
The Functional Diversity of Nitric Oxide Synthase Isoforms in Human Nose and Paranasal Sinuses: Contrasting Pathophysiological Aspects in Nasal Allergy and Chronic Rhinosinusitis

 , ,
, , 
Abstract
1. Background
2. NOS Activities in the Human Nose and Paranasal Sinuses
2.1. NOS Expression and NO Homeostasis in Human Paranasal Sinuses
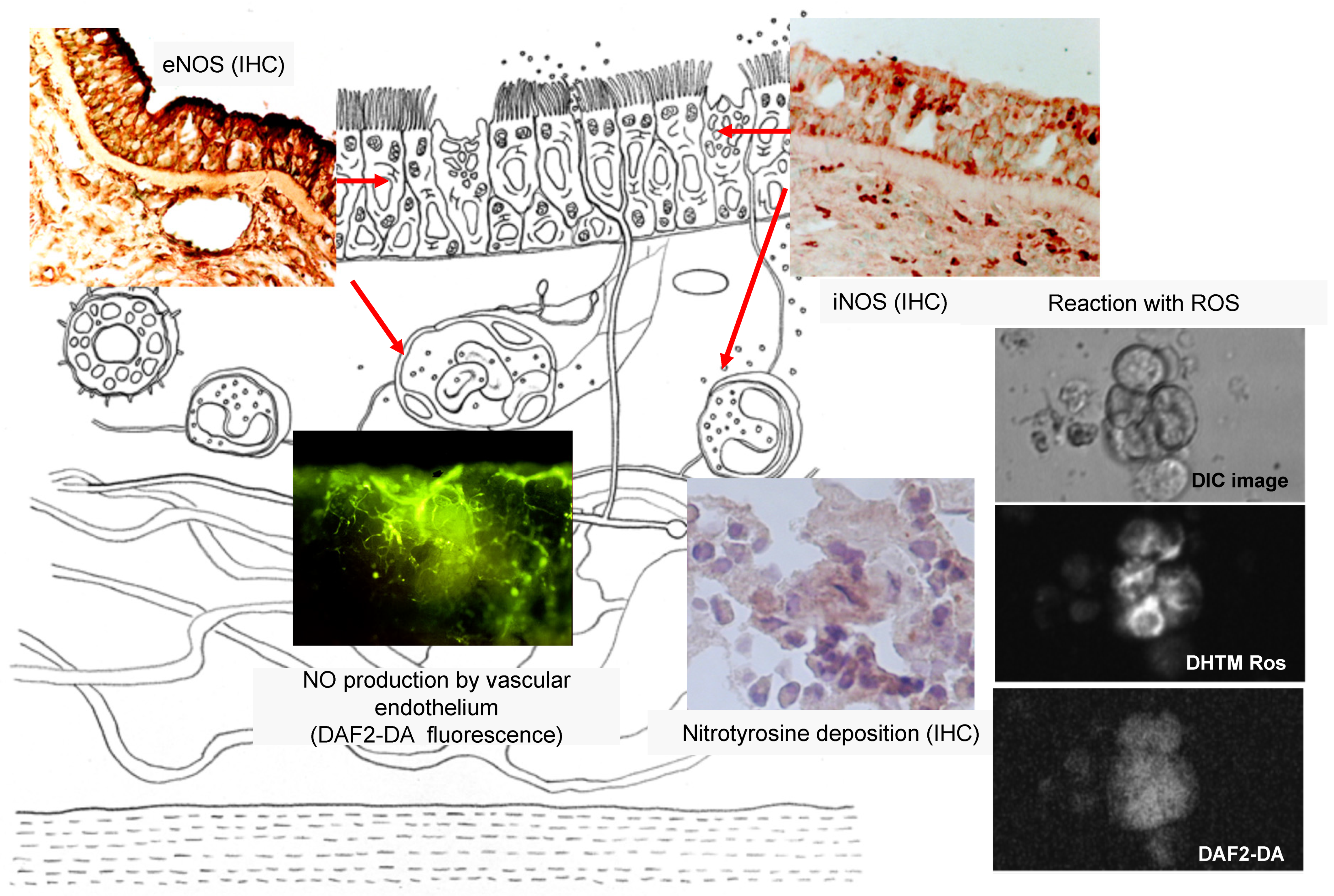
2.2. NOS Expression as an Inflammatory Mediator
3. Monitoring of NO in the Human Sinonasal Pathways
3.1. Paranasal Sinuses as a Physiological NO Reservoir
3.2. Nasal NO Measurement
4. Allergic Rhinitis
4.1. Anatomy and Embryology of the Nose and Paranasal Sinuses
4.2. Increased iNOS Activities in AR

{kind=link}
{kind=link}
| Authors, Year [Ref. No.] | Disease (Sample Area) | Principal Results |
|---|---|---|
| Kawamoto et al. 1998 [66] | Perennial AR (IT) | eNOS localization in epithelial and endothelial cells. Increased iNOS staining of epithelial and inflammatory cells in AR patients’ in inferior turbinates. |
| Kawamoto et al. 1999 [67] | HD mite AR (IT) | iNOS expression of nasal epithelial cells was elevated in the AR group. No difference in iNOS expression after antigen provocation |
| Takeno et al. 2001 [68] | Perennial AR (IT) | DAF-2 DA imaging showed that epithelial ciliated cells produced a larger amount of NO than nonepithelial inflammatory cells. Preincubation with L-NAME resulted in a 40% decrease in NO production. |
| Yusel et al. 2008 [73] | Seasonal AR (IT) | iNOS immunoreactivity was higher both in seasonal AR patients and in BA patients. No difference in eNOS immunoreactivity was observed between the groups. |
| Takeno et al. 2012 [74] | Perennial and seasonal AR, vasomotor rhinitis (IT) | Nasal FeNO levels were higher in perennial AR than in normal subjects or VMR patients, and positive correlations existed between nasal symptom scores and FeNO levels. SAR patients showed increased nasal FeNO levels during the pollen dispersion season. |
| Takeno et al. 2014 [61] | Perennial AR (IT, MM) | AR patients showed higher nasal FeNO and nasal NO levels in the IT area. No significant difference in the MM area was observed among the groups. AR patients showed higher ECP and NT levels in nasal brushing cells. |
| Takeno et al. 2017 [78] | Perennial AR (IT) | AR patients showed higher nasal FeNO levels. The optimal cut-off point of the nasal FeNO level was 38.5 ppb for AR diagnosis. No significant correlation was found between nasal FeNO and NAR values. |
| Hou et al. 2018 [79] | Pollen symptomatic AR (IT) | Increased nasal NO levels were associated with nasal obstruction and NAR. Nasal NO and ECP in secretion were positively correlated in patients with mild-to-moderate nasal obstruction. |
| Takahara et al. 2019 [65] | Perennial AR (IT, MM) | Nasal NO levels in the IT area in AR patients decreased 2 months after INS treatment. No difference in nasal NO levels in the MM area was observed. |
4.3. Nasal NO as a Therapeutic Parameter
5. Chronic Rhinosinusitis
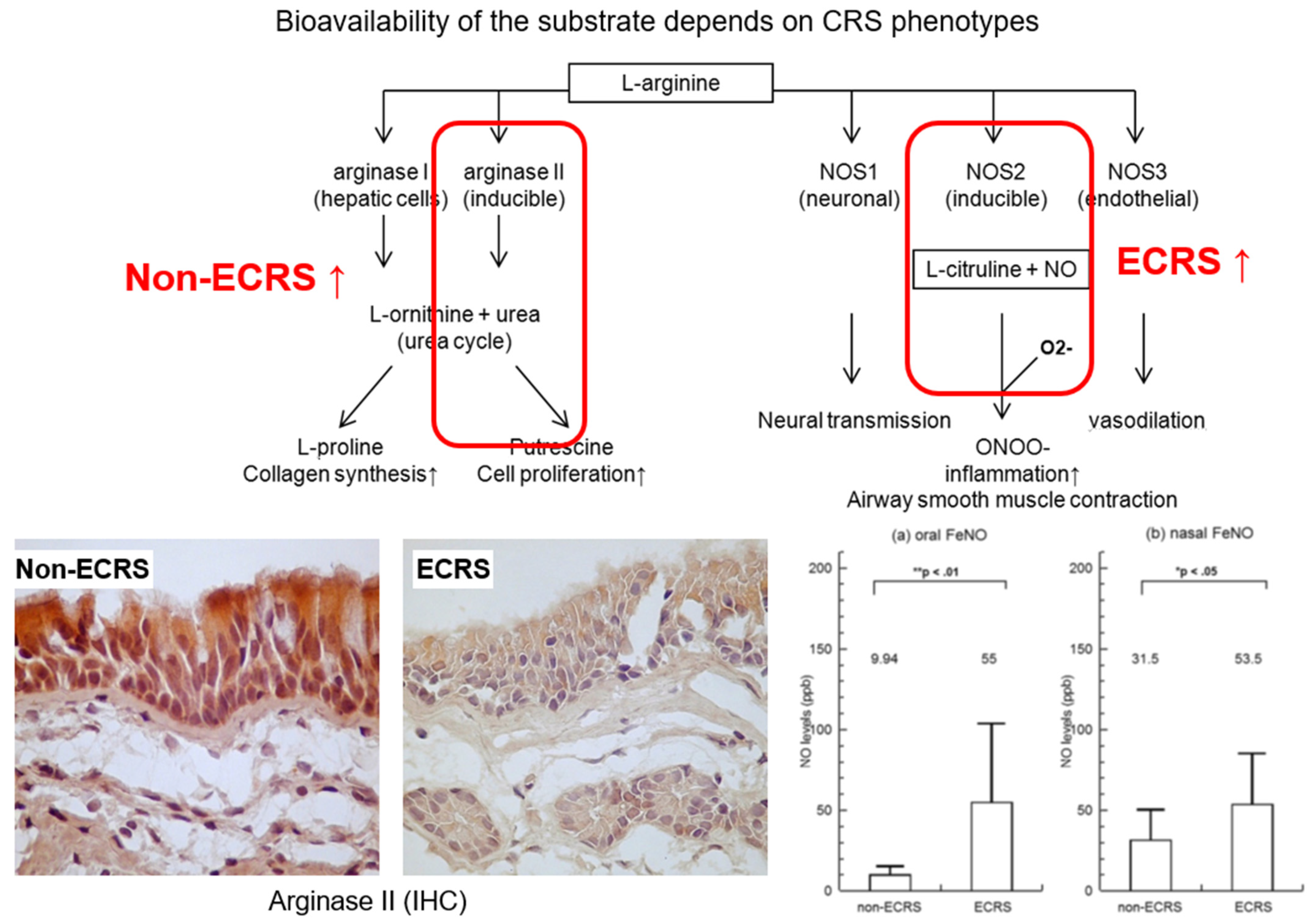
5.1. CRS Phenotypes and NO Production
5.2. NOS Activities in Eosinophilic Chronic Rhinosinusitis
5.3. NOS-Arginase Isoform Balance in CRS
| Authors, Year [Ref. No.] | Disease (Sample Area) | Principal Results |
|---|---|---|
| Chen et al. 2000 [28] | CRS (cultured ethmoid cells) | iNOS expression was augmented by TNF-α and attenuated by dexamethasone, whereas eNOS expression remained unchanged. TNF-α modulated CBF activities through NO production. |
| Kim et al. 2001 [29] | Normal mucosa (sphenoid sinus) | CBF increased after treatment with L-arginine and was inhibited by L-NAME. Both positive iNOS and eNOS immunostaining were observed in the ciliated cells. |
| Noda et al. 2012 [109] | ECRS (ethmoid mucosa, NP) | The surgical group showed higher nasal FeNO and lower oral FeNO levels 6 months after ESS, whereas the medical group remained unchanged. Up-regulation and positive immunoreactivity of iNOS was observed in both epithelial cells and submucosal inflammatory cells. |
| Takeno et al. 2013 [110] | ECRS and non-ECRS (ethmoid mucosa, NP) | ECRS patients showed higher oral FeNO levels and non-ECRS patients showed lower nasal FeNO levels. Positive correlations existed between blood eosinophils and FeNO levels in ECRS patients. Intense NT immunoreactivity was colocalized with eosinophil accumulation and higher NT-positive cells in ECRS patients. |
| Taruya et al. 2015 [140] | CRSsNP and CRSwNP (ethmoid mucosa, NP) | CRSsNP patients showed increased arginase-2 activities associated with lower nasal FeNO levels. CRSwNP patients showed iNOS upregulation with concomitant higher FeNO levels. |
| Kubota et al. 2017 [111] | ECRS and non-ECRS (frontal recess mucosa) | ECRS patients showed increased IL-5 and IL-6 mRNA levels in the frontal recess. No difference was observed in TGF-2 and iNOS levels. |
| Yoshida et al. 2019 [112] | ECRS and non-ECRS (NP) | Nasal NO levels were decreased in ECRS patients and negatively correlated with eosinophil levels and CT scores Nasal NO levels remained unchanged after ESS. Reduction in t-PA levels by Th2 cytokines may inhibit iNOS expression. |
