- Ritz, B.W.; Alexander, G.M.; Nogusa, S.; Perreault, M.J.; Peterlin, B.L.; Grothusen, J.R.; Schwartzman, R.J. Elevated blood levels of inflammatory monocytes (CD14+CD16+) in patients with complex regional pain syndrome. Clin. Exp. Immunol. 2011, 164, 108–117. [Google Scholar] [CrossRef]
- Tippett, E.; Cheng, W.-J.; Westhorpe, C.; Cameron, P.U.; Brew, B.J.; Lewin, S.R.; Jaworowski, A.; Crowe, S.M. Differential Expression of CD163 on Monocyte Subsets in Healthy and HIV-1 Infected Individuals. PLoS ONE 2011, 6, e19968. [Google Scholar] [CrossRef]
- Goehler, L.E.; Fischer-White, T.G.; Adelstein, K.E.; Murugesan, M.; Denomme, J.; Mensah, S.; Scott, M.; Gaykema, R.P.; Lewis, J.E.; Anderson, J.G.; et al. 18. Stress, pain and monocytes in fibromyalgia. Brain Behav. Immun. 2016, 40, e6. [Google Scholar] [CrossRef]
- Ożańska, A.; Szymczak, D.; Rybka, J. Pattern of human monocyte subpopulations in health and disease. Scand. J. Immunol. 2020, 92, e12883. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.G.; Fischer-White, T.G.; Anderson, J.G.; Adelstein, K.E.; Murugesan, M.; Lewis, J.E.; Scott, M.M.; Gaykema, R.P.A.; Goehler, L.E. Stress, Inflammation and Pain: A Potential Role for Monocytes in Fibromyalgia-related Symptom Severity. Stress Health 2016, 32, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Auffray, C.; Sieweke, M.H.; Geissmann, F. Blood Monocytes: Development, Heterogeneity, and Relationship with Dendritic Cells. Annu. Rev. Immunol. 2009, 27, 669–692. [Google Scholar] [CrossRef]
- Espinoza, V.; Emmady, P. Histology, Monocytes. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: Https://Www.Ncbi.Nlm.Nih.Gov/Books/NBK557618/ (accessed on 28 April 2022).
- Moura, D.F.d. Participação do CD163 na via Anti-Inflamatória do Polo Lepromatoso da Hanseníase. Rio de Janeiro. Master’s Thesis, Instituto Oswaldo Cruz, Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Santoni, G.; Cardinali, C.; Morelli, M.; Santoni, M.; Nabissi, M.; Amantini, C. Danger- and pathogen-associated molecular patterns recognition by pattern-recognition receptors and ion channels of the transient receptor potential family triggers the inflammasome activation in immune cells and sensory neurons. J. Neuroinflammation 2015, 12, 21. [Google Scholar] [CrossRef]
- Warden, V.; Hurley, A.C.; Volicer, L. Development and Psychometric Evaluation of the Pain Assessment in Advanced Dementia (PAINAD) Scale. J. Am. Med. Dir. Assoc. 2003, 4, 9–15. [Google Scholar] [CrossRef]
- Microsoft Corporation. Microsoft Excel. Available online: https://office.microsoft.com/excel (accessed on 1 January 2022).
