
Structural and Hemodynamic Changes of the Right Ventricle in PH-HFpEF


Abstract
1. Introduction
2. Pulmonary Hypertension: PAH and PH-HFpEF
3. Epidemiology
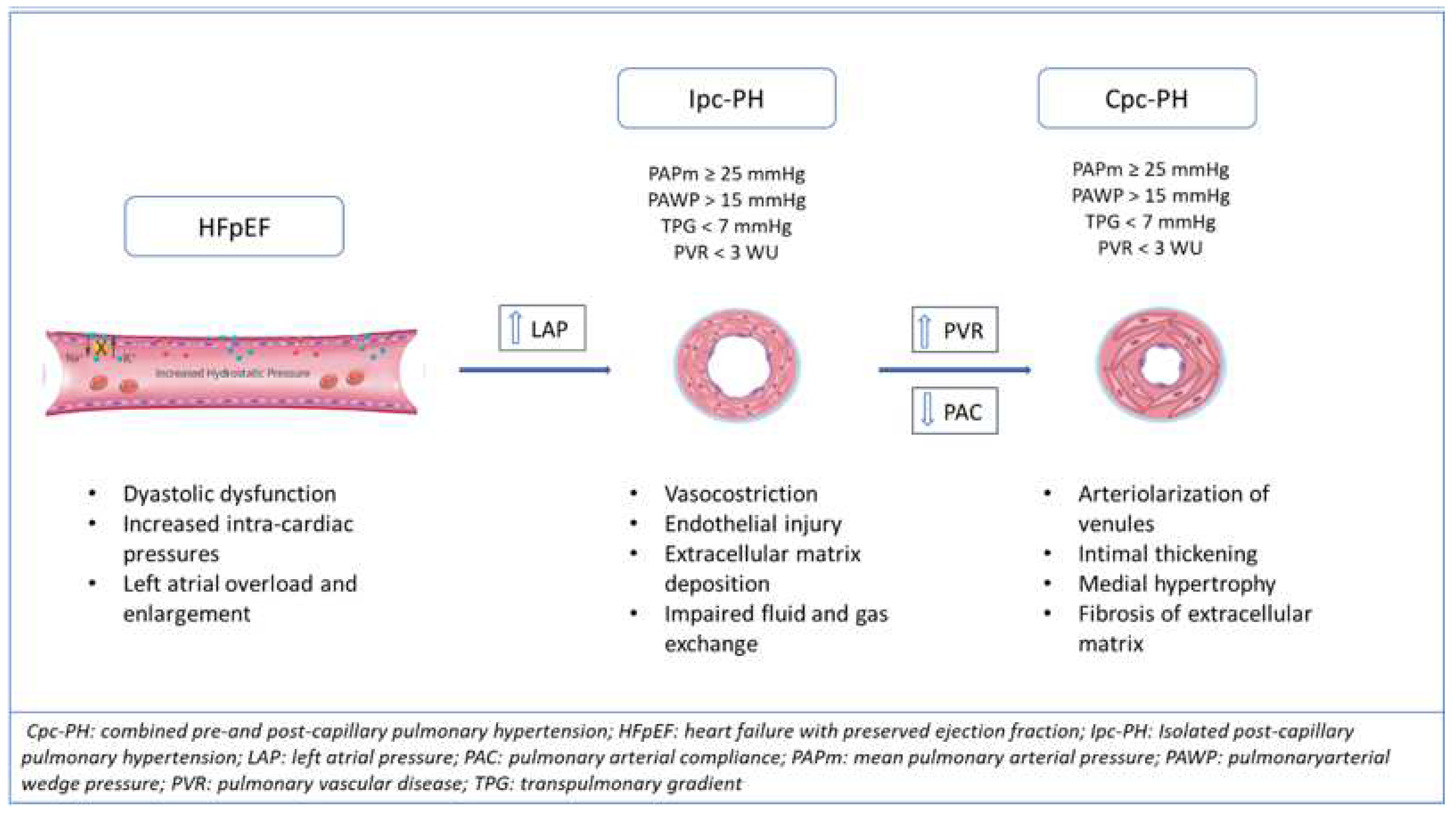
4. Hemodynamic and Pathobiological Alterations in PH-HFpEF
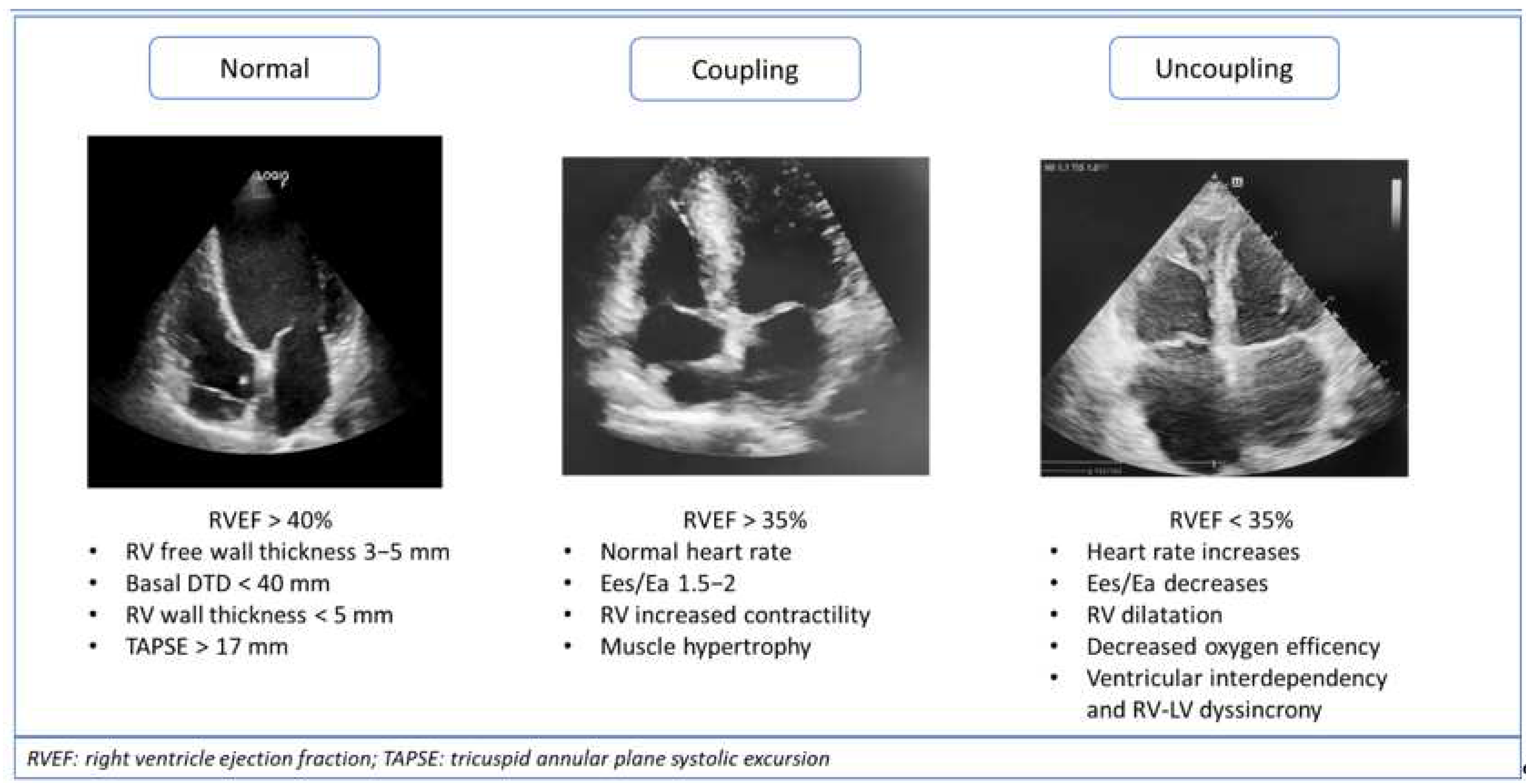
5. Right Ventricle Mechanisms of Adaptations to Afterload: Ventriculoarterial Coupling and Uncoupling
6. Noninvasive Diagnostic and Prognostic Tools and Potential Applications
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Galiè, N.; Hoeper, M.M.; Humbert, M.; Torbicki, A.; Vachiery, J.-L.; Barbera, J.A.; Beghetti, M.; Corris, P.; Gaine, S.; Gibbs, J.S.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; McLaughlin, V.V.; Rubin, L.J.; Simonneau, G. An overview of the 6th World Symposium on Pulmonary Hypertension. Eur. Respir. J. 2019, 53, 1802148. [Google Scholar] [CrossRef] [PubMed]
- Parker, F.; Weiss, S. The Nature and Significance of the Structural Changes in the Lungs in Mitral Stenosis. Am. J. Pathol. 1936, 12, 573–598.15. Available online: http://europepmc.org/abstract/MED/19970288 (accessed on 20 February 2021). [PubMed]
- Ruocco, G.; Gavazzi, A.; Gonnelli, S.; Palazzuoli, A. Pulmonary arterial hypertension and heart failure with preserved ejection fraction: Are they so discordant? Cardiovasc. Diagn. Ther. 2020, 10, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Ghio, S.; Adir, Y. Pulmonary Hypertension in HFpEF and HFrEF. J. Am. Coll. Cardiol. 2020, 76, 1102–1111. [Google Scholar] [CrossRef]
- Guazzi, M.; Naeije, R. Pulmonary Hypertension in Heart Failure. J. Am. Coll. Cardiol. 2017, 69, 1718–1734. [Google Scholar] [CrossRef]
- Vachiéry, J.-L.; Tedford, R.J.; Rosenkranz, S.; Palazzini, M.; Lang, I.; Guazzi, M.; Coghlan, G.; Chazova, I.; De Marco, T. Pulmonary hypertension due to left heart disease. Eur. Respir. J. 2019, 53, 1801897. [Google Scholar] [CrossRef]
- Gerges, M.; Gerges, C.; Pistritto, A.M.; Lang, M.B.; Trip, P.; Jakowitsch, J.; Binder, T.; Lang, I.M. Pulmonary Hypertension in Heart Failure. Epidemiology, Right Ventricular Function, and Survival. Am. J. Respir. Crit. Care Med. 2015, 192, 1234–1246. [Google Scholar] [CrossRef]
- Maeder, M.T. Selexipag and the pulmonary hypertension continuum. Eur. J. Heart Fail. 2022, 24, 215–218. [Google Scholar] [CrossRef]
- Tuder, R.M.; Archer, S.L.; Dorfmüller, P.; Erzurum, S.C.; Guignabert, C.; Michelakis, E.; Rabinovitch, M.; Schermuly, R.; Stenmark, K.R.; Morrell, N.W. Relevant Issues in the Pathology and Pathobiology of Pulmonary Hypertension. J. Am. Coll. Cardiol. 2013, 62, D4–D12. [Google Scholar] [CrossRef]
