Investigation of Structural Alterations in Inherited Retinal Diseases: A Quantitative SD-OCT-Analysis of Retinal Layer Thicknesses in Light of Underlying Genetic Mutations

 , , , , and
, , , , and
Abstract
1. Introduction
2. Results
2.1. Alterations of the Retinal Structure in IRDs
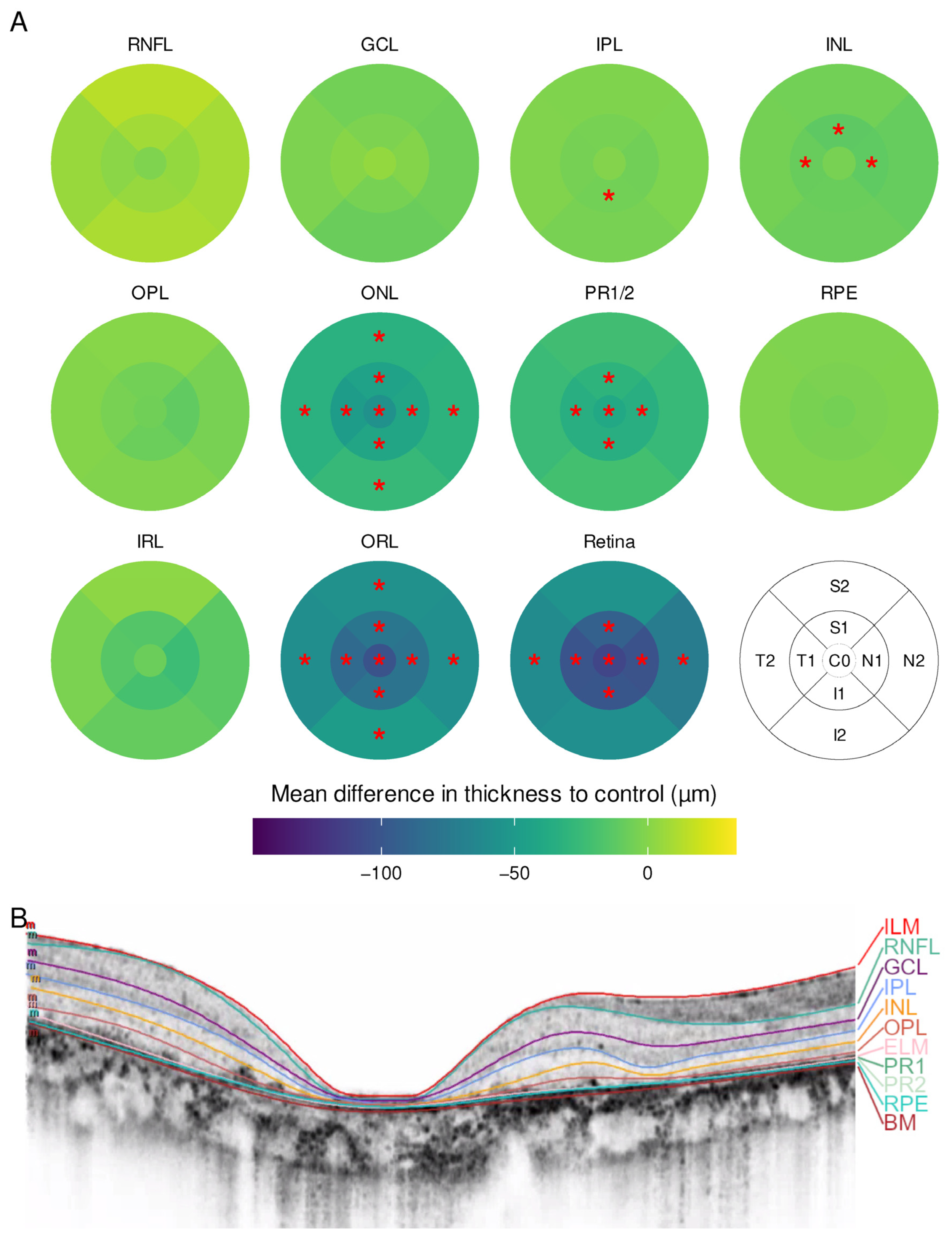
2.1.1. Retinitis Pigmentosa
2.1.2. Cone-Rod Dystrophy
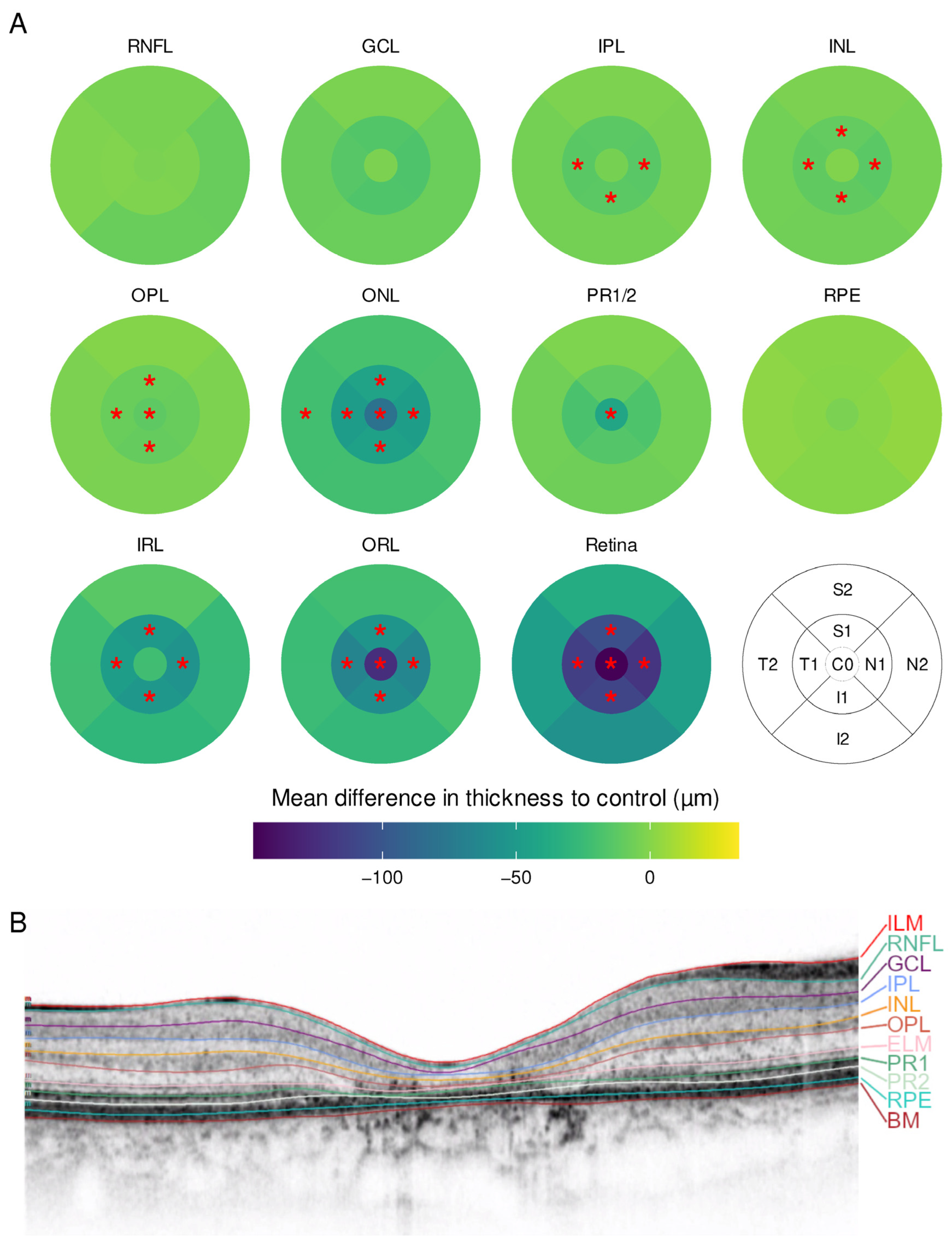
2.1.3. Stargardt Disease
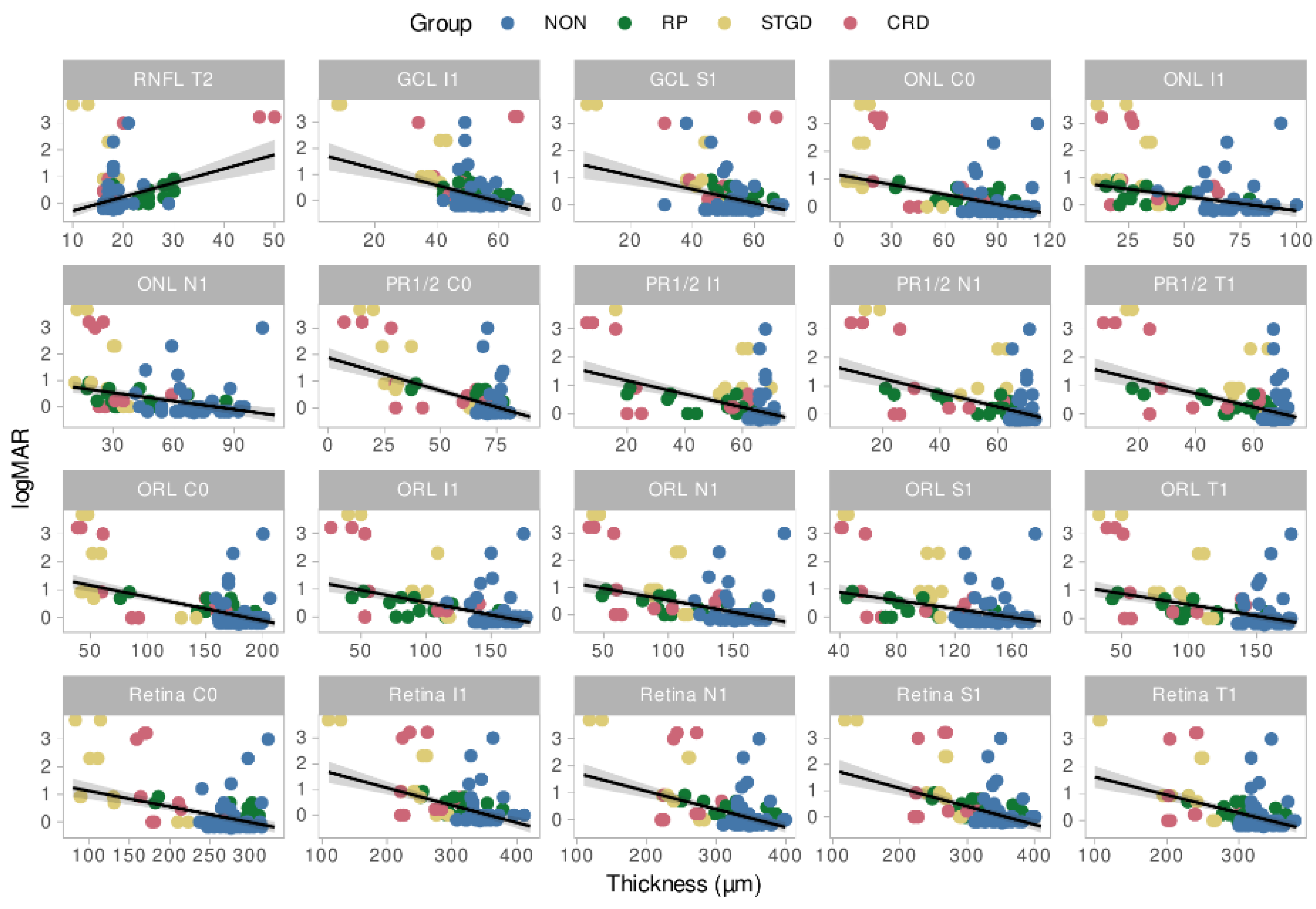
2.2. Association between Subfield Thicknesses and Visual Function
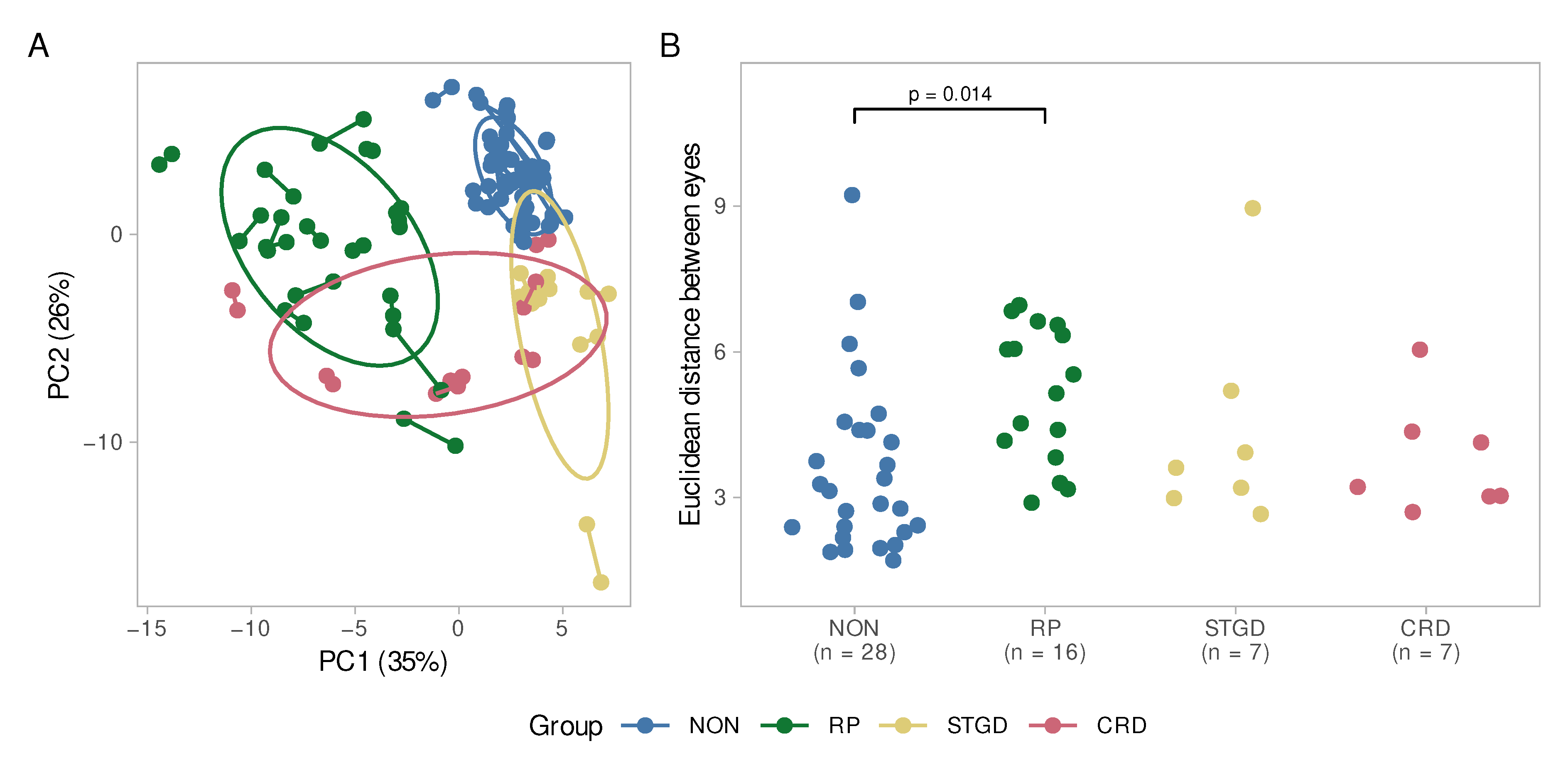
2.3. Interocular Symmetry
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Molecular Genetic Analysis
4.3. Imaging and Segmentation Using SD-OCT
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birtel, J.; Yusuf, I.H.; Priglinger, C.; Rudolph, G.; Charbel Issa, P. Diagnosis of Inherited Retinal Diseases. Klin. Mon. Für Augenheilkd. 2021, 238, 249–259. [Google Scholar] [CrossRef]
- Heath Jeffery, R.C.; Mukhtar, S.A.; McAllister, I.L.; Morgan, W.H.; Mackey, D.A.; Chen, F.K. Inherited Retinal Diseases Are the Most Common Cause of Blindness in the Working-Age Population in Australia. Ophthalmic Genet. 2021, 42, 431. [Google Scholar] [CrossRef]
- Liew, G.; Michaelides, M.; Bunce, C. A Comparison of the Causes of Blindness Certifications in England and Wales in Working Age Adults (16–64 Years), 1999–2000 with 2009–2010. BMJ Open 2014, 4, 4015. [Google Scholar] [CrossRef]
- Strauss, R.W.; Ho, A.; Muñoz, B.; Cideciyan, A.V.; Sahel, J.A.; Sunness, J.S.; Birch, D.G.; Bernstein, P.S.; Michaelides, M.; Traboulsi, E.I.; et al. The Natural History of the Progression of Atrophy Secondary to Stargardt Disease (ProgStar) Studies: Design and Baseline Characteristics: ProgStar Report No. 1. Ophthalmology 2016, 123, 817–828. [Google Scholar] [CrossRef]
- Hamel, C. Retinitis Pigmentosa. Orphanet J. Rare Dis. 2006, 1, 40. [Google Scholar] [CrossRef]
- Birtel, J.; Eisenberger, T.; Gliem, M.; Müller, P.L.; Herrmann, P.; Betz, C.; Zahnleiter, D.; Neuhaus, C.; Lenzner, S.; Holz, F.G.; et al. Clinical and Genetic Characteristics of 251 Consecutive Patients with Macular and Cone/Cone-Rod Dystrophy. Sci. Rep. 2018, 8, 4824. [Google Scholar] [CrossRef]
- Verbakel, S.K.; van Huet, R.A.C.; Boon, C.J.F.; den Hollander, A.I.; Collin, R.W.J.; Klaver, C.C.W.; Hoyng, C.B.; Roepman, R.; Klevering, B.J. Non-Syndromic Retinitis Pigmentosa. Prog. Retin. Eye Res. 2018, 66, 157–186. [Google Scholar] [CrossRef]
- Fujinami, K.; Zernant, J.; Chana, R.K.; Wright, G.A.; Tsunoda, K.; Ozawa, Y.; Tsubota, K.; Robson, A.G.; Holder, G.E.; Allikmets, R.; et al. Clinical and Molecular Characteristics of Childhood-Onset Stargardt Disease. Ophthalmology 2015, 122, 326–334. [Google Scholar] [CrossRef]
