

Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease

Abstract
1. Introduction
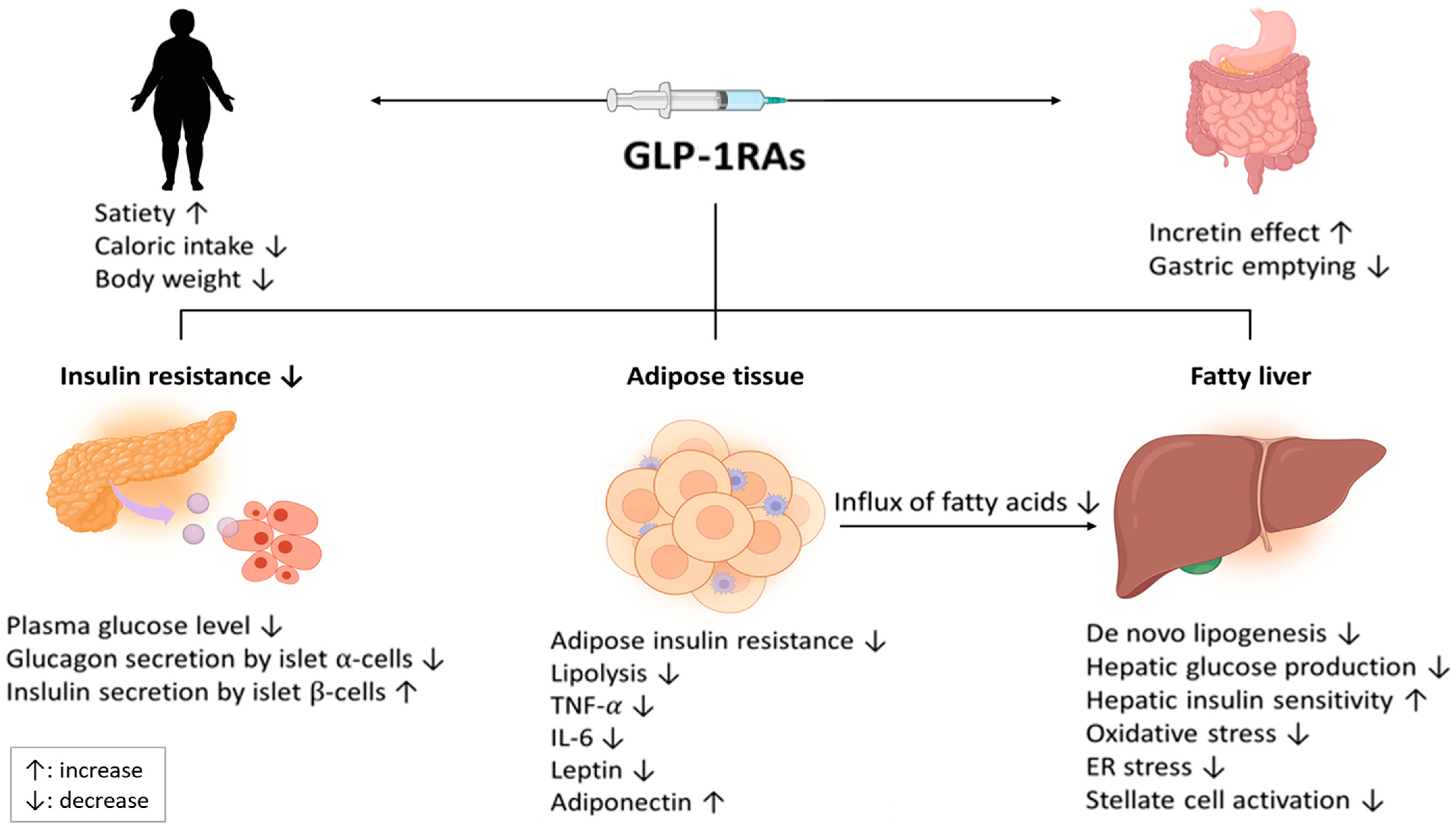
2. Treatment Mechanisms of GLP-1RAs on NAFLD
3. Beneficial Effects of GLP-1RAs in Patients with NAFLD
3.1. Liraglutide
3.2. Semaglutide
3.3. Exenatide
3.4. Dulaglutide
4. Meta-Analysis
5. Dual GIP and GLP-1 Receptor Agonist
6. Dual GLP-1 and Glucagon Receptor Agonist
7. The Effect of GLP-1RA Treatment in the Presence of T2DM
8. Ongoing Clinical Trials
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| NAFLD | nonalcoholic fatty liver disease |
| NASH | nonalcoholic steatohepatitis |
| GLP-1RA | glucagon-like peptide-1 receptor agonist |
| T2DM | type 2 diabetes mellitus |
| GIP | glucose-dependent insulinotropic peptide |
| LFC | liver fat content |
| SREBP | sterol regulatory element-binding transcription factor |
| SCD | stearoyl-CoA desaturase |
| PPAR | peroxisome proliferator-activated receptor |
| ALT | alanine aminotransferase |
| AMPK | adenosine monophosphate activated protein kinase |
| ChREBP | carbohydrate-responsive element-binding protein |
| VLDL | very low-density lipoprotein |
| SGLT2 | sodium-glucose co-transporter 2 |
| DPP-4 | dipeptidyl peptidase-4 |
| RR | relative risk |
| BMI | body mass index |
| GGT | γ-glutamyl transferase |
| LDL | low-density lipoprotein |
| MRI | magnetic resonance imaging |
| RCT | randomized controlled trial |
| PDFF | proton density fat fraction |
| LSM | lifestyle modification |
| MRE | magnetic resonance elastography |
| VAT | visceral adipose tissue |
| SAT | subcutaneous adipose tissue |
| OR | odds ratio |
| MRS | magnetic resonance spectroscopy |
| FIB-4 | fibrosis-4 index |
| TNF | tumor necrosis factor |
| ER | endoplasmic reticulum |
| NEFA | nonesterified fatty acids |
| FGF | fibroblast growth factor |
| FFA | fibroblast growth factor |
| LPS | lipopolysaccharide |
| ROS | reactive oxygen species |
| DNL | de novo lipogenesis |
| AE | adverse event |
| SAE | serious adverse event |
| CI | confidence interval |
| CT | computed tomography |
| VCTE | vibration-controlled transient elastography |
| LD | lipid droplet |
References
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of Liver Disease: 2023 Update. J. Hepatol. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Lee, H.W.; Yoo, J.J.; Cho, Y.; Kim, S.U.; Lee, T.H.; Jang, B.K.; Kim, S.G.; Ahn, S.B.; Kim, H.; et al. KASL clinical practice guidelines: Management of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2021, 27, 363–401. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef] [PubMed]
- Bugianesi, E.; Gentilcore, E.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; David, E.; Rizzetto, M.; Marchesini, G. A randomized controlled trial of metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2005, 100, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Uygun, A.; Kadayifci, A.; Isik, A.T.; Ozgurtas, T.; Deveci, S.; Tuzun, A.; Yesilova, Z.; Gulsen, M.; Dagalp, K. Metformin in the treatment of patients with non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2004, 19, 537–544. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef]
- American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of medical care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. S1), S111–S124. [Google Scholar] [CrossRef]
- Müller, T.D.; Finan, B.; Bloom, S.R.; D’Alessio, D.; Drucker, D.J.; Flatt, P.R.; Fritsche, A.; Gribble, F.; Grill, H.J.; Habener, J.F.; et al. Glucagon-like peptide 1 (GLP-1). Mol. Metab. 2019, 30, 72–130. [Google Scholar] [CrossRef]
- Meier, J.J. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2012, 8, 728–742. [Google Scholar] [CrossRef]