- Leopold, J.A. Pulmonary Venous Remodeling in Pulmonary Hypertension. Circulation 2018, 137, 1811–1813. [Google Scholar] [CrossRef] [PubMed]
- Fayyaz, A.U.; Edwards, W.D.; Maleszewski, J.J.; Ewa, A.; Konik, E.A.; Hilary, M.; DuBrock, H.M.; Barry, A.; Borlaug, B.A.; Robert, P.; et al. Global Pulmonary Vascular Remodeling in Pulmonary Hypertension Associated with Heart Failure and Preserved or Reduced Ejection Fraction. Circulation 2018, 137, 1796–1810. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; McMurray, J.; Massie, B.M.; Caspi, A.; Charlon, V.; Cohen-Solal, A.; Kiowski, W.; Kostuk, W.; Krum, H.; Levine, B.; et al. Clinical effects of endothelin receptor antagonism with bosentan in patients with severe chronic heart failure: Results of a pilot study. J. Card. Fail. 2005, 11, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Califf, R.M.; Adams, K.F.; McKenna, W.J.; Gheorghiade, M.; Uretsky, B.F.; McNulty, S.E.; Darius, H.; Schulman, K.; Zannad, F.; Handberg-Thurmond, F.; et al. A randomized controlled trial of epoprostenol therapy for severe congestive heart failure: The Flolan International Randomized Survival Trial (FIRST). Am. Heart J. 1997, 134, 44–54. [Google Scholar] [CrossRef]
- Hoeper, M.M.; Lam, C.S.P.; Vachiery, J.L.; Bauersachs, J.; Gerges, C.; Lang, I.M.; Bonderman, D.; Olsson, K.M.; Gibbs, J.S.R.; Dorfmuller, P.; et al. Pulmonary hypertension in heart failure with preserved ejection fraction: A plea for proper phenotyping and further research. Eur. Heart J. 2016, 38, 2869–2873. [Google Scholar] [CrossRef]
- Vanderpool, R.R.; Saul, M.; Nouraie, M.; Gladwin, M.T.; Simon, M.A. Association Between Hemodynamic Markers of Pulmonary Hypertension and Outcomes in Heart Failure with Preserved Ejection Fraction. JAMA Cardiol. 2018, 3, 298. [Google Scholar] [CrossRef]
- Elliott, C.G. The Fifth World Symposium on Pulmonary Hypertension and Robyn, J. Barst, MD. Adv. Pulm. Hypertens. 2014, 13, 15–16. [Google Scholar] [CrossRef]
- Thenappan, T.; Shah, S.J.; Gomberg-Maitland, M. Clinical Characteristics of Pulmonary Hypertension in Patients with Heart Failure and Preserved Ejection Fraction. Circ. Heart Fail. 2011, 4, 257–265. [Google Scholar] [CrossRef]
- Guazzi, M.; Dixon, D.; Labate, V.; Beussink-Nelson, L.; Bandera, F.; Cuttica, M.J.; Sanijv, J.; Shah, S.J. RV Contractile Function and its Coupling to Pulmonary Circulation in Heart Failure with Preserved Ejection Fraction. JACC Cardiovasc. Imaging 2017, 10, 1211–1221. [Google Scholar] [CrossRef]
- Frantz, R.P. Pulmonary arterial hypertension or left heart disease with pulmonary hypertension? Toward noninvasive clarity, but time for a new paradigm. Eur. Respir. J. 2015, 46, 299–302. [Google Scholar] [CrossRef]
