
A Sodium Oxalate-Rich Diet Induces Chronic Kidney Disease and Cardiac Dysfunction in Rats

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
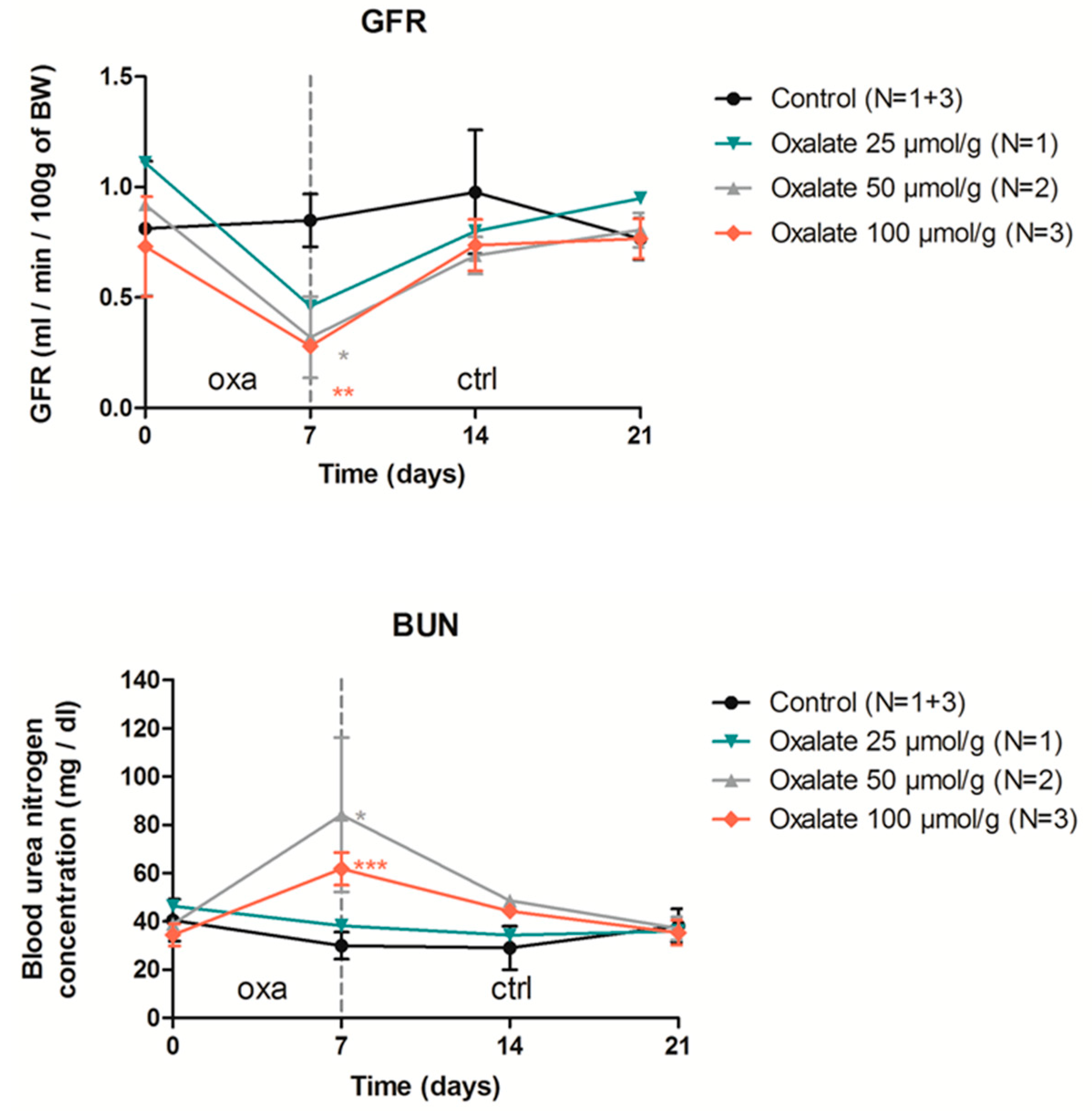
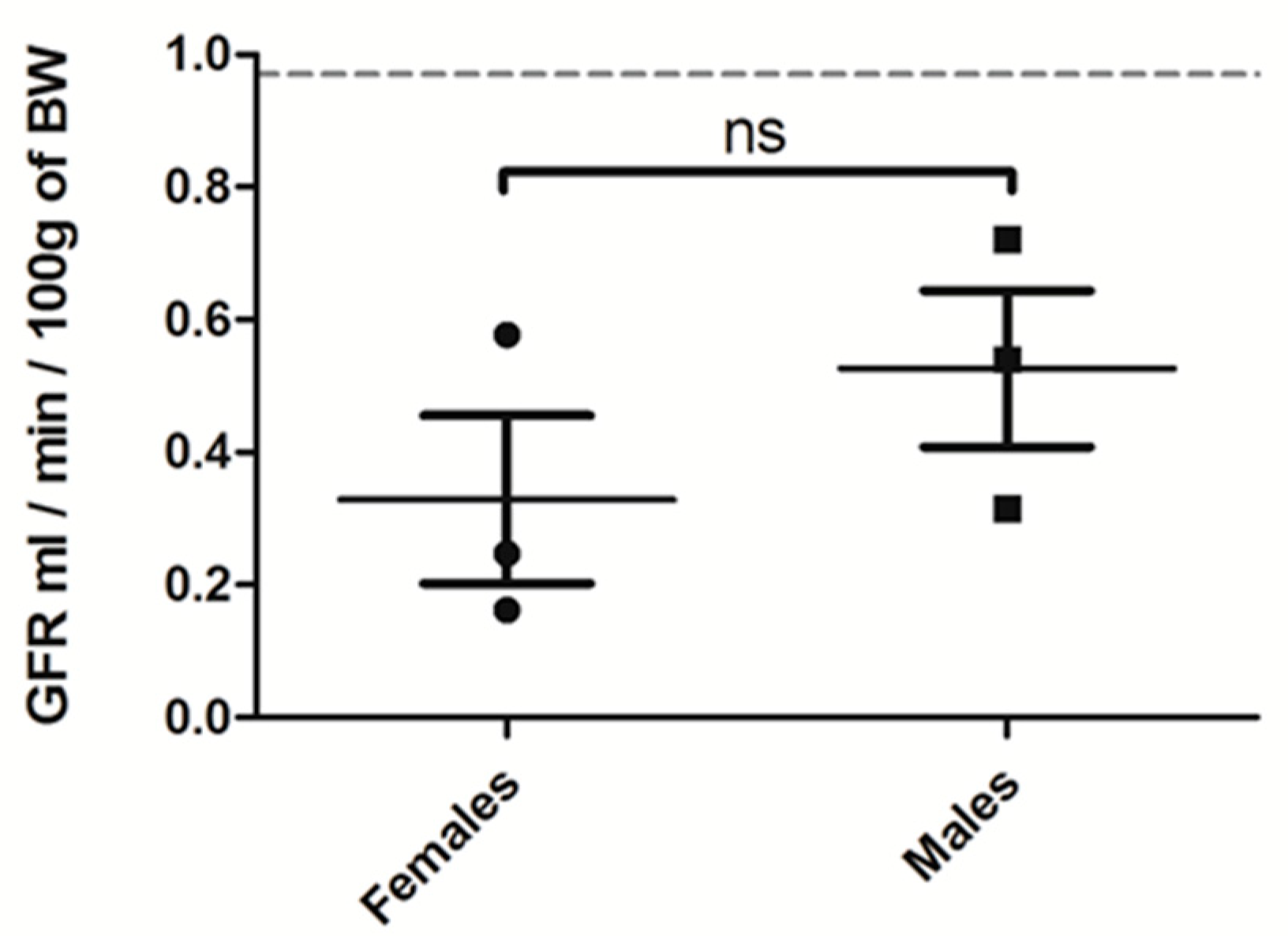
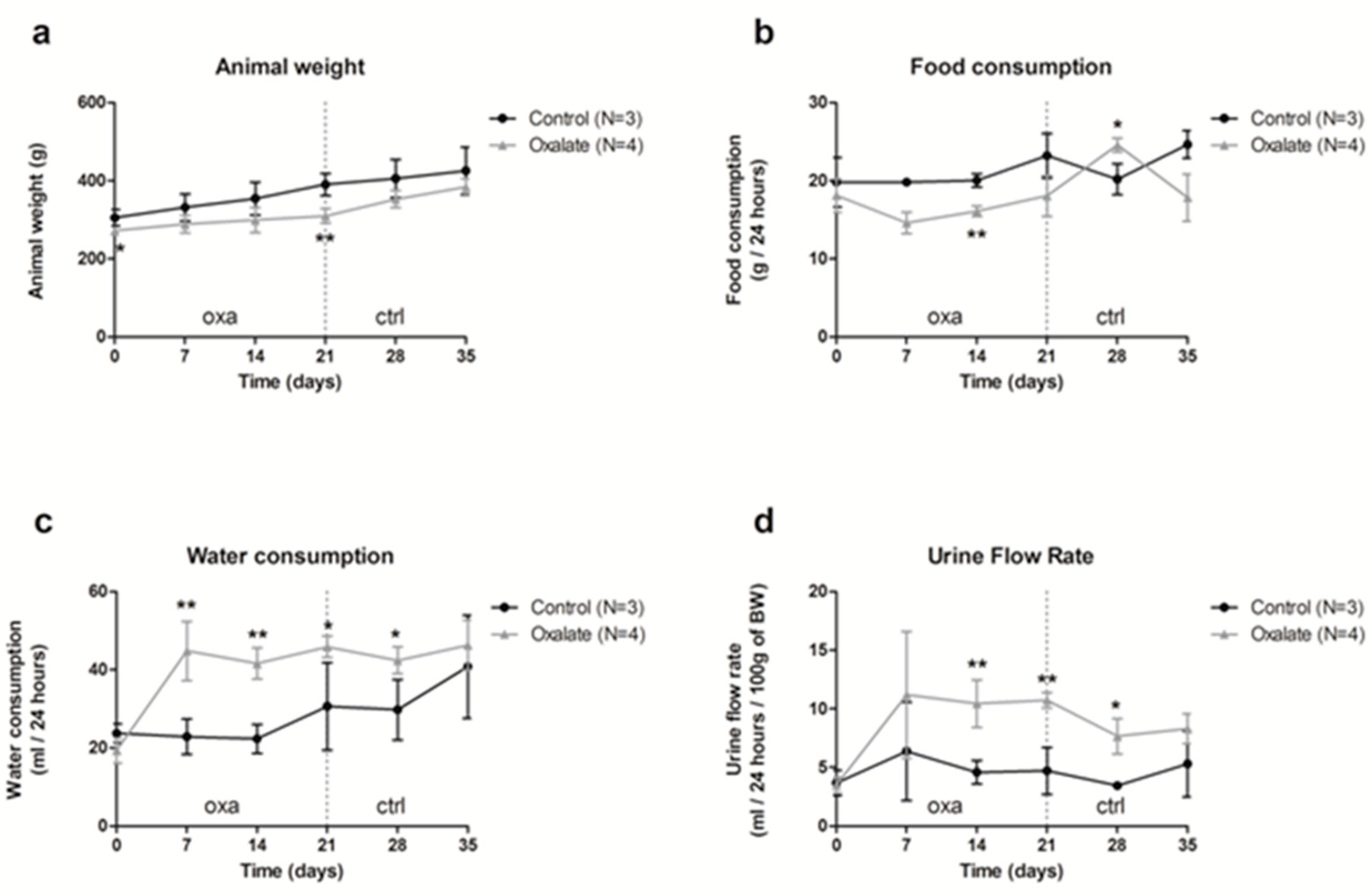
2.1. High Oxalate Diet Significantly Impaired Rats’ Biological Parameters and Kidney Function
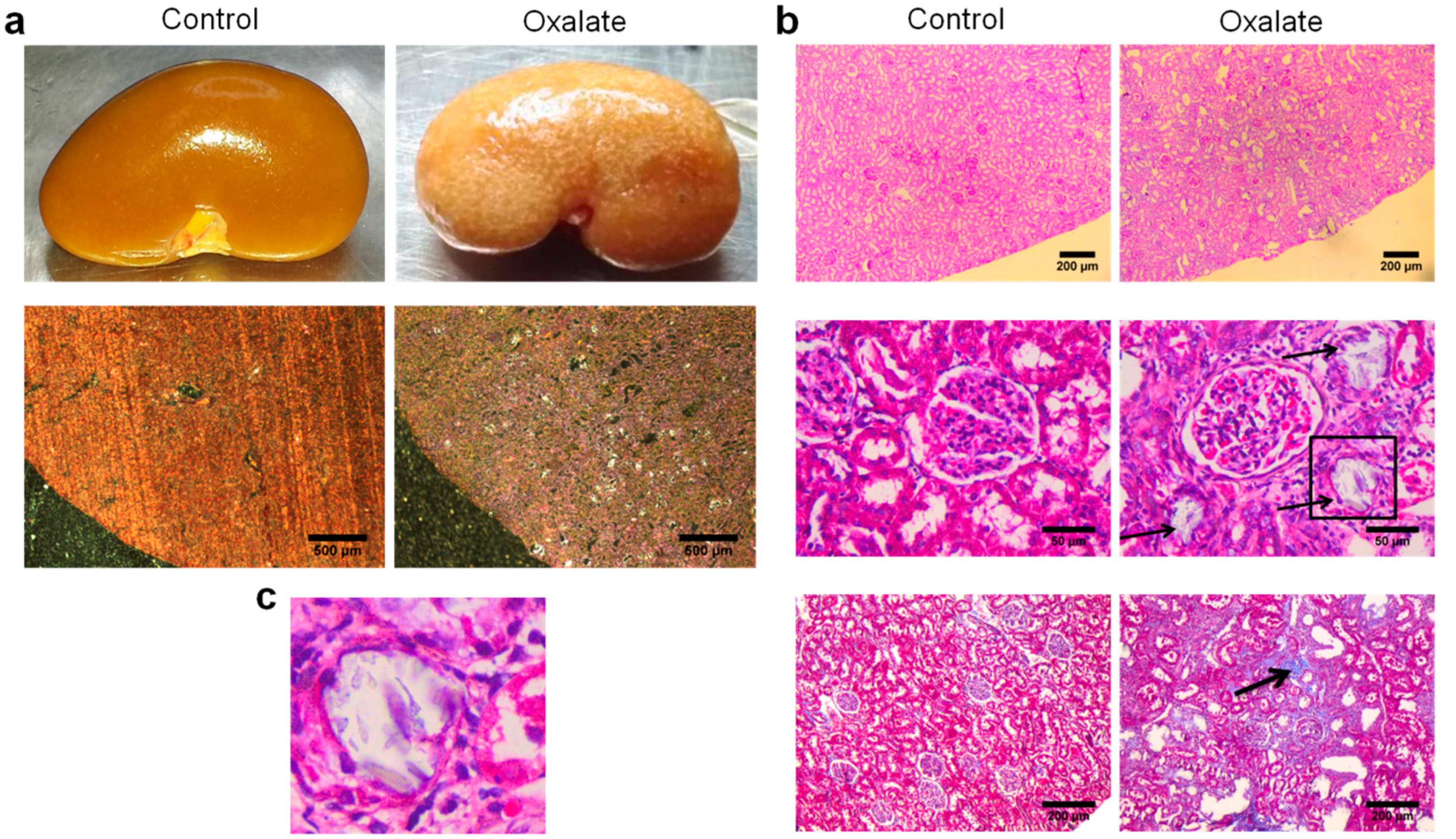
2.2. High Oxalate Diet Induced Tubular Atrophy and Fibrosis though Oxalate Crystals’ Deposition in the Tubular Lumen
2.3. Modulation of High Oxalate Diet
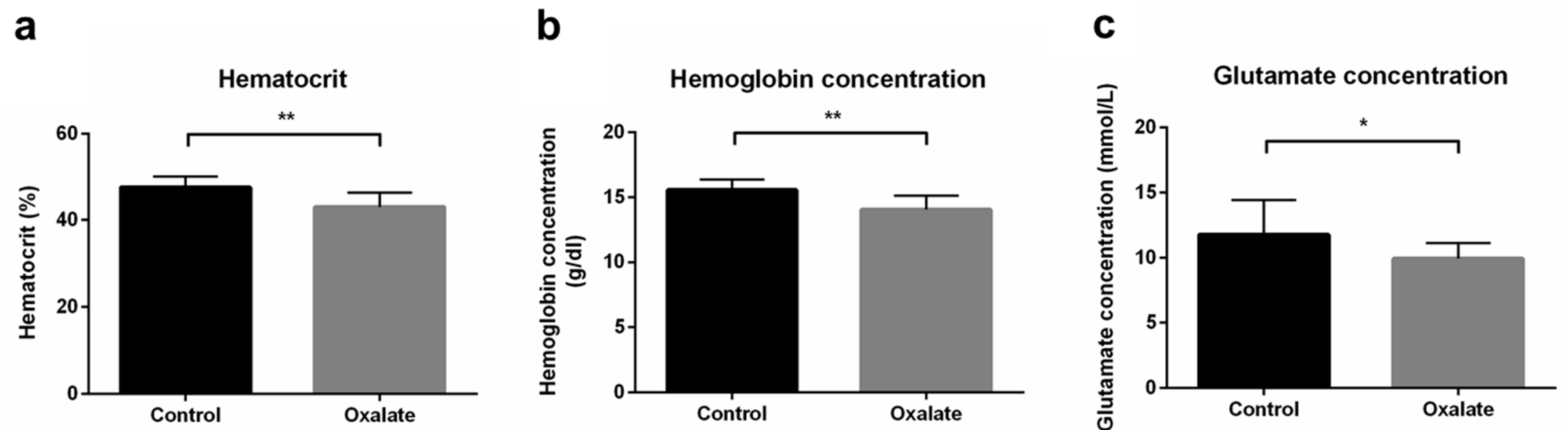
2.4. Effect of Oxalate Diet on Systemic Complications and Cardiovascular System
3. Discussion
4. Materials and Methods
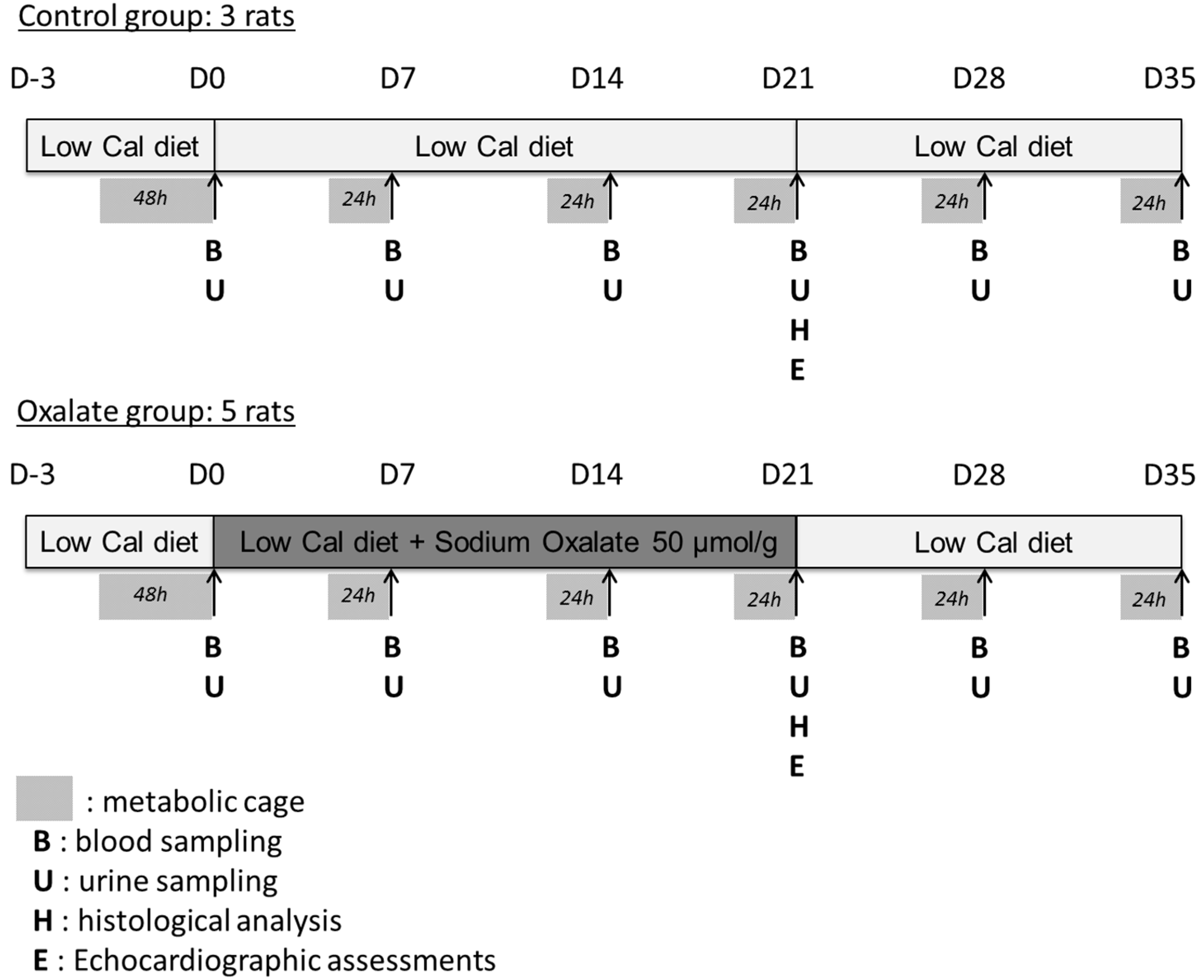
4.1. Animal Studies
4.2. Assessment of Renal Function
4.3. Blood Pressure Measurement
4.4. Echocardiographic Assessments
4.5. Histological Analyses
4.6. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BUN | blood urea nitrogen |
| Ca2+ | ionized calcium |
| cBase(Ecf) | standard base excess |
| cHCO3−(P,st) | standard bicarbonate |
| CKD | chronic kidney disease |
| Cl− | chloride |
| ctO2 | oxygen content |
| CTR | control diet |
| E/e’ | early diastolic transmitral flow velocity/mitral annular early diastolic velocity |
| FHHb | fraction of deoxyhemoglobin |
| FO2Hb | fraction of oxyhemoglobin |
| GFR | glomerular filtration rate |
| IVS | intraventricular septum |
| K+ | potassium |
| LV | left ventricular |
| Na+ | sodium |
| OXA | oxalate |
| p50 | oxygen tension at half saturation of blood |
| pCO2 | carbon dioxide partial pressure |
| PFA | paraformaldehyde |
| pO2 | oxygen partial pressure |
| PTX3 | pentraxin 3 |
| sO2 | oxygen saturation |
| TNF | tumor necrosis factor |
| TNFR | TNF receptor |
Appendix A
References
