
Chronic Kidney Disease Induced by Cadmium and Diabetes: A Quantitative Case-Control Study

 ,
,  , and
, and 
Abstract
1. Introduction
2. Results
2.1. Characteristics of the Study Subjects
2.2. Independent Associations of Cadmium and Diabetes with Measurement of Kidney Function
2.3. Effects of Cadmium and Diabetes on Risks of Adverse Kidney Outcomes
2.4. Quantitation of Effects of Cadmium and Diabetes on Kidney Tubular Reabsorption of β2M
2.5. Quantitation of Effects of GFR on Microalbuminuria
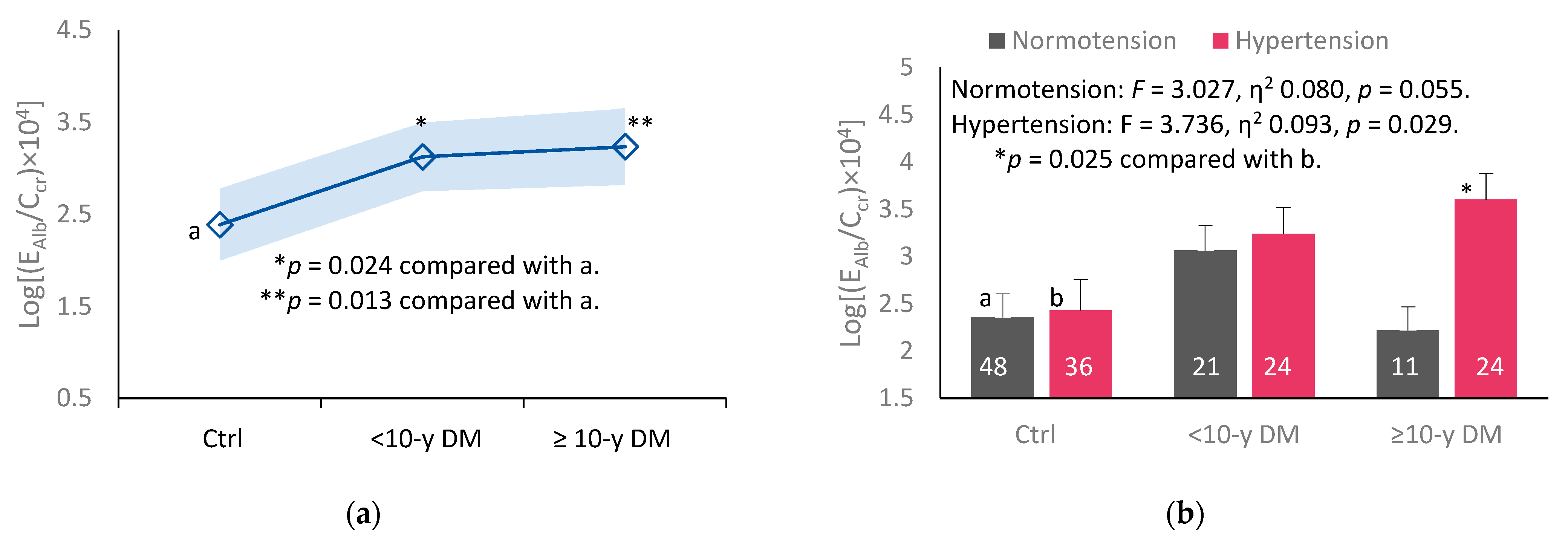
2.6. Quantification of Effects of Diabetes Duration and Hypertension on Alb Excretion Rate
3. Discussion
4. Materials and Methods
4.1. Recruitment of Cases and Controls
4.2. Blood and Urine Sampling and Analysis
4.3. Quantiation of Cd in Blood and Urine Samples
4.4. Normalization of ECd, Eβ2M and EAlb to Ecr and Ccr
4.5. Estimated Glomerular Filtration Rates (eGFRs)
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Il’yasova, D.; Ivanova, A. Urinary cadmium, impaired fasting glucose, and diabetes in the NHANES III. Diabetes Care 2003, 26, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Wallia, A.; Allen, N.B.; Badon, S.; El Muayed, M. Association between urinary cadmium levels and prediabetes in the NHANES 2005–2010 population. Int. J. Hyg. Environ. Health 2014, 217, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Little, B.B.; Reilly, R.; Walsh, B.; Vu, G.T. Cadmium is associated with type 2 diabetes in a Superfund Site Lead Smelter Community in Dallas, Texas. Int. J. Environ. Res. Public Health 2020, 17, 4558. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Li, W.; Zhu, C.; Yang, S.; Zhou, M.; Wang, B.; Wang, X.; Wang, D.; Ma, J.; Zhou, Y.; et al. Cadmium exposure, fasting blood glucose changes, and type 2 diabetes mellitus: A longitudinal prospective study in China. Environ. Res. 2021, 192, 110259. [Google Scholar] [CrossRef]
- Guo, F.F.; Hu, Z.Y.; Li, B.Y.; Qin, L.Q.; Fu, C.; Yu, H.; Zhang, Z.L. Evaluation of the association between urinary cadmium levels below threshold limits and the risk of diabetes mellitus: A dose-response meta-analysis. Environ. Sci. Pollut. Res. Int. 2019, 26, 19272–19281. [Google Scholar] [CrossRef]
- Filippini, T.; Wise, L.A.; Vinceti, M. Cadmium exposure and risk of diabetes and prediabetes: A systematic review and dose-response meta-analysis. Environ. Int. 2022, 158, 106920. [Google Scholar] [CrossRef]
- Hagedoorn, I.J.M.; Gant, C.M.; Huizen, S.V.; Maatman, R.G.H.J.; Navis, G.; Bakker, S.J.L.; Laverman, G.D. Lifestyle-related exposure to cadmium and lead is associated with diabetic kidney disease. J. Clin. Med. 2020, 9, 2432. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Hagedoorn, I.J.M.; Maatman, R.G.H.J.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Cadmium, active smoking and renal function deterioration in patients with type 2 diabetes. Nephrol. Dial. Transpl. 2023, 38, 876–883. [Google Scholar] [CrossRef]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef]
