
Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Subjects
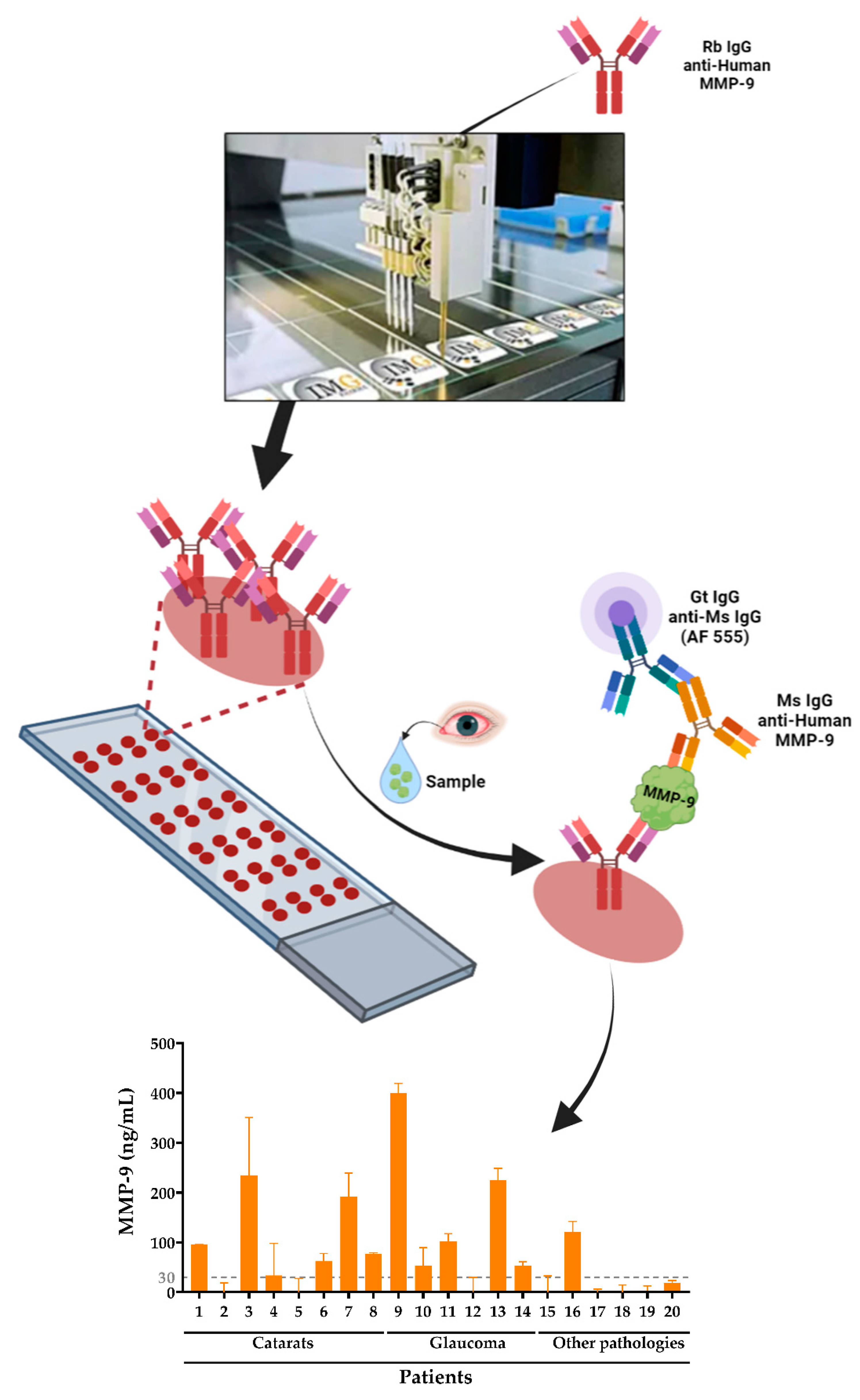
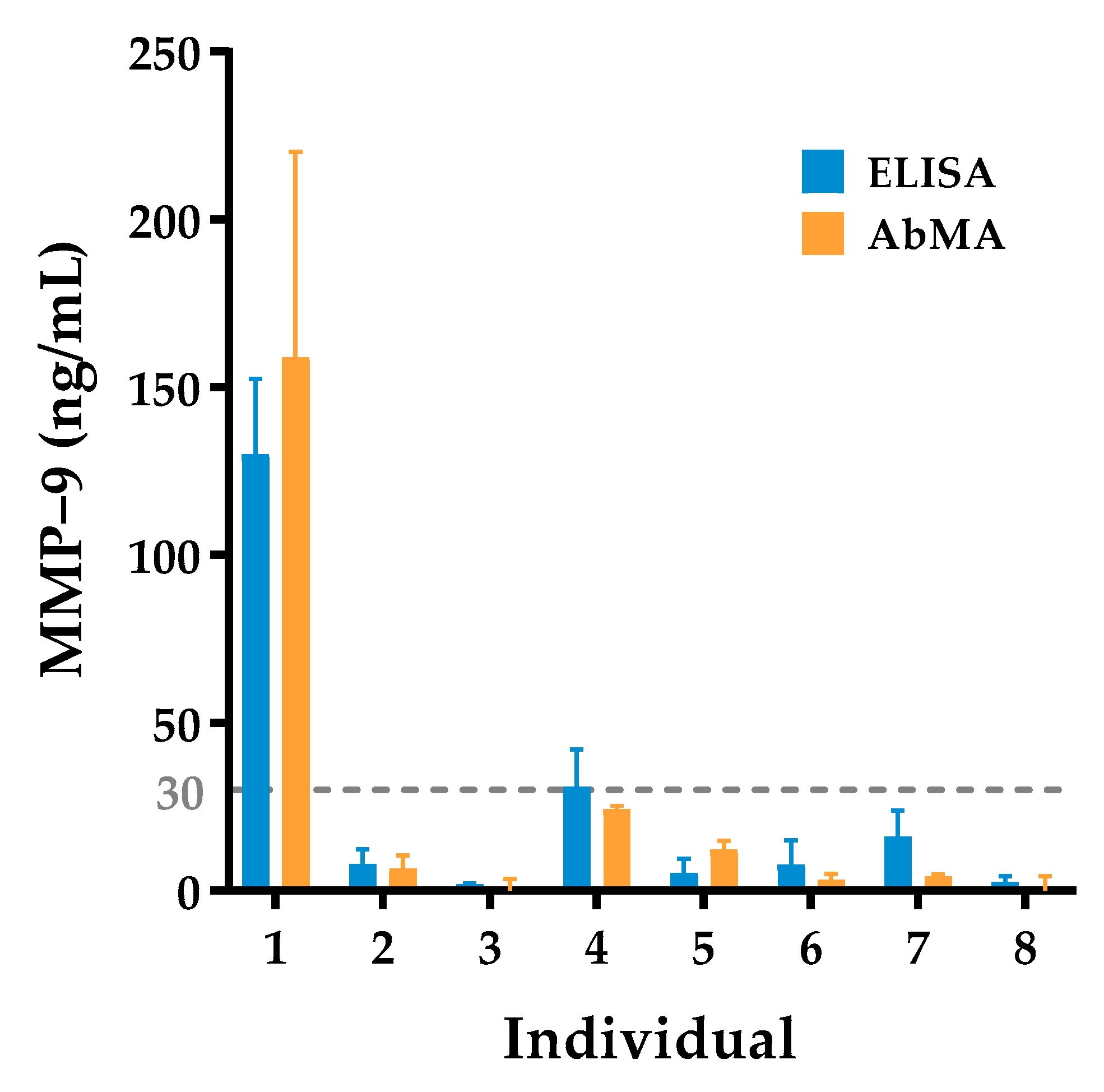
2.2. Antibody Microarray Validation
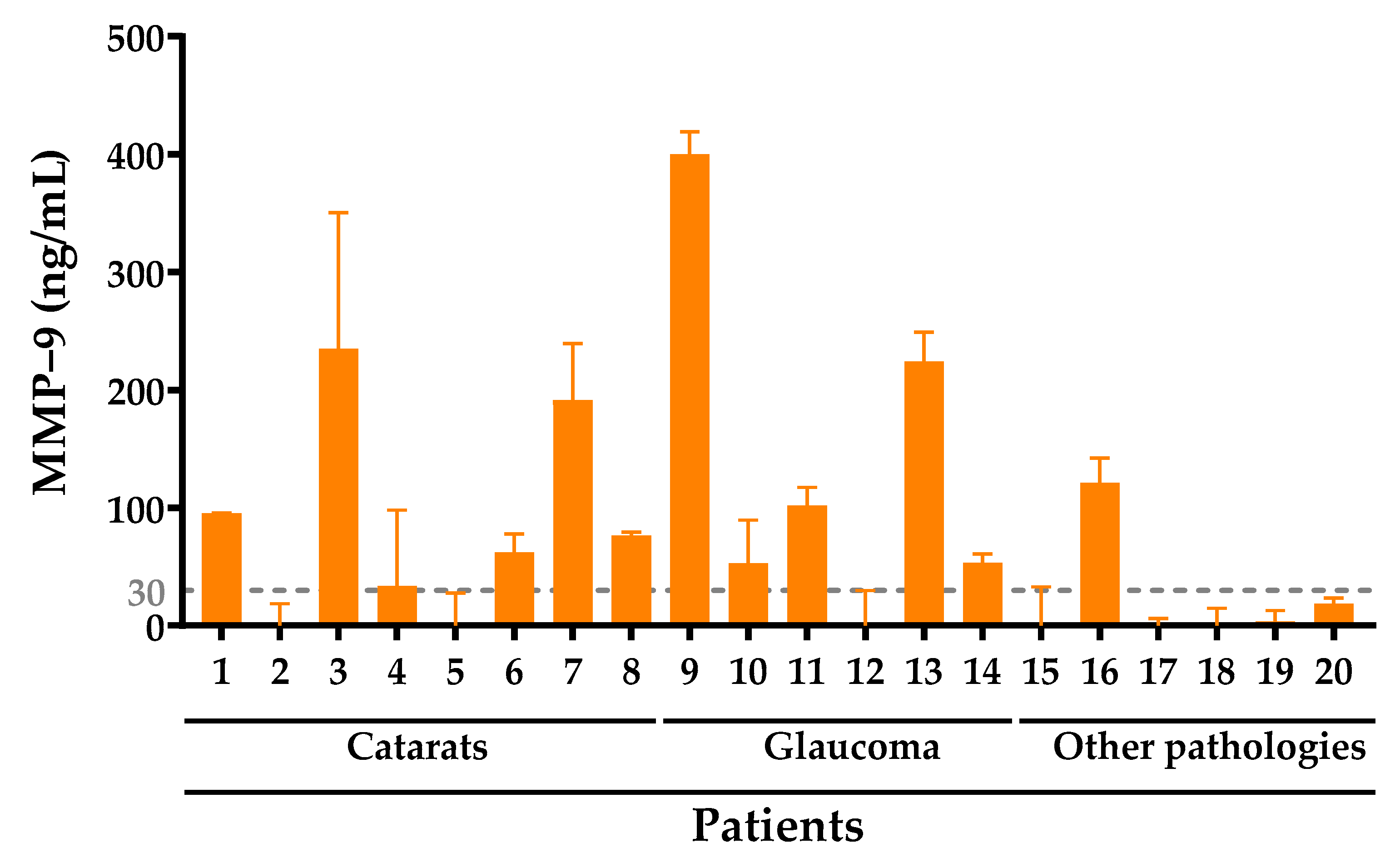
2.3. Analysis of Pathological Samples
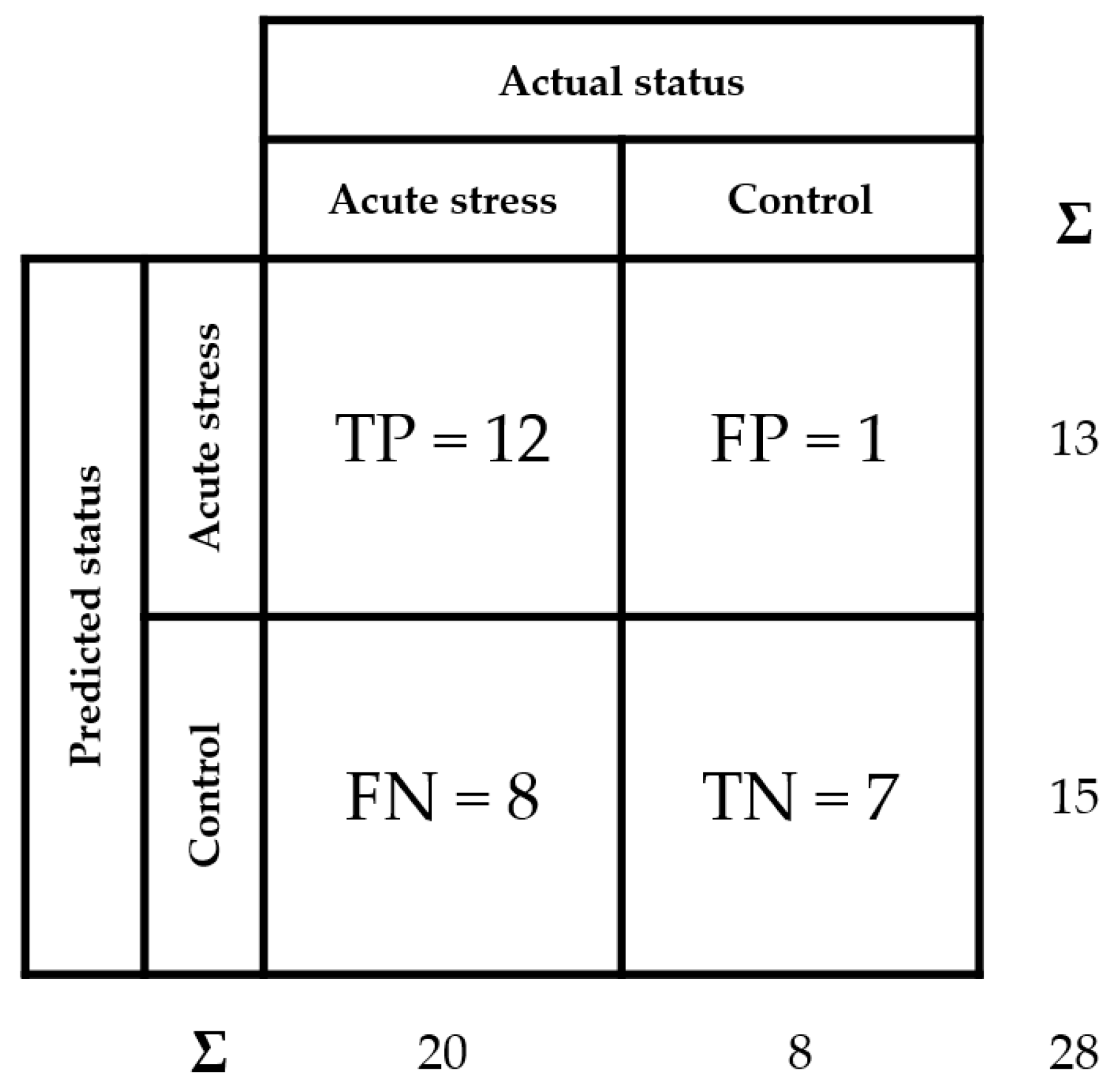
2.4. Evaluation of the Diagnostic Performance of the Test
3. Discussion
4. Materials and Methods
4.1. Tear Samples
4.2. Antibody Microarray Validation and Analysis of Pathological Samples
4.3. Evaluation of the Diagnostic Ability of the Test
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Clinical Enzymology. In Handbook of Clinical Biochemistry; World Scientific: Singapore, 2011; pp. 325–347. ISBN 978-981-283-737-0.
- Califf, R.M. Biomarker Definitions and Their Applications. Exp. Biol. Med. 2018, 243, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Hemalatha, T.; UmaMaheswari, T.; Krithiga, G.; Sankaranarayanan, P.; Puvanakrishnan, R. Enzymes in Clinical Medicine: An Overview. Indian J. Exp. Biol. 2013, 51, 777–788. [Google Scholar] [PubMed]
- Liang, S.-L.; Chan, D.W. Enzymes and Related Proteins as Cancer Biomarkers: A Proteomic Approach. Clin. Chim. Acta 2007, 381, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de la Fuente, M.; Lombardero, L.; Gómez-González, A.; Solari, C.; Angulo-Barturen, I.; Acera, A.; Vecino, E.; Astigarraga, E.; Barreda-Gómez, G. Enzyme Therapy: Current Challenges and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 9181. [Google Scholar] [PubMed]
- Smith, H.J.; Simons, C. Enzymes and Their Inhibitors. Drug Development; CRC Press: Boca Raton, FL, USA, 2019; ISBN 9780367393571. [Google Scholar]
- Coussens, L.M.; Werb, Z. Inflammation and Cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Glass, C.K.; Saijo, K.; Winner, B.; Marchetto, M.C.; Gage, F.H. Mechanisms Underlying Inflammation in Neurodegeneration. Cell 2010, 140, 918–934. [Google Scholar] [CrossRef] [Green Version]