- Centers for Disease Control and Prevention. Age-Adjusted Prevalence of CKD Stages 1–4 by Gender 1999–2012. Chronic Kidney Disease (CKD) Surveillance Project Website. Available online: https://Nccd.cdc.gov (accessed on 6 December 2016).
- Borghi, L.; Schianchi, T.; Meschi, T.; Guerra, A.; Allegri, F.; Maggiore, U.; Novarini, A. Comparison of Two Diets for the Prevention of Recurrent Stones in Idiopathic Hypercalciuria. N. Engl. J. Med. 2002, 346, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.; Kumar, P.; Reddy, T.; Wood, K.D.; Knight, J.; Assimos, D.G.; Holmes, R.P. Dietary oxalate and kidney stone formation. Am. J. Physiol. Physiol. 2019, 316, F409–F413. [Google Scholar] [CrossRef] [PubMed]
- Bargagli, M.; Tio, M.C.; Waikar, S.S.; Ferraro, P.M. Dietary Oxalate Intake and Kidney Outcomes. Nutrients 2020, 12, 2673. [Google Scholar] [CrossRef] [PubMed]
- Plata, C.; Cruz, C.; Cervantes, L.G.; Ramírez, V. The gut microbiota and its relationship with chronic kidney disease. Int. Urol. Nephrol. 2019, 51, 2209–2226. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, P.M.; Taylor, E.N.; Eisner, B.H.; Gambaro, G.; Rimm, E.B.; Mukamal, K.J.; Curhan, G.C. History of Kidney Stones and the Risk of Coronary Heart Disease. JAMA 2013, 310, 408–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, I.G.; Kang, T.; Bang, J.K.; Park, J.; Kim, W.; Hwang, S.S.; Kim, H.K.; Park, H.K. Association Between Metabolic Syndrome and the Presence of Kidney Stones in a Screened Population. Am. J. Kidney Dis. 2011, 58, 383–388. [Google Scholar] [CrossRef]
- Zhu, C.; Liang, Q.; Liu, Y.; Kong, D.; Zhang, J.; Wang, H.; Wang, K.; Guo, Z. Kidney injury in response to crystallization of calcium oxalate leads to rearrangement of the intrarenal T cell receptor delta immune repertoire. J. Transl. Med. 2019, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Stepanova, N. Role of Impaired Oxalate Homeostasis in Cardiovascular Disease in Patients With End-Stage Renal Disease: An Opinion Article. Front. Pharmacol. 2021, 12, 692429. [Google Scholar] [CrossRef] [PubMed]