- Berthelot, E.; Montani, D.; Algalarrondo, V.; Dreyfuss, C.; Rifai, R.; Benmalek, A.; Jais, W.; Bouchachi, A.; Savale, L.; Simonneau, G.; et al. A Clinical and Echocardiographic Score to Identify Pulmonary Hypertension Due to HFpEF. J. Card. Fail. 2017, 23, 29–35. [Google Scholar] [CrossRef]
- D’Alto, M.; Romeo, E.; Argiento, P.; Pavelescu, A.; Mélot, C.; D’Andrea, A.; Correra, A.; Bossone, E.; Calabrò, R.; Russo, M.G.; et al. Echocardiographic Prediction of Pre- versus Postcapillary Pulmonary Hypertension. J. Am. Soc. Echocardiogr. 2015, 28, 108–115. [Google Scholar] [CrossRef]
- Opotowsky, A.R.; Ojeda, J.; Rogers, F.; Prasanna, V.; Clair, M.; Moko, L.; Vaidya, A.; Jonathan Afilalo, J.; Paul, R.; Forfia, P.R. A Simple Echocardiographic Prediction Rule for Hemodynamics in Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 765–775. [Google Scholar] [CrossRef]
- Bonderman, D.; Wexberg, P.; Martischnig, A.M. A noninvasive algorithm to exclude pre-capillary pulmonary hypertension. Eur. Respir. J. 2011, 37, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Thenappan, T.; Prins, K.W.; Cogswell, R.; Shah, S.J. Pulmonary Hypertension Secondary to Heart Failure with Preserved Ejection Fraction. Can. J. Cardiol. 2015, 31, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Opitz, C.F.; Hoeper, M.M.; Gibbs, J.S.R. Pre-Capillary, Combined, and Post-Capillary Pulmonary Hypertension. J. Am. Coll. Cardiol. 2016, 68, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Barberà, J.A.; Frost, A.E.; Ghofrani, H.A.; Hoeper, M.M.; McLaughlin, V.V.; Peacock, A.J.; Simonneau, G.; Vachiery, J.L.; Grünig, E.; et al. Initial Use of Ambrisentan plus Tadalafil in Pulmonary Arterial Hypertension. N. Engl. J. Med. 2015, 373, 834–844. [Google Scholar] [CrossRef]
- Olsson, K.M.; Delcroix, M.; Ghofrani, H.A.; Tiede, H.; Huscher, D.; Speich, R.; Staehler, G.; Rosenktranz, S.; Halank, M.; Held, M.; et al. Anticoagulation and Survival in Pulmonary Arterial Hypertension. Circulation 2014, 129, 57–65. [Google Scholar] [CrossRef]
- McGoon, M.D.; Benza, R.L.; Escribano-Subias, P. Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2013, 62, D51–D59. [Google Scholar] [CrossRef]
- Peacock, A.J.; Murphy, N.F.; McMurray, J.J.V.; Caballero, L.; Stewart, S. An epidemiological study of pulmonary arterial hypertension. Eur. Respir. J. 2007, 30, 104–109. [Google Scholar] [CrossRef]