| Vlad et al. 2019 [141] | CRS with BA or AR (Eth) | Arginase 2 expression was higher in CRS patients than controls, especially in nonallergic and nonasthmatic CRSsNP patients. No correlation existed between arginase 2 and IL-13 expression. |
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Thoracic Society; European Respiratory Society. ATS/ERS Recommendations for Standardized Procedures for the Online and Offline Measurement of Exhaled Lower Respiratory Nitric Oxide and Nasal Nitric Oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.-C.; Plummer, A.L.; Taylor, D.R. An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Zhao, Y.; Xu, A.; Leung, S.W. Thirty Years of Saying NO: Sources, Fate, Actions, and Misfortunes of the Endothelium-Derived Vasodilator Mediator. Circ. Res. 2016, 119, 375–396. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.-Y.; Hong, F.-F.; Yang, S.-L. The Roles of Nitric Oxide Synthase/Nitric Oxide Pathway in the Pathology of Vascular Dementia and Related Therapeutic Approaches. Int. J. Mol. Sci. 2021, 22, 4540. [Google Scholar] [CrossRef]
- Maniscalco, M.; Sofia, M.; Pelaia, G. Nitric Oxide in Upper Airways Inflammatory Diseases. Inflamm. Res. 2007, 56, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Dweik, R.A.; Gelb, A.F.; Gibson, P.; George, S.C.; Grasemann, H.; Pavord, I.D.; Ratjen, F.; Silkoff, P.; Taylor, D.R.; et al. Exhaled Nitric Oxide in Pulmonary Diseases: A Comprehensive Review. Chest 2010, 138, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, K.; Altmann, H.M.; Straub, A.C.; Isenberg, J.S. Nitric Oxide: What’s New to NO. Am. J. Physiol. Cell Physiol. 2017, 312, C254–C262. [Google Scholar] [CrossRef]
- Maniscalco, M.; Bianco, A.; Mazzarella, G.; Motta, A. Recent Advances on Nitric Oxide in the Upper Airways. Curr. Med. Chem. 2016, 23, 2736–2745. [Google Scholar] [CrossRef]
- Antosova, M.; Mokra, D.; Pepucha, L.; Plevkova, J.; Buday, T.; Sterusky, M.; Bencova, A. Physiology of Nitric Oxide in the Respiratory System. Physiol. Res. 2017, 66, S159–S172. [Google Scholar] [CrossRef]
- Alderton, W.K.; Cooper, C.E.; Knowles, R.G. Nitric Oxide Synthases: Structure, Function and Inhibition. Biochem. J. 2001, 357, 593–615. [Google Scholar] [CrossRef]
- Förstermann, U.; Sessa, W.C. Nitric Oxide Synthases: Regulation and Function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef]
- Lind, M.; Hayes, A.; Caprnda, M.; Petrovic, D.; Rodrigo, L.; Kruzliak, P.; Zulli, A. Inducible Nitric Oxide Synthase: Good or Bad? Biomed. Pharmacother. 2017, 93, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Picón-Pagès, P.; Garcia-Buendia, J.; Muñoz, F.J. Functions and Dysfunctions of Nitric Oxide in Brain. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1949–1967. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Song, W.; Li, L.; Fan, X. Endothelial Nitric Oxide Synthase: A Potential Therapeutic Target for Cerebrovascular Diseases. Mol. Brain 2016, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Kleniewska, P.; Gorąca, A. Influence of Endothelin 1 Receptor Blockers and a Nitric Oxide Synthase Inhibitor on Reactive Oxygen Species Formation in Rat Lungs. Physiol. Res. 2016, 65, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Lakshminrusimha, S.; Konduri, G.G.; Steinhorn, R.H. Considerations in the Management of Hypoxemic Respiratory Failure and Persistent Pulmonary Hypertension in Term and Late Preterm Neonates. J. Perinatol. 2016, 36, S12–S19. [Google Scholar] [CrossRef]
- McLaughlin, V.V.; Archer, S.L.; Badesch, D.B.; Barst, R.J.; Farber, H.; Lindner, J.R.; Mathier, M.A.; McGoon, M.D.; Park, M.H.; Rosenson, R.S.; et al. ACCF/AHA 2009 Expert Consensus Document on Pulmonary Hypertension: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association Developed in Collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J. Am. Coll. Cardiol. 2009, 53, 1573–1619. [Google Scholar] [CrossRef]
- Osada, R.; Takeno, S.; Hirakawa, K.; Ueda, T.; Furukido, K.; Yajin, K. Expression and Localization of Nuclear Factor-Kappa B Subunits in Cultured Human Paranasal Sinus Mucosal Cells. Rhinol. J. 2003, 41, 80–86. [Google Scholar]
- Nishi, Y.; Takeno, S.; Ishino, T.; Hirakawa, K. Glucocorticoids Suppress NF-kB Activation Induced by LPS and PGN in Paranasal Sinus Epithelial Cells. Rhinology 2009, 47, 413–418. [Google Scholar] [CrossRef]
- Ueda, T.; Takumida, M.; Takeno, S.; Tashiro, T.; Kawamoto, H.; Yajin, K. Functional Role of Nitric Oxide in the Nasal Mucosa of the Guinea Pig After Instillation with Lipopolysaccharide. Acta Otolaryngol. 2001, 121, 510–516. [Google Scholar] [CrossRef]
- Takeno, S.; Hirakawa, K.; Ueda, T.; Furukido, K.; Osada, R.; Yajin, K. Nuclear Factor-Kappa B Activation in the Nasal Polyp Epithelium: Relationship to Local Cytokine Gene Expression. Laryngoscope 2002, 112, 53–58. [Google Scholar] [CrossRef]
- Ala, M.; Ghasemi, M.; Mohammad Jafari, R.; Dehpour, A.R. Beyond its Anti-Migraine Properties, Sumatriptan is an Anti-Inflammatory Agent: A Systematic Review. Drug Dev. Res. 2021. [Google Scholar] [CrossRef]
