
Differences in Synovial Cytokine Profile Associated with Long-Term Clinical Outcomes in Patients with Knee Osteoarthritis Undergoing Corrective Osteotomy with Platelet-Rich Plasma or Stromal Vascular Fraction Post-Treatments
 , and
, and
Abstract
1. Introduction
2. Results
2.1. Clinical Parameters in the Examined Subgroups of Subjects with OA before Surgery and after PRP or SVF Treatments
2.1.1. Clinical Parameters in the Examined Subjects with OA before Surgery
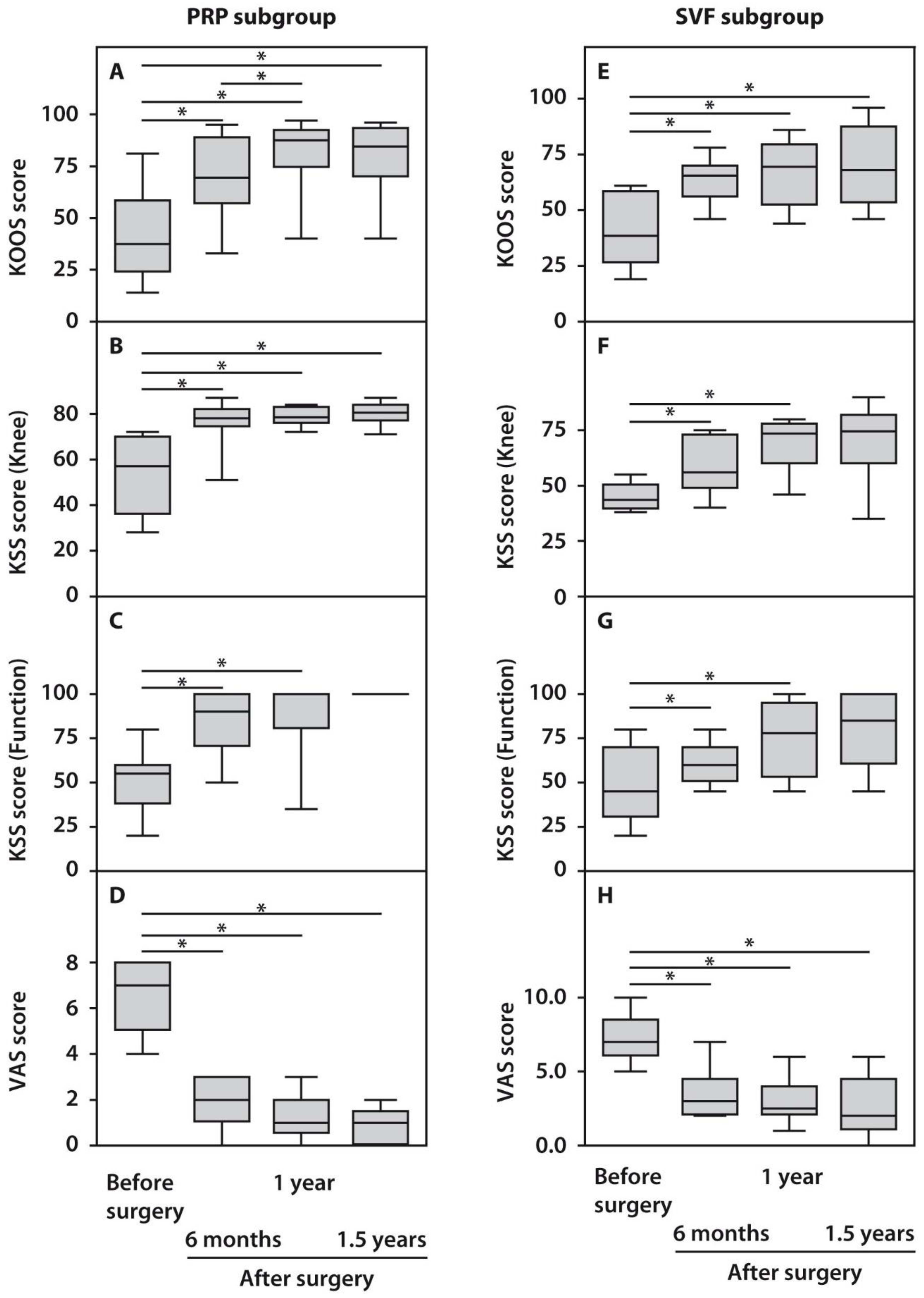
2.1.2. Clinical Parameters in the Examined Subjects with OA after PRP or SVF Treatments
2.1.3. Articular Cartilage Status in the Examined Subjects with OA after PRP or SVF Treatments
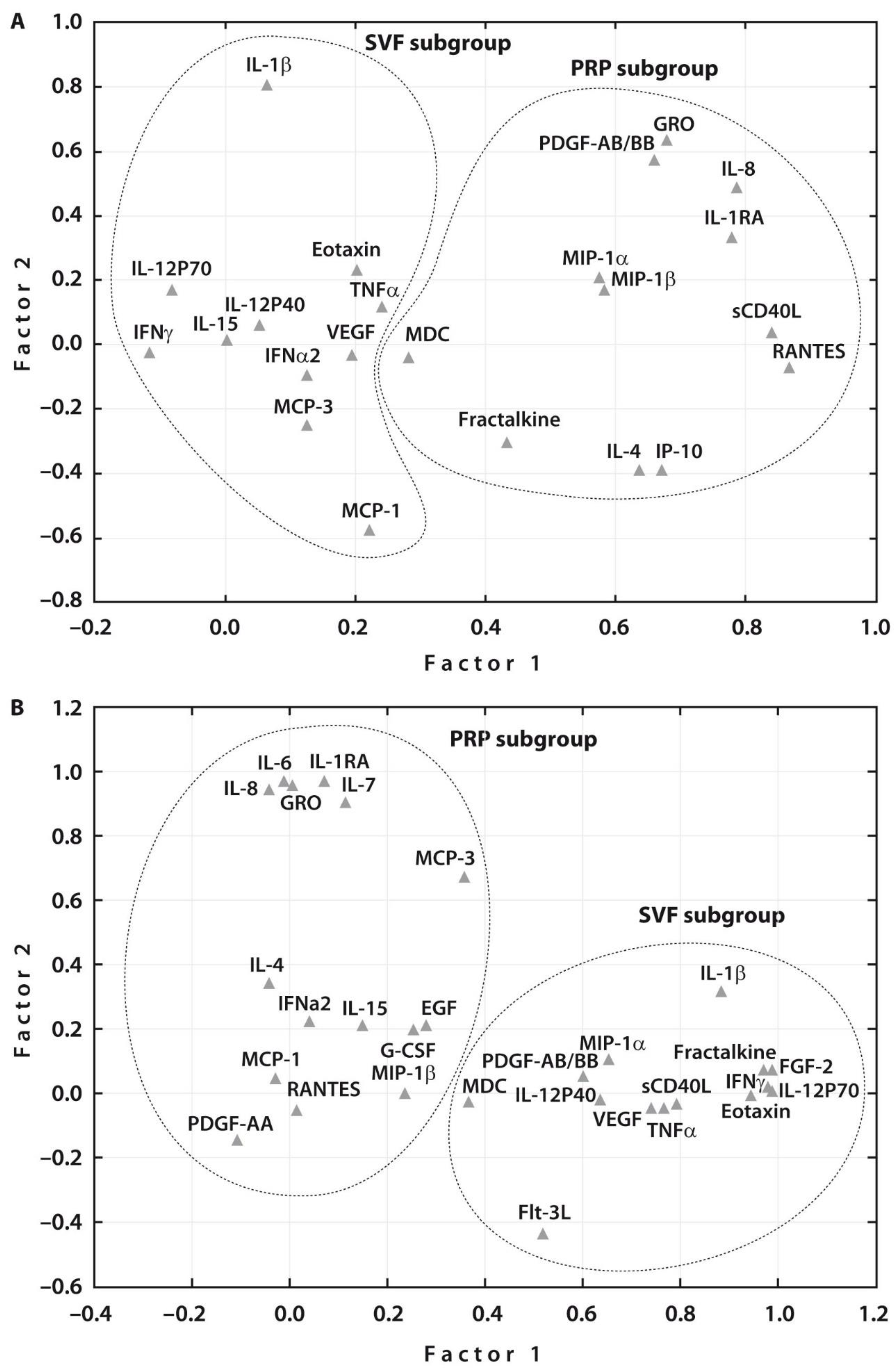
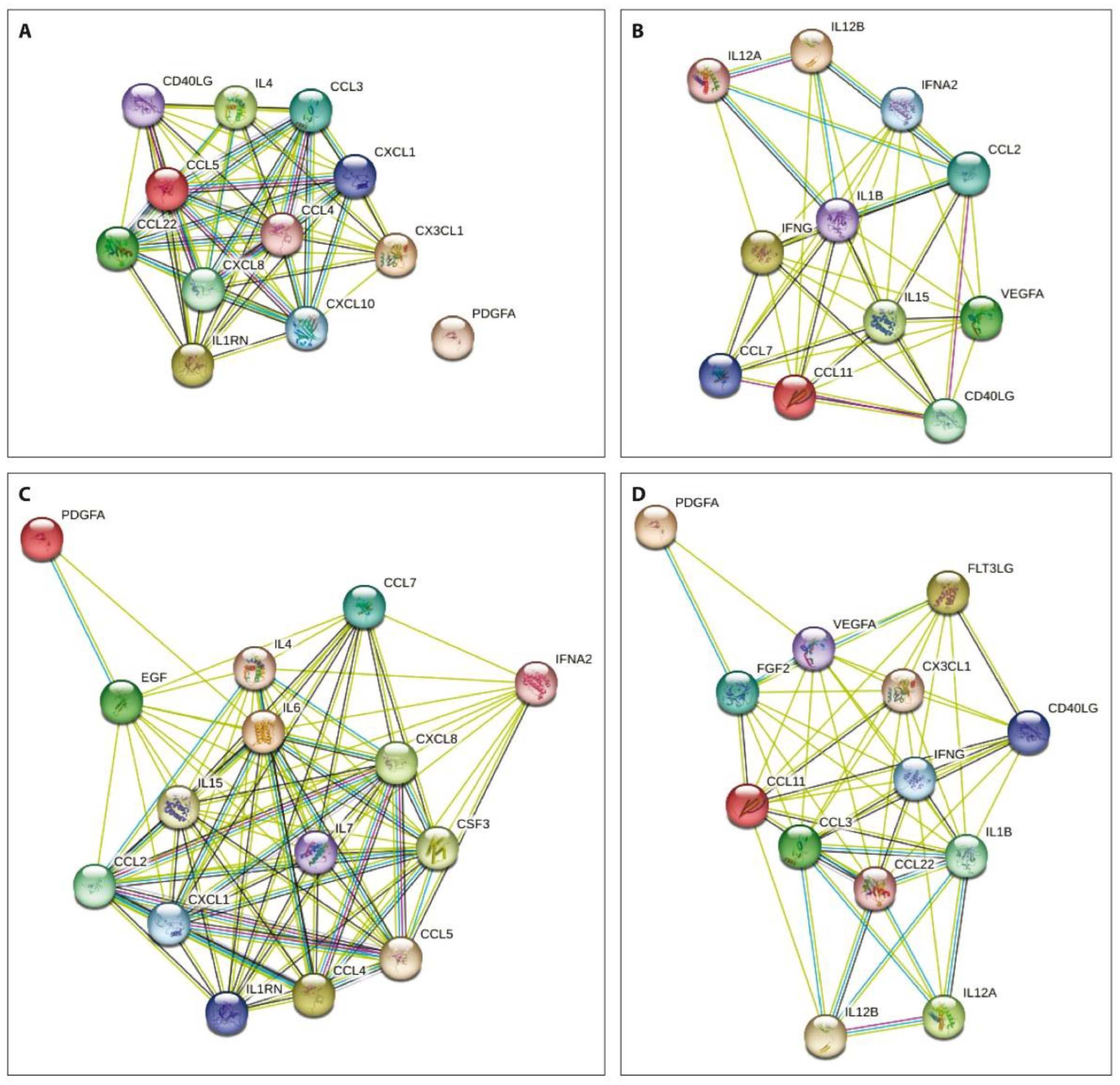
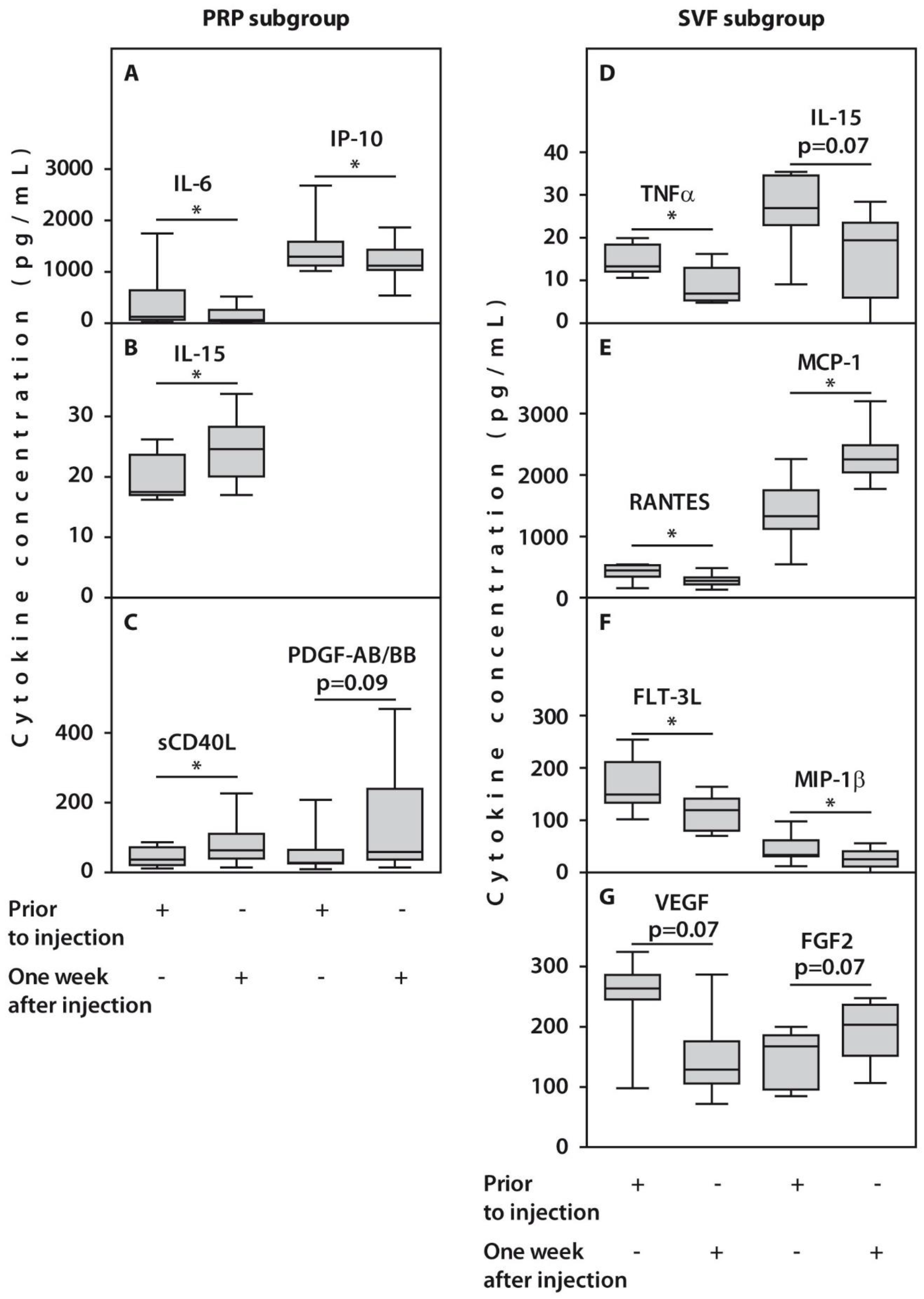
2.2. Synovial Cytokine Levels in the Examined Subgroups before and One Week after PRP or SVF Injection
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Clinical and Radiographic Testing
4.3. Surgical Techniques
4.4. Platelet-Rich Plasma (PRP) Preparation
4.5. Stromal Vascular Fraction (SVF) Preparation
4.6. Synovial Fluid (SF) Preparation
4.7. Cytokine Assay
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stoddart, J.C.; Dandridge, O.; Garner, A.; Cobb, J.; van Arkel, R.J. The compartmental distribution of knee osteoarthritis—A systematic review and meta-analysis. Osteoarthr. Cartil. 2021, 29, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Khanna, V.; Adili, A.; Ayeni, O.R.; Bedi, A.; Bhandari, M. Knee osteoarthritis: When arthroscopy can help. Pol. Arch. Intern. Med. 2018, 128, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Kumagai, K.; Akamatsu, Y.; Kobayashi, H.; Kusayama, Y. Five- to ten-year outcome following medial opening-wedge high tibial osteotomy with rigid plate fixation in combination with an artificial bone substitute. Bone Jt. J. 2014, 96, B339–B344. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, S.R.; Nagaraja, H.S.; Rajasekaran, S. Medial open wedge high tibial osteotomy for varus malunited tibial plateau fractures. Arthroscopy 2017, 33, 586–594. [Google Scholar] [CrossRef]
- Amendola, A.; Bonasia, D.B. Results of high tibial osteotomy: Review of the literature. Int. Orthop. (SICOT) 2010, 34, 155–160. [Google Scholar] [CrossRef]