- Elinder, C.G.; Lind, B.; Kjellström, T.; Linnman, L.; Friberg, L. Cadmium in kidney cortex, liver, and pancreas from Swedish autopsies. Estimation of biological half time in kidney cortex, considering calorie intake and smoking habits. Arch. Environ. Health 1976, 31, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Elinder, C.G.; Kjellstöm, T.; Lind, B.; Molander, M.L.; Silander, T. Cadmium concentrations in human liver, blood, and bile: Comparison with a metabolic model. Environ. Res. 1978, 17, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.H.; Roumelioti, M.E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering beta-2 microglobulin as a biomarker across the spectrum of kidney diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef]
- Madrigal, J.M.; Ricardo, A.C.; Persky, V.; Turyk, M. Associations between blood cadmium concentration and kidney function in the U.S. population: Impact of sex, diabetes and hypertension. Environ. Res. 2018, 169, 180–188. [Google Scholar] [CrossRef]
- Lin, Y.S.; Ho, W.C.; Caffrey, J.L.; Sonawane, B. Low serum zinc is associated with elevated risk of cadmium nephrotoxicity. Environ. Res. 2014, 134, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, P.M.; Costanzi, S.; Naticchia, A.; Sturniolo, A.; Gambaro, G. Low level exposure to cadmium increases the risk of chronic kidney disease: Analysis of the NHANES 1999–2006. BMC Public Health 2010, 10, 304. [Google Scholar] [CrossRef]
- Buchet, J.P.; Lauwerys, R.; Roels, H.; Bernard, A.; Bruaux, P.; Claeys, F.; Ducoffre, G.; de Plaen, P.; Staessen, J.; Amery., A.; et al. Renal effects of cadmium body burden of the general population. Lancet 1990, 336, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Akesson, A.; Lundh, T.; Vahter, M.; Bjellerup, P.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Strömberg, U.; Skerfving, S. Tubular and glomerular kidney effects in Swedish women with low environmental cadmium exposure. Environ. Health Perspect. 2005, 113, 1627–1631. [Google Scholar] [CrossRef]
- Barregard, L.; Bergstrom, G.; Fagerberg, B. Cadmium, type 2 diabetes, and kidney damage in a cohort of middle-aged women. Environ. Res. 2014, 135, 311–316. [Google Scholar] [CrossRef]
- Haswell-Elkins, M.; Satarug, S.; O’Rourke, P.; Moore, M.; Ng, J.; McGrath, V.; Walmby, M. Striking association between urinary cadmium level and albuminuria among Torres Strait Islander people with diabetes. Environ. Res. 2008, 106, 379–383. [Google Scholar] [CrossRef]
- Hwangbo, Y.; Weaver, V.M.; Tellez-Plaza, M.; Guallar, E.; Lee, B.K.; Navas-Acien, A. Blood cadmium and estimated glomerular filtration rate in Korean adults. Environ. Health Perspect. 2011, 119, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The source and pathophysiologic significance of excreted cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Scmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Dose–response analysis of the tubular and glomerular effects of chronic exposure to environmental cadmium. Int. J. Environ. Res. Public Health 2022, 19, 10572. [Google Scholar] [CrossRef] [PubMed]
- JECFA. Evaluation of certain Food Additives and Contaminants. In Proceedings of the Seventy-Third Meeting of the Joint FAO/WHO Expert Committee on Food Additives, Geneva, Switzerland, 8–17 June 2010; Food and Agriculture Organization of the United Nations: Rome, Italy; World Health Organization: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/44521 (accessed on 17 May 2023).