- Bagnasco, S.M.; Mohammed, B.S.; Mani, H.; Gandolfo, M.T.; Haas, M.; Racusen, L.C.; Montgomery, R.A.; Kraus, E. Oxalate deposits in biopsies from native and transplanted kidneys, and impact on graft function. Nephrol. Dial. Transplant. 2008, 24, 1319–1325. [Google Scholar] [CrossRef]
- Becker, G.J.; Hewitson, T.D. Animal models of chronic kidney disease: Useful but not perfect. Nephrol. Dial. Transplant. 2013, 28, 2432–2438. [Google Scholar] [CrossRef] [Green Version]
- Mulay, S.R.; Eberhard, J.N.; Pfann, V.; Marschner, J.A.; Darisipudi, M.N.; Daniel, C.; Romoli, S.; Desai, J.; Grigorescu, M.; Kumar, S.V.; et al. Oxalate-induced chronic kidney disease with its uremic and cardiovascular complications in C57BL/6 mice. Am. J. Physiol. Physiol. 2016, 310, F785–F795. [Google Scholar] [CrossRef] [Green Version]
- Efe, O.; Verma, A.; Waikar, S.S. Urinary oxalate as a potential mediator of kidney disease in diabetes mellitus and obesity. Curr. Opin. Nephrol. Hypertens. 2019, 28, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Lamarche, J.; Nair, R.; Peguero, A.; Courville, C. Vitamin C-Induced Oxalate Nephropathy. Int. J. Nephrol. 2011, 2011, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geraghty, R.; Wood, K.; Sayer, J.A. Calcium oxalate crystal deposition in the kidney: Identification, causes and consequences. Urolithiasis 2020, 48, 377–384. [Google Scholar] [CrossRef]