- Humbert, M.; Sitbon, O.; Chaouat, A.; Bertocchi, M.; Habib, G.; Gressin, V.; Yaici, A.; Weitzenblum, E.; Cordier, J.F.; Chabot, F.; et al. Pulmonary Arterial Hypertension in France. Am. J. Respir. Crit. Care Med. 2006, 173, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Thenappan, T.; Gomberg-Maitland, M. Epidemiology of Pulmonary Hypertension and Right Ventricular Failure in Left Heart Failure. Curr. Heart Fail. Rep. 2014, 11, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Shah, S.J.; Anand, I.S.; Sweitzer, N.K.; O’Meara, E.; Heitner, J.F.; Soplo, G.; Li, G.; Assmann, S.F.; McKinlay, S.M.; et al. Cardiac Structure and Function in Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2014, 7, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Cikes, M.; Prasad, N.; Li, G.; Getchevski, S.; Claggett, B.; Rizkala, A.; Lukashevich, I.; O’Meara, E.; Ryan, J.J.; et al. Echocardiographic Features of Patients with Heart Failure and Preserved Left Ventricular Ejection Fraction. J. Am. Coll. Cardiol. 2019, 74, 2858–2873. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.D.; Trivedi, A.; Shah, S.J. Combined post- and pre-capillary pulmonary hypertension in heart failure with preserved ejection fraction. Heart Fail. Rev. 2016, 21, 285–297. [Google Scholar] [CrossRef]
- Kanwar, M.; Tedford, R.J.; Agarwal, R.; Clarke, M.M.; Walter, C.; Sokos, G.; Murali, S.; Benza, R.L. Management of Pulmonary Hypertension due to Heart Failure with Preserved Ejection Fraction. Curr. Hypertens. Rep. 2014, 16, 501. [Google Scholar] [CrossRef] [PubMed]
- Vachiéry, J.L.; Adir, Y.; Barberà, J.A.; Champion, H.; Coghlan, J.G.; Cottin, V.; De Marco, T.; Galie, N.; Ghio, S.; Gibbs, S.R.; et al. Pulmonary Hypertension Due to Left Heart Diseases. J. Am. Coll. Cardiol. 2013, 62, D100–D108. [Google Scholar] [CrossRef]
- Georgiopoulou, V.V.; Kalogeropoulos, A.P.; Borlaug, B.A.; Gheorghiade, M.; Butler, J. Left Ventricular Dysfunction with Pulmonary Hypertension. Circ. Heart Fail. 2013, 6, 344–354. [Google Scholar] [CrossRef][Green Version]
- Vonk-Noordegraaf, A.; Haddad, F.; Chin, K.M.; Forfia, P.R.; Kawut, S.M.; Lumens, J.; Naeije, R.; Newman, J.; Oudiz, R.J.; Provencher, S.; et al. Right Heart Adaptation to Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2013, 62, D22–D33. [Google Scholar] [CrossRef]
- Gerges, C.; Gerges, M.; Lang, M.B.; Zhang, Y.; Jakowitsch, J.; Probst, P.; Maurer, G.; Lang, I.M. Diastolic Pulmonary Vascular Pressure Gradient. Chest 2013, 143, 758–766. [Google Scholar] [CrossRef]
- Harris, P. The Human Pulmonary Circulation: Its Form and Function in Health and Disease/Peter Harris, Donald Heath; Foreword by Melville, Arnott; distributed in the United States of America by Longman; Heath, D., Ed.; Churchill Livingstone: London, UK, 1977. [Google Scholar]
