


Effect of 12-Week BMI-Based Vitamin D3 Supplementation in Parkinson’s Disease with Deep Brain Stimulation on Physical Performance, Inflammation, and Vitamin D Metabolites
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Results
2.1. Demographic Characteristics
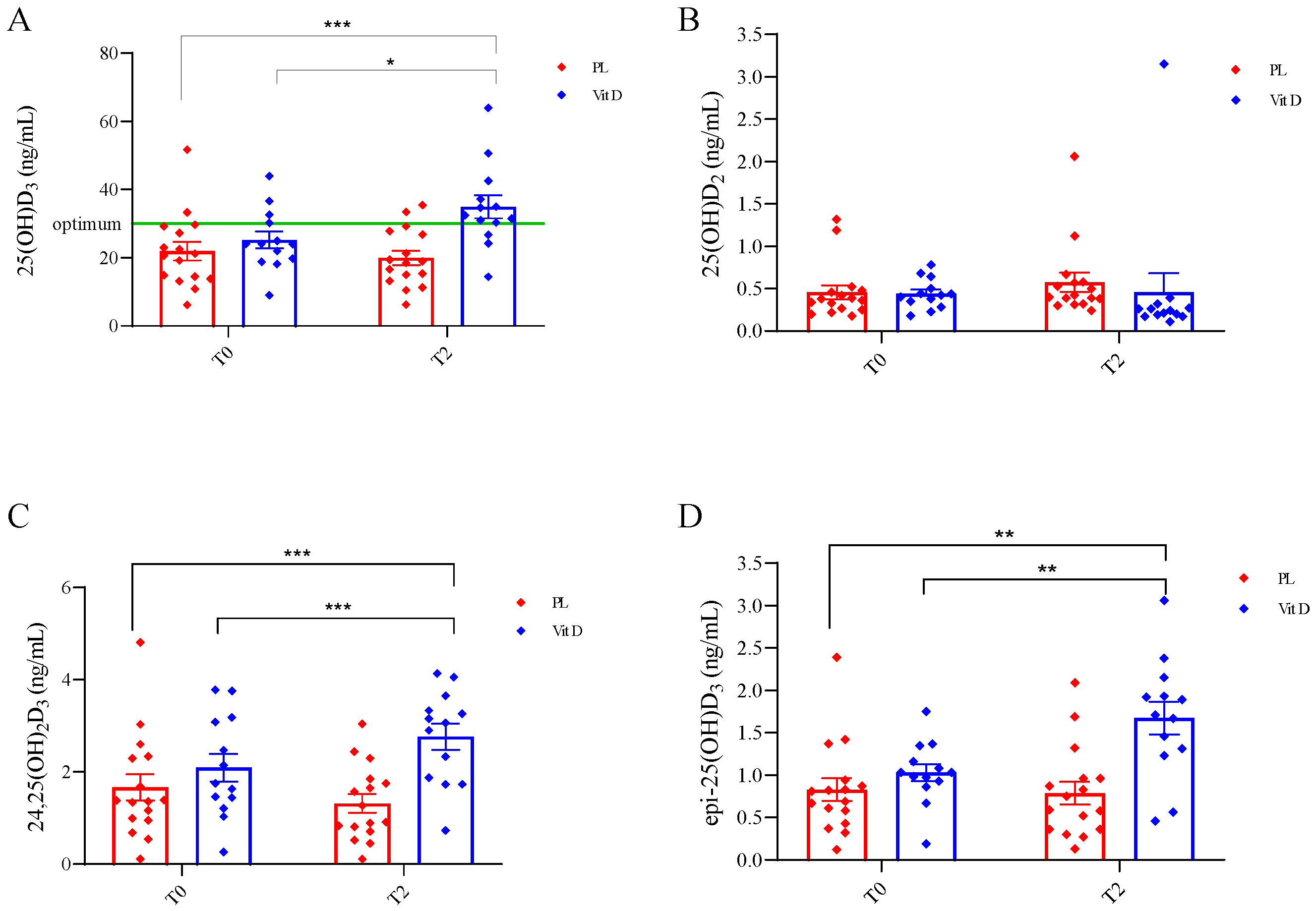
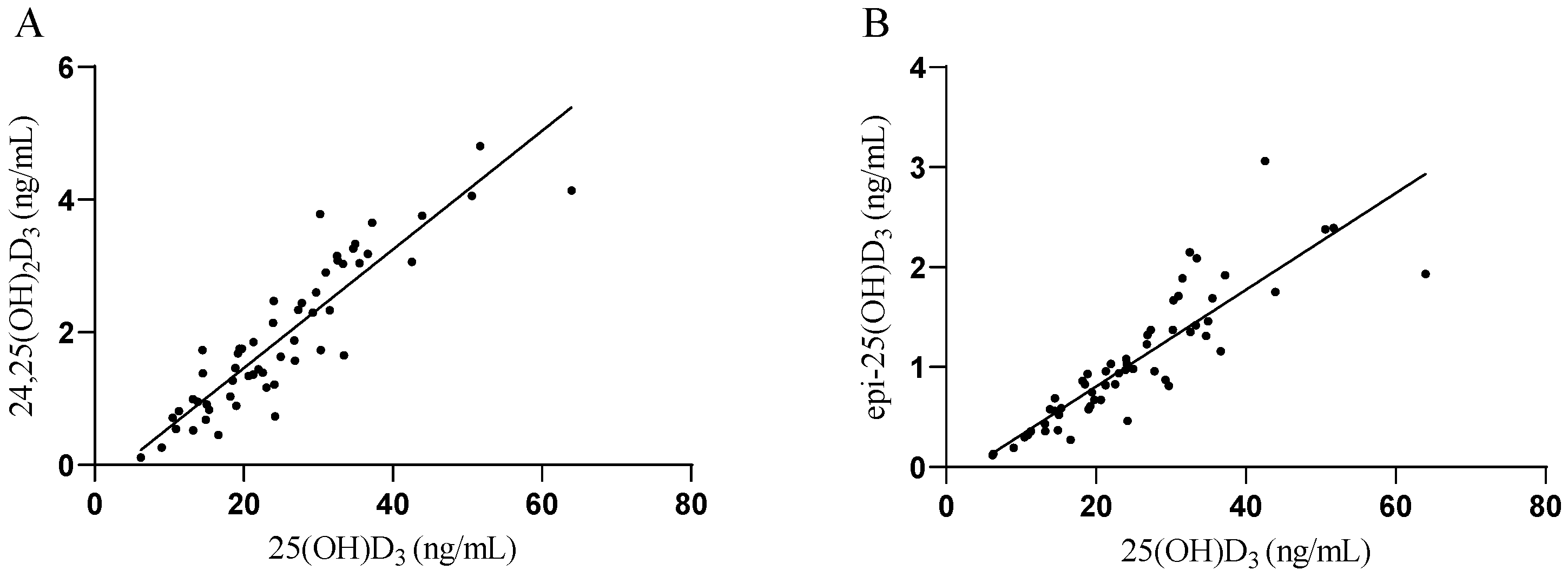
2.2. Vitamin D Metabolites

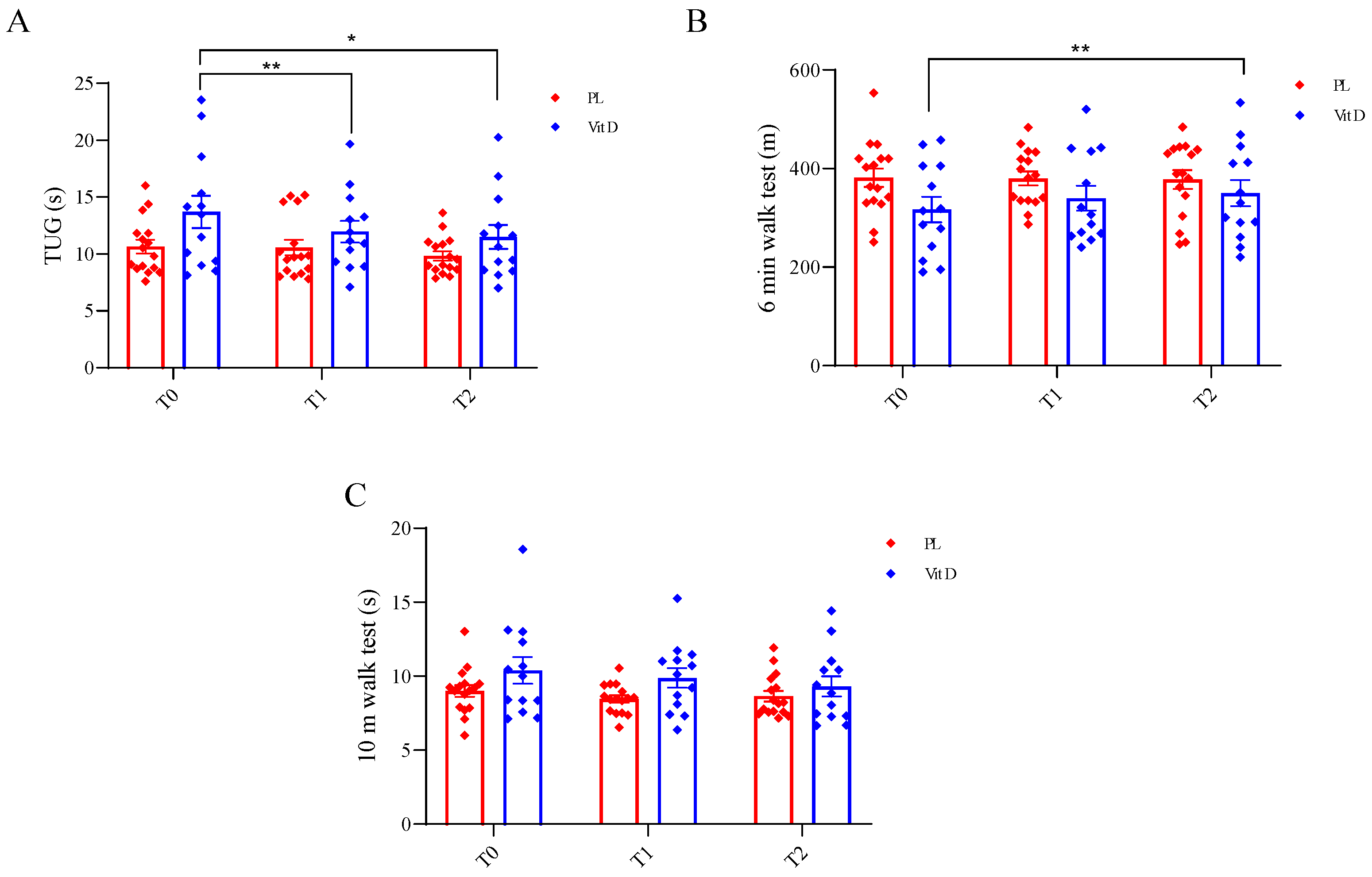
2.3. Functional Tests
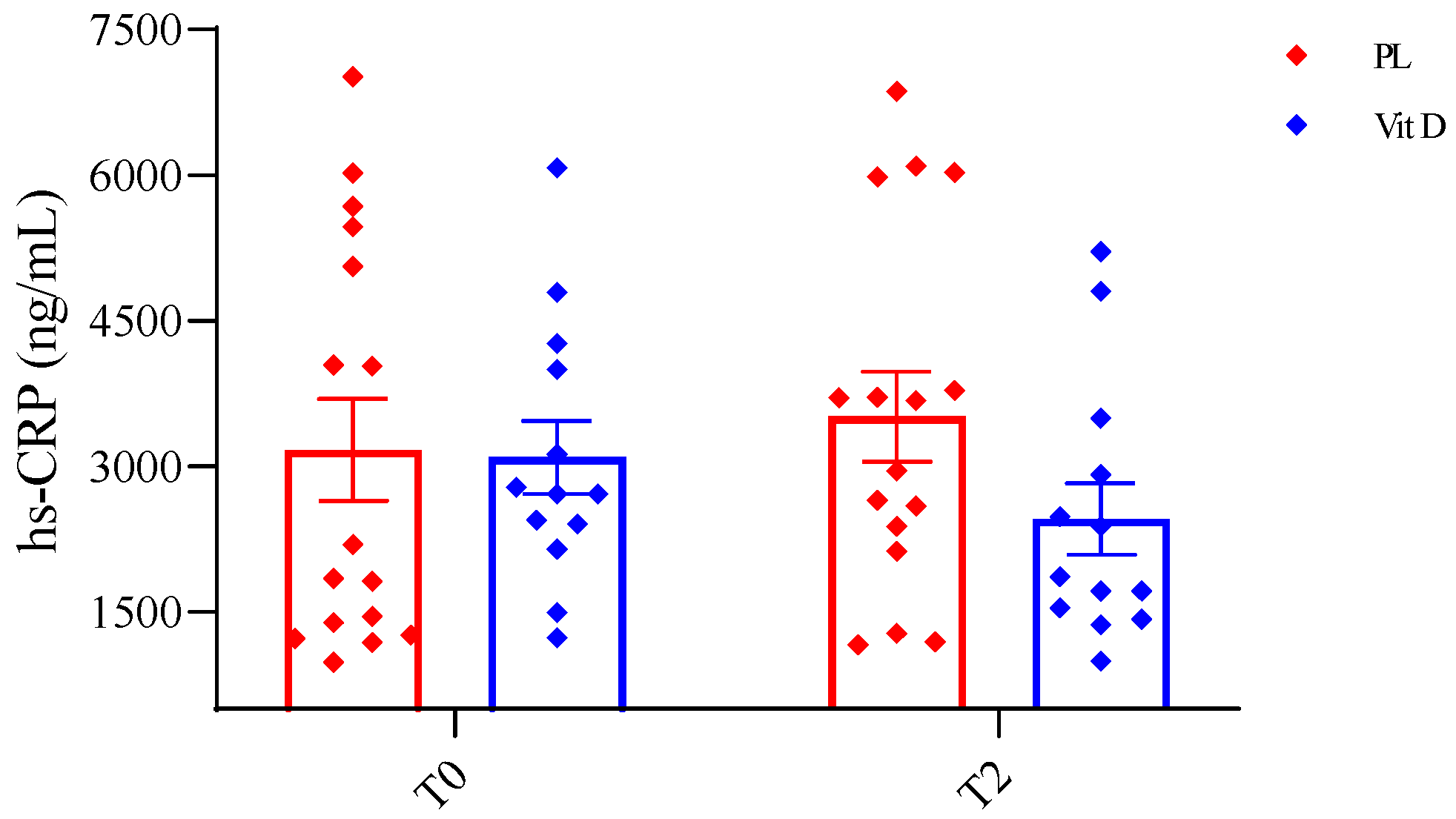
2.4. General Inflammation Status
3. Discussion
4. Materials and Methods
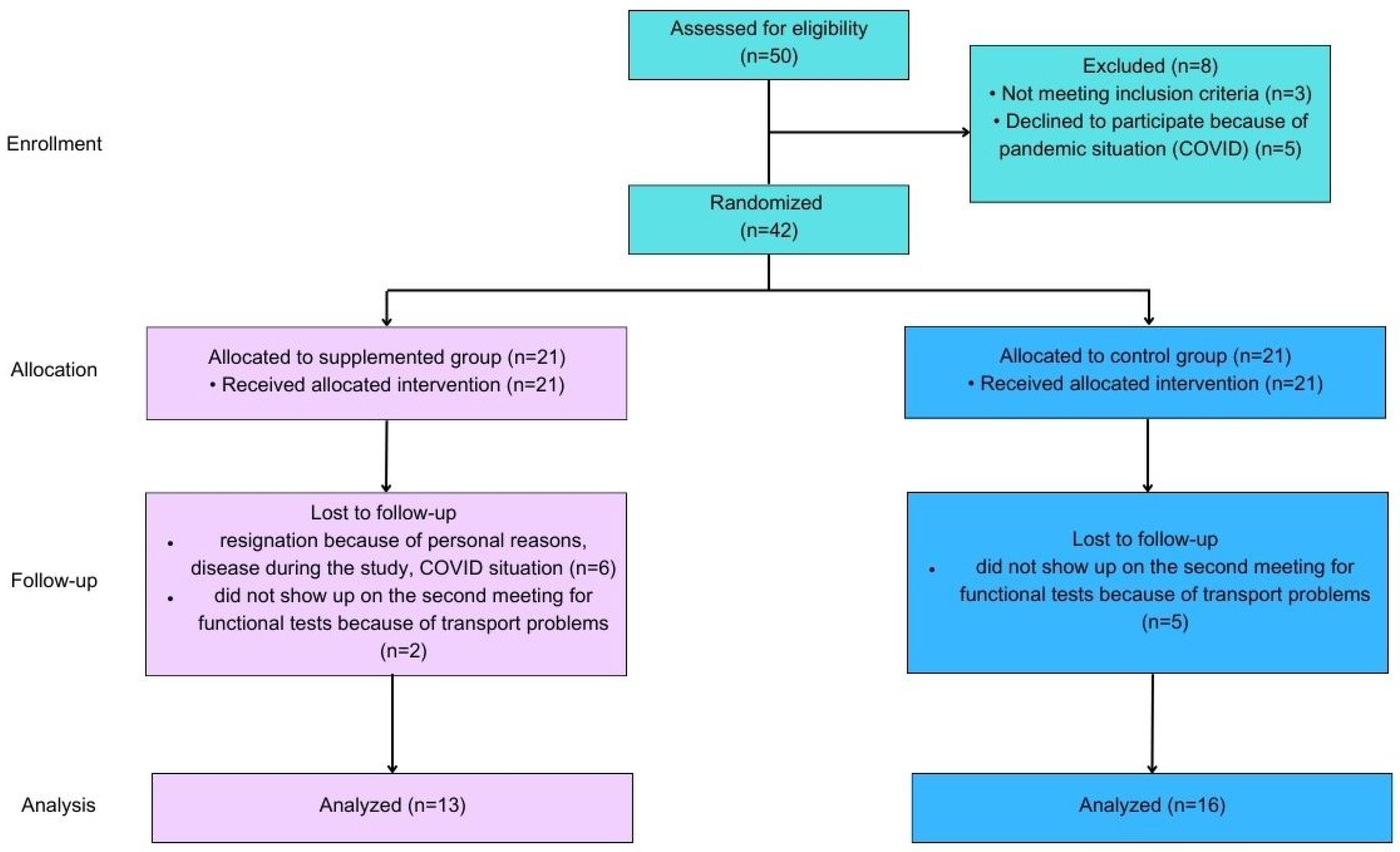
4.1. Design of the Study
4.2. Participants
4.3. Intervention
4.4. Visit Program and Material Collection
4.5. Functional Tests
4.6. Measurement of Vitamin D Metabolites
4.7. Measurement of C-Reactive Protein
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorsey, E.R.; Constantinescu, R.; Thompson, J.P.; Biglan, K.M.; Holloway, R.G.; Kieburtz, K.; Marshall, F.J.; Ravina, B.M.; Schifitto, G.; Siderowf, A.; et al. Projected Number of People with Parkinson Disease in the Most Populous Nations, 2005 through 2030. Neurology 2007, 68, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.E. Biology of Parkinson’s Disease: Pathogenesis and Pathophysiology of a Multisystem Neurodegenerative Disorder. Dialogues Clin. Neurosci. 2004, 6, 259–280. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease. JAMA 2020, 323, 548. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Tan, E.K. Parkinson’s Disease: Etiopathogenesis and Treatment. J. Neurol. Neurosurg. Psychiatry 2020, 91, 795–808. [Google Scholar] [CrossRef]
- Maiti, P.; Manna, J.; Dunbar, G.L. Current Understanding of the Molecular Mechanisms in Parkinson’s Disease: Targets for Potential Treatments. Transl. Neurodegener. 2017, 6, 28. [Google Scholar] [CrossRef]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson Disease. Nat. Rev. Dis. Prim. 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, X.; Yang, G. Adenosinergic Pathway in Parkinson’s Disease: Recent Advances and Therapeutic Perspective. Mol. Neurobiol. 2023, 60, 3054–3070. [Google Scholar] [CrossRef]