- Nauck, M.A.; Holst, J.J.; Willms, B.; Schmiegel, W. Glucagon-like peptide 1 (GLP-1) as a new therapeutic approach for type 2-diabetes. Exp. Clin. Endocrinol. Diabetes 1997, 105, 187–195. [Google Scholar] [CrossRef]
- Wettergren, A. Glucagon-like peptide-1. Gastrointestinal function and possible mechanism of action. Dan. Med. Bull. 2001, 48, 19–28. [Google Scholar] [PubMed]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; LEAN Trial Team; Abouda, G.; et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.S.; Harrison, S.A.; NN9931-4296 Investigators. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, S.; Zvibel, I.; Shnell, M.; Shlomai, A.; Chepurko, E.; Halpern, Z.; Barzilai, N.; Oren, R.; Fishman, S. Glucagon-like peptide-1 reduces hepatic lipogenesis via activation of AMP-activated protein kinase. J. Hepatol. 2011, 54, 1214–1223. [Google Scholar] [CrossRef]
- Gupta, N.A.; Mells, J.; Dunham, R.M.; Grakoui, A.; Handy, J.; Saxena, N.K.; Anania, F.A. Glucagon-like peptide-1 receptor is present on human hepatocytes and has a direct role in decreasing hepatic steatosis in vitro by modulating elements of the insulin signaling pathway. Hepatology 2010, 51, 1584–1592. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Hull, D.; Guo, K.; Barton, D.; Hazlehurst, J.M.; Gathercole, L.L.; Nasiri, M.; Yu, J.; Gough, S.C.; Newsome, P.N.; et al. Glucagon-like peptide 1 decreases lipotoxicity in non-alcoholic steatohepatitis. J. Hepatol. 2016, 64, 399–408. [Google Scholar] [CrossRef]
- Seghieri, M.; Christensen, A.S.; Andersen, A.; Solini, A.; Knop, F.K.; Vilsbøll, T. Future Perspectives on GLP-1 Receptor Agonists and GLP-1/glucagon Receptor Co-agonists in the Treatment of NAFLD. Front. Endocrinol. (Lausanne) 2018, 9, 649. [Google Scholar] [CrossRef]
- Hartman, M.L.; Sanyal, A.J.; Loomba, R.; Wilson, J.M.; Nikooienejad, A.; Bray, R.; Karanikas, C.A.; Duffin, K.L.; Robins, D.A.; Haupt, A. Effects of novel dual GIP and GLP-1 receptor agonist tirzepatide on biomarkers of nonalcoholic steatohepatitis in patients with Type 2 diabetes. Diabetes Care 2020, 43, 1352–1355. [Google Scholar] [CrossRef]
- Gastaldelli, A.; Cusi, K.; Fernández Landó, L.; Bray, R.; Brouwers, B.; Rodríguez, Á. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): A substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol. 2022, 10, 393–406. [Google Scholar] [CrossRef]
- Rajeev, S.P.; Wilding, J. GLP-1 as a target for therapeutic intervention. Curr. Opin. Pharmacol. 2016, 31, 44–49. [Google Scholar] [CrossRef]
- Mells, J.E.; Fu, P.P.; Sharma, S.; Olson, D.; Cheng, L.; Handy, J.A.; Saxena, N.K.; Sorescu, D.; Anania, F.A. GLP-1 analog, liraglutide, ameliorates hepatic steatosis and cardiac hypertrophy in C57BL/6J mice fed a Western diet. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G225–G235. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yang, M.; Ren, H.; Hu, H.; Boden, G.; Li, L.; Yang, G. GLP-1 analogue prevents NAFLD in ApoE KO mice with diet and Acrp30 knockdown by inhibiting c-JNK. Liver Int. 2013, 33, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Aldawsari, M.; Almadani, F.A.; Almuhammadi, N.; Algabsani, S.; Alamro, Y.; Aldhwayan, M. The efficacy of GLP-1 analogues on appetite parameters, gastric emptying, food preference and taste among adults with obesity: Systematic review of randomized controlled trials. Diabetes Metab. Syndr. Obes. 2023, 16, 575–595. [Google Scholar] [CrossRef] [PubMed]
- Trevaskis, J.L.; Griffin, P.S.; Wittmer, C.; Neuschwander-Tetri, B.A.; Brunt, E.M.; Dolman, C.S.; Erickson, M.R.; Napora, J.; Parkes, D.G.; Roth, J.D. Glucagon-like peptide-1 receptor agonism improves metabolic, biochemical, and histopathological indices of nonalcoholic steatohepatitis in mice. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G762–G772. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Saxena, N.K.; Lin, S.; Gupta, N.A.; Anania, F.A. Exendin-4, a glucagon-like protein-1 (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice. Hepatology 2006, 43, 173–181. [Google Scholar] [CrossRef]