- Pavord, I.D.; Afzalnia, S.; Menzies-Gow, A.; Heaney, L.G. The Current and Future Role of Biomarkers in Type 2 Cytokine-Mediated Asthma Management. Clin. Exp. Allergy 2017, 47, 148–160. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and Safety of Dupilumab in Patients with Severe Chronic Rhinosinusitis with Nasal Polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from Two Multicentre, Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Phase 3 Trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- Matsunaga, K.; Katoh, N.; Fujieda, S.; Izuhara, K.; Oishi, K. Dupilumab: Basic Aspects and Applications to Allergic Diseases. Allergol. Int. 2020, 69, 187–196. [Google Scholar] [CrossRef]
- Kopincová, J.; Calkovska, A. Meconium-Induced Inflammation and Surfactant Inactivation: Specifics of Molecular Mechanisms. Pediatr. Res. 2015, 79, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Heffler, E.; Carpagnano, G.E.; Favero, E.; Guida, G.; Maniscalco, M.; Motta, A.; Paoletti, G.; Rolla, G.; Baraldi, E.; Pezzella, V.; et al. Fractional Exhaled Nitric Oxide (FENO) in the Management of Asthma: A Position Paper of the Italian Respiratory Society (SIP/IRS) and Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC). Multidiscip. Respir. Med. 2020, 15, 36. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Takeno, S.; Osada, R.; Ueda, T.; Yajin, K. Modulation of Ciliary Activity by Tumor Necrosis Factor-Alpha in Cultured Sinus Epithelial Cells. Possible Roles of Nitric Oxide. Hiroshima J. Med Sci. 2000, 49, 49–55. [Google Scholar]
- Kim, J.-W.; Min, Y.-G.; Rhee, C.-S.; Lee, C.-H.; Koh, Y.Y.; Rhyoo, C.; Kwon, T.-Y.; Park, S.-W. Regulation of Mucociliary Motility by Nitric Oxide and Expression of Nitric Oxide Synthase in the Human Sinus Epithelial Cells. Laryngoscope 2001, 111, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.L.; Hernandez, M.; Jaspers, I.; Mills, K.; Brighton, L.; Zhou, H.; Zhang, J.; Hazucha, M.J. Interleukin-13 Stimulates Production of Nitric Oxide in Cultured Human Nasal Epithelium. Vitr. Cell Dev. Biol. Anim. 2018, 54, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Mahdavinia, M.; Keshavarzian, A.; Tobin, M.C.; Landay, A.L.; Schleimer, R.P. A Comprehensive Review of the Nasal Microbiome in Chronic Rhinosinusitis (CRS). Clin. Exp. Allergy 2016, 46, 21–41. [Google Scholar] [CrossRef]
- Miraglia, D.; Giudice, M.; Parisi, G.F.; Indolfi, C.; Manti, S.; Leonardi, S.; Decimo, F.; Ciprandi, G. Nasal Microbiome in Chronic Rhinosinusitis. Minerva Pediatr. 2020. [Google Scholar] [CrossRef]
- Carey, R.M.; Chen, B.; Adappa, N.D.; Palmer, J.N.; Kennedy, D.W.; Lee, R.J.; Cohen, N.A. Human Upper Airway Epithelium Produces Nitric Oxide in Response to Staphylococcus epidermidis. Int. Forum Allergy Rhinol. 2016, 6, 1238–1244. [Google Scholar] [CrossRef]
- Freund, J.; Mansfield, C.J.; Doghramji, L.J.; Adappa, N.D.; Palmer, J.N.; Kennedy, D.W.; Reed, D.R.; Jiang, P.; Lee, R.J. Activation of Airway Epithelial Bitter Taste Receptors by Pseudomonas aeruginosa Quinolones Modulates Calcium, Cyclic-AMP, and Nitric Oxide Signaling. J. Biol. Chem. 2018, 293, 9824–9840. [Google Scholar] [CrossRef]
- Antosova, M.; Bencova, A.; Mokra, D.; Plevkova, J.; Pepucha, L.; Buday, T. Exhaled and Nasal Nitric Oxide–Impact for Allergic Rhinitis. Physiol. Res. 2020, 69, S123–S130. [Google Scholar] [CrossRef] [PubMed]
- Ba, A.D.W.; Carey, R.M.; Kohanski, M.A.; Kennedy, D.W.; Palmer, J.N.; Adappa, N.D.; Cohen, N.A. Relative Susceptibility of Airway Organisms to Antimicrobial Effects of Nitric Oxide. Int. Forum Allergy Rhinol. 2017, 7, 770–776. [Google Scholar] [CrossRef]
- Lisi, F.; Zelikin, A.N.; Chandrawati, R. Nitric Oxide to Fight Viral Infections. Adv. Sci. 2021, 8, 2003895. [Google Scholar] [CrossRef]
- Sanders, S.P.; Proud, D.; Permutt, S.; Siekierski, E.S.; Yachechko, R.; Liu, M.C. Role of Nasal Nitric Oxide in the Resolution of Experimental Rhinovirus Infection. J. Allergy Clin. Immunol. 2004, 113, 697–702. [Google Scholar] [CrossRef]
- Klingström, J.; Akerström, S.; Hardestam, J.; Stoltz, M.; Simon, M.; Falk, K.I.; Mirazimi, A.; Rottenberg, M.; Lundkvist, A. Nitric Oxide and Peroxynitrite Have Different Antiviral Effects against Hantavirus Replication and Free Mature Virions. Eur. J. Immunol. 2006, 36, 2649–2657. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, L.M.; Rossini, C.V.; Lameu, C. Implications of SARS-Cov-2 Infection on eNOS and iNOS Activity: Consequences for the Respiratory and Vascular Systems. Nitric Oxide 2021, 111–112, 64–71. [Google Scholar] [CrossRef]
- Adappa, N.D.; Ba, D.F.; Palmer, J.N.; Kennedy, D.W.; Rn, L.D.; Bs, S.A.M.; Owens, D.; Bs, C.M.; Lysenko, A.; Lee, R.; et al. TAS2R38 Genotype Predicts Surgical Outcome in Nonpolypoid Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6, 25–33. [Google Scholar] [CrossRef]
- Lässer, C.; O’Neil, S.E.; Shelke, G.V.; Sihlbom, C.; Hansson, S.F.; Gho, Y.S.; Lundbäck, B.; Lötvall, J. Exosomes in the Nose Induce Immune Cell Trafficking and Harbour an Altered Protein Cargo in Chronic Airway Inflammation. J. Transl. Med. 2016, 14, 181. [Google Scholar] [CrossRef] [PubMed]