- Knauf, F.; Asplin, J.R.; Granja, I.; Schmidt, I.M.; Moeckel, G.; David, R.J.; Flavell, R.A.; Aronson, P.S. NALP3-mediated inflammation is a principal cause of progressive renal failure in oxalate nephropathy. Kidney Int. 2013, 84, 895–901. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.-L.; Teng, T.-Y.; Liao, M.-T.; Ma, M.-C. TRPV1 Hyperfunction Contributes to Renal Inflammation in Oxalate Nephropathy. Int. J. Mol. Sci. 2021, 22, 6204. [Google Scholar] [CrossRef] [PubMed]
- Knoll, T.; Steidler, A.; Trojan, L.; Sagi, S.; Schaaf, A.; Yard, B.; Michel, M.S.; Alken, P. The influence of oxalate on renal epithelial and interstitial cells. Urol. Res. 2004, 32, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Thamilselvan, V.; Menon, M.; Thamilselvan, S. Oxalate at physiological urine concentrations induces oxidative injury in renal epithelial cells: Effect of α-tocopherol and ascorbic acid. BJU Int. 2014, 114, 140–150. [Google Scholar] [CrossRef]
- Mulay, S.R.; Honarpisheh, M.M.; Foresto-Neto, O.; Shi, C.; Desai, J.; Zhao, Z.B.; Marschner, J.A.; Popper, B.; Buhl, E.M.; Boor, P.; et al. Mitochondria Permeability Transition versus Necroptosis in Oxalate-Induced AKI. J. Am. Soc. Nephrol. 2019, 30, 1857–1869. [Google Scholar] [CrossRef]
- Diwan, V.; Small, D.; Kauter, K.; Gobe, G.C.; Brown, L. Gender differences in adenine-induced chronic kidney disease and cardiovascular complications in rats. Am. J. Physiol. Physiol. 2014, 307, F1169–F1178. [Google Scholar] [CrossRef]
- Ma, H.-Y.; Chen, S.; Du, Y. Estrogen and estrogen receptors in kidney diseases. Ren. Fail. 2021, 43, 619–642. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, D.S.; Sigel, L.K.F.; Azurmendi, P.J.; Vlachovsky, S.G.; Oddo, E.M.; Armando, I.; Ibarra, F.R.; Silberstein, C. Estradiol stimulates cell proliferation via classic estrogen receptor-alpha and G protein-coupled estrogen receptor-1 in human renal tubular epithelial cell primary cultures. Biochem. Biophys. Res. Commun. 2019, 512, 170–175. [Google Scholar] [CrossRef]