- Aum, D.J.; Tierney, T.S. Deep Brain Stimulation: Foundations and Future Trends. Front. Biosci. 2018, 23, 4586. [Google Scholar] [CrossRef]
- Macerollo, A.; Zrinzo, L.; Akram, H.; Foltynie, T.; Limousin, P. Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease: Current Trends and Future Directions. Expert Rev. Med. Devices 2020, 17, 1063–1074. [Google Scholar] [CrossRef] [PubMed]
- Oz, F.; Yucekeya, B.; Huzmeli, I.; Yilmaz, A. Does Subthalamic Nucleus Deep Brain Stimulation Affect the Static Balance at Different Frequencies? Neurocirugía 2023, 34, 60–66. [Google Scholar] [CrossRef]
- Khundmiri, S.J.; Murray, R.D.; Lederer, E. PTH and Vitamin D. Compr. Physiol. 2016, 6, 561–601. [Google Scholar] [CrossRef]
- Dzik, K.P.; Kaczor, J.J. Mechanisms of Vitamin D on Skeletal Muscle Function: Oxidative Stress, Energy Metabolism and Anabolic State. Eur. J. Appl. Physiol. 2019, 119, 825–839. [Google Scholar] [CrossRef] [PubMed]
- Koduah, P.; Paul, F.; Dörr, J.-M. Vitamin D in the Prevention, Prediction and Treatment of Neurodegenerative and Neuroinflammatory Diseases. EPMA J. 2017, 8, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Plantone, D.; Primiano, G.; Manco, C.; Locci, S.; Servidei, S.; De Stefano, N. Vitamin D in Neurological Diseases. Int. J. Mol. Sci. 2023, 24, 87. [Google Scholar] [CrossRef]
- Evatt, M.L.; DeLong, M.R.; Khazai, N.; Rosen, A.; Triche, S.; Tangpricha, V. Prevalence of Vitamin D Insufficiency in Patients with Parkinson Disease and Alzheimer Disease. Arch. Neurol. 2008, 65, 1348–1352. [Google Scholar] [CrossRef]
- Fullard, M.E.; Duda, J.E. A Review of the Relationship Between Vitamin D and Parkinson Disease Symptoms. Front. Neurol. 2020, 11, 454. [Google Scholar] [CrossRef]
