

Peritoneal Fluid Analysis of Advanced Ovarian Cancers after Hyperthermic Intraperitoneal Chemotherapy
 , ,
, , 
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
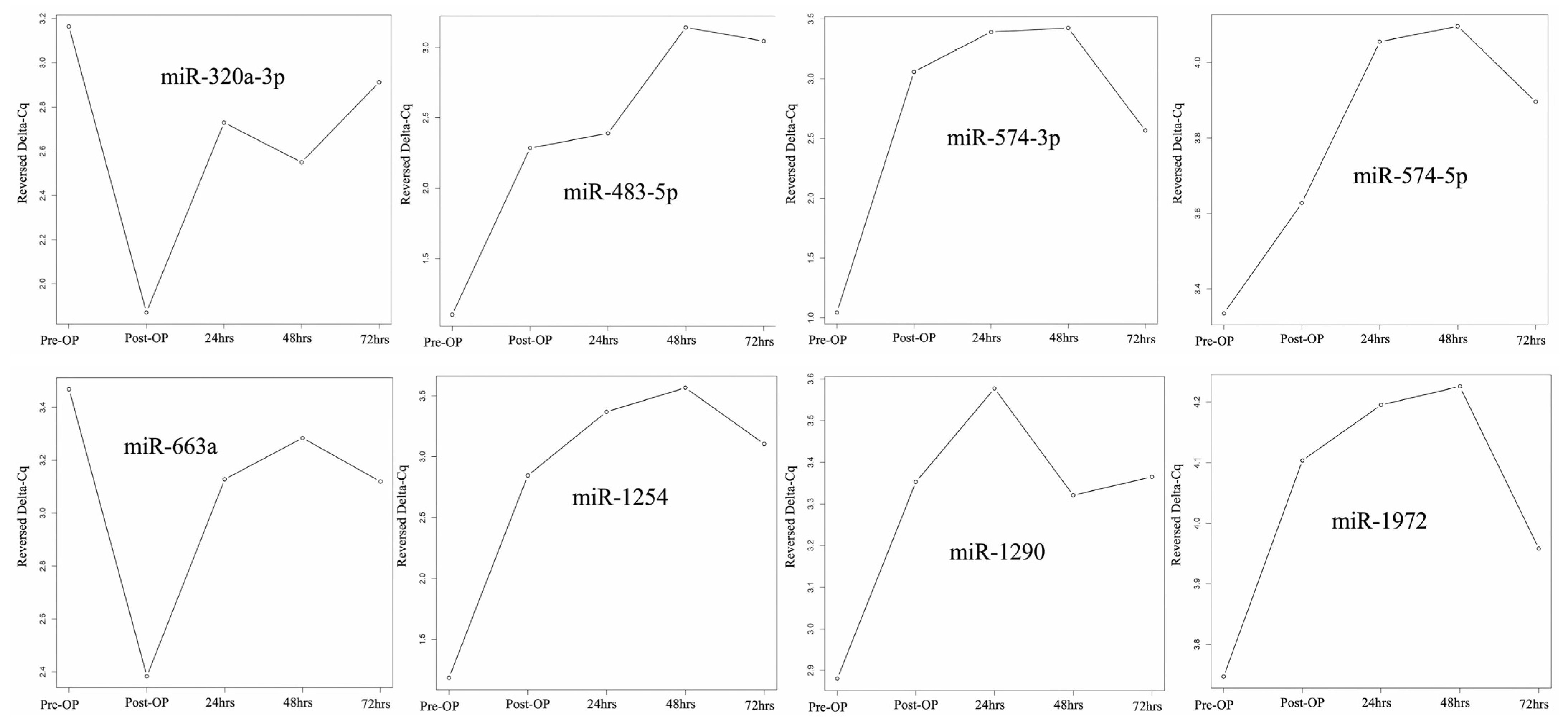
2.2. miRNA Expression before and after HIPEC
2.3. miRNA Expression between CRS with or without HIPEC
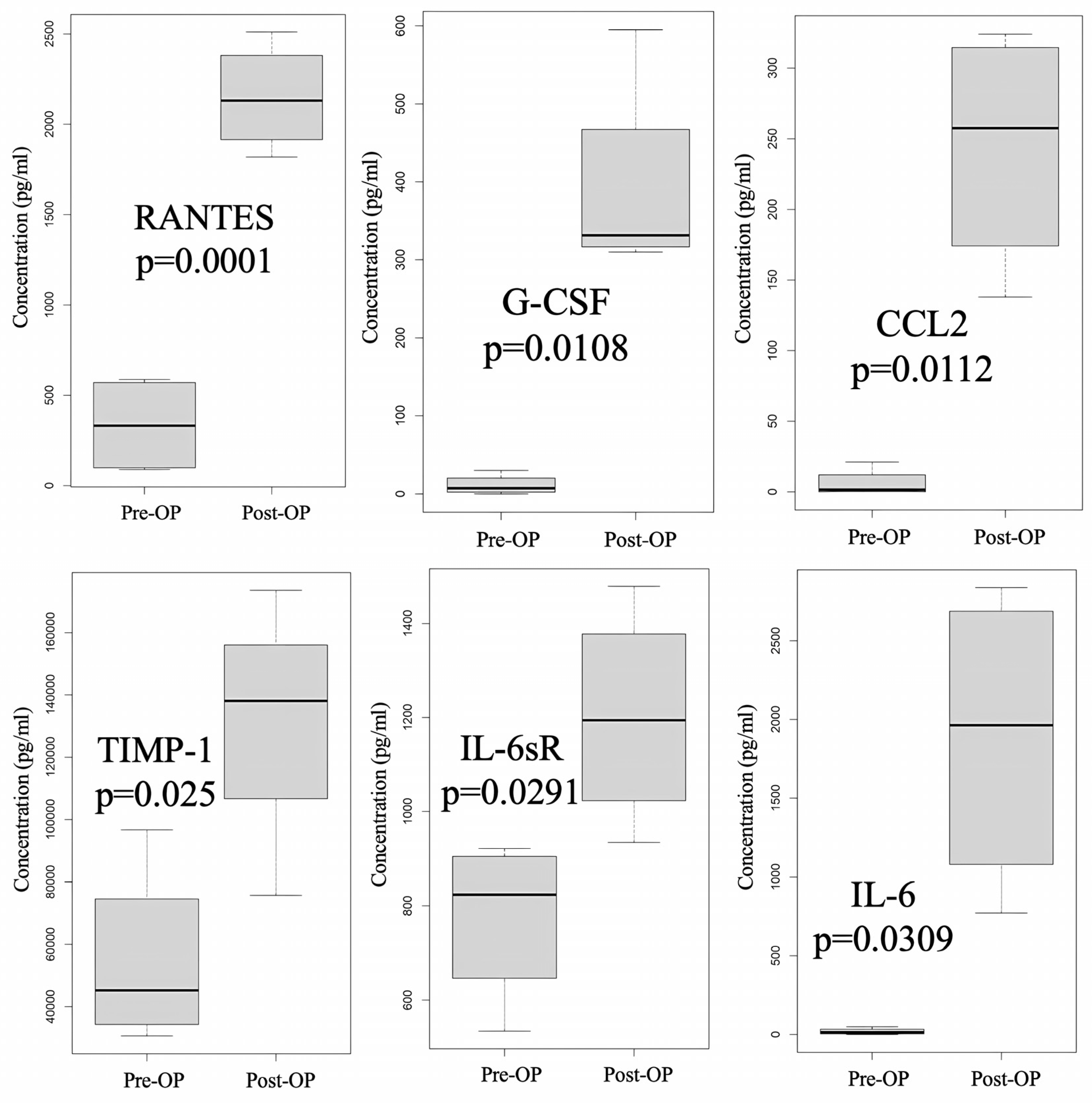
2.4. Cytokine Expression before and after CRS Plus HIPEC
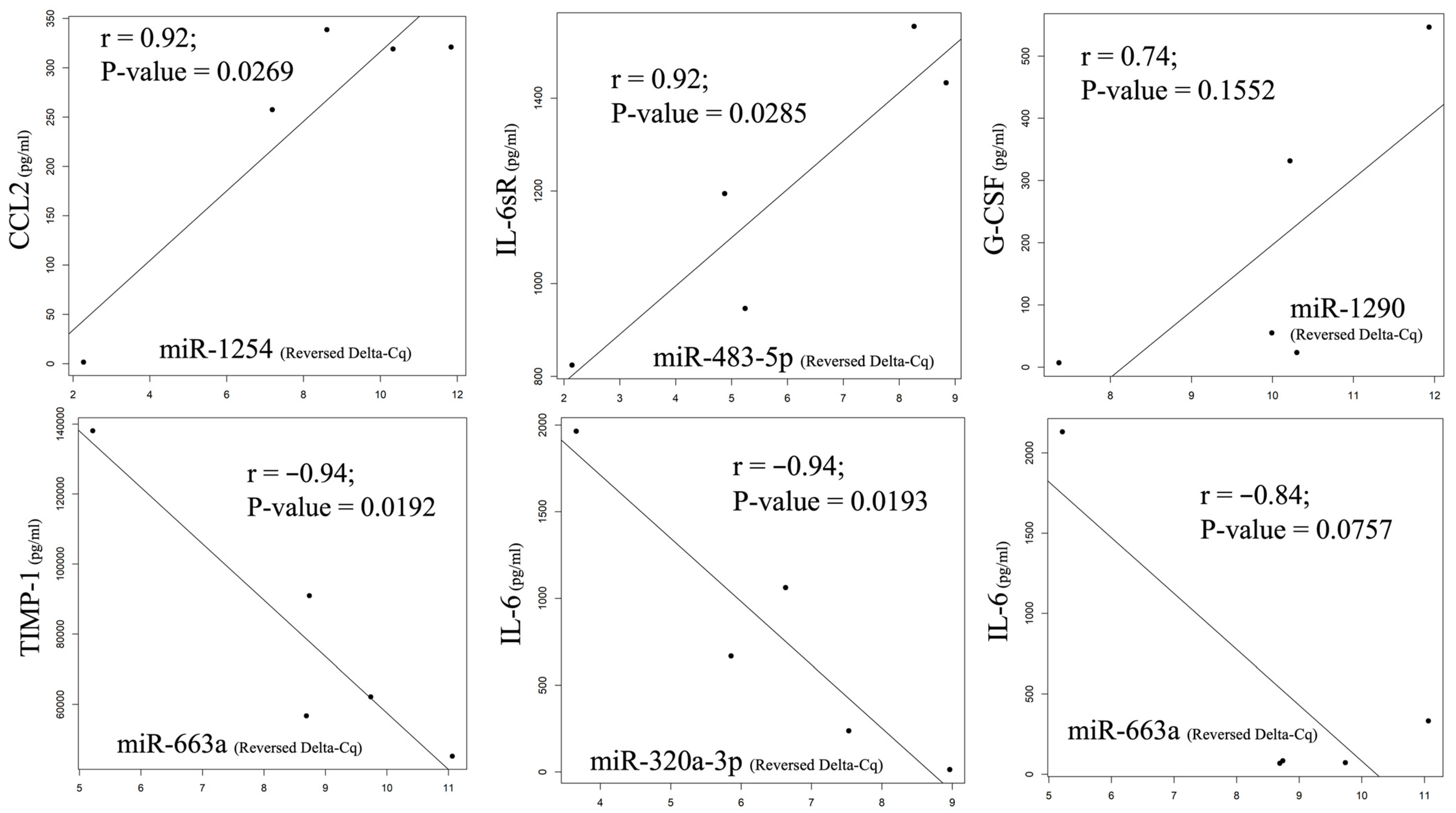
2.5. A Comparison of Changes in Expression Pattern between Cytokine and miRNA before and after HIPEC
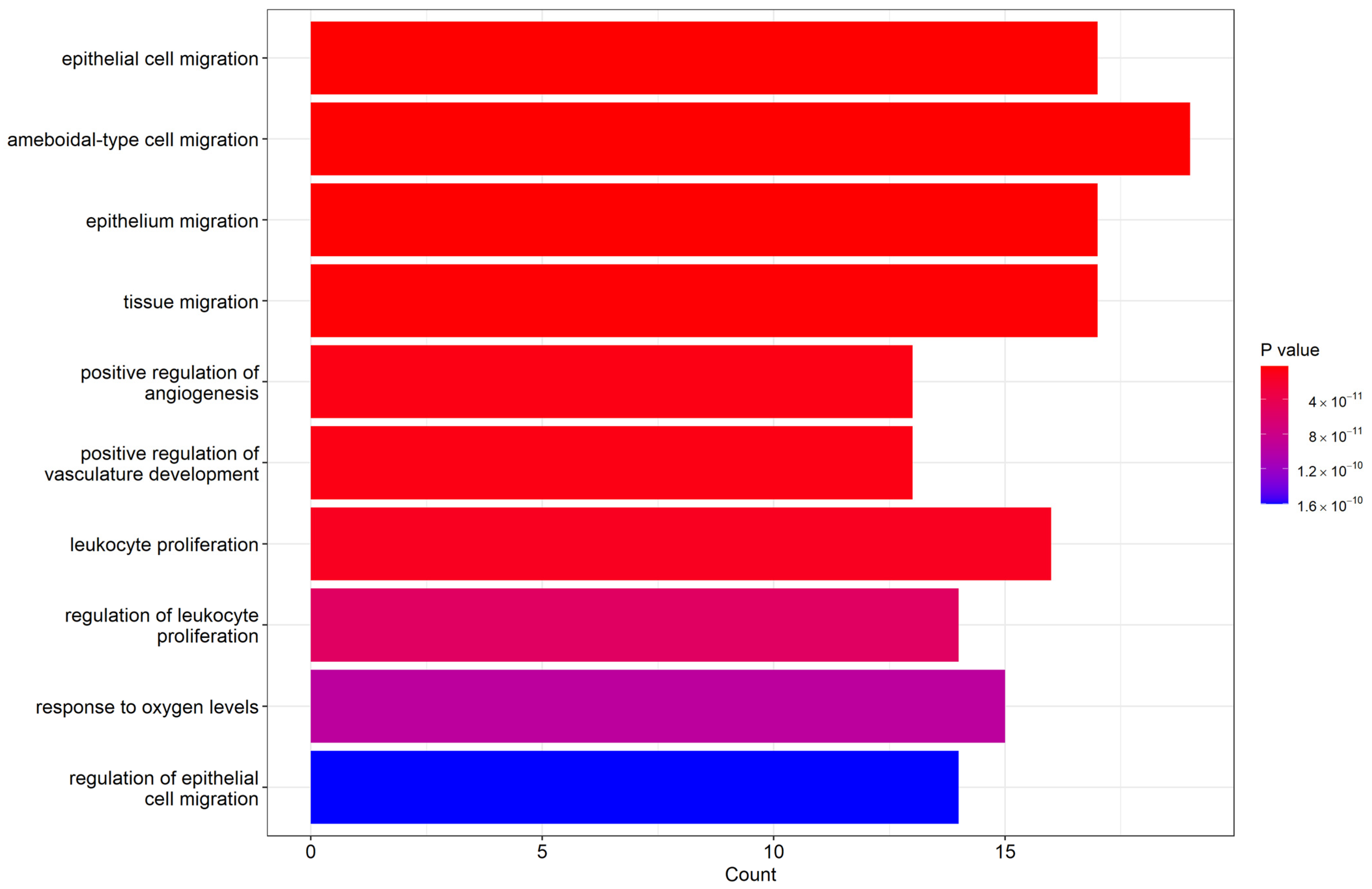
2.6. Biological Process Enrichment Gene Ontology (GO) Terms
3. Discussion
4. Materials and Methods
4.1. Patients Collection
4.2. CRS and HIPEC Treatment
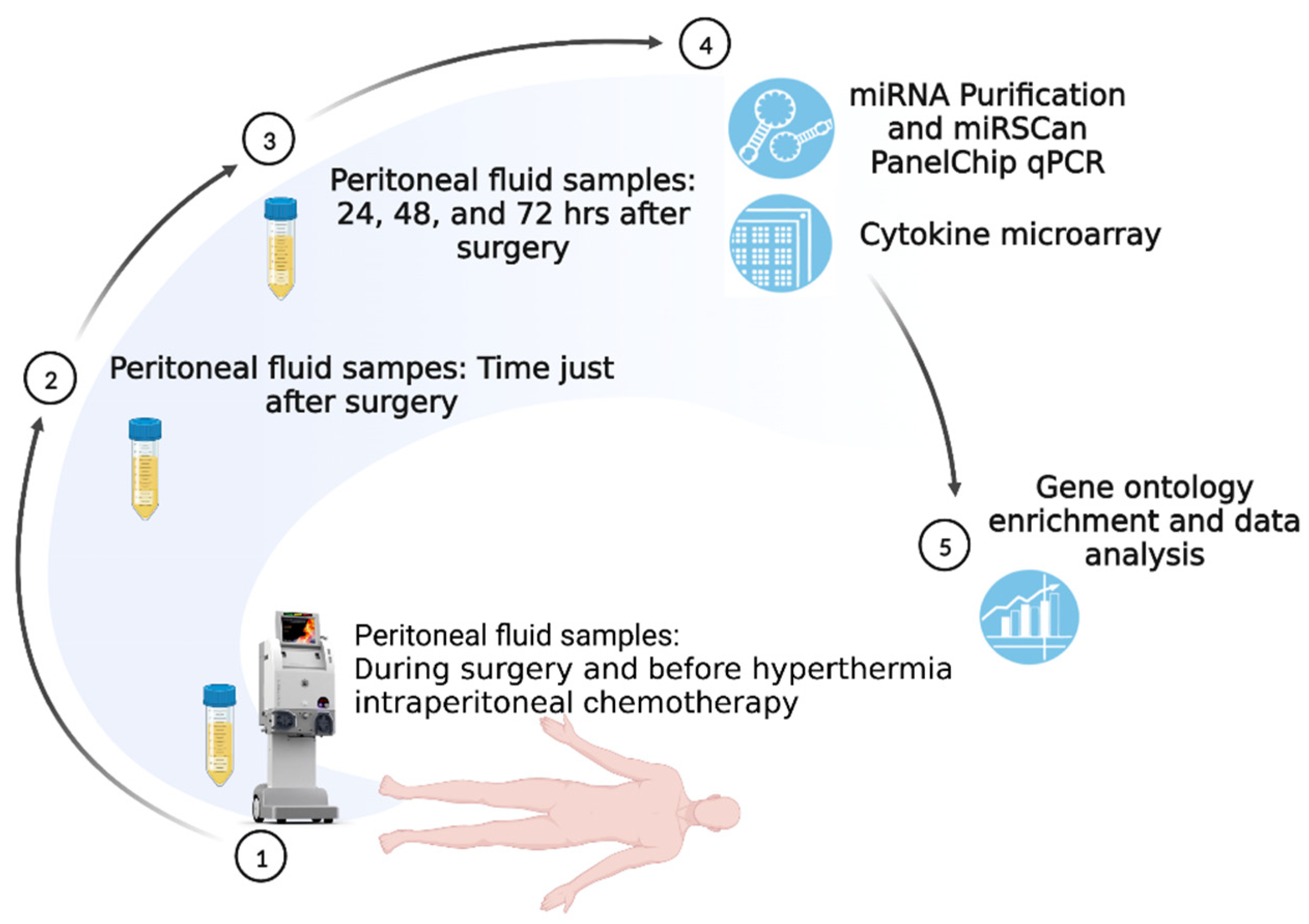
4.3. Samples Collection
4.4. Cytokine Microarray Analysis
4.5. miRNA Analysis
4.6. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Havrilesky, L.J.; Alvarez, A.A.; Sayer, R.A.; Lancaster, J.M.; Soper, J.T.; Berchuck, A.; Clarke-Pearson, D.L.; Rodriguez, G.C.; Carney, M.E. Weekly low-dose carboplatin and paclitaxel in the treatment of recurrent ovarian and peritoneal cancer. Gynecol. Oncol. 2003, 88, 51–57. [Google Scholar] [CrossRef]
- Runyon, B.A. Care of patients with ascites. N. Engl. J. Med. 1994, 330, 337–342. [Google Scholar] [CrossRef]
- Feldman, G.B.; Knapp, R.C.; Order, S.E.; Hellman, S. The role of lymphatic obstruction in the formation of ascites in a murine ovarian carcinoma. Cancer Res. 1972, 32, 1663–1666. [Google Scholar] [PubMed]
- Barton, D.P.; Cai, A.; Wendt, K.; Young, M.; Gamero, A.; De Cesare, S. Angiogenic protein expression in advanced epithelial ovarian cancer. Clin. Cancer Res. 1997, 3, 1579–1586. [Google Scholar]
- Yoneda, J.; Kuniyasu, H.; Crispens, M.A.; Price, J.E.; Bucana, C.D.; Fidler, I.J. Expression of angiogenesis-related genes and progression of human ovarian carcinomas in nude mice. J. Natl. Cancer Inst. 1998, 90, 447–454. [Google Scholar] [CrossRef]
- Loggie, B.W.; Perini, M.; Fleming, R.A.; Russell, G.B.; Geisinger, K. Treatment and prevention of malignant ascites associated with disseminated intraperitoneal malignancies by aggressive combined-modality therapy. Am. Surg. 1997, 63, 137–143. [Google Scholar]
- Ayantunde, A.A.; Parsons, S.L. Pattern and prognostic factors in patients with malignant ascites: A retrospective study. Ann. Oncol. 2007, 18, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Sherer, D.M.; Eliakim, R.; Abulafia, O. The role of angiogenesis in the accumulation of peritoneal fluid in benign conditions and the development of malignant ascites in the female. Gynecol. Obstet. Investig. 2000, 50, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Eitan, R.; Levine, D.A.; Abu-Rustum, N.; Sonoda, Y.; Huh, J.N.; Franklin, C.C.; Stevens, T.A.; Barakat, R.R.; Chi, D.S. The clinical significance of malignant pleural effusions in patients with optimally debulked ovarian carcinoma. Cancer 2005, 103, 1397–1401. [Google Scholar] [CrossRef]