- Nocera, A.L.; Mueller, S.; Stephan, J.R.; Hing, L.; Seifert, P.; Han, X.; Lin, D.T.; Amiji, M.M.; Libermann, T.; Bleier, B.S. Exosome Swarms Eliminate Airway Pathogens and Provide Passive Epithelial Immunoprotection Through Nitric Oxide. J. Allergy Clin. Immunol. 2019, 143, 1525–1535.e1. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free Radicals and Antioxidants in Normal Physiological Functions and Human Disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Zarkovic, N. Roles and Functions of ROS and RNS in Cellular Physiology and Pathology. Cells 2020, 9, 767. [Google Scholar] [CrossRef]
- Nesi, R.T.; Barroso, M.V.; Souza Muniz, V.; de Arantes, A.C.; Martins, M.A.; Brito Gitirana, L.; Neves, J.S.; Benjamim, C.F.; Lanzetti, M.; Valenca, S.S. Pharmacological Modulation of Reactive Oxygen Species (ROS) Improves the Airway Hyperresponsiveness by Shifting the Th1 Response in Allergic Inflammation Induced by Ovalbumin. Free Radic. Res. 2017, 51, 708–722. [Google Scholar] [CrossRef]
- Akdis, C.A.; Arkwright, P.D.; Brüggen, M.-C.; Busse, W.; Gadina, M.; Guttman-Yassky, E.; Kabashima, K.; Mitamura, Y.; Vian, L.; Wu, J.; et al. Type 2 Immunity in the Skin and Lungs. Allergy 2020, 75, 1582–1605. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.; Teixeira, L.; Moita, L. Disease Tolerance and Immunity in Host Protection against Infection. Nat. Rev. Immunol. 2017, 17, 83–96. [Google Scholar] [CrossRef]
- García-Ortiz, A.; Serrador, J.M. Nitric Oxide Signaling in T Cell-Mediated Immunity. Trends Mol. Med. 2018, 24, 412–427. [Google Scholar] [CrossRef]
- Monga, N.; Sethi, G.S.; Kondepudi, K.K.; Naura, A.S. Lipid Mediators and Asthma: Scope of Therapeutics. Biochem. Pharmacol. 2020, 179, 113925. [Google Scholar] [CrossRef]
- Huang, F.; Yin, J.-N.; Wang, H.-B.; Liu, S.-Y.; Li, Y.-N. Association of Imbalance of Effector T Cells and Regulatory Cells with the Severity of Asthma and Allergic Rhinitis in Children. Allergy Asthma Proc. 2017, 38, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.N.; Farkas-Szallasi, T.; Weitzberg, E.; Rinder, J.; Lidholm, J.; Änggåard, A.; Hökfelt, T.; Alving, K. High Nitric Oxide Production in Human Paranasal Sinuses. Nat. Med. 1995, 1, 370–373. [Google Scholar] [CrossRef]
- Weitzberg, E.; Lundberg, J.O. Humming Greatly Increases Nasal Nitric Oxide. Am. J. Respir. Crit. Care Med. 2002, 166, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Gungor, A.; Martino, B.; Dupont, S.; Kuo, L. A Human Study Model for Nitric Oxide Research in Sinonasal Disease. Am. J. Otolaryngol. 2013, 34, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.; Weitzberg, E.; Rinder, J.; Rudehill, A.; Jansson, O.; Wiklund, N.; Alving, K. Calcium-Independent and Steroid-Resistant Nitric Oxide Synthase Activity in Human Paranasal Sinus Mucosa. Eur. Respir. J. 1996, 9, 1344–1347. [Google Scholar] [CrossRef]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.-C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A.; et al. A European Respiratory Society Technical Standard: Exhaled Biomarkers in Lung Disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef]
- Jeppegaard, M.; Veidal, S.; Sverrild, A.; Backer, V.; Porsbjerg, C. Validation of ATS Clinical Practice Guideline Cut-Points for FeNO in Asthma. Respir. Med. 2018, 144, 22–29. [Google Scholar] [CrossRef]
- Wang, B.; Wu, Z.; Wang, F.; Yin, Z.; Shi, L.; Liu, Y. Nasal Nitric Oxide Testing for Allergic Rhinitis Patients: Systematic Review and Meta-Analysis. Immun. Inflamm. Dis. 2021. [Google Scholar] [CrossRef]
- Phillips, P.S.; Sacks, R.; Marcells, G.N.; Cohen, N.A.; Harvey, R.J. Nasal Nitric Oxide and Sinonasal Disease: A Systematic Review of Published Evidence. Otolaryngol. Head Neck Surg. 2011, 144, 159–169. [Google Scholar] [CrossRef]
- Ambrosino, P.; Parrella, P.; Formisano, R.; Papa, A.; Spedicato, G.A.; Di Minno, M.N.D.; Motta, A.; Maniscalco, M. Clinical Application of Nasal Nitric Oxide Measurement in Allergic Rhinitis: A Systematic Review and Meta-Analysis. Ann. Allergy Asthma Immunol. 2020, 125, 447–459.e5. [Google Scholar] [CrossRef] [PubMed]
- Takeno, S.; Yoshimura, H.; Kubota, K.; Taruya, T.; Ishino, T.; Hirakawa, K. Comparison of Nasal Nitric Oxide Levels between the Inferior Turbinate Surface and the Middle Meatus in Patients with Symptomatic Allergic Rhinitis. Allergol. Int. 2014, 63, 475–483. [Google Scholar] [CrossRef]
- Scadding, G. Nitric Oxide in the Airways. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 258–263. [Google Scholar] [CrossRef]
- Wake, M.; Takeno, S.; Hawke, M. The Early Development of Sino-Nasal Mucosa. Laryngoscope 1994, 104, 850–855. [Google Scholar] [CrossRef]