- Qin, X.-Y.; Zhang, S.-P.; Cao, C.; Loh, Y.P.; Cheng, Y. Aberrations in Peripheral Inflammatory Cytokine Levels in Parkinson Disease. JAMA Neurol. 2016, 73, 1316. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Gu, H.; Mao, C.; Chen, J.; Liu, C. Association of Inflammatory Factors and Aging in Parkinson’s Disease. Neurosci. Lett. 2020, 736, 135259. [Google Scholar] [CrossRef]
- Kim, R.; Kim, H.J.; Kim, A.; Jang, M.; Kim, A.; Kim, Y.; Yoo, D.; Im, J.H.; Choi, J.H.; Jeon, B. Peripheral Blood Inflammatory Markers in Early Parkinson’s Disease. J. Clin. Neurosci. 2018, 58, 30–33. [Google Scholar] [CrossRef]
- Chromiec, P.A.; Urbaś, Z.K.; Jacko, M.; Kaczor, J.J. The Proper Diet and Regular Physical Activity Slow Down the Development of Parkinson Disease. Aging Dis. 2021, 12, 1605. [Google Scholar] [CrossRef]
- Luthra, N.S.; Kim, S.; Zhang, Y.; Christine, C.W. Characterization of Vitamin D Supplementation and Clinical Outcomes in a Large Cohort of Early Parkinson’s Disease. J. Clin. Mov. Disord. 2018, 5, 7. [Google Scholar] [CrossRef]
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in Obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef]
- Suzuki, M.; Yoshioka, M.; Hashimoto, M.; Murakami, M.; Noya, M.; Takahashi, D.; Urashima, M. Randomized, Double-Blind, Placebo-Controlled Trial of Vitamin D Supplementation in Parkinson Disease. Am. J. Clin. Nutr. 2013, 97, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Evatt, M.L.; Delong, M.R.; Kumari, M.; Auinger, P.; Mcdermott, M.P.; Tangpricha, V. High Prevalence of Hypovitaminosis D Status in Patients With Early Parkinson Disease. Arch. Neurol. 2011, 68, 314–319. [Google Scholar] [CrossRef]
- Van Den Bos, F.; Speelman, A.D.; Van Nimwegen, M.; Van Der Schouw, Y.T.; Backx, F.J.G.; Bloem, B.R.; Munneke, M.; Verhaar, H.J.J. Bone Mineral Density and Vitamin D Status in Parkinson’s Disease Patients. J. Neurol. 2013, 260, 754–760. [Google Scholar] [CrossRef]