- Wu, J.; Wu, H.; An, J.; Ballantyne, C.M.; Cyster, J.G. Critical role of integrin CD11c in splenic dendritic cell capture of missing-self CD47 cells to induce adaptive immunity. Proc. Natl. Acad. Sci. USA 2018, 115, 6786–6791. [Google Scholar] [CrossRef]
- Sansom, D.M.; Manzotti, C.N.; Zheng, Y. What’s the difference between CD80 and CD86? Trends Immunol. 2003, 24, 313–318. [Google Scholar] [CrossRef]
- Kowal, K.; Silver, R.; Sławińska, E.; Bielecki, M.; Chyczewski, L.; Kowal-Bielecka, O. CD163 and its role in inflammation. Folia Histochem. Cytobiol. 2011, 49, 365–374. [Google Scholar] [CrossRef]
- Tsuchiya, K.; Suzuki, Y.; Yoshimura, K.; Yasui, H.; Karayama, M.; Hozumi, H.; Furuhashi, K.; Enomoto, N.; Fujisawa, T.; Nakamura, Y.; et al. Macrophage Mannose Receptor CD206 Predicts Prognosis in Community-acquired Pneumonia. Sci. Rep. 2019, 9, 18750. [Google Scholar] [CrossRef]
- Michels, W.M.; Grootendorst, D.C.; Verduijn, M.; Elliott, E.G.; Dekker, F.W.; Krediet, R.T. Performance of the Cockcroft-Gault, MDRD, and New CKD-EPI Formulas in Relation to GFR, Age, and Body Size. Clin. J. Am. Soc. Nephrol. 2010, 5, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Laliberte, L.; Morris, J.N.; Wiemann, M. The Karnofsky performance status scale: An examination of its reliability and validity in a research setting. Cancer 1984, 53, 2002–2007. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Isik, A.T.; Arik, F.; Kalan, U.; Eyvaz, A.; Veronese, N. Validity of the Mini-Nutritional Assessment Scale for Evaluating Frailty Status in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sarıcam, G. Relationship between migraine headache and hematological parameters. Acta Neurol. Belg. 2021, 121, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Ablin, J.; Fitzcharles, M.-A.; Buskila, D.; Shir, Y.; Sommer, C.; Häuser, W. Treatment of Fibromyalgia Syndrome: Recommendations of Recent Evidence-Based Interdisciplinary Guidelines with Special Emphasis on Complementary and Alternative Therapies. Evid. Complement. Altern. Med. 2013, 2013, 485272. [Google Scholar] [CrossRef]
- Forsythe, L.P.; Romano, J.M.; Jensen, M.P.; Thorn, B.E. Attachment style is associated with perceived spouse responses and pain-related outcomes. Rehabil. Psychol. 2012, 57, 290–300. [Google Scholar] [CrossRef]
- Marchi, A.; Vellucci, R.; Mameli, S.; Rita Piredda, A.; Finco, G. Pain Biomarkers. Clin. Drug Investig. 2009, 29 (Suppl. S1), 41–46. [Google Scholar] [CrossRef]