- De Araújo, L.; Costa-Pessoa, J.M.; De Ponte, M.C.; Oliveira-Souza, M. Sodium Oxalate-Induced Acute Kidney Injury Associated With Glomerular and Tubulointerstitial Damage in Rats. Front. Physiol. 2020, 11, 1076. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Benjamin, E.J. Diastolic Heart Failure—No Time to Relax. N. Engl. J. Med. 2001, 344, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Sas, D.J.; Enders, F.T.; Gunderson, T.M.; Mehta, R.A.; Olson, J.B.; Seide, B.M.; Banks, C.J.; Dehmel, B.; Pellikka, P.A.; Lieske, J.C.; et al. Natural History of Clinical, Laboratory, and Echocardiographic Parameters of a Primary Hyperoxaluria Cohort on Long Term Hemodialysis. Front. Med. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Si, Y.; Cheng, J.; Ding, J.; Zhao, H.; Liu, W.; Lin, Q.; Hou, J.; Guo, Z. Metabolic and Network Pharmacological Analyses of the Therapeutic Effect of Grona styracifolia on Calcium Oxalate-Induced Renal Injury. Front. Pharmacol. 2021, 12, 652989. [Google Scholar] [CrossRef]
- Hatch, M.; Cornelius, J.; Allison, M.; Sidhu, H.; Peck, A.; Freel, R. Oxalobacter sp. reduces urinary oxalate excretion by promoting enteric oxalate secretion. Kidney Int. 2006, 69, 691–698. [Google Scholar] [CrossRef] [Green Version]
- Nazzal, L.; Ho, M.; Wu, M.; Charytan, D. Oxalate Nephropathy in an Oxalobacter formigenes–Negative Subject. Kidney Int. Rep. 2020, 5, 754–757. [Google Scholar] [CrossRef]
- Marschner, J.A.; Mulay, S.R.; Steiger, S.; Anguiano, L.; Zhao, Z.; Boor, P.; Rahimi, K.; Inforzato, A.; Garlanda, C.; Mantovani, A.; et al. The Long Pentraxin PTX3 Is an Endogenous Inhibitor of Hyperoxaluria-Related Nephrocalcinosis and Chronic Kidney Disease. Front. Immunol. 2018, 9, 2173. [Google Scholar] [CrossRef]