- Zhang, H.J.; Zhang, J.R.; Mao, C.J.; Li, K.; Wang, F.; Chen, J.; Liu, C.F. Relationship between 25-Hydroxyvitamin D, Bone Density, and Parkinson’s Disease Symptoms. Acta Neurol. Scand. 2019, 140, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Barichella, M.; Cereda, E.; Iorio, L.; Pinelli, G.; Ferri, V.; Cassani, E.; Bolliri, C.; Caronni, S.; Pusani, C.; Schiaffino, M.G.; et al. Clinical Correlates of Serum 25-Hydroxyvitamin D in Parkinson’s Disease. Nutr. Neurosci. 2020, 25, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Couchman, L.; Moniz, C.F. Analytical Considerations for the Biochemical Assessment of Vitamin D Status. Ther. Adv. Musculoskelet. 2017, 9, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Kmieć, P.; Minkiewicz, I.; Rola, R.; Sworczak, K.; Żmijewski, M.A.; Kowalski, K. Vitamin D Status Including 3-Epi-25(OH)D3 among Adult Patients with Thyroid Disorders during Summer Months. Endokrynol. Pol. 2018, 69, 653–660. [Google Scholar] [CrossRef]
- Barichella, M.; Cereda, E.; Pinelli, G.; Iorio, L.; Caroli, D.; Masiero, I.; Ferri, V.; Cassani, E.; Bolliri, C.; Caronni, S.; et al. Muscle-Targeted Nutritional Support for Rehabilitation in Patients with Parkinsonian Syndrome. Neurology 2019, 93, E485–E496. [Google Scholar] [CrossRef]
- Dorszewska, J.; Prendecki, M.; Lianeri, M.; Kozubski, W. Molecular Effects of L-Dopa Therapy in Parkinson’s Disease. Curr. Genom. 2014, 15, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bayo-Olugbami, A.; Nafiu, A.B.; Amin, A.; Ogundele, O.M.; Lee, C.C.; Owoyele, B.V. Vitamin D Attenuated 6-OHDA-Induced Behavioural Deficits, Dopamine Dysmetabolism, Oxidative Stress, and Neuro-Inflammation in Mice. Nutr. Neurosci. 2020, 25, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Prtina, A.; Rašeta Simović, N.; Milivojac, T.; Vujnić, M.; Grabež, M.; Djuric, D.; Stojiljković, M.P.; Soldat Stanković, V.; Čolić, M.J.; Škrbić, R. The Effect of Three-Month Vitamin D Supplementation on the Levels of Homocysteine Metabolism Markers and Inflammatory Cytokines in Sera of Psoriatic Patients. Biomolecules 2021, 11, 1865. [Google Scholar] [CrossRef]