- Schneider, N.; Sundaresan, Y.; Gopalakrishnan, P.; Beryozkin, A.; Hanany, M.; Levanon, E.Y.; Banin, E.; Ben-Aroya, S.; Sharon, D. Inherited Retinal Diseases: Linking Genes, Disease-Causing Variants, and Relevant Therapeutic Modalities. Prog. Retin. Eye Res. 2021, 2021, 101029. [Google Scholar] [CrossRef]
- Lee, K.; Garg, S. Navigating the Current Landscape of Clinical Genetic Testing for Inherited Retinal Dystrophies. Genet. Med. 2015, 17, 245–252. [Google Scholar] [CrossRef]
- Duncker, T.; Stein, G.E.; Lee, W.; Tsang, S.H.; Zernant, J.; Bearelly, S.; Hood, D.C.; Greenstein, V.C.; Delori, F.C.; Allikmets, R.; et al. Quantitative Fundus Autofluorescence and Optical Coherence Tomography in ABCA4 Carriers. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7274–7285. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.S.; Georgiou, M.; Kalitzeos, A.; Moore, A.T.; Michaelides, M. Progressive Cone and Cone-Rod Dystrophies: Clinical Features, Molecular Genetics and Prospects for Therapy. Br. J. Ophthalmol. 2019, 103, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- McLellan, G.J.; Rasmussen, C.A. Optical Coherence Tomography for the Evaluation of Retinal and Optic Nerve Morphology in Animal Subjects: Practical Considerations. Vet. Ophthalmol. 2012, 15 (Suppl. 2), 13–28. [Google Scholar] [CrossRef]
- Velaga, S.B.; Nittala, M.G.; Jenkins, D.; Melendez, J.; Ho, A.; Strauss, R.W.; Scholl, H.P.; Sadda, S.V.R. Impact of Segmentation Density on Spectral Domain Optical Coherence Tomography Assessment in Stargardt Disease. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 549–556. [Google Scholar] [CrossRef]
- Kim, M.; Lee, S.; Han, J.; Yu, S.Y.; Kwak, H. Segmentation Error and Macular Thickness Measurements Obtained with Spectral-Domain Optical Coherence Tomography Devices in Neovascular Age-Related Macular Degeneration. Indian J. Ophthalmol. 2013, 61, 213. [Google Scholar] [CrossRef]
- Yang, Q.; Reisman, C.A.; Chan, K.; Ramachandran, R.; Raza, A.; Hood, D.C. Automated Segmentation of Outer Retinal Layers in Macular OCT Images of Patients with Retinitis Pigmentosa. Biomed. Opt. Express 2011, 2, 2493. [Google Scholar] [CrossRef]
- Gomes, N.L.; Greenstein, V.C.; Carlson, J.N.; Tsang, S.H.; Theodore Smith, R.; Carr, R.E.; Hood, D.C.; Chang, S. A Comparison of Fundus Autofluorescence and Retinal Structure in Patients with Stargardt Disease. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3953. [Google Scholar] [CrossRef]