- Pohl, D.; Benseler, S. Systemic Inflammatory and Autoimmune Disorders. Handb. Clin. Neurol. 2013, 112, 1243–1252. [Google Scholar] [CrossRef]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and Metabolic Disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Fox, R.I. Sjögren’s Syndrome. Lancet 2005, 366, 321–331. [Google Scholar] [CrossRef]
- Golden, M.I.; Meyer, J.J.; Patel, B.C. Dry Eye Syndrome. In Treasure Island (FL); Cassell: London, UK, 2021. [Google Scholar]
- Kalogeropoulos, D.; Sung, V.C. Pathogenesis of Uveitic Glaucoma. J. Curr. Glaucoma Pract. 2018, 12, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.C.; Stewart, J.A.; Nelson, L.A. Ocular Surface Disease in Patients with Ocular Hypertension and Glaucoma. Curr. Eye Res. 2011, 36, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Labbé, A.; Liang, H.; Pauly, A.; Brignole-Baudouin, F. Preservatives in Eyedrops: The Good, the Bad and the Ugly. Prog. Retin. Eye Res. 2010, 29, 312–334. [Google Scholar] [CrossRef] [PubMed]
- Manicone, A.M.; McGuire, J.K. Matrix metalloproteinases as modulators of inflammation. Semin Cell Dev Biol. 2008, 19, 34–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissinen, L.; Kähäri, V.-M. Matrix Metalloproteinases in Inflammation. Biochim. Biophys. Acta 2014, 1840, 2571–2580. [Google Scholar] [CrossRef]
- Hardy, E.; Fernandez-Patron, C. Destroy to Rebuild: The Connection Between Bone Tissue Remodeling and Matrix Metalloproteinases. Front. Physiol. 2020, 11, 47. [Google Scholar] [CrossRef]
- Caley, M.P.; Martins, V.L.C.; O’Toole, E.A. Metalloproteinases and Wound Healing. Adv. Wound Care 2015, 4, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef]
- Recalde, J.I.; Duran, J.A.; Rodriguez-Agirretxe, I.; Soria, J.; Sanchez-Tena, M.A.; Pereiro, X.; Suarez, T.; Acera, A. Changes in Tear Biomarker Levels in Keratoconus after Corneal Collagen Crosslinking. Mol. Vis. 2019, 25, 12–21. [Google Scholar]
- Nagaraj, V.J.; Eaton, S.; Wiktor, P.; Casillo, L.; Von Thun Und Hohenstein-Blaul, N.; Kunst, S.; Pfeiffer, N.; Grus, F.H.; de Paiva, C.S.; Izzotti, A.; et al. Tear Proteome Analysis in Ocular Surface Diseases Using Label-Free LC-MS/MS and Multiplexed-Microarray Biomarker Validation. Sci. Rep. 2017, 16, 17478. [Google Scholar] [CrossRef] [Green Version]