- Lundberg, J.O. Nitric Oxide and the Paranasal Sinuses. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2008, 291, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Takahara, D.; Kono, T.; Takeno, S.; Ishino, T.; Hamamoto, T.; Kubota, K.; Ueda, T. Nasal Nitric Oxide in the Inferior Turbinate Surface Decreases with Intranasal Steroids in Allergic Rhinitis: A Prospective Study. Auris Nasus Larynx 2019, 46, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, H.; Takumida, M.; Takeno, S.; Watanabe, H.; Fukushima, N.; Yajin, K. Localization of Nitric Oxide Synthase in Human Nasal Mucosa with Nasal Allergy. Acta Otolaryngol. Suppl. 1998, 539, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, H.; Takeno, S.; Yajin, K. Increased Expression of Inducible Nitric Oxide Synthase in Nasal Epithelial Cells in Patients with Allergic Rhinitis. Laryngoscope 1999, 109, 2015–2020. [Google Scholar] [CrossRef] [PubMed]
- Takeno, S.; Osada, R.; Furukido, K.; Chen, J.H.; Yajin, K. Increased Nitric Oxide Production in Nasal Epithelial Cells from Allergic Patients—RT-PCR Analysis and Direct Imaging by a Fluorescence Indicator: DAF-2 DA. Clin. Exp. Allergy 2001, 31, 881–888. [Google Scholar] [CrossRef] [PubMed]
- You, S.; Zhang, J.; Bai, Y.; Ji, L.; Wang, H. Normal Values of Nasal NO and Exhaled NO in Young Chinese People Aged 9–22 years. World J. Otorhinolaryngol. Head Neck Surg. 2016, 2, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Takabayashi, T.; Schleimer, R.P. Formation of Nasal Polyps: The Roles of Innate Type 2 Inflammation and Deposition of Fibrin. J. Allergy Clin. Immunol. 2020, 145, 740–750. [Google Scholar] [CrossRef]
- Okubo, K.; Kurono, Y.; Ichimura, K.; Enomoto, T.; Okamoto, Y.; Kawauchi, H.; Suzaki, H.; Fujieda, S.; Masuyama, K. Japanese Guidelines for Allergic Rhinitis 2017. Allergol. Int. 2017, 66, 205–219. [Google Scholar] [CrossRef]
- Struben, V.M.D.; Wieringa, M.H.; Feenstra, L.; De Jongste, J.C. Nasal Nitric Oxide and Nasal Allergy. Allergy 2006, 61, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, H.; Kirmaz, C.; Yilmaz, O.; Pinar, E.; Vatansever, S.; Degirmenci, P.B.; Ozbilgin, K. Nasal Mucosal Expression of Nitric Oxide Synthases in Patients with Allergic Rhinitis and Its Relation to Asthma. Ann. Allergy Asthma Immunol. 2008, 100, 12–16. [Google Scholar] [CrossRef]
- Takeno, S.; Noda, N.; Hirakawa, K. Measurements of Nasal Fractional Exhaled Nitric Oxide with a Hand-Held Device in Patients with Allergic Rhinitis: Relation to Cedar Pollen Dispersion and Laser Surgery. Allergol. Int. 2012, 61, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Radi, R. Oxygen Radicals, Nitric Oxide, and Peroxynitrite: Redox Pathways in Molecular Medicine. Proc. Natl. Acad. Sci. USA 2018, 115, 5839–5848. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Tochino, Y.; Chibana, K.; Trudeau, J.B.; Holguin, F.; Wenzel, S.E. Nitric Oxide and Related Enzymes in Asthma: Relation to Severity, Enzyme Function and Inflammation. Clin. Exp. Allergy 2011, 42, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; DELLA Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative Stress, Aging, and Diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [PubMed]
- Takeno, S.; Okabayashi, Y.; Kohno, T.; Yumii, K.; Hirakawa, K. The Role of Nasal Fractional Exhaled Nitric Oxide as an Objective Parameter Independent of Nasal Airflow Resistance in the Diagnosis of Allergic Rhinitis. Auris Nasus Larynx 2017, 44, 435–441. [Google Scholar] [CrossRef]
- Hou, J.; Lou, H.; Wang, Y.; He, F.; Cao, F.; Wang, C.; Zhang, L. Nasal Ventilation is an Important Factor in Evaluating the Diagnostic Value of Nasal Nitric Oxide in Allergic Rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 686–694. [Google Scholar] [CrossRef]
- Asano, T.; Takemura, M.; Kanemitsu, Y.; Yokota, M.; Fukumitsu, K.; Takeda, N.; Ichikawa, H.; Hijikata, H.; Uemura, T.; Takakuwa, O.; et al. Combined Measurements of Fractional Exhaled Nitric Oxide and Nasal Nitric Oxide Levels for Assessing Upper Airway Diseases in Asthmatic Patients. J. Asthma 2018, 55, 300–309. [Google Scholar] [CrossRef]
- Brindisi, G.; De Vittori, V.; De Nola, R.; Di Mauro, A.; De Castro, G.; Baldassarre, M.E.; Cicinelli, E.; Cinicola, B.; Duse, M.; Zicari, A.M. The Role of Nasal Nitric Oxide and Anterior Active Rhinomanometry in the Diagnosis of Allergic Rhinitis and Asthma: A Message for Pediatric Clinical Practice. J. Asthma Allergy 2021, 14, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Moody, A.; Fergusson, W.; Wells, A.; Bartley, J.; Kolbe, J. Nasal Levels of Nitric Oxide as an Outcome Variable in Allergic Upper Respiratory Tract Disease: Influence of Atopy and Hayfever on nNO. Am. J. Rhinol. 2006, 20, 425–429. [Google Scholar] [CrossRef]
- Alexanderson, C.; Olin, A.-C.; Dahlman-Höglund, A.; Finizia, C.; Torén, K. Nasal Nitric Oxide in a Random Sample of Adults and Its Relationship to Sensitization, Cat Allergen, Rhinitis, and Ambient Nitric Oxide. Am. J. Rhinol. Allergy 2012, 26, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Zhang, W.; Zhang, Y.; Zhang, L. Nasal Nitric Oxide Is Correlated with Nasal Patency and Nasal Symptoms. Allergy Asthma Immunol. Res. 2019, 11, 367–380. [Google Scholar] [CrossRef] [PubMed]
- Canakcioglu, S.; Tahamiler, R.; Saritzali, G.; Isildak, H.; Alimoglu, Y. Nasal Patency by Rhinomanometry in Patients with Sensation of Nasal Obstruction. Am. J. Rhinol. Allergy 2009, 23, 300–302. [Google Scholar] [CrossRef]