- Ooi, H.; Colucci, W.S.; Givertz, M.M. Endothelin Mediates Increased Pulmonary Vascular Tone in Patients with Heart Failure. Circulation 2002, 106, 1618–1621. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.J.; Jevnikar, F.W.; Walsh, T.; Dickinson, J.; Mouhaffel, A.; Selwyn, A.P. The influence of basal nitric oxide activity on pulmonary vascular resistance in patients with congestive heart failure. Am. J. Cardiol. 1998, 82, 609–614. [Google Scholar] [CrossRef]
- Guazzi, M.; Borlaug, B.A. Pulmonary Hypertension Due to Left Heart Disease. Circulation 2012, 126, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Saouti, N.; Westerhof, N.; Postmus, P.E.; Vonk-Noordegraaf, A. The arterial load in pulmonary hypertension. Eur. Respir. Rev. 2010, 19, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Lankhaar, J.W.; Westerhof, N.; Faes, T.J.C.; Gan, T.J.; Marques, K.M.; Boonstra, A.; van den Berg, F.G.; Postmus, P.E.; Vonk-Noordegraaf, A. Pulmonary vascular resistance and compliance stay inversely related during treatment of pulmonary hypertension. Eur. Heart J. 2008, 29, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Reuben, S.R. Compliance of the Human Pulmonary Arterial System in Disease. Circ. Res. 1971, 29, 40–50. [Google Scholar] [CrossRef]
- Kind, T.; Faes, T.J.C.; Vonk-Noordegraaf, A.; Westerhof, N. Proportional Relations Between Systolic, Diastolic and Mean Pulmonary Artery Pressure are Explained by Vascular Properties. Cardiovasc. Eng. Technol. 2011, 2, 15–23. [Google Scholar] [CrossRef][Green Version]
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship Between the Right Ventricle and its Load in Pulmonary Hypertension. J. Am. Coll. Cardiol. 2017, 69, 236–243. [Google Scholar] [CrossRef]
- Tumminello, G.; Lancellotti, P.; Lempereur, M.; D’Orio, V.; Pierard, L.A. Determinants of pulmonary artery hypertension at rest and during exercise in patients with heart failure. Eur. Heart J. 2006, 28, 569–574. [Google Scholar] [CrossRef]
- Swift, A.J.; Rajaram, S.; Condliffe, R.; Capener, D.; Hurdman, J.; Elliot, C.; Kiely, D.G.; Wild, J.M. Pulmonary Artery Relative Area Change Detects Mild Elevations in Pulmonary Vascular Resistance and Predicts Adverse Outcome in Pulmonary Hypertension. Investig. Radiol. 2012, 47, 571–577. [Google Scholar] [CrossRef]
- D’Alonzo, G.E. Survival in Patients with Primary Pulmonary Hypertension. Ann. Intern. Med. 1991, 115, 343. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.T.J.; Lankhaar, J.W.; Westerhof, N.; Marcus, J.T.; Becker, A.; Twisk, J.W.R.; Boonstra, A.; Postmus, P.E.; Vonk-Noordegraaf, A. Noninvasively Assessed Pulmonary Artery Stiffness Predicts Mortality in Pulmonary Arterial Hypertension. Chest 2007, 132, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Pazzano, A.S.; Klersy, C.; Scelsi, L.; Raineri, C.; Camporotondo, R.; D’Armini, A.; Visconti, L.O. Clinical and Prognostic Relevance of Echocardiographic Evaluation of Right Ventricular Geometry in Patients with Idiopathic Pulmonary Arterial Hypertension. Am. J. Cardiol. 