- Bhan, S.; Dave, P.K. High valgus tibial osteotomy for osteoarthritis of the knee. Int. Orthop. (SICOT) 1992, 16, 13–17. [Google Scholar] [CrossRef]
- Shen, L.; Yuan, T.; Chen, S.; Xie, X.; Zhang, C. The temporal effect of platelet-rich plasma on pain and physical function in the treatment of knee osteoarthritis: Systematic review and meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2017, 12, 16. [Google Scholar] [CrossRef]
- Shanmugasundaram, S.; Vaish, A.; Chavada, V.; Murrell, W.D.; Vaishya, R. Assessment of safety and efficacy of intra-articular injection of stromal vascular fraction for the treatment of knee osteoarthritis—A systematic review. Int. Orthop. 2021, 45, 615–625. [Google Scholar] [CrossRef]
- Yang, W.-T.; Ke, C.-Y.; Yeh, K.-T.; Huang, S.-G.; Lin, Z.-Y.; Wu, W.-T.; Lee, R.-P. Stromal-vascular fraction and adipose-derived stem cell therapies improve cartilage regeneration in osteoarthritis-induced rats. Sci. Rep. 2022, 12, 2828. [Google Scholar] [CrossRef]
- Betzler, B.K.; Bin Muhammad Ridzwan Chew, A.H.; Bin Abd Razak, H.R. Intra-articular injection of orthobiologics in patients undergoing high tibial osteotomy for knee osteoarthritis is safe and effective—A systematic review. J. Exp. Orthop. 2021, 8, 83. [Google Scholar] [CrossRef]
- Kim, Y.S.; Koh, Y.G. Comparative Matched-Pair Analysis of Open-Wedge High Tibial Osteotomy with Versus without an Injection of Adipose-Derived Mesenchymal Stem Cells for Varus Knee Osteoarthritis: Clinical and Second-Look Arthroscopic Results. Am. J. Sports Med. 2018, 46, 2669–2677. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.-G.; Kwon, O.-R.; Kim, Y.-S.; Choi, Y.-J. Comparative outcomes of open-wedge high tibial osteotomy with platelet-rich plasma alone or in combination with mesenchymal stem cell treatment: A prospective study. Arthroscopy 2014, 30, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.L.; Lee, K.B.L.; Tai, B.C.; Law, P.; Lee, E.H.; Hui, J.H.P. Injectable cultured bone marrow-derived mesenchymal stem cells in varus knees with cartilage defects undergoing high tibial osteotomy: A prospective, randomized controlled clinical trial with 2 years’ follow-up. Arthroscopy 2013, 29, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Lotz, M. Cytokines in cartilage injury and repair. Clin. Orthop. Relat. Res. 2001, 391, S108–S115. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, J.C.; Bertrand, J.; Eldridge, S.E.; Dell’Accio, F. Cellular and molecular mechanisms of cartilage damage and repair. Drug Discov. Today 2014, 19, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Sellam, J.; Berenbaum, F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat. Rev. Rheumatol. 2010, 6, 625–635. [Google Scholar] [CrossRef]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and treatment of hip and knee osteoarthritis: A review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Kumagai, K.; Fujimaki, H.; Yamada, S.; Nejima, S.; Matsubara, J.; Inaba, Y. Changes of synovial fluid biomarker levels after opening wedge high tibial osteotomy in patients with knee osteoarthritis. Osteoarthr. Cartil. 2021, 29, 1020–1028. [Google Scholar] [CrossRef]
- Beekhuizen, M.; Giermanzxa, L.M.; van Spil, W.-E.; Van Osch, G.J.V.M.; Huizinga, T.W.J.; Saris, D.B.F.; Creemersy, L.B.; Zuurmond, A.-M. An explorative study comparing levels of soluble mediators in control and osteoarthritic synovial fluid. Osteoarthr. Cartil. 2013, 21, 918–922. [Google Scholar] [CrossRef]
- Nees, T.; Rosshirt, N.; Zhang, J.A.; Reiner, T.; Sorbi, R.; Tripel, E.; Walker, T.; Schiltenwolf, M.; Hagmann, S.; Moradi, B. Synovial cytokines significantly correlate with osteoarthritis-related knee pain and disability, inflammatory mediators of potential clinical relevance. J. Clin. Med. 2019, 8, 1343. [Google Scholar] [CrossRef]
- Kaszynski, J.; Bakowski, P.; Kiedrowski, B.; Stołowski, Ł.; Wasilewska-Burczyk, A.; Grzywacz, K.; Piontek, T. Intra-Articular Injections of Autologous Adipose Tissue or Platelet-Rich Plasma Comparably Improve Clinical and Functional Outcomes in Patients with Knee Osteoarthritis. Biomedicines 2022, 10, 684. [Google Scholar] [CrossRef] [PubMed]