- Jaradeh, S.S.; Smith, T.L.; Torrico, L.; Prieto, T.E.; Loehrl, T.A.; Darling, R.J.; Toohill, R.J. Autonomic Nervous System Evaluation of Patients with Vasomotor Rhinitis. Laryngoscope 2000, 110, 1828–1831. [Google Scholar] [CrossRef]
- Loehrl, T.A.; Smith, T.L.; Darling, R.J.; Torrico, L.; Prieto, T.E.; Shaker, R.; Toohill, R.J.; Jaradeh, S.S. Autonomic Dysfunction, Vasomotor Rhinitis, and Extraesophageal Manifestations of Gastroesophageal Reflux. Otolaryngol. Neck Surg. 2002, 126, 382–387. [Google Scholar] [CrossRef]
- Ruffoli, R.; Fattori, B.; Giambelluca, M.A.; Soldani, P.; Giannessi, F. Ultracytochemical Localization of the NADPH-d Activity in the Human Nasal Respiratory Mucosa in Vasomotor Rhinitis. Laryngoscope 2000, 110, 1361–1365. [Google Scholar] [CrossRef]
- Giannessi, F.; Fattori, B.; Ursino, F.; Giambelluca, M.A.; Soldani, P.; Scavuzzo, M.C.; Ruffoli, R. Ultrastructural and Ultracytochemical Study of the Human Nasal Respiratory Epithelium in Vasomotor Rhinitis. Acta. Otolaryngol. 2003, 123, 943–949. [Google Scholar] [CrossRef]
- Liu, C.; Zheng, K.; Liu, X.; Zheng, M.; Liu, Z.; Wang, X.; Zhang, L. Use of Nasal Nitric Oxide in the Diagnosis of Allergic Rhinitis and Nonallergic Rhinitis in Patients with and without Sinus Inflammation. J. Allergy Clin. Immunol. Pract. 2020, 8, 1574–1581.e4. [Google Scholar] [CrossRef]
- Barnes, M.L.; Menzies, D.; Fardon, T.C.; Burns, P.; Wilson, A.M.; Lipworth, B.J. Combined Mediator Blockade or Topical Steroid for Treating the Unified Allergic Airway. Allergy 2006, 62, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Krantz, C.; Janson, C.; Alving, K.; Malinovschi, A. Nasal Nitric Oxide in Relation to Asthma Characteristics in a Longitudinal Asthma Cohort Study. Nitric Oxide 2021, 106, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Krantz, C.; Janson, C.; Borres, M.P.; Nordvall, L.; Alving, K.; Malinovschi, A. Nasal Nitric Oxide is Associated with Exhaled NO, Bronchial Responsiveness and Poor Asthma Control. J. Breath Res. 2014, 8, 026002. [Google Scholar] [CrossRef] [PubMed]
- Kharitonov, S.A.; Rajakulasingam, K.; O’Connor, B.; Durham, S.R.; Barnes, P.J. Nasal Nitric Oxide is Increased in Patients with Asthma and Allergic Rhinitis and May Be Modulated by Nasal Glucocorticoids. J. Allergy Clin. Immunol. 1997, 99, 58–64. [Google Scholar] [CrossRef]
- Baraldi, E.; Azzolin, N.; Carra’, S.; Dario, C.; Marchesini, L.; Zacchello, F. Effect of Topical Steroids on Nasal Nitric OXIDE Production in Children with Perennial Allergic Rhinitis: A Pilot Study. Respir. Med. 1998, 92, 558–561. [Google Scholar] [CrossRef]
- Yamada, T.; Yamamoto, H.; Kubo, S.; Sakashita, M.; Tokunaga, T.; Susuki, D.; Narita, N.; Ogi, K.; Kanno, M.; Yamashita, S.; et al. Efficacy of Mometasone Furoate Nasal Spray for Nasal Symptoms, Quality of Life, Rhinitis-Disturbed Sleep, and Nasal Nitric Oxide in Patients with Perennial Allergic Rhinitis. Allergy Asthma Proc. 2012, 33, 9–16. [Google Scholar] [CrossRef]
- Boot, J.D.; De Kam, M.L.; Mascelli, M.A.; Miller, B.; Van Wijk, R.G.; De Groot, H.; Cohen, A.F.; Diamant, Z. Original Article: Nasal Nitric Oxide: Longitudinal Reproducibility and the Effects of a Nasal Allergen Challenge in Patients with Allergic Rhinitis. Allergy 2007, 62, 378–384. [Google Scholar] [CrossRef]
- Bautista, A.P.; Eisenlohr, C.P.; Lanz, M.J. Nasal Nitric Oxide and Nasal Eosinophils Decrease with Levocetirizine in Subjects with Perennial Allergic Rhinitis. Am. J. Rhinol. Allergy 2011, 25, 383–387. [Google Scholar] [CrossRef]
- Shusterman, D.J.; Weaver, E.M.; Goldberg, A.N.; Schick, S.F.; Wong, H.H.; Balmes, J.R. Pilot Evaluation of the Nasal Nitric Oxide Response to Humming as an Index of Osteomeatal Patency. Am. J. Rhinol. Allergy 2012, 26, 123–126. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis 2021. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.-O.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory Endotypes of Chronic Rhinosinusitis Based on Cluster Analysis of Biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456.e4. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of TH Cytokine Profiles in Patients with Chronic Rhinosinusitis: A Multicenter Study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef]
- Bachert, C.; Zhang, N.; Hellings, P.W.; Bousquet, J. Endotype-Driven Care Pathways in Patients with Chronic Rhinosinusitis. J. Allergy Clin. Immunol. 2018, 141, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Fujieda, S.; Imoto, Y.; Kato, Y.; Ninomiya, T.; Tokunaga, T.; Tsutsumiuchi, T.; Yoshida, K.; Kidoguchi, M.; Takabayashi, T. Eosinophilic Chronic Rhinosinusitis. Allergol. Int. 2019, 68, 403–412. [Google Scholar] [CrossRef]
- Khan, A.; Vandeplas, G.; Huynh, T.; Joish, V.; Mannent, L.; Tomassen, P.; Van Zele, T.; Cardell, L.; Arebro, J.; Olze, H.; et al. The Global Allergy and Asthma European Network (GALEN Rhinosinusitis Cohort: A Large European Cross-Sectional Study of Chronic Rhinosinusitis Patients with and without Nasal Polyps. Rhinol. J. 2019, 57, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Albu, S. Chronic Rhinosinusitis—An Update on Epidemiology, Pathogenesis and Management. J. Clin. Med. 2020, 18, 2285. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Marioni, G. Structured Histopathology for Endotyping and Planning Rational Treatment in Chronic Rhinosinusitis. Am. J. Otolaryngol. 2021, 42, 102795. [Google Scholar] [CrossRef]