- Park, J.C.; Collison, F.T.; Fishman, G.A.; Allikmets, R.; Zernant, J.; Liu, M.; Jason McAnany, J. Objective Analysis of Hyperreflective Outer Retinal Bands Imaged by Optical Coherence Tomography in Patients with Stargardt Disease. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4662. [Google Scholar] [CrossRef]
- Park, S.P.; Chang, S.; Allikmets, R.; Smith, R.T.; Burke, T.R.; Gregory-Roberts, E.; Tsang, S.H. Disruption in Bruch Membrane in Patients with Stargardt Disease. Ophthalmic Genet. 2012, 33, 49. [Google Scholar] [CrossRef]
- Battaglia Parodi, M.; la Spina, C.; Triolo, G.; Riccieri, F.; Pierro, L.; Gagliardi, M.; Bandello, F. Correlation of SD-OCT Findings and Visual Function in Patients with Retinitis Pigmentosa. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1275–1279. [Google Scholar] [CrossRef]
- Lima, L.H.; Sallum, J.M.; Spaide, R.F. Outer Retina Analysis by Optical Coherence Tomography in Cone-Rod Dystrophy Patients. Retina 2013, 33, 1877–1880. [Google Scholar] [CrossRef] [PubMed]
- Aleman, T.S.; Cideciyan, A.V.; Sumaroka, A.; Schwartz, S.B.; Roman, A.J.; Windsor, E.A.M.; Steinberg, J.D.; Branham, K.; Othman, M.; Swaroop, A.; et al. Inner Retinal Abnormalities in X-Linked Retinitis Pigmentosa with RPGR Mutations. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4759. [Google Scholar] [CrossRef]
- Tanna, P.; Georgiou, M.; Strauss, R.W.; Ali, N.; Kumaran, N.; Kalitzeos, A.; Fujinami, K.; Michaelides, M. Cross-Sectional and Longitudinal Assessment of the Ellipsoid Zone in Childhood-Onset Stargardt Disease. Transl. Vis. Sci. Technol. 2019, 8, 1. [Google Scholar] [CrossRef]
- Ergun, E.; Hermann, B.; Wirtitsch, M.; Unterhuber, A.; Ko, T.H.; Sattmann, H.; Scholda, C.; Fujimoto, J.G.; Stur, M.; Drexler, W. Assessment of Central Visual Function in Stargardt’s Disease/Fundus Flavimaculatus with Ultrahigh-Resolution Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2005, 46, 310–316. [Google Scholar] [CrossRef]
- Arrigo, A.; Romano, F.; Aragona, E.; Nunzio, C.D.; Sperti, A.; Bandello, F.; Parodi, M.B. OCTA-Based Identification of Different Vascular Patterns in Stargardt Disease. Transl. Vis. Sci. Technol. 2019, 8, 26. [Google Scholar] [CrossRef]
- Burke, T.R.; Rhee, D.W.; Theodore Smith, R.; Tsang, S.H.; Allikmets, R.; Chang, S.; Lazow, M.A.; Hood, D.C.; Greenstein, V.C. Quantification of Peripapillary Sparing and Macular Involvement in Stargardt Disease (STGD1). Investig. Ophthalmol. Vis. Sci. 2011, 52, 8006. [Google Scholar] [CrossRef]
- Holladay, J.T. Visual Acuity Measurements. J. Cataract. Refract. Surg. 2004, 30, 287–290. [Google Scholar] [CrossRef]
- Li, G.; de La Garza, B.; Shih, Y.Y.I.; Muir, E.R.; Duong, T.Q. Layer-Specific Blood-Flow MRI of Retinitis Pigmentosa in RCS Rats. Exp. Eye Res. 2012, 101, 90. [Google Scholar] [CrossRef]