- Keyt, L.K.; Hevesi, M.; Levy, B.A.; Krych, A.J.; Camp, C.L.; Stuart, M.J. High Tibial Osteotomy with a Modern Polyetheretherketone (PEEK) System: Mid-Term Results at a Mean of 6 Years Follow-Up. J. Knee Surg. 2020, 38, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Sawaguchi, T.; Takeuchi, R.; Nakamura, R.; Yonekura, A.; Akiyama, T.; Kerstan, M.; Goldhahn, S. Outcome after treatment of osteoarthritis with open-wedge high-tibial osteotomy with a plate: 2-year results of a Japanese cohort study. J. Orthop. Surg. 2020, 28, 2309499019887997. [Google Scholar] [CrossRef] [PubMed]
- Tchetina, E.V.; Glemba, K.E.; Markova, G.A.; Naryshkin, E.A.; Taskina, E.A.; Makarov, M.A.; Lila, A.M. Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery. Life 2020, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, Z.; Li, Y.; Hu, X.; Zhang, Y.; Fan, P. Profiling of inflammatory mediators in the synovial fluid related to pain in knee osteoarthritis. BMC Musculoskelet. Disord. 2020, 21, 99. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, B.; Stone, A.V.; Conley, C.E.W.; Hunt, E.R.; Lattermann, C.; Jacobs, C.A. Human synovial fluid interleukin-6, but not type II collagen breakdown, positively correlated with pain after anterior cruciate ligament injury and reconstruction. J. Orthop. Res. 2022. accepted. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Perricone, C.; Alessandri, C.; Modesti, M.; Iagnocco, A.; Croia, C.; Franco, M.D.; Valesini, G. Exploratory data analysis on the effects of non-pharmacological treatment for knee osteoarthritis. Clin. Exp. Rheumatol. 2010, 28, 250–253. [Google Scholar]
- Tsuchida, A.T.; Beekhuizen, M.; Rutgers, M.; van Osch, G.J.V.M.; Bekkers, J.E.J.; Bot, A.G.J.; Geurts, B.; Dhert, W.J.A.; Saris, D.B.F.; Creemers, L.B. Interleukin-6 is elevated in synovial fluid of patients with focal cartilage defects and stimulates cartilage matrix production in an in vitro regeneration model. Arthritis Res. Ther. 2012, 14, R262. [Google Scholar] [CrossRef]
- Liu, N.Q.; Lin, Y.; Li, L.; Lu, J.; Geng, D.; Zhang, J.; Jashashvili, T.; Buser, Z.; Magallanes, J.; Tassey, J.; et al. gp130/STAT3 signaling is required for homeostatic proliferation and anabolism in postnatal growth plate and articular chondrocytes. Commun. Biol. 2022, 5, 64. [Google Scholar] [CrossRef]
- Hong, Z.; Chen, J.; Zhang, S.; Zhao, C.; Bi, M.; Chen, X.; Bi, Q. Intra-articular injection of autologous adipose-derived stromal vascular fractions for knee osteoarthritis: A double-blind randomized self-controlled trial. Int. Orthop. 2019, 43, 1123–1134. [Google Scholar] [CrossRef]