- Wong, C.; Roberts, S.M.; Saab, I.N. Review of regulatory reference values and background levels for heavy metals in the human diet. Regul. Toxicol. Pharmacol. 2022, 130, 105122. [Google Scholar] [CrossRef]
- Grau-Perez, M.; Pichler, G.; Galan-Chilet, I.; Briongos-Figuero, L.S.; Rentero-Garrido, P.; Lopez-Izquierdo, R.; Navas-Acien, A.; Weaver, V.; García-Barrera, T.; Gomez-Ariza, J.L.; et al. Urine cadmium levels and albuminuria in a general population from Spain: A gene-environment interaction analysis. Environ. Int. 2017, 106, 27–36. [Google Scholar] [CrossRef]
- Tsai, H.J.; Hung, C.H.; Wang, C.W.; Tu, H.P.; Li, C.H.; Tsai, C.C.; Lin, W.Y.; Chen, S.C.; Kuo, C.H. Associations among heavy metals and proteinuria and chronic kidney disease. Diagnostics 2021, 11, 282. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- Portman, R.J.; Kissane, J.M.; Robson, A.M. Use of B2-microglobulin to diagnose tubulo-interstitial renal lesions in children. Kidney Int. 1986, 30, 91–98. [Google Scholar] [CrossRef]
- Gauthier, C.; Nguyen-Simonnet, H.; Vincent, C.; Revillard, J.-P.; Pellet, M.V. Renal tubular absorption of beta 2 microglobulin. Kidney Int. 1984, 26, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Peterson, P.A.; Evrin, P.-E.; Berggard, I. Differentiation of glomerular, tubular, and normal proteinuria: Determination of urinary excretion of B2-microglobulin, albumin, and total protein. J. Clin. Investig. 1969, 48, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Đorđević, A.B. The validity of benchmark dose limit analysis for estimating permissible accumulation of cadmium. Int. J. Environ. Res. Public Health 2022, 19, 15697. [Google Scholar] [CrossRef]
- Molitoris, B.A.; Sandoval, R.M.; Yadav, S.P.S.; Wagner, M.C. Albumin uptake and processing by the proximal tubule: Physiological, pathological, and therapeutic implications. Physiol. Rev. 2022, 102, 1625–1667. [Google Scholar] [CrossRef]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal handling of albumin-from early findings to current concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef]
- Santoyo-Sánchez, M.P.; Pedraza-Chaverri, J.; Molina-Jijón, E.; Arreola-Mendoza, L.; Rodríguez-Muñoz, R.; Barbier, O.C. Impaired endocytosis in proximal tubule from subchronic exposure to cadmium involves angiotensin II type 1 and cubilin receptors. BMC Nephrol. 2013, 14, 211. [Google Scholar] [CrossRef] [PubMed]
- Gena, P.; Calamita, G.; Guggino, W.B. Cadmium impairs albumin reabsorption by down-regulating megalin and ClC5 channels in renal proximal tubule cells. Environ. Health Perspect. 2010, 118, 1551–1556. [Google Scholar] [CrossRef]
- Li, L.; Dong, F.; Xu, D.; Du, L.; Yan, S.; Hu, H.; Lobe, C.G.; Yi, F.; Kapron, C.M.; Liu, J. Short-term, low-dose cadmium exposure induces hyperpermeability in human renal glomerular endothelial cells. J. Appl. Toxicol. 2016, 36, 257–265. [Google Scholar] [CrossRef]
