
Neuroprotective Potential of Dendritic Cells and Sirtuins in Multiple Sclerosis

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Dendritic Cells Classification
3. Dendritic Cells Shape the Autoimmune Response in Neuroinflammation
4. Immunomodulatory DCs in the Context of Neuroinflammation
5. Disease-Modifying Drugs (DMDs) Targeting DCs in MS
6. Alternative Strategies to Target DCs in Autoimmune Disorders
7. Role of Sirtuins in DCs
7.1. Sirtuin 1
7.2. Sirtuin 6
8. Role of Sirtuins in Neuroinflammation
8.1. Sirtuin 1
8.2. Sirtuin 2
8.3. Sirtuin 3
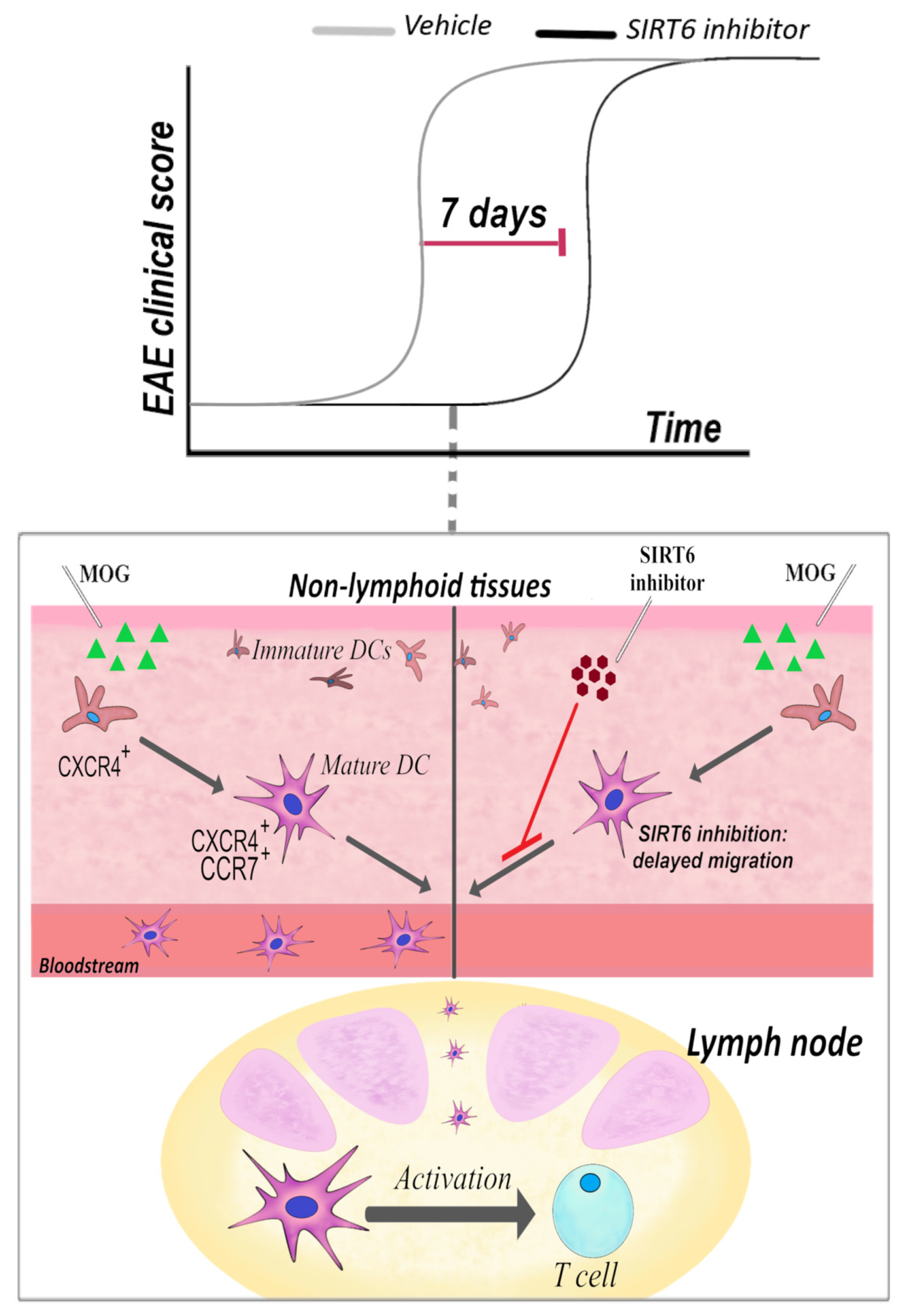
8.4. Sirtuin 6
8.5. Sirtuin 7
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hannoodee, S.; Nasuruddin, D.N. Acute Inflammatory Response; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Pahwa, R.; Goyal, A.; Jialal, I. Chronic Inflammation; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Miyano, A.; Miyamichi, T.; Nakayama, M.; Kitajima, H.; Shimizu, A. Differences among acute, subacute, and chronic chorioamnionitis based on levels of inflammation-associated proteins in cord blood. Pediatric Dev. Pathol. 1998, 1, 513–521. [Google Scholar]
- Hunter, P. The inflammation theory of disease. The growing realization that chronic inflammation is crucial in many diseases opens new avenues for treatment. EMBO Rep. 2012, 13, 968–970. [Google Scholar]
- Tiberi, M.; Chiurchiu, V. Specialized Pro-resolving Lipid Mediators and Glial Cells: Emerging Candidates for Brain Homeostasis and Repair. Front. Cell. Neurosci. 2021, 15, 673549. [Google Scholar]
- Chiurchiu, V.; Leuti, A.; Maccarrone, M. Bioactive Lipids and Chronic Inflammation: Managing the Fire Within. Front. Immunol. 2018, 9, 38. [Google Scholar]
- DiSabato, D.J.; Quan, N.; Godbout, J.P. Neuroinflammation: The devil is in the details. J. Neurochem. 2016, 139, 136–153. [Google Scholar]
- Lyman, M.; Lloyd, D.G.; Ji, X.; Vizcaychipi, M.P.; Ma, D. Neuroinflammation: The role and consequences. Neurosci. Res. 2014, 79, 1–12. [Google Scholar]
- Ajami, B.; Bennett, J.L.; Krieger, C.; McNagny, K.M.; Rossi, F.M. Infiltrating monocytes trigger EAE progression, but do not contribute to the resident microglia pool. Nat. Neurosci. 2011, 14, 1142–1149. [Google Scholar]
- Fletcher, J.M.; Lalor, S.J.; Sweeney, C.M.; Tubridy, N.; Mills, K.H. T cells in multiple sclerosis and experimental autoimmune encephalomyelitis. Clin. Exp. Immunol. 2010, 162, 1–11. [Google Scholar]
- Raine, C.S.; Cannella, B.; Duijvestijn, A.M.; Cross, A.H. Homing to central nervous system vasculature by antigen-specific lymphocytes. II. Lymphocyte/endothelial cell adhesion during the initial stages of autoimmune demyelination. Lab. Investig. 1990, 63, 476–489. [Google Scholar]
- Giles, D.A.; Duncker, P.C.; Wilkinson, N.M.; Washnock-Schmid, J.M.; Segal, B.M. CNS-resident classical DCs play a critical role in CNS autoimmune disease. J. Clin. Investig. 2018, 128, 5322–5334. [Google Scholar]
- Zozulya, A.L.; Clarkson, B.D.; Ortler, S.; Fabry, Z.; Wiendl, H. The role of dendritic cells in CNS autoimmunity. J. Mol. Med. 2010, 88, 535–544. [Google Scholar]
- Serafini, B.; Rosicarelli, B.; Magliozzi, R.; Stigliano, E.; Capello, E.; Mancardi, G.L.; Aloisi, F. Dendritic cells in multiple sclerosis lesions: Maturation stage, myelin uptake, and interaction with proliferating T cells. J. Neuropathol. Exp. Neurol. 2006, 65, 124–141. [Google Scholar]
- Rusconi, M.; Gerardi, F.; Santus, W.; Lizio, A.; Sansone, V.A.; Lunetta, C.; Zanoni, I.; Granucci, F. Inflammatory role of dendritic cells in Amyotrophic Lateral Sclerosis revealed by an analysis of patients’ peripheral blood. Sci. Rep. 2017, 7, 7853. [Google Scholar]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar]
- MacDonald, K.P.; Munster, D.J.; Clark, G.J.; Dzionek, A.; Schmitz, J.; Hart, D.N. Characterization of human blood dendritic cell subsets. Blood 2002, 100, 4512–4520. [Google Scholar]
- Thomas, R.; Lipsky, P.E. Human peripheral blood dendritic cell subsets. Isolation and characterization of precursor and mature antigen-presenting cells. J. Immunol. 1994, 153, 4016–4028. [Google Scholar]
- Sato, K.; Fujita, S. Dendritic cells: Nature and classification. Allergol. Int. Off. J. Jpn. Soc. Allergol. 2007, 56, 183–191. [Google Scholar]
- Collin, M.; Bigley, V. Human dendritic cell subsets: An update. Immunology 2018, 154, 3–20. [Google Scholar]
- Maecker, H.T.; McCoy, J.P.; Nussenblatt, R. Standardizing immunophenotyping for the Human Immunology Project. Nat. Rev. Immunol. 2012, 12, 191–200. [Google Scholar]
- Dzionek, A.; Fuchs, A.; Schmidt, P.; Cremer, S.; Zysk, M.; Miltenyi, S.; Buck, D.W.; Schmitz, J. Bdca-2, bdca-3, and bdca-4: Three markers for distinct subsets of dendritic cells in human peripheral blood. J. Immunol. 2000, 165, 6037–6046. [Google Scholar]
- Segura, E. Human dendritic cell subsets: An updated view of their ontogeny and functional specialization. Eur. J. Immunol. 2022. [Google Scholar] [CrossRef]
- Dutertre, C.A.; Wang, L.F.; Ginhoux, F. Aligning bona fide dendritic cell populations across species. Cell. Immunol. 2014, 291, 3–10. [Google Scholar]
- Wu, L.; D’Amico, A.; Hochrein, H.; O’Keeffe, M.; Shortman, K.; Lucas, K. Development of thymic and splenic dendritic cell populations from different hemopoietic precursors. Blood 2001, 98, 3376–3382. [Google Scholar]
- Vremec, D.; Pooley, J.; Hochrein, H.; Wu, L.; Shortman, K. Cd4 and cd8 expression by dendritic cell subtypes in mouse thymus and spleen. J. Immunol. 2000, 164, 2978–2986. [Google Scholar]
- Proietto, A.I.; O’Keeffe, M.; Gartlan, K.; Wright, M.D.; Shortman, K.; Wu, L.; Lahoud, M.H. Differential production of inflammatory chemokines by murine dendritic cell subsets. Immunobiology 2004, 209, 163–172. [Google Scholar]
- Ingulli, E.; Ulman, D.R.; Lucido, M.M.; Jenkins, M.K. In situ analysis reveals physical interactions between cd11b+ dendritic cells and antigen-specific cd4 t cells after subcutaneous injection of antigen. J. Immunol. 2002, 169, 2247–2252. [Google Scholar]
- Shortman, K.; Heath, W.R. The cd8+ dendritic cell subset. Immunol. Rev. 2010, 234, 18–31. [Google Scholar]
- Yasumi, T.; Katamura, K.; Yoshioka, T.; Meguro, T.A.; Nishikomori, R.; Heike, T.; Inobe, M.; Kon, S.; Uede, T.; Nakahata, T. Differential requirement for the cd40-cd154 costimulatory pathway during th cell priming by cd8 alpha+ and cd8 alpha- murine dendritic cell subsets. J. Immunol. 2004, 172, 4826–4833. [Google Scholar]
- Soltani, S.; Mahmoudi, M.; Farhadi, E. Dendritic cells currently under the spotlight; classification and subset based upon new markers. Immunol. Investig. 2021, 50, 646–661. [Google Scholar]
- Guilliams, M.; Henri, S.; Tamoutounour, S.; Ardouin, L.; Schwartz-Cornil, I.; Dalod, M.; Malissen, B. From skin dendritic cells to a simplified classification of human and mouse dendritic cell subsets. Eur. J. Immunol. 2010, 40, 2089–2094. [Google Scholar]
- Shi, Q.; Zhuang, F.; Liu, J.T.; Li, N.; Chen, Y.X.; Su, X.B.; Yao, A.H.; Yao, Q.P.; Han, Y.; Li, S.S.; et al. Single-cell analyses reveal functional classification of dendritic cells and their potential roles in inflammatory disease. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2019, 33, 3784–3794. [Google Scholar]