- Strem, B.M.; Hicok, K.C.; Zhu, M.; Wulur, I.; Alfonso, Z.; Schreiber, R.E.; Fraser, J.K.; Hedrick, M.H. Multipotential differentiation of adipose tissue-derived stem cells. Keio J. Med. 2005, 54, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Stannus, O.; Jones, G.; Cicuttini, F.; Parameswaran, V.; Quinn, S.; Burgess, J.; Bing, C. Circulating levels of IL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults. Osteoarthr. Cartil. 2010, 18, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Raghu, H.; Lepus, C.M.; Wang, Q.; Wong, H.H.; Lingampalli, N.; Oliviero, F.; Punzi, L.; Giori, N.J.; Goo, S.B. CCL2/CCR2, but not CCL5/CCR5, mediates monocyte recruitment, inflammation and cartilage destruction in osteoarthritis. Ann. Rheum. Dis. 2017, 76, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Joung, S.; Yoon, D.S.; Cho, S.; Ko, E.A.; Lee, K.M.; Park, K.H.; Lee, J.W.; Kim, S.H. Downregulation of MicroRNA-495 Alleviates IL-1β Responses among Chondrocytes by Preventing SOX9 Reduction. Yonsei Med. J. 2021, 62, 650–659. [Google Scholar] [CrossRef]
- Li, L.; Jiang, B.E. Serum and synovial fluid chemokine ligand 2/monocyte chemoattractant protein 1 concentrations correlates with symptomatic severity in patients with knee osteoarthritis. Ann. Clin. Biochem. 2015, 52, 276–282. [Google Scholar] [CrossRef]
- Dansereau, M.A.; Midavaine, E.; Bégin-Lavallée, V.; Belkouch, M.; Beaudet, N.; Longpré, J.-M.; Mélik-Parsadaniantz, S.; Sarret, P. Mechanistic insights into the role of the chemokine CCL2/CCR2 axis in dorsal root ganglia to peripheral inflammation and pain hypersensitivity. J. Neuroinflamm. 2021, 18, 79. [Google Scholar] [CrossRef]
- Tsou, C.L.; Peters, W.; Si, Y.; Slaymaker, S.; Aslanian, A.M.; Weisberg, S.P.; Mack, M.; Charo, I.F. Critical roles for CCR2 and MCP-3 in monocyte mobilization from bone marrow and recruitment to inflammatory sites. J. Clin. Investig. 2007, 117, 902–909. [Google Scholar] [CrossRef]