- Li, Z.; Jiang, L.; Tao, T.; Su, W.; Guo, Y.; Yu, H.; Qin, J. Assessment of cadmium-induced nephrotoxicity using a kidney-on-a-chip device. Toxicol. Res. 2017, 6, 372–380. [Google Scholar] [CrossRef]
- Mohandes, S.; Doke, T.; Hu, H.; Mukhi, D.; Dhillon, P.; Susztak, K. Molecular pathways that drive diabetic kidney disease. J. Clin. Investig. 2023, 133, e165654. [Google Scholar] [CrossRef]
- Fu, J.; Lee, K.; Chuang, P.Y.; Liu, Z.; He, J.C. Glomerular endothelial cell injury and cross talk in diabetic kidney disease. Am. J. Physiol. Ren. Physiol. 2015, 308, F287–F297. [Google Scholar] [CrossRef] [PubMed]
- Järup, L.; Rogenfelt, A.; Elinder, C.G.; Nogawa, K.; Kjellström, T. Biological half-time of cadmium in the blood of workers after cessation of exposure. Scand. J. Work Environ. Health. 1983, 9, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Oh, S.; Kang, H.; Kim, S.; Lee, G.; Li, L.; Kim, C.T.; An, J.N.; Oh, Y.K.; Lim, C.S.; et al. Environment-wide association study of CKD. Clin. J. Am. Soc. Nephrol. 2020, 15, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Schnaper, H.W. The tubulointerstitial pathophysiology of progressive kidney disease. Adv. Chronic Kidney Dis. 2017, 24, 107–116. [Google Scholar] [CrossRef]
- Chevalier, R.L. The proximal tubule is the primary target of injury and progression of kidney disease: Role of the glomerulotubular junction. Am. J. Physiol. Ren. Physiol. 2016, 311, F145–F161. [Google Scholar] [CrossRef]
- Sharma, S.; Smyth, B. From proteinuria to fibrosis: An update on pathophysiology and treatment options. Kidney Blood Press Res. 2021, 46, 411–420. [Google Scholar] [CrossRef]
- Barregard, L.; Sallsten, G.; Lundh, T.; Mölne, J. Low-level exposure to lead, cadmium and mercury, and histopathological findings in kidney biopsies. Environ. Res. 2022, 211, 113119. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C. The inverse association of glomerular function and urinary β2-MG excretion and its implications for cadmium health risk assessment. Environ. Res. 2019, 173, 40–47. [Google Scholar] [CrossRef]
- Kudo, K.; Konta, T.; Mashima, Y.; Ichikawa, K.; Takasaki, S.; Ikeda, A.; Hoshikawa, M.; Suzuki, K.; Shibata, Y.; Watanabe, T.; et al. The association between renal tubular damage and rapid renal deterioration in the Japanese population: The Takahata study. Clin. Exp. Nephrol. 2011, 15, 235–241. [Google Scholar] [CrossRef]
- Mashima, Y.; Konta, T.; Kudo, K.; Takasaki, S.; Ichikawa, K.; Suzuki, K.; Shibata, Y.; Watanabe, T.; Kato, T.; Kawata, S.; et al. Increases in urinary albumin and beta2-microglobulin are independently associated with blood pressure in the Japanese general population: The Takahata Study. Hypertens. Res. 2011, 34, 831–835. [Google Scholar] [CrossRef]