2011, 107, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Raymond, R.J.; Hinderliter, A.L.; Willis, P.W.; Ralph, D.; Caldwell, E.J.; WSilliams, W.; Ettinger, N.A.; Hill, N.S.; Summer, W.R.; de Boisblanc, B.; et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J. Am. Coll. Cardiol. 2002, 39, 1214–1219. [Google Scholar] [CrossRef]
- Sachdev, A.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Hsiao, J.F.; Maalouf, J.F.; Ammash, N.M.; McCully, R.B.; Miller, F.A.; Pellikka, P.A.; et al. Right Ventricular Strain for Prediction of Survival in Patients with Pulmonary Arterial Hypertension. Chest 2011, 139, 1299–1309. [Google Scholar] [CrossRef]
- Ruocco, G.; Palazzuoli, A. Early detection of pulmonary arterial hypertension: Do not forget the right ventricle. Nat. Rev. Cardiol. 2015, 12, 134. [Google Scholar] [CrossRef]
- Guihaire, J.; Haddad, F.; Boulate, D. Non-invasive indices of right ventricular function are markers of ventricular-arterial coupling rather than ventricular contractility: Insights from a porcine model of chronic pressure overload. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1140–1149. [Google Scholar] [CrossRef]
- Kuehne, T.; Yilmaz, S.; Steendijk, P.; Moore, P.; Groenink, M.; Saaed, M.; Weber, O.; Higgins, C.B.; Ewert, P.; Fleck, E.; et al. Magnetic Resonance Imaging Analysis of Right Ventricular Pressure-Volume Loops. Circulation 2004, 110, 2010–2016. [Google Scholar] [CrossRef]
- Sano, M.; Minamino, T.; Toko, H.; Miyauchi, H.; Orimo, M.; Qin, Y.; Akazawa, H.; Tateno, K.; Kayama, Y.; Harada, M.; et al. p53-induced inhibition of Hif-1 causes cardiac dysfunction during pressure overload. Nature 2007, 446, 444–448. [Google Scholar] [CrossRef]
- Chen, D.D.; Dong, Y.G.; Yuan, H.; Chen, A.F. Endothelin 1 Activation of Endothelin A Receptor/NADPH Oxidase Pathway and Diminished Antioxidants Critically Contribute to Endothelial Progenitor Cell Reduction and Dysfunction in Salt-Sensitive Hypertension. Hypertension 2012, 59, 1037–1043. [Google Scholar] [CrossRef]
- Tji-Joong Gan, C.; Lankhaar, J.W.; Marcus, J.T.; Westerhof, N.; Marques, K.M.; Bronzwaer, J.G.F.; Boonstra, A.; Postmus, P.E.; Vonk-Noordegraaf, A. Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am. J. Physiol.-Heart Circ. Physiol. 2006, 290, H1528–H1533. [Google Scholar] [CrossRef]