- Sharma, S.; Mells, J.E.; Fu, P.P.; Saxena, N.K.; Anania, F.A. GLP-1 analogs reduce hepatocyte steatosis and improve survival by enhancing the unfolded protein response and promoting macroautophagy. PLoS ONE 2011, 6, e25269. [Google Scholar] [CrossRef]
- Kim Chung le, T.; Hosaka, T.; Yoshida, M.; Harada, N.; Sakaue, H.; Sakai, T.; Nakaya, Y. Exendin-4, a GLP-1 receptor agonist, directly induces adiponectin expression through protein kinase A pathway and prevents inflammatory adipokine expression. Biochem. Biophys Res. Commun. 2009, 390, 613–618. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kountouras, J.; Zavos, C.; Tsiaousi, E. The role of adiponectin in the pathogenesis and treatment of non-alcoholic fatty liver disease. Diabetes Obes. Metab. 2010, 12, 365–383. [Google Scholar] [CrossRef]
- Tong, W.; Ju, L.; Qiu, M.; Xie, Q.; Chen, Y.; Shen, W.; Sun, W.; Wang, W.; Tian, J. Liraglutide ameliorates non-alcoholic fatty liver disease by enhancing mitochondrial architecture and promoting autophagy through the SIRT1/SIRT3-FOXO3a pathway. Hepatol. Res. 2016, 46, 933–943. [Google Scholar] [CrossRef]
- Lee, J.; Hong, S.W.; Chae, S.W.; Kim, D.H.; Choi, J.H.; Bae, J.C.; Park, S.E.; Rhee, E.J.; Park, C.Y.; Oh, K.W.; et al. Exendin-4 improves steatohepatitis by increasing Sirt1 expression in high-fat diet-induced obese C57BL/6J mice. PLoS ONE 2012, 7, e31394. [Google Scholar] [CrossRef]
- Cariou, B. Pleiotropic effects of insulin and GLP-1 receptor agonists: Potential benefits of the association. Diabetes Metab. 2015, 41 (Suppl. S1), 6S28–6S35. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Iizuka, K.; Miller, B.C.; Uyeda, K. Carbohydrate response element binding protein directly promotes lipogenic enzyme gene transcription. Proc. Natl Acad. Sci. USA 2004, 101, 15597–15602. [Google Scholar] [CrossRef] [PubMed]
- Parlevliet, E.T.; Wang, Y.; Geerling, J.J.; Schröder-Van der Elst, J.P.; Picha, K.; O’Neil, K.; Stojanovic-Susulic, V.; Ort, T.; Havekes, L.M.; Romijn, J.A.; et al. GLP-1 receptor activation inhibits VLDL production and reverses hepatic steatosis by decreasing hepatic lipogenesis in high-fat-fed APOE*3-Leiden mice. PLoS ONE 2012, 7, e49152. [Google Scholar] [CrossRef] [PubMed]
- Samson, S.L.; Bajaj, M. Potential of incretin-based therapies for non-alcoholic fatty liver disease. J. Diabetes Complicat. 2013, 27, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Flock, G.; Baggio, L.L.; Longuet, C.; Drucker, D.J. Incretin receptors for glucagon-like peptide 1 and glucose-dependent insulinotropic polypeptide are essential for the sustained metabolic actions of vildagliptin in mice. Diabetes 2007, 56, 3006–3013. [Google Scholar] [CrossRef]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of hyperglycemia in Type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 487–493; Erratum in Diabetes Care 2020, 43, 1670. [Google Scholar] [CrossRef]
- Drucker, D.J. Mechanisms of action and therapeutic application of glucagon-like Peptide-1. Cell Metab. 2018, 27, 740–756. [Google Scholar] [CrossRef]
- Yan, J.; Yao, B.; Kuang, H.; Yang, X.; Huang, Q.; Hong, T.; Li, Y.; Dou, J.; Yang, W.; Qin, G.; et al. Liraglutide, sitagliptin, and insulin glargine added to metformin: The effect on body weight and intrahepatic lipid in patients with type 2 diabetes mellitus and nonalcoholic fatty liver disease. Hepatology 2019, 69, 2414–2426. [Google Scholar] [CrossRef]
- Bizino, M.B.; Jazet, I.M.; de Heer, P.; van Eyk, H.J.; Dekkers, I.A.; Rensen, P.C.N.; Paiman, E.H.M.; Lamb, H.J.; Smit, J.W. Placebo-controlled randomised trial with liraglutide on magnetic resonance endpoints in individuals with type 2 diabetes: A pre-specified secondary study on ectopic fat accumulation. Diabetologia 2020, 63, 65–74. [Google Scholar] [CrossRef]