- Ikeda, A.; Konta, T.; Takasaki, S.; Hao, Z.; Suzuki, K.; Sato, H.; Shibata, Y.; Takeishi, Y.; Kato, T.; Kawata, S.; et al. In a non-diabetic Japanese population, the combination of macroalbuminuria and increased urine beta 2-microglobulin predicts a decline of renal function: The Takahata study. Nephrol. Dial. Transpl. 2009, 24, 841–847. [Google Scholar] [CrossRef]
- Siddiqui, K.; George, T.P.; Joy, S.S.; Alfadda, A.A. Risk factors of chronic kidney disease among type 2 diabetic patients with longer duration of diabetes. Front. Endocrinol. 2022, 13, 1079725. [Google Scholar] [CrossRef] [PubMed]
- Keefe, J.A.; Hwang, S.J.; Huan, T.; Mendelson, M.; Yao, C.; Courchesne, P.; Saleh, M.A.; Madhur, M.S.; Levy, D. Evidence for a causal role of the SH2B3-β2M axis in blood pressure regulation. Hypertension 2019, 73, 497–503. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Denic, A.; Elsherbiny, H.; Rule, A.D. In-vivo techniques for determining nephron number. Curr. Opin. Nephrol. Hypertens. 2019, 28, 545–551. [Google Scholar] [CrossRef]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.E.; SBU GFR Review Group. Measuring GFR: A systematic review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef] [PubMed]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | All Subjects n = 176 | Non-DM n = 88 | <10-yr DM n = 48 | ≥10-yr DM n = 37 | p |
|---|---|---|---|---|---|
| Duration of diabetes a, yrs | n/a | 0 | 4.2 ± 2.1 | 15.8 ± 7.2 | − |
| Fasting plasma glucose, mg/dL | 131.7 ± 61.3 | 94 ± 12 | 177 ± 76 | 161 ± 55 | <0.001 |
| Blood Cd, µg/L | 0.59 ± 0.74 | 0.64 ± 0.85 | 0.52 ± 0.61 | 0.57 ± 0.61 | 0.677 |
| Female, % | 80.9 | 80.7 | 79.2 | 83.9 | 0.863 |
| Smoking, % | 9.8 | 11.4 | 10.4 | 5.4 | 0.586 |
| Hypertension, % | 51.8 | 44.7 | 54.2 | 64.9 | 0.114 |
| Age, years | 59.9 ± 9.7 | 60.4 ± 9.2 | 59.2 ± 9.6 | 59.0 ± 11.2 | 0.489 |
| BMI, kg/m2 | 25.4 ± 4.7 | 24.7 ± 4.4 | 26.3 ± 5.2 | 25.7 ± 4.6 | 0.098 |
| Obese b (%) | 10.4 | 5.7 | 18.8 | 10.3 | 0.058 |
| eGFR c, mL/min/1.73 m2 | 79.4 ± 18.0 | 79.4 ± 14.4 | 82.0 ± 19.6 | 77.6 ± 23.3 | 0.399 |
| Reduced eGFR d (%) | 15.6 | 11.4 | 14.6 | 27.0 | 0.086 |
| Normalized to Ccr as Ex/Ccr e | |||||
| (ECd/Ccr) × 100, µg/L filtrate | 0.84 ± 1.66 | 0.86 ± 1.69 | 0.53 ± 1.13 | 1.33 ± 2.21 | 0.248 |
| (Eβ2M/Ccr) × 100, µg/L filtrate | 1313 ± 2396 | 543 ± 625 | 1975 ± 2914 | 2294 ± 3725 | <0.001 |
| (EAlb/Ccr) × 100, mg/L filtrate | 43.2 ± 127.7 | 8.8 ± 17.9 | 54.3 ± 99.2 | 112.4 ± 240.9 | 0.001 |
| (Eβ2M/Ccr) × 100 ≥ 300 µg/L (%) | 66.2 | 54.2 | 78.0 | 80.8 | 0.008 |
| (Eβ2M/Ccr) × 100 ≥ 1000 µg/L (%) | 32.4 | 15.3 | 46.3 | 57.7 | <0.001 |
| EAlb/Ccr) × 100 ≥ 20 mg/L (%) | 24.4 | 10.7 | 33.3 | 45.7 | <0.001 |
| EAlb/Ccr) × 100, mg/L (%) | |||||
| <20 | 75.6 | 89.3 | 66.7 | 54.3 | <0.001 |
| 20–199 | 18.3 | 10.7 | 20.0 | 34.3 | <0.001 |
| ≥200 | 6.1 | 0 | 13.3 | 11.4 | 0.008 |
| Normalized to Ecr as Ex/Ecr f | |||||