- Messmer, E.M.; von Lindenfels, V.; Garbe, A.; Kampik, A. Matrix Metalloproteinase 9 Testing in Dry Eye Disease Using a Commercially Available Point-of-Care Immunoassay. Ophthalmology 2016, 123, 2300–2308. [Google Scholar] [CrossRef] [PubMed]
- Benitez-Del-Castillo, J.M.; Soria, J.; Acera, A.; Muñoz, A.M.; Rodríguez, S.; Suárez, T. Quantification of a Panel for Dry-Eye Protein Biomarkers in Tears: A Comparative Pilot Study Using Standard ELISA and Customized Microarrays. Mol. Vis. 2021, 27, 243–261. [Google Scholar] [PubMed]
- Acera, A.; Vecino, E.; Duran, J.A. Tear MMP-9 Levels as a Marker of Ocular Surface Inflammation in Conjunctivochalasis. Investig. Ophthalmol. Vis. Sci. 2013, 54, 8285–8291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanza, N.L.; Valenzuela, F.; Perez, V.L.; Galor, A. The Matrix Metalloproteinase 9 Point-of-Care Test in Dry Eye. Ocul. Surf. 2016, 14, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Gordon, G.M.; Ledee, D.R.; Feuer, W.J.; Fini, M.E. Cytokines and Signaling Pathways Regulating Matrix Metalloproteinase-9 (MMP-9) Expression in Corneal Epithelial Cells. J. Cell. Physiol. 2009, 221, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Messmer, E.M. The Pathophysiology, Diagnosis, and Treatment of Dry Eye Disease. Dtsch. Arztebl. Int. 2015, 112, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Nichols, K.K.; Nichols, J.J.; Mitchell, G.L. The Lack of Association between Signs and Symptoms in Patients with Dry Eye Disease. Cornea 2004, 23, 762–770. [Google Scholar] [CrossRef]
- Nagaraj, V.J.; Eaton, S.; Wiktor, P.; Casillo, L.; Von Thun Und Hohenstein-Blaul, N.; Kunst, S.; Pfeiffer, N.; Grus, F.H.; de Paiva, C.S.; Izzotti, A.; et al. In Vitro Validation of the Tear Matrix Metalloproteinase 9 In-Situ Immunoassay. Lancet 2020, 15, 225–234. [Google Scholar]