- Psarras, A.; Antanaviciute, A.; Alase, A.; Carr, I.; Wittmann, M.; Emery, P.; Tsokos, G.C.; Vital, E.M. Tnf-alpha regulates human plasmacytoid dendritic cells by suppressing ifn-alpha production and enhancing t cell activation. J. Immunol. 2021, 206, 785–796. [Google Scholar]
- Wu, M.; Gao, L.; He, M.; Liu, H.; Jiang, H.; Shi, K.; Shang, R.; Liu, B.; Gao, S.; Chen, H.; et al. Plasmacytoid dendritic cell deficiency in neonates enhances allergic airway inflammation via reduced production of ifn-alpha. Cell. Mol. Immunol. 2020, 17, 519–532. [Google Scholar]
- Arai, Y.; Yamashita, K.; Kuriyama, K.; Shiokawa, M.; Kodama, Y.; Sakurai, T.; Mizugishi, K.; Uchida, K.; Kadowaki, N.; Takaori-Kondo, A.; et al. Plasmacytoid dendritic cell activation and ifn-alpha production are prominent features of murine autoimmune pancreatitis and human igg4-related autoimmune pancreatitis. J. Immunol. 2015, 195, 3033–3044. [Google Scholar]
- Berggren, O.; Alexsson, A.; Morris, D.L.; Tandre, K.; Weber, G.; Vyse, T.J.; Syvanen, A.C.; Ronnblom, L.; Eloranta, M.L. Ifn-alpha production by plasmacytoid dendritic cell associations with polymorphisms in gene loci related to autoimmune and inflammatory diseases. Hum. Mol. Genet. 2015, 24, 3571–3581. [Google Scholar]
- Cella, M.; Facchetti, F.; Lanzavecchia, A.; Colonna, M. Plasmacytoid dendritic cells activated by influenza virus and cd40l drive a potent th1 polarization. Nat. Immunol. 2000, 1, 305–310. [Google Scholar]
- Broughton, S.E.; Dhagat, U.; Hercus, T.R.; Nero, T.L.; Grimbaldeston, M.A.; Bonder, C.S.; Lopez, A.F.; Parker, M.W. The gm-csf/il-3/il-5 cytokine receptor family: From ligand recognition to initiation of signaling. Immunol. Rev. 2012, 250, 277–302. [Google Scholar]
- Galicia-Rosas, G.; Pikor, N.; Schwartz, J.A.; Rojas, O.; Jian, A.; Summers-Deluca, L.; Ostrowski, M.; Nuesslein-Hildesheim, B.; Gommerman, J.L. A sphingosine-1-phosphate receptor 1-directed agonist reduces central nervous system inflammation in a plasmacytoid dendritic cell-dependent manner. J. Immunol. 2012, 189, 3700–3706. [Google Scholar]
- Gold, R.; Linington, C.; Lassmann, H. Understanding pathogenesis and therapy of multiple sclerosis via animal models: 70 years of merits and culprits in experimental autoimmune encephalomyelitis research. Brain J. Neurol. 2006, 129, 1953–1971. [Google Scholar]
- The International Multiple Sclerosis Genetics Consortium; The Wellcome Trust Case Control Consortium. Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature 2011, 476, 214–219. [Google Scholar]
- Raddassi, K.; Kent, S.C.; Yang, J.; Bourcier, K.; Bradshaw, E.M.; Seyfert-Margolis, V.; Nepom, G.T.; Kwok, W.W.; Hafler, D.A. Increased frequencies of myelin oligodendrocyte glycoprotein/mhc class ii-binding cd4 cells in patients with multiple sclerosis. J. Immunol. 2011, 187, 1039–1046. [Google Scholar]
- Patsopoulos, N.A.; Bayer Pharma MS Genetics Working Group; Steering Committees of Studies Evaluating IFNβ-1b and a CCR1-Antagonist; ANZgene Consortium; GeneMSA; International Multiple Sclerosis Genetics Consortium; Esposito, F.; Reischl, J.; Lehr, S.; Bauer, D.; et al. Genome-wide meta-analysis identifies novel multiple sclerosis susceptibility loci. Ann. Neurol. 2011, 70, 897–912. [Google Scholar]
- Greter, M.; Heppner, F.L.; Lemos, M.P.; Odermatt, B.M.; Goebels, N.; Laufer, T.; Noelle, R.J.; Becher, B. Dendritic cells permit immune invasion of the cns in an animal model of multiple sclerosis. Nat. Med. 2005, 11, 328–334. [Google Scholar]
- Iribarren, P.; Cui, Y.H.; Le, Y.; Wang, J.M. The role of dendritic cells in neurodegenerative diseases. Arch. Immunol. Ther. Exp. 2002, 50, 187–196. [Google Scholar]
- Vieira, P.L.; Heystek, H.C.; Wormmeester, J.; Wierenga, E.A.; Kapsenberg, M.L. Glatiramer acetate (copolymer-1, copaxone) promotes th2 cell development and increased il-10 production through modulation of dendritic cells. J. Immunol. 2003, 170, 4483–4488. [Google Scholar]
- Herz, J.; Zipp, F.; Siffrin, V. Neurodegeneration in autoimmune cns inflammation. Exp. Neurol. 2010, 225, 9–17. [Google Scholar]
- Regen, T.; Waisman, A. Modeling a complex disease: Multiple sclerosis-update 2020. Adv. Immunol. 2021, 149, 25–34. [Google Scholar]
- Prinz, M.; Erny, D.; Hagemeyer, N. Ontogeny and homeostasis of cns myeloid cells. Nat. Immunol. 2017, 18, 385–392. [Google Scholar]
- King, I.L.; Kroenke, M.A.; Segal, B.M. Gm-csf-dependent, cd103+ dermal dendritic cells play a critical role in th effector cell differentiation after subcutaneous immunization. J. Exp. Med. 2010, 207, 953–961. [Google Scholar]
- Edelson, B.T.; Bradstreet, T.R.; Kc, W.; Hildner, K.; Herzog, J.W.; Sim, J.; Russell, J.H.; Murphy, T.L.; Unanue, E.R.; Murphy, K.M. Batf3-dependent cd11b(low/-) peripheral dendritic cells are gm-csf-independent and are not required for th cell priming after subcutaneous immunization. PLoS ONE 2011, 6, e25660. [Google Scholar]
- Rodda, L.B.; Bannard, O.; Ludewig, B.; Nagasawa, T.; Cyster, J.G. Phenotypic and morphological properties of germinal center dark zone cxcl12-expressing reticular cells. J. Immunol. 2015, 195, 4781–4791. [Google Scholar]
- Aguzzi, A.; Kranich, J.; Krautler, N.J. Follicular dendritic cells: Origin, phenotype, and function in health and disease. Trends Immunol. 2014, 35, 105–113. [Google Scholar]
- Heesters, B.A.; Myers, R.C.; Carroll, M.C. Follicular dendritic cells: Dynamic antigen libraries. Nat. Rev. Immunol. 2014, 14, 495–504. [Google Scholar]
- Le Hir, M.; Bluethmann, H.; Kosco-Vilbois, M.H.; Muller, M.; di Padova, F.; Moore, M.; Ryffel, B.; Eugster, H.P. Differentiation of follicular dendritic cells and full antibody responses require tumor necrosis factor receptor-1 signaling. J. Exp. Med. 1996, 183, 2367–2372. [Google Scholar]
- Fu, Y.X.; Chaplin, D.D. Development and maturation of secondary lymphoid tissues. Annu. Rev. Immunol. 1999, 17, 399–433. [Google Scholar]
- Walker, C.A.; Huttner, A.J.; O’Connor, K.C. Cortical injury in multiple sclerosis; the role of the immune system. BMC Neurol. 2011, 11, 152. [Google Scholar]
- Cosgrove, J.; Novkovic, M.; Albrecht, S.; Pikor, N.B.; Zhou, Z.; Onder, L.; Morbe, U.; Cupovic, J.; Miller, H.; Alden, K.; et al. B cell zone reticular cell microenvironments shape cxcl13 gradient formation. Nat. Commun. 2020, 11, 3677. [Google Scholar]
- Ohtani, H.; Komeno, T.; Agatsuma, Y.; Kobayashi, M.; Noguchi, M.; Nakamura, N. Follicular dendritic cell meshwork in angioimmunoblastic t-cell lymphoma is characterized by accumulation of cxcl13(+) cells. J. Clin. Exp. Hematop. 2015, 55, 61–69. [Google Scholar]
- Stingl, G.; Tamaki, K.; Katz, S.I. Origin and function of epidermal langerhans cells. Immunol. Rev. 1980, 53, 149–174. [Google Scholar]
- Merad, M.; Ginhoux, F.; Collin, M. Origin, homeostasis and function of langerhans cells and other langerin-expressing dendritic cells. Nature reviews. Immunology 2008, 8, 935–947. [Google Scholar]
- Collin, M.; Milne, P. Langerhans cell origin and regulation. Curr. Opin. Hematol. 2016, 23, 28–35. [Google Scholar]