- Feng, W.; Gao, C.; Bi, Y.; Wu, M.; Li, P.; Shen, S.; Chen, W.; Yin, T.; Zhu, D. Randomized trial comparing the effects of gliclazide, liraglutide, and metformin on diabetes with non-alcoholic fatty liver disease. J. Diabetes 2017, 9, 800–809. [Google Scholar] [CrossRef]
- Guo, W.; Tian, W.; Lin, L.; Xu, X. Liraglutide or insulin glargine treatments improves hepatic fat in obese patients with type 2 diabetes and nonalcoholic fatty liver disease in twenty-six weeks: A randomized placebo-controlled trial. Diabetes Res. Clin. Pract. 2020, 170, 108487. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Y.; Qu, X.N.; Sun, Z.Y.; Zhang, Y. Effect of liraglutide therapy on serum fetuin A in patients with type 2 diabetes and non-alcoholic fatty liver disease. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Bouchi, R.; Nakano, Y.; Fukuda, T.; Takeuchi, T.; Murakami, M.; Minami, I.; Izumiyama, H.; Hashimoto, K.; Yoshimoto, T.; Ogawa, Y. Reduction of visceral fat by liraglutide is associated with ameliorations of hepatic steatosis, albuminuria, and micro-inflammation in type 2 diabetic patients with insulin treatment: A randomized control trial. Endocr. J. 2017, 64, 269–281. [Google Scholar] [CrossRef]
- Khoo, J.; Hsiang, J.C.; Taneja, R.; Koo, S.H.; Soon, G.H.; Kam, C.J.; Law, N.M.; Ang, T.L. Randomized trial comparing effects of weight loss by liraglutide with lifestyle modification in non-alcoholic fatty liver disease. Liver Int. 2019, 39, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Volpe, S.; Lisco, G.; Fanelli, M.; Racaniello, D.; Colaianni, V.; Triggiani, D.; Donghia, R.; Crudele, L.; Rinaldi, R.; Sabbà, C.; et al. Once-Weekly Subcutaneous Semaglutide Improves Fatty Liver Disease in Patients with Type 2 Diabetes: A 52-Week Prospective Real-Life Study. Nutrients 2022, 14, 4673. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Sundby Palle, M.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised clinical trial: Semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment. Pharmacol. Ther. 2021, 54, 1150–1161. [Google Scholar] [CrossRef]
- Loomba, R.; Abdelmalek, M.F.; Armstrong, M.J.; Jara, M.; Kjær, M.S.; Krarup, N.; Lawitz, E.; Ratziu, V.; Sanyal, A.J.; Schattenberg, J.M.; et al. Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: A randomised, placebo-controlled phase 2 trial. Lancet Gastroenterol. Hepatol. 2023, 6, 511–522. [Google Scholar] [CrossRef]
- Liu, L.; Yan, H.; Xia, M.; Zhao, L.; Lv, M.; Zhao, N.; Rao, S.; Yao, X.; Wu, W.; Pan, B.; et al. Efficacy of exenatide and insulin glargine on nonalcoholic fatty liver disease in patients with type 2 diabetes. Diabetes Metab. Res. Rev. 2020, 36, e3292. [Google Scholar] [CrossRef]
- Dutour, A.; Abdesselam, I.; Ancel, P.; Kober, F.; Mrad, G.; Darmon, P.; Ronsin, O.; Pradel, V.; Lesavre, N.; Martin, J.C.; et al. Exenatide decreases liver fat content and epicardial adipose tissue in patients with obesity and type 2 diabetes: A prospective randomized clinical trial using magnetic resonance imaging and spectroscopy. Diabetes Obes. Metab. 2016, 18, 882–891. [Google Scholar] [CrossRef]
- Shao, N.; Kuang, H.Y.; Hao, M.; Gao, X.Y.; Lin, W.J.; Zou, W. Benefits of exenatide on obesity and non-alcoholic fatty liver disease with elevated liver enzymes in patients with type 2 diabetes. Diabetes Metab. Res. Rev. 2014, 30, 521–529. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Choudhary, N.S.; Singh, M.K.; Wasir, J.S.; Kaur, P.; Gill, H.K.; Bano, T.; Farooqui, K.J.; et al. Effect of dulaglutide on liver fat in patients with type 2 diabetes and NAFLD: Randomised controlled trial (D-LIFT trial). Diabetologia 2020, 63, 2434–2445. [Google Scholar] [CrossRef] [PubMed]