- Sasada, T.; Kimura, M.; Yoshida, Y.; Kanai, M.; Takabayashi, A. CD4+CD25+ regulatory T cells in patients with gastrointestinal malignancies: Possible involvement of regulatory T cells in disease progression. Cancer 2003, 98, 1089–1099. [Google Scholar] [CrossRef]
- Lim, B.; Kim, C.; Kim, J.H.; Kwon, W.S.; Lee, W.S.; Kim, J.M.; Park, J.Y.; Kim, H.S.; Park, K.H.; Kim, T.S.; et al. Genetic alterations and their clinical implications in gastric cancer peritoneal carcinomatosis revealed by whole-exome sequencing of malignant ascites. Oncotarget 2016, 7, 8055–8066. [Google Scholar] [CrossRef] [PubMed]
- Zhan, N.; Dong, W.G.; Wang, J. The clinical significance of vascular endothelial growth factor in malignant ascites. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2016, 37, 3719–3725. [Google Scholar] [CrossRef]
- Wada, J.; Suzuki, H.; Fuchino, R.; Yamasaki, A.; Nagai, S.; Yanai, K.; Koga, K.; Nakamura, M.; Tanaka, M.; Morisaki, T.; et al. The contribution of vascular endothelial growth factor to the induction of regulatory T-cells in malignant effusions. Anticancer. Res. 2009, 29, 881–888. [Google Scholar]
- Simpson-Abelson, M.R.; Loyall, J.L.; Lehman, H.K.; Barnas, J.L.; Minderman, H.; O’Loughlin, K.L.; Wallace, P.K.; George, T.C.; Peng, P.; Kelleher, R.J., Jr.; et al. Human ovarian tumor ascites fluids rapidly and reversibly inhibit T cell receptor-induced NF-κB and NFAT signaling in tumor-associated T cells. Cancer Immun. 2013, 13, 14. [Google Scholar] [PubMed]
- Matte, I.; Lane, D.; Laplante, C.; Rancourt, C.; Piché, A. Profiling of cytokines in human epithelial ovarian cancer ascites. Am. J. Cancer Res. 2012, 2, 566–580. [Google Scholar] [PubMed]
- Kolomeyevskaya, N.; Eng, K.H.; Khan, A.N.; Grzankowski, K.S.; Singel, K.L.; Moysich, K.; Segal, B.H. Cytokine profiling of ascites at primary surgery identifies an interaction of tumor necrosis factor-α and interleukin-6 in predicting reduced progression-free survival in epithelial ovarian cancer. Gynecol. Oncol. 2015, 138, 352–357. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chang, M.C.; Chen, C.A.; Lin, H.W.; Cheng, W.F.; Chien, C.L. Depletion of regulatory T lymphocytes reverses the imbalance between pro- and anti-tumor immunities via enhancing antigen-specific T cell immune responses. PLoS ONE 2012, 7, e47190. [Google Scholar] [CrossRef]