- Marcus, J.T.; Gan, C.T.J.; Zwanenburg, J.J.M.; Boonstra, A.; Allaart, C.P.; Götte, M.J.; Vonk-Noordegraaf, A. Interventricular Mechanical Asynchrony in Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2008, 51, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Mauritz, G.J.; Marcus, J.T.; Westerhof, N.; Postmus, P.E.; Vonk-Noordegraaf, A. Prolonged right ventricular post-systolic isovolumic period in pulmonary arterial hypertension is not a reflection of diastolic dysfunction. Heart 2011, 97, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Chin, K.M.; Haddad, F.; Hassoun, P.M.; Hemnes, A.R.; Hopkins, S.R.; Kawut, S.M.; Langleben, D.; Lumens, J.; Naeije, R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019, 53, 1801900. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Guazzi, M.; Scardovi, A.B.; Klersy, C.; Clemenza, F.; Carluccio, E.; Temporelli, P.L.; Rossi, A.; Faggiano, P.; Traversi, E.; et al. Different correlates but similar prognostic implications for right ventricular dysfunction in heart failure patients with reduced or preserved ejection fraction. Eur. J. Heart Fail. 2017, 19, 873–879. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Borlaug, B.A.; Kane, G.C.; Enders, F.T.; Rodeheffer, R.J.; Redfield, M.M. Age-Associated Increases in Pulmonary Artery Systolic Pressure in the General Population. Circulation 2009, 119, 2663–2670. [Google Scholar] [CrossRef]
- Kjaergaard, J.; Akkan, D.; Iversen, K.K.; Kjoller, E.; Kober, L.; Torp-Pedersen, C.; Hassager, C. Prognostic Importance of Pulmonary Hypertension in Patients with Heart Failure. Am. J. Cardiol. 2007, 99, 1146–1150. [Google Scholar] [CrossRef]
- Damy, T.; Kallvikbacka-Bennett, A.; Goode, K.; Khaleva, O.; Lewinter, C.; Hobkirk, J.; Nikitin, N.P.; Dubois-Rande, J.L.; Hittinger, L.; Vlark, A.J.; et al. Prevalence of, Associations With, and Prognostic Value of Tricuspid Annular Plane Systolic Excursion (TAPSE) Among Out-Patients Referred for the Evaluation of Heart Failure. J. Card. Fail. 2012, 18, 216–225. [Google Scholar] [CrossRef]
- Ghio, S.; Recusani, F.; Klersy, C.; Sebastiani, R.; Laudisa, M.L.; Campana, C.; Gavazzi, A.; Tavazzi, L. Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am. J. Cardiol. 2000, 85, 837–842. [Google Scholar] [CrossRef]
- Guazzi, M.; Bandera, F.; Pelissero, G.; Castelvecchio, S.; Menicanti, L.; Ghio, S.; Temporelli, P.L.; Arena, R. Tricuspid annular plane systolic excursion and pulmonary arterial systolic pressure relationship in heart failure: An index of right ventricular contractile function and prognosis. Am. J. Physiol.-Heart Circ. Physiol. 2013, 305, H1373–H1381. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Ruocco, G.; Evangelista, I.; de Vivo, O.; Nuti, R.; Ghio, S. Prognostic Significance of an Early Echocardiographic Evaluation of Right Ventricular Dimension and Function in Acute Heart Failure. J. Card. Fail. 2020, 26, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Melenovsky, V.; Hwang, S.J.; Lin, G.; Redfield, M.M.; Borlaug, B.A. Right heart dysfunction in heart failure with preserved ejection fraction. Eur. Heart J. 2014, 35, 3452–3462. [Google Scholar] [CrossRef] [PubMed]