- Noda, N.; Takeno, S.; Fukuiri, T.; Hirakawa, K. Monitoring of Oral and Nasal Exhaled Nitric Oxide in Eosinophilic Chronic Rhinosinusitis: A Prospective Study. Am. J. Rhinol. Allergy 2012, 26, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Takeno, S.; Taruya, T.; Ueda, T.; Noda, N.; Hirakawa, K. Increased Exhaled Nitric Oxide and Its Oxidation Metabolism in Eosinophilic Chronic Rhinosinusitis. Auris Nasus Larynx 2013, 40, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Takeno, S.; Taruya, T.; Sasaki, A.; Ishino, T.; Hirakawa, K. IL-5 and IL-6 are Increased in the Frontal Recess of Eosinophilic Chronic Rhinosinusitis Patients. J. Otolaryngol. Head Neck Surg. 2017, 46, 36. [Google Scholar] [CrossRef]
- Yoshida, K.; Takabayashi, T.; Imoto, Y.; Sakashita, M.; Narita, N.; Fujieda, S. Reduced Nasal Nitric Oxide Levels in Patients with Eosinophilic Chronic Rhinosinusitis. Allergol. Int. 2019, 68, 225–232. [Google Scholar] [CrossRef]
- Arnal, J.-F.; Flores, P.; Rami, J.; Murris-Espin, M.; Bremont, F.; Aguilla, M.P.I.; Serrano, E.; Didier, A. Nasal Nitric Oxide Concentration in Paranasal Sinus Inflammatory Diseases. Eur. Respir. J. 1999, 13, 307–312. [Google Scholar] [CrossRef]
- Ragab, S.; Lund, V.J.; Scadding, G. Evaluation of the Medical and Surgical Treatment of Chronic Rhinosinusitis: A Prospective, Randomised, Controlled Trial. Laryngoscope 2004, 114, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Ragab, S.; Lund, V.J.; Saleh, H.A.; Scadding, G. Nasal Nitric Oxide in Objective Evaluation of Chronic Rhinosinusitis Therapy. Allergy 2006, 61, 717–724. [Google Scholar] [CrossRef]
- Liu, C.; Zheng, M.; He, F.; Wang, X.; Zhang, L. Role of Exhaled Nasal Nitric Oxide in Distinguishing between Chronic Rhinosinusitis with and without Nasal Polyps. Am. J. Rhinol. Allergy 2017, 31, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Nishida, M.; Takeno, S.; Takemoto, K.; Takahara, D.; Hamamoto, T.; Ishino, T.; Kawasumi, T. Increased Tissue Expression of Lectin-Like Oxidized LDL Receptor-1 (LOX-1) Is Associated with Disease Severity in Chronic Rhinosinusitis with Nasal Polyps. Diagnostics 2020, 10, 246. [Google Scholar] [CrossRef]
- Ambrosino, P.; Molino, A.; Spedicato, G.A.; Parrella, P.; Formisano, R.; Motta, A.; Di Minno, M.N.D.; Maniscalco, M. Nasal Nitric Oxide in Chronic Rhinosinusitis with or without Nasal Polyps: A Systematic Review with Meta-Analysis. J. Clin. Med. 2020, 9, 200. [Google Scholar] [CrossRef] [PubMed]
- Ramadass, S.K.; Nazir, L.S.; Thangam, R.; Perumal, R.K.; Manjubala, I.; Madhan, B.; Seetharaman, S. Type I Collagen Peptides and Nitric Oxide Releasing Electrospun Silk Fibroin Scaffold: A Multifunctional Approach for the Treatment of Ischemic Chronic Wounds. Colloids Surf. B Biointerfaces 2019, 175, 636–643. [Google Scholar] [CrossRef]
- Póvoa, V.C.O.; Dos Santos, G.J.V.P.; Picheth, G.F.; Jara, C.P.; da Silva, L.C.E.; de Araújo, E.P.; de Oliveira, M.G. Wound Healing Action of Nitric Oxide-Releasing Self-Expandable Collagen Sponge. J. Tissue Eng. Regen. Med. 2020, 14, 807–818. [Google Scholar] [CrossRef]
- Kim, H.S.; Sun, X.; Lee, J.-H.; Kim, H.-W.; Fu, X.; Leong, K.W. Advanced Drug Delivery Systems and Artificial Skin Grafts for Skin Wound Healing. Adv. Drug Deliv. Rev. 2019, 146, 209–239. [Google Scholar] [CrossRef]
- Ren, J.; Yang, M.; Chen, J.; Ma, S.; Wang, N. Anti-Inflammatory and Wound Healing Potential of Kirenol in Diabetic Rats through the Suppression of Inflammatory Markers and Matrix Metalloproteinase Expressions. Biomed. Pharmacother. 2020, 129, 110475. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Gao, X.; Zhu, Z.; Hu, X.; Zhou, H.; Liu, J. The Roles of Nasal Nitric Oxide in Diagnosis and Endotypes of Chronic Rhinosinusitis with Nasal Polyps. J. Otolaryngol. Head Neck Surg. 2020, 49, 68. [Google Scholar] [CrossRef] [PubMed]
- Takeno, S.; Hirakawa, K.; Ishino, T. Pathological Mechanisms and Clinical Features of Eosinophilic Chronic Rhinosinusitis in the Japanese Population. Allergol. Int. 2010, 59, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Sakashita, M.; Haruna, T.; Asaka, D.; Takeno, S.; Ikeda, H.; Nakayama, T.; Seki, N.; Ito, S.; Murata, J.; et al. Novel Scoring System and Algorithm for Classifying Chronic Rhinosinusitis: The JESREC Study. Allergy 2015, 70, 995–1003. [Google Scholar] [CrossRef]
- Kurokawa, R.; Kanemitsu, Y.; Fukumitsu, K.; Takeda, N.; Yap, J.M.; Ozawa, Y.; Masaki, A.; Ono, J.; Izuhara, K.; Nishiyama, H.; et al. Nasal Polyp Eosinophilia and FeNO May Predict Asthma Symptoms Development after Endoscopic Sinus Surgery in CRS Patients without Asthma. J. Asthma 2021, 15. [Google Scholar] [CrossRef]