- Loukov, D.; Karampatos, S.; Maly, M.R.; Bowdish, D.M.E. Monocyte activation is elevated in women with knee-osteoarthritis and associated with inflammation, BMI and pain. Osteoarthr. Cartil. 2018, 26, 255–263. [Google Scholar] [CrossRef]
- Wong, K.L.; Tai, J.J.-Y.; Wong, W.-C.; Han, H.; Sem, X.; Yeap, W.-H.; Kourilsky, P.; Wong, S.-C. Gene expression profiling reveals the defining features of the classical, intermediate, and nonclassical human monocyte subsets. Blood 2011, 118, e16–e31. [Google Scholar] [CrossRef]
- Peng, J.; Gu, N.; Zhou, L.B.; Eyo, U.; Murugan, M.; Gan, W.-B.; Wu, L.-J. Microglia and monocytes synergistically promote the transition from acute to chronic pain after nerve injury. Nat. Commun. 2016, 7, 12029. [Google Scholar] [CrossRef] [PubMed]
- Boland, J.; Foulds, G.; Ahmedzai, S.; Pockley, G. Effect of opioids on the phagocytosis of neutrophils and monocytes: A systematic in vitro analysis. BMJ Support. Palliat. Care 2012, 2 (Suppl. S1), A3. [Google Scholar] [CrossRef]
- Wen, S.; Jiang, Y.; Liang, S.; Cheng, Z.; Zhu, X.; Guo, Q. Opioids Regulate the Immune System: Focusing on Macrophages and Their Organelles. Front. Pharmacol. Sec. Pharmacol. Anti Cancer Drugs 2022, 12, 814241. [Google Scholar] [CrossRef] [PubMed]
- Craig, D.G.; Lee, P.; Pryde, E.A.; Hayes, P.C.; Simpson, K.J. Serum neopterin and soluble CD163 as markers of macrophage activation in paracetamol (acetaminophen)-induced human acute liver injury. Aliment. Pharmacol. Ther. 2013, 38, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- Siggaard, C.B.; Kazankov, K.; Rødgaard-Hansen, S.; Møller, H.J.; Donnelly, M.C.; Simpson, K.J.; Grønbaek, H. Macrophage markers soluble CD163 and soluble mannose receptor are associated with liver injury in patients with paracetamol overdose. Scand. J. Gastroenterol. 2019, 54, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ye, Y.; Wang, F.; Zhu, J.; Zhao, Q.; Zheng, Y.; Gu, Y.; Xie, C.; Huang, Z.; Tai, Q.; et al. Liver myofibroblasts up-regulate monocyte CD163 expression via PGE2 during hepatitis B induced liver failure. J. Transl. Med. 2014, 12, 60. [Google Scholar] [CrossRef]
- Busse, S.; Hoffmann, J.; Michler, E.; Hartig, R.; Frodl, T.; Busse, M. Dementia-associated changes of immune cell composition within the cerebrospinal fluid. Brain Behav. Immun. Health 2021, 14, 100218. [Google Scholar] [CrossRef]
- Chen, S.-H.; Tian, D.-Y.; Shen, Y.-Y.; Cheng, Y.; Fan, D.-Y.; Sun, H.-L.; He, C.-Y.; Sun, P.-Y.; Bu, X.-L.; Zeng, F.; et al. Amyloid-beta uptake by blood monocytes is reduced with ageing and Alzheimer’s disease. Transl. Psychiatry 2020, 10, 423. [Google Scholar] [CrossRef] [PubMed]