- Habibi, A.H.; Anamoradi, A.; Shahidi, G.A.; Razmeh, S.; Alizadeh, E.; Moradian Kokhedan, K. Treatment of Levodopa-Induced Dyskinesia with Vitamin D: A Randomized, Double-Blind, Placebo-Controlled Trial. Neurol. Int. 2018, 10, 7737. [Google Scholar] [CrossRef]
- Dzik, K.; Skrobot, W.; Flis, D.J.; Karnia, M.; Libionka, W.; Kloc, W.; Kaczor, J.J. Vitamin D Supplementation Attenuates Oxidative Stress in Paraspinal Skeletal Muscles in Patients with Low Back Pain. Eur. J. Appl. Physiol. 2018, 118, 143–151. [Google Scholar] [CrossRef]
- Nocera, J.R.; Stegemöller, E.L.; Malaty, I.A.; Okun, M.S.; Marsiske, M.; Hass, C.J. Using the Timed Up & Go Test in a Clinical Setting to Predict Falling in Parkinson’s Disease. Arch. Phys. Med. Rehabil. 2013, 94, 1300–1305. [Google Scholar] [CrossRef]
- Rodziewicz-Flis, E.A.; Kawa, M.; Skrobot, W.R.; Flis, D.J.; Wilczyńska, D.; Szaro-Truchan, M.; Bolek-Adamek, J.; Kaczor, J.J. The Positive Impact of 12 Weeks of Dance and Balance Training on the Circulating Amyloid Precursor Protein and Serotonin Concentration as Well as Physical and Cognitive Abilities in Elderly Women. Exp. Gerontol. 2022, 162, 111746. [Google Scholar] [CrossRef] [PubMed]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between Gait Speed and Well-Known Fall Risk Factors among Community-Dwelling Older Adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef]
- Aschauer, R.; Unterberger, S.; Zöhrer, P.A.; Draxler, A.; Franzke, B.; Strasser, E.-M.; Wagner, K.-H.; Wessner, B. Effects of Vitamin D3 Supplementation and Resistance Training on 25-Hydroxyvitamin D Status and Functional Performance of Older Adults: A Randomized Placebo-Controlled Trial. Nutrients 2021, 14, 86. [Google Scholar] [CrossRef]
- Lang, J.T.; Kassan, T.O.; Devaney, L.L.; Colon-Semenza, C.; Joseph, M.F. Test-Retest Reliability and Minimal Detectable Change for the 10-Meter Walk Test in Older Adults with Parkinson’s Disease. J. Geriatr. Phys. Ther. 2016, 39, 165–170. [Google Scholar] [CrossRef]