- Mhawech-Fauceglia, P.; Wang, D.; Ali, L.; Lele, S.; Huba, M.A.; Liu, S.; Odunsi, K. Intraepithelial T cells and tumor-associated macrophages in ovarian cancer patients. Cancer Immun. 2013, 13, 1. [Google Scholar]
- Han, H.S.; Yun, J.; Lim, S.N.; Han, J.H.; Lee, K.H.; Kim, S.T.; Kang, M.H.; Son, S.M.; Lee, Y.M.; Choi, S.Y.; et al. Downregulation of cell-free miR-198 as a diagnostic biomarker for lung adenocarcinoma-associated malignant pleural effusion. Int. J. Cancer 2013, 133, 645–652. [Google Scholar] [CrossRef]
- Di Leva, G.; Croce, C.M. Roles of small RNAs in tumor formation. Trends Mol. Med. 2010, 16, 257–267. [Google Scholar] [CrossRef]
- Braicu, O.L.; Budisan, L.; Buiga, R.; Jurj, A.; Achimas-Cadariu, P.; Pop, L.A.; Braicu, C.; Irimie, A.; Berindan-Neagoe, I. miRNA expression profiling in formalin-fixed paraffin-embedded endometriosis and ovarian cancer samples. OncoTargets Ther. 2017, 10, 4225–4238. [Google Scholar] [CrossRef]
- Záveský, L.; Jandáková, E.; Weinberger, V.; Minář, L.; Hanzíková, V.; Dušková, D.; Drábková, L.Z.; Hořínek, A. Ovarian Cancer: Differentially Expressed microRNAs in Tumor Tissue and Cell-Free Ascitic Fluid as Potential Novel Biomarkers. Cancer Investig. 2019, 37, 440–452. [Google Scholar] [CrossRef]
- Zhu, T.; Gao, W.; Chen, X.; Zhang, Y.; Wu, M.; Zhang, P.; Wang, S. A Pilot Study of Circulating MicroRNA-125b as a Diagnostic and Prognostic Biomarker for Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2017, 27, 3–10. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, L.; Bagnoli, M.; Chiodini, P.; Pignata, S.; Mezzanzanica, D. Prognostic Evidence of the miRNA-Based Ovarian Cancer Signature MiROvaR in Independent Datasets. Cancers 2021, 13, 1544. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.; van der Velden, J.; Arts, H.J.; Massuger, L.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Huang, H.J.; Yang, L.Y.; Pan, Y.B.; Huang, K.G.; Lin, C.T.; Chen, M.Y.; Tang, Y.H.; Chang, T.C.; Lai, C.H.; et al. Hyperthermic intraperitoneal chemotherapy for recurrent epithelial ovarian cancer. Biomed. J. 2022, 45, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Berthet, B.; Sugarbaker, T.A.; Chang, D.; Sugarbaker, P.H. Quantitative methodologies for selection of patients with recurrent abdominopelvic sarcoma for treatment. Eur. J. Cancer 1999, 35, 413–419. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Successful management of microscopic residual disease in large bowel cancer. Cancer Chemother. Pharm. 1999, 43, S15–S25. [Google Scholar] [CrossRef] [PubMed]