- Tchetina, E.V.; Antoniou, J.; Tanzer, M.; Zukor, D.J.; Poole, A.R. TGFβ2 suppresses collagen cleavage in cultured human osteoarthritic cartilage, reduces expression of genes associated with chondrocyte hypertrophy and degradation, and increases prostaglandin E2 production. Am. J. Pathol. 2006, 168, 131–140. [Google Scholar] [CrossRef]
- Shah, P.; Keppler, L.; Rutkowski, J. A review of platelet derived growth factor playing pivotal role in bone regeneration. J. Oral Implantol. 2014, 40, 330–340. [Google Scholar] [CrossRef]
- Choi, W.S.; Jeon, O.H.; Kim, D.S. CD40 ligand shedding is regulated by interaction between matrix metalloproteinase-2 and platelet integrin αIIbβ3. J. Thromb. Haemost. 2010, 8, 1364–1371. [Google Scholar] [CrossRef]
- Scanzello, C.R.; Umoh, E.; Pessler, F.; Diaz-Torne, C.; Miles, T.; Dicarlo, E.; Potter, H.G.; Mandl, L.; Marx, R.; Rodeo, S.; et al. Local cytokine profiles in knee osteoarthritis: Elevated synovial fluid interleukin-15 differentiates early from end-stage disease. Osteoarthr. Cartil. 2009, 17, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, H.; Jingushi, S.; Izumi, T.; Fukunaga, M.; Matsushita, T.; Nakamura, T.; Mizuno, K.; Nakamura, T.; Nakamura, K. Local application of recombinant human fibroblast growth factor-2 on bone repair: A dose-escalation prospective trial on patients with osteotomy. J. Orthop. Res. 2007, 25, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Olmos Calvo, I.; Fodor, E.; Kardos, D.; Hornyák, I.; Hinsenkamp, A.; Kuten-Pella, O.; Gyevnár, Z.; Erdélyi, G.; Bárdos, T.; Mirkó Paukovits, T.; et al. A Pilot Clinical Study of Hyperacute Serum Treatment in Osteoarthritic Knee Joint: Cytokine Changes and Clinical Effects. Curr. Issues Mol. Biol. 2021, 43, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Asch, E.; Bloch, D. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1052. [Google Scholar] [CrossRef]
- Stoller, D.W.; Martin, C.; Crues, J.V., 3rd; Kaplan, L.; Mink, J.H. Meniscal tears: Pathologic correlation with MR imaging. Radiology 1987, 163, 731–735. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar]
- Outerbridge, R.E. The etiology of chondromalacia patellae. J. Bone Jt. Surg. Br. 1961, 43, 752–757. [Google Scholar] [CrossRef]
- Saragaglia, D.; Mercier, N.; Colle, P.-E. Computer-assisted osteotomies for genu varum deformity: Which osteotomy for which varus? Int. Orthop. (SICOT) 2010, 34, 185–190. [Google Scholar] [CrossRef]