- Urell, C.; Zetterberg, L.; Hellström, K.; Anens, E. Factors Explaining Physical Activity Level in Parkinson´s Disease: A Gender Focus. Physiother. Theory Pract. 2021, 37, 507–516. [Google Scholar] [CrossRef]
- Da Costa, R.O.; Gadelha-Filho, C.V.J.; de Aquino, P.E.A.; Lima, L.A.R.; de Lucena, J.D.; Ribeiro, W.L.C.; Lima, F.A.V.; Neves, K.R.T.; de Barros Viana, G.S. Vitamin D (VD3) Intensifies the Effects of Exercise and Prevents Alterations of Behavior, Brain Oxidative Stress, and Neuroinflammation, in Hemiparkinsonian Rats. Neurochem. Res. 2023, 48, 142–160. [Google Scholar] [CrossRef]
- Smith, M.P.; Fletcher-Turner, A.; Yurek, D.M.; Cass, W.A. Calcitriol Protection against Dopamine Loss Induced by Intracerebroventricular Administration of 6-Hydroxydopamine. Neurochem. Res. 2006, 31, 533–539. [Google Scholar] [CrossRef]
- Lima, L.A.R.; Lopes, M.J.P.; Costa, R.O.; Lima, F.A.V.; Neves, K.R.T.; Calou, I.B.F.; Andrade, G.M.; Viana, G.S.B. Vitamin D Protects Dopaminergic Neurons against Neuroinflammation and Oxidative Stress in Hemiparkinsonian Rats. J. Neuroinflammation 2018, 15, 249. [Google Scholar] [CrossRef]
- Krasowska, K.; Skrobot, W.; Liedtke, E.; Sawicki, P.; Flis, D.J.; Dzik, K.P.; Libionka, W.; Kloc, W.; Kaczor, J.J. The Preoperative Supplementation with Vitamin D Attenuated Pain Intensity and Reduced the Level of Pro-Inflammatory Markers in Patients after Posterior Lumbar Interbody Fusion. Front. Pharmacol. 2019, 10, 527. [Google Scholar] [CrossRef]
- Ticinesi, A.; Meschi, T.; Lauretani, F.; Felis, G.; Franchi, F.; Pedrolli, C.; Barichella, M.; Benati, G.; Di Nuzzo, S.; Ceda, G.; et al. Nutrition and Inflammation in Older Individuals: Focus on Vitamin D, n-3 Polyunsaturated Fatty Acids and Whey Proteins. Nutrients 2016, 8, 186. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Li, J.; Qin, Q.; Wang, D.; Zhao, J.; An, K.; Mao, Z.; Min, Z.; Xiong, Y.; Li, J.; et al. A Systematic Review and Meta-Analysis of Inflammatory Biomarkers in Parkinson’s Disease. NPJ Park. Dis. 2023, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Song, I.-U.; Cho, H.-J.; Kim, J.-S.; Park, I.-S.; Lee, K.-S. Serum Hs-CRP Levels Are Increased in de Novo Parkinson’s Disease Independently from Age of Onset. Eur. Neurol. 2014, 72, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.; Baig, F.; Toulson, G.; Morovat, A.; Evetts, S.G.; Ben-Shlomo, Y.; Hu, M.T. Blood Biomarkers with Parkinson’s Disease Clusters and Prognosis: The Oxford Discovery Cohort. Mov. Disord. 2019, 35, 279–287. [Google Scholar] [CrossRef] [PubMed]
- De Amorim, J.S.C.; Torres, K.C.L.; Teixeira-Carvalho, A.; Martins-Filho, O.A.; Lima-Costa, M.F.; Peixoto, S.V. Inflammatory Markers and Occurrence of Falls. Rev. Saúde Pública 2019, 53, 35. [Google Scholar] [CrossRef]
- Dědečková, E.; Viták, R.; Jirásko, M.; Králová, M.; Topolčan, O.; Pecen, L.; Fürst, T.; Brož, P.; Kučera, R. Vitamin D3 Supplementation: Comparison of 1000 IU and 2000 IU Dose in Healthy Individuals. Life 2023, 13, 808. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Yalamanchili, V.; Smith, L.M. The Effect of Vitamin D Supplementation on Serum 25OHD in Thin and Obese Women. J. Steroid Biochem. Mol. Biol. 2013, 136, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Perna, S. The Enigma of Vitamin D Supplementation in Aging with Obesity. Minerva Gastroenterol 2022, 68, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Bacha, D.S.; Rahme, M.; Al-Shaar, L.; Baddoura, R.; Halaby, G.; Singh, R.J.; Mahfoud, Z.R.; Habib, R.; Arabi, A.; El-Hajj Fuleihan, G. Vitamin D3 Dose Requirement That Raises 25-Hydroxyvitamin D to Desirable Level in Overweight and Obese Elderly. J. Clin. Endocrinol. Metab. 2021, 106, e3644–e3654. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VitD Group (n = 13) | PL Group (n = 16) | |
|---|---|---|
| Age (years) | 63 ± 9 | 66 ± 6 |