| ECd/Ecr, µg/g creatinine | 0.96 ± 1.83 | 0.99 ± 1.94 | 0.69 ± 1.49 | 1.36 ± 2.08 | 0.376 |
| Eβ2M/Ecr, µg/g creatinine | 1284 ± 1747 | 633 ± 762 | 2012 ± 2549 | 1856 ± 1589 | <0.001 |
| EAlb/Ecr, mg/g creatinine | 41 ± 104 | 11 ± 24 | 60 ± 112 | 90 ± 173 | <0.001 |
| Eβ2M/Ecr ≥ 300 µg/g creatinine (%) | 70.5 | 58.3 | 80.5 | 88.5 | 0.004 |
| Eβ2M/Ecr ≥ 1000 µg/g creatinine (%) | 37.4 | 20.8 | 48.8 | 65.4 | <0.001 |
| EAlb/Ecr ≥ 20 or ≥ 30 mg/g creatinine | 20.7 | 7.1 | 33.3 | 37.1 | <0.001 |
| EAlb/Ecr, mg/g creatinine (%) | |||||
| <30 | 79.3 | 92.9 | 66.7 | 62.9 | <0.001 |
| 30–299 | 16.5 | 7.1 | 26.7 | 25.7 | <0.001 |
| ≥300 | 4.3 | 0 | 6.7 | 11.4 | 0.001 |
| Independent Variables/Factors | Log[(Eβ2M/Ccr) × 103] | Log[(EAlb/Ccr) × 104] | eGFR | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | η2 | p | β | η2 | p | β | η2 | p | |
| Age | 0.164 | 0.034 | 0.043 | 0.104 | 0.008 | 0.325 | −0.357 | 0.131 | <0.001 |
| BMI | −0.141 | 0.028 | 0.065 | −0.022 | 0.005 | 0.450 | 0.079 | 0.009 | 0.308 |
| Log10[Cd]b | 0.138 | 0.022 | 0.103 | 0.050 | 0.003 | 0.527 | −0.077 | 0.006 | 0.383 |
| Log2[(ECd/Ccr) × 105] | 0.244 | 0.077 | 0.002 | 0.033 | 0.000032 | 0.950 | −0.104 | 0.010 | 0.272 |
| Smoking | 0.015 | 0.008 | 0.339 | −0.036 | 0.002 | 0.622 | 0.012 | 0.000071 | 0.926 |
| Gender (female) | −0.114 | 0.009 | 0.288 | 0.041 | 0.000025 | 0.955 | 0.089 | 0.010 | 0.269 |
| Hypertension | 0.048 | 0.024 | 0.088 | 0.259 | 0.036 | 0.035 | 0.023 | 0.001 | 0.732 |
| Diabetes | 0.432 | 0.083 | 0.001 | 0.286 | 0.042 | 0.023 | −0.069 | 0.018 | 0.138 |
| Interactions a | − | 0.038 | 0.031 | − | 0.053 | 0.010 | − | 0.038 | 0.031 |
| Adjusted R2 | 0.330 | − | <0.001 | 0.171 | − | 0.001 | 0.141 | − | 0.001 |
| Independent Variables/Factors | (Eβ2M/Ccr) × 100 ≥ 300 µg/L | (Ealb/Ccr) × 100 ≥ 20 mg/L | eGFR ≤ 60 mL/min/1.73 m2 | |||
|---|---|---|---|---|---|---|
| POR (95% CI) | p | POR (95% CI) | p | POR (95% CI) | p | |
| Age | 1.060 (1.006, 1.117) | 0.029 | 1.038 (0.986, 1.094) | 0.154 | 1.147 (1.058, 1.244) | 0.001 |
| BMI | 0.945 (0.861, 1.038) | 0.240 | 0.971 (0.888, 1.063) | 0.527 | 0.981 (0.866, 1.110) | 0.755 |
| Log10[Cd]b | 1.859 (0.976, 3.543) | 0.059 | 1.235 (0.630, 2.422) | 0.538 | 1.137 (0.475, 2.725) | 0.773 |
| Log2[(ECd/Ccr) × 105] | 1.260 (1.007, 1.577) | 0.044 | 1.025 (0.843, 1.245) | 0.807 | 1.138 (0.894, 1.449) | 0.293 |
| Smoking | 2.643 (0.465, 15.04) | 0.273 | 1.877 (0.124, 28.49) | 0.650 | 1.877 (0.124, 28.49) | 0.650 |
| Gender (female) | 2.043 (0.605, 6.900) | 0.250 | 0.301 (0.085, 1.065) | 0.062 | 0.448 (0.040, 4.989) | 0.514 |
| Hypertension | 1.249 (0.521, 2.991) | 0.618 | 2.317 (0.915, 5.865) | 0.076 | 0.559 (0.165, 1.895) | 0.350 |
| Non-diabetics | Referent | Referent | Referent | |||
| <10-yr DM | 0.842 (0.209, 3.394) | 0.809 | 2.315 (0.764, 7.016) | 0.138 | 3.384 (0.736, 15.55) | 0.117 |