- Bausset, O.; Giraudo, L.; Veran, J.; Magalon, J.; Coudreuse, J.-M.; Magalon, G.; Dubois, C.; Serratrice, N.; Dignat-George, F.; Sabatier, F. Formulation and Storage of Platelet-Rich. Plasma Homemade Prod. BioRes. Open Access 2012, 1, 3. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRP Subgroup (n = 10) Me [IQR] | SVF Subgroup (n = 10) Me [IQR] | P (Mann–Whitney U-Test) | |
|---|---|---|---|
| Age, years | 56.5 [52.5; 63.5] | 52.5 [45.0; 57.0] | n.s. |
| BMI, kg/m2 | 30.2 [26.5; 33.2] | 32.8 [25.2; 34.9] | n.s. |
| Outerbridge score | |||
| Medial femur | |||
| before surgery | |||
| 4 | 9 | 9 | - |
| 3 | 1 | 1 | - |
| Medial femur | |||
| 1.5 years after surgery | |||
| 4 | 7 | 9 | n.s. |
| 3 | 3 | 1 | n.s. |
| Lateral femur | |||
| before surgery | |||
| 1 | 3 | 1 | n.s. |
| 0 | 7 | 9 | n.s. |
| Lateral femur | |||
| 1.5 years after surgery | |||
| 2 | 1 | 1 | - |
| 1 | 4 | 0 | - |
| 0 | 5 | 9 | 0.05 * |
| Medial tibia | |||
| before surgery | |||
| 4 | 8 | 8 | - |
| 3 | 2 | 2 | - |
| Medial tibia | |||
| 1.5 years after surgery | |||
| 4 | 6 | 6 | - |
| 3 | 3 | 4 | n.s. |
| 2 | 1 | 0 | - |
| Lateral tibia | |||
| before surgery | |||
| 1 | 10 | 8 | n.s. |
| 0 | 0 | 2 | - |
| Lateral tibia | |||
| 1.5 years after surgery 2 | |||
| 1 | 3 | 3 | - |
| 0 | 7 | 6 | n.s. |
| 0 | 1 | - | |
| Koshino score | |||
| 1.5 years after surgery | |||
| Medial femur | |||
| C2 | 0 | 0 | - |
| C1 | 1 | 1 | - |
| B | 2 | 7 | 0.02 * |
| A | 6 | 2 | n.s. |
| Lateral femur | |||
| A | 10 | 10 | - |
| Medial tibia | |||
| C2 | 2 | 2 | - |
| C1 | 1 | 1 | - |
| B | 3 | 4 | n.s. |
| A | 4 | 3 | n.s. |
| Lateral tibia | |||
| A | 10 | 10 | - |
| MPTA (°) | |||
| Before surgery | 84.5 [83.5; 85.5] | 85.5 [84.6; 87.3] | n.s. |
| 1.5 years after surgery | 91.8 [90.7; 94.0] | 90.7 [90.3; 92.9] | n.s. |
| p ≤ 0.01 * | p ≤ 0.01 * | ||
| Varus–Valgus (°) | |||
| Varus before surgery | 8.3 [5; 11] | 6.2 [5; 7] | n.s. |
| Valgus 1.5 years after surgery | 1.6 [0.5; 3.5] | 1.2 [0.2; 3.35] | n.s. |
| Cytokine | Median Change | %Change | |
|---|---|---|---|
| PRP subgroup | IL-6 | 59.7 | −47.8 |
| IL-15 | 7.1 | +40.5 | |
| sCD40L | 27.2 | +74.3 | |
| IP-10 | 178 | −13.8 | |