- Seko, Y.; Sumida, Y.; Tanaka, S.; Mori, K.; Taketani, H.; Ishiba, H.; Hara, T.; Okajima, A.; Umemura, A.; Nishikawa, T.; et al. Effect of 12-week dulaglutide therapy in Japanese patients with biopsy-proven non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol. Res. 2017, 47, 1206–1211. [Google Scholar] [CrossRef] [PubMed]
- Capehorn, M.S.; Catarig, A.M.; Furberg, J.K.; Janez, A.; Price, H.C.; Tadayon, S.; Vergès, B.; Marre, M. Efficacy and safety of once-weekly semaglutide 1.0mg vs once-daily liraglutide 1.2mg as add-on to 1-3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab. 2020, 46, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Fala, L. Trulicity (dulaglutide): A new GLP-1 receptor agonist once-weekly subcutaneous injection approved for the treatment of patients with Type 2 diabetes. Am. Health Drug Benefits 2015, 8, 131–134. [Google Scholar]
- Li, Z.; Zhang, Y.; Quan, X.; Yang, Z.; Zeng, X.; Ji, L.; Sun, F.; Zhan, S. Efficacy and acceptability of glycemic control of glucagon-like Peptide-1 receptor agonists among Type 2 diabetes: A systematic review and network meta-analysis. PLoS ONE 2016, 11, e0154206. [Google Scholar] [CrossRef]
- Borodavkin, P.; Sheridan, W.; Coelho, C.; Oštarijaš, E.; Zaïr, Z.M.; Miras, A.D.; McGowan, B.; le Roux, C.W.; Vincent, R.P.; Dimitriadis, G.K. Effects of glucagon-like peptide-1 receptor agonists on histopathological and secondary biomarkers of non-alcoholic steatohepatitis: A systematic review and meta-analysis. Diabetes Obes. Metab. 2022, 24, 337–342. [Google Scholar] [CrossRef]
- Zhu, Y.; Xu, J.; Zhang, D.; Mu, X.; Shi, Y.; Chen, S.; Wu, Z.; Li, S. Efficacy and safety of GLP-1 receptor agonists in patients with type 2 diabetes mellitus and non-alcoholic fatty liver disease: A systematic review and meta-analysis. Front. Endocrinol. (Lausanne) 2021, 12, 769069. [Google Scholar] [CrossRef]
- Gu, Y.; Sun, L.; He, Y.; Yang, L.; Deng, C.; Zhou, R.; Kong, T.; Zhang, W.; Chen, Y.; Li, J.; et al. Comparative efficacy of glucagon-like peptide 1 (GLP-1) receptor agonists, pioglitazone and vitamin E for liver histology among patients with nonalcoholic fatty liver disease: Systematic review and pilot network meta-analysis of randomized controlled trials. Expert Rev. Gastroenterol. Hepatol. 2023, 17, 273–282. [Google Scholar]
- Zou, C.Y.; Sun, Y.; Liang, J. Comparative efficacy of diabetes medications on liver enzymes and fat fraction in patients with nonalcoholic fatty liver disease: A network meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102053. [Google Scholar] [CrossRef]
- Coskun, T.; Sloop, K.W.; Loghin, C.; Alsina-Fernandez, J.; Urva, S.; Bokvist, K.B.; Cui, X.; Briere, D.A.; Cabrera, O.; Roell, W.C.; et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Mol. Metab. 2018, 18, 3–14. [Google Scholar] [CrossRef]
- Frias, J.P.; Nauck, M.A.; Van, J.; Kutner, M.E.; Cui, X.; Benson, C.; Urva, S.; Gimeno, R.E.; Milicevic, Z.; Robins, D.; et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: A randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet 2018, 392, 2180–2193. [Google Scholar] [CrossRef] [PubMed]
- Frías, J.P.; Davies, M.J.; Rosenstock, J.; Pérez Manghi, F.C.; Fernández Landó, L.; Bergman, B.K.; Liu, B.; Cui, X.; Brown, K.; SURPASS-2 Investigators. Tirzepatide versus semaglutide Once Weekly in Patients with Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide once weekly for the treatment of obesity. N. Engl. J. Med. 2022, 387, 205–216. [Google Scholar] [CrossRef]