- Weliwitigoda, A.; Palle, P.; Gessner, M.; Hubbard, N.W.; Oukka, M.; Bettelli, E. Cutting edge: Dock8 regulates a subset of dendritic cells that is critical for the development of experimental autoimmune encephalomyelitis. J. Immunol. 2021, 207, 2417–2422. [Google Scholar]
- Théry, C.; Duban, L.; Segura, E.; Véron, P.; Lantz, O.; Amigorena, S. Indirect activation of naïve cd4+ t cells by dendritic cell-derived exosomes. Nat. Immunol. 2002, 3, 1156–1162. [Google Scholar]
- Guermonprez, P.; Valladeau, J.; Zitvogel, L.; Thery, C.; Amigorena, S. Antigen presentation and t cell stimulation by dendritic cells. Annu. Rev. Immunol. 2002, 20, 621–667. [Google Scholar]
- McMahon, E.J.; Bailey, S.L.; Castenada, C.V.; Waldner, H.; Miller, S.D. Epitope spreading initiates in the cns in two mouse models of multiple sclerosis. Nat. Med. 2005, 11, 335–339. [Google Scholar]
- Hemmer, B.; Kerschensteiner, M.; Korn, T. Role of the innate and adaptive immune responses in the course of multiple sclerosis. Lancet. Neurol. 2015, 14, 406–419. [Google Scholar]
- Steel, C.D.; Hahto, S.M.; Ciavarra, R.P. Peripheral dendritic cells are essential for both the innate and adaptive antiviral immune responses in the central nervous system. Virology 2009, 387, 117–126. [Google Scholar]
- El Behi, M.; Dubucquoi, S.; Lefranc, D.; Zephir, H.; De Seze, J.; Vermersch, P.; Prin, L. New insights into cell responses involved in experimental autoimmune encephalomyelitis and multiple sclerosis. Immunol. Lett. 2005, 96, 11–26. [Google Scholar]
- Hawiger, D.; Inaba, K.; Dorsett, Y.; Guo, M.; Mahnke, K.; Rivera, M.; Ravetch, J.V.; Steinman, R.M.; Nussenzweig, M.C. Dendritic cells induce peripheral t cell unresponsiveness under steady state conditions in vivo. J. Exp. Med. 2001, 194, 769–779. [Google Scholar]
- McMenamin, P.G.; Wealthall, R.J.; Deverall, M.; Cooper, S.J.; Griffin, B. Macrophages and dendritic cells in the rat meninges and choroid plexus: Three-dimensional localisation by environmental scanning electron microscopy and confocal microscopy. Cell Tissue Res. 2003, 313, 259–269. [Google Scholar]
- Quintana, E.; Fernandez, A.; Velasco, P.; de Andres, B.; Liste, I.; Sancho, D.; Gaspar, M.L.; Cano, E. Dngr-1(+) dendritic cells are located in meningeal membrane and choroid plexus of the noninjured brain. Glia 2015, 63, 2231–2248. [Google Scholar]
- Anandasabapathy, N.; Victora, G.D.; Meredith, M.; Feder, R.; Dong, B.; Kluger, C.; Yao, K.; Dustin, M.L.; Nussenzweig, M.C.; Steinman, R.M.; et al. Flt3l controls the development of radiosensitive dendritic cells in the meninges and choroid plexus of the steady-state mouse brain. J. Exp. Med. 2011, 208, 1695–1705. [Google Scholar]
- Hesske, L.; Vincenzetti, C.; Heikenwalder, M.; Prinz, M.; Reith, W.; Fontana, A.; Suter, T. Induction of inhibitory central nervous system-derived and stimulatory blood-derived dendritic cells suggests a dual role for granulocyte-macrophage colony-stimulating factor in central nervous system inflammation. Brain J. Neurol. 2010, 133, 1637–1654. [Google Scholar]
- Tsuchida, M.; Hanawa, H.; Hirahara, H.; Watanabe, H.; Matsumoto, Y.; Sekikawa, H.; Abo, T. Identification of cd4-cd8-alpha beta t cells in the subarachnoid space of rats with experimental autoimmune encephalomyelitis. A possible route by which effector cells invade the lesions. Immunology 1994, 81, 420–427. [Google Scholar]
- Bartholomaus, I.; Kawakami, N.; Odoardi, F.; Schlager, C.; Miljkovic, D.; Ellwart, J.W.; Klinkert, W.E.; Flugel-Koch, C.; Issekutz, T.B.; Wekerle, H.; et al. Effector t cell interactions with meningeal vascular structures in nascent autoimmune cns lesions. Nature 2009, 462, 94–98. [Google Scholar]
- Banchereau, J.; Steinman, R.M. Dendritic cells and the control of immunity. Nature 1998, 392, 245–252. [Google Scholar]
- Cools, N.; Ponsaerts, P.; Van Tendeloo, V.F.; Berneman, Z.N. Balancing between immunity and tolerance: An interplay between dendritic cells, regulatory T cells, and effector T cells. J. Leukoc. Biol. 2007, 82, 1365–1374. [Google Scholar]
- Cao, Y.; Goods, B.A.; Raddassi, K.; Nepom, G.T.; Kwok, W.W.; Love, J.C.; Hafler, D.A. Functional inflammatory profiles distinguish myelin-reactive T cells from patients with multiple sclerosis. Sci. Transl. Med. 2015, 7, 287ra74. [Google Scholar]
- Mbongue, J.; Nicholas, D.; Firek, A.; Langridge, W. The role of dendritic cells in tissue-specific autoimmunity. J. Immunol. Res. 2014, 2014, 857143. [Google Scholar]
- Ganguly, D.; Haak, S.; Sisirak, V.; Reizis, B. The role of dendritic cells in autoimmunity. Nat. Rev. Immunol. 2013, 13, 566–577. [Google Scholar]
- Stinissen, P.; Hellings, N. Activation of myelin reactive T cells in multiple sclerosis: A possible role for T cell degeneracy? Eur. J. Immunol. 2008, 38, 1190–1193. [Google Scholar]
- Robinson, A.P.; Harp, C.T.; Noronha, A.; Miller, S.D. The experimental autoimmune encephalomyelitis (EAE) model of MS: Utility for understanding disease pathophysiology and treatment. Handb. Clin. Neurol. 2014, 122, 173–189. [Google Scholar]
- Constantinescu, C.S.; Farooqi, N.; O’Brien, K.; Gran, B. Experimental autoimmune encephalomyelitis (EAE) as a model for multiple sclerosis (MS). Br. J. Pharmacol. 2011, 164, 1079–1106. [Google Scholar]
- Kretschmer, K.; Apostolou, I.; Hawiger, D.; Khazaie, K.; Nussenzweig, M.C.; von Boehmer, H. Inducing and expanding regulatory t cell populations by foreign antigen. Nat. Immunol. 2005, 6, 1219–1227. [Google Scholar]
- Goverman, J. Autoimmune t cell responses in the central nervous system. Nat. Rev. Immunol. 2009, 9, 393–407. [Google Scholar]
- Crawford, M.P.; Yan, S.X.; Ortega, S.B.; Mehta, R.S.; Hewitt, R.E.; Price, D.A.; Stastny, P.; Douek, D.C.; Koup, R.A.; Racke, M.K.; et al. High prevalence of autoreactive, neuroantigen-specific cd8+ t cells in multiple sclerosis revealed by novel flow cytometric assay. Blood 2004, 103, 4222–4231. [Google Scholar]
- Dardalhon, V.; Korn, T.; Kuchroo, V.K.; Anderson, A.C. Role of th1 and th17 cells in organ-specific autoimmunity. J. Autoimmun. 2008, 31, 252–256. [Google Scholar]
- Sapoznikov, A.; Jung, S. Probing in vivo dendritic cell functions by conditional cell ablation. Immunol. Cell Biol. 2008, 86, 409–415. [Google Scholar]
- Pobezinsky, L.A.; Angelov, G.S.; Tai, X.; Jeurling, S.; Van Laethem, F.; Feigenbaum, L.; Park, J.H.; Singer, A. Clonal deletion and the fate of autoreactive thymocytes that survive negative selection. Nat. Immunol. 2012, 13, 569–578. [Google Scholar]
- Sprent, J.; Webb, S.R. Intrathymic and extrathymic clonal deletion of t cells. Curr. Opin. Immunol. 1995, 7, 196–205. [Google Scholar]
- Marx, A.; Yamada, Y.; Simon-Keller, K.; Schalke, B.; Willcox, N.; Strobel, P.; Weis, C.A. Thymus and autoimmunity. Semin. Immunopathol. 2021, 43, 45–64. [Google Scholar]
- Brocker, T.; Riedinger, M.; Karjalainen, K. Targeted expression of major histocompatibility complex (mhc) class ii molecules demonstrates that dendritic cells can induce negative but not positive selection of thymocytes in vivo. J. Exp. Med. 1997, 185, 541–550. [Google Scholar]
- Phillips, B.E.; Garciafigueroa, Y.; Trucco, M.; Giannoukakis, N. Clinical tolerogenic dendritic cells: Exploring therapeutic impact on human autoimmune disease. Front. Immunol. 2017, 8, 1279. [Google Scholar]