| PDGF-AB/BB | 30.8 | +110.7 | |
| SVF subgroup | TNFα | 6.4 | −48.2 |
| IL-15 | 7.5 | −27.9 | |
| Flt-3L | 25.6 | −23.9 | |
| MIP-1β | 8.4 | −24.9 | |
| RANTES | 169.9 | −38.1 | |
| MCP-1 | 928 | +69.8 | |
| VEGF | 137.8 | −51.1 | |
| FGF2 | 35.6 | +21.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prizov, A.; Tchetina, E.; Eremin, I.; Zagorodniy, N.; Pulin, A.; Belyak, E.; Goncharov, E.; Kotenko, K.; Smyshlyaev, I.; Glukhova, S.; et al. Differences in Synovial Cytokine Profile Associated with Long-Term Clinical Outcomes in Patients with Knee Osteoarthritis Undergoing Corrective Osteotomy with Platelet-Rich Plasma or Stromal Vascular Fraction Post-Treatments. Int. J. Mol. Sci. 2022, 23, 12835. https://doi.org/10.3390/ijms232112835
Prizov A, Tchetina E, Eremin I, Zagorodniy N, Pulin A, Belyak E, Goncharov E, Kotenko K, Smyshlyaev I, Glukhova S, et al. Differences in Synovial Cytokine Profile Associated with Long-Term Clinical Outcomes in Patients with Knee Osteoarthritis Undergoing Corrective Osteotomy with Platelet-Rich Plasma or Stromal Vascular Fraction Post-Treatments. International Journal of Molecular Sciences. 2022; 23(21):12835. https://doi.org/10.3390/ijms232112835
Chicago/Turabian StylePrizov, Aleksey, Elena Tchetina, Ilya Eremin, Nikolay Zagorodniy, Andrey Pulin, Evgeniy Belyak, Evgeniy Goncharov, Konstantin Kotenko, Ivan Smyshlyaev, Svetlana Glukhova, and et al. 2022. "Differences in Synovial Cytokine Profile Associated with Long-Term Clinical Outcomes in Patients with Knee Osteoarthritis Undergoing Corrective Osteotomy with Platelet-Rich Plasma or Stromal Vascular Fraction Post-Treatments" International Journal of Molecular Sciences 23, no. 21: 12835. https://doi.org/10.3390/ijms232112835
APA StylePrizov, A., Tchetina, E., Eremin, I., Zagorodniy, N., Pulin, A., Belyak, E., Goncharov, E., Kotenko, K., Smyshlyaev, I., Glukhova, S., & Lila, A. (2022). Differences in Synovial Cytokine Profile Associated with Long-Term Clinical Outcomes in Patients with Knee Osteoarthritis Undergoing Corrective Osteotomy with Platelet-Rich Plasma or Stromal Vascular Fraction Post-Treatments. International Journal of Molecular Sciences, 23(21), 12835. https://doi.org/10.3390/ijms232112835