- Clemmensen, C.; Finan, B.; Müller, T.D.; Dimarchi, R.D.; Tschöp, M.H.; Hofmann, S.M. Emerging hormonal-based combination pharmacotherapies for the treatment of metabolic diseases. Nat. Rev. Endocrinol. 2019, 15, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Nahra, R.; Wang, T.; Gadde, K.M.; Oscarsson, J.; Stumvoll, M.; Jermutus, L.; Hirshberg, B.; Ambery, P. Effects of cotadutide on metabolic and hepatic parameters in adults with overweight or obesity and type 2 diabetes: A 54-week randomized phase 2b study. Diabetes Care 2021, 44, 1433–1442. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| GLP-1RA | First Approved | Molecular Weight (Da) | Reference Amino Acid Sequence | Included Components | Elimination Half-Life | Administration Schedule |
|---|---|---|---|---|---|---|
| Short-acting compounds | ||||||
| Exenatide | 2005 | 4186.6 | Exendin-4 | None | 3.3–4.0 h | Twice daily |
| Long-acting compounds | ||||||
| Liraglutide | 2009 | 3751.2 | Mammalian GLP-1 | Free fatty acid * | 12.6–14.3 h | Once daily |
| Dulaglutide | 2014 | 59,670.6 | Mammalian GLP-1 | Immunoglobulin Fc fragment | 4.7–5.5 day | Once weekly |
| Semaglutide | 2017 | 4113.6 | Mammalian GLP-1 | Free fatty acid * | 5.7–6.7 day | Once weekly |
| Author | Population | Comparators | Duration | Assessment | Findings | Safety (GLP-1RAs) |
|---|---|---|---|---|---|---|
| Armstrong et al. (UK) [12] | Overweight NASH | Liraglutide 1.8 mg/day (n = 26) Placebo (n = 26) | 48 weeks | Histology | NASH resolution with no worsening of fibrosis: 39% with liraglutide vs. 9% with placebo (p = 0.019) Progression of fibrosis: 9% with liraglutide vs. 36% with placebo (p = 0.04) | SAE in 8% and treatment withdrawl due to AE in 8% of patients with liraglutide |
| Yan et al. (China) [38] | T2DM and NAFLD | Liraglutide 1.8 mg/day (n = 24) Sitagliptin 100 mg/day (n = 27) Insulin glargine 0.2 IU/kg/day (n = 24) | 26 weeks | MRI-PDFF | Change in LFC: −4.0% with liraglutide vs. −3.8% with sitagliptin vs. −0.8% with insulin glargine (p = 0.911 for liraglutide vs. sitagliptin; p = 0.039 for liraglutide vs. insuline glargine; p = 0.043 for sitagliptin vs. insulin glargine) | AE in 20.8% and gastrointestinal disorders in 16.7% of patients with liraglutide |
| Bizino et al. (The Netherlands) [39] | T2DM with obesity or uncontrolled T2DM | Liraglutide 1.8 mg/day (n = 23) Placebo (n = 26) | 26 weeks | MRI-PDFF | Change in LFC: 18.1% to 12.0% with liraglutide vs. 18.4% to 14.7% with placebo (estimated treatment effect −2.1% [95% CI −5.3 to 1.0]) | Not reported |
| Feng et al. (China) [40] | T2DM and NAFLD | Liraglutide 1.8 mg/day (n = 31) Gliclazide 120 mg/day (n = 31) Metformin 2000 mg/day (n = 31) | 24 weeks | Ultrasonography | Change in LFC: 36.7% to 13.1% with liraglutide vs. 33.0% to 19.6% with gliclazide vs. 35.1% to 18.4% with metformin (p < 0.01 for liraglutide vs. gliclazide) | Not reported |
| Guo et al. (China) [41] | Uncontrolled T2DM, obesity, and NAFLD | Insulin glargine (n = 30) Liraglutide 1.8 mg/day (n = 31) Placebo (n = 30) | 26 weeks | H-MRS | Change in LFC: 26.4% to 20.6% with liraglutide (p < 0.05) vs. 25.0% to 22.6% with insulin glargine (p > 0.05) | Not reported |
| Zhang et al. (China) [42] | T2DM and NAFLD | Liraglutide 1.2 mg/day (n = 30) Pioglitazone 30 mg/day (n = 30) | 24 weeks | H-MRS | Change in LFC: 24.1 to 20.1 with liraglutide vs. 23.9 to 22.4 with pioglitazone (p < 0.05) | AE in 33.3% and gastrointestinal reactions in 30% of patients with liraglutide |
| Bouchi et al. (Japan) [43] | T2DM with insulin treatment and obesity | Liraglutide 0.9 mg/day + insulin (n = 8) Insulin (n = 9) | 36 weeks | CT | Change in liver attenuation index: 0.84 to 0.99 with liraglutide + insulin vs. 0.99 to 1.06 with insulin (p = 0.065) | No severe AE |
| Khoo et al. (Singapore) [44] | NAFLD and obesity without T2DM | Liraglutide 3 mg/day (n = 15) Moderate-intensity exercise (n = 15) | 26 weeks | MRI | Change in LFC: −7.0 ± 7.1% with liraglutide vs. −8.1 ± 13.2% with exercise (p = 0.78) Change in liver stiffness: −0.25 ± 0.27 kPa with liraglutide vs. −0.12 ± 0.19 kPa with exercise (p = 0.17) | Nausea in 80%, abdominal discomfort in 100%, and diarrhea in 33% of patients with liraglutide |