- Wohlfert, E.; Belkaid, Y. Role of endogenous and induced regulatory t cells during infections. J. Clin. Immunol. 2008, 28, 707–715. [Google Scholar]
- Wakkach, A.; Fournier, N.; Brun, V.; Breittmayer, J.P.; Cottrez, F.; Groux, H. Characterization of dendritic cells that induce tolerance and t regulatory 1 cell differentiation in vivo. Immunity 2003, 18, 605–617. [Google Scholar]
- Gregori, S.; Tomasoni, D.; Pacciani, V.; Scirpoli, M.; Battaglia, M.; Magnani, C.F.; Hauben, E.; Roncarolo, M.G. Differentiation of type 1 t regulatory cells (tr1) by tolerogenic dc-10 requires the il-10-dependent ilt4/hla-g pathway. Blood 2010, 116, 935–944. [Google Scholar]
- Luckey, U.; Schmidt, T.; Pfender, N.; Romer, M.; Lorenz, N.; Martin, S.F.; Bopp, T.; Schmitt, E.; Nikolaev, A.; Yogev, N.; et al. Crosstalk of regulatory t cells and tolerogenic dendritic cells prevents contact allergy in subjects with low zone tolerance. J. Allergy Clin. Immunol. 2012, 130, 781–797.e11. [Google Scholar]
- Jonuleit, H.; Schmitt, E.; Schuler, G.; Knop, J.; Enk, A.H. Induction of interleukin 10-producing, nonproliferating cd4(+) t cells with regulatory properties by repetitive stimulation with allogeneic immature human dendritic cells. J. Exp. Med. 2000, 192, 1213–1222. [Google Scholar]
- Leone, D.A.; Rees, A.J.; Kain, R. Dendritic cells and routing cargo into exosomes. Immunol. Cell Biol. 2018. [Google Scholar] [CrossRef] [Green Version]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding light on the cell biology of extracellular vesicles. Nature reviews. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar]
- Kalluri, R.; LeBleu, V.S. The biology, function, and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar]
- Montecalvo, A.; Larregina, A.T.; Shufesky, W.J.; Stolz, D.B.; Sullivan, M.L.; Karlsson, J.M.; Baty, C.J.; Gibson, G.A.; Erdos, G.; Wang, Z.; et al. Mechanism of transfer of functional micrornas between mouse dendritic cells via exosomes. Blood 2012, 119, 756–766. [Google Scholar]
- Pang, X.L.; Wang, Z.G.; Liu, L.; Feng, Y.H.; Wang, J.X.; Xie, H.C.; Yang, X.L.; Li, J.F.; Feng, G.W. Immature dendritic cells derived exosomes promotes immune tolerance by regulating t cell differentiation in renal transplantation. Aging 2019, 11, 8911–8924. [Google Scholar]
- Wang, J.; Zhao, C.; Kong, P.; Bian, G.; Sun, Z.; Sun, Y.; Guo, L.; Li, B. Methylene blue alleviates experimental autoimmune encephalomyelitis by modulating ampk/sirt1 signaling pathway and th17/treg immune response. J. Neuroimmunol. 2016, 299, 45–52. [Google Scholar]
- Mastorodemos, V.; Ioannou, M.; Verginis, P. Cell-based modulation of autoimmune responses in multiple sclerosis and experimental autoimmmune encephalomyelitis: Therapeutic implications. Neuroimmunomodulation 2015, 22, 181–195. [Google Scholar]
- Boks, M.A.; Kager-Groenland, J.R.; Haasjes, M.S.; Zwaginga, J.J.; van Ham, S.M.; ten Brinke, A. Il-10-generated tolerogenic dendritic cells are optimal for functional regulatory t cell induction--a comparative study of human clinical-applicable dc. Clin. Immunol. 2012, 142, 332–342. [Google Scholar]
- Maldonado, R.A.; von Andrian, U.H. How tolerogenic dendritic cells induce regulatory t cells. Adv. Immunol. 2010, 108, 111–165. [Google Scholar]
- Mitchell, R.E.; Hassan, M.; Burton, B.R.; Britton, G.; Hill, E.V.; Verhagen, J.; Wraith, D.C. Il-4 enhances il-10 production in th1 cells: Implications for th1 and th2 regulation. Sci. Rep. 2017, 7, 11315. [Google Scholar]
- Ferrara, G.; Errede, M.; Girolamo, F.; Morando, S.; Ivaldi, F.; Panini, N.; Bendotti, C.; Perris, R.; Furlan, R.; Virgintino, D.; et al. Ng2, a common denominator for neuroinflammation, blood-brain barrier alteration, and oligodendrocyte precursor response in eae, plays a role in dendritic cell activation. Acta Neuropathol. 2016, 132, 23–42. [Google Scholar]
- Legutko, A.; Marichal, T.; Fievez, L.; Bedoret, D.; Mayer, A.; de Vries, H.; Klotz, L.; Drion, P.V.; Heirman, C.; Cataldo, D.; et al. Sirtuin 1 promotes th2 responses and airway allergy by repressing peroxisome proliferator-activated receptor-gamma activity in dendritic cells. J. Immunol. 2011, 187, 4517–4529. [Google Scholar]
- Toda, A.; Terawaki, K.; Yamazaki, S.; Saeki, K.; Shimizu, T.; Yokomizo, T. Attenuated th1 induction by dendritic cells from mice deficient in the leukotriene b4 receptor 1. Biochimie 2010, 92, 682–691. [Google Scholar]
- Li, H.; Zhang, G.X.; Chen, Y.; Xu, H.; Fitzgerald, D.C.; Zhao, Z.; Rostami, A. Cd11c+cd11b+ dendritic cells play an important role in intravenous tolerance and the suppression of experimental autoimmune encephalomyelitis. J. Immunol. 2008, 181, 2483–2493. [Google Scholar]
- Kenison, J.E.; Jhaveri, A.; Li, Z.; Khadse, N.; Tjon, E.; Tezza, S.; Nowakowska, D.; Plasencia, A.; Stanton, V.P., Jr.; Sherr, D.H.; et al. Tolerogenic nanoparticles suppress central nervous system inflammation. Proc. Natl. Acad. Sci. USA 2020, 117, 32017–32028. [Google Scholar]
- Benkhoucha, M.; Santiago-Raber, M.L.; Schneiter, G.; Chofflon, M.; Funakoshi, H.; Nakamura, T.; Lalive, P.H. Hepatocyte growth factor inhibits cns autoimmunity by inducing tolerogenic dendritic cells and cd25+foxp3+ regulatory t cells. Proc. Natl. Acad. Sci. USA 2010, 107, 6424–6429. [Google Scholar]
- Kim, R.Y.; Mangu, D.; Hoffman, A.S.; Kavosh, R.; Jung, E.; Itoh, N.; Voskuhl, R. Oestrogen receptor β ligand acts on cd11c+ cells to mediate protection in experimental autoimmune encephalomyelitis. Brain J. Neurol. 2018, 141, 132–147. [Google Scholar]
- Zhang, X.; Jin, J.; Tang, Y.; Speer, D.; Sujkowska, D.; Markovic-Plese, S. Ifn-beta1a inhibits the secretion of th17-polarizing cytokines in human dendritic cells via tlr7 up-regulation. J. Immunol. 2009, 182, 3928–3936. [Google Scholar]
- Pellegrini, P.; Totaro, R.; Contasta, I.; Berghella, A.M.; Russo, T.; Carolei, A.; Adorno, D. Ifnbeta-1a treatment and reestablishment of th1 regulation in ms patients: Dose effects. Clin. Neuropharmacol. 2004, 27, 258–269. [Google Scholar]
- Ramgolam, V.S.; Sha, Y.; Jin, J.; Zhang, X.; Markovic-Plese, S. Ifn-beta inhibits human th17 cell differentiation. J. Immunol. 2009, 183, 5418–5427. [Google Scholar]
- Durelli, L.; Conti, L.; Clerico, M.; Boselli, D.; Contessa, G.; Ripellino, P.; Ferrero, B.; Eid, P.; Novelli, F. T-helper 17 cells expand in multiple sclerosis and are inhibited by interferon-beta. Ann. Neurol. 2009, 65, 499–509. [Google Scholar]
- Axtell, R.C.; de Jong, B.A.; Boniface, K.; van der Voort, L.F.; Bhat, R.; De Sarno, P.; Naves, R.; Han, M.; Zhong, F.; Castellanos, J.G.; et al. T helper type 1 and 17 cells determine efficacy of interferon-beta in multiple sclerosis and experimental encephalomyelitis. Nat. Med. 2010, 16, 406–412. [Google Scholar]
- Aung, L.L.; Fitzgerald-Bocarsly, P.; Dhib-Jalbut, S.; Balashov, K. Plasmacytoid dendritic cells in multiple sclerosis: Chemokine and chemokine receptor modulation by interferon-beta. J. Neuroimmunol. 2010, 226, 158–164. [Google Scholar]
- Paik, J. Diroximel fumarate in relapsing forms of multiple sclerosis: A profile of its use. CNS Drugs 2021, 35, 691–700. [Google Scholar]