- Jun, J.H.; Lee, Y.H.; Son, M.J.; Kim, H. Importance of Tear Volume for Positivity of Tear Matrix Metalloproteinase-9 Immunoassay. PLoS ONE 2020, 15, e0235408. [Google Scholar] [CrossRef]
- Manuel, I.; Barreda-Gómez, G.; González de San Román, E.; Veloso, A.; Fernández, J.A.; Giralt, M.T.; Rodríguez-Puertas, R. Neurotransmitter Receptor Localization: From Autoradiography to Imaging Mass Spectrometry. ACS Chem. Neurosci. 2015, 6, 362–373. [Google Scholar] [CrossRef]
- Hebert-Chatelain, E.; Desprez, T.; Serrat, R.; Bellocchio, L.; Soria-Gomez, E.; Busquets-Garcia, A.; Zottola, A.C.P.; Delamarre, A.; Cannich, A.; Vincent, P.; et al. A Cannabinoid Link between Mitochondria and Memory. Nature 2016, 539, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Rienda, B.; Elexpe, A.; Tolentino-Cortez, T.; Gulak, M.; Bruzos-Cidón, C.; Torrecilla, M.; Astigarraga, E.; Barreda-Gómez, G. Analysis of Acetylcholinesterase Activity in Cell Membrane Microarrays of Brain Areas as a Screening Tool to Identify Tissue Specific Inhibitors. Analytica 2021, 2, 25–36. [Google Scholar] [CrossRef]
- Fernández, R.; Garate, J.; Tolentino-Cortez, T.; Herraiz, A.; Lombardero, L.; Ducrocq, F.; Rodríguez-Puertas, R.; Trifilieff, P.; Astigarraga, E.; Barreda-Gómez, G.; et al. Microarray and Mass Spectrometry-Based Methodology for Lipid Profiling of Tissues and Cell Cultures. Anal. Chem. 2019, 91, 15967–15973. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Magraner, L.; de la Fuente, M.; Evans, C.; Miles, J.; Elexpe, A.; Rodriguez-Astigarraga, M.; Astigarraga, E.; Barreda-Gómez, G. Quantification of PD-1/PD-L1 Interaction between Membranes from PBMCs and Melanoma Samples Using Cell Membrane Microarray and Time-Resolved Förster Resonance Energy Transfer. Analytica 2021, 2, 156–170. [Google Scholar] [CrossRef]
- Borrebaeck, C.A.K. Antibody Microarray-Based Oncoproteomics. Expert Opin. Biol. Ther. 2006, 6, 833–838. [Google Scholar] [CrossRef]
- Izzotti, A.; Centofanti, M.; Saccà, S.C. Molecular Diagnostics of Ocular Diseases: The Application of Antibody Microarray. Expert Rev. Mol. Diagn. 2012, 12, 629–643. [Google Scholar] [CrossRef]