| Nwesome et al. (UK) [13] | Biopsy-confirmed NASH and liver fibrosis of stage F1–3 and obesity | Semaglutide 0.1 mg (n = 80), 0.2 mg (n = 78), 0.4 mg/day (n = 82) Placebo (n = 80) | 72 weeks | Histology | NASH resolution with no worsening of fibrosis: 40% with semaglutide 0.1 mg, 36% with 0.2 mg, 59% with 0.4 mg, and 17% with placebo (p < 0.001 for semaglutide 0.4 mg vs. placebo) Improvement in fibrosis stage: 43% of semaglutide 0.4 mg vs. 33% of placebo (p = 0.48). | Nausea in 40%, constipation in 22%, vomiting in 15%, and malignancy in 1% of patients with semaglutide |
| Volpe et al. (Italy) [45] | Uncontrolled T2DM and NAFLD | Semaglutide 0.5 mg/week (n = 40) | 52 weeks | Ultrasonography | 70% achieved at least one-class reduction in the 4-point semiquantitative staging (p < 0.001) | Not reported |
| Flint et al. (Multinational) [46] | NAFLD and obesity | Semaglutide 0.4 mg/day (n = 34) Placebo (n = 33) | 48 weeks | MRI-PDFFMRE | ≥30% reduction in LFC: 76.5% with semaglutide vs. 30.3% with placebo (estimated treatment ratio 0.47 [95% CI 0.36 to 0.60; p < 0.001]) ≥15% reduction in liver stiffness: 17.6% with semaglutide vs. 15.2% with placebo (etimated treatment ratio 0.96 [95% CI 0.89 to 1.03; p = 0.2798]) | AE in 93.9%, SAE in 12.1%, drug discontinuation due to AE in 3.0% of patients with semaglutide |
| Loomba et al. (USA) [47] | Biopsy-confirmed NASH-related cirrhosis and BMI ≥27 kg/m2 | Semaglutide 2.4 mg/week (n = 47) Placebo (n = 24) | 48 weeks | Histology | Improvement in liver fibrosis of one stage or more without worsening of NASH: 11% with semaglutide vs. 29% with placebo (OR 0.28 [95% CI 0.06 to 1.24; p = 0.087]) NASH resolution: 34% with semaglutide vs. 21% with placebo (OR 1.97 [95% CI 0.56 to 7.91; p = 0.29]) | AE in 89%, SAE in 13%, nausea in 45%, diarrhea in 19%, and vomiting in 17% of patients with semaglutide |
| Liu et al. (China) [48] | Newly diagnosed T2DM and NAFLD | Exenatide 5 μg/10 μg bid (n = 38) Insulin glargine 0.1–0.3 IU/kg/day (n = 38) | 24 weeks | H-MRS | Change in LFC: −17.55 ± 12.93% (p < 0.05) with exenatide vs. −10.49 ± 11.38% (p < 0.05) with insulin glargine | AE in 13.16% and hypoglycemia in 7.89% of patients with exenatide |
| Dutour, et al. (France) [49] | Uncontrolled T2DM and obesity | Exenatide 5 μg/10 μg bid (n = 22) Control (n = 22) | 26 weeks | H-MRS | Change in LFC: −23.8 ± 9.5% with exenatide vs. +12.5 ± 9.6% with control (p = 0.007) | Not reported |
| Shao et al. (China) [50] | Newly diagnosed obesity, T2DM, and NAFLD | Exenatide + Insulin glargine (n = 30) Insulin (n = 30) | 12 weeks | Ultrasonography | Reversal rate of fatty liver: 93.3% with exenatide vs. 66.7% with insulin (p < 0.01) | Not reported |
| Kuchay et al. (India) [51] | T2DM and NAFLD | Dulaglutide 1.5 mg/week (n = 27) Control (n = 25) | 24 weeks | MRI-PDFF VCTE | Change in LFC: −5.8 ± 1.0% with dulaglutide vs. −2.3 ± 1.2% with control (between-group difference −3.5% [95% CI −6.6 to −0.4; p = 0.025]) Change in liver stiffness: −1.43 ± 0.56% with dulaglutide vs. −0.12 ± 0.63% with control (between-group difference −1.31% [95% CI −2.99 to 0.37; p = 0.123]) | Three discontinued due to upper gastrointestinal upset and no SAE in patients with dulaglutide |
| Seko et al. (Japan) [52] | Biopsy-proven NAFLD with T2DM | Dulaglutide 0.75 mg/week (n = 15) | 12 weeks | Controlled attenuation parameter, VCTE | Change in LFC: 313.6 to 333.4 dB/m (p = 0.080) Change in liver stiffness: 9.3 to 6.9 kPa (p = 0.043) | One with diarrhea |