- Munawara, U.; Catanzaro, M.; Xu, W.; Tan, C.; Hirokawa, K.; Bosco, N.; Dumoulin, D.; Khalil, A.; Larbi, A.; Lévesque, S.; et al. Hyperactivation of monocytes and macrophages in MCI patients contributes to the progression of Alzheimer’s disease. Immun. Ageing 2021, 18, 29. [Google Scholar] [CrossRef]
- Guo, S.; Wang, H.; Yin, Y. Microglia Polarization from M1 to M2 in Neurodegenerative Diseases. Front. Aging Neurosci. 2022, 14, 815347. [Google Scholar] [CrossRef]
- Holder, G.E.; McGary, C.M.; Johnson, E.M.; Zheng, R.; John, V.T.; Sugimoto, C.; Kuroda, M.J.; Kim, W.-K. Expression of the Mannose Receptor CD206 in HIV and SIV Encephalitis: A Phenotypic Switch of Brain Perivascular Macrophages with Virus Infection. J. Neuroimmune Pharmacol. 2014, 9, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.K.; Ferreira, S.A.; Nielsen, M.C.; Schulte, C.; Shrivastava, K.; Hennig, D.; Etzerodt, A.; Graversen, J.H.; Berg, D.; Maetzler, W.; et al. Soluble CD163 Changes Indicate Monocyte Association with Cognitive Deficits in Parkinson’s Disease. Mov. Disord. 2021, 36, 963–976. [Google Scholar] [CrossRef] [PubMed]
- Pey, P.; Pearce, R.K.; Kalaitzakis, M.E.; Griffin, W.S.T.; Gentleman, S.M. Phenotypic profile of alternative activation marker CD163 is different in Alzheimer’s and Parkinson’s disease. Acta Neuropathol. Commun. 2014, 2, 21. [Google Scholar] [CrossRef]
- Roberts, E.S.; Masliah, E.; Fox, H.S. CD163 Identifies a Unique Population of Ramified Microglia in HIV Encephalitis (HIVE). J. Neuropathol. Exp. Neurol. 2004, 63, 1255–1264. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, X.; Ma, J.; Liu, Z.; Qi, Y.; Fang, L.; Zheng, Y.; Cai, Z. Circulating Soluble CD163: A Potential Predictor for the Functional Outcome of Acute Ischemic Stroke. Front. Neurol. 2021, 12, 740420. [Google Scholar] [CrossRef]
- Leng, F.; Edison, P. Neuroinflammation and microglial activation in Alzheimer disease: Where do we go from here? Nat. Rev. Neurol. 2021, 17, 157–172. [Google Scholar] [CrossRef]
- Tian, Z.; Ji, X.; Liu, J. Neuroinflammation in Vascular Cognitive Impairment and Dementia: Current Evidence, Advances, and Prospects. Int. J. Mol. Sci. 2022, 23, 6224. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total of Patients: (n = 53) | Patients with Pain and Dementia (n = 38) | Patients with Pain without Dementia (n = 6) | Patients without Pain and without Dementia (Controls) (n = 9) | |
|---|---|---|---|---|
| Gender | Male | 29% (n = 11) | 50% (n = 3) | 0 |