- Nagasaka, Y.; Ito, Y.; Ueno, S.; Terasaki, H. Increased Aqueous Flare Is Associated with Thickening of Inner Retinal Layers in Eyes with Retinitis Pigmentosa. Sci. Rep. 2016, 6, 33921. [Google Scholar] [CrossRef]
- Liu, G.; Li, H.; Liu, X.; Xu, D.; Wang, F. Structural Analysis of Retinal Photoreceptor Ellipsoid Zone and Postreceptor Retinal Layer Associated with Visual Acuity in Patients with Retinitis Pigmentosa by Ganglion Cell Analysis Combined with OCT Imaging. Medicine 2016, 95, e5785. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Lazow, M.A.; Locke, K.G.; Greenstein, V.C.; Birch, D.G. The Transition Zone between Healthy and Diseased Retina in Patients with Retinitis Pigmentosa. Investig. Ophthalmol. Vis. Sci. 2011, 52, 101. [Google Scholar] [CrossRef] [PubMed]
- Sousa, K.; Fernandes, T.; Gentil, R.; Mendonça, L.; Falcão, M. Outer Retinal Layers as Predictors of Visual Acuity in Retinitis Pigmentosa: A Cross-Sectional Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 265–271. [Google Scholar] [CrossRef]
- Vámos, R.; Tátrai, E.; Németh, J.; Holder, G.E.; DeBuc, D.C.; Somfai, G.M. The Structure and Function of the Macula in Patients with Advanced Retinitis Pigmentosa. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8425–8432. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, M.; Hara, A.; Ishiguro, S.I. Optical Coherence Tomography of Animal Models of Retinitis Pigmentosa: From Animal Studies to Clinical Applications. Biomed. Res. Int. 2019, 2019, 8276140. [Google Scholar] [CrossRef] [PubMed]
- Aleman, T.S.; Cideciyan, A.V.; Sumaroka, A.; Windsor, E.A.M.; Herrera, W.; White, D.A.; Kaushal, S.; Naidu, A.; Roman, A.J.; Schwartz, S.B.; et al. Retinal Laminar Architecture in Human Retinitis Pigmentosa Caused by Rhodopsin Gene Mutations. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1580. [Google Scholar] [CrossRef] [PubMed]
- Gartner, S.; Henkind, P. Pathology of Retinitis Pigmentosa. Ophthalmology 1982, 89, 1425–1432. [Google Scholar] [CrossRef]
- Milam, A.H.; Li, Z.Y.; Fariss, R.N. Histopathology of the Human Retina in Retinitis Pigmentosa. Prog. Retin. Eye Res. 1998, 17, 175–205. [Google Scholar] [CrossRef]
- Yoon, C.K.; Yu, H.G. Ganglion Cell-Inner Plexiform Layer and Retinal Nerve Fibre Layer Changes within the Macula in Retinitis Pigmentosa: A Spectral Domain Optical Coherence Tomography Study. Acta Ophthalmol. 2018, 96, e180–e188. [Google Scholar] [CrossRef]
- Hood, D.C.; Lin, C.E.; Lazow, M.A.; Locke, K.G.; Zhang, X.; Birch, D.G. Thickness of Receptor and Post-Receptor Retinal Layers in Patients with Retinitis Pigmentosa Measured with Frequency-Domain Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2328. [Google Scholar] [CrossRef]