| Gastaldelli et al. (Italy) [19] | Uncontrolled T2DM and obesity | Tirzepatide 5 mg (n = 71); 10 mg (n = 79); 15 mg (n = 72) Insulin degludec (n = 74) | 52 weeks | MRI-PDFF | Change in LFC: –8.09 ± 0.57% with pooled tirzepatide 10 mg and 15 mg vs. –3.38 ± 0.83% with insulin degludec group (estimated treatment difference –4.71% [95% CI –6.72 to –2.70; p < 0.0001]) | One discontinued due to adverse event |
| Name | Phase | Population | Comparators | Duration | Assessment | Primary Endpoints |
|---|---|---|---|---|---|---|
| ESSENCE, NCT04822181 | III | Biopsy-confirmed NASH with fibrosis stage 2 and 3 (n = 1200) | Semaglutide once weekly Placebo | 72 weeks | Histology | Resolution of steatohepatitis and no worsening of liver fibrosis Improvement in liver fibrosis and no worsening of steatohepatitis Time to first liver-related clinical event |
| COMBATT2NASH, NCT04639414 | IV | T2DM and biopsy-confirmed NASH with fibrosis stage 1–3 (n = 192) | Combined treatment with Empagliflozin once daily and Semaglutide once weekly Empagliflozin once daily monotherapy Placebo | 48 weeks | Histology | Histological resolution of NASH without worsening of fibrosis |
| NCT04971785 | II | Biopsy confirmed NASH-related cirrhosis (n = 440) | Semaglutide once weekly + cilofexor and firsocostat Semaglutide once weekly monotherapy Cilofexor and firsocostat monotherapy Placebo | 72 weeks | Histology | Percentage of participants who achieve ≥1-stage improvement in fibrosis without worsening of NASH Percentage of participants with NASH resolution |
| NCT03884075 | II | Histological or imaging evidence of hepatic steatosis (n = 84) | Semaglutide once weekly No intervention | 30 weeks | Histology MRS | ≥1 point decrease in NAFLD activity score Reduction in liver fat content ≥25% and reduction in ALT by ≥25% or normalization of ALT |
| NCT05067621 | III | Impaired glucose tolerance or T2DM and NAFLD (n = 60) | Semaglutide once weekly Placebo | 24 weeks | MRI-PDFF | Change in oral disposition index Change in MRI-PDFF |
| NCT05016882 | II | Biopsy-confirmed NASH with fibrosis stage 2–4 (n = 672) | NNC0194 0499 once weekly + semaglutide once weekly Semaglutide once weekly monotherapy Placebo | 52 weeks | Histology | Improvement in liver fibrosis and no worsening of NASH |
| SYNERGY-NASH; NCT04166773 | II | T2DM and biopsy-confirmed NASH with fibrosis stage 2–3, and obesity (n = 196) | Tirzepatide once weekly Placebo | 52 weeks | Histology | Percentage of participants with absence of NASH with no worsening of fibrosis |
| NCT05751720 | I/II | T2DM and NAFLD with fibrosis stage 3 and 4 (n = 30) | Tirzepatide once weekly | 12 months | VCTE, MRI-PDFF | Change in liver stiffness in terms of kPa Change in liver fat quantification |
| PROXYMO-ADV, NCT05364931 | IIb/III | Biopsy-confirmed NASH with fibrosis stage 2 and 3 (n = 45) | Cotadutide once daily Placebo | 84 weeks | Histology | Proportion of participants with resolution of NASH without worsening of liver fibrosis Proportion of participants with improvement in liver fibrosis by at least one stage without worsening of NASH |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.A.; Kim, H.Y. Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2023, 24, 9324. https://doi.org/10.3390/ijms24119324
Lee HA, Kim HY. Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease. International Journal of Molecular Sciences. 2023; 24(11):9324. https://doi.org/10.3390/ijms24119324
Chicago/Turabian StyleLee, Han Ah, and Hwi Young Kim. 2023. "Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease" International Journal of Molecular Sciences 24, no. 11: 9324. https://doi.org/10.3390/ijms24119324
APA StyleLee, H. A., & Kim, H. Y. (2023). Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease. International Journal of Molecular Sciences, 24(11), 9324. https://doi.org/10.3390/ijms24119324