- Bosch, L.; Lam, C.S.P.; Gong, L.; Chan, S.P.; Sim, D.; Yeo, D.; Jaufeerallu, F.; Leong, K.T.G.; Ong, H.Y.; Ng, T.P.; et al. Right ventricular dysfunction in left-sided heart failure with preserved versus reduced ejection fraction. Eur. J. Heart Fail. 2017, 19, 1664–1671. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | ||
|---|---|---|
| PAH | Clinical | PH-LHD |
| <65 | Age | >65 |
| Rare | Hypertension | Common |
| Uncommon | Metabolic syndrome | Common |
| Uncommon | Diabetes | Common |
| Uncommon | Obesity | Common |
| Uncommon | CAD | Common |
| Rare | Artial Fibrillation | Common |
| Rare | Obstructive sleep apnoea | Common |
| Echocardiographical | ||
| Usually small | LA size | Enlarged |
| Increased | RA/LA ratio | Normal |
| Typical | RV hypertrophy | Atypical |
| Atypical | LV Hypertrophy | Typical |
| <8 | Lateral E/e’ | >10 |
| <1 | E/A ratio | >1 |
| Common | RVOT notching | Rare |
| Study | N° Subjects | Hemodynamic Characteristics | Duration |
|---|---|---|---|
| Guazzi | 44 | mPAP > 25 mmHg PCWP > 15 mmHg TPG > 12 mmHg | 1 year |
| Hoendermis | 52 | mPAP > 25 mmHg PCWP > 15 mmHg DPG ≥ 17 mmHg | 12 weeks |
| DILATE 1 | 39 | mPAP > 25 mmHg PCWP > 15 mmHg | 12 weeks |
| BADDHY | 20 | mPAP > 25 mmHg PCWP > 15 mmHg 6 MW distance > 150 mt and <400 mt | 12 weeks |
| DYNAMIC | 114 | mPAP > 25 mmHg PCWP > 15 mmHg | 26 weeks |
| PASSION | 320 | PAWP > 15 mmHg mPAP > 25 mmHg PVR > 3WU | NA |
| SERENADE | 300 | PCWP or LVEDP > 15 mmHg | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barilli, M.; Tavera, M.C.; Valente, S.; Palazzuoli, A. Structural and Hemodynamic Changes of the Right Ventricle in PH-HFpEF. Int. J. Mol. Sci. 2022, 23, 4554. https://doi.org/10.3390/ijms23094554
Barilli M, Tavera MC, Valente S, Palazzuoli A. Structural and Hemodynamic Changes of the Right Ventricle in PH-HFpEF. International Journal of Molecular Sciences. 2022; 23(9):4554. https://doi.org/10.3390/ijms23094554
Chicago/Turabian StyleBarilli, Maria, Maria Cristina Tavera, Serafina Valente, and Alberto Palazzuoli. 2022. "Structural and Hemodynamic Changes of the Right Ventricle in PH-HFpEF" International Journal of Molecular Sciences 23, no. 9: 4554. https://doi.org/10.3390/ijms23094554
APA StyleBarilli, M., Tavera, M. C., Valente, S., & Palazzuoli, A. (2022). Structural and Hemodynamic Changes of the Right Ventricle in PH-HFpEF. International Journal of Molecular Sciences, 23(9), 4554. https://doi.org/10.3390/ijms23094554