- Chen, Z.; Dodig-Crnković, T.; Schwenk, J.M.; Tao, S.-C. Current Applications of Antibody Microarrays. Clin. Proteom. 2018, 15, 7. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Wark, A.W.; Corn, R.M. Microarray Methods for Protein Biomarker Detection. Analyst 2008, 133, 975–983. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, T. An Introduction to ROC Analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Örnemark, U.; Magnusson, B. Eurachem Guide: The Fitness for Purpose of Analytical Methods—A Laboratory Guide to Method Validation and Related Topics, 2nd ed.; Eurachem: Warwick, UK, 2014; ISBN 978-91-87461-59-0. [Google Scholar]
- Jamerson, E.C.; Elhusseiny, A.M.; ElSheikh, R.H.; Eleiwa, T.K.; el Sayed, Y.M. Role of Matrix Metalloproteinase 9 in Ocular Surface Disorders. Eye Contact Lens 2020, 46 (Suppl. 2), S57–S63. [Google Scholar] [CrossRef] [PubMed]
- McCluskey, P.; Powell, R.J. The Eye in Systemic Inflammatory Diseases. Lancet 2004, 364, 2125–2133. [Google Scholar] [CrossRef]
- Chotikavanich, S.; de Paiva, C.S.; Li, D.Q.; Chen, J.J.; Bian, F.; Farley, W.J.; Pflugfelder, S.C. Production and Activity of Matrix Metalloproteinase-9 on the Ocular Surface Increase in Dysfunctional Tear Syndrome. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3203–3209. [Google Scholar] [CrossRef] [PubMed]
- Macbeth, G.; Razumiejczyk, E.; Ledesma, R.D. Cliff’s Delta Calculator: A Non-Parametric Effect Size Program for Two Groups of Observations. Univ. Psychol. 2011, 10, 545–555. [Google Scholar] [CrossRef]
- Von Thun Und Hohenstein-Blaul, N.; Kunst, S.; Pfeiffer, N.; Grus, F.H. Biomarkers for Glaucoma: From the Lab to the Clinic. Eye 2017, 31, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Nagaraj, V.J.; Eaton, S.; Wiktor, P. NanoProbeArrays for the Analysis of Ultra-Low-Volume Protein Samples Using Piezoelectric Liquid Dispensing Technology. J. Lab. Autom. 2011, 16, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Seo, J.H.; Lim, S.-H. Evaluation of Ocular Surface Disease in Elderly Patients with Glaucoma: Expression of Matrix Metalloproteinase-9 in Tears. Eye 2021, 35, 892–900. [Google Scholar] [CrossRef]