- Kraus, S.H.; Luessi, F.; Trinschek, B.; Lerch, S.; Hubo, M.; Poisa-Beiro, L.; Paterka, M.; Jonuleit, H.; Zipp, F.; Jolivel, V. Cladribine exerts an immunomodulatory effect on human and murine dendritic cells. Int. Immunopharmacol. 2014, 18, 347–357. [Google Scholar]
- Mitosek-Szewczyk, K.; Tabarkiewicz, J.; Wilczynska, B.; Lobejko, K.; Berbecki, J.; Nastaj, M.; Dworzanska, E.; Kolodziejczyk, B.; Stelmasiak, Z.; Rolinski, J. Impact of cladribine therapy on changes in circulating dendritic cell subsets, t cells and b cells in patients with multiple sclerosis. J. Neurol. Sci. 2013, 332, 35–40. [Google Scholar]
- Kim, H.J.; Ifergan, I.; Antel, J.P.; Seguin, R.; Duddy, M.; Lapierre, Y.; Jalili, F.; Bar-Or, A. Type 2 monocyte and microglia differentiation mediated by glatiramer acetate therapy in patients with multiple sclerosis. J. Immunol. 2004, 172, 7144–7153. [Google Scholar]
- Weber, M.S.; Prod’homme, T.; Youssef, S.; Dunn, S.E.; Rundle, C.D.; Lee, L.; Patarroyo, J.C.; Stuve, O.; Sobel, R.A.; Steinman, L.; et al. Type ii monocytes modulate t cell-mediated central nervous system autoimmune disease. Nat. Med. 2007, 13, 935–943. [Google Scholar]
- Burger, D.; Molnarfi, N.; Weber, M.S.; Brandt, K.J.; Benkhoucha, M.; Gruaz, L.; Chofflon, M.; Zamvil, S.S.; Lalive, P.H. Glatiramer acetate increases il-1 receptor antagonist but decreases t cell-induced il-1beta in human monocytes and multiple sclerosis. Proc. Natl. Acad. Sci. USA 2009, 106, 4355–4359. [Google Scholar]
- Stuve, O.; Marra, C.M.; Jerome, K.R.; Cook, L.; Cravens, P.D.; Cepok, S.; Frohman, E.M.; Phillips, J.T.; Arendt, G.; Hemmer, B.; et al. Immune surveillance in multiple sclerosis patients treated with natalizumab. Ann. Neurol. 2006, 59, 743–747. [Google Scholar]
- del Pilar Martin, M.; Cravens, P.D.; Winger, R.; Frohman, E.M.; Racke, M.K.; Eagar, T.N.; Zamvil, S.S.; Weber, M.S.; Hemmer, B.; Karandikar, N.J.; et al. Decrease in the numbers of dendritic cells and cd4+ t cells in cerebral perivascular spaces due to natalizumab. Arch. Neurol. 2008, 65, 1596–1603. [Google Scholar]
- de Andres, C.; Teijeiro, R.; Alonso, B.; Sanchez-Madrid, F.; Martinez, M.L.; Guzman de Villoria, J.; Fernandez-Cruz, E.; Sanchez-Ramon, S. Long-term decrease in vla-4 expression and functional impairment of dendritic cells during natalizumab therapy in patients with multiple sclerosis. PLoS ONE 2012, 7, e34103. [Google Scholar]
- Lamb, Y.N. Ocrelizumab: A review in multiple sclerosis. Drugs 2022, 82, 323–334. [Google Scholar]
- Gross, C.C.; Ahmetspahic, D.; Ruck, T.; Schulte-Mecklenbeck, A.; Schwarte, K.; Jorgens, S.; Scheu, S.; Windhagen, S.; Graefe, B.; Melzer, N.; et al. Alemtuzumab treatment alters circulating innate immune cells in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2016, 3, e289. [Google Scholar]
- Zeng, X.; Wang, T.; Zhu, C.; Xing, X.; Ye, Y.; Lai, X.; Song, B.; Zeng, Y. Topographical and biological evidence revealed fty720-mediated anergy-polarization of mouse bone marrow-derived dendritic cells in vitro. PLoS ONE 2012, 7, e34830. [Google Scholar]
- Lan, Y.Y.; De Creus, A.; Colvin, B.L.; Abe, M.; Brinkmann, V.; Coates, P.T.; Thomson, A.W. The sphingosine-1-phosphate receptor agonist fty720 modulates dendritic cell trafficking in vivo. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2005, 5, 2649–2659. [Google Scholar]
- Kuczynski, A.M.; Oh, J. Ozanimod for the treatment of relapsing forms of multiple sclerosis. Neurodegener. Dis. Manag. 2021, 11, 207–220. [Google Scholar]
- McRae, B.L.; Semnani, R.T.; Hayes, M.P.; van Seventer, G.A. Type i ifns inhibit human dendritic cell il-12 production and th1 cell development. J. Immunol. 1998, 160, 4298–4304. [Google Scholar]
- Polman, C.H.; O’Connor, P.W.; Havrdova, E.; Hutchinson, M.; Kappos, L.; Miller, D.H.; Phillips, J.T.; Lublin, F.D.; Giovannoni, G.; Wajgt, A.; et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N. Engl. J. Med. 2006, 354, 899–910. [Google Scholar]
- Moraes, A.S.; Boldrini, V.O.; Dionete, A.C.; Andrade, M.D.; Longhini, A.L.F.; Santos, I.; Lima, A.D.R.; Silva, V.; Dias Carneiro, R.P.C.; Quintiliano, R.P.S.; et al. Decreased neurofilament l chain levels in cerebrospinal fluid and tolerogenic plasmacytoid dendritic cells in natalizumab-treated multiple sclerosis patients-brief research report. Front. Cell. Neurosci. 2021, 15, 705618. [Google Scholar]
- Dominguez-Villar, M.; Raddassi, K.; Danielsen, A.C.; Guarnaccia, J.; Hafler, D.A. Fingolimod modulates t cell phenotype and regulatory t cell plasticity in vivo. J. Autoimmun. 2019, 96, 40–49. [Google Scholar]
- Thomas, K.; Sehr, T.; Proschmann, U.; Rodriguez-Leal, F.A.; Haase, R.; Ziemssen, T. Fingolimod additionally acts as immunomodulator focused on the innate immune system beyond its prominent effects on lymphocyte recirculation. J. Neuroinflamm. 2017, 14, 41. [Google Scholar]
- Luessi, F.; Kraus, S.; Trinschek, B.; Lerch, S.; Ploen, R.; Paterka, M.; Roberg, T.; Poisa-Beiro, L.; Klotz, L.; Wiendl, H.; et al. Fty720 (fingolimod) treatment tips the balance towards less immunogenic antigen-presenting cells in patients with multiple sclerosis. Mult. Scler. 2015, 21, 1811–1822. [Google Scholar]
- Di Dario, M.; Colombo, E.; Govi, C.; De Feo, D.; Messina, M.J.; Romeo, M.; Sangalli, F.; Moiola, L.; Rodegher, M.; Martino, G.; et al. Myeloid cells as target of fingolimod action in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e157. [Google Scholar]
- Sadiq, S.A.; Puccio, L.M.; Brydon, E.W. Jcv detection in multiple sclerosis patients treated with natalizumab. J. Neurol. 2010, 257, 954–958. [Google Scholar]
- Walczak, A.; Siger, M.; Ciach, A.; Szczepanik, M.; Selmaj, K. Transdermal application of myelin peptides in multiple sclerosis treatment. JAMA Neurol. 2013, 70, 1105–1109. [Google Scholar]
- Streeter, H.B.; Rigden, R.; Martin, K.F.; Scolding, N.J.; Wraith, D.C. Preclinical development and first-in-human study of atx-ms-1467 for immunotherapy of ms. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e93. [Google Scholar]
- Jurynczyk, M.; Walczak, A.; Jurewicz, A.; Jesionek-Kupnicka, D.; Szczepanik, M.; Selmaj, K. Immune regulation of multiple sclerosis by transdermally applied myelin peptides. Ann. Neurol. 2010, 68, 593–601. [Google Scholar]
- Kaushansky, N.; Kerlero de Rosbo, N.; Zilkha-Falb, R.; Yosef-Hemo, R.; Cohen, L.; Ben-Nun, A. ‘Multi-epitope-targeted’ immune-specific therapy for a multiple sclerosis-like disease via engineered multi-epitope protein is superior to peptides. PLoS ONE 2011, 6, e27860. [Google Scholar]
- Smolen, J.S.; Beaulieu, A.; Rubbert-Roth, A.; Ramos-Remus, C.; Rovensky, J.; Alecock, E.; Woodworth, T.; Alten, R.; Investigators, O. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (option study): A double-blind, placebo-controlled, randomised trial. Lancet 2008, 371, 987–997. [Google Scholar]
- Deiss, A.; Brecht, I.; Haarmann, A.; Buttmann, M. Treating multiple sclerosis with monoclonal antibodies: A 2013 update. Expert Rev. Neurother. 2013, 13, 313–335. [Google Scholar]
- Constantinescu, C.S.; Asher, A.; Fryze, W.; Kozubski, W.; Wagner, F.; Aram, J.; Tanasescu, R.; Korolkiewicz, R.P.; Dirnberger-Hertweck, M.; Steidl, S.; et al. Randomized phase 1b trial of mor103, a human antibody to gm-csf, in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e117. [Google Scholar]