- Kambara, R.; Minami, T.; Akazawa, H.; Tsuji, F.; Sasaki, T.; Inohara, H.; Horii, A. Lower Airway Inflammation in Eosinophilic Chronic Rhinosinusitis as Determined by Exhaled Nitric Oxide. Int. Arch. Allergy Immunol. 2017, 173, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, J.F.; Shan, J.; Tewfik, M.; Hamid, Q.; Frenkiel, S.; Eidelman, D.H. Protein Nitration in Chronic Sinusitis and Nasal Polyposis: Role of Eosinophils. Otolaryngol. Neck Surg. 2004, 131, 696–703. [Google Scholar] [CrossRef]
- Naraghi, M.; Deroee, A.F.; Ebrahimkhani, M.R.; Kiani, S.; Dehpour, A.R. Nitric Oxide: A New Concept in Chronic Sinusitis Pathogenesis. Am. J. Otolaryngol. 2007, 28, 334–337. [Google Scholar] [CrossRef]
- Grayson, J.W.; Li, W.; Ho, J.; Alvarado, R.; Rimmer, J.; Sewell, W.A.; Harvey, R.J. Topography of Polyp Recurrence in Eosinophilic Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2020, 10, 604–609. [Google Scholar] [CrossRef]
- Frendø, M.; Hakansson, K.; Schwer, S.; Ravn, A.; Meteran, H.; Porsbjerg, C.; Backer, V.; von Buchwald, C. Exhaled and Nasal Nitric Oxide in Chronic Rhinosinusitis Patients with Nasal Polyps in Primary Care. Rhinol. J. 2018, 56, 59–64. [Google Scholar] [CrossRef]
- Alexandersson, C.; Tuomi, L.; Olin, A.-C. Measurement of Nasal Nitric Oxide in Chronic Rhinosinusitis and Its Relationship to Patient-Reported Outcome: A Longitudinal Pilot Study. Ear Nose Throat J. 2019, 145561319880624. [Google Scholar] [CrossRef]
- Fu, C.-H.; Tseng, H.-J.; Huang, C.-C.; Chang, P.-H.; Chen, Y.-W.; Lee, T.-J. Nasal Nitric Oxide in Unilateral Sinus Disease. PLoS ONE 2017, 12, e0171965. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Yip, J.; Lee, J.M. Nasal Nitric Oxide as a Long-Term Monitoring and Prognostic Biomarker of Mucosal Health in Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2020, 10, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Collette, J.R.; Zhou, H.; Lorenz, M.C. Candida Albicans Suppresses Nitric Oxide Generation from Macrophages via a Secreted Molecule. PLoS ONE 2014, 9, e96203. [Google Scholar] [CrossRef] [PubMed]
- Luiking, Y.C.; Ten Have, G.A.; Wolfe, R.R.; Deutz, N.E. Arginine De Novo and Nitric Oxide Production in Disease States. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E1177–E1189. [Google Scholar] [CrossRef] [PubMed]
- Lara, A.; Khatri, S.B.; Wang, Z.; Comhair, S.A.; Xu, W.; Dweik, R.A.; Bodine, M.; Levison, B.S.; Hammel, J.; Bleecker, E.; et al. National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. Alterations of the Arginine Metabolome in Asthma. Am. J. Respir. Crit. Care Med. 2008, 178, 673–681. [Google Scholar] [CrossRef]
- Maarsingh, H.; Dekkers, B.G.J.; Zuidhof, A.B.; Bos, I.S.T.; Menzen, M.H.; Klein, T.; Flik, G.; Zaagsma, J.; Meurs, H.; Maarsingh, H.; et al. Increased Arginase Activity Contributes to Airway Remodelling in Chronic Allergic Asthma. Eur. Respir. J. 2011, 38, 318–328. [Google Scholar] [CrossRef]
- Cho, W.S.; Kim, T.H.; Kim, K.H.; Lee, H.M.; Lee, S.H.; Ju, Y.H.; Park, E.H.; Kim, K.W.; Lee, S.H. Increased Expression of Arginase I and II in Allergic Nasal Mucosa. Laryngoscope 2011, 121, 236–240. [Google Scholar] [CrossRef]
- Taruya, T.; Takeno, S.; Kubota, K.; Sasaki, A.; Ishino, T.; Hirakawa, K. Comparison of Arginase Isoform Expression in Patients with Different Subtypes of Chronic Rhinosinusitis. J. Laryngol. Otol. 2015, 129, 1194–1200. [Google Scholar] [CrossRef][Green Version]
- Vlad, D.; Albu, S. Arginase Isoform Expression in Chronic Rhinosinusitis. J. Clin. Med. 2019, 8, 1809. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawasumi, T.; Takeno, S.; Ishikawa, C.; Takahara, D.; Taruya, T.; Takemoto, K.; Hamamoto, T.; Ishino, T.; Ueda, T. The Functional Diversity of Nitric Oxide Synthase Isoforms in Human Nose and Paranasal Sinuses: Contrasting Pathophysiological Aspects in Nasal Allergy and Chronic Rhinosinusitis. Int. J. Mol. Sci. 2021, 22, 7561. https://doi.org/10.3390/ijms22147561
Kawasumi T, Takeno S, Ishikawa C, Takahara D, Taruya T, Takemoto K, Hamamoto T, Ishino T, Ueda T. The Functional Diversity of Nitric Oxide Synthase Isoforms in Human Nose and Paranasal Sinuses: Contrasting Pathophysiological Aspects in Nasal Allergy and Chronic Rhinosinusitis. International Journal of Molecular Sciences. 2021; 22(14):7561. https://doi.org/10.3390/ijms22147561
Chicago/Turabian StyleKawasumi, Tomohiro, Sachio Takeno, Chie Ishikawa, Daisuke Takahara, Takayuki Taruya, Kota Takemoto, Takao Hamamoto, Takashi Ishino, and Tsutomu Ueda. 2021. "The Functional Diversity of Nitric Oxide Synthase Isoforms in Human Nose and Paranasal Sinuses: Contrasting Pathophysiological Aspects in Nasal Allergy and Chronic Rhinosinusitis" International Journal of Molecular Sciences 22, no. 14: 7561. https://doi.org/10.3390/ijms22147561
APA StyleKawasumi, T., Takeno, S., Ishikawa, C., Takahara, D., Taruya, T., Takemoto, K., Hamamoto, T., Ishino, T., & Ueda, T. (2021). The Functional Diversity of Nitric Oxide Synthase Isoforms in Human Nose and Paranasal Sinuses: Contrasting Pathophysiological Aspects in Nasal Allergy and Chronic Rhinosinusitis. International Journal of Molecular Sciences, 22(14), 7561. https://doi.org/10.3390/ijms22147561