- Zaleska-Żmijewska, A.; Strzemecka, E.; Wawrzyniak, Z.M.; Szaflik, J.P. Extracellular MMP-9-Based Assessment of Ocular Surface Inflammation in Patients with Primary Open-Angle Glaucoma. J. Ophthalmol. 2019, 2019, 1240537. [Google Scholar] [CrossRef] [Green Version]
- Sahay, P.; Rao, A.; Padhy, D.; Sarangi, S.; Das, G.; Reddy, M.M.; Modak, R. Functional Activity of Matrix Metalloproteinases 2 and 9 in Tears of Patients With Glaucoma. Investig. Ophthalmol. Vis. Sci. 2017, 58, BIO106–BIO113. [Google Scholar] [CrossRef]
- Kim, J.M.; Sung, K.R.; Lee, J.W.; Kyung, H.; Rho, S.; Kim, C.Y. Efficacy and Safety of Newly Developed Preservative-Free Latanoprost 0.005% Eye Drops versus Preserved Latanoprost 0.005% in Open Angle Glaucoma and Ocular Hypertension: 12-Week Results of a Randomized, Multicenter, Controlled Phase III Trial. Int. J. Ophthalmol. 2021, 14, 1539–1547. [Google Scholar] [CrossRef]
- Labbé, A.; Terry, O.; Brasnu, E.; Van Went, C.; Baudouin, C. Tear Film Osmolarity in Patients Treated for Glaucoma or Ocular Hypertension. Cornea 2012, 31, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Aragona, P.; Messmer, E.M.; Tomlinson, A.; Calonge, M.; Boboridis, K.G.; Akova, Y.A.; Geerling, G.; Labetoulle, M.; Rolando, M. Role of Hyperosmolarity in the Pathogenesis and Management of Dry Eye Disease: Proceedings of the OCEAN Group Meeting. Ocul. Surf. 2013, 11, 246–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herreras, J.M.; Pastor, J.C.; Calonge, M.; Asensio, V.M. Ocular Surface Alteration after Long-Term Treatment with an Antiglaucomatous Drug. Ophthalmology 1992, 99, 1082–1088. [Google Scholar] [CrossRef]