- Rådestad, E.; Klynning, C.; Stikvoort, A.; Mogensen, O.; Nava, S.; Magalhaes, I.; Uhlin, M. Immune profiling and identification of prognostic immune-related risk factors in human ovarian cancer. Oncoimmunology 2019, 8, e1535730. [Google Scholar] [CrossRef]
- Davidson, B.; Espina, V.; Steinberg, S.M.; Flørenes, V.A.; Liotta, L.A.; Kristensen, G.B.; Tropé, C.G.; Berner, A.; Kohn, E.C. Proteomic analysis of malignant ovarian cancer effusions as a tool for biologic and prognostic profiling. Clin. Cancer Res. 2006, 12, 791–799. [Google Scholar] [CrossRef]
- van Jaarsveld, M.T.; Helleman, J.; Berns, E.M.; Wiemer, E.A. MicroRNAs in ovarian cancer biology and therapy resistance. Int. J. Biochem. Cell Biol. 2010, 42, 1282–1290. [Google Scholar] [CrossRef]
- Iorio, M.V.; Croce, C.M. MicroRNA dysregulation in cancer: Diagnostics, monitoring and therapeutics. A comprehensive review. EMBO Mol. Med. 2012, 4, 143–159. [Google Scholar] [CrossRef]
- Vidigal, J.A.; Ventura, A. The biological functions of miRNAs: Lessons from in vivo studies. Trends Cell Biol. 2015, 25, 137–147. [Google Scholar] [CrossRef]
- Rupaimoole, R.; Slack, F.J. MicroRNA therapeutics: Towards a new era for the management of cancer and other diseases. Nat. Rev. Drug. Discov. 2017, 16, 203–222. [Google Scholar] [CrossRef]
- Jiang, Y.; Shi, Y.; Lyu, T.; Liu, H.; Shen, L.; Zhou, T.; Feng, W. Identification and Functional Validation of Differentially Expressed microRNAs in Ascites-Derived Ovarian Cancer Cells Compared with Primary Tumour Tissue. Cancer Manag. Res. 2021, 13, 6585–6597. [Google Scholar] [CrossRef] [PubMed]
- Záveský, L.; Jandáková, E.; Weinberger, V.; Minář, L.; Hanzíková, V.; Dušková, D.; Drábková, L.Z.; Svobodová, I.; Hořínek, A. Ascites-Derived Extracellular microRNAs as Potential Biomarkers for Ovarian Cancer. Reprod. Sci. (Thousand oaks Calif.) 2019, 26, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.S.; Zou, Y.; Dai, D.Q. MicroRNA-320a suppresses tumor progression by targeting PBX3 in gastric cancer and is downregulated by DNA methylation. World J. Gastrointest. Oncol. 2019, 11, 842–856. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, A.; Sharma, U.; Barwal, T.S.; Seam, R.K.; Gupta, M.; Rana, M.K.; Vasquez, K.M.; Jain, A. Circulating miR-320a Acts as a Tumor Suppressor and Prognostic Factor in Non-small Cell Lung Cancer. Front. Oncol. 2021, 11, 645475. [Google Scholar] [CrossRef]
- Peng, J.; Wang, R.; Sun, W.; Huang, M.; Wang, R.; Li, Y.; Wang, P.; Sun, G.; Xie, S. Delivery of miR-320a-3p by gold nanoparticles combined with photothermal therapy for directly targeting Sp1 in lung cancer. Biomater. Sci. 2021, 9, 6528–6541. [Google Scholar] [CrossRef]