- Mulay, S.R.; Eberhard, J.N.; Desai, J.; Marschner, J.A.; Kumar, S.V.; Weidenbusch, M.; Grigorescu, M.; Lech, M.; Eltrich, N.; Müller, L.; et al. Hyperoxaluria Requires TNF Receptors to Initiate Crystal Adhesion and Kidney Stone Disease. J. Am. Soc. Nephrol. 2016, 28, 761–768. [Google Scholar] [CrossRef] [Green Version]
- Ermer, T.; Eckardt, K.-U.; Aronson, P.S.; Knauf, F. Oxalate, inflammasome, and progression of kidney disease. Curr. Opin. Nephrol. Hypertens. 2016, 25, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, Y.; Guan, X.; Kang, J.; Wang, X.; Liu, Q.; Li, D.; Xu, H.; Tao, Z.; Deng, Y. Atorvastatin inhibits renal inflammatory response induced by calcium oxalate crystals via inhibiting the activation of TLR4/NF-κB and NLRP3 inflammasome. IUBMB Life 2020, 72, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, B.P.; Crajoinas, R.O.; Couto, G.K.; Davel, A.P.C.; Lessa, L.M.; Rossoni, L.V.; Girardi, A.C. Dipeptidyl peptidase IV inhibition attenuates blood pressure rising in young spontaneously hypertensive rats. J. Hypertens. 2011, 29, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unit | Control (n = 6) | Oxalate (n = 18) | p Value | |
|---|---|---|---|---|
| Oxygen Status | ||||
| Oxygen partial pressure (pO2) | mmHg | 56.82 ± 4.41 | 58.44 ± 2.12 | 0.717 |
| Carbon dioxide partial pressure (pCO2) | mmHg | 39.60 ± 1.01 | 34.29 ± 1.51 | 0.062 |
| Oxygen tension at half saturationof blood (p50) | mmHg | 33.43 ± 1.79 | 31.21 ± 0.94 | 0.260 |
| Oxygen saturation (sO2) | % | 79.53 ± 4.06 | 84.49 ± 1.41 | 0.152 |
| Hematocrit | % | 47.60 ± 1.30 | 43.07 ± 0.77 | 0.006 ** |
| Hemoglobin | g/dL | 15.53 ± 0.34 | 14.03 ± 0.26 | 0.006 ** |
| Fraction of oxyhemoglobin (FO2Hb) | % | 78.88 ± 3.90 | 83.26 ± 1.31 | 0.178 |
| Fraction of deoxyhemoglobin (FHHb) | % | 20.33 ± 4.05 | 15.38 ± 1.40 | 0.150 |