- Baudouin, C.; Liang, H.; Hamard, P.; Riancho, L.; Creuzot-Garcher, C.; Warnet, J.-M.; Brignole-Baudouin, F. The Ocular Surface of Glaucoma Patients Treated over the Long Term Expresses Inflammatory Markers Related to Both T-Helper 1 and T-Helper 2 Pathways. Ophthalmology 2008, 115, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Martinez-de-la-Casa, J.M.; Perez-Bartolome, F.; Urcelay, E.; Santiago, J.L.; Moreno-Montañes, J.; Arriola-Villalobos, P.; Benitez-Del-Castillo, J.M.; Garcia-Feijoo, J. Tear Cytokine Profile of Glaucoma Patients Treated with Preservative-Free or Preserved Latanoprost. Ocul. Surf. 2017, 15, 723–729. [Google Scholar] [CrossRef]
- VanDerMeid, K.R.; Su, S.P.; Ward, K.W.; Zhang, J.-Z. Correlation of Tear Inflammatory Cytokines and Matrix Metalloproteinases with Four Dry Eye Diagnostic Tests. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1512–1518. [Google Scholar] [CrossRef]
- Honda, N.; Miyai, T.; Nejima, R.; Miyata, K.; Mimura, T.; Usui, T.; Aihara, M.; Araie, M.; Amano, S. Effect of Latanoprost on the Expression of Matrix Metalloproteinases and Tissue Inhibitor of Metalloproteinase 1 on the Ocular Surface. Arch. Ophthalmol. 2010, 128, 466–471. [Google Scholar] [CrossRef]
- Weinreb, R.; Robinson, M.; Dibas, M.; Stamer, W. Matrix Metalloproteinases and Glaucoma Treatment. J. Ocul. Pharmacol. Ther. 2020, 36, 208–228. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma: A Review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Casillo, L. Glaucoma: May New Technologies Help in Early Diagnosis? J. Clin. Res. Ophthalmol. 2018, 5, 5–8. [Google Scholar] [CrossRef] [Green Version]
- Garway-Heath, D.F. Early Diagnosis in Glaucoma. Prog. Brain Res. 2008, 173, 47–57. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tear Sample | Group | Age | Gender | Conditions | Schirmer’s Test (mm) |
|---|---|---|---|---|---|
| HC 1 | Healthy Control | 25 | Male | n/a | n/a |
| HC 2 | Healthy Control | 26 | Female | n/a | n/a |
| HC 3 | Healthy Control | 30 | Female | n/a | n/a |
| HC 4 | Healthy Control | 23 | Female | n/a | n/a |
| HC 5 | Healthy Control | 40 | Male | n/a | n/a |
| HC 6 | Healthy Control | 23 | Female | n/a | n/a |
| HC 7 | Healthy Control | 24 | Female | n/a | n/a |
| HC 8 | Healthy Control | 29 | Female | n/a | n/a |
| P 1 | Patient | 79 | Female | Cataracts | 5 |