- Shapira, I.; Oswald, M.; Lovecchio, J.; Khalili, H.; Menzin, A.; Whyte, J.; Dos Santos, L.; Liang, S.; Bhuiya, T.; Keogh, M.; et al. Circulating biomarkers for detection of ovarian cancer and predicting cancer outcomes. Br. J. Cancer 2014, 110, 976–983. [Google Scholar] [CrossRef]
- Guo, J.; Pan, H. Long Noncoding RNA LINC01125 Enhances Cisplatin Sensitivity of Ovarian Cancer via miR-1972. Med. Sci. Monit. 2019, 25, 9844–9854. [Google Scholar] [CrossRef]
- Jiang, M.; Shi, L.; Yang, C.; Ge, Y.; Lin, L.; Fan, H.; He, Y.; Zhang, D.; Miao, Y.; Yang, L. miR-1254 inhibits cell proliferation, migration, and invasion by down-regulating Smurf1 in gastric cancer. Cell Death Dis. 2019, 10, 32. [Google Scholar] [CrossRef]
- Li, X.; Kong, S.; Cao, Y. miR-1254 inhibits progression of glioma in vivo and in vitro by targeting CSF-1. J. Cell Mol. Med. 2020, 24, 3128–3138. [Google Scholar] [CrossRef]
- Chen, L.; Xia, J.S.; Wu, J.H.; Chen, Y.G.; Qiu, C.J. Quercetin suppresses cell survival and invasion in oral squamous cell carcinoma via the miR-1254/CD36 cascade in vitro. Hum. Exp. Toxicol. 2021, 40, 1413–1421. [Google Scholar] [CrossRef]
- Zhu, D.; Hao, Q.; Qian, M.; Hu, Y.; Wu, F. LncRNA ABHD11-AS1 Participates in the Progression of Cervical Carcinoma by Targeting miR-1254 and Is the Key to the Diagnosis and Treatment of Cervical Carcinoma in the Future. J. Healthc. Eng. 2022, 2022, 8387458. [Google Scholar] [CrossRef]
- Lu, X.; Yang, C.; Hu, Y.; Xu, J.; Shi, C.; Rao, J.; Yu, W.; Cheng, F. Upregulation of miR-1254 promotes Hepatocellular Carcinoma Cell Proliferation, Migration, and Invasion via Inactivation of the Hippo-YAP signaling pathway by decreasing PAX5. J. Cancer 2021, 12, 771–789. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Xu, Y.; Yang, C.; Chen, Z.; Jia, C.; Chen, J.; Zhang, Y.; Lai, P.; Fan, X.; Zhou, X.; et al. miR-483-5p promotes invasion and metastasis of lung adenocarcinoma by targeting RhoGDI1 and ALCAM. Cancer Res. 2014, 74, 3031–3042. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Xu, G.; Sun, H.; Lin, T.; Xu, S.; Zhao, Y. Inhibition of miR-483-5p improves the proliferation, invasion and inflammatory response of triple-negative breast cancer cells by targeting SOCS3. Exp. Med. 2021, 22, 1047. [Google Scholar] [CrossRef] [PubMed]
- Chiyomaru, T.; Yamamura, S.; Fukuhara, S.; Hidaka, H.; Majid, S.; Saini, S.; Arora, S.; Deng, G.; Shahryari, V.; Chang, I.; et al. Genistein up-regulates tumor suppressor microRNA-574-3p in prostate cancer. PLoS ONE 2013, 8, e58929. [Google Scholar] [CrossRef]
- Tong, R.; Zhang, J.; Wang, C.; Li, Q.; Wang, L.; Ju, M. Inhibition of miR-574-5p suppresses cell growth and metastasis and enhances chemosensitivity by targeting RNA binding protein QKI in cervical cancer cells. Naunyn Schmiedebergs Arch. Pharm. 2020, 393, 951–966. [Google Scholar] [CrossRef] [PubMed]