- Chen, S.; Zhou, J.; Cai, Y.; Zheng, X.; Xie, S.; Liao, Y.; Zhu, Y.; Qin, C.; Lai, W.; Yang, C.; et al. Discovery of bvdu as a promising drug for autoimmune diseases therapy by dendritic-cell-based functional screening. Sci. Rep. 2017, 7, 43820. [Google Scholar]
- Hawiger, D.; Masilamani, R.F.; Bettelli, E.; Kuchroo, V.K.; Nussenzweig, M.C. Immunological unresponsiveness characterized by increased expression of cd5 on peripheral t cells induced by dendritic cells in vivo. Immunity 2004, 20, 695–705. [Google Scholar]
- Jones, A.; Bourque, J.; Kuehm, L.; Opejin, A.; Teague, R.M.; Gross, C.; Hawiger, D. Immunomodulatory functions of btla and hvem govern induction of extrathymic regulatory t cells and tolerance by dendritic cells. Immunity 2016, 45, 1066–1077. [Google Scholar]
- Idoyaga, J.; Cheong, C.; Suda, K.; Suda, N.; Kim, J.Y.; Lee, H.; Park, C.G.; Steinman, R.M. Cutting edge: Langerin/cd207 receptor on dendritic cells mediates efficient antigen presentation on mhc i and ii products in vivo. J. Immunol. 2008, 180, 3647–3650. [Google Scholar]
- Hemmi, H.; Zaidi, N.; Wang, B.; Matos, I.; Fiorese, C.; Lubkin, A.; Zbytnuik, L.; Suda, K.; Zhang, K.; Noda, M.; et al. Treml4, an ig superfamily member, mediates presentation of several antigens to t cells in vivo, including protective immunity to her2 protein. J. Immunol. 2012, 188, 1147–1155. [Google Scholar]
- Joffre, O.P.; Sancho, D.; Zelenay, S.; Keller, A.M.; Reis e Sousa, C. Efficient and versatile manipulation of the peripheral cd4+ t-cell compartment by antigen targeting to dngr-1/clec9a. Eur. J. Immunol. 2010, 40, 1255–1265. [Google Scholar]
- Dudziak, D.; Kamphorst, A.O.; Heidkamp, G.F.; Buchholz, V.R.; Trumpfheller, C.; Yamazaki, S.; Cheong, C.; Liu, K.; Lee, H.W.; Park, C.G.; et al. Differential antigen processing by dendritic cell subsets in vivo. Science 2007, 315, 107–111. [Google Scholar]
- Loschko, J.; Heink, S.; Hackl, D.; Dudziak, D.; Reindl, W.; Korn, T.; Krug, A.B. Antigen targeting to plasmacytoid dendritic cells via siglec-h inhibits th cell-dependent autoimmunity. J. Immunol. 2011, 187, 6346–6356. [Google Scholar]
- Loschko, J.; Schlitzer, A.; Dudziak, D.; Drexler, I.; Sandholzer, N.; Bourquin, C.; Reindl, W.; Krug, A.B. Antigen delivery to plasmacytoid dendritic cells via bst2 induces protective t cell-mediated immunity. J. Immunol. 2011, 186, 6718–6725. [Google Scholar]
- Gross, C.C.; Jonuleit, H.; Wiendl, H. Fulfilling the dream: Tolerogenic dendritic cells to treat multiple sclerosis. Eur. J. Immunol. 2012, 42, 569–572. [Google Scholar]
- Kim, S.H.; Jung, H.H.; Lee, C.K. Generation, characteristics and clinical trials of ex vivo generated tolerogenic dendritic cells. Yonsei Med. J. 2018, 59, 807–815. [Google Scholar]
- Getts, D.R.; Shea, L.D.; Miller, S.D.; King, N.J. Harnessing nanoparticles for immune modulation. Trends Immunol. 2015, 36, 419–427. [Google Scholar]
- Kishimoto, T.K.; Ferrari, J.D.; LaMothe, R.A.; Kolte, P.N.; Griset, A.P.; O’Neil, C.; Chan, V.; Browning, E.; Chalishazar, A.; Kuhlman, W.; et al. Improving the efficacy and safety of biologic drugs with tolerogenic nanoparticles. Nat. Nanotechnol. 2016, 11, 890–899. [Google Scholar]
- Hunter, Z.; McCarthy, D.P.; Yap, W.T.; Harp, C.T.; Getts, D.R.; Shea, L.D.; Miller, S.D. A biodegradable nanoparticle platform for the induction of antigen-specific immune tolerance for treatment of autoimmune disease. ACS Nano 2014, 8, 2148–2160. [Google Scholar]
- Maldonado, R.A.; LaMothe, R.A.; Ferrari, J.D.; Zhang, A.H.; Rossi, R.J.; Kolte, P.N.; Griset, A.P.; O’Neil, C.; Altreuter, D.H.; Browning, E.; et al. Polymeric synthetic nanoparticles for the induction of antigen-specific immunological tolerance. Proc. Natl. Acad. Sci. USA 2015, 112, E156–E165. [Google Scholar]
- Cappellano, G.; Woldetsadik, A.D.; Orilieri, E.; Shivakumar, Y.; Rizzi, M.; Carniato, F.; Gigliotti, C.L.; Boggio, E.; Clemente, N.; Comi, C.; et al. Subcutaneous inverse vaccination with plga particles loaded with a mog peptide and il-10 decreases the severity of experimental autoimmune encephalomyelitis. Vaccine 2014, 32, 5681–5689. [Google Scholar]
- Caminschi, I.; Proietto, A.I.; Ahmet, F.; Kitsoulis, S.; Shin Teh, J.; Lo, J.C.; Rizzitelli, A.; Wu, L.; Vremec, D.; van Dommelen, S.L.; et al. The dendritic cell subtype-restricted c-type lectin clec9a is a target for vaccine enhancement. Blood 2008, 112, 3264–3273. [Google Scholar]
- Petzold, C.; Schallenberg, S.; Stern, J.N.; Kretschmer, K. Targeted antigen delivery to dec-205(+) dendritic cells for tolerogenic vaccination. Rev. Diabet. Stud. 2012, 9, 305–318. [Google Scholar]
- Ufer, F.; Vargas, P.; Engler, J.B.; Tintelnot, J.; Schattling, B.; Winkler, H.; Bauer, S.; Kursawe, N.; Willing, A.; Keminer, O.; et al. Arc/Arg3.1 governs inflammatory dendritic cell migration from the skin and thereby controls T cell activation. Sci. Immunol. 2016, 1, eaaf8665. [Google Scholar]
- Ji, Z.; Liu, G.H.; Qu, J. Mitochondrial sirtuins, metabolism, and aging. J. Genet. Genom. 2021. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, S.W.; Kim, H.Y.; Lee, S.Y.; Lee, W.S.; Hong, K.W.; Kim, C.D. SIRT1 inhibits differentiation of monocytes to macrophages: Amelioration of synovial inflammation in rheumatoid arthritis. J. Mol. Med. 2016, 94, 921–931. [Google Scholar]
- Kitada, M.; Ogura, Y.; Koya, D. The protective role of Sirt1 in vascular tissue: Its relationship to vascular aging and atherosclerosis. Aging 2016, 8, 2290–2307. [Google Scholar]
- Cheresh, P.; Kim, S.J.; Jablonski, R.; Watanabe, S.; Lu, Z.; Chi, M.; Helmin, K.A.; Gius, D.; Budinger, G.R.S.; Kamp, D.W. SIRT3 Overexpression Ameliorates Asbestos-Induced Pulmonary Fibrosis, mt-DNA Damage, and Lung Fibrogenic Monocyte Recruitment. Int. J. Mol. Sci. 2021, 22, 6856. [Google Scholar]
- Xi, J.; Chen, Y.; Jing, J.; Zhang, Y.; Liang, C.; Hao, Z.; Zhang, L. Sirtuin 3 suppresses the formation of renal calcium oxalate crystals through promoting M2 polarization of macrophages. J. Cell. Physiol. 2019, 234, 11463–11473. [Google Scholar]
- Liu, P.; Huang, G.; Wei, T.; Gao, J.; Huang, C.; Sun, M.; Zhu, L.; Shen, W. Sirtuin 3-induced macrophage autophagy in regulating NLRP3 inflammasome activation. Biochim. Biophys. Acta-Mol. Basis Dis. 2018, 1864, 764–777. [Google Scholar]
- Zou, Y.; Zhang, J.; Xu, J.; Fu, L.; Xu, Y.; Wang, X.; Li, Z.; Zhu, L.; Sun, H.; Zheng, H.; et al. SIRT6 inhibition delays peripheral nerve recovery by suppressing migration, phagocytosis and M2-polarization of macrophages. Cell Biosci. 2021, 11, 210. [Google Scholar]
- Ji, L.; Chen, Y.; Wang, H.; Zhang, W.; He, L.; Wu, J.; Liu, Y. Overexpression of Sirt6 promotes M2 macrophage transformation, alleviating renal injury in diabetic nephropathy. Int. J. Oncol. 2019, 55, 103–115. [Google Scholar]
- Woo, S.J.; Noh, H.S.; Lee, N.Y.; Cheon, Y.H.; Yi, S.M.; Jeon, H.M.; Bae, E.J.; Lee, S.I.; Park, B.H. Myeloid sirtuin 6 deficiency accelerates experimental rheumatoid arthritis by enhancing macrophage activation and infiltration into synovium. eBioMedicine 2018, 38, 228–237. [Google Scholar]