| Oxygen content (ctO2) | Vol% | 17.22 ± 0.98 | 16.58 ± 0.46 | 0.516 |
| Electrolytes concentration | ||||
| Sodium (Na+) | mmol/L | 137.80 ± 1.81 | 139.60 ± 1.32 | 0.502 |
| Potassium (K+) | mmol/L | 4.05 ± 0.19 | 3.80 ± 0.06 | 0.109 |
| Ionized calcium (Ca2+) | mmol/L | 1.16 ± 0.05 | 1.08 ± 0.03 | 0.194 |
| Chloride (Cl‒) | mmol/L | 119.80 ± 3.89 | 124.90 ± 3.70 | 0.343 |
| Metabolite concentrations | ||||
| Glutamate | mmol/L | 11.77 ± 1.09 | 9.92 ± 0.28 | 0.027 * |
| Lactate | mmol/L | 2.18 ± 0.33 | 2.56 ± 0.18 | 0.330 |
| Glucose | mg/dL | 106.69 ± 39.79 | 105.34 ± 45.10 | 0.969 |
| Acid/base status | ||||
| Standard base excess (cBase(Ecf)) | mmol/L | −9.32 ± 1.04 | −9.58 ± 0.72 | 0.852 |
| Standard bicarbonate (cHCO3‒(p,st)) | mmol/L | 16.40 ± 0.829 | 16.70 ± 0.460 | 0.7498 |
| Blood pH | 7.245 ± 0.023 | 7.287 ± 0.009 | 0.0520. |
| Unit | Control (n = 5) | Oxalate (n = 27) | p Value | |
|---|---|---|---|---|
| Heart Rate | BPM | 366.20 ± 7.55 | 359.0 ± 7.746 | 0.7012 |
| Left Ventricle Diameter (d) | mm/g | 0.023 ± 0.0008 | 0.024 ± 0.0005 | 0.582 |
| Left Ventricle Diameter (s) | mm/g | 0.0127 ± 0.0008 | 0.014 ± 0.0006 | 0.345 |
| Interventricular septum tickness (d) | mm/g | 0.0042 ± 0.0003 | 0.005 ± 0.0001 | 0.032 |
| Interventricular septum tickness (s) | mm/g | 0.00797 ± 0.0008 | 0.0083 ± 0.0002 | 0.630 |
| LV Mass | mg/g | 2.22 ± 0.16 | 2.70 ± 0.102 | 0.0601 |
| Volume (s) | µl | 117.00 ± 7.84 | 133.8 ± 12.40 | 0.5643 |
| Volume (d) | µl | 389.4 ± 34.59 | 449.7 ± 20.05 | 0.2231 |
| Ejection fraction | % | 68.99 ± 3.592 | 70.43 ± 2.136 | 0.7810 |
| Fractional shortening | % | 19.25 ± 1.956 | 21.66 ± 0.924 | 0.2932 |
| Stroke Volume | µl | 272.4 ± 34.24 | 313.9 ± 15.66 | 0.2937 |
| E-wave Velocity | mm/s | 991.3 ± 53.99 | 1030 ± 26.20 | 0.5558 |
| A-wave Velocity | mm/s | 516.0 ± 42.95 | 547.5 ± 23.94 | 0.5966 |