- Michaille, J.J.; Piurowski, V.; Rigot, B.; Kelani, H.; Fortman, E.C.; Tili, E. MiR-663, a MicroRNA Linked with Inflammation and Cancer That Is under the Influence of Resveratrol. Medicines 2018, 5, 74. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Hu, H.; Zhou, Z.; Sun, L.; Peng, L.; Yu, L.; Sun, L.; Liu, J.; Yang, Z.; Ran, Y. Tumor-suppressive mir-663 gene induces mitotic catastrophe growth arrest in human gastric cancer cells. Oncol. Rep. 2010, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.W.; Kim, E.Y.; Jeon, D.; Liu, J.L.; Kim, H.S.; Choi, J.W.; Ahn, W.S. Differential microRNA expression signatures and cell type-specific association with Taxol resistance in ovarian cancer cells. Drug. Des. Devel 2014, 8, 293–314. [Google Scholar] [CrossRef]
- Xie, H.H.; Huan, W.T.; Han, J.Q.; Ren, W.R.; Yang, L.H. MicroRNA-663 facilitates the growth, migration and invasion of ovarian cancer cell by inhibiting TUSC2. Biol. Res. 2019, 52, 18. [Google Scholar] [CrossRef]
- Wertel, I.; Tarkowski, R.; Bednarek, W.; Kotarski, J. Relationship between RANTES and dendritic cells in ovarian cancer patients. Front. Biosci. (Elite Ed) 2011, 3, 227–232. [Google Scholar] [CrossRef][Green Version]
- Tsukishiro, S.; Suzumori, N.; Nishikawa, H.; Arakawa, A.; Suzumori, K. Elevated serum RANTES levels in patients with ovarian cancer correlate with the extent of the disorder. Gynecol. Oncol. 2006, 102, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Azenshtein, E.; Luboshits, G.; Shina, S.; Neumark, E.; Shahbazian, D.; Weil, M.; Wigler, N.; Keydar, I.; Ben-Baruch, A. The CC chemokine RANTES in breast carcinoma progression: Regulation of expression and potential mechanisms of promalignant activity. Cancer Res. 2002, 62, 1093–1102. [Google Scholar]
- Gallo, M.; Frezzetti, D.; Roma, C.; Chicchinelli, N.; Barbieri, A.; Arra, C.; Scognamiglio, G.; Botti, G.; De Luca, A.; Normanno, N. RANTES and IL-6 cooperate in inducing a more aggressive phenotype in breast cancer cells. Oncotarget 2018, 9, 17543–17553. [Google Scholar] [CrossRef]
- Kumar, J.; Fraser, F.W.; Riley, C.; Ahmed, N.; McCulloch, D.R.; Ward, A.C. Granulocyte colony-stimulating factor receptor signalling via Janus kinase 2/signal transducer and activator of transcription 3 in ovarian cancer. Br. J. Cancer 2014, 110, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Jackson, H.W.; Defamie, V.; Waterhouse, P.; Khokha, R. TIMPs: Versatile extracellular regulators in cancer. Nat. Rev. Cancer 2017, 17, 38–53. [Google Scholar] [CrossRef]