| Female | 71% (n = 27) | 50% (n = 3) | 100% | |
| Average age (years) | 84.1 | 62.5 | 44.7 | |
| PAINAD scale | <5 | 15.8% (n = 6) | NA | NA * |
| 5–7 | 73.7% (n = 28) | NA | NA | |
| 8–10 | 10.5% (n = 4) | NA | NA | |
| Average numeric pain scale | NA | 4.3 | 0 | |
| Type of Pain | Nociceptive | 39.5% (n = 15) | 50% (n = 3) | NA |
| Neuropathic | 2.6% (n = 1) | 16.7% (n = 1) | NA | |
| Mixed | 57.9% (n = 22) | 33.3% (n = 2) | NA | |
| Type of Dementia | Vascular | 36.8% (n = 14) | NA | NA |
| Alzheimer | 36.8% (n = 14) | NA | NA | |
| Mixed | 7.9% (n = 3) | NA | NA | |
| Other | 18.4% (n = 7) | NA | NA | |
| Under opioid treatment | 39.5% (n = 15) | 66.7% (n = 4) | NA | |
| Without Pain (n = 9) | With Pain (n = 44) | ||
|---|---|---|---|
| M ± SD | M ± SD | p | |
| Monocytes | |||
| % | 4.19 ± 1.45 | 10.27± 20.5 | 0.025 * |
| % CD11c | 88.52 ± 7.23 | 294.67 ± 923.03 | 0.181 |
| MIF 11c | 816.98 ± 313.70 | 820.86 ± 303.38 | 0.503 |
| % CD86 | 32.69 ± 12.27 | 705.21 ± 3073.33 | 0.130 |
| MIF 86 | 634.20 ± 20.58 | 608.65 ± 143.02 | 0.850 |
| % CD163 | 85.63 ± 6.36 | 115.35 ± 150.62 | 0.487 |
| MIF 163 | 3061.99 ± 1033.45 | 2378.85 ± 1840.89 | 0.050 * |
| % CD206 | 14.08 ± 7.80 | 59.36 ± 230.35 | 0.047 * |
| MIF 206 | 534.29 ± 54.31 | 469.01 ± 14.66 | 0.019 * |
| % 11c/86 | 31.76± 12.10 | 99.96 ± 352.47 | 0.123 |
| % 163/206 | 9.5 ± 5.7 | 4.8 ± 5.6 | 0.004 ** |
| Classical monocytes | |||
| % | 85.3 ± 5.4 | 91.1 ± 4.2 | 0.003 ** |
| % CD11c | 91.9 ± 8.3 | 93.6 ± 9.4 | 0.250 |
| MIF 11c | 740.6 ± 286.2 | 825.4 ± 260.7 | 0.182 |
| % CD86 | 30.1 ± 12.3 | 21.7 ± 13.7 | 0.070 |
| MIF 86 | 592.1 ± 13.7 | 593.1 ± 23.8 | 0.781 |
| % CD163 | 95.6 ± 6.3 | 88.0 ± 9.4 | 0.010 ** |
| MIF 163 | 3185.1 ± 1119.8 | 2526.7 ± 1799.5 | 0.079 |
| % CD206 | 11.2 ± 6.9 | 6.7 ± 6.3 | 0.039 * |
| MIF 206 | 503.4 ± 48.6 | 472.9 ± 89.8 | 0.021 * |
| % 11c/86 | 29.0 ± 12.1 | 21.0 ± 13.0 | 0.091 |
| % 163/206 | 11.1 ± 6.8 | 6.5 ± 6.1 | 0.038 * |
| Intermediate | |||
| % | 5.7 ± 2.6 | 3.1 ± 2.0 | 0.008 ** |
| % CD11c | 98.9 ± 1.0 | 98.4 ± 3.1 | 0.770 |
| MIF 11c | 1769.1 ± 601.1 | 1743.8 ± 551.8 | 0.947 |
| % CD86 | 78.0 ± 9.5 | 68.5 ± 22.5 | 0.376 |
| MIF 86 | 813.7 ± 90.3 | 853.4 ± 103.1 | 0.174 |
| % CD163 | 88.1 ± 9.6 | 79.7 ± 13.9 | 0.064 |
| MIF 163 | 2397.9 ± 1125.5 | 2843.9 ± 3818.2 | 0.174 |
| % CD206 | 43.7 ± 17.6 | 35.7 ± 15.5 | 0.328 |
| MIF 206 | 537.4 ± 70.1 | 548.4 ± 185.5 | 0.682 |
| % 11c/86 | 77.8 ± 9.6 | 68.4 ± 22.4 | 0.362 |
| % 163/206 | 41.5 ± 18.0 | 33.2 ± 15.3 | 0.229 |
| Non-classical | |||
| % | 5.53 ± 3.25 | 2.79 ± 2.50 | 0.011 * |