- Ilhan, C.; Citirik, M. Glial Proliferation and Atrophy: Two Poles of Optic Disc in Patients with Retinitis Pigmentosa. J. Curr. Ophthalmol. 2019, 31, 416. [Google Scholar] [CrossRef]
- Birtel, T.H.; Birtel, J.; Hess, K.; Clemens, A.C.; Lindner, M.; Herrmann, P.; Holz, F.G.; Gliem, M. Analysis of Imaging Biomarkers and Retinal Nerve Fiber Layer Thickness in RPGR-Associated Retinitis Pigmentosa. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 3597–3604. [Google Scholar] [CrossRef]
- Sobaci, G.; Özge, G.; Gündoǧan, F.Ç. Cone Dysfunctions in Retinitis Pigmentosa with Retinal Nerve Fiber Layer Thickening. Clin. Ophthalmol. 2012, 6, 473. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Anastasakis, A.; Genead, M.A.; McAnany, J.J.; Fishman, G.A. Evaluation of Retinal Nerve Fiber Layer Thickness in Retinitis Pigmentosa Patients Using Spectral-Domain OCT. Retina 2012, 32, 358. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Liu, X.; Li, H.; Du, Q.; Wang, F. Optical Coherence Tomographic Analysis of Retina in Retinitis Pigmentosa Patients. Ophthalmic Res. 2016, 56, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Friesacher, A.; Lopez Torres, L.T.; Valmaggia, C.; Rüesch, R.; Todorova, M.G. Linking the Presence of Macular Oedema to Structural and Functional Alterations in Retinitis Pigmentosa. Klin. Mon. Für Augenheilkd. 2021, 238, 418–427. [Google Scholar] [CrossRef]
- Stefanov, A.; Novelli, E.; Strettoi, E. Inner Retinal Preservation in the Photoinducible I307N Rhodopsin Mutant Mouse, a Model of Autosomal Dominant Retinitis Pigmentosa. J. Comp. Neurol. 2020, 528, 1502. [Google Scholar] [CrossRef]
- Zahlava, J.; Lestak, J.; Karel, I. Optical Coherence Tomography in Progressive Cone Dystrophy. Biomed. Pap. Med. Fac. Palacky Univ. Olomouc 2014, 158, 628–634. [Google Scholar] [CrossRef]
- Cho, S.C.; Woo, S.J.; Park, K.H.; Hwang, J.M. Morphologic Characteristics of the Outer Retina in Cone Dystrophy on Spectral-Domain Optical Coherence Tomography. Korean J. Ophthalmol. 2013, 27, 19–27. [Google Scholar] [CrossRef]
- Turney, C.; Chong, N.H.V.; Alexander, R.A.; Hogg, C.R.; Fleming, L.; Flack, D.; Barnett, K.C.; Bird, A.C.; Holder, G.E.; Luthert, P.J. Pathological and Electrophysiological Features of a Canine Cone–Rod Dystrophy in the Miniature Longhaired Dachshund. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4240–4249. [Google Scholar] [CrossRef]
- Reich, M.; Lübke, J.; Joachimsen, L.; Stifter, J.; Küchlin, S.; Böhringer, D.; Lange, C.; Lagrèze, W.A. Thinner Temporal Peripapillary Retinal Nerve Fibre Layer in Stargardt Disease Detected by Optical Coherence Tomography. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 1521–1528. [Google Scholar] [CrossRef]