- Gong, Y.; Scott, E.; Lu, R.; Xu, Y.; Oh, W.K.; Yu, Q. TIMP-1 promotes accumulation of cancer associated fibroblasts and cancer progression. PLoS ONE 2013, 8, e77366. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Fan, X.; Hao, M.; Wang, J.; Zhou, X.; Sun, X. Higher levels of TIMP-1 expression are associated with a poor prognosis in triple-negative breast cancer. Mol. Cancer 2016, 15, 30. [Google Scholar] [CrossRef]
- Steffensen, K.D.; Waldstrøm, M.; Christensen, R.K.; Bartels, A.; Brünner, N.; Jakobsen, A. Lack of relationship between TIMP-1 tumour cell immunoreactivity, treatment efficacy and prognosis in patients with advanced epithelial ovarian cancer. BMC Cancer 2010, 10, 185. [Google Scholar] [CrossRef]
- Sun, C.; Li, X.; Guo, E.; Li, N.; Zhou, B.; Lu, H.; Huang, J.; Xia, M.; Shan, W.; Wang, B.; et al. MCP-1/CCR-2 axis in adipocytes and cancer cell respectively facilitates ovarian cancer peritoneal metastasis. Oncogene 2020, 39, 1681–1695. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Soeda, S.; Kiko, Y.; Suzuki, O.; Hashimoto, Y.; Watanabe, T.; Nishiyama, H.; Tasaki, K.; Hojo, H.; Abe, M.; et al. MCP-1 promotes invasion and adhesion of human ovarian cancer cells. Anticancer. Res. 2013, 33, 4785–4790. [Google Scholar] [PubMed]
- Geller, M.A.; Bui-Nguyen, T.M.; Rogers, L.M.; Ramakrishnan, S. Chemotherapy induces macrophage chemoattractant protein-1 production in ovarian cancer. Int. J. Gynecol. Cancer 2010, 20, 918–925. [Google Scholar] [CrossRef]
- Andrews, B.; Shariat, S.F.; Kim, J.H.; Wheeler, T.M.; Slawin, K.M.; Lerner, S.P. Preoperative plasma levels of interleukin-6 and its soluble receptor predict disease recurrence and survival of patients with bladder cancer. J. Urol. 2002, 167, 1475–1481. [Google Scholar] [CrossRef]
- Schuettfort, V.M.; Pradere, B.; Trinh, Q.D.; D’Andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Sari Motlagh, R.; Rink, M.; et al. Impact of preoperative plasma levels of interleukin 6 and interleukin 6 soluble receptor on disease outcomes after radical cystectomy for bladder cancer. Cancer Immunol. Immunother. CII 2022, 71, 85–95. [Google Scholar] [CrossRef]
- Chen, C.; Wang, Y.; Yang, S.; Li, H.; Zhao, G.; Wang, F.; Yang, L.; Wang, D.W. MiR-320a contributes to atherogenesis by augmenting multiple risk factors and down-regulating SRF. J. Cell Mol. Med. 2015, 19, 970–985. [Google Scholar] [CrossRef]
- Wang, W.; Gao, J.; Wang, F. MiR-663a/MiR-423-5p are involved in the pathogenesis of lupus nephritis via modulating the activation of NF-κB by targeting TNIP2. Am. J. Transl. Res. 2017, 9, 3796–3803. [Google Scholar] [PubMed]
- RayBiotech. Homepage of RayBiotech Company. Available online: https://www.raybiotech.com/ (accessed on 11 September 2021).