| ≥10-yr DM | 4.035 (1.094, 14.88) | 0.036 | 6.142 (2.004, 18.83) | 0.001 | 6.949 (1.613, 29.93) | 0.009 |
| Severe Tubular Dysfunction a | |||||
|---|---|---|---|---|---|
| Independent Variables/ Factors | β Coefficient (SE) | POR | 95% CI | p | |
| Lower | Upper | ||||
| Age | 0.010 (0.027) | 1.010 | 0.957 | 1.066 | 0.705 |
| BMI | 0.000019 (0.055) | 1.000 | 0.899 | 1.113 | 1.000 |
| Log10[Cd]b | −0.317 (0.354) | 0.728 | 0.364 | 1.457 | 0.370 |
| Log2[(ECd/Ccr) × 105] | 0.276 (0.103) | 1.317 | 1.077 | 1.612 | 0.007 |
| Gender (female) | 0.026 (0.742) | 1.026 | 0.239 | 4.397 | 0.972 |
| Hypertension | 0.964 (0.476) | 2.621 | 1.030 | 6.668 | 0.043 |
| Smoking | 0.598 (1.011) | 1.819 | 0.251 | 13.185 | 0.554 |
| eGFR, mL/min/1.73 m2 | |||||
| ≥90 | Referent | ||||
| 61−89 | 2.646 (0.730) | 14.094 | 3.369 | 58.971 | <0.001 |
| ≤60 | 4.430 (1.004) | 83.958 | 11.742 | 600.342 | <0.001 |
| Microalbuminuria a | |||||
|---|---|---|---|---|---|
| Independent Variables/ Factors | β Coefficient (SE) | POR | 95% CI | p | |
| Lower | Upper | ||||
| Age | 0.002 (0.027) | 1.002 | 0.951 | 1.056 | 0.950 |
| BMI | 0.039 (0.046) | 1.039 | 0.950 | 1.138 | 0.401 |
| Log10[Cd]b | 0.144 (0.341) | 1.155 | 0.592 | 2.251 | 0.672 |
| Log2[(ECd/Ccr) × 105] | 0.024 (0.098) | 1.025 | 0.845 | 1.242 | 0.804 |
| Gender (female) | 1.022 (0.617) | 2.780 | 0.830 | 9.314 | 0.097 |
| Hypertension | 1.199 (0.463) | 3.318 | 1.340 | 8.218 | 0.010 |
| Smoking | 0.885 (0.914) | 2.423 | 0.404 | 14.531 | 0.333 |
| eGFR, mL/min/1.73 m2 | |||||
| ≥90 | Referent | ||||
| 61−89 | 1.500 (0.596) | 4.483 | 1.394 | 14.421 | 0.012 |
| ≤60 | 1.518 (0.725) | 4.565 | 1.103 | 18.888 | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yimthiang, S.; Vesey, D.A.; Pouyfung, P.; Khamphaya, T.; Gobe, G.C.; Satarug, S. Chronic Kidney Disease Induced by Cadmium and Diabetes: A Quantitative Case-Control Study. Int. J. Mol. Sci. 2023, 24, 9050. https://doi.org/10.3390/ijms24109050
Yimthiang S, Vesey DA, Pouyfung P, Khamphaya T, Gobe GC, Satarug S. Chronic Kidney Disease Induced by Cadmium and Diabetes: A Quantitative Case-Control Study. International Journal of Molecular Sciences. 2023; 24(10):9050. https://doi.org/10.3390/ijms24109050
Chicago/Turabian StyleYimthiang, Supabhorn, David A. Vesey, Phisit Pouyfung, Tanaporn Khamphaya, Glenda C. Gobe, and Soisungwan Satarug. 2023. "Chronic Kidney Disease Induced by Cadmium and Diabetes: A Quantitative Case-Control Study" International Journal of Molecular Sciences 24, no. 10: 9050. https://doi.org/10.3390/ijms24109050
APA StyleYimthiang, S., Vesey, D. A., Pouyfung, P., Khamphaya, T., Gobe, G. C., & Satarug, S. (2023). Chronic Kidney Disease Induced by Cadmium and Diabetes: A Quantitative Case-Control Study. International Journal of Molecular Sciences, 24(10), 9050. https://doi.org/10.3390/ijms24109050