- Liu, G.; Bi, Y.; Xue, L.; Zhang, Y.; Yang, H.; Chen, X.; Lu, Y.; Zhang, Z.; Liu, H.; Wang, X.; et al. Dendritic cell sirt1-hif1alpha axis programs the differentiation of cd4+ t cells through il-12 and tgf-beta1. Proc. Natl. Acad. Sci. USA 2015, 112, E957–E965. [Google Scholar]
- Woo, S.J.; Lee, S.M.; Lim, H.S.; Hah, Y.S.; Jung, I.D.; Park, Y.M.; Kim, H.O.; Cheon, Y.H.; Jeon, M.G.; Jang, K.Y.; et al. Myeloid deletion of sirt1 suppresses collagen-induced arthritis in mice by modulating dendritic cell maturation. Exp. Mol. Med. 2016, 48, e221. [Google Scholar]
- Lasiglie, D.; Boero, S.; Bauer, I.; Morando, S.; Damonte, P.; Cea, M.; Monacelli, F.; Odetti, P.; Ballestrero, A.; Uccelli, A.; et al. Sirt6 regulates dendritic cell differentiation, maturation, and function. Aging 2016, 8, 34–49. [Google Scholar]
- Ferrara, G.; Benzi, A.; Sturla, L.; Marubbi, D.; Frumento, D.; Spinelli, S.; Abbotto, E.; Ivaldi, F.; von Holtey, M.; Murone, M.; et al. Sirt6 inhibition delays the onset of experimental autoimmune encephalomyelitis by reducing dendritic cell migration. J. Neuroinflamm. 2020, 17, 228. [Google Scholar]
- Jiang, H.; Khan, S.; Wang, Y.; Charron, G.; He, B.; Sebastian, C.; Du, J.; Kim, R.; Ge, E.; Mostoslavsky, R.; et al. Sirt6 regulates tnf-alpha secretion through hydrolysis of long-chain fatty acyl lysine. Nature 2013, 496, 110–113. [Google Scholar]
- Bauer, I.; Grozio, A.; Lasiglie, D.; Basile, G.; Sturla, L.; Magnone, M.; Sociali, G.; Soncini, D.; Caffa, I.; Poggi, A.; et al. The nad+-dependent histone deacetylase sirt6 promotes cytokine production and migration in pancreatic cancer cells by regulating ca2+ responses. J. Biol. Chem. 2012, 287, 40924–40937. [Google Scholar]
- Merad, M.; Sathe, P.; Helft, J.; Miller, J.; Mortha, A. The dendritic cell lineage: Ontogeny and function of dendritic cells and their subsets in the steady state and the inflamed setting. Annu. Rev. Immunol. 2013, 31, 563–604. [Google Scholar]
- Caux, C.; Dezutter-Dambuyant, C.; Schmitt, D.; Banchereau, J. Gm-csf and tnf-alpha cooperate in the generation of dendritic langerhans cells. Nature 1992, 360, 258–261. [Google Scholar]
- Yamaguchi, Y.; Tsumura, H.; Miwa, M.; Inaba, K. Contrasting effects of tgf-beta 1 and tnf-alpha on the development of dendritic cells from progenitors in mouse bone marrow. Stem Cells 1997, 15, 144–153. [Google Scholar]
- Parodi, B.; Rossi, S.; Morando, S.; Cordano, C.; Bragoni, A.; Motta, C.; Usai, C.; Wipke, B.T.; Scannevin, R.H.; Mancardi, G.L.; et al. Fumarates modulate microglia activation through a novel hcar2 signaling pathway and rescue synaptic dysregulation in inflamed cns. Acta Neuropathol. 2015, 130, 279–295. [Google Scholar]
- Yan, J.; Luo, A.; Gao, J.; Tang, X.; Zhao, Y.; Zhou, B.; Zhou, Z.; Li, S. The role of SIRT1 in neuroinflammation and cognitive dysfunction in aged rats after anesthesia and surgery. Am. J. Transl. Res. 2019, 11, 1555–1568. [Google Scholar]
- Xie, J.; Zhang, X.; Zhang, L. Negative regulation of inflammation by SIRT1. Pharmacol. Res. 2013, 67, 60–67. [Google Scholar]
- Li, L.; Sun, Q.; Li, Y.; Yang, Y.; Yang, Y.; Chang, T.; Man, M.; Zheng, L. Overexpression of SIRT1 Induced by Resveratrol and Inhibitor of miR-204 Suppresses Activation and Proliferation of Microglia. J. Mol. Neurosci. 2015, 56, 858–867. [Google Scholar]
- Qian, Y.; Xin, Z.; Lv, Y.; Wang, Z.; Zuo, L.; Huang, X.; Li, Y.; Xin, H.B. Asiatic acid suppresses neuroinflammation in BV2 microglia via modulation of the Sirt1/NF-kappaB signaling pathway. Food Funct. 2018, 9, 1048–1057. [Google Scholar]
- Chen, H.; Ji, H.; Zhang, M.; Liu, Z.; Lao, L.; Deng, C.; Chen, J.; Zhong, G. An Agonist of the Protective Factor SIRT1 Improves Functional Recovery and Promotes Neuronal Survival by Attenuating Inflammation after Spinal Cord Injury. J. Neurosci. 2017, 37, 2916–2930. [Google Scholar]
- Dolati, S.; Aghebati-Maleki, L.; Ahmadi, M.; Marofi, F.; Babaloo, Z.; Ayramloo, H.; Jafarisavari, Z.; Oskouei, H.; Afkham, A.; Younesi, V.; et al. Nanocurcumin restores aberrant mirna expression profile in multiple sclerosis, randomized, double-blind, placebo-controlled trial. J. Cell. Physiol. 2018, 233, 5222–5230. [Google Scholar]
- Nimmagadda, V.K.; Bever, C.T.; Vattikunta, N.R.; Talat, S.; Ahmad, V.; Nagalla, N.K.; Trisler, D.; Judge, S.I.; Royal, W., 3rd; Chandrasekaran, K.; et al. Overexpression of sirt1 protein in neurons protects against experimental autoimmune encephalomyelitis through activation of multiple sirt1 targets. J. Immunol. 2013, 190, 4595–4607. [Google Scholar]
- Tegla, C.A.; Azimzadeh, P.; Andrian-Albescu, M.; Martin, A.; Cudrici, C.D.; Trippe, R., 3rd; Sugarman, A.; Chen, H.; Boodhoo, D.; Vlaicu, S.I.; et al. Sirt1 is decreased during relapses in patients with multiple sclerosis. Exp. Mol. Pathol. 2014, 96, 139–148. [Google Scholar]
- Martin, A.; Tegla, C.A.; Cudrici, C.D.; Kruszewski, A.M.; Azimzadeh, P.; Boodhoo, D.; Mekala, A.P.; Rus, V.; Rus, H. Role of sirt1 in autoimmune demyelination and neurodegeneration. Immunol. Res. 2015, 61, 187–197. [Google Scholar]
- Tatomir, A.; Rao, G.; Boodhoo, D.; Ciriello, J.; Rus, V.; Rus, H. Histone Deacetylase SIRT1 Mediates C5b-9-Induced Cell Cycle in Oligodendrocytes. Front Immunol. 2020, 11, 619. [Google Scholar]
- Prozorovski, T.; Ingwersen, J.; Lukas, D.; Gottle, P.; Koop, B.; Graf, J.; Schneider, R.; Franke, K.; Schumacher, S.; Britsch, S.; et al. Regulation of sirtuin expression in autoimmune neuroinflammation: Induction of sirt1 in oligodendrocyte progenitor cells. Neurosci. Lett. 2019, 704, 116–125. [Google Scholar]
- Rafalski, V.A.; Ho, P.P.; Brett, J.O.; Ucar, D.; Dugas, J.C.; Pollina, E.A.; Chow, L.M.; Ibrahim, A.; Baker, S.J.; Barres, B.A.; et al. Expansion of oligodendrocyte progenitor cells following sirt1 inactivation in the adult brain. Nat. Cell Biol. 2013, 15, 614–624. [Google Scholar]
- Lim, H.W.; Kang, S.G.; Ryu, J.K.; Schilling, B.; Fei, M.; Lee, I.S.; Kehasse, A.; Shirakawa, K.; Yokoyama, M.; Schnolzer, M.; et al. Sirt1 deacetylates rorgammat and enhances th17 cell generation. J. Exp. Med. 2015, 212, 607–617. [Google Scholar]
- Sato, F.; Martinez, N.E.; Shahid, M.; Rose, J.W.; Carlson, N.G.; Tsunoda, I. Resveratrol exacerbates both autoimmune and viral models of multiple sclerosis. Am. J. Pathol. 2013, 183, 1390–1396. [Google Scholar]
- Guo, J.; Wang, J.; Guo, R.; Shao, H.; Guo, L. Pterostilbene protects the optic nerves and retina in a murine model of experimental autoimmune encephalomyelitis via activation of sirt1 signaling. Neuroscience 2022, 487, 35–46. [Google Scholar]
- Guo, J.; Li, B.; Wang, J.; Guo, R.; Tian, Y.; Song, S.; Guo, L. Protective effect and mechanism of nicotinamide adenine dinucleotide against optic neuritis in mice with experimental autoimmune encephalomyelitis. Int. Immunopharmacol. 2021, 98, 107846. [Google Scholar]
- Liu, C.; Zhang, N.; Zhang, R.; Jin, L.; Petridis, A.K.; Loers, G.; Zheng, X.; Wang, Z.; Siebert, H.C. Cuprizone-induced demyelination in mouse hippocampus is alleviated by ketogenic diet. J. Agric. Food Chem. 2020, 68, 11215–11228. [Google Scholar]