| % CD11c | 78.1 ± 30.4 | 78.7 ± 26.2 | 0.812 |
| MIF 11c | 1612.8 ± 623.4 | 1713.7 ± 548.2 | 0.518 |
| % CD86 | 58.8 ± 26.0 | 64.2 ± 26.9 | 0.391 |
| MIF 86 | 791.0 ± 82.1 | 854.3 ± 121.9 | 0.129 |
| % CD163 | 14.6 ± 12.4 | 12.6 ± 7.6 | 0.771 |
| MIF 163 | 813.05 ± 196.72 | 885.05 ± 327.74 | 0.947 |
| % CD206 | 17.0 ± 16.3 | 11.4 ± 9.2 | 0.187 |
| MIF 206 | 634.7 ± 203.5 | 572.9 ± 347.5 | 0.099 |
| % 11c/86 | 58.7 ± 26.0 | 64.1 ± 26.9 | 0.383 |
| % 163/206 | 4.1 ± 4.7 | 3.8 ± 4.9 | 0.561 |
| Nociceptive (n = 18) | Mixed (n = 20) | ||
|---|---|---|---|
| M ± SD | M ± SD | p | |
| Granulocytes | 71.75 ± 12.42 | 73.00 ± 11.06 | 0.808 |
| Linfocytes | 20.51 ± 10.86 | 637.36 ± 1843.35 | 0.395 |
| Monocytes | |||
| % | 5.48 ± 2.26 | 15.77 ± 29.48 | 0.301 |
| % CD11c | 83.16 ± 20.92 | 539.46 ± 1332.28 | 0.002 ** |
| MIF 11c | 743.56 ± 165.92 | 870.15 ± 362.37 | 0.068 |
| % CD86 | 24.11 ± 13.78 | 1494.07 ± 4445.82 | 0.649 |
| MIF 86 | 639.67 ± 37.13 | 574.51 ± 204.14 | 0.466 |
| % CD163 | 82.39 ± 9.20 | 153.51 ± 217.85 | 0.671 |
| MIF 163 | 3010.81 ± 2422.58 | 1698.99 ± 793.94 | 0.013 ** |
| % CD206 | 8.42 ± 5.07 | 118.12 ± 333.30 | 0.605 |
| MIF 206 | 510.91 ± 54.65 | 425.07 ± 197.91 | 0.000 *** |
| % 11c/86 | 23.16 ± 12.93 | 189.30 ± 510.08 | 0.605 |
| % 163/206 | 5.42 ± 3.46 | 4.24 ± 7.72 | 0.027 * |
| Classical monocytes | |||
| % | 89.68 ± 4.39 | 92.26 ± 2.55 | 0.092 |
| % CD11c | 91.57 ± 9.69 | 97.88 ± 2.13 | 0.005 ** |
| MIF 11c | 709.87 ± 157.26 | 928.22 ± 249.20 | 0.008 ** |
| % CD86 | 21.13 ± 13.76 | 22.16 ± 14.10 | 0.779 |
| MIF 86 | 586.91 ± 15.35 | 598.80 ± 27.90 | 0.291 |
| % CD163 | 89.06 ± 9.86 | 86.85 ± 9.09 | 0.269 |
| MIF 163 | 3053.45 ± 2405.70 | 1905.96 ± 555.69 | 0.041 * |
| % CD206 | 6.79 ± 4.50 | 6.18 ± 7.92 | 0.166 |
| MIF 206 | 478.14 ± 39.38 | 469.28 ± 129.75 | 0.016 ** |
| % 11c/86 | 20.14 ± 12.67 | 22.05 ± 14.04 | 0.741 |
| % 163/206 | 6.64 ± 4.19 | 5.98 ± 7.64 | 0.137 |
| Intermediate | |||
| % | 3.77 ± 2.37 | 2.77 ± 1.27 | 0.290 |
| % CD11c | 97.99 ± 2.65 | 99.66 ± 0.39 | 0.004 ** |
| MIF 11c | 1518.99 ± 474.10 | 1976.88 ± 536.37 | 0.013 * |
| % CD86 | 66.96 ± 26.87 | 70.89 ± 17.14 | 0.974 |
| MIF 86 | 832.39 ± 98.82 | 871.68 ± 104.54 | 0.488 |
| % CD163 | 80.41 ± 15.61 | 79.65 ± 13.11 | 0.644 |
| MIF 163 | 3678.20 ± 5385.99 | 1849.45 ± 629.27 | 0.488 |
| % CD206 | 36.37 ± 16.27 | 33.21 ± 15.31 | 0.668 |
| MIF 206 | 575.94 ± 124.37 | 517.74 ± 247.86 | 0.041 * |
| % 11c/86 | 66.79 ± 26.82 | 70.88 ± 17.13 | 0.974 |
| % 163/206 | 34.37 ± 16.14 | 30.24 ± 15.10 | 0.530 |