- Bojinova, R.I.; Türksever, C.; Schötzau, A.; Valmaggia, C.; Schorderet, D.F.; Todorova, M.G. Reduced Metabolic Function and Structural Alterations in Inherited Retinal Dystrophies: Investigating the Effect of Peripapillary Vessel Oxygen Saturation and Vascular Diameter on the Retinal Nerve Fibre Layer Thickness. Acta Ophthalmol. 2017, 95, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Whitmore, S.S.; Fortenbach, C.R.; Cheng, J.L.; DeLuca, A.P.; Critser, D.B.; Geary, E.L.; Hoffmann, J.M.; Stone, E.M.; Han, I.C. Analysis of Retinal Sublayer Thicknesses and Rates of Change in ABCA4-Associated Stargardt Disease. Sci. Rep. 2020, 10, 16576. [Google Scholar] [CrossRef] [PubMed]
- Genead, M.A.; Fishman, G.A.; Anastasakis, A. Spectral-Domain OCT Peripapillary Retinal Nerve Fibre Layer Thickness Measurements in Patients with Stargardt Disease. Br. J. Ophthalmol. 2011, 95, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Nakazawa, M.; Saito, M.; Suzuki, Y. The Qualitative Assessment of Optical Coherence Tomography and the Central Retinal Sensitivity in Patients with Retinitis Pigmentosa. PLoS ONE 2020, 15, e0232700. [Google Scholar] [CrossRef]
- Mucciolo, D.P.; Lippera, M.; Giorgio, D.; Sodi, A.; Passerini, I.; Cipollini, F.; Virgili, G.; Giansanti, F.; Murro, V. Outer Nuclear Layer Relevance in Visual Function Correlated to Quantitative Enface OCT Parameters in Stargardt Disease. Eur. J. Ophthalmol. 2021, 31, 3248–3258. [Google Scholar] [CrossRef]
- Tanna, P.; Strauss, R.W.; Fujinami, K.; Michaelides, M. Stargardt Disease: Clinical Features, Molecular Genetics, Animal Models and Therapeutic Options. Br. J. Ophthalmol. 2017, 101, 25. [Google Scholar] [CrossRef]
- Heath Jeffery MChD, R.C.; Chen, F.K.; Fred Chen, C.K. Stargardt Disease: Multimodal Imaging: A Review. Clin. Exp. Ophthalmol. 2021, 49, 498–515. [Google Scholar] [CrossRef]
- Dias, M.F.; Joo, K.; Kemp, J.A.; Fialho, S.L.; da Silva Cunha, A.; Woo, S.J.; Kwon, Y.J. Molecular Genetics and Emerging Therapies for Retinitis Pigmentosa: Basic Research and Clinical Perspectives. Prog. Retin. Eye Res. 2018, 63, 107–131. [Google Scholar] [CrossRef]
- Galli-Resta, L.; Falsini, B.; Rossi, G.; Piccardi, M.; Ziccardi, L.; Fadda, A.; Minnella, A.; Marangoni, D.; Placidi, G.; Campagna, F.; et al. Bilateral Symmetry of Visual Function Loss in Cone–Rod Dystrophies. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3759–3768. [Google Scholar] [CrossRef][Green Version]