- Fraley, E.; LeMaster, C.; Geanes, E.; Banerjee, D.; Khanal, S.; Grundberg, E.; Selvarangan, R.; Bradley, T. Humoral immune responses during SARS-CoV-2 mRNA vaccine administration in seropositive and seronegative individuals. BMC Med. 2021, 19, 169. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | BMI | Cancer Stage | Cell Type | PCI Score | CC Score | NAC | HIPEC Regimen | PD | Current Status |
|---|---|---|---|---|---|---|---|---|---|---|
| A | 66 | 23.98 | 4B | HGSC | 11 | 0 | yes | Carbo + Taxol | Yes * | Alive with disease |
| B | 49 | 22.84 | 3C2 | HGSC | 6 | 0 | yes | Carbo + Taxol | nil | NED |
| C | 56 | 22.09 | 3C2 | HGSC | 16 | 0 | yes | Carbo + Taxol | nil | NED |
| D | 60 | 29.61 | 3C2 | HGSC | 13 | 1 | nil | Carbo + Taxol | nil | NED |
| E | 58 | 21.60 | 3C2 | LGSC | 5 | 0 | nil | Carbo + Taxol | nil | NED |
| F | 57 | 16.63 | 4A | HGSC | 6 | 0 | nil | nil | nil | NED |
| Pre-HIPEC | Immediate Post-HIPEC | ΔΔCq | |
|---|---|---|---|
| hsa-miR-1254 | 2.27 | 7.19 | 4.91 |
| hsa-miR-1290 | 7.36 | 10.22 | 2.85 |
| hsa-miR-1972 | 13.43 | 17.19 | 3.76 |
| hsa-miR-320a-3p | 8.96 | 3.66 | −5.31 |
| hsa-miR-483-5p | 2.14 | 4.88 | 2.73 |
| hsa-miR-574-3p | 2.06 | 8.32 | 6.26 |
| hsa-miR-574-5p | 10.09 | 12.36 | 2.27 |
| hsa-miR-663a | 11.06 | 5.22 | −5.85 |
| CRS + HIPEC (Patient E) | CRS Alone (Patient F) | ΔΔCq | |
|---|---|---|---|
| hsa-miR-1290 | 10.30 | 7.92 | 2.39 |
| hsa-miR-596 | 10.89 | 8.60 | 2.30 |
| hsa-miR-1972 | 15.55 | 16.55 | −1.01 |
| hsa-miR-191-5p | 7.90 | 2.77 | 5.13 |
| hsa-miR-423-5p | 6.15 | 10.30 | −4.15 |
| hsa-miR-320a-3p | 7.53 | 5.78 | 1.75 |
| hsa-miR-885-5p | 7.59 | 1.07 | 6.52 |
| hsa-miR-30b-5p | 2.35 | 11.67 | −9.32 |
| hsa-miR-1228-5p | 9.29 | 7.73 | 1.57 |
| hsa-miR-589-5p | 9.31 | 4.78 | 4.53 |
| hsa-miR-202-3p | 6.53 | 4.06 | 2.47 |
| hsa-miR-151a-3p | 9.31 | 10.51 | −1.20 |
| hsa-miR-378a-5p | 5.97 | 8.24 | −2.27 |
| GO | Description | Gene |
|---|---|---|
| GO:0010631 | epithelial cell migration | SRF/MECP2/RAC1/HMGB1/ITGB3/NRP1/PTEN/KITLG/ANGPT2/FGF1/PIK3CA/TGFBR2/AKT3/IL4/KLF4/TGFB1/PIK3CD |
| GO:0001667 | ameboidal-type cell migration | SRF/MECP2/RAC1/ACVR1B/HMGB1/AQP1/ITGB3/NRP1/PTEN/KITLG/ANGPT2/FGF1/PIK3CA/TGFBR2/AKT3/IL4/KLF4/TGFB1/PIK3CD |
| GO:0090132 | epithelium migration | SRF/MECP2/RAC1/HMGB1/ITGB3/NRP1/PTEN/KITLG/ANGPT2/FGF1/PIK3CA/TGFBR2/AKT3/IL4/KLF4/TGFB1/PIK3CD |
| GO:0090130 | tissue migration | SRF/MECP2/RAC1/HMGB1/ITGB3/NRP1/PTEN/KITLG/ANGPT2/FGF1/PIK3CA/TGFBR2/AKT3/IL4/KLF4/TGFB1/PIK3CD |
| GO:0045766 | positive regulation of angiogenesis | ADM/HSPB6/AQP1/XBP1/ITGB3/NRP1/MTDH/ANGPT2/FGF1/TGFBR2/AKT3/KLF4/PIK3CD |
| GO:1904018 | positive regulation of vasculature development | ADM/HSPB6/AQP1/XBP1/ITGB3/NRP1/MTDH/ANGPT2/FGF1/TGFBR2/AKT3/KLF4/PIK3CD |
| GO:0070661 | leukocyte proliferation | MAPK3/MAPK1/IGF2/HMGB1/TFRC/BMI1/PTEN/KITLG/CRP/TGFBR2/IL4/CD274/JUNB/CEBPB/TP53/CDKN1A |
| GO:0070663 | regulation of leukocyte proliferation | MAPK3/MAPK1/IGF2/HMGB1/TFRC/BMI1/PTEN/KITLG/CRP/TGFBR2/IL4/CD274/CEBPB/CDKN1A |
| GO:0070482 | response to oxygen levels | SRF/MECP2/EP300/SMAD4/ADM/ND5/TFRC/AQP1/PTEN/ANGPT2/SIRT4/TGFBR2/JUND/SLC7A5/TP53 |
| GO:0010632 | regulation of epithelial cell migration | MECP2/RAC1/HMGB1/ITGB3/NRP1/PTEN/ANGPT2/FGF1/TGFBR2/AKT3/IL4/KLF4/TGFB1/PIK3CD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.-C.; Chang, T.-C.; Chou, H.-H.; Cheng, M.-H.; Hong, J.-J.; Hsieh, Y.-S.; Cheng, C.-M. Peritoneal Fluid Analysis of Advanced Ovarian Cancers after Hyperthermic Intraperitoneal Chemotherapy. Int. J. Mol. Sci. 2023, 24, 9748. https://doi.org/10.3390/ijms24119748
Chen W-C, Chang T-C, Chou H-H, Cheng M-H, Hong J-J, Hsieh Y-S, Cheng C-M. Peritoneal Fluid Analysis of Advanced Ovarian Cancers after Hyperthermic Intraperitoneal Chemotherapy. International Journal of Molecular Sciences. 2023; 24(11):9748. https://doi.org/10.3390/ijms24119748
Chicago/Turabian StyleChen, Wei-Chun, Ting-Chang Chang, Hung-Hsueh Chou, Mei-Hsiu Cheng, Jun-Jie Hong, Yi-Shan Hsieh, and Chao-Min Cheng. 2023. "Peritoneal Fluid Analysis of Advanced Ovarian Cancers after Hyperthermic Intraperitoneal Chemotherapy" International Journal of Molecular Sciences 24, no. 11: 9748. https://doi.org/10.3390/ijms24119748
APA StyleChen, W.-C., Chang, T.-C., Chou, H.-H., Cheng, M.-H., Hong, J.-J., Hsieh, Y.-S., & Cheng, C.-M. (2023). Peritoneal Fluid Analysis of Advanced Ovarian Cancers after Hyperthermic Intraperitoneal Chemotherapy. International Journal of Molecular Sciences, 24(11), 9748. https://doi.org/10.3390/ijms24119748