| Non-classical | |||
| % | 3.72 ± 2.69 | 1.82 ± 1.09 | 0.037 * |
| % CD11c | 74.93 ± 30.12 | 87.43 ± 18.27 | 0.409 |
| MIF 11c | 1522.18 ± 466.66 | 1999.55 ± 447.14 | 0.005 ** |
| % CD86 | 60.33 ± 31.01 | 73.32 ± 17.57 | 0.276 |
| MIF 86 | 828.17 ± 104.68 | 864.42 ± 98.72 | 0.269 |
| % CD163 | 13.68 ± 7.98 | 12.84 ± 7.77 | 0.520 |
| MIF 163 | 941.04 ± 357.84 | 775.93 ± 89.13 | 0.276 |
| % CD206 | 12.46 ± 10.10 | 10.40 ± 7.58 | 0.869 |
| MIF 206 | 729.17 ± 465.05 | 443.38 ± 70.24 | 0.060 |
| % 11c/86 | 60.24 ± 31.02 | 73.22 ± 17.65 | 0.283 |
| % 163/20 | 4.45 ± 4.52 | 3.54 ± 5.76 | 0.209 |
| Without Opioids | Opioid Therapy | |||
|---|---|---|---|---|
| M ± SD | M ± SD | p | ||
| Monocytes | %163 | 126.57 ± 169.27 | 80.54 ± 9.92 | 0.135 |
| MIF163 | 2645.37 ± 2041.58 | 2246.61 ± 985.25 | 0.441 | |
| Classical monocytes | ||||
| %163 | 91.1 ± 8.1 | 86.6 ± 10.7 | 0.108 | |
| MIF163 | 2858.3 ± 1978.5 | 2303.3 ± 1064.9 | 0.279 | |
| Intermediate monocytes | ||||
| %163 | 85.7 ± 9.2 | 74.0 ± 16.3 | 0.010 * | |
| MIF163 | 3363.0 ± 4288.1 | 1755.8 ± 440.3 | 0.051 | |
| Non-classical monocytes | ||||
| %163 | 13.9 ± 10.1 | 11.4 ± 5.1 | 0.334 | |
| MIF163 | 936.97 ± 362.22 | 762.52 ± 128.76 | 0.056 | |
| Without Dementia | With Dementia | |||
|---|---|---|---|---|
| M ± SD | M ± SD | p | ||
| Monocytes | ||||
| % | 4.73 ± 2.11 | 11.08 | 22.11 | 0.037 * |
| % CD11c | 88.29 ± 10.05 | 330.11 ± 996.73 | 0.125 | |
| MIF 11c | 784.79 ± 256.61 | 835.32 ± 321.77 | 0.305 | |
| % CD86 | 29.65 ± 14.25 | 821.8 ± 3319.12 | 0.271 | |
| MIF 86 | 631.93± 24.31 | 605.24 ± 154.41 | 0.791 | |
| % CD163 | 85.39 ± 7.11 | 120.54 ± 162.75 | 0.335 | |
| MIF 163 | 3420.37 ± 2557.46 | 2108.14 ± 1055.71 | 0.032 * | |
| % CD206 | 12.68 ± 9.22 | 67.72 ± 248.83 | 0.138 | |
| MIF 206 | 562.85± 129.08 | 445.58 ± 123 | 0.001 *** | |
| % 11c/86 | 28.83 ± 13.73 | 112.91 ± 380.71 | 0.236 | |
| % 163/206 | 9.2 ± 8.5 | 4.1 ± 3.2 | 0.010 ** | |
| Classical monocytes | ||||
| % | 87.8 ± 5.6 | 91 ± 4.4 | 0.054 | |
| % CD11c | 91.1 ± 10.3 | 94.3 ± 8.6 | 0.097 | |
| MIF 11c | 726 ± 234.2 | 847.4 ± 272.2 | 0.081 | |
| % CD86 | 27.5 ± 13.9 | 21.4 ± 13.4 | 0.114 | |
| MIF 86 | 591.7 ± 11.9 | 593.5 ± 25.7 | 0.991 | |
| % CD163 | 93.6 ± 8.2 | 87.5 ± 9.3 | 0.012 * | |
| MIF 163 | 3497.5 ± 2534.9 | 2265 ± 978.4 | 0.063 | |
| % CD206 | 10.6 ± 9.2 | 6.1 ± 4.5 | 0.087 | |
| MIF 206 | 528.2 ± 127 | 456.1 ± 40.6 | 0.002 ** | |
| % 11c/86 | 26.5 ± 13.3 | 20.6 ± 12.8 | 0.114 | |
| % 163/206 | 10.4 ± 9 | 6 ± 4.3 | 0.089 | |
| Intermediate | ||||