- Georgiou, M.; Kane, T.; Tanna, P.; Bouzia, Z.; Singh, N.; Kalitzeos, A.; Strauss, R.W.; Fujinami, K.; Michaelides, M. Prospective Cohort Study of Childhood-Onset Stargardt Disease: Fundus Autofluorescence Imaging, Progression, Comparison with Adult-Onset Disease, and Disease Symmetry. Am. J. Ophthalmol. 2020, 211, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Massof, R.W.; Finkelstein, D.; Starr, S.J.; Kenyon, K.R.; Fleischman, J.A.; Maumenee, I.H. Bilateral Symmetry of Vision Disorders in Typical Retinitis Pigmentosa. Br. J. Ophthalmol. 1979, 63, 90. [Google Scholar] [CrossRef] [PubMed]
- Fakin, A.; Jarc-Vidmar, M.; Glavač, D.; Bonnet, C.; Petit, C.; Hawlina, M. Fundus Autofluorescence and Optical Coherence Tomography in Relation to Visual Function in Usher Syndrome Type 1 and 2. Vis. Res. 2012, 75, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Tee, J.J.L.; Carroll, J.; Webster, A.R.; Michaelides, M. Quantitative Analysis of Retinal Structure Using Spectral-Domain Optical Coherence Tomography in RPGR-Associated Retinopathy. Am. J. Ophthalmol. 2017, 178, 18. [Google Scholar] [CrossRef]
- Marquardt, A.; Stöhr, H.; Passmore, L.A.; Krämer, F.; Rivera, A.; Weber, B.H.F. Mutations in a Novel Gene, VMD2, Encoding a Protein of Unknown Properties Cause Juvenile-Onset Vitelliform Macular Dystrophy (Best’s Disease). Hum. Mol. Genet. 1998, 7, 1517–1525. [Google Scholar] [CrossRef]
- Schulz, H.L.; Grassmann, F.; Kellner, U.; Spital, G.; Rüther, K.; Jägle, H.; Hufendiek, K.; Rating, P.; Huchzermeyer, C.; Baier, M.J.; et al. Mutation Spectrum of the ABCA4 Gene in 335 Stargardt Disease Patients from a Multicenter German Cohort—Impact of Selected Deep Intronic Variants and Common SNPs. Investig. Ophthalmol. Vis. Sci. 2017, 58, 394. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 17 August 2022).
- Pinheiro, J.; Bates, D. Nlme: Linear and Nonlinear Mixed Effects Models. Available online: https://cran.r-project.org/web/packages/nlme/index.html (accessed on 17 August 2022).
- Pinheiro, J.; Bates, D. Mixed-Effects Models in S and S-PLUS; Springer: New York, NY, USA, 2000; ISBN 978-0-387-98957-0. [Google Scholar]
- Koller, M. Robustlmm: An R Package for Robust Estimation of Linear Mixed-Effects Models. J. Stat. Softw. 2016, 75, 1–24. [Google Scholar] [CrossRef]
- Lüdecke, D.; Ben-Shachar, M.; Patil, I.; Makowski, D. Extracting, Computing and Exploring the Parameters of Statistical Models Using R. J. Open Source Softw. 2020, 5, 2445. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Pohlert, T. PMCMRplus: Calculate Pairwise Multiple Comparisons of Mean Rank Sums Extended. Available online: https://cran.r-project.org/web/packages/PMCMRplus/index.html (accessed on 17 August 2022).
- Lenth, R. Emmeans: Estimated Marginal Means, Aka Least-Squares Means. Available online: https://cran.r-project.org/web/packages/emmeans/index.html (accessed on 17 August 2022).