| Isovolumetric relaxation time | ms | 23.11 ± 1.174 | 23.08 ± 0.605 | 0.9845 |
| Deceleration Time | ms | 28.22 ± 4.247 | 28.44 ± 1.544 | 0.9572 |
| E’-wave Velocity | mm/s * BPM−1 | 0.18 ± 0.067 | 0.13 ± 0.010 | 0.0421 * |
| A’-wave Velocity | mm/s * BPM−1 | 0.13 ± 0.023 | 0.15 ± 0.009 | 0.5861 |
| A’/E’ ratio | NA | 0.88 ± 0.292 | 1.40 ± 0.148 | 0.1702 |
| E’/A’ ratio | NA | 1.60 ± 0.393 | 0.99 ± 0.111 | 0.0556 |
| E/A ratio | NA | 1.98 ± 0.208 | 0.19 ± 0.095 | 0.8772 |
| E/E’ ratio | NA | 16.29 ± 3.352 | 26.04 ± 1.851 | 0.0366 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crestani, T.; Crajoinas, R.O.; Jensen, L.; Dima, L.L.; Burdeyron, P.; Hauet, T.; Giraud, S.; Steichen, C. A Sodium Oxalate-Rich Diet Induces Chronic Kidney Disease and Cardiac Dysfunction in Rats. Int. J. Mol. Sci. 2021, 22, 9244. https://doi.org/10.3390/ijms22179244
Crestani T, Crajoinas RO, Jensen L, Dima LL, Burdeyron P, Hauet T, Giraud S, Steichen C. A Sodium Oxalate-Rich Diet Induces Chronic Kidney Disease and Cardiac Dysfunction in Rats. International Journal of Molecular Sciences. 2021; 22(17):9244. https://doi.org/10.3390/ijms22179244
Chicago/Turabian StyleCrestani, Thayane, Renato O. Crajoinas, Leonardo Jensen, Leno L. Dima, Perrine Burdeyron, Thierry Hauet, Sebastien Giraud, and Clara Steichen. 2021. "A Sodium Oxalate-Rich Diet Induces Chronic Kidney Disease and Cardiac Dysfunction in Rats" International Journal of Molecular Sciences 22, no. 17: 9244. https://doi.org/10.3390/ijms22179244
APA StyleCrestani, T., Crajoinas, R. O., Jensen, L., Dima, L. L., Burdeyron, P., Hauet, T., Giraud, S., & Steichen, C. (2021). A Sodium Oxalate-Rich Diet Induces Chronic Kidney Disease and Cardiac Dysfunction in Rats. International Journal of Molecular Sciences, 22(17), 9244. https://doi.org/10.3390/ijms22179244