| % | 4.7 ± 2.5 | 3.1 ± 2.1 | 0.028 * | |
| % CD11c | 98.6 ± 2.1 | 98.4 ± 3.2 | 0.832 | |
| MIF 11c | 1653.2 ± 565.9 | 1791.9 ± 552.9 | 0.417 | |
| % CD86 | 71.5 ± 20.5 | 69.7 ± 21.4 | 0.920 | |
| MIF 86 | 820.3 ± 98.1 | 857.6 ± 101.8 | 0.158 | |
| % CD163 | 87.4 ± 10 | 78.5 ± 14.1 | 0.021 * | |
| MIF 163 | 3726.8 ± 5665.9 | 2320.9 ± 1730.1 | 0.085 | |
| % CD206 | 42.5 ± 15.9 | 34.8 ± 15.8 | 0.213 | |
| MIF 206 | 607.6 ± 226.6 | 518.5 ± 130.7 | 0.107 | |
| % 11c/86 | 71.4 ± 20.4 | 69.6 ± 21.4 | 0.903 | |
| % 163/206 | 40.5 ± 15.9 | 32.1 ± 15.6 | 0.095 | |
| Non-classical | ||||
| % | 4.27 ± 3.41 | 2.87 ± 2.46 | 0.221 | |
| % CD11c | 76.5 ± 30 | 79.5 ± 25.5 | 0.656 | |
| MIF 11c | 1636.6 ± 577.9 | 1721.2 ± 554.9 | 0.601 | |
| % CD86 | 61.5 ± 27.9 | 64 ± 26.3 | 0.648 | |
| MIF 86 | 828.5 ± 94.4 | 848.7 ± 127.4 | 0.664 | |
| % CD163 | 13.3 ± 9.7 | 12.9 ± 8.2 | 0.764 | |
| MIF 163 | 870.87 ± 339.24 | 871.86 ± 296.75 | 0.714 | |
| % CD206 | 14.6 ± 13.8 | 11.5 ± 9.3 | 0.368 | |
| MIF 206 | 752.9 ± 447.3 | 507.9 ± 218.5 | 0.008 ** | |
| % 11c/86 | 61.4 ± 27.9 | 63.9 ± 26.3 | 0.640 | |
| % 163/206 | 3.8 ± 4 | 3.9 ± 5.2 | 0.490 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, H.; Alves, R.; Jorge, J.; Gonçalves, A.C.; Sarmento-Ribeiro, A.B.; Teixeira-Veríssimo, M.; Andrade, J.P.; Dourado, M. Monocytes in the Characterization of Pain in Palliative Patients with Severe Dementia—A Pilot Study. Int. J. Mol. Sci. 2023, 24, 10723. https://doi.org/10.3390/ijms241310723
Ribeiro H, Alves R, Jorge J, Gonçalves AC, Sarmento-Ribeiro AB, Teixeira-Veríssimo M, Andrade JP, Dourado M. Monocytes in the Characterization of Pain in Palliative Patients with Severe Dementia—A Pilot Study. International Journal of Molecular Sciences. 2023; 24(13):10723. https://doi.org/10.3390/ijms241310723
Chicago/Turabian StyleRibeiro, Hugo, Raquel Alves, Joana Jorge, Ana Cristina Gonçalves, Ana Bela Sarmento-Ribeiro, Manuel Teixeira-Veríssimo, José Paulo Andrade, and Marília Dourado. 2023. "Monocytes in the Characterization of Pain in Palliative Patients with Severe Dementia—A Pilot Study" International Journal of Molecular Sciences 24, no. 13: 10723. https://doi.org/10.3390/ijms241310723
APA StyleRibeiro, H., Alves, R., Jorge, J., Gonçalves, A. C., Sarmento-Ribeiro, A. B., Teixeira-Veríssimo, M., Andrade, J. P., & Dourado, M. (2023). Monocytes in the Characterization of Pain in Palliative Patients with Severe Dementia—A Pilot Study. International Journal of Molecular Sciences, 24(13), 10723. https://doi.org/10.3390/ijms241310723