- Giacometti, J.; Grubic-Kezele, T. Olive leaf polyphenols attenuate the clinical course of experimental autoimmune encephalomyelitis and provide neuroprotection by reducing oxidative stress, regulating microglia and sirt1, and preserving myelin integrity. Oxidative Med. Cell. Longev. 2020, 2020, 6125638. [Google Scholar]
- Elbaz, E.M.; Senousy, M.A.; El-Tanbouly, D.M.; Sayed, R.H. Neuroprotective effect of linagliptin against cuprizone-induced demyelination and behavioural dysfunction in mice: A pivotal role of ampk/sirt1 and jak2/stat3/nf-kappab signalling pathway modulation. Toxicol. Appl. Pharmacol. 2018, 352, 153–161. [Google Scholar]
- Khan, R.S.; Dine, K.; Das Sarma, J.; Shindler, K.S. Sirt1 activating compounds reduce oxidative stress mediated neuronal loss in viral induced cns demyelinating disease. Acta Neuropathol. Commun. 2014, 2, 3. [Google Scholar]
- Shindler, K.S.; Ventura, E.; Rex, T.S.; Elliott, P.; Rostami, A. Sirt1 activation confers neuroprotection in experimental optic neuritis. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3602–3609. [Google Scholar]
- Shindler, K.S.; Ventura, E.; Dutt, M.; Elliott, P.; Fitzgerald, D.C.; Rostami, A. Oral resveratrol reduces neuronal damage in a model of multiple sclerosis. J. Neuro-Ophthalmol. Off. J. North Am. Neuro-Ophthalmol. Soc. 2010, 30, 328–339. [Google Scholar]
- Pais, T.F.; Szegő, É.M.; Marques, O.; Miller-Fleming, L.; Antas, P.; Guerreiro, P.; de Oliveira, R.M.; Kasapoglu, B.; Outeiro, T.F. The NAD-dependent deacetylase sirtuin 2 is a suppressor of microglial activation and brain inflammation. EMBO J. 2013, 32, 2603–2616. [Google Scholar]
- Wang, B.; Zhang, Y.; Cao, W.; Wei, X.; Chen, J.; Ying, W. SIRT2 Plays Significant Roles in Lipopolysaccharides-Induced Neuroinflammation and Brain Injury in Mice. Neurochem. Res. 2016, 41, 2490–2500. [Google Scholar]
- Zhou, D.; Jiang, Y. Sirtuin 3 attenuates neuroinflammation-induced apoptosis in BV-2 microglia. Aging 2019, 11, 9075–9089. [Google Scholar]
- Parenti, M.D.; Grozio, A.; Bauer, I.; Galeno, L.; Damonte, P.; Millo, E.; Sociali, G.; Franceschi, C.; Ballestrero, A.; Bruzzone, S.; et al. Discovery of novel and selective sirt6 inhibitors. J. Med. Chem. 2014, 57, 4796–4804. [Google Scholar]
- Sociali, G.; Galeno, L.; Parenti, M.D.; Grozio, A.; Bauer, I.; Passalacqua, M.; Boero, S.; Donadini, A.; Millo, E.; Bellotti, M.; et al. Quinazolinedione sirt6 inhibitors sensitize cancer cells to chemotherapeutics. Eur. J. Med. Chem. 2015, 102, 530–539. [Google Scholar]
- Damonte, P.; Sociali, G.; Parenti, M.D.; Soncini, D.; Bauer, I.; Boero, S.; Grozio, A.; Holtey, M.V.; Piacente, F.; Becherini, P.; et al. Sirt6 inhibitors with salicylate-like structure show immunosuppressive and chemosensitizing effects. Bioorganic Med. Chem. 2017, 25, 5849–5858. [Google Scholar]
- Sociali, G.; Magnone, M.; Ravera, S.; Damonte, P.; Vigliarolo, T.; Von Holtey, M.; Vellone, V.G.; Millo, E.; Caffa, I.; Cea, M.; et al. Pharmacological sirt6 inhibition improves glucose tolerance in a type 2 diabetes mouse model. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2017, 31, 3138–3149. [Google Scholar]
- Van Gool, F.; Galli, M.; Gueydan, C.; Kruys, V.; Prevot, P.P.; Bedalov, A.; Mostoslavsky, R.; Alt, F.W.; De Smedt, T.; Leo, O. Intracellular nad levels regulate tumor necrosis factor protein synthesis in a sirtuin-dependent manner. Nat. Med. 2009, 15, 206–210. [Google Scholar]
- Bruzzone, S.; Fruscione, F.; Morando, S.; Ferrando, T.; Poggi, A.; Garuti, A.; D’Urso, A.; Selmo, M.; Benvenuto, F.; Cea, M.; et al. Catastrophic nad+ depletion in activated t lymphocytes through nampt inhibition reduces demyelination and disability in eae. PLoS ONE 2009, 4, e7897. [Google Scholar]
- Montecucco, F.; Bauer, I.; Braunersreuther, V.; Bruzzone, S.; Akhmedov, A.; Luscher, T.F.; Speer, T.; Poggi, A.; Mannino, E.; Pelli, G.; et al. Inhibition of nicotinamide phosphoribosyltransferase reduces neutrophil-mediated injury in myocardial infarction. Antioxid. Redox Signal. 2013, 18, 630–641. [Google Scholar]
- Trevejo, J.M.; Marino, M.W.; Philpott, N.; Josien, R.; Richards, E.C.; Elkon, K.B.; Falck-Pedersen, E. Tnf-alph -dependent maturation of local dendritic cells is critical for activating the adaptive immune response to virus infection. Proc. Natl. Acad. Sci. USA 2001, 98, 12162–12167. [Google Scholar]
- Ebrahimi, M.; Hassan, Z.M.; Hadjati, J.; Hayat, P.; Moazzeni, S.M. Immediate exposure to tnf-alpha activate dendritic cells derived from non-purified cord blood mononuclear cells. Iran. J. Immunol. 2009, 6, 107–118. [Google Scholar]
- Grigoriadis, N.; van Pesch, V.; Paradig, M.S.G. A basic overview of multiple sclerosis immunopathology. Eur. J. Neurol. 2015, 22 (Suppl. 2), 3–13. [Google Scholar]
- Burg, N.; Bittner, S.; Ellwardt, E. Role of the epigenetic factor sirt7 in neuroinflammation and neurogenesis. Neurosci. Res. 2018, 131, 1–9. [Google Scholar]

{kind=link}
| Type | Anatomical Sites | Surface Markers | Main Functions | |||
|---|---|---|---|---|---|---|
| CD4 | CD8α | CD205 | CD11b | |||
| Lymphoid | Thymus, spleen, lymph nodes | − | high | + | − | Induction of cross-tolerance, antigen cross preservation for the stimulation of cytotoxic response |
| + | − | − | + | Lymphocyte polarization toward T helper | ||
| − | − | − | + | Lymphocyte polarization toward T helper | ||
| Myeloid | Spleen, lymph nodes, lymphatic system | − | − | + | + | CD4+ T cell activation toward TH1 generation |
| − | low | high | − | |||
| Sirtuin | Effects on DCs | Derived Effects on Immune Cells | Ref |
|---|---|---|---|
| Sirtuin 1 | ↓IL-12; ↑TGF-β | ↓TH1 and ↑Treg differentiation | Liu G. et al. 2015 [181] |
| promotes maturation of CD80+CD86+ in mice DCs | TH1 and TH17 differentiation | Woo S.J. et al. 2016 [182] | |
| ↑IL-12p70, IL-1β, and IL-6; ↓IL-10 | |||
| ↓PPARγ; ↑IL-4, IL-5, IL-13 in lung DCs | ↑TH2 maturation | Legutko A. et al. 2011 [112] | |
| Sirtuin 6 | ↑TNF-α, MHC-II, CD80, CD86, CD40, IL-12; ↓IL-6 in CD11c+ BMDCs | - | Lasigliè D. et al. 2016 [183] |
| promotes maturation of CD11c+ BMDCs | |||
| ↑CXCR4 and CCR7 | - | Ferrara G. et al. 2020 [184] | |
| promotes migration of DCs to lymph nodes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piacente, F.; Bottero, M.; Benzi, A.; Vigo, T.; Uccelli, A.; Bruzzone, S.; Ferrara, G. Neuroprotective Potential of Dendritic Cells and Sirtuins in Multiple Sclerosis. Int. J. Mol. Sci. 2022, 23, 4352. https://doi.org/10.3390/ijms23084352
Piacente F, Bottero M, Benzi A, Vigo T, Uccelli A, Bruzzone S, Ferrara G. Neuroprotective Potential of Dendritic Cells and Sirtuins in Multiple Sclerosis. International Journal of Molecular Sciences. 2022; 23(8):4352. https://doi.org/10.3390/ijms23084352
Chicago/Turabian StylePiacente, Francesco, Marta Bottero, Andrea Benzi, Tiziana Vigo, Antonio Uccelli, Santina Bruzzone, and Giovanni Ferrara. 2022. "Neuroprotective Potential of Dendritic Cells and Sirtuins in Multiple Sclerosis" International Journal of Molecular Sciences 23, no. 8: 4352. https://doi.org/10.3390/ijms23084352
APA StylePiacente, F., Bottero, M., Benzi, A., Vigo, T., Uccelli, A., Bruzzone, S., & Ferrara, G. (2022). Neuroprotective Potential of Dendritic Cells and Sirtuins in Multiple Sclerosis. International Journal of Molecular Sciences, 23(8), 4352. https://doi.org/10.3390/ijms23084352