- Hastie, T.; Tibshirani, R.; Narasimhan, B.; Chu, G. Impute: Imputation for Microarray Data. Available online: http://www.bioconductor.org/packages/release/bioc/html/impute.html (accessed on 17 August 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Retinitis Pigmentosa | Stargardt Disease | Cone-Rod Dystrophy | ||||
|---|---|---|---|---|---|---|
| Controls (n = 16) | RP (n = 16) | Controls (n = 7) | STGD (n = 7) | Controls (n = 7) | CRD (n = 7) | |
| Age | ||||||
| Mean (SD) | 37.0 (15.2) | 36.7 (15.7) | 40.0 (18.4) | 40.3 (17.2) | 34.7 (11.8) | 33.4 (10.8) |
| Median | 39.3 | 39.2 | 37.5 | 37.2 | 36.2 | 36.0 |
| [Min, Max] | [8.09, 59.0] | [7.95, 60.0] | [10.8, 70.2] | [14.1, 69.8] | [17.7, 52.3] | [18.4, 49.5] |
| Sex (n) | ||||||
| Female | 8 | 8 | 5 | 5 | 3 | 3 |
| Male | 8 | 8 | 2 | 2 | 4 | 4 |
| Disease | Patient ID | Family ID | Age | Sex | Gene | Sequence Variant | Status |
|---|---|---|---|---|---|---|---|
| CRD | 1 | 1 | 49.5 | m | ABCA4 | c.4615_4625del, c.5603A>T | heterozygous |
| 2 | 2 | 18.4 | f | ABCA4 | c.5917del | homozygous | |
| 3 | 3 | 24 | f | ABCA4 | c.1903C>T c.5882G>A | heterozygous | |
| 4 | 4 | 40.1 | f | CACNA2D4 | c.2854C>T | heterozygous | |
| 5 | 5 | 26.9 | m | ABCA4 | c.5917del | homozygous | |
| 6 | 6 | 36 | m | RPGR | c.3070G>T | hemizygous | |
| 7 | 7 | 38.9 | m | ABCA4 | c.[1622T>C(;)3113C>T], c.5714+5G>A | heterozygous | |
| STGD | 8 | 8 | 37.2 | f | ABCA4 | c.5882G>A, c.5381C>A | heterozygous |
| 9 | 8 | 69.8 | f | ABCA4 | c.5381C>A | homozygous | |
| 10 | 9 | 35.3 | f | ABCA4 | c.5582G>A, c.1609C>T | heterozygous | |
| 11 | 10 | 50.6 | m | ABCA4 | c.5882G>A | homozygous | |
| 12 | 11 | 42.4 | m | ABCA4 | c.67-1G>C, c.2804T>C | heterozygous | |
| 13 | 12 | 32.6 | f | ABCA4 | c.4849-2A>G, c.5882G>A | heterozygous | |
| 14 | 13 | 14.1 | f | ABCA4 | c.[1609C>T;5881G>A] | homozygous | |
| RP | 15 | 14 | 35.6 | f | PRPH2 | c.646C>T | heterozygous |
| 16 | 15 | 30 | m | RP1 | c.662del | homozygous | |
| 17 | 16 | 60 | m | NR2E3 | c.166G>A | heterozygous | |
| 18 | 17 | 48.1 | f | USH2A | c.3551T>A, c.14131C>T | heterozygous | |
| 19 | 18 | 41 | m | EYS | deletion Exon 12 | homozygous | |
| 20 | 19 | 37.4 | m | PRPF31 | c.1060C>T | heterozygous | |
| 21 | 20 | 52.2 | m | USH2A | c.[2299del(;)4714C>T], c.2276G>T | heterozygous | |
| 22 | 21 | 24 | f | PCARE | c.1541del | homozygous | |
| 23 | 22 | 48.6 | f | RP1 | c.2332A>T | heterozygous | |
| 24 | 23 | 56.2 | f | FLVCR1 | c.1092+5G>A | homozygous | |
| 25 | 24 | 43.8 | f | PCARE | c.1541del | homozygous | |
| 26 | 25 | 8.34 | f | USH2A | c.2299del | heterozygous | |
| 27 | 26 | 7.95 | m | CDH23 | c.2206C>T, c.6000C>A | heterozygous | |
| 28 | 27 | 35 | m | USH2A | c.1876C>T, c.11864G>A | heterozygous | |
| 29 | 28 | 18.2 | f | NPHP1 | deletion Exon 1-20 | homozygous | |
| 30 | 29 | 41.2 | m | USH2A | c.2276G>T, c.10010G>T | heterozygous |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gersch, J.; Hufendiek, K.; Delarocque, J.; Framme, C.; Jacobsen, C.; Stöhr, H.; Kellner, U.; Hufendiek, K. Investigation of Structural Alterations in Inherited Retinal Diseases: A Quantitative SD-OCT-Analysis of Retinal Layer Thicknesses in Light of Underlying Genetic Mutations. Int. J. Mol. Sci. 2022, 23, 16007. https://doi.org/10.3390/ijms232416007
Gersch J, Hufendiek K, Delarocque J, Framme C, Jacobsen C, Stöhr H, Kellner U, Hufendiek K. Investigation of Structural Alterations in Inherited Retinal Diseases: A Quantitative SD-OCT-Analysis of Retinal Layer Thicknesses in Light of Underlying Genetic Mutations. International Journal of Molecular Sciences. 2022; 23(24):16007. https://doi.org/10.3390/ijms232416007
Chicago/Turabian StyleGersch, Julia, Katerina Hufendiek, Julien Delarocque, Carsten Framme, Christina Jacobsen, Heidi Stöhr, Ulrich Kellner, and Karsten Hufendiek. 2022. "Investigation of Structural Alterations in Inherited Retinal Diseases: A Quantitative SD-OCT-Analysis of Retinal Layer Thicknesses in Light of Underlying Genetic Mutations" International Journal of Molecular Sciences 23, no. 24: 16007. https://doi.org/10.3390/ijms232416007
APA StyleGersch, J., Hufendiek, K., Delarocque, J., Framme, C., Jacobsen, C., Stöhr, H., Kellner, U., & Hufendiek, K. (2022). Investigation of Structural Alterations in Inherited Retinal Diseases: A Quantitative SD-OCT-Analysis of Retinal Layer Thicknesses in Light of Underlying Genetic Mutations. International Journal of Molecular Sciences, 23(24), 16007. https://doi.org/10.3390/ijms232416007