| P 2 | Patient | 73 | Female | Cataracts | 5 |
| P 3 | Patient | 66 | Female | Cataracts | 3 |
| P 4 | Patient | 81 | Female | Cataracts | 5 |
| P 5 | Patient | 89 | Female | Cataracts | 2 |
| P 6 | Patient | 62 | Female | Cataracts | 0 |
| P 7 | Patient | 70 | Male | Cataracts | 1 |
| P 8 | Patient | 73 | Female | Cataracts | 3 |
| P 9 | Patient | 68 | Female | Glaucoma | 6 |
| P 10 | Patient | 60 | Male | Glaucoma | 5 |
| P 11 | Patient | 75 | Female | Glaucoma | 7 |
| P 12 | Patient | 70 | Female | Glaucoma | 4 |
| P 13 | Patient | 82 | Male | Glaucoma | 5 |
| P 14 | Patient | 82 | Male | Glaucoma | 5 |
| P 15 | Patient | 52 | Male | MGD | 5 |
| P 16 | Patient | 49 | Female | Allergy | 4 |
| P 17 | Patient | 29 | Female | DE | 5 |
| P 18 | Patient | 30 | Female | DE | 6 |
| P 19 | Patient | 49 | Female | Allergy | 5 |
| P 20 | Patient | 38 | Female | MGD + DE | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Fuente, M.; Rodríguez-Agirretxe, I.; Vecino, E.; Astigarraga, E.; Acera, A.; Barreda-Gómez, G. Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays. Int. J. Mol. Sci. 2022, 23, 5639. https://doi.org/10.3390/ijms23105639
de la Fuente M, Rodríguez-Agirretxe I, Vecino E, Astigarraga E, Acera A, Barreda-Gómez G. Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays. International Journal of Molecular Sciences. 2022; 23(10):5639. https://doi.org/10.3390/ijms23105639
Chicago/Turabian Stylede la Fuente, Miguel, Iñaki Rodríguez-Agirretxe, Elena Vecino, Egoitz Astigarraga, Arantxa Acera, and Gabriel Barreda-Gómez. 2022. "Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays" International Journal of Molecular Sciences 23, no. 10: 5639. https://doi.org/10.3390/ijms23105639
APA Stylede la Fuente, M., Rodríguez-Agirretxe, I., Vecino, E., Astigarraga, E., Acera, A., & Barreda-Gómez, G. (2022). Elevation of Tear MMP-9 Concentration as a Biomarker of Inflammation in Ocular Pathology by Antibody Microarray Immunodetection Assays. International Journal of Molecular Sciences, 23(10), 5639. https://doi.org/10.3390/ijms23105639