| Sex | 6 M, 7 W | 13 M, 3 W |
| Height (cm) | 169 ± 12 | 174 ± 8 |
| Body mass (kg) | 78 ± 11 | 80 ± 20 |
| DBS implantation | 3–5 years ago | 3–5 years ago |
| H&Y | 2.5 | 2.5 |
| Duration of the disease | 8–13 years | 8–13 years |
| BMI | ≤25 → 3 | ≤25 → 6 |
| 25–30 → 8 | 25–30 → 8 | |
| ≥30 → 2 | ≥30 → 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bytowska, Z.K.; Korewo-Labelle, D.; Berezka, P.; Kowalski, K.; Przewłócka, K.; Libionka, W.; Kloc, W.; Kaczor, J.J. Effect of 12-Week BMI-Based Vitamin D3 Supplementation in Parkinson’s Disease with Deep Brain Stimulation on Physical Performance, Inflammation, and Vitamin D Metabolites. Int. J. Mol. Sci. 2023, 24, 10200. https://doi.org/10.3390/ijms241210200
Bytowska ZK, Korewo-Labelle D, Berezka P, Kowalski K, Przewłócka K, Libionka W, Kloc W, Kaczor JJ. Effect of 12-Week BMI-Based Vitamin D3 Supplementation in Parkinson’s Disease with Deep Brain Stimulation on Physical Performance, Inflammation, and Vitamin D Metabolites. International Journal of Molecular Sciences. 2023; 24(12):10200. https://doi.org/10.3390/ijms241210200
Chicago/Turabian StyleBytowska, Zofia Kinga, Daria Korewo-Labelle, Paweł Berezka, Konrad Kowalski, Katarzyna Przewłócka, Witold Libionka, Wojciech Kloc, and Jan Jacek Kaczor. 2023. "Effect of 12-Week BMI-Based Vitamin D3 Supplementation in Parkinson’s Disease with Deep Brain Stimulation on Physical Performance, Inflammation, and Vitamin D Metabolites" International Journal of Molecular Sciences 24, no. 12: 10200. https://doi.org/10.3390/ijms241210200
APA StyleBytowska, Z. K., Korewo-Labelle, D., Berezka, P., Kowalski, K., Przewłócka, K., Libionka, W., Kloc, W., & Kaczor, J. J. (2023). Effect of 12-Week BMI-Based Vitamin D3 Supplementation in Parkinson’s Disease with Deep Brain Stimulation on Physical Performance, Inflammation, and Vitamin D Metabolites. International Journal of Molecular Sciences, 24(12), 10200. https://doi.org/10.3390/ijms241210200